
Systemic Changes in Endocannabinoids and Endocannabinoid-like Molecules in Response to Partial Nephrectomy-Induced Ischemia in Humans

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Results
2.1. Renal Function and Surgical Data
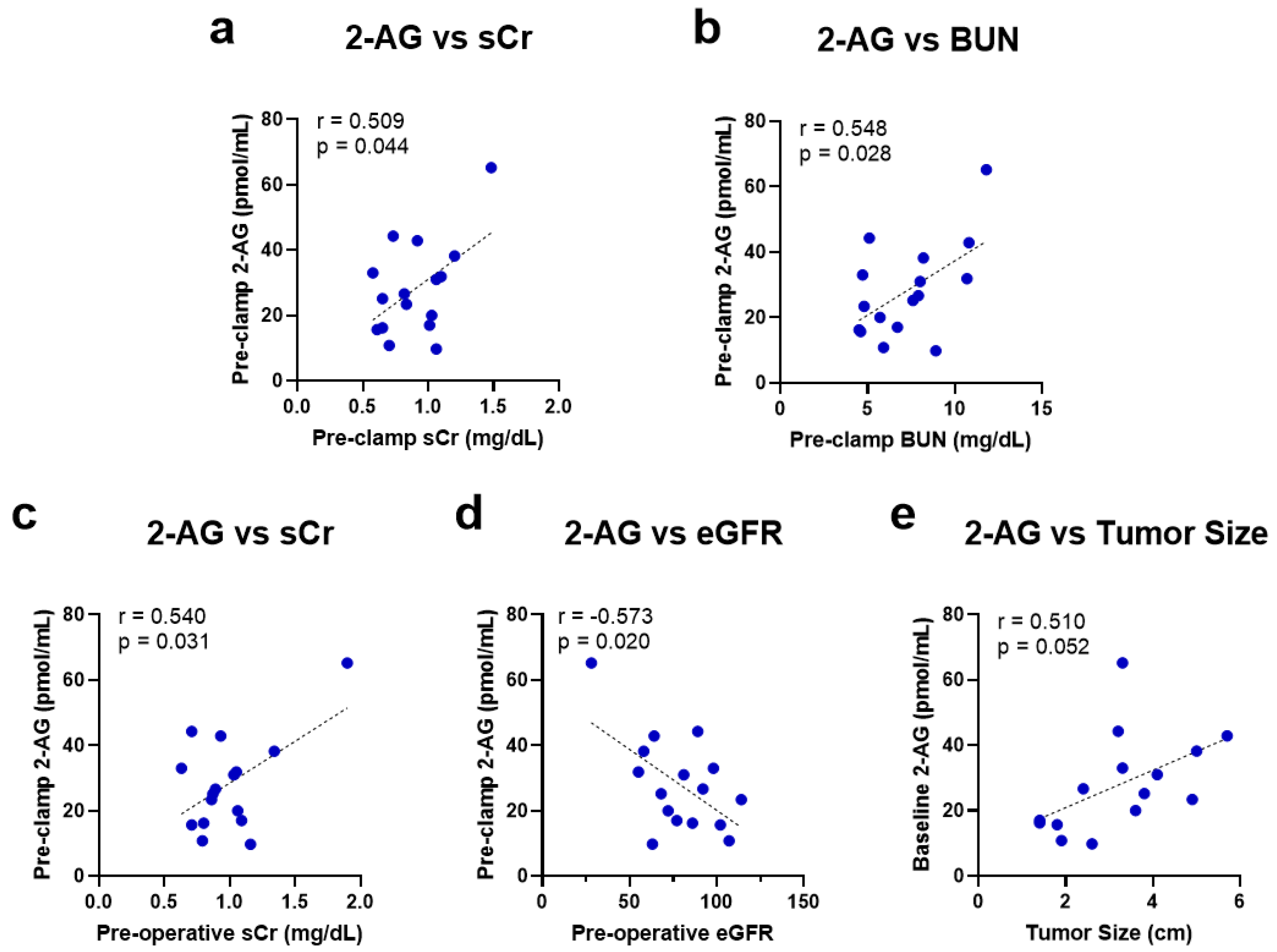
2.2. Baseline Kidney Function Correlates with Higher 2-AG Levels
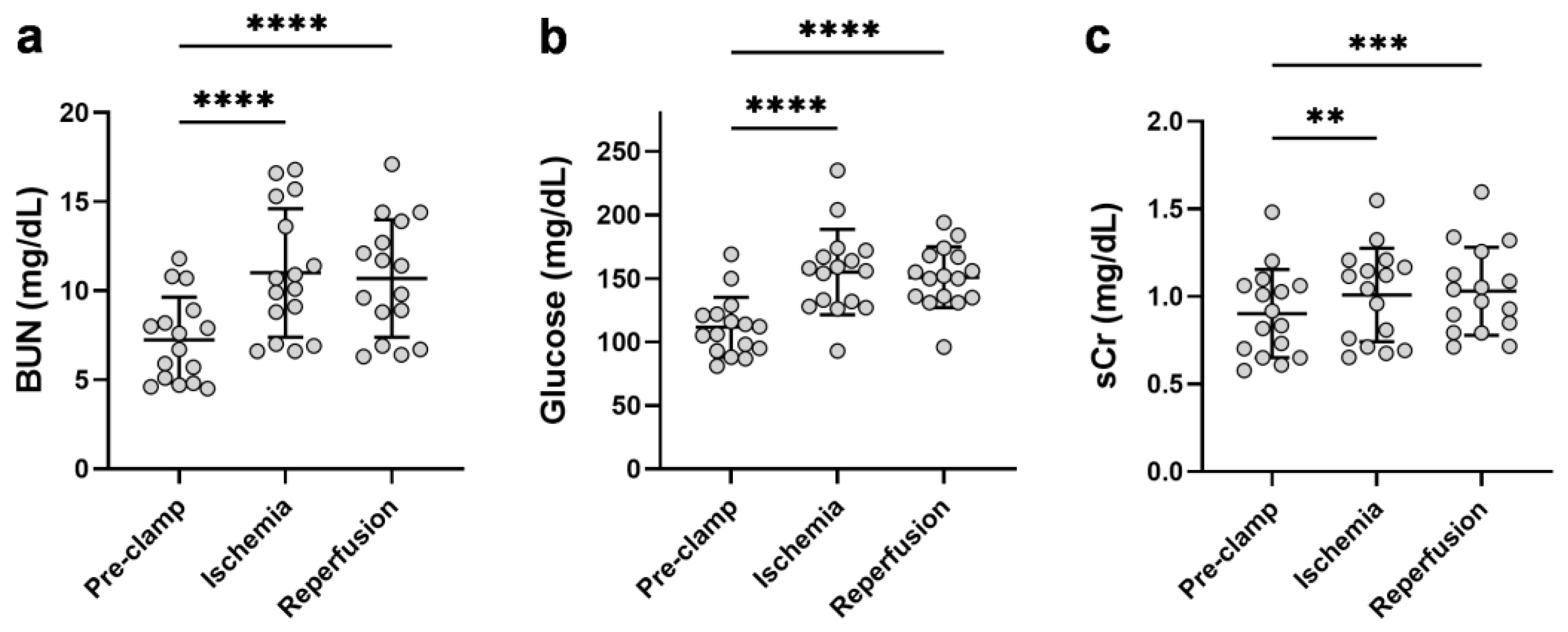
2.3. Unilateral Ischemia Increases the Circulating Kidney Dysfunction Parameters
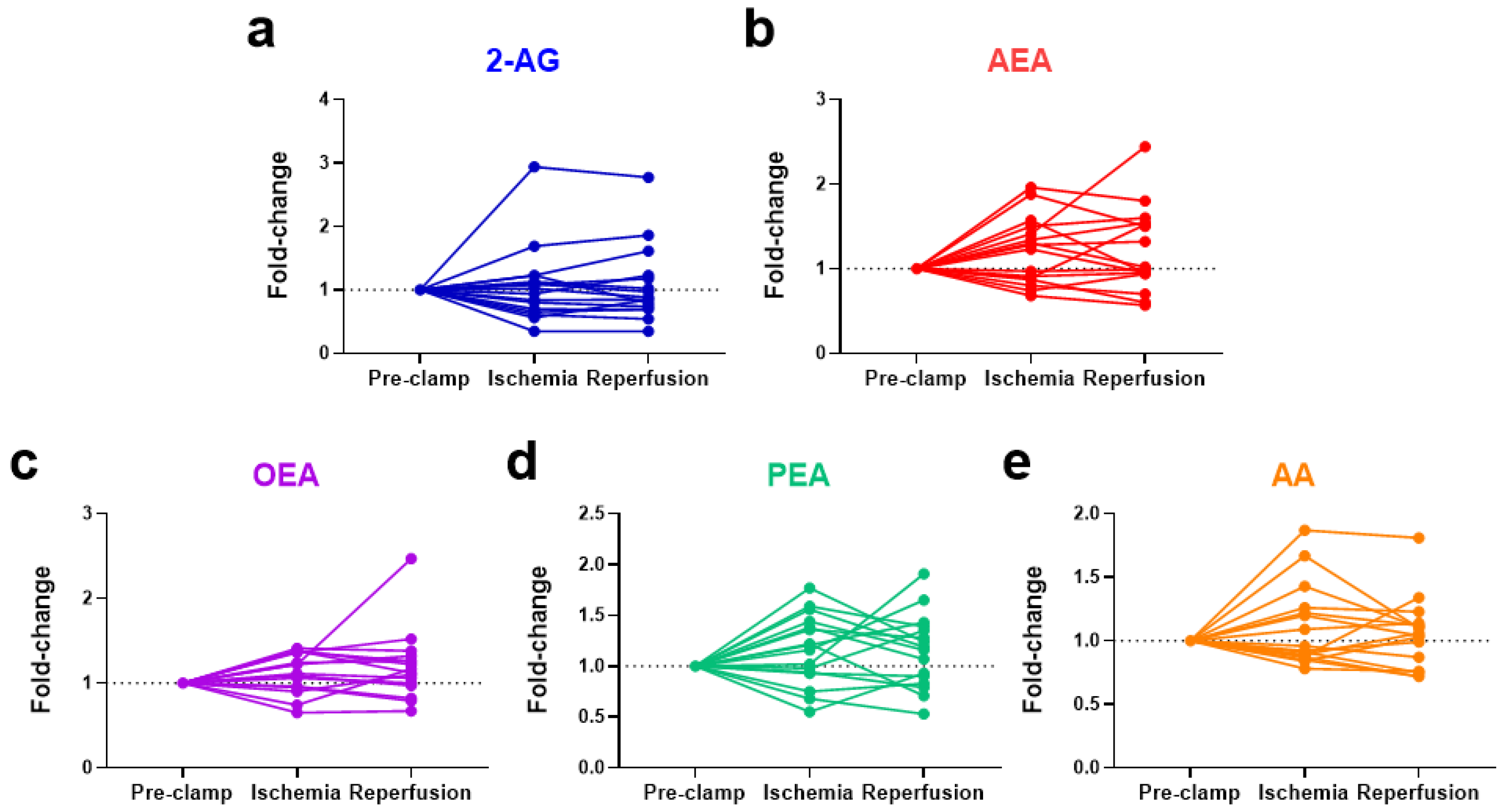
2.4. Ischemia Increases Circulating N-Acylethanolamines in Non-Obese Patients
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Study Protocol
4.3. Biochemistry Measurements
4.4. Endocannabinoid Extraction and Measurement by LCMS/MS
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Serum Creatinine (mg/dL) | |||||
|---|---|---|---|---|---|
| Subject No. | Pre-Operation | 24 h Post-Operation | Maximal Value within 48 h Post-Operation | Maximal Change 48 h Post-Operation | Long-Term Follow-Up (Days Post-Operation) |
| 1 | 1.16 | 1.08 | 1.08 | −0.08 | 1.3 (114) |
| 2 | 0.79 | 0.65 | 0.65 | −0.14 | 0.7 (114) |
| 3 | 0.87 | 0.92 | 0.92 | 0.05 | 0.81 (133) |
| 4 | 1.03 | 1.62 | 2.3 | 1.27 * | 1.17 (140) |
| 5 | 0.71 | 0.69 | 0.74 | 0.03 | 0.79 (166) |
| 6 | 1.06 | 1.05 | 1.05 | −0.01 | N/A |
| 7 | 1.34 | 1.51 | 1.51 | 0.17 | 1.4 (205) |
| 8 | 0.63 | 0.84 | 0.84 | 0.21 | 0.62 (179) |
| 9 | 0.80 | 0.73 | 0.73 | −0.07 | 0.77 (137) |
| 10 | 1.05 | 1.28 | 1.28 | 0.23 | 1.25 (22) |
| 11 | 0.71 | 0.7 | 0.7 | −0.01 | 0.8 (23) |
| 12 | 0.89 | 0.9 | 0.9 | 0.01 | 0.81 (130) |
| 13 | 1.90 | 1.92 | 2.28 | 0.38 * | 1.3 (141) |
| 14 | 1.09 | 1.1 | 1.1 | 0.01 | 1.19 (174) |
| 15 | 0.93 | 1.2 | 1.2 | 0.27 | 0.9 (101) |
| 16 | 0.86 | 1.49 | 1.71 | 0.85 * | 1.3 (21) |
| eGFR (mL/min per 1.73 m2) | |||||
|---|---|---|---|---|---|
| Subject No. | Pre-Operation | 24 h Post-Operation | Minimal Value within 48 h Post-Operation | Maximal Change 48 h Post-Operation | Long-Term Follow-Up (Days Post-Operation) |
| 1 | 63 | 73 | 73 | 10 | 56 (114) |
| 2 | 107 | 107 | 107 | 0 | 102 (114) |
| 3 | 68 | 63 | 63 | −5 | 74 (133) |
| 4 | 81 | 47 | 29 | −52 | 69 (140) |
| 5 | 89 | 90 | 84 | −5 | 78 (166) |
| 6 | 72 | 73 | 73 | 1 | N/A |
| 7 | 58 | 51 | 51 | −7 | 55 (205) |
| 8 | 98 | 77 | 77 | −21 | 99 (179) |
| 9 | 86 | 96 | 96 | 10 | 91 (137) |
| 10 | 55 | 44 | 44 | −11 | 47 (22) |
| 11 | 102 | 104 | 104 | 2 | 89 (23) |
| 12 | 92 | 92 | 92 | 0 | 94 (130) |
| 13 | 28 | 28 | 14 | −14 | 44 (141) |
| 14 | 77 | 76 | 76 | −1 | 69 (174) |
| 15 | 64 | 47 | 47 | −17 | 66 (101) |
| 16 | 114 | 62 | 52 | −62 | 73 (21) |
| Subject No. | 2-AG (pmol/mL) | AEA (pmol/mL) | OEA (pmol/mL) | PEA (pmol/mL) | AA (pmol/mL) |
|---|---|---|---|---|---|
| 1 | 9.8 | 0.621 | 12.4 | 13.9 | 1056 |
| 2 | 10.8 | 0.238 | 9.3 | 7.5 | 1155 |
| 3 | 25.2 | 0.477 | 13.6 | 9.7 | 2285 |
| 4 | 31.0 | 0.432 | 10.6 | 6.9 | 1227 |
| 5 | 44.3 | 0.821 | 19.1 | 8.6 | 2084 |
| 6 | 20.0 | 0.484 | 12.3 | 7.6 | 1399 |
| 7 | 38.2 | 0.429 | 9.7 | 5.9 | 1537 |
| 8 | 33.0 | 0.893 | 19.6 | 14.3 | 1614 |
| 9 | 16.2 | 0.376 | 17.1 | 20.8 | 2088 |
| 10 | 31.9 | 0.334 | 14.1 | 9.0 | 1576 |
| 11 | 15.7 | 0.807 | 22.2 | 11.5 | 1413 |
| 12 | 26.7 | 0.605 | 17.6 | 14.7 | 1947 |
| 13 | 65.2 | 0.826 | 13.8 | 11.0 | 2183 |
| 14 | 17.0 | 0.745 | 12.8 | 8.0 | 2524 |
| 15 | 42.9 | 1.190 | 22.5 | 18.3 | 1778 |
| 16 | 23.4 | 0.527 | 13.5 | 8.1 | 1923 |
| Serum Glucose (mg/dL) | ||||
|---|---|---|---|---|
| Subject No. | Pre-Operation | 24 h Post-Operation | Maximal Value within 48 h Post-Operation | Maximal Change 48 h Post-Operation |
| 1 | 105 | 102 | 102 | −3 |
| 2 | 122 | 117 | 117 | −5 |
| 3 | 132 | 97 | 127 | −5 |
| 4 | 91 | 151 | 290 | 199 |
| 5 | 102 | 95 | 95 | −7 |
| 6 | 82 | 173 | 173 | 91 |
| 7 | 100 | 108 | 108 | 8 |
| 8 | 103 | 94 | 94 | −9 |
| 9 | 116 | 119 | 119 | 3 |
| 10 | 96 | 146 | 146 | 50 |
| 11 | 100 | 112 | 122 | 22 |
| 12 | 93 | 96 | 96 | 3 |
| 13 | 184 | 153 | 153 | −31 |
| 14 | 122 | 109 | 109 | −13 |
| 15 | 125 | 127 | 127 | 2 |
| 16 | 106 | 127 | 136 | 30 |
| Analyte | Molecular Ion [M + H] + [M − H]− for AA [m/z] | Fragment [m/z] | DP [volts] | CE [volts] | CXP [volts] |
|---|---|---|---|---|---|
| 2-AG | 379.2 | 287.1 (quantifier) | 70 | 19 | 14 |
| 91 (qualifier) | 70 | 67 | 10 | ||
| AEA | 348.2 | 287.1 (quantifier) | 26 | 13 | 16 |
| 62 (qualifier) | 26 | 13 | 8 | ||
| PEA | 300.3 | 283.2 (quantifier) | 130 | 19 | 24 |
| 62 (qualifier) | 130 | 17 | 8 | ||
| AA | 305.3 | 91 (quantifier) | 1 | 49 | 10 |
| 287.1 (qualifier) | 1 | 13 | 22 | ||
| OEA | 326.3 | 61.9 (quantifier) | 146 | 21 | 24 |
| 309.1 (qualifier) | 146 | 21 | 42 | ||
| d4-AEA | 352.3 | 287.1 (quantifier) | 66 | 15 | 20 |
| 66 (qualifier) | 66 | 21 | 8 |
References
- Ljungberg, B.; Albiges, L.; Abu-Ghanem, Y.; Bensalah, K.; Dabestani, S.; Montes, S.F.P.; Giles, R.H.; Hofmann, F.; Hora, M.; Kuczyk, M.A.; et al. European Association of Urology Guidelines on Renal Cell Carcinoma: The 2019 Update. Eur. Urol. 2019, 75, 799–810. [Google Scholar] [CrossRef] [PubMed]
- Greco, F.; Autorino, R.; Altieri, V.; Campbell, S.; Ficarra, V.; Gill, I.; Kutikov, A.; Mottrie, A.; Mirone, V.; van Poppel, H. Ischemia Techniques in Nephron-Sparing Surgery: A Systematic Review and Meta-Analysis of Surgical, Oncological, and Functional Outcomes. Eur. Urol. 2019, 75, 477–491. [Google Scholar] [CrossRef] [PubMed]
- Volpe, A.; Blute, M.L.; Ficarra, V.; Gill, I.S.; Kutikov, A.; Porpiglia, F.; Rogers, C.; Touijer, K.A.; van Poppel, H.; Thompson, R.H. Renal Ischemia and Function after Partial Nephrectomy: A Collaborative Review of the Literature. Eur. Urol. 2015, 68, 61–74. [Google Scholar] [CrossRef]
- Parekh, D.J.; Weinberg, J.M.; Ercole, B.; Torkko, K.C.; Hilton, W.; Bennett, M.; Devarajan, P.; Venkatachalam, M.A. Tolerance of the Human Kidney to Isolated Controlled Ischemia. J. Am. Soc. Nephrol. 2013, 24, 506–517. [Google Scholar] [CrossRef] [Green Version]
- Kallingal, G.J.S.; Weinberg, J.M.; Reis, I.M.; Nehra, A.; Venkatachalam, M.A.; Parekh, D.J. Long-Term Response to Renal Ischaemia in the Human Kidney after Partial Nephrectomy: Results from a Prospective Clinical Trial. BJU Int. 2016, 117, 766–774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Z.; Zhao, J.; Dong, W.; Remer, E.; Li, J.; Demirjian, S.; Zabell, J.; Campbell, S.C. Acute Kidney Injury after Partial Nephrectomy: Role of Parenchymal Mass Reduction and Ischemia and Impact on Subsequent Functional Recovery. Eur. Urol. 2016, 69, 745–752. [Google Scholar] [CrossRef]
- Pacher, P.; Haskó, G. Endocannabinoids and Cannabinoid Receptors in Ischaemia-Reperfusion Injury and Preconditioning. Br. J. Pharmacol. 2008, 153, 252–262. [Google Scholar] [CrossRef] [Green Version]
- Tsuboi, K.; Uyama, T.; Okamoto, Y.; Ueda, N. Endocannabinoids and Related N-Acylethanolamines: Biological Activities and Metabolism. Inflamm. Regen. 2018, 38, 28. [Google Scholar] [CrossRef]
- Dao, M.; François, H. Cannabinoid Receptor 1 Inhibition in Chronic Kidney Disease: A New Therapeutic Toolbox. Front. Endocrinol. 2021, 12, 830. [Google Scholar] [CrossRef]
- Li, X.H.; Liu, Y.Q.; Gong, D.Y.; Hai, K.R.; Ke, B.W.; Zuo, Y.X. The Critical Role of Cannabinoid Receptor 2 in URB602-Induced Protective Effects against Renal Ischemia-Reperfusion Injury in the Rat. Shock 2020, 54, 520–530. [Google Scholar] [CrossRef]
- Moradi, H.; Oveisi, F.; Khanifar, E.; Moreno-Sanz, G.; Vaziri, N.D.; Piomelli, D. Increased Renal 2-Arachidonoylglycerol Level Is Associated with Improved Renal Function in a Mouse Model of Acute Kidney Injury. Cannabis Cannabinoid Res. 2016, 1, 218–228. [Google Scholar] [CrossRef]
- Sampaio, L.S.; Iannotti, F.A.; Veneziani, L.; Borelli-Tôrres, R.T.; de Maio, F.; Piscitelli, F.; Reis, R.A.M.; di Marzo, V.; Einicker-Lamas, M. Experimental Ischemia/Reperfusion Model Impairs Endocannabinoid Signaling and Na + /K + ATPase Expression and Activity in Kidney Proximal Tubule Cells. Biochem. Pharmacol 2018, 154, 482–491. [Google Scholar] [CrossRef]
- Zhou, S.; Wu, Q.; Lin, X.; Ling, X.; Miao, J.; Liu, X.; Hu, C.; Zhang, Y.; Jia, N.; Hou, F.F.; et al. Cannabinoid Receptor Type 2 Promotes Kidney Fibrosis through Orchestrating β-Catenin Signaling. Kidney Int. 2021, 99, 364–381. [Google Scholar] [CrossRef] [PubMed]
- Eltzschig, H.K.; Eckle, T. Ischemia and Reperfusion—From Mechanism to Translation. Nat. Med. 2011, 17, 1391–1401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soranno, D.E.; Gil, H.W.; Kirkbride-Romeo, L.; Altmann, C.; Montford, J.R.; Yang, H.; Levine, A.; Buchanan, J.; Faubel, S. Matching Human Unilateral AKI, a Reverse Translational Approach to Investigate Kidney Recovery after Ischemia. J. Am. Soc. Nephrol. 2019, 30, 990–1005. [Google Scholar] [CrossRef] [PubMed]
- Spaliviero, M.; Power, N.E.; Murray, K.S.; Sjoberg, D.D.; Benfante, N.E.; Bernstein, M.L.; Wren, J.; Russo, P.; Coleman, J.A. Intravenous Mannitol versus Placebo during Partial Nephrectomy in Patients with Normal Kidney Function: A Double-Blind, Clinically-Integrated, Randomized Trial. Eur. Urol. 2018, 73, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Zabell, J.; Isharwal, S.; Dong, W.; Abraham, J.; Wu, J.; Suk-Ouichai, C.; Palacios, D.A.; Remer, E.; Li, J.; Campbell, S.C. Acute Kidney Injury after Partial Nephrectomy of Solitary Kidneys: Impact on Long-Term Stability of Renal Function. J. Urol. 2018, 200, 1295–1301. [Google Scholar] [CrossRef]
- Lane, B.R.; Campbell, S.C.; Demirjian, S.; Fergany, A.F. Surgically Induced Chronic Kidney Disease May Be Associated with a Lower Risk of Progression and Mortality than Medical Chronic Kidney Disease. J. Urol. 2013, 189, 1649–1655. [Google Scholar] [CrossRef]
- Hillard, C.J. Circulating Endocannabinoids: From Whence Do They Come and Where Are They Going. Neuropsychopharmacol. Rev. 2017, 43, 155–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deutsch, D.G.; Goligorsky, M.S.; Schmid, P.C.; Krebsbach, R.J.; Schmid, H.H.O.; Das, S.K.; Dey, S.K.; Arreaza, G.; Thorup, C.; Stefano, G.; et al. Production and Physiological Actions of Anandamide in the Vasculature of the Rat Kidney. J. Clin. Investig. 1997, 100, 1538–1546. [Google Scholar] [CrossRef] [Green Version]
- Koura, Y.; Ichihara, A.; Tada, Y.; Kaneshiro, Y.; Okada, H.; Temm, C.J.; Hayashi, M.; Saruta, T. Anandamide Decreases Glomerular Filtration Rate through Predominant Vasodilation of Efferent Arterioles in Rat Kidneys. J. Am. Soc. Nephrol. 2004, 15, 1488–1494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.; Wang, W.; Poklis, J.L.; Lichtman, A.H.; Ritter, J.K.; Hu, G.; Xie, D.; Li, N. Inactivation of Fatty Acid Amide Hydrolase Protects against Ischemic Reperfusion Injury-Induced Renal Fibrogenesis. Biochim. Biophys. Acta Mol. Basis Dis. 2022, 1868, 166456. [Google Scholar] [CrossRef] [PubMed]
- di Paola, R.; Impellizzeri, D.; Mondello, P.; Velardi, E.; Aloisi, C.; Cappellani, A.; Esposito, E.; Cuzzocrea, S. Palmitoylethanolamide Reduces Early Renal Dysfunction and Injury Caused by Experimental Ischemia and Reperfusion in Mice. Shock 2012, 38, 356–366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cravatt, B.F.; Demarest, K.; Patricelli, M.P.; Bracey, M.H.; Giang, D.K.; Martin, B.R.; Lichtman, A.H. Supersensitivity to Anandamide and Enhanced Endogenous Cannabinoid Signaling in Mice Lacking Fatty Acid Amide Hydrolase. Proc. Natl. Acad. Sci. USA 2001, 98, 9371–9376. [Google Scholar] [CrossRef] [Green Version]
- Fanelli, F.; Mezzullo, M.; Repaci, A.; Belluomo, I.; Ibarra Gasparini, D.; di Dalmazi, G.; Mastroroberto, M.; Vicennati, V.; Gambineri, A.; Morselli-Labate, A.M.; et al. Profiling Plasma N-Acylethanolamine Levels and Their Ratios as a Biomarker of Obesity and Dysmetabolism. Mol. Metab. 2018, 14, 82–94. [Google Scholar] [CrossRef]
- Renehan, A.G.; Tyson, M.; Egger, M.; Heller, R.F.; Zwahlen, M. Body-Mass Index and Incidence of Cancer: A Systematic Review and Meta-Analysis of Prospective Observational Studies. Lancet 2008, 371, 569–578. [Google Scholar] [CrossRef]
- Tartakover Matalon, S.; Azar, S.; Meiri, D.; Hadar, R.; Nemirovski, A.; Abu Jabal, N.; Konikoff, F.M.; Drucker, L.; Tam, J.; Naftali, T. Endocannabinoid Levels in Ulcerative Colitis Patients Correlate with Clinical Parameters and Are Affected by Cannabis Consumption. Front. Endocrinol. 2021, 12, 685289. [Google Scholar] [CrossRef]
- Pagano, C.; Navarra, G.; Coppola, L.; Bifulco, M.; Laezza, C. Molecular Mechanism of Cannabinoids in Cancer Progression. Int. J. Mol. Sci. 2021, 22, 3680. [Google Scholar] [CrossRef]
- Larrinaga, G.; Sanz, B.; Pérez, I.; Blanco, L.; Cándenas, M.L.; Pinto, F.M.; Gil, J.; López, J.I. Cannabinoid CB1 Receptor Is Downregulated in Clear Cell Renal Cell Carcinoma. J. Histochem. Cytochem. 2010, 58, 1129–1134. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Xu, Y.; Zhu, L.; Zou, Y.; Kong, W.; Dong, B.; Huang, J.; Chen, Y.; Xue, W.; Huang, Y.; et al. Cannabinoid Receptor 2 as a Novel Target for Promotion of Renal Cell Carcinoma Prognosis and Progression. J. Cancer Res. Clin. Oncol. 2018, 144, 39–52. [Google Scholar] [CrossRef]
- Wang, J.; Xu, Y.; Zou, Y.; Zhu, L.; Dong, B.; Huang, J.; Chen, Y.; Xue, W.; Huang, Y.; Kong, W.; et al. Overexpression of Cannabinoid Receptor 1 Promotes Renal Cell Carcinoma Progression. Tumour Biol. 2016, 37, 16237–16247. [Google Scholar] [CrossRef] [PubMed]





| Parameters | n = 16 |
|---|---|
| Demographic Data | |
| Age (years) | 68 (37–79) |
| Women, n (%) | 8 (50) |
| BMI (kg/m2) | 27.8 (22.5–40.1) |
| Hypertension, n (%) | 7 (44) |
| Diabetes mellitus, n (%) | 4 (25) |
| Renal Functional and Tumor Data | |
| Creatinine (serum) (mg/dL) | 0.91 (0.63–1.90) |
| eGFR (mL/min per 1.73 m2) | 79 (28–114) |
| BUN (mg/dL) | 7.2 (4.5–11.8) |
| Tumor Size 1 (cm) | 3.3 (1.4–5.7) |
| RCC Pathology, n (%) | |
| Clear cell RCC | 9 (56) |
| Papillary RCC | 4 (25) |
| Oncocytoma | 3 (19) |
| Surgical Data | |
| Surgical Technique | |
| Robotic intraperitoneal | 11 (69) |
| Robotic extraperitoneal | 4 (25) |
| Open | 1 (6) |
| Ischemia Time (min) | 19 (8–32) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rothner, A.; Gov, T.; Hinden, L.; Nemirovski, A.; Tam, J.; Rosenzweig, B. Systemic Changes in Endocannabinoids and Endocannabinoid-like Molecules in Response to Partial Nephrectomy-Induced Ischemia in Humans. Int. J. Mol. Sci. 2023, 24, 4216. https://doi.org/10.3390/ijms24044216
Rothner A, Gov T, Hinden L, Nemirovski A, Tam J, Rosenzweig B. Systemic Changes in Endocannabinoids and Endocannabinoid-like Molecules in Response to Partial Nephrectomy-Induced Ischemia in Humans. International Journal of Molecular Sciences. 2023; 24(4):4216. https://doi.org/10.3390/ijms24044216
Chicago/Turabian StyleRothner, Ariel, Tom Gov, Liad Hinden, Alina Nemirovski, Joseph Tam, and Barak Rosenzweig. 2023. "Systemic Changes in Endocannabinoids and Endocannabinoid-like Molecules in Response to Partial Nephrectomy-Induced Ischemia in Humans" International Journal of Molecular Sciences 24, no. 4: 4216. https://doi.org/10.3390/ijms24044216
APA StyleRothner, A., Gov, T., Hinden, L., Nemirovski, A., Tam, J., & Rosenzweig, B. (2023). Systemic Changes in Endocannabinoids and Endocannabinoid-like Molecules in Response to Partial Nephrectomy-Induced Ischemia in Humans. International Journal of Molecular Sciences, 24(4), 4216. https://doi.org/10.3390/ijms24044216