
Myeloperoxidase PET Imaging Tracks Intracellular and Extracellular Treatment Changes in Experimental Myocardial Infarction

 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
2.1. Radiochemistry
2.2. 18F-MAPP Can Cross the Cell Membrane
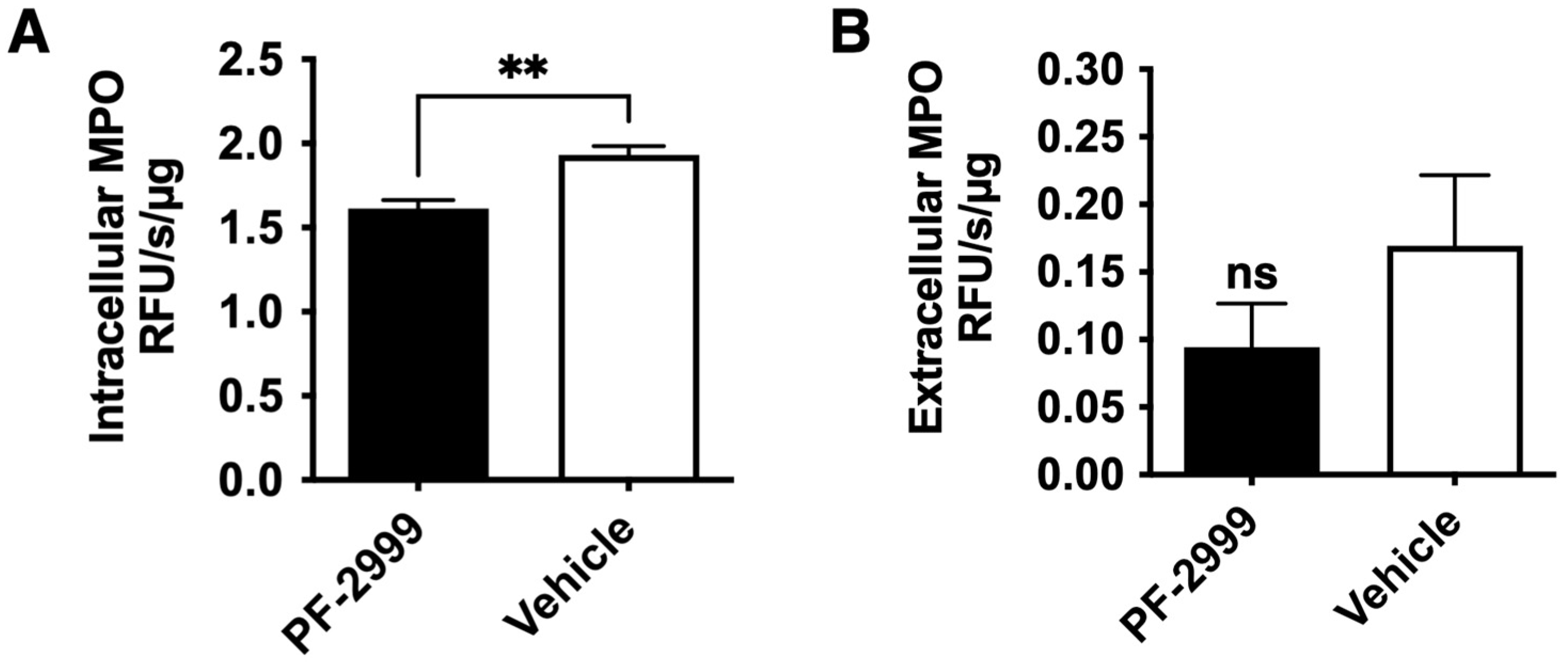
2.3. 18F-MAPP Can Monitor the Treatment Effect of MPO Inhibitor PF-2999
2.4. 18F-MAPP Imaging Correlates with Both Intracellular and Extracellular MPO Activities in MI
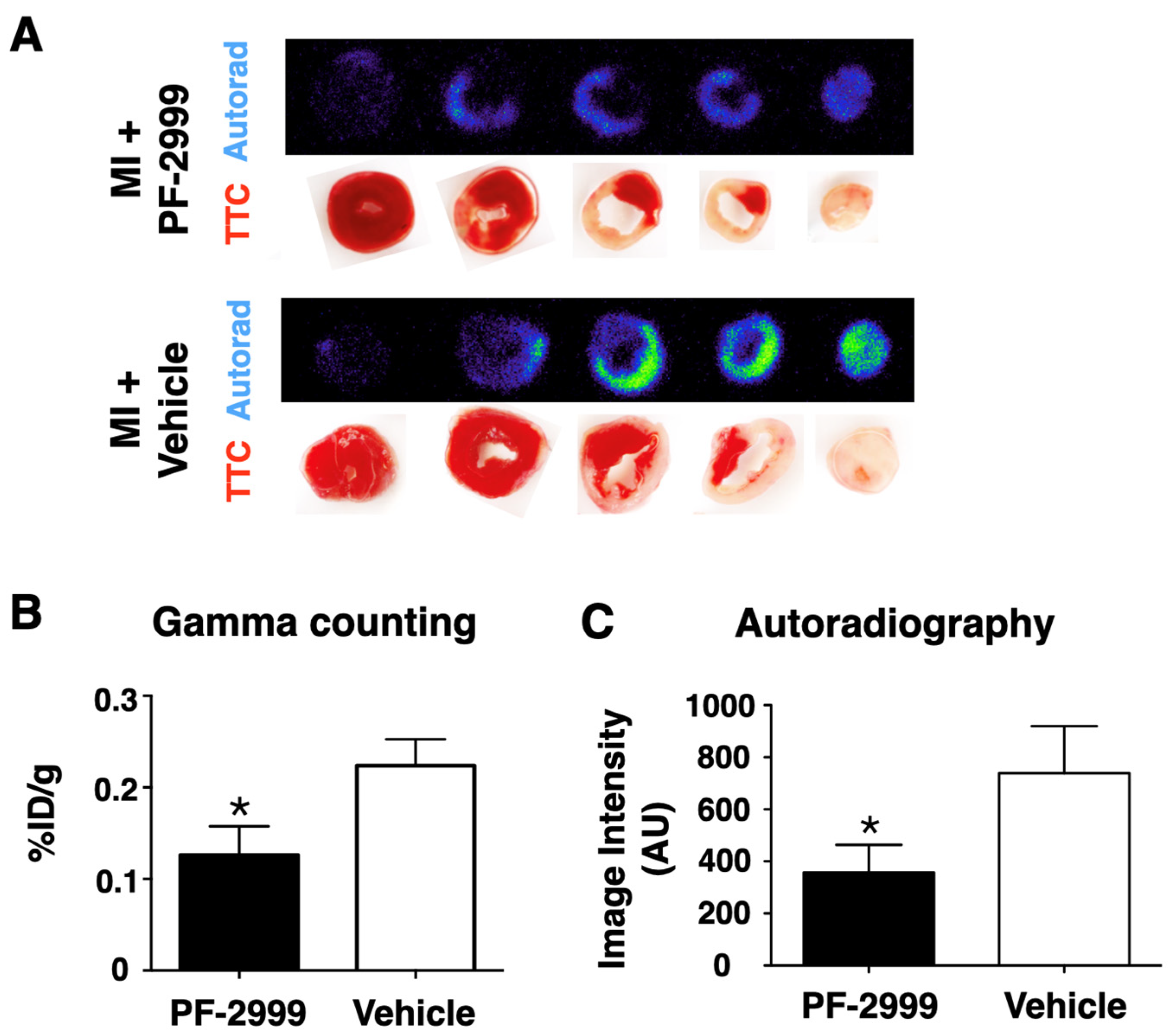
2.5. 18F-MAPP Imaging Correlates with Ex Vivo Validation in MI
3. Discussion
4. Materials and Methods
4.1. Chemicals and Radiochemistry
4.2. Cell Penetration
4.3. Myocardial Infarction (MI) and Treatment with PF-2999
4.4. PET-CT Imaging
4.5. Autoradiography
4.6. MPO Activity Assay
4.7. Statistical Analysis
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Saleh, M.; Ambrose, J.A. Understanding myocardial infarction. F1000Research 2018, 7, 1378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerber, Y.; Weston, S.A.; Berardi, C.; McNallan, S.M.; Jiang, R.; Redfield, M.M.; Roger, V.L. Contemporary Trends in Heart Failure With Reduced and Preserved Ejection Fraction After Myocardial Infarction: A Community Study. Am. J. Epidemiology 2013, 178, 1272–1280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Velagaleti, R.S.; Pencina, M.J.; Murabito, J.; Wang, T.; Parikh, N.I.; D’Agostino, R.B.; Levy, D.; Kannel, W.B.; Vasan, R.S. Long-Term Trends in the Incidence of Heart Failure After Myocardial Infarction. Circulation 2008, 118, 2057–2062. [Google Scholar] [CrossRef] [PubMed]
- Swirski, F.K.; Nahrendorf, M. Leukocyte Behavior in Atherosclerosis, Myocardial Infarction, and Heart Failure. Science 2013, 339, 161–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zidar, N.; Jeruc, J.; Balažic, J.; Štajer, D. Neutrophils in human myocardial infarction with rupture of the free wall. Cardiovasc. Pathol. 2005, 14, 247–250. [Google Scholar] [CrossRef]
- Klebanoff, S.J. Myeloperoxidase: Friend and foe. J. Leukoc. Biol. 2005, 77, 598–625. [Google Scholar] [CrossRef] [Green Version]
- Teng, N.; Maghzal, G.J.; Talib, J.; Rashid, I.; Lau, A.K.; Stocker, R. The roles of myeloperoxidase in coronary artery disease and its potential implication in plaque rupture. Redox Rep. 2017, 22, 51–73. [Google Scholar] [CrossRef] [Green Version]
- Mollenhauer, M.; Friedrichs, K.; Lange, M.; Gesenberg, J.; Remane, L.; Kerkenpaß, C.; Krause, J.; Schneider, J.; Ravekes, T.; Maass, M.; et al. Myeloperoxidase Mediates Postischemic Arrhythmogenic Ventricular Remodeling. Circ. Res. 2017, 121, 56–70. [Google Scholar] [CrossRef]
- Vasilyev, N.; Williams, T.; Brennan, M.L.; Unzek, S.; Zhou, X.; Heinecke, J.W.; Spitz, D.R.; Topol, E.J.; Hazen, S.L.; Penn, M.S. Myeloperoxidase-Generated Oxidants Modulate Left Ventricular Remodeling but Not Infarct Size After Myocardial Infarction. Circulation 2005, 112, 2812–2820. [Google Scholar] [CrossRef] [Green Version]
- Ali, M.; Pulli, B.; Courties, G.; Tricot, B.; Sebas, M.; Iwamoto, Y.; Hilgendorf, I.; Schob, S.; Dong, A.; Zheng, W.; et al. Myeloperoxidase Inhibition Improves Ventricular Function and Remodeling After Experimental Myocardial Infarction. JACC Basic Transl. Sci. 2016, 1, 633–643. [Google Scholar] [CrossRef]
- Askari, A.T.; Brennan, M.L.; Zhou, X.; Drinko, J.; Morehead, A.; Thomas, J.D.; Topol, E.; Hazen, S.L.; Penn, M.S. Myeloperoxidase and Plasminogen Activator Inhibitor 1 Play a Central Role in Ventricular Remodeling after Myocardial Infarction. J. Exp. Med. 2003, 197, 615–624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruggeri, R.B.; Buckbinder, L.; Bagley, S.W.; Carpino, P.A.; Conn, E.L.; Dowling, M.S. Discovery of 2-(6-(5-Chloro-2-methoxyphenyl)-4-oxo-2-thioxo-3,4-dihydropyrimidin-1(2H)-yl)acet amide (PF-06282999): A Highly Selective Mechanism-Based Myeloperoxidase Inhibitor for the Treatment of Cardiovascular Diseases. J. Med. Chem. 2015, 58, 8513–8528. [Google Scholar] [CrossRef]
- Roth Flach, R.J.; Su, C.; Bollinger, E.; Cortes, C.; Robertson, A.W.; Opsahl, A.C. Myeloperoxidase inhibition in mice alters atherosclerotic lesion composition. PLoS ONE 2019, 14, e0214150. [Google Scholar] [CrossRef] [Green Version]
- Jucaite, A.; Svenningsson, P.; Rinne, J.O.; Cselényi, Z.; Varnäs, K.; Johnström, P.; Amini, N.; Kirjavainen, A.; Helin, S.; Minkwitz, M.; et al. Effect of the myeloperoxidase inhibitor AZD3241 on microglia: A PET study in Parkinson’s disease. Brain 2015, 138, 2687–2700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, W.; Warner, R.; Ruggeri, R.; Su, C.; Cortes, C.; Skoura, A. PF-1355, a mechanism-based myeloperoxidase inhibitor, prevents immune complex vasculitis and anti-glomerular basement membrane glomerulonephritis. J. Pharm. Exp. Ther. 2015, 353, 288–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nelander, K.; Lagerstrom-Fermer, M.; Amilon, C.; Michaëlsson, E.; Heijer, M.; Kjaer, M.; Russell, M.; Han, D.; Lindstedt, E.; Whatling, C.; et al. Early Clinical Experience With AZD4831, A Novel Myeloperoxidase Inhibitor, Developed for Patients With Heart Failure With Preserved Ejection Fraction. Clin. Transl. Sci. 2020, 14, 812. [Google Scholar] [CrossRef]
- Wang, C.; Keliher, E.; Zeller, M.W.G.; Wojtkiewicz, G.R.; Aguirre, A.D.; Buckbinder, L.; Kim, H.Y.; Chen, J.; Maresca, K.; Ahmed, M.S.; et al. An activatable PET imaging radioprobe is a dynamic reporter of myeloperoxidase activity in vivo. Proc. Natl. Acad. Sci. USA 2019, 116, 11966–11971. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez, E.; Nilges, M.; Weissleder, R.; Chen, J.W. Activatable Magnetic Resonance Imaging Agents for Myeloperoxidase Sensing: Mechanism of Activation, Stability, and Toxicity. J. Am. Chem. Soc. 2009, 132, 168–177. [Google Scholar] [CrossRef] [Green Version]
- Pulli, B.; Ali, M.; Forghani, R.; Schob, S.; Hsieh, K.L.C.; Wojtkiewicz, G.; Linnoila, J.J.; Chen, J.W. Measuring Myeloperoxidase Activity in Biological Samples. PLoS ONE 2013, 8, e67976. [Google Scholar] [CrossRef] [Green Version]
- Thackeray, J.T.; Bengel, F.M. Molecular Imaging of Myocardial Inflammation with Positron Emission Tomography Post-Ischemia: A Determinant of Subsequent Remodeling or Recovery. JACC Cardiovasc. Imaging 2018, 11, 1340–1355. [Google Scholar] [CrossRef]
- Horckmans, M.; Ring, L.; Duchene, J.; Santovito, D.; Schloss, M.J.; Drechsler, M.; Weber, C.; Soehnlein, O.; Steffens, S. Neutrophils orchestrate post-myocardial infarction healing by polarizing macrophages towards a reparative phenotype. Eur. Heart J. 2017, 38, 187–197. [Google Scholar] [CrossRef] [Green Version]
- Mehta, J.; Dinerman, J.; Mehta, P.; Saldeen, T.G.; Lawson, D.; Donnelly, W.H.; Wallin, R. Neutrophil function in ischemic heart disease. Circulation 1989, 79, 549–556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thackeray, J.T.; Bankstahl, J.P.; Wang, Y.; Wollert, K.C.; Bengel, F.M. Clinically relevant strategies for lowering cardiomyocyte glucose uptake for 18F-FDG imaging of myocardial inflammation in mice. Eur. J. Nucl. Med. 2014, 42, 771–780. [Google Scholar] [CrossRef] [PubMed]
- Harisankar, C.N.B.; Mittal, B.R.; Agrawal, K.; Abrar, M.L.; Bhattacharya, A. Utility of high fat and low carbohydrate diet in suppressing myocardial FDG uptake. J. Nucl. Cardiol. 2011, 18, 926–936. [Google Scholar] [CrossRef]
- Swirski, F.K.; Wildgruber, M.; Ueno, T.; Figueiredo, J.L.; Panizzi, P.; Iwamoto, Y.; Zhang, E.; Stone, J.R.; Rodriguez, E.; Chen, J.W.; et al. Myeloperoxidase-rich Ly-6C+ myeloid cells infiltrate allografts and contribute to an imaging signature of organ rejection in mice. J. Clin. Investig. 2010, 120, 2627–2634. [Google Scholar] [CrossRef] [Green Version]
- Daugherty, A.; Dunn, J.L.; Rateri, D.L.; Heinecke, J.W. Myeloperoxidase, a catalyst for lipoprotein oxidation, is expressed in human atherosclerotic lesions. J. Clin. Investig. 1994, 94, 437–444. [Google Scholar] [CrossRef] [Green Version]
- Hazell, L.J.; Arnold, L.; Flowers, D.; Waeg, G.; Malle, E.; Stocker, R. Presence of hypochlorite-modified proteins in human atherosclerotic lesions. J. Clin. Investig. 1996, 97, 1535–1544. [Google Scholar] [CrossRef] [PubMed]
- Rashid, I.; Maghzal, G.J.; Chen, Y.C.; Cheng, D.; Talib, J.; Newington, D.; Ren, M.; Vajandar, S.K.; Searle, A.; Maluenda, A.; et al. Myeloperoxidase is a potential molecular imaging and therapeutic target for the identification and stabilization of high-risk atherosclerotic plaque. Eur. Hear. J. 2018, 39, 3301–3310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meuwese, M.C.; Stroes, E.S.; Hazen, S.L.; van Miert, J.N.; Kuivenhoven, J.A.; Schaub, R.G.; Wareham, N.J.; Luben, R.; Kastelein, J.J.; Khaw, K.T.; et al. Serum Myeloperoxidase Levels Are Associated with the Future Risk of Coronary Artery Disease in Apparently Healthy Individuals: The EPIC-Norfolk Prospective Population Study. J. Am. Coll. Cardiol. 2007, 50, 159–165. [Google Scholar] [CrossRef] [Green Version]
- Vita, J.A.; Brennan, M.L.; Gokce, N.; Mann, S.A.; Goormastic, M.; Shishehbor, M.H.; Penn, M.S.; Keaney, J.F.; Hazen, S.L. Serum Myeloperoxidase Levels Independently Predict Endothelial Dysfunction in Humans. Circulation 2004, 110, 1134–1139. [Google Scholar] [CrossRef] [Green Version]
- Nicholls, S.J.; Hazen, S.L. Myeloperoxidase and Cardiovascular Disease. Arter. Thromb. Vasc. Biol. 2005, 25, 1102–1111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.; Motlagh, N.J.; Kuellenberg, E.G.; Chen, J.W. Imaging the reactivity of myeloperoxidase in vivo. In Mammalian Heme Peroxidases; CRC Press: Boca Raton, FL, USA, 2021; pp. 207–223. [Google Scholar] [CrossRef]
- Yang, N.J.; Hinner, M.J. Getting across the cell membrane: An overview for small molecules, peptides, and proteins. Methods Mol. Biol. 2015, 1266, 29–53. [Google Scholar] [PubMed] [Green Version]
- DiStasi, M.R.; Ley, K. Opening the flood-gates: How neutrophil-endothelial interactions regulate permeability. Trends Immunol. 2009, 30, 547–556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rytting, M.E.; Kantarjian, H.; Albitar, M. Acute Lymphoblastic Leukemia with Burkitt-like Morphologic Features and High Myeloperoxidase Activity. Am. J. Clin. Pathol. 2009, 132, 182–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bononi, A.; Lanza, F.; Dabusti, M.; Gusella, M.; Gilli, G.; Menon, D.; Toso, S.; Crepaldi, G.; Marenda, B.; Abbasciano, V.; et al. Increased myeloperoxidase index and large unstained cell values can predict the neutropenia phase of cancer patients treated with standard dose chemotherapy. Cytometry 2001, 46, 92–97. [Google Scholar] [CrossRef]
- Davies, M.J.; Hawkins, C.L. The Role of Myeloperoxidase in Biomolecule Modification, Chronic Inflammation, and Disease. Antioxid. Redox Signal. 2020, 32, 957–981. [Google Scholar] [CrossRef] [Green Version]
- Lloyd, M.M.; van Reyk, D.M.; Davies, M.J.; Hawkins, C.L. Hypothiocyanous acid is a more potent inducer of apoptosis and protein thiol depletion in murine macrophage cells than hypochlorous acid or hypobromous acid. Biochem. J. 2008, 414, 271–280. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.T.; Whiteman, M.; Gieseg, S.P. Intracellular glutathione protects human monocyte-derived macrophages from hypochlorite damage. Life Sci. 2012, 90, 682–688. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zeller, M.W.G.; Wang, C.; Keliher, E.J.; Wojtkiewicz, G.R.; Aguirre, A.; Maresca, K.; Su, C.; Buckbinder, L.; Wang, J.; Nahrendorf, M.; et al. Myeloperoxidase PET Imaging Tracks Intracellular and Extracellular Treatment Changes in Experimental Myocardial Infarction. Int. J. Mol. Sci. 2023, 24, 5704. https://doi.org/10.3390/ijms24065704
Zeller MWG, Wang C, Keliher EJ, Wojtkiewicz GR, Aguirre A, Maresca K, Su C, Buckbinder L, Wang J, Nahrendorf M, et al. Myeloperoxidase PET Imaging Tracks Intracellular and Extracellular Treatment Changes in Experimental Myocardial Infarction. International Journal of Molecular Sciences. 2023; 24(6):5704. https://doi.org/10.3390/ijms24065704
Chicago/Turabian StyleZeller, Matthias W. G., Cuihua Wang, Edmund J. Keliher, Gregory R. Wojtkiewicz, Aaron Aguirre, Kevin Maresca, Chunyan Su, Leonard Buckbinder, Jing Wang, Matthias Nahrendorf, and et al. 2023. "Myeloperoxidase PET Imaging Tracks Intracellular and Extracellular Treatment Changes in Experimental Myocardial Infarction" International Journal of Molecular Sciences 24, no. 6: 5704. https://doi.org/10.3390/ijms24065704
APA StyleZeller, M. W. G., Wang, C., Keliher, E. J., Wojtkiewicz, G. R., Aguirre, A., Maresca, K., Su, C., Buckbinder, L., Wang, J., Nahrendorf, M., & Chen, J. W. (2023). Myeloperoxidase PET Imaging Tracks Intracellular and Extracellular Treatment Changes in Experimental Myocardial Infarction. International Journal of Molecular Sciences, 24(6), 5704. https://doi.org/10.3390/ijms24065704