

Unraveling Structural Alerts in Marketed Drugs for Improving Adverse Outcome Pathway Framework of Drug-Induced QT Prolongation


Abstract
:1. Introduction
2. Results
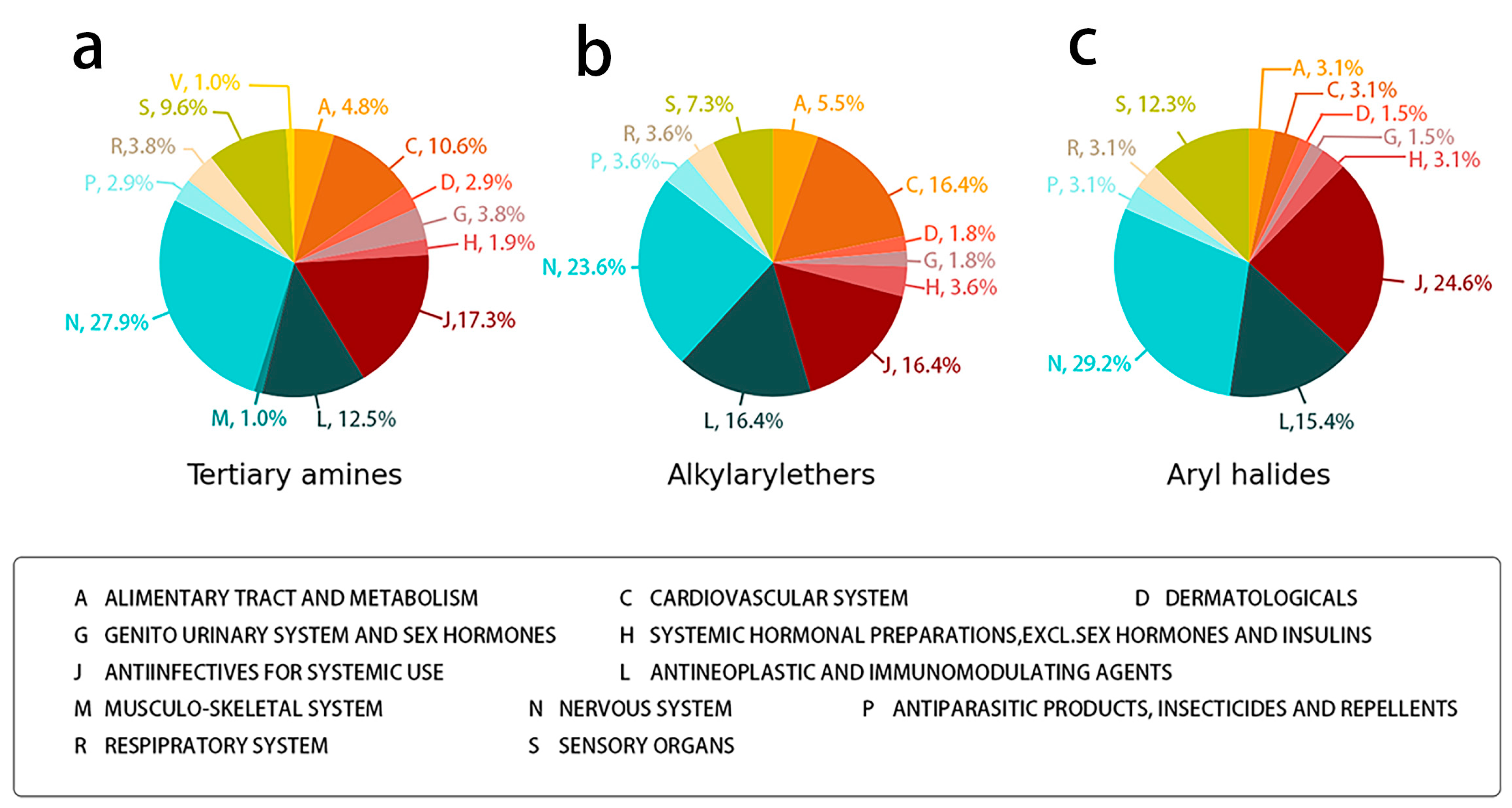
2.1. Structural Differences between QT and Non-QT-Prolonging Drugs
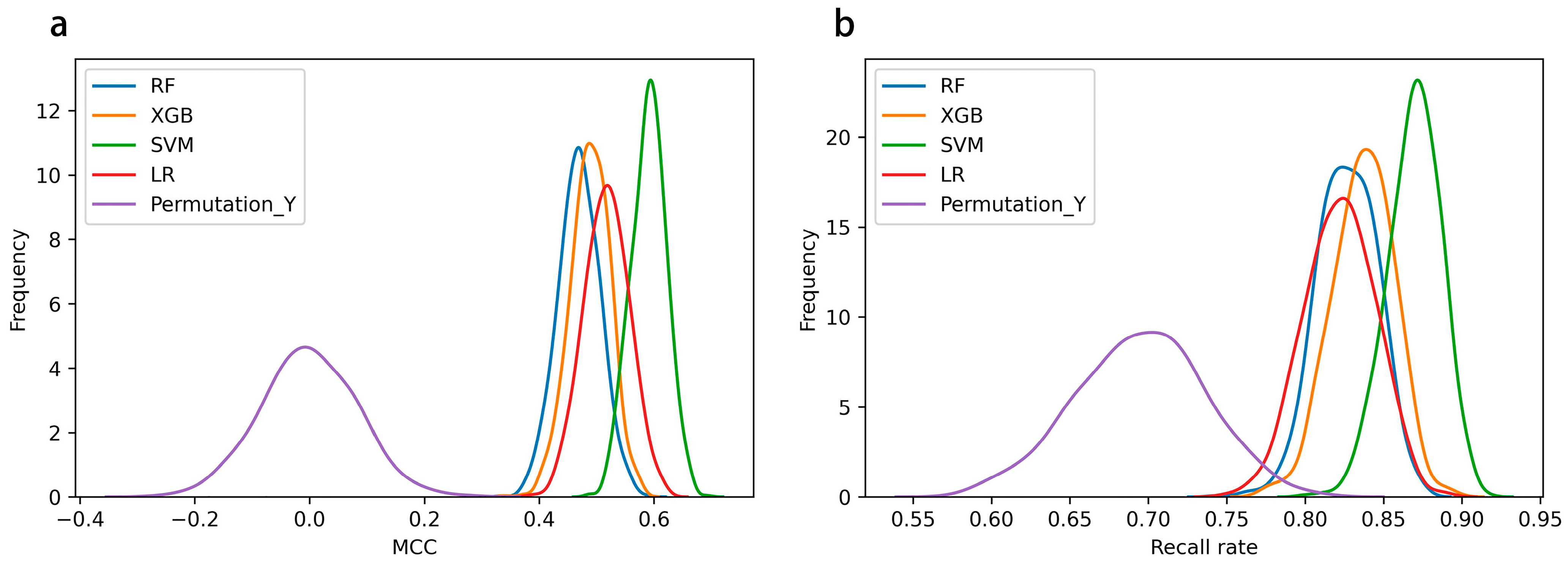
2.2. SAR Model Performance on DIQTA Dataset
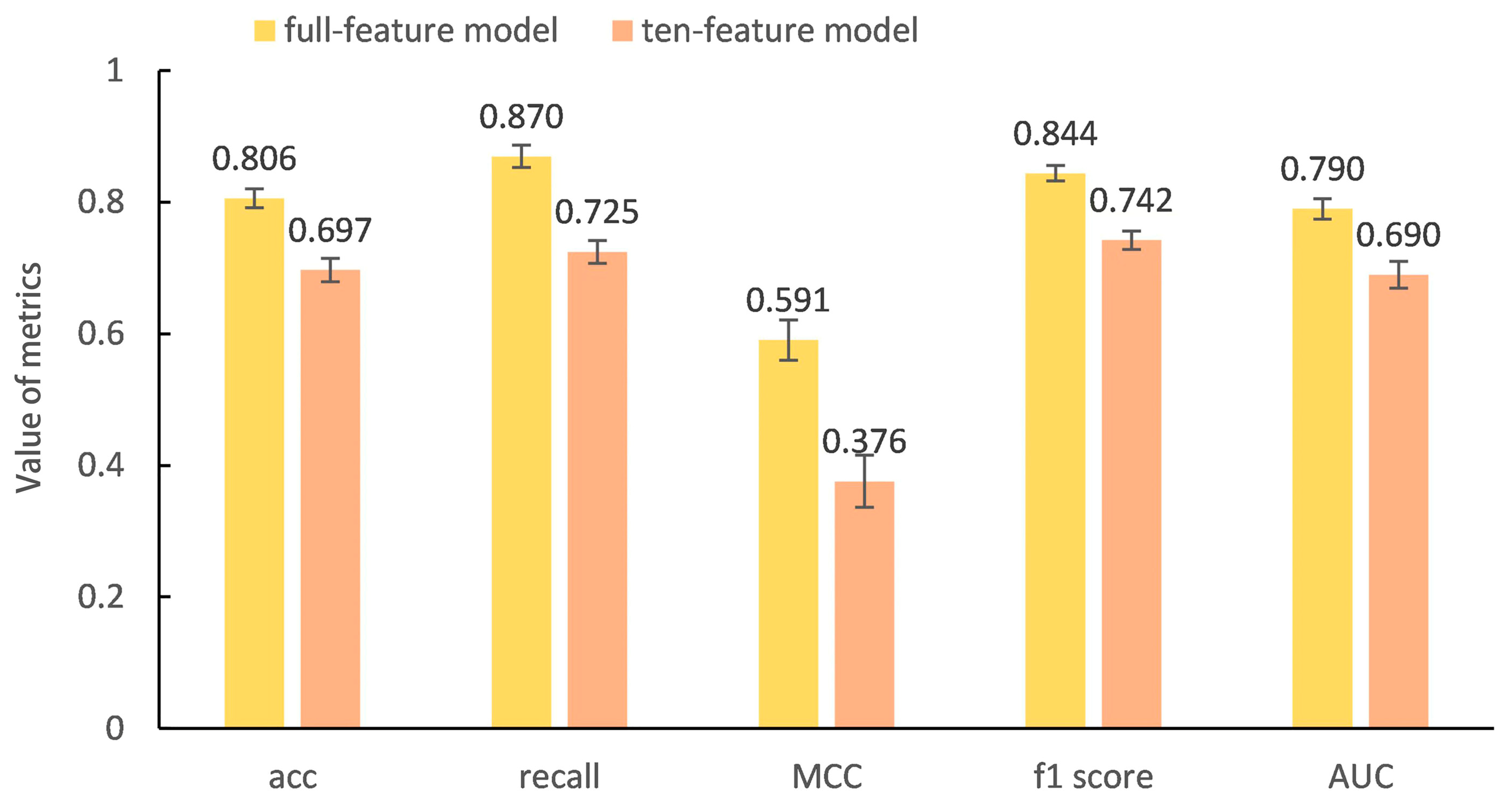
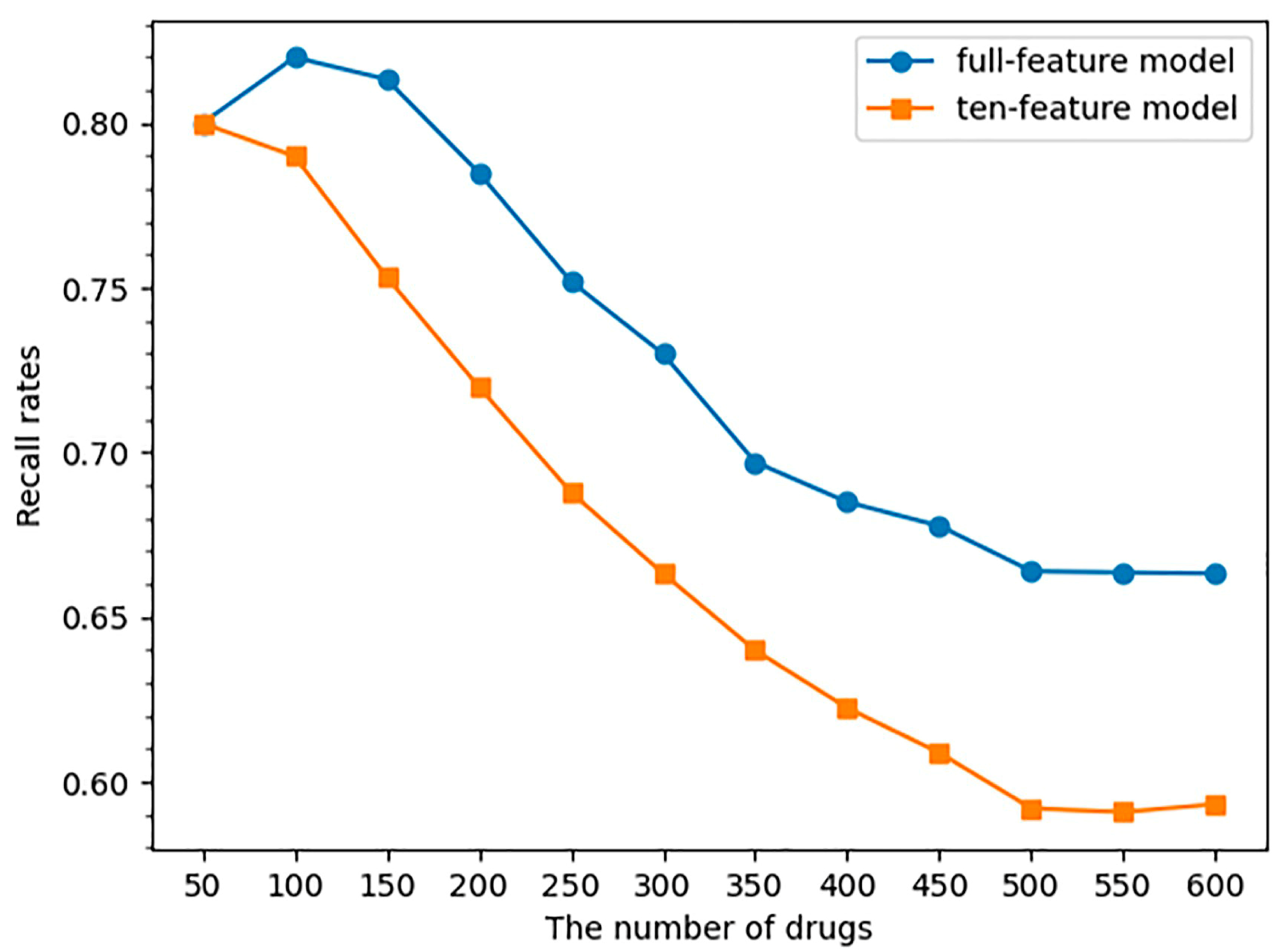
2.3. SAR Model Performance on FAERS Dataset
3. Discussion
4. Materials and Methods
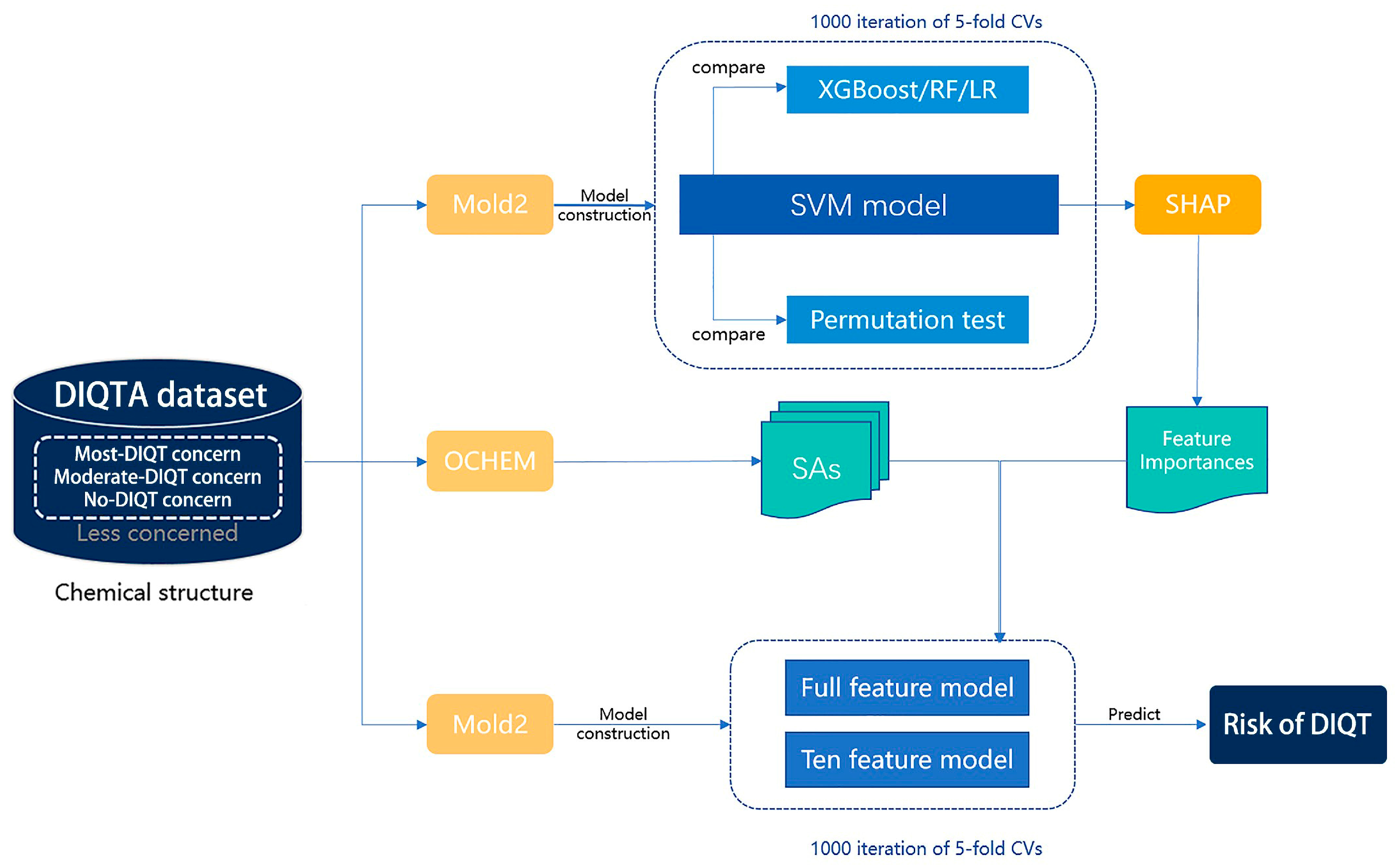
4.1. Study Design
4.2. DIQTA Dataset
4.3. FAERS Dataset
4.4. Identification of Structural Alerts
4.5. Calculation and Selection of Molecular Descriptors
4.6. SAR Model Construction
4.7. Feature Selection
4.8. Evaluation of Model Performance
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Riad, F.S.; Davis, A.M.; Moranville, M.P.; Beshai, J.F. Drug-Induced QTc Prolongation. Am. J. Cardiol. 2017, 119, 280–283. [Google Scholar] [CrossRef] [PubMed]
- Isbister, G.K.; Page, C.B. Drug induced QT prolongation: The measurement and assessment of the QT interval in clinical practice. Br. J. Clin. Pharmacol. 2013, 76, 48–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roden, D.M. Drug therapy: Drug-induced prolongation of the QT interval. N. Engl. J. Med. 2004, 350, 1013–1022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mirams, G.R.; Davies, M.R.; Cui, Y.; Kohl, P.; Noble, D. Application of cardiac electrophysiology simulations to pro-arrhythmic safety testing. Br. J. Pharmacol. 2012, 167, 932–945. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smilowitz, N.R.; Berger, J.S. Perioperative Cardiovascular Risk Assessment and Management for Noncardiac Surgery A Review. JAMA-J. Am. Med. Assoc. 2020, 324, 279–290. [Google Scholar] [CrossRef]
- Jabbar, A.; Pingitore, A.; Pearce, S.; Zaman, A.; Iervasi, G.; Razvi, S. Thyroid hormones and cardiovascular disease. Nat. Rev. Cardiol. 2017, 14, 39–55. [Google Scholar] [CrossRef]
- Curigliano, G.; Cardinale, D.; Dent, S.; Criscitiello, C.; Aseyev, O.; Lenihan, D.; Cipolla, C.M. Cardiotoxicity of Anticancer Treatments: Epidemiology, Detection, and Management. CA-Cancer J. Clin. 2016, 66, 310–325. [Google Scholar] [CrossRef] [Green Version]
- Kavousi, M.; Leening, M.; Nanchen, D.; Greenland, P.; Graham, I.M.; Steyerberg, E.W.; Ikram, M.A.; Stricker, B.H.; Hofman, A.; Franco, O.H. Comparison of Application of the ACC/AHA Guidelines, Adult Treatment Panel III Guidelines, and European Society of Cardiology Guidelines for Cardiovascular Disease Prevention in a European Cohort. JAMA-J. Am. Med. Assoc. 2014, 311, 1416–1423. [Google Scholar] [CrossRef]
- Carmeliet, P.; Jain, R.K. Molecular mechanisms and clinical applications of angiogenesis. Nature 2011, 473, 298–307. [Google Scholar] [CrossRef] [Green Version]
- Fermini, B.; Fossa, A.A. The impact of drug-induced qt interval prolongation on drug discovery and development. Nat. Rev. Drug Discov. 2003, 2, 439–447. [Google Scholar] [CrossRef]
- Thomas, S.H.L.; Behr, E.R. Pharmacological treatment of acquired QT prolongation and torsades de pointes. Br. J. Clin. Pharmacol. 2016, 81, 420–427. [Google Scholar] [CrossRef] [PubMed]
- Drew, B.J.; Ackerman, M.J.; Funk, M.; Gibler, W.B.; Kligfield, P.; Menon, V.; Philippides, G.J.; Roden, D.M.; Zareba, W.; Council, C.C.; et al. Prevention of Torsade de Pointes in Hospital Settings A Scientific Statement From the American Heart Association and the American College of Cardiology Foundation Endorsed by the American Association of Critical-Care Nurses and the International Society for Computerized Electrocardiology. J. Am. Coll. Cardiol. 2010, 55, 934–947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bednar, M.M.; Harrigan, E.P.; Anziano, R.J.; Camm, A.J.; Ruskin, J.N. The QT interval. Prog. Cardiovasc. Dis. 2001, 43, 21469. [Google Scholar] [CrossRef]
- Baracaldo-Santamaria, D.; Llinas-Caballero, K.; Miguel Corso-Ramirez, J.; Martin Restrepo, C.; Alberto Dominguez-Dominguez, C.; Janeth Fonseca-Mendoza, D.; Alberto Calderon-Ospina, C. Genetic and Molecular Aspects of Drug-Induced QT Interval Prolongation. Int. J. Mol. Sci. 2021, 22, 8090. [Google Scholar] [CrossRef]
- Lu, Z.; Wu, C.C.; Jiang, Y.; Ballou, L.M.; Clausen, C.; Cohen, I.S.; Lin, R.Z. Suppression of Phosphoinositide 3-Kinase Signaling and Alteration of Multiple Ion Currents in Drug-Induced Long QT Syndrome. Sci. Transl. Med. 2012, 4, 3623. [Google Scholar] [CrossRef] [Green Version]
- Wilke, R.A.; Lin, D.W.; Roden, D.M.; Watkins, P.B.; Flockhart, D.; Zineh, I.; Giacomini, K.M.; Krauss, R.M. Identifying genetic risk factors for serious adverse drug reactions: Current progress and challenges. Nat. Rev. Drug Discov. 2007, 6, 904–916. [Google Scholar] [CrossRef]
- Friedrichs, G.S.; Patmore, L.; Bass, A. Non-clinical evaluation of ventricular repolarization (ICH S7B): Results of an interim survey of international pharmaceutical companies. J. Pharmacol. Tox Met. 2005, 52, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Bennett, P.B.; Yazawa, K.; Makita, N.; George, A.L. Molecular Mechanism for an Inherited Cardiac-Arrhythmia. Nature 1995, 376, 683–685. [Google Scholar] [CrossRef]
- Colatsky, T.; Fermini, B.; Gintant, G.; Pierson, J.B.; Sager, P.; Sekino, Y.; Strauss, D.G.; Stockbridge, N. The Comprehensive in Vitro Proarrhythmia Assay (CiPA) initiative Update on progress. J. Pharmacol. Tox Met. 2016, 81, 15–20. [Google Scholar] [CrossRef] [Green Version]
- Choi, K.; Balupuri, A.; Kang, N.S. The Study on the hERG Blocker Prediction Using Chemical Fingerprint Analysis. Molecules 2020, 25, 2615. [Google Scholar] [CrossRef]
- Cai, C.; Fang, J.; Guo, P.; Wang, Q.; Hong, H.; Moslehi, J.; Cheng, F. In Silico Pharmacoepidemiologic Evaluation of Drug-Induced Cardiovascular Complications Using Combined Classifiers. J. Chem. Inf. Model 2018, 58, 943–956. [Google Scholar] [CrossRef]
- Chavan, S.; Abdelaziz, A.; Wiklander, J.G.; Nicholls, I.A. A k-nearest neighbor classification of hERG K+ channel blockers. J. Comput. Aid Mol. Des. 2016, 30, 229–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, L.; Lu, J.; Lu, Y.; Zheng, M.; Luo, X.; Zhu, W.; Jiang, H.; Chen, K. Novel Bayesian classification models for predicting compounds blocking hERG potassium channels. Acta Pharmacol. Sin. 2014, 35, 1093–1102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, R.L.M.; Glen, R.C.; Mitchell, J.B.O. Development and Comparison of hERG Blocker Classifiers: Assessment on Different Datasets Yields Markedly Different Results. Mol. Inform. 2011, 30, 443–458. [Google Scholar] [CrossRef]
- Jia, L.; Sun, H. Support vector machines classification of hERG liabilities based on atom types. Bioorgan. Med. Chem. 2008, 16, 6252–6260. [Google Scholar] [CrossRef]
- Song, M.H.; Clark, M. Development and evaluation of an in silico model for hERG binding. J. Chem. Inf. Model 2006, 46, 392–400. [Google Scholar] [CrossRef]
- Sun, H. An accurate and interpretable Bayesian classification model for prediction of hERG liability. ChemMedChem 2006, 1, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Yap, C.W.; Cai, C.Z.; Xue, Y.; Chen, Y.Z. Prediction of torsade-causing potential of drugs by support vector machine approach. Toxicol. Sci. 2004, 79, 170–177. [Google Scholar] [CrossRef] [PubMed]
- Karim, A.; Lee, M.; Balle, T.; Sattar, A. CardioTox net: A robust predictor for hERG channel blockade based on deep learning meta-feature ensembles. J. Cheminformatics 2021, 13, 60. [Google Scholar] [CrossRef]
- Cai, C.; Guo, P.; Zhou, Y.; Zhou, J.; Wang, Q.; Zhang, F.; Fang, J.; Cheng, F. Deep Learning-Based Prediction of Drug-Induced Cardiotoxicity. J. Chem. Inf. Model 2019, 59, 1073–1084. [Google Scholar] [CrossRef]
- Li, S.; Xu, Z.; Guo, M.; Li, M.; Wen, Z. Drug-induced QT Prolongation Atlas (DIQTA) for enhancing cardiotoxicity management. Drug Discov. Today 2022, 27, 831–837. [Google Scholar] [CrossRef]
- Kannankeril, P.; Roden, D.M.; Darbar, D. Drug-Induced Long QT Syndrome. Pharmacol. Rev. 2010, 62, 760–781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kannankeril, P.J.; Roden, D.M. Drug-induced long QT and torsade de pointes: Recent advances. Curr. Opin. Cardiol. 2007, 22, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.F.; Chan, S.Y.; Goh, B.C.; Chan, E.; Duan, W.; Huang, M.; McLeod, H.L. Mechanism-based inhibition of cytochrome P450 3A4 by therapeutic drugs. Clin. Pharmacokinet. 2005, 44, 279–304. [Google Scholar] [CrossRef]
- Li, M.; Ramos, L.G. Drug-Induced QT Prolongation And Torsades de Pointes. Pharm. Ther. A Peer-Rev. J. Formul. Manag. 2017, 42, 473–477. [Google Scholar]
- Vilar, S.; Harpaz, R.; Chase, H.S.; Costanzi, S.; Rabadan, R.; Friedman, C. Facilitating adverse drug event detection in pharmacovigilance databases using molecular structure similarity: Application to rhabdomyolysis. J. Am. Med. Inform. Assn. 2011, 18, I73–I80. [Google Scholar] [CrossRef] [Green Version]
- Wen, Z.; Liang, Y.; Hao, Y.; Delavan, B.; Huang, R.; Mikailov, M.; Tong, W.; Li, M.; Liu, Z. Drug-Induced Rhabdomyolysis Atlas (DIRA) for idiosyncratic adverse drug reaction management. Drug Discov. Today 2019, 24, 9–15. [Google Scholar] [CrossRef]
- Sushko, I.; Salmina, E.; Potemkin, V.A.; Poda, G.; Tetko, I.V. ToxAlerts: A Web Server of Structural Alerts for Toxfic Chemicals and Compounds with Potential Adverse Reactions. J. Chem. Inf. Model 2012, 52, 2310–2316. [Google Scholar] [CrossRef]
- Sushko, I.; Novotarskyi, S.; Koerner, R.; Pandey, A.K.; Rupp, M.; Teetz, W.; Brandmaier, S.; Abdelaziz, A.; Prokopenko, V.V.; Tanchuk, V.Y.; et al. Online chemical modeling environment (OCHEM): Web platform for data storage, model development and publishing of chemical information. J. Comput. Aid Mol. Des. 2011, 25, 533–554. [Google Scholar] [CrossRef] [Green Version]
- Hong, H.; Harvey, B.G.; Palmese, G.R.; Stanzione, J.F.I.; Ng, H.W.; Sakkiah, S.; Tong, W.; Sadler, J.M. Experimental Data Extraction and in Silico Prediction of the Estrogenic Activity of Renewable Replacements for Bisphenol A. Int. J. Environ. Res. Public Health 2016, 13, 705. [Google Scholar] [CrossRef]
- Hong, H.; Rua, D.; Sakkiah, S.; Selvaraj, C.; Ge, W.; Tong, W. Consensus Modeling for Prediction of Estrogenic Activity of Ingredients Commonly Used in Sunscreen Products. Int. J. Environ. Res. Public Health 2016, 13, 958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, H.; Xie, Q.; Ge, W.; Qian, F.; Fang, H.; Shi, L.; Su, Z.; Perkins, R.; Tong, W. Mold(2), molecular descriptors from 2D structures for chemoinformatics and toxicoinformatics. J. Chem. Inf. Model 2008, 48, 1337–1344. [Google Scholar] [CrossRef] [PubMed]
- Hong, H.X.; Xin, X.Q. Essesa, an expert system for structure elucidation from spectral-analysis: 2. Novel algorithm of perception of the linear independent smallest set of smallest rings. Anal. Chim. Acta 1992, 262, 179–191. [Google Scholar] [CrossRef]
- Cortes, C.; Vapnik, V. Support-vector networks. Mach. Learn. 1995, 20, 273–297. [Google Scholar] [CrossRef]
- Zhang, L.; Ai, H.; Chen, W.; Yin, Z.; Hu, H.; Zhu, J.; Zhao, J.; Zhao, Q.; Liu, H. CarcinoPred-EL: Novel models for predicting the carcinogenicity of chemicals using molecular fingerprints and ensemble learning methods. Sci. Rep. 2017, 7, 2118. [Google Scholar] [CrossRef] [Green Version]
- Park, H. An Introduction to Logistic Regression: From Basic Concepts to Interpretation with Particular Attention to Nursing Domain. J. Korean Acad. Nurs. 2013, 43, 154–164. [Google Scholar] [CrossRef] [Green Version]
- Chen, T.; Guestrin, C.; Assoc, C.M. XGBoost: A Scalable Tree Boosting System. In Proceedings of the 22nd ACM SIGKDD International Conference on Knowledge Discovery and Data Mining, 22nd ACM SIGKDD International Conference on Knowledge Discovery and Data Mining (KDD), San Francisco, CA, USA, 13–17 August 2016; pp. 785–794. [Google Scholar]
- Lundberg, S.M.; Lee, S.-I. A Unified Approach to Interpreting Model Predictions. In Proceedings of the Advances in Neural Information Processing Systems; Guyon, I., Luxburg, U., Von Bengio, S., Wallach, H., Fergus, R., Vishwanathan, S., Garnett, R., Eds.; Curran Associates, Inc.: Red Hook, NY, USA, 2017; Volume 30. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID | Class | Name | SA | Number of QT-Prolonging Drugs | Proportion of QT-Prolonging Drugs | Number of Non-QT-Prolonging Drugs | Proportion of Non-QT-Prolonging Drugs | Difference |
|---|---|---|---|---|---|---|---|---|
| 1 | amines | tertiary amines |  | 88 | 0.6111 | 12 | 0.1263 | 0.4848 |
| 2 | sp3-hybridized carbon atoms (2) |  | 117 | 0.8125 | 36 | 0.3789 | 0.4336 | |
| 3 | tertiary aliphatic amines |  | 76 | 0.5278 | 9 | 0.0947 | 0.4330 | |
| 4 | 16-tertiary amine |  | 91 | 0.6319 | 19 | 0.2 | 0.4319 | |
| 5 | amines |  | 119 | 0.8264 | 38 | 0.4 | 0.4264 | |
| 6 | B3-tertiary amine |  | 76 | 0.5278 | 10 | 0.1053 | 0.4225 | |
| 7 | nitrogen atoms (1) |  | 78 | 0.5417 | 12 | 0.1263 | 0.4154 | |
| 8 | 36-CH2N |  | 65 | 0.4514 | 14 | 0.1474 | 0.3040 | |
| 9 | ethers | ethers |  | 68 | 0.4722 | 17 | 0.1789 | 0.2933 |
| 10 | sp3-hybridized carbon atoms (6) |  | 86 | 0.5972 | 32 | 0.3368 | 0.2604 | |
| 11 | 13-ether |  | 65 | 0.4514 | 20 | 0.2105 | 0.2409 | |
| 12 | alkylarylethers |  | 49 | 0.3403 | 11 | 0.1158 | 0.2245 | |
| 13 | aromatic compounds | arenes |  | 127 | 0.8819 | 56 | 0.5895 | 0.2925 |
| 14 | 11-AC(3-Aromatic carbon) |  | 119 | 0.8264 | 55 | 0.5789 | 0.2474 | |
| 15 | aryl halide |  | 54 | 0.375 | 13 | 0.1368 | 0.2382 | |
| 16 | 4-aromatic carbon-alkane |  | 81 | 0.5625 | 31 | 0.3263 | 0.2362 | |
| 17 | aromatichalogen |  | 53 | 0.3681 | 13 | 0.1368 | 0.2312 | |
| 18 | 10-ACH (3-aromatic carbon) |  | 129 | 0.8958 | 65 | 0.6842 | 0.2116 | |
| 19 | others | base |  | 126 | 0.875 | 49 | 0.5158 | 0.3592 |
| 20 | six-membered heterocycles with one heteroatom (LS) |  | 69 | 0.4792 | 21 | 0.2211 | 0.2581 | |
| 21 | 2-CH2 (1-Alkane group) |  | 130 | 0.9028 | 63 | 0.6632 | 0.2396 | |
| 22 | halogen derivatives |  | 66 | 0.4583 | 22 | 0.2316 | 0.2268 | |
| 23 | halogens |  | 66 | 0.4583 | 22 | 0.2316 | 0.2268 | |
| 24 | NUC |  | 91 | 0.6319 | 40 | 0.4211 | 0.2109 |
| XGBoost | RF | LR | SVM | Permutation_Y | |
|---|---|---|---|---|---|
| Accuracy | 0.758 ± 0.016 | 0.749 ± 0.017 | 0.770 ± 0.019 | 0.806 ± 0.014 | 0.540 ± 0.037 |
| Recall score | 0.837 ± 0.020 | 0.827 ± 0.019 | 0.822 ± 0.022 | 0.870 ± 0.017 | 0.695 ± 0.041 |
| Precision score | 0.779 ± 0.014 | 0.773 ± 0.015 | 0.801 ± 0.017 | 0.820 ± 0.014 | 0.602 ± 0.027 |
| MCC | 0.488 ± 0.034 | 0.469 ± 0.036 | 0.517 ± 0.039 | 0.591 ± 0.031 | −0.001 ± 0.084 |
| BACC | 0.738 ± 0.017 | 0.729 ± 0.018 | 0.756 ± 0.019 | 0.790 ± 0.015 | 0.500 ± 0.039 |
| F1 score | 0.807 ± 0.013 | 0.799 ± 0.014 | 0.811 ± 0.016 | 0.844 ± 0.012 | 0.645 ± 0.030 |
| AUC | 0.738 ± 0.017 | 0.729 ± 0.018 | 0.756 ± 0.019 | 0.790 ± 0.015 | 0.500 ± 0.039 |
| AP | 0.750 ± 0.013 | 0.744 ± 0.014 | 0.766 ± 0.016 | 0.791 ± 0.013 | 0.603 ± 0.019 |
| SE | 0.837 ± 0.020 | 0.827 ± 0.019 | 0.822 ± 0.022 | 0.870 ± 0.017 | 0.695 ± 0.041 |
| SP | 0.640 ± 0.028 | 0.632 ± 0.032 | 0.691 ± 0.032 | 0.710 ± 0.026 | 0.305 ± 0.061 |
| Descriptor | Description |
|---|---|
| D718 | number of CH3X groups |
| D756 | number of Al-O-Ar or Ar-O-Ar or R-O-C=X groups |
| D661 | number of quaternary ammonium (aliphatic) groups |
| D759 | number of tertiary aliphatic amine groups |
| D627 | number of tertiary amides (aliphatic) groups |
| D130 | number of halogen atoms in each molecule |
| D647 | number of primary amines (aliphatic) groups * |
| D626 | number of secondary amides (aromatic) groups |
| D757 | number of Al-NH2 groups |
| D598 | number of total tertiary C-sp3 |
| Drug Name | Odds Ratio | ATC Code |
|---|---|---|
| Doxapram | 398.298 | R07 |
| Cisapride * | 272.797 | A03 |
| Ibutilide * | 223.102 | C01 |
| Tropisetron * | 113.799 | A04 |
| Trimebutine * | 113.799 | A03 |
| Alfacalcidol * | 106.213 | M05, A11 |
| Bedaquiline * | 97.265 | J04 |
| Ethionamide | 79.660 | J04 |
| Bepridil * | 78.360 | C08 |
| Procainamide * | 59.457 | C01 |
| Cases with Current ADR | Cases without Current ADR | |
|---|---|---|
| Cases with current drugs | a | b |
| Cases without current drugs | c | d |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Long, W.; Li, S.; He, Y.; Lin, J.; Li, M.; Wen, Z. Unraveling Structural Alerts in Marketed Drugs for Improving Adverse Outcome Pathway Framework of Drug-Induced QT Prolongation. Int. J. Mol. Sci. 2023, 24, 6771. https://doi.org/10.3390/ijms24076771
Long W, Li S, He Y, Lin J, Li M, Wen Z. Unraveling Structural Alerts in Marketed Drugs for Improving Adverse Outcome Pathway Framework of Drug-Induced QT Prolongation. International Journal of Molecular Sciences. 2023; 24(7):6771. https://doi.org/10.3390/ijms24076771
Chicago/Turabian StyleLong, Wulin, Shihai Li, Yujie He, Jinzhu Lin, Menglong Li, and Zhining Wen. 2023. "Unraveling Structural Alerts in Marketed Drugs for Improving Adverse Outcome Pathway Framework of Drug-Induced QT Prolongation" International Journal of Molecular Sciences 24, no. 7: 6771. https://doi.org/10.3390/ijms24076771
APA StyleLong, W., Li, S., He, Y., Lin, J., Li, M., & Wen, Z. (2023). Unraveling Structural Alerts in Marketed Drugs for Improving Adverse Outcome Pathway Framework of Drug-Induced QT Prolongation. International Journal of Molecular Sciences, 24(7), 6771. https://doi.org/10.3390/ijms24076771