
COVID-19, Possible Hepatic Pathways and Alcohol Abuse—What Do We Know up to 2023?


Abstract
:1. Introduction
2. Hepatic Face of Novel Coronavirus Infection
3. SARS-CoV-2 and Liver—Direct or Indirect Implications?
4. Certain Molecular Pathways in COVID-19-Induced Liver Failure
4.1. Inflammatory Storm
4.2. Hypoxic–Ischemic Liver Failure
4.3. Impaired Iron Metabolism
4.4. Side Effects of Underlying Treatment
5. COVID-19 in Patients without Previously Diagnosed Liver Disorders—Should We Expect Hepatic Complications?
5.1. Hepatic Imaging Findings in COVID-19 Patients
5.2. The Issue of Vaccination against COVID-19
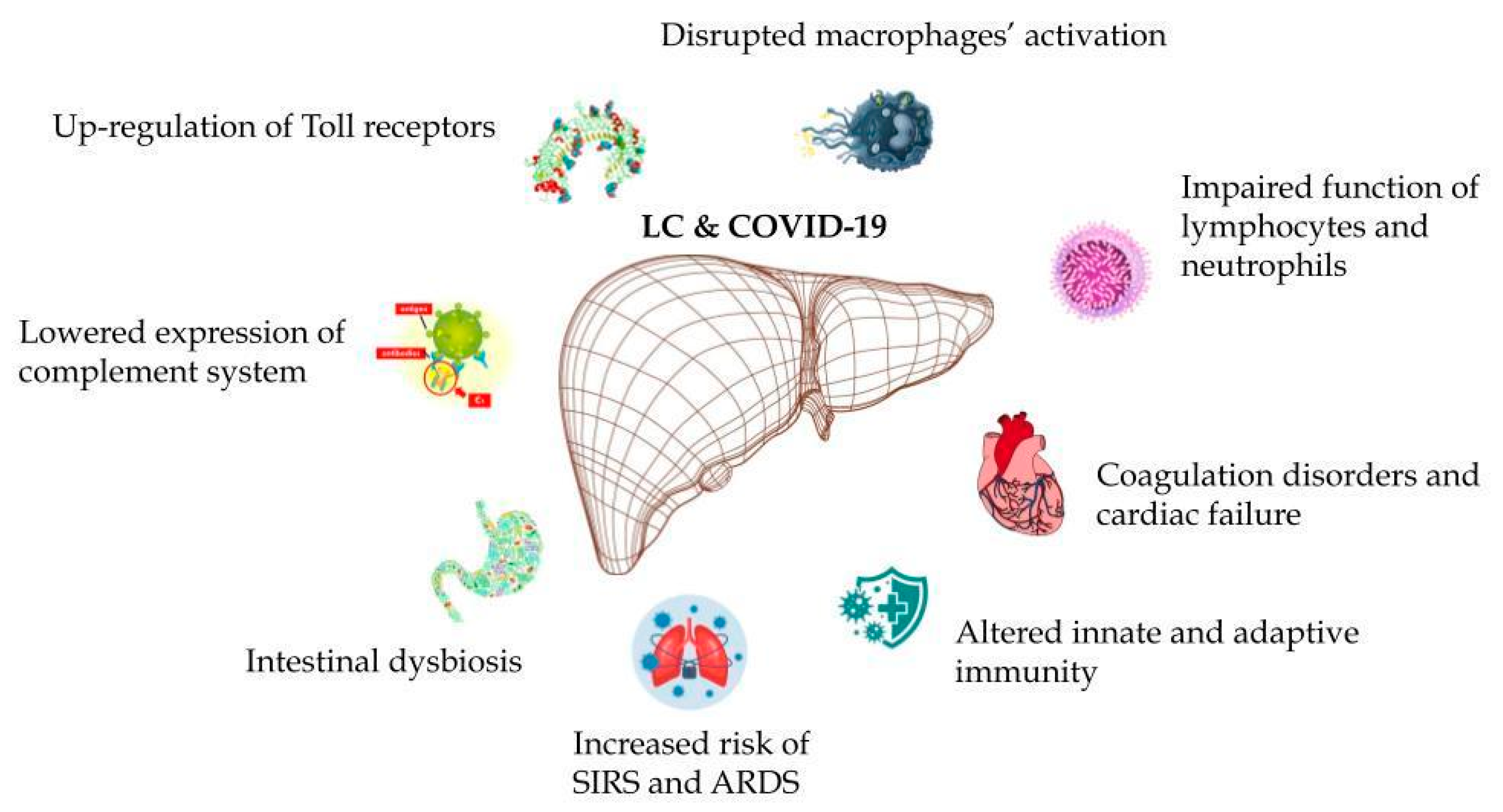
6. COVID-19 in Patients with Pre-Existing Liver Failure—General Observations
7. Ethanol, Liver and COVID-19—A Global Perspective
8. ALC and SARS-CoV-2—Any Specific Patterns and Relationships?
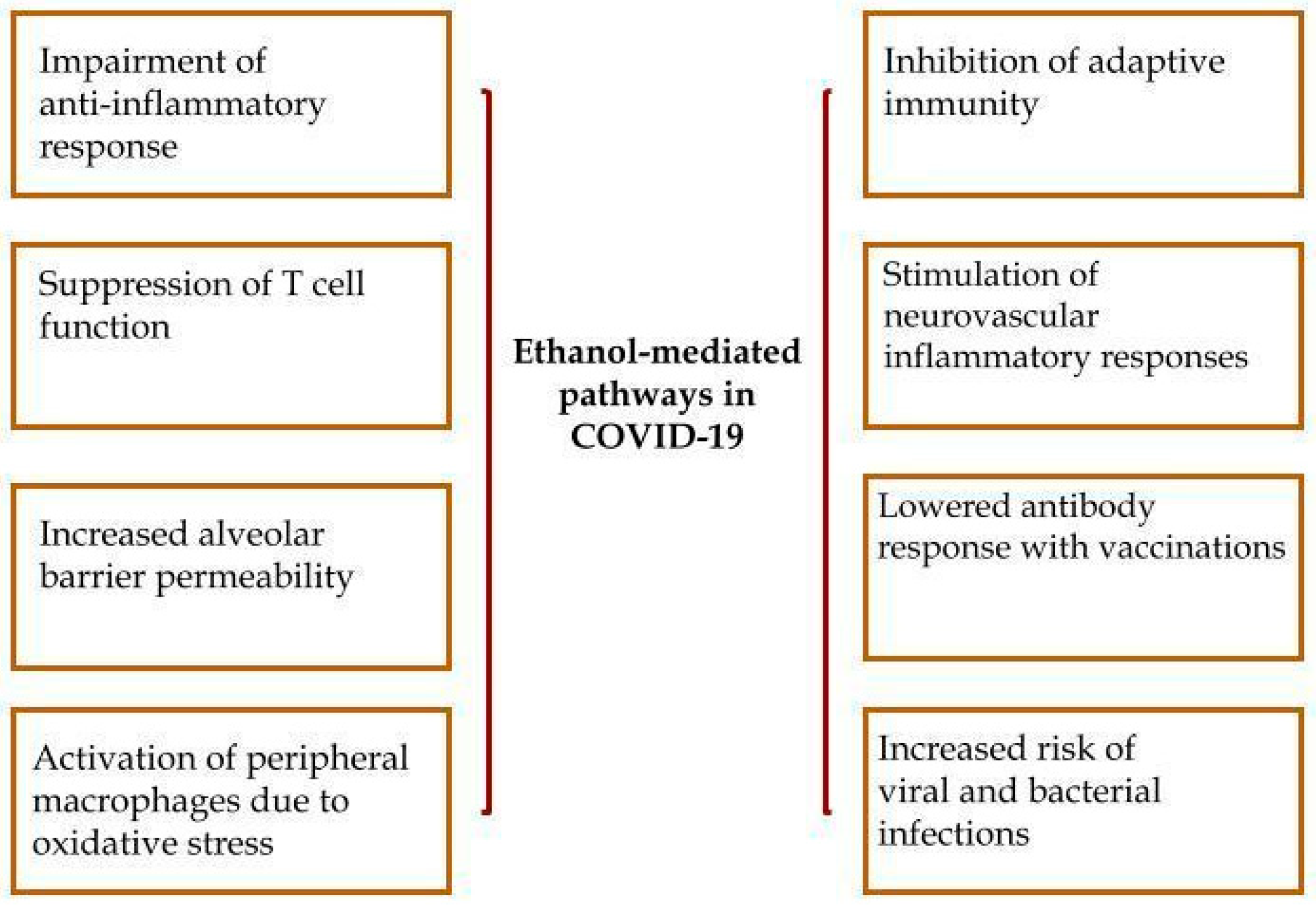
8.1. Alcohol-Mediated Pathological Pathways and Coronavirus—A Complex Scenario
8.2. Characteristic Features of ALD Patients in the Scope of COVID-19
9. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Al-Qudimat, A.R.; Al Darwish, M.B.; Elaarag, M.; Al-Zoubi, R.M.; Rejeb, M.A.; Ojha, L.K.; Nashwan, A.J.; Alshunag, T.; Adawi, K.; Omri, A.E.; et al. COVID-19 effect on patients with noncommunicable diseases: A narrative review. Health Sci. Rep. 2023, 6, e995. [Google Scholar] [CrossRef]
- Ghanemi, A.; Yoshioka, M.; St-Amand, J. Coronavirus Disease 2019 (COVID-19) Crisis: Losing Our Immunity When We Need It the Most. Biology 2021, 10, 545. [Google Scholar] [CrossRef]
- World Health Organization. WHO COVID-19 Dashboard. Available online: https://data.who.int/dashboards/covid19/cases?n=c. (accessed on 24 December 2023).
- Elhence, A.; Vaishnav, M.; Biswas, S.; Anand, A.; Gunjan, D.; Kedia, S.; Mahapatra, S.J.; Nayak, B.; Sheikh, S.; Soni, K.D.; et al. Predictors of in-hospital Outcomes in Patients with Cirrhosis and Coronavirus Disease-2019. J. Clin. Exp. Hepatol. 2022, 12, 876–886. [Google Scholar] [CrossRef]
- Kopańska, M.; Barnaś, E.; Błajda, J.; Kuduk, B.; Łagowska, A.; Banaś-Ząbczyk, A. Effects of SARS-CoV-2 Inflammation on Selected Organ Systems of the Human Body. Int. J. Mol. Sci. 2022, 23, 4178. [Google Scholar] [CrossRef]
- Ozkurt, Z.; Tanrıverdi, E.Ç. COVID-19: Gastrointestinal manifestations, liver injury and recommendations. World J. Clin. Cases 2022, 10, 1140–1163. [Google Scholar] [CrossRef]
- Russo, F.P.; Burra, P.; Zanetto, A. COVID-19 and liver disease: Where are we now? Nat. Rev. Gastroenterol. Hepatol. 2022, 19, 277–278. [Google Scholar] [CrossRef] [PubMed]
- Sagnelli, C.; Macera, M.; Camaioni, C.; Salvati, A.; Coppola, N.; Sagnelli, E. SARS-CoV-2 infection: A hurricane that does not ignore chronic hepatitis. Infection 2022, 50, 849–858. [Google Scholar] [CrossRef] [PubMed]
- Aquino-Matus, J.; Uribe, M.; Chavez-Tapia, N. COVID-19: Current Status in Gastrointestinal, Hepatic, and Pancreatic Diseases—A Concise Review. Trop. Med. Infect. Dis. 2022, 7, 187. [Google Scholar] [CrossRef]
- Ghazanfar, H.; Kandhi, S.; Shin, D.; Muthumanickam, A.; Gurjar, H.; Qureshi, Z.A.; Shaban, M.; Farag, M.; Haider, A.; Budhathoki, P.; et al. Impact of COVID-19 on the Gastrointestinal Tract: A Clinical Review. Cureus 2022, 14, e23333. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Madhavan, M.V.; Sehgal, K.; Nair, N.; Mahajan, S.; Sehrawat, T.S.; Bikdeli, B.; Ahluwalia, N.; Ausiello, J.C.; Wan, E.Y.; et al. Extrapulmonary manifestations of COVID-19. Nat. Med. 2020, 26, 1017–1032. [Google Scholar] [CrossRef] [PubMed]
- Hawkings, M.J.; Vaselli, N.M.; Charalampopoulos, D.; Brierley, L.; Elliot, A.J.; Buchan, I.; Hungerford, D. A Systematic Review of the Prevalence of Persistent Gastrointestinal Symptoms and Incidence of New Gastrointestinal Illness after Acute SARS-CoV-2 Infection. Viruses 2023, 15, 1625. [Google Scholar] [CrossRef] [PubMed]
- Sarkesh, A.; Sorkhabi, A.D.; Sheykhsaran, E.; Alinezhad, F.; Mohammadzadeh, N.; Hemmat, N.; Baghi, H.B. Extrapulmonary Clinical Manifestations in COVID-19 Patients. Am. J. Trop. Med. Hyg. 2020, 103, 1783–1796. [Google Scholar] [CrossRef] [PubMed]
- Tafaj, I.; Cuko, L.; Çili, Q.; Hysenj, A.; Sadiku, E. The Outcome of COVID-19 Infection in Patients with Gastrointestinal Diseases: An Experience at a Tertiary Center. Cureus 2023, 15, e35629. [Google Scholar] [CrossRef] [PubMed]
- Ekpanyapong, S.; Bunchorntavakul, C.; Reddy, K.R. COVID-19 and the Liver: Lessons Learnt from the EAST and the WEST, A Year Later. J. Viral Hepat. 2022, 29, 4–20. [Google Scholar] [CrossRef]
- Ge, J.; Pletcher, M.J.; Lai, J.C.; Harper, J.R.; Chute, C.G.; Haendel, M.A. Outcomes of SARS-CoV-2 Infection in Patients with Chronic Liver Disease and Cirrhosis: A National COVID Cohort Collaborative Study. Gastroenterology 2021, 161, 1487–1501.e5. [Google Scholar] [CrossRef]
- Gracia-Ramos, A.E.; Jaquez-Quintana, J.O.; Contreras-Omaña, R.; Auron, M. Liver dysfunction and SARS-CoV-2 infection. World J. Gastroenterol. 2021, 27, 3951–3970. [Google Scholar] [CrossRef]
- Philips, C.A.; Kakkar, K.; Joseph, M.; Yerol, P.K.; Ahamed, R.; Rajesh, S.; Augustine, P. Critically Ill COVID-19 Patient with Chronic Liver Disease—Insights into a Comprehensive Liver Intensive Care. J. Clin. Transl. Hepatol. 2021, 9, 576. [Google Scholar] [CrossRef]
- Pott-Junior, H.; Bittencourt, N.Q.P.; Chacha, S.F.G.; Luporini, R.L.; Cominetti, M.R.; Anibal, F.D.F. Elevations in Liver Transaminases in COVID-19: (How) Are They Related? Front. Med. 2021, 8, 705247. [Google Scholar] [CrossRef]
- Su, F. COVID-19 and Cirrhosis: A Combination We Must Strive to Prevent. Gastroenterology 2021, 161, 1371–1373. [Google Scholar] [CrossRef]
- Yan, Z.; Yang, M.; Lai, C.-L. Long COVID-19 Syndrome: A Comprehensive Review of Its Effect on Various Organ Systems and Recommendation on Rehabilitation Plans. Biomedicines 2021, 9, 966. [Google Scholar] [CrossRef]
- Al-Kuraishy, H.M.; Al-Gareeb, A.I.; Bungau, S.G.; Radu, A.-F.; Batiha, G.E.-S. The potential molecular implications of adiponectin in the evolution of SARS-CoV-2: Inbuilt tendency. J. King Saud Univ. Sci. 2022, 34, 102347. [Google Scholar] [CrossRef]
- Fitero, A.; Bungau, S.G.; Tit, D.M.; Endres, L.; Khan, S.A.; Bungau, A.F.; Romanul, I.; Vesa, C.M.; Radu, A.-F.; Tarce, A.G.; et al. Comorbidities, Associated Diseases, and Risk Assessment in COVID-19—A Systematic Review. Int. J. Clin. Pract. 2022, 2022, 1571826. [Google Scholar] [CrossRef]
- Boraschi, P.; Giugliano, L.; Mercogliano, G.; Donati, F.; Romano, S.; Neri, E. Abdominal and gastrointestinal manifestations in COVID-19 patients: Is imaging useful? World J. Gastroenterol. 2021, 27, 4143–4159. [Google Scholar] [CrossRef]
- Hanif, F.M.; Majid, Z.; Ahmed, S.; Luck, N.H.; Mubarak, M. Hepatic manifestations of coronavirus disease 2019 infection: Clinical and laboratory perspective. World J. Virol. 2022, 11, 453–466. [Google Scholar] [CrossRef] [PubMed]
- Mao, R.; Qiu, Y.; He, J.-S.; Tan, J.-Y.; Li, X.-H.; Liang, J.; Shen, J.; Zhu, L.-R.; Chen, Y.; Iacucci, M.; et al. Manifestations and prognosis of gastrointestinal and liver involvement in patients with COVID-19: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2020, 5, 667–678. [Google Scholar] [CrossRef]
- Wang, F.; Wang, H.; Fan, J.; Zhang, Y.; Wang, H.; Zhao, Q. Pancreatic Injury Patterns in Patients with Coronavirus Disease 19 Pneumonia. Gastroenterology 2020, 159, 367–370. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.Y.; Chu, H.K.; Bai, T.; Tu, S.J.; Wei, Y.; Li, Z.L.; Hu, L.L.; Zhu, R.; Zhang, L.; Han, C.Q.; et al. Liver damage at admission is an independent prognostic factor for COVID-19. J. Dig. Dis. 2020, 21, 512–518. [Google Scholar] [CrossRef]
- Negru, P.A.; Radu, A.-F.; Vesa, C.M.; Behl, T.; Abdel-Daim, M.M.; Nechifor, A.C.; Endres, L.; Stoicescu, M.; Pasca, B.; Tit, D.M.; et al. Therapeutic dilemmas in addressing SARS-CoV-2 infection: Favipiravir versus Remdesivir. Biomed. Pharmacother. 2022, 147, 112700. [Google Scholar] [CrossRef] [PubMed]
- Naeem, M.; Bano, N.; Manzoor, S.; Ahmad, A.; Munawar, N.; Razak, S.I.A.; Lee, T.Y.; Devaraj, S.; Hazafa, A. Pathogenetic Mechanisms of Liver-Associated Injuries, Management, and Current Challenges in COVID-19 Patients. Biomolecules 2023, 13, 99. [Google Scholar] [CrossRef]
- Baroiu, L.; Dumitru, C.; Iancu, A.; Le, A.-C.; Drăgănescu, M.; Baroiu, N.; Anghel, L. COVID-19 impact on the liver. World J. Clin. Cases 2021, 9, 3814–3825. [Google Scholar] [CrossRef]
- Bigdelou, B.; Sepand, M.R.; Najafikhoshnoo, S.; Negrete, J.A.T.; Sharaf, M.; Ho, J.Q.; Sullivan, I.; Chauhan, P.; Etter, M.; Shekarian, T.; et al. COVID-19 and Preexisting Comorbidities: Risks, Synergies, and Clinical Outcomes. Front. Immunol. 2022, 13, 890517. [Google Scholar] [CrossRef] [PubMed]
- Cao, T.-T.; Zhang, G.-Q.; Pellegrini, E.; Zhao, Q.; Li, J.; Luo, L.; Pan, H.-Q. COVID-19 and its effects on the digestive system. World J. Gastroenterol. 2021, 27, 3502–3515. [Google Scholar] [CrossRef]
- Herta, T.; Berg, T. COVID-19 and the liver—Lessons learned. Liver Int. 2021, 41, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Magro, F.; Nuzzo, A.; Abreu, C.; Libânio, D.; Rodriguez-Lago, I.; Pawlak, K.; Hollenbach, M.; Brouwer, W.P.; Siau, K. COVID-19 in gastroenterology: Where are we now? Current evidence on the impact of COVID-19 in gastroenterology. United Eur. Gastroenterol. J. 2021, 9, 750–765. [Google Scholar] [CrossRef] [PubMed]
- Zyoud, S.H. Research landscape on COVID-19 and liver dysfunction: A bibliometric analysis. World J. Gastroenterol. 2023, 29, 4356–4367. [Google Scholar] [CrossRef] [PubMed]
- Elrobaa, I.H.; New, K.J. COVID-19: Pulmonary and Extra Pulmonary Manifestations. Front. Public Health 2021, 9, 711616. [Google Scholar] [CrossRef]
- Lee, I.-C.; Huo, T.-I.; Huang, Y.-H. Gastrointestinal and liver manifestations in patients with COVID-19. J. Chin. Med. Assoc. 2020, 83, 521–523. [Google Scholar] [CrossRef]
- Roshanshad, A.; Ashraf, M.A.; Roshanshad, R.; Kharmandar, A.; Zomorodian, S.A.; Ashraf, H. Ocular Manifestations of Patients with Coronavirus Disease 2019: A Comprehensive Review. J. Ophthalmic Vis. Res. 2021, 16, 234. [Google Scholar] [CrossRef]
- Nasa, P.; Alexander, G. COVID-19 and the liver: What do we know so far? World J. Hepatol. 2021, 13, 522–532. [Google Scholar] [CrossRef]
- Papa, A.; Covino, M.; De Lucia, S.S.; Del Gaudio, A.; Fiorani, M.; Polito, G.; Settanni, C.R.; Piccioni, A.; Franceschi, F.; Gasbarrini, A. Impact of COVID-19 in individuals with and without pre-existent digestive disorders with a particular focus on elderly patients. World J. Gastroenterol. 2023, 29, 4099–4119. [Google Scholar] [CrossRef] [PubMed]
- Fernández, S.S.; Medina, P.G.; Lafuente, A.A.; Vizoso, M.A.B.; Trillo, A.Z.; Mercadal, G.C.; Enrech, G.S.; Garcés, M.L.; Ruiz, A.R.G.; Pastor, O.O.; et al. Impact of SARS-CoV-2 infection on liver disease. Adv. Lab. Med. Av. Med. Lab. 2022, 3, 126–133. [Google Scholar] [CrossRef]
- Fierro, N.A. COVID-19 and the liver: What do we know after six months of the pandemic? Ann. Hepatol. 2020, 19, 590–591. [Google Scholar] [CrossRef]
- Hamming, I.; Timens, W.; Bulthuis, M.; Lely, A.; Navis, G.; Van Goor, H. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J. Pathol. 2004, 203, 631–637. [Google Scholar] [CrossRef]
- Lizardo-Thiebaud, M.J.; Cervantes-Alvarez, E.; La Rosa, N.L.-D.; Tejeda-Dominguez, F.; Palacios-Jimenez, M.; Méndez-Guerrero, O.; Delaye-Martinez, M.; Rodriguez-Alvarez, F.; Romero-Morales, B.; Liu, W.-H.; et al. Direct or Collateral Liver Damage in SARS-CoV-2–Infected Patients. Semin. Liver Dis. 2020, 40, 321–330. [Google Scholar] [CrossRef]
- Loganathan, S.; Kuppusamy, M.; Wankhar, W.; Gurugubelli, K.R.; Mahadevappa, V.H.; Lepcha, L.; Choudhary, A.K. Angiotensin-converting enzyme 2 (ACE2): COVID 19 gate way to multiple organ failure syndromes. Respir. Physiol. Neurobiol. 2021, 283, 103548. [Google Scholar] [CrossRef]
- Metawea, M.I.; Yousif, W.I.; Moheb, I. COVID 19 and liver: An A–Z literature review. Dig. Liver Dis. 2021, 53, 146–152. [Google Scholar] [CrossRef]
- Cai, Q.; Xu, L.; Chen, J. Reply to: “Liver tests abnormalities in COVID-19: Trick or treat?”. J. Hepatol. 2020, 73, 1277–1278. [Google Scholar] [CrossRef]
- Feng, Y.; Liu, Y.; Zhao, Q.; Zhu, J.; Kang, X.; Mi, C.; Li, P.; Li, W.; Lu, G.; Jia, A.; et al. Liver Injury in Patients with COVID-19: A Retrospective Study. Int. J. Med. Sci. 2023, 20, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Yadav, D.K.; Singh, A.; Zhang, Q.; Bai, X.; Zhang, W.; Yadav, R.K.; Singh, A.; Zhiwei, L.; Adhikari, V.P.; Liang, T. Involvement of liver in COVID-19: Systematic review and meta-analysis. Gut 2021, 70, 807–809. [Google Scholar] [CrossRef] [PubMed]
- Akkiz, H. Unraveling the Molecular and Cellular Pathogenesis of COVID-19-Associated Liver Injury. Viruses 2023, 15, 1287. [Google Scholar] [CrossRef] [PubMed]
- Said, Z.N.A.; El Habashy, S.A.; Zaky, S. ESCMID Study Group for Viral Hepatitis, COVID-19-induced transaminitis and hyperbilirubinemia: Presentation and outcomes. World J. Gastroenterol. 2023, 29, 1123–1130. [Google Scholar] [CrossRef]
- Buchynskyi, M.; Kamyshna, I.; Oksenych, V.; Zavidniuk, N.; Kamyshnyi, A. The Intersection of COVID-19 and Metabolic-Associated Fatty Liver Disease: An Overview of the Current Evidence. Viruses 2023, 15, 1072. [Google Scholar] [CrossRef]
- Roshanshad, R.; Roshanshad, A.; Fereidooni, R.; Hosseini-Bensenjan, M. COVID-19 and liver injury: Pathophysiology, risk factors, outcome and management in special populations. World J. Hepatol. 2023, 15, 441–459. [Google Scholar] [CrossRef]
- Fernandes, S.; Sosa-Napolskij, M.; Lobo, G.; Silva, I. Relation of COVID-19 with liver diseases and their impact on healthcare systems: The Portuguese case. World J. Gastroenterol. 2023, 29, 1109–1122. [Google Scholar] [CrossRef] [PubMed]
- Kovalic, A.J.; Satapathy, S.K.; Thuluvath, P.J. Prevalence of chronic liver disease in patients with COVID-19 and their clinical outcomes: A systematic review and meta-analysis. Hepatol. Int. 2020, 14, 612–620. [Google Scholar] [CrossRef] [PubMed]
- Sivandzadeh, G.R.; Askari, H.; Safarpour, A.R.; Ejtehadi, F.; Raeis-Abdollahi, E.; Lari, A.V.; Abazari, M.F.; Tarkesh, F.; Lankarani, K.B. COVID-19 infection and liver injury: Clinical features, biomarkers, potential mechanisms, treatment, and management challenges. World J. Clin. Cases 2021, 9, 6178–6200. [Google Scholar] [CrossRef] [PubMed]
- Ali, N.; Hossain, K. Liver injury in severe COVID-19 infection: Current insights and challenges. Expert Rev. Gastroenterol. Hepatol. 2020, 14, 879–884. [Google Scholar] [CrossRef] [PubMed]
- La Rosa, N.L.-D.; Cervantes-Alvarez, E.; Navarro-Alvarez, N. Increased Hepatic Expression of SARS-CoV-2 Entry Points and Proinflammatory Cytokines in Cirrhosis. Clin. Gastroenterol. Hepatol. 2022, 20, 239–241.e3. [Google Scholar] [CrossRef] [PubMed]
- Paštrovic, F.; Lucijanic, M.; Atic, A.; Stojic, J.; Jaman, M.B.; Drinkovic, I.T.; Zelenika, M.; Milosevic, M.; Medic, B.; Loncar, J.; et al. Prevalence and Prognostic Impact of Deranged Liver Blood Tests in COVID-19: Experience from the Regional COVID-19 Center over the Cohort of 3812 Hospitalized Patients. J. Clin. Med. 2021, 10, 4222. [Google Scholar] [CrossRef] [PubMed]
- Premkumar, M.; Kedarisetty, C.K. Cytokine Storm of COVID-19 and its Impact on Patients with and without Chronic Liver Disease. J. Clin. Transl. Hepatol. 2021, 9, 256. [Google Scholar] [CrossRef]
- Su, Y.-J.; Chang, C.-W.; Chen, M.-J.; Lai, Y.-C. Impact of COVID-19 on liver. World J. Clin. Cases 2021, 9, 7998–8007. [Google Scholar] [CrossRef]
- Moya, L.; Farashi, S.; Suravajhala, P.; Janaththani, P.; Batra, J. Severe COVID-19 May Impact Hepatic Fibrosis/Hepatic Stellate Cells Activation as Indicated by a Pathway and Population Genetic Study. Genes 2022, 14, 22. [Google Scholar] [CrossRef]
- Papagiouvanni, I.; Kotoulas, S.-C.; Pataka, A.; Spyratos, D.G.; Porpodis, K.; Boutou, A.K.; Papagiouvannis, G.; Grigoriou, I.; Vettas, C.; Goulis, I. COVID-19 and liver injury: An ongoing challenge. World J. Gastroenterol. 2023, 29, 257–271. [Google Scholar] [CrossRef]
- Taylor-Robinson, S.; Morgan, M. COVID-19 and the Liver: A Complex and Evolving Picture. Hepatic Med. Evid. Res. 2023, 15, 209–220. [Google Scholar] [CrossRef]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.-H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280.e8. [Google Scholar] [CrossRef]
- Vitiello, A.; La Porta, R.; D’Aiuto, V.; Ferrara, F. The risks of liver injury in COVID-19 patients and pharmacological management to reduce or prevent the damage induced. Egypt. Liver J. 2021, 11, 11. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Liu, S.; Liu, H.; Li, W.; Lin, F.; Jiang, L.; Li, X.; Xu, P.; Zhang, L.; Zhao, L.; et al. SARS-CoV-2 infection of the liver directly contributes to hepatic impairment in patients with COVID-19. J. Hepatol. 2020, 73, 807–816. [Google Scholar] [CrossRef] [PubMed]
- Barnes, E. Infection of liver hepatocytes with SARS-CoV-2. Nat. Metab. 2022, 4, 301–302. [Google Scholar] [CrossRef] [PubMed]
- Wanner, N.; Andrieux, G.; Badia-i-Mompel, P.; Edler, C.; Pfefferle, S.; Lindenmeyer, M.T.; Schmidt-Lauber, C.; Czogalla, J.; Wong, M.N.; Okabayashi, Y.; et al. Molecular consequences of SARS-CoV-2 liver tropism. Nat. Metab. 2022, 4, 310–319. [Google Scholar] [CrossRef] [PubMed]
- Biglione, L.; Corcione, S.; Shbaklo, N.; Rosso, T.; Lupia, T.; Pinna, S.M.; Scabini, S.; Ciccone, G.; De Benedetto, I.; Borre, S.; et al. Liver involvement and mortality in COVID-19: A retrospective analysis from the CORACLE study group. Infez. Med. 2022, 30, 80. [Google Scholar] [CrossRef]
- Desai, J.; Patel, U.; Arjun, S.; Farraj, K.; Yeroushalmi, K.; Paz, S.G.; Im, J.; Castillo, A.; Rammohan, R.; Mustacchia, P. Impact of Liver Injury in COVID-19 Patients: Single-center Retrospective Cohort Analysis. J. Clin. Transl. Hepatol. 2020, 8, 476–478. [Google Scholar] [CrossRef]
- Shousha, H.I.; Afify, S.; Maher, R.; Asem, N.; Fouad, E.; Mostafa, E.F.; Medhat, M.A.; Abdalazeem, A.; Elmorsy, H.; Aziz, M.M.; et al. Hepatic and gastrointestinal disturbances in Egyptian patients infected with coronavirus disease 2019: A multicentre cohort study. World J. Gastroenterol. 2021, 27, 6951–6966. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Yan, W.; Qi, W.; Wu, D.; Zhu, L.; Li, W.; Wang, X.; Ma, K.; Ni, M.; Xu, D.; et al. Clinical characteristics and risk factors of liver injury in COVID-19: A retrospective cohort study from Wuhan, China. Hepatol. Int. 2020, 14, 723–732. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; He, W.; Yu, X.; Hu, D.; Bao, M.; Liu, H.; Zhou, J.; Jiang, H. Coronavirus disease 2019 in elderly patients: Characteristics and prognostic factors based on 4-week follow-up. J. Infect. 2020, 80, 639–645. [Google Scholar] [CrossRef]
- Piano, S.; Dalbeni, A.; Vettore, E.; Benfaremo, D.; Mattioli, M.; Gambino, C.G.; Framba, V.; Cerruti, L.; Mantovani, A.; Martini, A.; et al. Abnormal liver function tests predict transfer to intensive care unit and death in COVID-19. Liver Int. 2020, 40, 2394–2406. [Google Scholar] [CrossRef]
- Phipps, M.M.; Barraza, L.H.; LaSota, E.D.; Sobieszczyk, M.E.; Pereira, M.R.; Zheng, E.X.; Fox, A.N.; Zucker, J.; Verna, E.C. Acute Liver Injury in COVID-19: Prevalence and Association with Clinical Outcomes in a Large U.S. Cohort. Hepatology 2020, 72, 807–817. [Google Scholar] [CrossRef]
- Mishra, K.; Naffouj, S.; Gorgis, S.; Ibrahim, H.; Gill, S.; Fadel, R.; Chatfield, A.; Tang, A.; Salgia, R. Liver Injury as a Surrogate for Inflammation and Predictor of Outcomes in COVID-19. Hepatol. Commun. 2021, 5, 24–32. [Google Scholar] [CrossRef]
- Chew, M.; Tang, Z.; Radcliffe, C.; Caruana, D.; Doilicho, N.; Ciarleglio, M.M.; Deng, Y.; Garcia-Tsao, G. Significant Liver Injury During Hospitalization for COVID-19 Is Not Associated with Liver Insufficiency or Death. Clin. Gastroenterol. Hepatol. 2021, 19, 2182–2191.e7. [Google Scholar] [CrossRef]
- Chen, F.; Chen, W.; Chen, J.; Xu, D.; Xie, W.; Wang, X.; Xie, Y. Clinical features and risk factors of COVID-19-associated liver injury and function: A retrospective analysis of 830 cases. Ann. Hepatol. 2021, 21, 100267. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, A.; Prichett, L.; Tao, X.; Alqahtani, S.A.; Hamilton, J.P.; Mezey, E.; Strauss, A.T.; Kim, A.; Potter, J.J.; Chen, P.-H.; et al. Abnormal liver chemistries as a predictor of COVID-19 severity and clinical outcomes in hospitalized patients. World J. Gastroenterol. 2022, 28, 570–587. [Google Scholar] [CrossRef]
- Zhang, S.-S.; Dong, L.; Wang, G.-M.; Tian, Y.; Ye, X.-F.; Zhao, Y.; Liu, Z.-Y.; Zhai, J.-Y.; Zhao, Z.-L.; Wang, J.-H.; et al. Progressive liver injury and increased mortality risk in COVID-19 patients: A retrospective cohort study in China. World J. Gastroenterol. 2021, 27, 835–853. [Google Scholar] [CrossRef]
- Sikkema, B.J.; Sint Nicolaas, J.; van Wijngaarden, P. No association between COVID-19 related liver injury and the course of disease: A retrospective study. Scand. J. Gastroenterol. 2021, 56, 68–71. [Google Scholar] [CrossRef]
- Chu, H.; Bai, T.; Chen, L.; Hu, L.; Xiao, L.; Yao, L.; Zhu, R.; Niu, X.; Li, Z.; Zhang, L.; et al. Multicenter Analysis of Liver Injury Patterns and Mortality in COVID-19. Front. Med. 2020, 7, 584342. [Google Scholar] [CrossRef]
- Hassanin, T.M.; Fathelbab, H.; Ibraheem, H.; Hassany, S.; Zaghloul, A.; Fathelbab, A. Impact of COVID-19 infection on liver and alimentary tract: Clinical insight. Clin. Exp. Hepatol. 2021, 7, 364–369. [Google Scholar] [CrossRef]
- Cai, Q.; Huang, D.; Yu, H.; Zhu, Z.; Xia, Z.; Su, Y.; Li, Z.; Zhou, G.; Gou, J.; Qu, J.; et al. COVID-19: Abnormal liver function tests. J. Hepatol. 2020, 73, 566–574. [Google Scholar] [CrossRef]
- Fu, Y.; Zhu, R.; Bai, T.; Han, P.; He, Q.; Jing, M.; Xiong, X.; Zhao, X.; Quan, R.; Chen, C.; et al. Clinical Features of Patients Infected with Coronavirus Disease 2019 with Elevated Liver Biochemistries: A Multicenter, Retrospective Study. Hepatology 2021, 73, 1509–1520. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, M.A.; Suresh, S.; Simmer, S.; Abu-Ghanimeh, M.; Karrick, M.; Nimri, F.; Musleh, M.; Mediratta, V.; Al-Shammari, M.; Russell, S.; et al. Increased Morbidity and Mortality in COVID-19 Patients with Liver Injury. Dig. Dis. Sci. 2022, 67, 2577–2583. [Google Scholar] [CrossRef] [PubMed]
- Dinevari, M.F.; Somi, M.H.; Majd, E.S.; Fattahzadeh, A.; Nikniaz, Z. Elevated Liver Aminotransferases Level and COVID-19 Prognosis in Hospitalized Patients: A Prospective Study from Iran. Middle East J. Dig. Dis. 2022, 14, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Cholongitas, E. Prevalence of abnormal liver biochemistry and its impact on COVID-19 patients’ outcomes: A single-center Greek study. Ann. Gastroenterol. 2022, 35, 290. [Google Scholar] [CrossRef] [PubMed]
- Ali, F.E.M.; Mohammedsaleh, Z.M.; Ali, M.M.; Ghogar, O.M. Impact of cytokine storm and systemic inflammation on liver impairment patients infected by SARS-CoV-2: Prospective therapeutic challenges. World J. Gastroenterol. 2021, 27, 1531–1552. [Google Scholar] [CrossRef] [PubMed]
- Choudhary, N.S.; Dhampalwar, S.; Saraf, N.; Soin, A.S. Outcomes of COVID-19 in Patients with Cirrhosis or Liver Transplantation. J. Clin. Exp. Hepatol. 2021, 11, 713–719. [Google Scholar] [CrossRef]
- Mikolasevic, I.; Bozic, D.; Pavić, T.; Ruzic, A.; Hauser, G.; Radic, M.; Radic-Kristo, D.; Razov-Radas, M.; Puljiz, Z.; Milic, S. Liver disease in the era of COVID-19: Is the worst yet to come? World J. Gastroenterol. 2021, 27, 6039–6052. [Google Scholar] [CrossRef] [PubMed]
- Su, H.-Y.; Hsu, Y.-C. Patients with cirrhosis during the COVID-19 pandemic: Current evidence and future perspectives. World J. Clin. Cases 2021, 9, 2951–2968. [Google Scholar] [CrossRef] [PubMed]
- Zhao, C.L.; Rapkiewicz, A.; Maghsoodi-Deerwester, M.; Gupta, M.; Cao, W.; Palaia, T.; Zhou, J.; Ram, B.; Vo, D.; Rafiee, B.; et al. Pathological findings in the postmortem liver of patients with coronavirus disease 2019 (COVID-19). Hum. Pathol. 2021, 109, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Baiges, A.; Cerda, E.; Amicone, C.; Téllez, L.; Alvarado-Tapias, E.; Puente, A.; Fortea, J.I.; Llop, E.; Rocha, F.; Orts, L.; et al. Impact of SARS-CoV-2 Pandemic on Vascular Liver Diseases. Clin. Gastroenterol. Hepatol. 2022, 20, 1525–1533.e5. [Google Scholar] [CrossRef] [PubMed]
- McConnell, M.J.; Kondo, R.; Kawaguchi, N.; Iwakiri, Y. COVID-19 and Liver Injury: Role of Inflammatory Endotheliopathy, Platelet Dysfunction, and Thrombosis. Hepatol. Commun. 2022, 6, 255–269. [Google Scholar] [CrossRef] [PubMed]
- Middleton, P.; Hsu, C.; Lythgoe, M.P. Clinical outcomes in COVID-19 and cirrhosis: A systematic review and meta-analysis of observational studies. BMJ Open Gastroenterol. 2021, 8, e000739. [Google Scholar] [CrossRef] [PubMed]
- Taneva, G.; Dimitrov, D.; Velikova, T. Liver dysfunction as a cytokine storm manifestation and prognostic factor for severe COVID-19. World J. Hepatol. 2021, 13, 2005–2012. [Google Scholar] [CrossRef] [PubMed]
- Tian, D.; Ye, Q. Hepatic complications of COVID-19 and its treatment. J. Med. Virol. 2020, 92, 1818–1824. [Google Scholar] [CrossRef]
- Tsafaridou, M.; Maniadaki, I.; Koutroubakis, I.; Samonakis, D.N. Coagulation disorders and vascular diseases of the liver in patients with COVID-19. Clin. Exp. Hepatol. 2022, 8, 97–102. [Google Scholar] [CrossRef]
- Ciobanu, A.O.; Gherasim, L. Ischemic Hepatitis—Intercorrelated Pathology. Maedica J. Clin. Med. 2018, 13, 5–11. [Google Scholar] [CrossRef]
- Hanidziar, D.; Bittner, E.A. Hypotension, Systemic Inflammatory Response Syndrome, and COVID-19: A Clinical Conundrum. Anesth. Analg. 2020, 131, e175–e176. [Google Scholar] [CrossRef]
- Hollenberg, S.M.; Safi, L.; Parrillo, J.E.; Fata, M.; Klinkhammer, B.; Gayed, N.; Glotzer, T.; Go, R.C.; Gourna-Paleoudis, E.; Landers, D.; et al. Hemodynamic Profiles of Shock in Patients with COVID-19. Am. J. Cardiol. 2021, 153, 135–139. [Google Scholar] [CrossRef]
- Nardo, A.D.; Schneeweiss-Gleixner, M.; Bakail, M.; Dixon, E.D.; Lax, S.F.; Trauner, M. Pathophysiological mechanisms of liver injury in COVID-19. Liver Int. 2021, 41, 20–32. [Google Scholar] [CrossRef]
- Olwal, C.O.; Nganyewo, N.N.; Tapela, K.; Zune, A.L.D.; Owoicho, O.; Bediako, Y.; Duodu, S. Parallels in Sepsis and COVID-19 Conditions: Implications for Managing Severe COVID-19. Front. Immunol. 2021, 12, 602848. [Google Scholar] [CrossRef]
- D’Ardes, D.; Boccatonda, A.; Cocco, G.; Fabiani, S.; Rossi, I.; Bucci, M.; Guagnano, M.T.; Schiavone, C.; Cipollone, F. Impaired coagulation, liver dysfunction and COVID-19: Discovering an intriguing relationship. World J. Gastroenterol. 2022, 28, 1102–1112. [Google Scholar] [CrossRef]
- Li, P.; Liu, Y.; Cheng, Z.; Yu, X.; Li, Y. COVID-19-associated liver injury: Clinical characteristics, pathophysiological mechanisms and treatment management. Biomed. Pharmacother. 2022, 154, 113568. [Google Scholar] [CrossRef] [PubMed]
- Mendizabal, M.; Ridruejo, E.; Piñero, F.; Anders, M.; Padilla, M.; Toro, L.G.; Torre, A.; Montes, P.; Urzúa, A.; Ballerga, E.G.; et al. Comparison of different prognostic scores for patients with cirrhosis hospitalized with SARS-CoV-2 infection. Ann. Hepatol. 2021, 25, 100350. [Google Scholar] [CrossRef]
- Sonzogni, A.; Previtali, G.; Seghezzi, M.; Alessio, M.G.; Gianatti, A.; Licini, L.; Morotti, D.; Zerbi, P.; Carsana, L.; Rossi, R.; et al. Liver histopathology in severe COVID 19 respiratory failure is suggestive of vascular alterations. Liver Int. 2020, 40, 2110–2116. [Google Scholar] [CrossRef] [PubMed]
- Tavabie, O.D.; Clough, J. Gastroenterology 2021: From the heart of the COVID-19 pandemic. Frontline Gastroenterol. 2021, 12, 249–251. [Google Scholar] [CrossRef] [PubMed]
- Benedé-Ubieto, R.; Estévez-Vázquez, O.; Flores-Perojo, V.; Macías-Rodríguez, R.U.; Ruiz-Margáin, A.; Martínez-Naves, E.; Regueiro, J.R.; Ávila, M.A.; Trautwein, C.; Bañares, R.; et al. Abnormal Liver Function Test in Patients Infected with Coronavirus (SARS-CoV-2): A Retrospective Single-Center Study from Spain. J. Clin. Med. 2021, 10, 1039. [Google Scholar] [CrossRef]
- Beraldo, R.F.; Marcondes, M.B.; Santos, M.N.M.D.; Grillo, T.G.; Pires, G.B.T.; De Oliveira, C.V. COVID-19 in a Patient with Liver Cirrhosis. Am. J. Case Rep. 2021, 22, e929948. [Google Scholar] [CrossRef]
- Mao, R.; Rieder, F.; Ben-Horin, S.; Kaplan, G.G.; Ng, S.C.; Wong, G.L.; Ghosh, S.; Chen, M.-H. Implications of COVID-19 for patients with pre-existing digestive diseases: An update. Lancet Gastroenterol. Hepatol. 2021, 6, 258–260. [Google Scholar] [CrossRef]
- Marjot, T.; Webb, G.J.; Barritt, A.S.; Moon, A.M.; Stamataki, Z.; Wong, V.W.; Barnes, E. COVID-19 and liver disease: Mechanistic and clinical perspectives. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 348–364. [Google Scholar] [CrossRef] [PubMed]
- Díaz, L.A.; Idalsoaga, F.; Cannistra, M.; Candia, R.; Cabrera, D.; Barrera, F.; Soza, A.; Graham, R.; Riquelme, A.; Arrese, M.; et al. High prevalence of hepatic steatosis and vascular thrombosis in COVID-19: A systematic review and meta-analysis of autopsy data. World J. Gastroenterol. 2020, 26, 7693–7706. [Google Scholar] [CrossRef] [PubMed]
- Kukla, M.; Skonieczna-Żydecka, K.; Kotfis, K.; Maciejewska, D.; Łoniewski, I.; Lara, L.F.; Pazgan-Simon, M.; Stachowska, E.; Kaczmarczyk, M.; Koulaouzidis, A.; et al. COVID-19, MERS and SARS with Concomitant Liver Injury—Systematic Review of the Existing Literature. J. Clin. Med. 2020, 9, 1420. [Google Scholar] [CrossRef]
- Chen, Y.; Xu, Y.; Zhang, K.; Shen, L.; Deng, M. Ferroptosis in COVID-19-related liver injury: A potential mechanism and therapeutic target. Front. Cell. Infect. Microbiol. 2022, 12, 922511. [Google Scholar] [CrossRef] [PubMed]
- Pasini, A.M.F.; Stranieri, C.; Girelli, D.; Busti, F.; Cominacini, L. Is Ferroptosis a Key Component of the Process Leading to Multiorgan Damage in COVID-19? Antioxidants 2021, 10, 1677. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Cao, F.; Yin, H.; Huang, Z.; Lin, Z.; Mao, N.; Sun, B.; Wang, G. Ferroptosis: Past, present and future. Cell Death Dis. 2020, 11, 88. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Wang, Y.; Jiang, R.; Xue, R.; Yin, X.; Wu, M.; Meng, Q. Ferroptosis in liver disease: New insights into disease mechanisms. Cell Death Discov. 2021, 7, 276. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Lai, C.L. SARS-CoV-2 infection: Can ferroptosis be a potential treatment target for multiple organ involvement? Cell Death Discov. 2020, 6, 130. [Google Scholar] [CrossRef]
- Zhao, K.; Huang, J.; Dai, D.; Feng, Y.; Liu, L.; Nie, S. Serum Iron Level as a Potential Predictor of Coronavirus Disease 2019 Severity and Mortality: A Retrospective Study. Open Forum Infect. Dis. 2020, 7, ofaa250. [Google Scholar] [CrossRef]
- Roshanshad, A.; Kamalipour, A.; Ashraf, M.A.; Roshanshad, R.; Jafari, S.; Nazemi, P.; Akbari, M. The efficacy of remdesivir in coronavirus disease 2019 (COVID-19): A systematic review. Iran. J. Microbiol. 2020, 12, 376. [Google Scholar] [CrossRef]
- Sodeifian, F.; Seyedalhosseini, Z.S.; Kian, N.; Eftekhari, M.; Najari, S.; Mirsaeidi, M.; Farsi, Y.; Nasiri, M.J. Drug-Induced Liver Injury in COVID-19 Patients: A Systematic Review. Front. Med. 2021, 8, 731436. [Google Scholar] [CrossRef]
- Aleem, A.; Mahadevaiah, G.; Shariff, N.; Kothadia, J.P. Hepatic manifestations of COVID-19 and effect of remdesivir on liver function in patients with COVID-19 illness. Bayl. Univ. Med. Cent. Proc. 2021, 34, 473–477. [Google Scholar] [CrossRef] [PubMed]
- Laar, S.A.; Boer, M.G.J.; Gombert-Handoko, K.B.; Guchelaar, H.; Zwaveling, J. LUMC-COVID-19 research group, Liver and kidney function in patients with COVID-19 treated with remdesivir. Br. J. Clin. Pharmacol. 2021, 87, 4450–4454. [Google Scholar] [CrossRef] [PubMed]
- Rahimi, M.M.; Jahantabi, E.; Lotfi, B.; Forouzesh, M.; Valizadeh, R.; Farshid, S. Renal and liver injury following the treatment of COVID-19 by remdesivir. J. Nephropathol. 2020, 10, e10. [Google Scholar] [CrossRef]
- Zampino, R.; Mele, F.; Florio, L.L.; Bertolino, L.; Andini, R.; Galdo, M.; De Rosa, R.; Corcione, A.; Durante-Mangoni, E. Liver injury in remdesivir-treated COVID-19 patients. Hepatol. Int. 2020, 14, 881–883. [Google Scholar] [CrossRef] [PubMed]
- Olry, A.; Meunier, L.; Délire, B.; Larrey, D.; Horsmans, Y.; Le Louët, H. Drug-Induced Liver Injury and COVID-19 Infection: The Rules Remain the Same. Drug Saf. 2020, 43, 615–617. [Google Scholar] [CrossRef] [PubMed]
- Yip, T.C.-F.; Lui, G.C.-Y.; Wong, V.W.-S.; Chow, V.C.-Y.; Ho, T.H.-Y.; Li, T.C.-M.; Tse, Y.-K.; Hui, D.S.-C.; Chan, H.L.-Y.; Wong, G.L.-H. Liver injury is independently associated with adverse clinical outcomes in patients with COVID-19. Gut 2021, 70, 733–742. [Google Scholar] [CrossRef] [PubMed]
- Gabrielli, M.; Franza, L.; Esperide, A.; Gasparrini, I.; Gasbarrini, A.; Franceschi, F.; on behalf of GEMELLI AGAINST COVID 2019. Liver Injury in Patients Hospitalized for COVID-19: Possible Role of Therapy. Vaccines 2022, 10, 192. [Google Scholar] [CrossRef]
- Hu, P.F.; Xie, W.F. Corticosteroid therapy in drug-induced liver injury: Pros and cons. J. Dig. Dis. 2019, 20, 122–126. [Google Scholar] [CrossRef]
- Alqahtani, S.A.; Schattenberg, J.M. Liver injury in COVID-19: The current evidence. United Eur. Gastroenterol. J. 2020, 8, 509–519. [Google Scholar] [CrossRef] [PubMed]
- Muhović, D.; Bojović, J.; Bulatović, A.; Vukčević, B.; Ratković, M.; Lazović, R.; Smolović, B. First case of drug-induced liver injury associated with the use of tocilizumab in a patient with COVID-19. Liver Int. 2020, 40, 1901–1905. [Google Scholar] [CrossRef] [PubMed]
- Galil, S.M.A. Hydroxychloroquine-induced toxic hepatitis in a patient with systemic lupus erythematosus: A case report. Lupus 2015, 24, 638–640. [Google Scholar] [CrossRef]
- Falcão, M.B.; De Góes Cavalcanti, L.P.; Filgueiras Filho, N.M.; Antunes De Brito, C.A. Case Report: Hepatotoxicity Associated with the Use of Hydroxychloroquine in a Patient with COVID-19. Am. J. Trop. Med. Hyg. 2020, 102, 1214–1216. [Google Scholar] [CrossRef]
- Makin, A.J.; Wendon, J.; Fitt, S.; Portmann, B.C.; Williams, R. Fulminant hepatic failure secondary to hydroxychloroquine. Gut 1994, 35, 569–570. [Google Scholar] [CrossRef]
- Brito, C.A.; Barros, F.M.; Lopes, E.P. Mechanisms and consequences of COVID-19 associated liver injury: What can we affirm? World J. Hepatol. 2020, 12, 413–422. [Google Scholar] [CrossRef]
- Echeverría-Esnal, D.; Martin-Ontiyuelo, C.; Navarrete-Rouco, M.E.; Cuscó, M.D.-A.; Ferrández, O.; Horcajada, J.P.; Grau, S. Azithromycin in the treatment of COVID-19: A review. Expert Rev. Anti Infect. Ther. 2021, 19, 147–163. [Google Scholar] [CrossRef] [PubMed]
- Martinez, M.A.; Vuppalanchi, R.; Fontana, R.J.; Stolz, A.; Kleiner, D.E.; Hayashi, P.H.; Gu, J.; Hoofnagle, J.H.; Chalasani, N. Clinical and Histologic Features of Azithromycin-Induced Liver Injury. Clin. Gastroenterol. Hepatol. 2015, 13, 369–376.e3. [Google Scholar] [CrossRef]
- Veit, O.; Beck, B.; Steuerwald, M.; Hatz, C. First case of ivermectin-induced severe hepatitis. Trans. R. Soc. Trop. Med. Hyg. 2006, 100, 795–797. [Google Scholar] [CrossRef]
- Elghannam, M.T.; Hassanien, M.H.; Ameen, Y.A.; ELattar, G.M.; ELRay, A.A.; Turky, E.A.; ELTalkawy, M.D. COVID-19 and liver diseases. Egypt. Liver J. 2022, 12, 43. [Google Scholar] [CrossRef]
- Larson, A.M. Acetaminophen Hepatotoxicity. Clin. Liver Dis. 2007, 11, 525–548. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.; Yan, M.Z.; Li, X.; Lau, E.H.Y. Sequelae of COVID-19 among previously hospitalized patients up to 1 year after discharge: A systematic review and meta-analysis. Infection 2022, 50, 1067–1109. [Google Scholar] [CrossRef]
- Ding, Z.; Li, G.; Chen, L.; Shu, C.; Song, J.; Wang, W.; Wang, Y.; Chen, Q.; Jin, G.; Liu, T.; et al. Association of liver abnormalities with in-hospital mortality in patients with COVID-19. J. Hepatol. 2021, 74, 1295–1302. [Google Scholar] [CrossRef]
- Hindson, J. SARS-CoV-2 in patients with chronic liver disease. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 714. [Google Scholar] [CrossRef] [PubMed]
- Hunt, R.H.; East, J.E.; Lanas, A.; Malfertheiner, P.; Satsangi, J.; Scarpignato, C.; Webb, G.J. COVID-19 and Gastrointestinal Disease: Implications for the Gastroenterologist. Dig. Dis. 2021, 39, 119–139. [Google Scholar] [CrossRef]
- Ferreira, A.I.; Sarmento, M.H.; Cotter, J. Predictors of clinical outcomes of hospitalized patients with COVID-19: Focusing on pre-existing liver disease. Intern. Emerg. Med. 2022, 17, 2209–2217. [Google Scholar] [CrossRef] [PubMed]
- Hartl, L.; Haslinger, K.; Angerer, M.; Jachs, M.; Simbrunner, B.; Bauer, D.J.M.; Semmler, G.; Scheiner, B.; Eigenbauer, E.; Strassl, R.; et al. Age-adjusted mortality and predictive value of liver chemistries in a Viennese cohort of COVID-19 patients. Liver Int. 2022, 42, 1297–1307. [Google Scholar] [CrossRef]
- Gato, S.; Lucena-Valera, A.; Muñoz-Hernández, R.; Sousa, J.M.; Romero-Gómez, M.; Ampuero, J. Impact of COVID-19 on liver disease: From the experimental to the clinic perspective. World J. Virol. 2021, 10, 301–311. [Google Scholar] [CrossRef]
- Kariyawasam, J.C.; Jayarajah, U.; Abeysuriya, V.; Riza, R.; Seneviratne, S.L. Involvement of the Liver in COVID-19: A Systematic Review. Am. J. Trop. Med. Hyg. 2022, 106, 1026–1041. [Google Scholar] [CrossRef]
- Kezer, C.A.; Simonetto, D.A.; Shah, V.H. Sex Differences in Alcohol Consumption and Alcohol-Associated Liver Disease. Mayo Clin. Proc. 2021, 96, 1006–1016. [Google Scholar] [CrossRef]
- Lonardo, A.; Nascimbeni, F.; Ballestri, S.; Fairweather, D.; Win, S.; Than, T.A.; Abdelmalek, M.F.; Suzuki, A. Sex Differences in Nonalcoholic Fatty Liver Disease: State of the Art and Identification of Research Gaps. Hepatology 2019, 70, 1457–1469. [Google Scholar] [CrossRef] [PubMed]
- Poudel, S.; Mishra, A.; Poudel, S.C.; Baskota, A.; Bhattarai, M.; Aryal, A.; Kunwar, A. Liver injury at admission and outcomes in patients with COVID-19 disease: A prospective cohort study. Ann. Med. Surg. 2023, 85, 1534. [Google Scholar] [CrossRef] [PubMed]
- Balaban, H.Y. An overview of SARS-COV-2 related hepatic injury. Hepatol. Forum 2021, 2, 122. [Google Scholar] [CrossRef]
- Soetedjo, N.N.M.; Iryaningrum, M.R.; Damara, F.A.; Permadhi, I.; Sutanto, L.B.; Hartono, H.; Rasyid, H. Prognostic properties of hypoalbuminemia in COVID-19 patients: A systematic review and diagnostic meta-analysis. Clin. Nutr. ESPEN 2021, 45, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Weber, S.; Hellmuth, J.C.; Scherer, C.; Muenchhoff, M.; Mayerle, J.; Gerbes, A.L. Liver function test abnormalities at hospital admission are associated with severe course of SARS-CoV-2 infection: A prospective cohort study. Gut 2021, 70, 1925–1932. [Google Scholar] [CrossRef] [PubMed]
- Gul, Y.; Kilicarslan, G.; Cilengir, A.H.; Balaban, M.; Gul, E. The Relationship of Liver and Pancreas Density with Chest Computed Tomography Score Progression and Laboratory Findings in Patients with COVID-19. J. Comput. Assist. Tomogr. 2022, 46, 848–853. [Google Scholar] [CrossRef] [PubMed]
- Uchida, Y.; Uemura, H.; Yamaba, S.; Hamada, D.; Tarumoto, N.; Maesaki, S.; Mochida, S. Significance of liver dysfunction associated with decreased hepatic CT attenuation values in Japanese patients with severe COVID-19. J. Gastroenterol. 2020, 55, 1098–1106. [Google Scholar] [CrossRef] [PubMed]
- Abdelmohsen, M.A.; Alkandari, B.M.; Gupta, V.K.; ElBeheiry, A.A. Diagnostic value of abdominal sonography in confirmed COVID-19 intensive care patients. Egypt. J. Radiol. Nucl. Med. 2020, 51, 198. [Google Scholar] [CrossRef]
- Spogis, J.; Hagen, F.; Thaiss, W.M.; Hoffmann, T.; Malek, N.; Nikolaou, K.; Berg, C.P.; Singer, S.; Bösmüller, H.; Kreth, F.; et al. Sonographic findings in coronavirus disease-19 associated liver damage. PLoS ONE 2021, 16, e0244781. [Google Scholar] [CrossRef]
- Hirayama, Y.; Daniels, N.F.; Evans, S.; Clarke, D.; Purvis, S.; Oliver, C.; Woodmansey, S.; Staniforth, J.; Soilleux, E.J. High Prevalence of Pre-Existing Liver Abnormalities Identified via Autopsies in COVID-19: Identification of a New Silent Risk Factor? Diagnostics 2021, 11, 1703. [Google Scholar] [CrossRef]
- Hines, A.; Shen, J.G.; Olazagasti, C.; Shams, S. Immune thrombocytopenic purpura and acute liver injury after COVID-19 vaccine. BMJ Case Rep. 2021, 14, e242678. [Google Scholar] [CrossRef] [PubMed]
- Keskin, O.; Oral, H.; Sahin, T.; Kav, T.; Parlak, E. The impact of COVID-19 disease on the natural course of cirrhosis: Before and after starting vaccination. Front. Med. 2023, 9, 1039202. [Google Scholar] [CrossRef] [PubMed]
- Mann, R.; Sekhon, S.; Sekhon, S. Drug-Induced Liver Injury after COVID-19 Vaccine. Cureus 2021, 13, e16491. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.K.H.; Mak, L.Y.; Au, I.C.H.; Lai, F.T.T.; Li, X.; Wan, E.Y.F.; Chui, C.S.L.; Chan, E.W.Y.; Cheng, W.Y.; Cheng, F.W.T.; et al. Risk of acute liver injury following the mRNA (BNT162b2) and inactivated (CoronaVac) COVID-19 vaccines. J. Hepatol. 2022, 77, 1339–1348. [Google Scholar] [CrossRef] [PubMed]
- Efe, C.; Kulkarni, A.V.; Beretta-Piccoli, B.T.; Magro, B.; Stättermayer, A.; Cengiz, M.; Clayton-Chubb, D.; Lammert, C.; Bernsmeier, C.; Gül, Ö.; et al. Liver injury after SARS-CoV-2 vaccination: Features of immune-mediated hepatitis, role of corticosteroid therapy and outcome. Hepatology 2022, 76, 1576–1586. [Google Scholar] [CrossRef] [PubMed]
- Lodato, F.; Larocca, A.; D’Errico, A.; Cennamo, V. An unusual case of acute cholestatic hepatitis after m-RNABNT162b2 (Comirnaty) SARS-CoV-2 vaccine: Coincidence, autoimmunity or drug-related liver injury. J. Hepatol. 2021, 75, 1254–1256. [Google Scholar] [CrossRef] [PubMed]
- Roy, A.; Verma, N.; Singh, S.; Pradhan, P.; Taneja, S.; Singh, M. Immune-mediated liver injury following COVID-19 vaccination: A systematic review. Hepatol. Commun. 2022, 6, 2513–2522. [Google Scholar] [CrossRef]
- Shroff, H.; Satapathy, S.K.; Crawford, J.M.; Todd, N.J.; VanWagner, L.B. Liver injury following SARS-CoV-2 vaccination: A multicenter case series. J. Hepatol. 2022, 76, 211–214. [Google Scholar] [CrossRef]
- Luxenburger, H.; Thimme, R. SARS-CoV-2 and the liver: Clinical and immunological features in chronic liver disease. Gut 2023, 72, 1783–1794. [Google Scholar] [CrossRef]
- Mekritthikrai, K.; Jaru-Ampornpan, P.; Komolmit, P.; Thanapirom, K. Autoimmune Hepatitis Triggered by COVID-19 Vaccine: The First Case from Inactivated Vaccine. ACG Case Rep. J. 2022, 9, e00811. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.Q.; Terrault, N.A.; Tacke, F.; Gluud, L.L.; Arrese, M.; Bugianesi, E.; Loomba, R. Global epidemiology of cirrhosis—Aetiology, trends and predictions. Nat. Rev. Gastroenterol. Hepatol. 2023, 20, 388–398. [Google Scholar] [CrossRef] [PubMed]
- James, S.L.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Murray, Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef]
- Ray, G. Management of liver diseases: Current perspectives. World J. Gastroenterol. 2022, 28, 5818–5826. [Google Scholar] [CrossRef] [PubMed]
- Vos, T.; Lim, S.S.; Abbafati, C.; Abbas, K.M.; Abbasi, M.; Abbasifard, M.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd-Allah, F.; Abdelalim, A.; et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Vujčić, I. Outcomes of COVID-19 among patients with liver disease. World J. Gastroenterol. 2023, 29, 815–824. [Google Scholar] [CrossRef]
- Ekpanyapong, S.; Reddy, K.R. Liver and Biliary Tract Disease in Patients with Coronavirus disease-2019 Infection. Gastroenterol. Clin. N. Am. 2023, 52, 13–36. [Google Scholar] [CrossRef]
- Gupta, T.; Sharma, H. COVID-19 and the liver: Are footprints still there? World J. Gastroenterol. 2023, 29, 656–669. [Google Scholar] [CrossRef]
- Walia, D.; Saraya, A.; Gunjan, D. COVID-19 in patients with pre-existing chronic liver disease—Predictors of outcomes. World J. Virol. 2023, 12, 30–43. [Google Scholar] [CrossRef]
- Perreault, G.; Ching, C.; Nobel, Y.R. COVID-19 in patients with liver disease and liver transplant: Clinical implications, prevention, and management. Ther. Adv. Gastroenterol. 2023, 16, 17562848231188586. [Google Scholar] [CrossRef] [PubMed]
- Ali, F.E.M.; El-Aziz, M.K.A.; Ali, M.M.; Ghogar, O.M.; Bakr, A.G. COVID-19 and hepatic injury: Diversity and risk assessment. World J. Gastroenterol. 2023, 29, 425–449. [Google Scholar] [CrossRef]
- Campbell, P.T.; Fix, O.K. Coronavirus Disease-2019 and Implications on the Liver. Clin. Liver Dis. 2023, 27, 27–45. [Google Scholar] [CrossRef]
- Nagarajan, R.; Krishnamoorthy, Y.; Rajaa, S.; Hariharan, V.S. COVID-19 Severity and Mortality Among Chronic Liver Disease Patients: A Systematic Review and Meta-Analysis. Prev. Chronic Dis. 2022, 19, 210228. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, J.S.; Garcia-Tsao, G.; Biggins, S.W.; Kamath, P.S.; Wong, F.; McGeorge, S.; Shaw, J.; Pearson, M.; Chew, M.; Fagan, A.; et al. Comparison of mortality risk in patients with cirrhosis and COVID-19 compared with patients with cirrhosis alone and COVID-19 alone: Multicentre matched cohort. Gut 2021, 70, 531–536. [Google Scholar] [CrossRef]
- Iavarone, M.; D’Ambrosio, R.; Soria, A.; Triolo, M.; Pugliese, N.; Del Poggio, P.; Perricone, G.; Massironi, S.; Spinetti, A.; Buscarini, E.; et al. High rates of 30-day mortality in patients with cirrhosis and COVID-19. J. Hepatol. 2020, 73, 1063–1071. [Google Scholar] [CrossRef] [PubMed]
- Qi, X.; Liu, Y.; Wang, J.; Fallowfield, J.A.; Wang, J.; Li, X.; Shi, J.; Pan, H.; Zou, S.; Zhang, H.; et al. Clinical course and risk factors for mortality of COVID-19 patients with pre-existing cirrhosis: A multicentre cohort study. Gut 2021, 70, 433–436. [Google Scholar] [CrossRef]
- Wang, Y.; Hu, M.; Yang, H. Cirrhosis is an independent predictor for COVID-19 mortality: A meta-analysis of confounding cofactors-controlled data. J. Hepatol. 2023, 78, e28–e31. [Google Scholar] [CrossRef]
- Brozat, J.F.; Hanses, F.; Haelberger, M.; Stecher, M.; Dreher, M.; Tometten, L.; Ruethrich, M.M.; Vehreschild, J.J.; Trautwein, C.; Borgmann, S.; et al. COVID-19 mortality in cirrhosis is determined by cirrhosis-associated comorbidities and extrahepatic organ failure: Results from the multinational LEOSS registry. United Eur. Gastroenterol. J. 2022, 10, 409–424. [Google Scholar] [CrossRef]
- Nawghare, P.; Jain, S.; Chandnani, S.; Bansal, S.; Patel, S.; Debnath, P.; Rane, S.; Deshmukh, R.; Rathi, P.; Contractor, Q. Predictors of Severity and Mortality in Chronic Liver Disease Patients with COVID-19 During the Second Wave of the Pandemic in India. Cureus 2022, 14, e20891. [Google Scholar] [CrossRef]
- Fedeli, U.; Amidei, C.B.; Casotto, V.; Grande, E.; Saia, M.; Zanetto, A.; Russo, F.P. Mortality from chronic liver disease: Recent trends and impact of the COVID-19 pandemic. World J. Gastroenterol. 2023, 29, 4166–4173. [Google Scholar] [CrossRef] [PubMed]
- Gacouin, A.; Locufier, M.; Uhel, F.; Letheulle, J.; Bouju, P.; Fillatre, P.; Le Tulzo, Y.; Tadié, J.M. Liver Cirrhosis is Independently Associated with 90-Day Mortality in ARDS Patients. Shock 2016, 45, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.Q.; Mathurin, P.; Cortez-Pinto, H.; Loomba, R. Global epidemiology of alcohol-associated cirrhosis and HCC: Trends, projections and risk factors. Nat. Rev. Gastroenterol. Hepatol. 2023, 20, 37–49. [Google Scholar] [CrossRef] [PubMed]
- Martinez, M.A.; Franco, S. Impact of COVID-19 in Liver Disease Progression. Hepatol. Commun. 2021, 5, 1138–1150. [Google Scholar] [CrossRef] [PubMed]
- Masi, P.; Hékimian, G.; Lejeune, M.; Chommeloux, J.; Desnos, C.; De Chambrun, M.P.; Martin-Toutain, I.; Nieszkowska, A.; Lebreton, G.; Bréchot, N.; et al. Systemic Inflammatory Response Syndrome Is a Major Contributor to COVID-19-Associated Coagulopathy: Insights From a Prospective, Single-Center Cohort Study. Circulation 2020, 142, 611–614. [Google Scholar] [CrossRef]
- Ziehr, D.R.; Alladina, J.; Petri, C.R.; Maley, J.H.; Moskowitz, A.; Medoff, B.D.; Hibbert, K.A.; Thompson, B.T.; Hardin, C.C. Respiratory Pathophysiology of Mechanically Ventilated Patients with COVID-19: A Cohort Study. Am. J. Respir. Crit. Care Med. 2020, 201, 1560–1564. [Google Scholar] [CrossRef]
- Aslam, A.; Kwo, P.Y. Epidemiology and Disease Burden of Alcohol Associated Liver Disease. J. Clin. Exp. Hepatol. 2023, 13, 88–102. [Google Scholar] [CrossRef]
- Hu, W.-S.; Jiang, F.-Y.; Shu, W.; Zhao, R.; Cao, J.-M.; Wang, D.-P. Liver injury in COVID-19: A minireview. World J. Gastroenterol. 2022, 28, 6716–6731. [Google Scholar] [CrossRef]
- Kapuria, D.; Gangu, K.; Chourasia, P.; Boba, A.; Nguyen, A.; Ryu, M.; Peicher, M.; Flores, M.; Chela, H.K.; Daglilar, E.S.; et al. COVID-19 Alcoholic Cirrhosis and Non-Alcoholic Steatohepatitis Cirrhosis Outcomes among Hospitalized Patients in the United States: Insight from National Inpatient Sample Database. Trop. Med. Infect. Dis. 2022, 7, 421. [Google Scholar] [CrossRef]
- Quarleri, J.; Delpino, M.V. Molecular mechanisms implicated in SARS-CoV-2 liver tropism. World J. Gastroenterol. 2022, 28, 6875–6887. [Google Scholar] [CrossRef]
- Cholankeril, G.; Goli, K.; Rana, A.; Hernaez, R.; Podboy, A.; Jalal, P.; Da, B.L.; Satapathy, S.K.; Kim, D.; Ahmed, A.; et al. Impact of COVID-19 Pandemic on Liver Transplantation and Alcohol-Associated Liver Disease in the USA. Hepatology 2021, 74, 3316–3329. [Google Scholar] [CrossRef] [PubMed]
- Han, L.; Shi, H.; Li, Y.; Qi, H.; Wang, Y.; Gu, J.; Wu, J.; Zhao, S.; Cao, P.; Xu, L.; et al. Excess Deaths of Gastrointestinal, Liver, and Pancreatic Diseases During the COVID-19 Pandemic in the United States. Int. J. Public Health 2023, 68, 1606305. [Google Scholar] [CrossRef] [PubMed]
- Deutsch-Link, S.; Curtis, B.; Singal, A.K. COVID-19 and alcohol associated liver disease. Dig. Liver Dis. 2022, 54, 1459–1468. [Google Scholar] [CrossRef] [PubMed]
- Mougharbel, F.; Sampasa-Kanyinga, H.; Heidinger, B.; Corace, K.; Hamilton, H.A.; Goldfield, G.S. Psychological and Demographic Determinants of Substance Use and Mental Health During the COVID-19 Pandemic. Front. Public Health 2021, 9, 680028. [Google Scholar] [CrossRef] [PubMed]
- Steffen, J.; Schlichtiger, J.; Huber, B.C.; Brunner, S. Altered alcohol consumption during COVID-19 pandemic lockdown. Nutr. J. 2021, 20, 44. [Google Scholar] [CrossRef]
- Manikat, R.; Ahmed, A.; Kim, D. The Impact of Alcohol Consumption and Addiction on Liver Transplantation Programs in the COVID-19 Era. Hepatic Med. Evid. Res. 2023, 15, 141–149. [Google Scholar] [CrossRef]
- Ahmed, M.Z.; Ahmed, O.; Aibao, Z.; Hanbin, S.; Siyu, L.; Ahmad, A. Epidemic of COVID-19 in China and associated Psychological Problems. Asian J. Psychiatry 2020, 51, 102092. [Google Scholar] [CrossRef]
- Jackson, S.E.; Garnett, C.; Shahab, L.; Oldham, M.; Brown, J. Association of the COVID-19 lockdown with smoking, drinking and attempts to quit in England: An analysis of 2019–20 data. Addiction 2021, 116, 1233–1244. [Google Scholar] [CrossRef]
- Jain, A.; Sobotka, L.A.; Allen, K.D.; McShane, C.J.; Ramsey, M.L.; Wellner, M.R.; Kirkpatrick, R.B. S1067 Alcohol-Related Liver Disease Increased in Severity During the COVID-19 Pandemic. Am. J. Gastroenterol. 2021, 116, S506. [Google Scholar] [CrossRef]
- Mahmud, N.; Hubbard, R.A.; Kaplan, D.E.; Serper, M. Declining Cirrhosis Hospitalizations in the Wake of the COVID-19 Pandemic: A National Cohort Study. Gastroenterology 2020, 159, 1134–1136.e3. [Google Scholar] [CrossRef]
- Kuo, Y.-F.; Kwo, P.; Wong, R.J.; Singal, A.K. Impact of COVID-19 on Liver Transplant Activity in the USA: Variation by Etiology and Cirrhosis Complications. J. Clin. Transl. Hepatol. 2022, 11, 130. [Google Scholar] [CrossRef]
- Milivojević, V.; Bogdanović, J.; Babić, I.; Todorović, N.; Ranković, I. Metabolic Associated Fatty Liver Disease (MAFLD) and COVID-19 Infection: An Independent Predictor of Poor Disease Outcome? Medicina 2023, 59, 1438. [Google Scholar] [CrossRef]
- Bhurwal, A.; Minacapelli, C.D.; Orosz, E.; Gupta, K.; Tait, C.; Dalal, I.; Zhang, C.; Zhao, E.; Rustgi, V.K. COVID-19 status quo: Emphasis on gastrointestinal and liver manifestations. World J. Gastroenterol. 2021, 27, 7969–7981. [Google Scholar] [CrossRef]
- Gaspar, R.; Branco, C.C.; Macedo, G. Liver and COVID-19: From care of patients with liver diseases to liver injury. World J. Hepatol. 2021, 13, 1367–1377. [Google Scholar] [CrossRef]
- Kayaaslan, B.; Guner, R. COVID-19 and the liver: A brief and core review. World J. Hepatol. 2021, 13, 2013–2023. [Google Scholar] [CrossRef] [PubMed]
- Sirinawasatien, A.; Chantarojanasiri, T.; Ekpanyapong, S.; Tivatunsakul, N.; Luvira, V. Coronavirus disease 2019 gastrointestinal and liver manifestations in adults: A review. JGH Open 2021, 5, 1257–1265. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, H.C.; Trudeau, S. COVID-19 + Cirrhosis = Excess Hospital Confinement, Excess Casualties. Dig. Dis. Sci. 2023, 68, 4290–4291. [Google Scholar] [CrossRef] [PubMed]
- Marano, G.; Traversi, G.; Gaetani, E.; Pola, R.; Claro, A.E.; Mazza, M. Alcohol use disorder and liver injury related to the COVID-19 pandemic. World J. Hepatol. 2022, 14, 1875–1883. [Google Scholar] [CrossRef] [PubMed]
- Nayak, B.; Lal, G.; Kumar, S.; Das, C.J.; Saraya, A. Shalimar, Host Response to SARS-CoV2 and Emerging Variants in Pre-Existing Liver and Gastrointestinal Diseases. Front. Cell. Infect. Microbiol. 2021, 11, 753249. [Google Scholar] [CrossRef] [PubMed]
- Cargill, Z.; Kattiparambil, S.; Hansi, N.; Barnabas, A.; Shawcross, D.L.; Williams, R.; Agarwal, K. Severe alcohol-related liver disease admissions post-COVID-19 lockdown: Canary in the coal mine? Frontline Gastroenterol. 2021, 12, 354–355. [Google Scholar] [CrossRef] [PubMed]
- Moon, A.M.; Curtis, B.; Mandrekar, P.; Singal, A.K.; Verna, E.C.; Fix, O.K. Alcohol-Associated Liver Disease before and after COVID-19—An Overview and Call for Ongoing Investigation. Hepatol. Commun. 2021, 5, 1616–1621. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Huang, Y.; Zheng, T.; Sun, C.; Yang, K.; Pang, M. Gastrointestinal hospitalization during COVID-19 pandemic in the United States: Analysis of a nationwide inpatient sample. J. Gastroenterol. Hepatol. 2023, 38, 1971–1979. [Google Scholar] [CrossRef] [PubMed]
- Sobotka, L.A.; Jain, A.; Peng, J.; Allen, K.D.; McShane, C.J.; Ramsey, M.L.; Wellner, M.R.; Kirkpatrick, R.B. Patients with alcohol-related liver disease hospitalized during the COVID-19 pandemic experienced worse outcomes. Ann. Hepatol. 2023, 28, 101088. [Google Scholar] [CrossRef] [PubMed]
- Philips, C.A.; Rela, M.; Soin, A.S.; Gupta, S.; Surendran, S.; Augustine, P. Critical Update on the Diagnosis and Management of COVID-19 in Advanced Cirrhosis and Liver Transplant Recipients. J. Clin. Transl. Hepatol. 2021, 9, 947. [Google Scholar] [CrossRef] [PubMed]
- Sedarous, M.; Youssef, M.; Adekunle, A.D.; Babajide, O.; Rubens, M.; Okafor, P.N. A63 trends and outcomes of liver disease hospitalizations during the coronavirus pandemic in the United States: A nationwide population-level analysis. J. Can. Assoc. Gastroenterol. 2023, 6, 34–35. [Google Scholar] [CrossRef]
- Nuovo, G.J.; Suster, D.; Awad, H.; Michaille, J.-J.; Tili, E. The histologic and molecular correlates of liver disease in fatal COVID-19 including with alcohol use disorder. Ann. Diagn. Pathol. 2022, 57, 151881. [Google Scholar] [CrossRef]
- Bucurica, S.; Radu, F.I.; Bucurica, A.; Socol, C.; Prodan, I.; Tudor, I.; Sirbu, C.A.; Plesa, F.C.; Jinga, M. Risk of New-Onset Liver Injuries Due to COVID-19 in Preexisting Hepatic Conditions—Review of the Literature. Medicina 2022, 59, 62. [Google Scholar] [CrossRef]
- Zanon, M.; Neri, M.; Pizzolitto, S.; Radaelli, D.; Concato, M.; Peruch, M.; D’Errico, S. Liver pathology in COVID-19 related death and leading role of autopsy in the pandemic. World J. Gastroenterol. 2023, 29, 200–220. [Google Scholar] [CrossRef]
- Brandi, N.; Spinelli, D.; Granito, A.; Tovoli, F.; Piscaglia, F.; Golfieri, R.; Renzulli, M. COVID-19: Has the Liver Been Spared? Int. J. Mol. Sci. 2023, 24, 1091. [Google Scholar] [CrossRef]
- Singh, S.; Khan, A. Clinical Characteristics and Outcomes of Coronavirus Disease 2019 among Patients with Preexisting Liver Disease in the United States: A Multicenter Research Network Study. Gastroenterology 2020, 159, 768–771.e3. [Google Scholar] [CrossRef]
- Kim, D.; Adeniji, N.; Latt, N.; Kumar, S.; Bloom, P.P.; Aby, E.S.; Perumalswami, P.; Roytman, M.; Li, M.; Vogel, A.S.; et al. Predictors of Outcomes of COVID-19 in Patients with Chronic Liver Disease: US Multi-center Study. Clin. Gastroenterol. Hepatol. 2021, 19, 1469–1479.e19. [Google Scholar] [CrossRef]
- Marjot, T.; Moon, A.M.; Cook, J.A.; Abd-Elsalam, S.; Aloman, C.; Armstrong, M.J.; Pose, E.; Brenner, E.J.; Cargill, T.; Catana, M.-A.; et al. Outcomes following SARS-CoV-2 infection in patients with chronic liver disease: An international registry study. J. Hepatol. 2021, 74, 567–577. [Google Scholar] [CrossRef]
- Holbeck, M.; DeVries, H.S.; Singal, A.K. Integrated Multidisciplinary Management of Alcohol-Associated Liver Disease. J. Clin. Transl. Hepatol. 2023, 11, 1404. [Google Scholar] [CrossRef] [PubMed]
- Parker, R.; Allison, M.; Anderson, S.; Aspinall, R.; Bardell, S.; Bains, V.; Buchanan, R.; Corless, L.; Davidson, I.; Dundas, P.; et al. Quality standards for the management of alcohol-related liver disease: Consensus recommendations from the British Association for the Study of the Liver and British Society of Gastroenterology ARLD special interest group. BMJ Open Gastroenterol. 2023, 10, e001221. [Google Scholar] [CrossRef]
- Shah, N.D.; Ventura-Cots, M.; Abraldes, J.G.; Alboraie, M.; Alfadhli, A.; Argemi, J.; Badia-Aranda, E.; Arús-Soler, E.; Barritt, A.S.; Bessone, F.; et al. Alcohol-Related Liver Disease Is Rarely Detected at Early Stages Compared with Liver Diseases of Other Etiologies Worldwide. Clin. Gastroenterol. Hepatol. 2019, 17, 2320–2329.e12. [Google Scholar] [CrossRef] [PubMed]
- Mitrovic, N.; Sabanovic, M.; Vujovic, A.; Jovanovic, J.; Nikolic, N.; Jug, M.; Todorovic, N.; Filipovic, A.; Milosevic, I. Influence of chronic liver diseases on the course and outcome of COVID-19. PLoS ONE 2023, 18, e0288350. [Google Scholar] [CrossRef]
- Paterson, C.W.; Gutierrez, M.B.; Coopersmith, C.M.; Ford, M.L. Impact of chronic alcohol exposure on conventional and regulatory murine T cell subsets. Front. Immunol. 2023, 14, 1142614. [Google Scholar] [CrossRef]
- Varghese, J.; Dakhode, S. Effects of Alcohol Consumption on Various Systems of the Human Body: A Systematic Review. Cureus 2022, 14, 30057. [Google Scholar] [CrossRef]
- De Jesus, R.P.; De Carvalho, J.F.; De Oliveira, L.P.M.; Cunha, C.D.M.; Alves, T.C.H.S.; Vieira, S.T.B.; Figueiredo, V.M.; Bueno, A.A. Metabolic and nutritional triggers associated with increased risk of liver complications in SARS-CoV-2. World J. Hepatol. 2022, 14, 80–97. [Google Scholar] [CrossRef] [PubMed]
- Luo, M.; Ballester, M.P.; Soffientini, U.; Jalan, R.; Mehta, G. SARS-CoV-2 infection and liver involvement. Hepatol. Int. 2022, 16, 755–774. [Google Scholar] [CrossRef]
- Baldelli, L.; Marjot, T.; Barnes, E.; Barritt, A.S.; Webb, G.J.; Moon, A.M. SARS-CoV-2 Infection and Liver Disease: A Review of Pathogenesis and Outcomes. Gut Liver 2023, 17, 12–23. [Google Scholar] [CrossRef]
- Forsyth, C.B.; Voigt, R.M.; Swanson, G.R.; Bishehsari, F.; Shaikh, M.; Zhang, L.; Engen, P.; Keshavarzian, A. Alcohol use disorder as a potential risk factor for COVID-19 severity: A narrative review. Alcohol. Clin. Exp. Res. 2022, 46, 1930–1943. [Google Scholar] [CrossRef]
- Testino, G. Are Patients with Alcohol Use Disorders at Increased Risk for COVID-19 Infection? Alcohol Alcohol. 2020, 55, 344–346. [Google Scholar] [CrossRef] [PubMed]
- Zsichla, L.; Müller, V. Risk Factors of Severe COVID-19: A Review of Host, Viral and Environmental Factors. Viruses 2023, 15, 175. [Google Scholar] [CrossRef]
- Park, S.H.; Lee, Y.-S.; Sim, J.; Seo, S.; Seo, W. Alcoholic liver disease: A new insight into the pathogenesis of liver disease. Arch. Pharm. Res. 2022, 45, 447–459. [Google Scholar] [CrossRef]
- Lewis, S.A.; Doratt, B.M.; Sureshchandra, S.; Jankeel, A.; Newman, N.; Shen, W.; Grant, K.A.; Messaoudi, I. Ethanol Consumption Induces Nonspecific Inflammation and Functional Defects in Alveolar Macrophages. Am. J. Respir. Cell Mol. Biol. 2022, 67, 112–124. [Google Scholar] [CrossRef]
- Murthy, P.; Narasimha, V.L. Effects of the COVID-19 pandemic and lockdown on alcohol use disorders and complications. Curr. Opin. Psychiatry 2021, 34, 376–385. [Google Scholar] [CrossRef] [PubMed]
- Bailey, K.L.; Samuelson, D.R.; Wyatt, T.A. Alcohol use disorder: A pre-existing condition for COVID-19? Alcohol 2021, 90, 11–17. [Google Scholar] [CrossRef]
- Rodriguez-Miguelez, P.; Heefner, A.; Carbone, S. Recognizing risk factors associated with poor outcomes among patients with COVID-19. Prog. Cardiovasc. Dis. 2023, 76, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Zhong, R.; Zhang, Q.; Qiu, Y.; Chen, L.; Xie, J.; Chen, Y.; Zou, Y.; Zhu, L.; Tong, L.; Zou, Y.; et al. Results of the Adult COVID-19 Lifestyle Matching Study. Int. J. Public Health 2022, 67, 1604329. [Google Scholar] [CrossRef]
- Antwi, I.; Watkins, D.; Pedawi, A.; Ghrayeb, A.; Van De Vuurst, C.; Cory, T.J. Substances of abuse and their effect on SAR-CoV-2 pathogenesis. NeuroImmune Pharmacol. Ther. 2023, 2, 301–316. [Google Scholar] [CrossRef]
- Lewis, S.A.; Doratt, B.M.; Qiao, Q.; Blanton, M.; Grant, K.A.; Messaoudi, I. Integrated single cell analysis shows chronic alcohol drinking disrupts monocyte differentiation in the bone marrow. Stem Cell Rep. 2023, 18, 1884–1897. [Google Scholar] [CrossRef]
- Iheanacho, C.O.; Enechukwu, O.H. COVID-19-associated liver injury, role of drug therapy and management: A review. Egypt. Liver J. 2022, 12, 66. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Liu, J.; Zhou, Y.; Zhao, X.; Zhao, Q.; Liu, J. The effect of corticosteroid treatment on patients with coronavirus infection: A systematic review and meta-analysis. J. Infect. 2020, 81, e13–e20. [Google Scholar] [CrossRef]
- Huang, B.-H.; Inan-Eroglu, E.; Shaban, R.Z.; Hamer, M.; Britton, A.; Stamatakis, E. Alcohol intake and mortality risk of COVID-19, pneumonia, and other infectious diseases: An analysis of 437191 UK biobank participants. Prev. Med. Rep. 2022, 26, 101751. [Google Scholar] [CrossRef]
- Chick, J. Alcohol and COVID-19. Alcohol Alcohol. 2020, 55, 341–342. [Google Scholar] [CrossRef] [PubMed]
- Inayat, F.; Ali, H.; Patel, P.; Dhillon, R.; Afzal, A.; Rehman, A.U.; Afzal, M.S.; Zulfiqar, L.; Nawaz, G.; Goraya, M.H.N.; et al. Association between alcohol-associated cirrhosis and inpatient complications among COVID-19 patients: A propensity-matched analysis from the United States. World J. Virol. 2023, 12, 221–232. [Google Scholar] [CrossRef]
- Nevola, R.; Criscuolo, L.; Beccia, D.; Femine, A.D.; Ruocco, R.; Imbriani, S.; Alfano, M.; Villani, A.; Russo, A.; Perillo, P.; et al. Impact of chronic liver disease on SARS-CoV-2 infection outcomes: Roles of stage, etiology and vaccination. World J. Gastroenterol. 2023, 29, 800–814. [Google Scholar] [CrossRef]
- Bhangui, P. Impact of the COVID-19 Pandemic on Patients with End-Stage Liver Disease: One Virus—A Plethora of Consequences. J. Clin. Exp. Hepatol. 2023, 13, 725–727. [Google Scholar] [CrossRef]
- Krishnan, A.; Prichett, L.; Liu, Y.; Ting, P.; Alqahtani, S.A.; Kim, A.K.; Ma, M.; Hamilton, J.P.; Woreta, T.A.; Chen, P.-H. Risk of Severe Illness and Risk Factors of Outcomes of COVID-19 in Hospitalized Patients with Chronic Liver Disease in a Major U.S. Hospital Network. Can. J. Gastroenterol. Hepatol. 2022, 2022, 8407990. [Google Scholar] [CrossRef]
- Wang, Q.; Davis, P.B.; Xu, R. COVID-19 risk, disparities and outcomes in patients with chronic liver disease in the United States. eClinicalMedicine 2021, 31, 100688. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.; Zhou, H.; Hodgkinson, C.; Montero, A.; Goldman, D.; Chang, S.L. Network Meta-Analysis on the Mechanisms Underlying Alcohol Augmentation of COVID-19 Pathologies. Alcohol. Clin. Exp. Res. 2021, 45, 675–688. [Google Scholar] [CrossRef] [PubMed]
- Marjot, T.; Eberhardt, C.S.; Boettler, T.; Belli, L.S.; Berenguer, M.; Buti, M.; Jalan, R.; Mondelli, M.U.; Moreau, R.; Shouval, D.; et al. Impact of COVID-19 on the liver and on the care of patients with chronic liver disease, hepatobiliary cancer, and liver transplantation: An updated EASL position paper. J. Hepatol. 2022, 77, 1161–1197. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Research Type | Markers of ALF (ALT, AST or TBIL) | Cases | ALF | Prognostic Indicator | |
|---|---|---|---|---|---|
| 1. Bogline 2022 [71] | Retrospective | >1 ULN | 434 | 123 | NR |
| 2. Desai 2020 [72] | Retrospective | >1 ULN | 639 | 476 | b |
| 3. Shousha 2021 [73] | Cohort study | >1 ULN | 428 | 137 | b |
| 4. Wang 2020 [74] | Cohort study | >1 ULN | 657 | 303 | a |
| 5. Wang 2020 [75] | Cohort study | >1 ULN | 339 | 96 | b |
| 6. Piano 2020 [76] | Retrospective | >1 ULN | 565 | 329 | bc |
| 7. Phipps 2020 [77] | Retrospective | >2 ULN | 2273 | 489 | ab |
| 8. Mishra 2021 [78] | Retrospective | >1 ULN | 348 | 184 | c |
| 9. Chew 2021 [79] | Cohort study | >5 ULN | 834 | 105 | bc |
| 10. Chen 2021 [80] | Cohort study | >1 ULN | 830 | 227 | ab |
| 11. Krishnan 2022 [81] | Retrospective | >1 ULN | 3830 | 2698 | ab |
| 12. Zhang 2021 [82] | Retrospective | >1 ULN | 440 | 254 | abc |
| 13. BJ 2021 [83] | Retrospective | >1 ULN | 382 | 159 | abc |
| 14. Chu 2020 [84] | Cohort study | >2 ULN | 838 | 429 | ab |
| 15. Hassanin 2021 [85] | Retrospective | >2 ULN | 1238 | 296 | c |
| 16. Cai 2020 [86] | Cohort study | >1 ULN | 417 | 192 | a |
| 17. Fu 2020 [87] | Retrospective | >1 ULN | 482 | 142 | abc |
| 18. Siddiqui 2021 [88] | Retrospective | >4 ULN | 1935 | 396 | NR |
| 19. Faghih 2022 [89] | Cohort study | >1 ULN | 1017 | 324 | ab |
| 20. Cholongitas 2022 [90] | Retrospective | >5 ULN | 1046 | 53 | c |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Michalak, A.; Lach, T.; Szczygieł, K.; Cichoż-Lach, H. COVID-19, Possible Hepatic Pathways and Alcohol Abuse—What Do We Know up to 2023? Int. J. Mol. Sci. 2024, 25, 2212. https://doi.org/10.3390/ijms25042212
Michalak A, Lach T, Szczygieł K, Cichoż-Lach H. COVID-19, Possible Hepatic Pathways and Alcohol Abuse—What Do We Know up to 2023? International Journal of Molecular Sciences. 2024; 25(4):2212. https://doi.org/10.3390/ijms25042212
Chicago/Turabian StyleMichalak, Agata, Tomasz Lach, Karolina Szczygieł, and Halina Cichoż-Lach. 2024. "COVID-19, Possible Hepatic Pathways and Alcohol Abuse—What Do We Know up to 2023?" International Journal of Molecular Sciences 25, no. 4: 2212. https://doi.org/10.3390/ijms25042212
APA StyleMichalak, A., Lach, T., Szczygieł, K., & Cichoż-Lach, H. (2024). COVID-19, Possible Hepatic Pathways and Alcohol Abuse—What Do We Know up to 2023? International Journal of Molecular Sciences, 25(4), 2212. https://doi.org/10.3390/ijms25042212