
Interactions between Gut Microbiota and Oral Antihyperglycemic Drugs: A Systematic Review


 ,
, 

Abstract
:1. Introduction
2. Methods
- Population: individuals aged 19 years and older who have been diagnosed with type 2 diabetes mellitus.
- Treatment: oral antihyperglycemic medications given to these subjects.
- Comparison: regular treatment vs. placebo.
- Objective: to determine the correlation between gut microbiota and oral antihyperglycemic medications.
3. Results
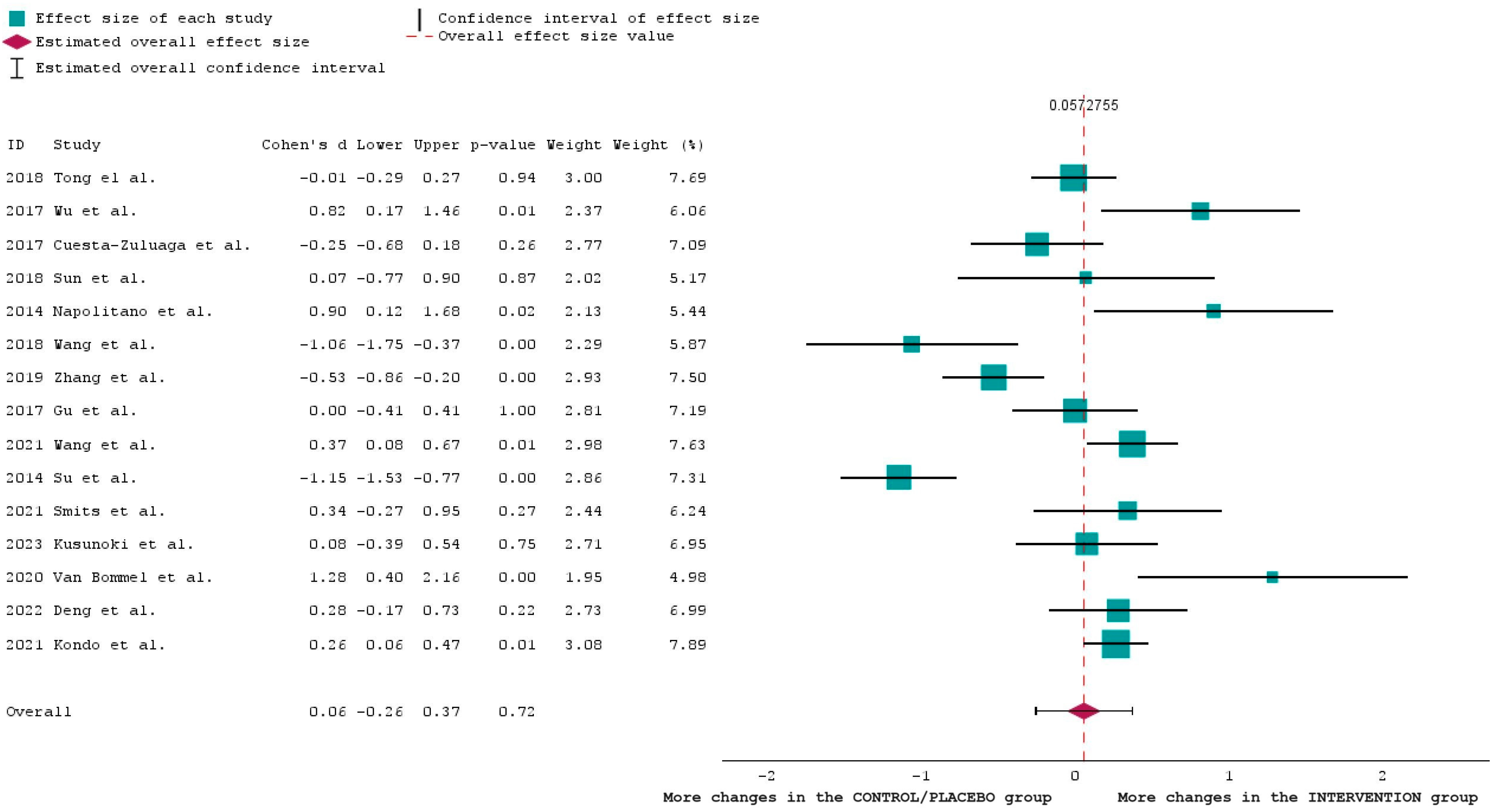
Statistical Analysis of the Results
4. Discussion
4.1. Bacterial Phyla Commonly Found in the Gut Microbiota and Their Potential Interactions with Antidiabetic Drugs
4.2. Microbial-Based Therapeutics as a Preventative Measure for T2DM
4.3. Mechanisms of Antihyperglycemic Drugs
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Liu, W.; Luo, Z.; Zhou, J.; Sun, B. Gut Microbiota and Antidiabetic Drugs: Perspectives of Personalized Treatment in Type 2 Diabetes Mellitus. Front. Cell. Infect. Microbiol. 2022, 12, 853771. [Google Scholar] [CrossRef]
- Diabetes Facets and Figures|International Diabetes Federation. International Diabetes Federation. Available online: https://idf.org/about-diabetes/diabetes-facts-figures/ (accessed on 14 September 2023).
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2009, 32, S62–S67. [Google Scholar] [CrossRef]
- Wu, Y.; Ding, Y.; Tanaka, Y.; Zhang, W. Risk factors contributing to type 2 diabetes and recent advances in the treatment and prevention. Int. J. Med. Sci. 2014, 11, 1185–1200. [Google Scholar] [CrossRef]
- Craciun, C.-I.; Neag, M.-A.; Catinean, A.; Mitre, A.-O.; Rusu, A.; Bala, C.; Roman, G.; Buzoianu, A.-D.; Muntean, D.-M.; Craciun, A.-E. The Relationships between Gut Microbiota and Diabetes Mellitus, and Treatments for Diabetes Mellitus. Biomedicines 2022, 10, 308. [Google Scholar] [CrossRef]
- Iatcu, C.O.; Steen, A.; Covasa, M. Gut Microbiota and Complications of Type-2 Diabetes. Nutrients 2021, 14, 166. [Google Scholar] [CrossRef]
- Paul, P.; Kaul, R.; Abdellatif, B.; Arabi, M.; Upadhyay, R.; Saliba, R.; Sebah, M.; Chaari, A. The Promising Role of Microbiome Therapy on Biomarkers of Inflammation and Oxidative Stress in Type 2 Diabetes: A Systematic and Narrative Review. Front. Nutr. 2022, 9, 906243. [Google Scholar] [CrossRef] [PubMed]
- Guinane, C.M.; Cotter, P.D. Role of the gut microbiota in health and chronic gastrointestinal disease: Understanding a hidden metabolic organ. Ther. Adv. Gastroenterol. 2013, 6, 295–308. [Google Scholar] [CrossRef] [PubMed]
- Kant, R.; Chandra, L.; Verma, V.; Nain, P.; Bello, D.; Patel, S.; Ala, S.; Chandra, R.; Antony, M.A. Gut microbiota interactions with anti-diabetic medications and pathogenesis of type 2 diabetes mellitus. World J. Methodol. 2022, 12, 246–257. [Google Scholar] [CrossRef] [PubMed]
- Rinninella, E.; Raoul, P.; Cintoni, M.; Franceschi, F.; Miggiano, G.A.D.; Gasbarrini, A.; Mele, M.C. What Is the Healthy Gut Microbiota Composition? A Changing Ecosystem across Age, Environment, Diet, and Diseases. Microorganisms 2019, 7, 14. [Google Scholar] [CrossRef] [PubMed]
- LeBlanc, J.G.; Milani, C.; de Giori, G.S.; Sesma, F.; van Sinderen, D.; Ventura, M. Bacteria as vitamin suppliers to their host: A gut microbiota perspective. Curr. Opin. Biotechnol. 2012, 24, 160–168. [Google Scholar] [CrossRef] [PubMed]
- Kovatcheva-Datchary, P.; Tremaroli, V.; Bäckhed, F. The Gut Microbiota. In The Prokaryotes; Rosenberg, E., DeLong, E.F., Lory, S., Stackebrandt, E., Thompson, F., Eds.; Springer: Berlin/Heidelberg, Germany, 2013. [Google Scholar] [CrossRef]
- Hou, K.; Wu, Z.-X.; Chen, X.-Y.; Wang, J.-Q.; Zhang, D.; Xiao, C.; Zhu, D.; Koya, J.B.; Wei, L.; Li, J.; et al. Microbiota in health and diseases. Signal Transduct. Target. Ther. 2022, 7, 135. [Google Scholar] [CrossRef]
- Bull, M.J.; Plummer, N.T. Part 1: The Human Gut Microbiome in Health and Disease. Integr. Med. 2014, 13, 17–22. [Google Scholar]
- Eriksen, M.B.; Frandsen, T.F. The impact of patient, intervention, comparison, outcome (PICO) as a search strategy tool on literature search quality: A systematic review. J. Med. Libr. Assoc. 2018, 106, 420–431. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews Systematic reviews and Meta-Analyses. BMJ 2021, 372, 71. [Google Scholar] [CrossRef]
- Tong, X.; Xu, J.; Lian, F.; Yu, X.; Zhao, Y.; Xu, L.; Zhang, M.; Zhao, X.; Shen, J.; Wu, S.; et al. Structural Alteration of Gut Microbiota during the Amelioration of Human Type 2 Diabetes with Hyperlipidemia by Metformin and a Traditional Chinese Herbal Formula: A Multicenter, Randomized, Open Label Clinical Trial. mBio 2018, 9, e02392-17. [Google Scholar] [CrossRef]
- Hosomi, K.; Saito, M.; Park, J.; Murakami, H.; Shibata, N.; Ando, M.; Nagatake, T.; Konishi, K.; Ohno, H.; Tanisawa, K.; et al. Oral administration of Blautia wexlerae ameliorates obesity and type 2 diabetes via metabolic remodeling of the gut microbiota. Nat. Commun. 2022, 13, 4477. [Google Scholar] [CrossRef]
- Martín, R.; Rios-Covian, D.; Huillet, E.; Auger, S.; Khazaal, S.; Bermúdez-Humarán, L.G.; Sokol, H.; Chatel, J.-M.; Langella, P. Faecalibacterium: A bacterial genus with promising human health applications. FEMS Microbiol. Rev. 2023, 47, fuad039. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Esteve, E.; Tremaroli, V.; Khan, M.T.; Caesar, R.; Mannerås-Holm, L.; Ståhlman, M.; Olsson, L.M.; Serino, M.; Planas-Fèlix, M.; et al. Metformin alters the gut microbiome of individuals with treatment-naive type 2 diabetes, contributing to the therapeutic effects of the drug. Nat. Med. 2017, 23, 850–858. [Google Scholar] [CrossRef] [PubMed]
- E. coli Infection: Symptoms and Prevention|familydoctor.org. Available online: https://familydoctor.org/condition/e-coli-infection/ (accessed on 29 September 2023).
- Center, C.S.M. Gut Bacteria May Play a Role in Diabetes. 10 May 2023. Available online: https://www.cedars-sinai.org/newsroom/gut-bacteria-may-play-a-role-in-diabetes/ (accessed on 11 February 2024).
- Pintarič, M.; Langerholc, T. Probiotic Mechanisms Affecting Glucose Homeostasis: A Scoping Review. Life 2022, 12, 1187. [Google Scholar] [CrossRef] [PubMed]
- Bojović, K.; Ignjatović, Đ.; Bajic, S.S.; Milutinović, D.V.; Tomić, M.; Golić, N.; Tolinački, M. Gut Microbiota Dysbiosis Associated With Altered Production of Short Chain Fatty Acids in Children With Neurodevelopmental Disorders. Front. Cell. Infect. Microbiol. 2020, 10, 223. [Google Scholar] [CrossRef] [PubMed]
- de la Cuesta-Zuluaga, J.; Mueller, N.T.; Corrales-Agudelo, V.; Velásquez-Mejía, E.P.; Carmona, J.A.; Abad, J.M.; Escobar, J.S. Metformin Is Associated With Higher Relative Abundance of Mucin-Degrading Akkermansia muciniphilaand Several Short-Chain Fatty Acid–Producing Microbiota in the Gut. Diabetes Care 2017, 40, 54–62. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, V.F.; Elias-Oliveira, J.; Pereira, S.; Pereira, J.A.; Barbosa, S.C.; Machado, M.S.G.; Carlos, D. Akkermansia muciniphila and Gut Immune System: A Good Friendship That Attenuates Inflammatory Bowel Disease, Obesity, and Diabetes. Front. Immunol. 2022, 13, 934695. [Google Scholar] [CrossRef] [PubMed]
- Butyrivibrio|Healthmatters.io. Available online: https://healthmatters.io/understand-blood-test-results/butyrivibrio#:~:text=’Butyrivibrio’%20is%20a%20genus%20of,bacterial%20richness%20in%20the%20gut (accessed on 11 February 2024).
- Robertson, R. Why Bifidobacteria Are So Good for You. Healthline. Available online: https://www.healthline.com/nutrition/why-bifidobacteria-are-good#:~:text=Bifidobacteria%20help%20produce%20other%20important,into%20the%20blood%20(%2018%20) (accessed on 13 July 2023).
- Carey, M.A.; Medlock, G.L.; Alam, M.; Kabir, M.; Uddin, J.; Nayak, U.; Papin, J.; Faruque, A.S.G.; Haque, R.; Petri, W.A.; et al. Megasphaera in the Stool Microbiota Is Negatively Associated with Diarrheal Cryptosporidiosis. Clin. Infect. Dis. 2021, 73, e1242–e1251. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Zhou, L.; Sun, L.; Ye, X.; Ma, M.; Dou, M.; Shi, L. Association Between Intestinal Prevotella copri Abundance and Glycemic Fluctuation in Patients with Brittle Diabetes. Diabetes Metab. Syndr. Obes. Targets Ther. 2023, 16, 1613–1621. [Google Scholar] [CrossRef] [PubMed]
- Vasilakopoulou, A.; Vourli, S.; Siafakas, N.; Kavatha, D.; Tziolos, N.; Pournaras, S. Enterococcus casseliflavus Bacteraemia in a Patient with Chronic Renal Disease. Infect. Dis. Rep. 2020, 12, 70–73. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Xie, C.; Wang, G.; Wu, Y.; Wu, Q.; Wang, X.; Liu, J.; Deng, Y.; Xia, J.; Chen, B.; et al. Gut microbiota and intestinal FXR mediate the clinical benefits of metformin. Nat. Med. 2018, 24, 1919–1929. [Google Scholar] [CrossRef] [PubMed]
- Gilmore, W.J.; Johnston, E.L.; Bitto, N.J.; Zavan, L.; O’Brien-Simpson, N.; Hill, A.F.; Kaparakis-Liaskos, M. Bacteroides fragilis outer membrane vesicles preferentially activate innate immune receptors compared to their parent bacteria. Front. Immunol. 2022, 13, 970725. [Google Scholar] [CrossRef]
- Napolitano, A.; Miller, S.; Nicholls, A.W.; Baker, D.; Van Horn, S.; Thomas, E.; Rajpal, D.; Spivak, A.; Brown, J.R.; Nunez, D.J. Novel gut-based pharmacology of metformin in patients with type 2 diabetes mellitus. PLoS ONE 2014, 9, e100778, Erratum in PLoS ONE 2014, 9, e106594. [Google Scholar] [CrossRef]
- Knoop, F.C. Bacteroides Infections. In xPharm: The Comprehensive Pharmacology Reference; Elsevier: Amsterdam, The Netherlands, 2007. [Google Scholar] [CrossRef]
- Wang, Z.; Saha, S.; Van Horn, S.; Thomas, E.; Traini, C.; Sathe, G.; Rajpal, D.K.; Brown, J.R. Gut microbiome differences between metformin- and liraglutide-treated T2DM subjects. Endocrinol. Diabetes Metab. 2017, 1, e00009. [Google Scholar] [CrossRef]
- Hiippala, K.; Kainulainen, V.; Kalliomäki, M.; Arkkila, P.; Satokari, R. Mucosal Prevalence and Interactions with the Epithelium Indicate Commensalism of Sutterella spp. Front. Microbiol. 2016, 7, 1706. [Google Scholar] [CrossRef]
- Rios-Covian, D.; Salazar, N.; Gueimonde, M.; de los Reyes-Gavilan, C.G. Shaping the Metabolism of Intestinal Bacteroides Population through Diet to Improve Human Health. Front. Microbiol. 2017, 8, 376. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Wang, M.; Yang, J.; Xu, Q.; Liang, C.; Chen, B.; Zhang, J.; Yang, Y.; Wang, H.; Shang, Y.; et al. Response of gut microbiota in type 2 diabetes to hypoglycemic agents. Endocrine 2019, 66, 485–493. [Google Scholar] [CrossRef]
- Spirochetal Diseases (Syphilis, Lyme Disease, and Leptospirosis): Transmission, Pathogenesis, Host-Pathogen Interactions, Prevention, and Treatment. Frontiers. Available online: https://www.frontiersin.org/research-topics/57789/spirochetal-diseases-syphilis-lyme-disease-and-leptospirosis-transmission-pathogenesis-host-pathogen-interactions-prevention-and-treatment (accessed on 17 February 2024).
- Lynch, J.B.; Gonzalez, E.L.; Choy, K.; Faull, K.F.; Jewell, T.; Arellano, A.; Liang, J.; Yu, K.B.; Paramo, J.; Hsiao, E.Y. Gut microbiota Turicibacter strains differentially modify bile acids and host lipids. Nat. Commun. 2023, 14, 3669. [Google Scholar] [CrossRef] [PubMed]
- Groeger, S.; Zhou, Y.; Ruf, S.; Meyle, J. Pathogenic Mechanisms of Fusobacterium nucleatum on Oral Epithelial Cells. Front. Oral Health 2022, 3, 831607. [Google Scholar] [CrossRef] [PubMed]
- Gao, H.; Li, X.; Chen, X.; Hai, D.; Wei, C.; Zhang, L.; Li, P. The Functional Roles of Lactobacillus acidophilus in Different Physiological and Pathological Processes. J. Microbiol. Biotechnol. 2022, 32, 1226–1233. [Google Scholar] [CrossRef] [PubMed]
- Gu, Y.; Wang, X.; Li, J.; Zhang, Y.; Zhong, H.; Liu, R.; Zhang, D.; Feng, Q.; Xie, X.; Hong, J.; et al. Analyses of gut microbiota and plasma bile acids enable stratification of patients for antidiabetic treatment. Nat. Commun. 2017, 8, 1785. [Google Scholar] [CrossRef]
- Su, B.; Liu, H.; Li, J.; Sunli, Y.; Liu, B.; Liu, D.; Zhang, P.; Meng, X. Acarbose treatment affects the serum levels of inflammatory cytokines and the gut content of bifidobacteria in Chinese patients with type 2 diabetes mellitus. J. Diabetes 2015, 7, 729–739. [Google Scholar] [CrossRef]
- Rios-Covian, D.; Arboleya, S.; Hernandez-Barranco, A.M.; Alvarez-Buylla, J.R.; Ruas-Madiedo, P.; Gueimonde, M.; Reyes-Gavilan, C.G.d.L. Interactions between bifidobacterium and bacteroides species in cofermentations are affected by carbon sources, including exopolysaccharides produced by bifidobacteria. Appl. Environ. Microbiol. 2013, 79, 7518–7524. [Google Scholar] [CrossRef]
- Said, M.S.; Tirthani, E.; Lesho, E. Enterococcus Infections. [Updated 2022 May 2]. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK567759/ (accessed on 22 January 2024).
- Kondo, Y.; Hashimoto, Y.; Hamaguchi, M.; Ando, S.; Kaji, A.; Sakai, R.; Inoue, R.; Kashiwagi, S.; Mizushima, K.; Uchiyama, K.; et al. Unique Habitual Food Intakes in the Gut Microbiota Cluster Associated with Type 2 Diabetes Mellitus. Nutrients 2021, 13, 3816. [Google Scholar] [CrossRef]
- Liu, H.; Li, X.; Zhu, Y.; Huang, Y.; Zhang, Q.; Lin, S.; Fang, C.; Li, L.; Lv, Y.; Mei, W.; et al. Effect of Plant-Derived n-3 Polyunsaturated Fatty Acids on Blood Lipids and Gut Microbiota: A Double-Blind Randomized Controlled Trial. Front. Nutr. 2022, 9, 830960. [Google Scholar] [CrossRef]
- Kusunoki, M.; Hisano, F.; Matsuda, S.-I.; Kusunoki, A.; Wakazono, N.; Tsutsumi, K.; Miyata, T. Effects of SGLT2 inhibitors on the intestinal bacterial flora in Japanese patients with type 2 diabetes mellitus. Drug Res. 2023, 73, 412–416. [Google Scholar] [CrossRef] [PubMed]
- Cronin, P.; Joyce, S.A.; O’Toole, P.W.; O’Connor, E.M. Dietary Fibre Modulates the Gut Microbiota. Nutrients 2021, 13, 1655. [Google Scholar] [CrossRef] [PubMed]
- van Bommel, E.J.M.; Herrema, H.; Davids, M.; Kramer, M.H.H.; Nieuwdorp, M.; van Raalte, D.H. Effects of 12-week treatment with dapagliflozin and gliclazide on faecal microbiome: Results of a double-blind randomized trial in patients with type 2 diabetes. Diabetes Metab. 2019, 46, 164–168. [Google Scholar] [CrossRef] [PubMed]
- Deng, X.; Zhang, C.; Wang, P.; Wei, W.; Shi, X.; Wang, P.; Yang, J.; Wang, L.; Tang, S.; Fang, Y.; et al. Cardiovascular Benefits of Empagliflozin Are Associated with Gut Microbiota and Plasma Metabolites in Type 2 Diabetes. J. Clin. Endocrinol. Metab. 2022, 107, 1888–1896. [Google Scholar] [CrossRef]
- Nie, K.; Ma, K.; Luo, W.; Shen, Z.; Yang, Z.; Xiao, M.; Tong, T.; Yang, Y.; Wang, X. Roseburia intestinalis: A Beneficial Gut Organism from the Discoveries in Genus and Species. Front. Cell. Infect. Microbiol. 2021, 11, 757718. [Google Scholar] [CrossRef]
- Mukherjee, A.; Lordan, C.; Ross, R.P.; Cotter, P.D. Gut microbes from the phylogenetically diverse genus Eubacterium and their various contributions to gut health. Gut Microbes 2020, 12, 1802866. [Google Scholar] [CrossRef]
- Belotserkovsky, I.; Sansonetti, P.J. Shigella and Enteroinvasive Escherichia coli. Curr. Top. Microbiol. Immunol. 2018, 416, 1–26. [Google Scholar] [CrossRef] [PubMed]
- Murros, K.E. Hydrogen Sulfide Produced by Gut Bacteria May Induce Parkinson’s Disease. Cells 2022, 11, 978. [Google Scholar] [CrossRef]
- Patton, M.J.; Orihuela, C.J.; Harrod, K.S.; Bhuiyan, M.A.N.; Dominic, P.; Kevil, C.G.; Fort, D.; Liu, V.X.; Farhat, M.; Koff, J.L.; et al. COVID-19 bacteremic co-infection is a major risk factor for mortality, ICU admission, and mechanical ventilation. Crit. Care 2023, 27, 34. [Google Scholar] [CrossRef]
- Wang, Z.; Wang, J.; Hu, J.; Chen, Y.; Dong, B.; Wang, Y. A comparative study of acarbose, vildagliptin and saxagliptin intended for better efficacy and safety on type 2 diabetes mellitus treatment. Life Sci. 2021, 274, 119069. [Google Scholar] [CrossRef]
- Lee, H.; An, J.; Kim, J.; Choi, D.; Song, Y.; Lee, C.-K.; Kong, H.; Kim, S.B.; Kim, K. A Novel Bacterium, Butyricimonas virosa, Preventing HFD-Induced Diabetes and Metabolic Disorders in Mice via GLP-1 Receptor. Front. Microbiol. 2022, 13, 858192. [Google Scholar] [CrossRef]
- Yang, X.; Zhang, M.; Liu, Y.; Wei, F.; Li, X.; Feng, Y.; Jin, X.; Liu, D.; Guo, Y.; Hu, Y. Inulin-enriched Megamonas funiformis ameliorates metabolic dysfunction-associated fatty liver disease by producing propionic acid. NPJ Biofilms Microbiomes 2023, 9, 1–16. [Google Scholar] [CrossRef]
- Li, X.; Gu, N.; Huang, T.Y.; Zhong, F.; Peng, G. Pseudomonas aeruginosa: A typical biofilm forming pathogen and an emerging but underestimated pathogen in food processing. Front. Microbiol. 2023, 13, 1114199. [Google Scholar] [CrossRef]
- Klebsiella pneumoniae in Healthcare Settings|HAI|CDC. Available online: https://www.cdc.gov/hai/organisms/klebsiella/klebsiella.html (accessed on 16 January 2024).
- Smits, M.M.; Fluitman, K.S.; Herrema, H.; Davids, M.; Kramer, M.H.; Groen, A.K.; Belzer, C.; de Vos, W.M.; Cahen, D.L.; Nieuwdorp, M.; et al. Liraglutide and sitagliptin have no effect on intestinal microbiota composition: A 12-week randomized placebo-controlled trial in adults with type 2 diabetes. Diabetes Metab. 2021, 47, 101223. [Google Scholar] [CrossRef]
- Li, G.; Zeng, J.; Tian, J.; Levine, M.A.; Thabane, L. Multiple uses of forest plots in presenting analysis results in health research: A Tutorial. J. Clin. Epidemiol. 2019, 117, 89–98. [Google Scholar] [CrossRef]
- Ahn, E.; Kang, H. Introduction to systematic review and meta-analysis. Korean J. Anesthesiol. 2018, 71, 103–112. [Google Scholar] [CrossRef]
- Yi, M. A Complete Guide to Bubble Charts. Chartio. Available online: https://chartio.com/learn/charts/bubble-chart-complete-guide/ (accessed on 23 October 2019).
- Gurung, M.; Li, Z.; You, H.; Rodrigues, R.; Jump, D.B.; Morgun, A.; Shulzhenko, N. Role of gut microbiota in type 2 diabetes pathophysiology. EBioMedicine 2020, 51, 102590. [Google Scholar] [CrossRef]
- Dash, N.R.; Al Bataineh, M.T.; Alili, R.; Al Safar, H.; Alkhayyal, N.; Prifti, E.; Zucker, J.D.; Belda, E.; Clément, K. Functional alterations and predictive capacity of gut microbiome in type 2 diabetes. Sci. Rep. 2023, 13, 22386. [Google Scholar] [CrossRef] [PubMed]
- Petakh, P.; Oksenych, V.; Kamyshnyi, A. The F/B ratio as a biomarker for inflammation in COVID-19 and T2D: Impact of metformin. Biomed. Pharmacother. 2023, 163, 114892. [Google Scholar] [CrossRef] [PubMed]
- Stojanov, S.; Berlec, A.; Štrukelj, B. The Influence of Probiotics on the Firmicutes/Bacteroidetes Ratio in the Treatment of Obesity and Inflammatory Bowel disease. Microorganisms 2020, 8, 1715. [Google Scholar] [CrossRef] [PubMed]
- Magne, F.; Gotteland, M.; Gauthier, L.; Zazueta, A.; Pesoa, S.; Navarrete, P.; Balamurugan, R. The Firmicutes/Bacteroidetes Ratio: A Relevant Marker of Gut Dysbiosis in Obese Patients? Nutrients 2020, 12, 1474. [Google Scholar] [CrossRef]
- Sierra, A.C.; Ramos-Lopez, O.; Riezu-Boj, J.I.; Milagro, F.I.; Martinez, J.A. Diet, Gut Microbiota, and Obesity: Links with Host Genetics and Epigenetics and Potential Applications. Adv. Nutr. 2019, 10, S17–S30. [Google Scholar] [CrossRef]
- Tilg, H.; Moschen, A.R. Microbiota and diabetes: An evolving relationship. Gut 2014, 63, 1513–1521. [Google Scholar] [CrossRef]
- Ryan, P.M.; Patterson, E.; Carafa, I.; Mandal, R.; Wishart, D.S.; Dinan, T.G.; Cryan, J.F.; Tuohy, K.M.; Stanton, C.; Ross, R.P. Metformin and Dipeptidyl Peptidase-4 Inhibitor Differentially Modulate the Intestinal Microbiota and Plasma Metabolome of Metabolically Dysfunctional Mice. Can. J. Diabetes 2019, 44, 146–155.e2. [Google Scholar] [CrossRef]
- Ye, J.; Wu, Z.; Zhao, Y.; Zhang, S.; Liu, W.; Su, Y. Role of gut microbiota in the pathogenesis and treatment of diabetes mullites: Advanced research-based review. Front. Microbiol. 2022, 13, 1029890. [Google Scholar] [CrossRef] [PubMed]
- Rizzatti, G.; Lopetuso, L.R.; Gibiino, G.; Binda, C.; Gasbarrini, A. Proteobacteria: A Common Factor in Human Diseases. BioMed Res. Int. 2017, 2017, 9351507. [Google Scholar] [CrossRef] [PubMed]
- Meloni, A.R.; DeYoung, M.B.; Lowe, C.; Parkes, D.G. GLP-1 receptor activated insulin secretion from pancreatic β-cells: Mechanism and glucose dependence. Diabetes Obes. Metab. 2012, 15, 15–27. [Google Scholar] [CrossRef] [PubMed]
- Jia, L.; Huang, S.; Sun, B.; Shang, Y.; Zhu, C. Pharmacomicrobiomics and type 2 diabetes mellitus: A novel perspective towards possible treatment. Front. Endocrinol. 2023, 14, 1149256. [Google Scholar] [CrossRef] [PubMed]
- Whang, A.; Nagpal, R.; Yadav, H. Bi-directional drug-microbiome interactions of anti-diabetics. EBioMedicine 2018, 39, 591–602. [Google Scholar] [CrossRef]
- Geerlings, S.Y.; Kostopoulos, I.; De Vos, W.M.; Belzer, C. Akkermansia muciniphila in the Human Gastrointestinal Tract: When, Where, and How? Microorganisms 2018, 6, 75. [Google Scholar] [CrossRef] [PubMed]
- Letchumanan, G.; Abdullah, N.; Marlini, M.; Baharom, N.; Lawley, B.; Omar, M.R.; Mohideen, F.B.S.; Addnan, F.H.; Fariha, M.M.N.; Ismail, Z.; et al. Gut Microbiota Composition in Prediabetes and Newly Diagnosed Type 2 Diabetes: A Systematic Review of Observational Studies. Front. Cell. Infect. Microbiol. 2022, 12, 943427. [Google Scholar] [CrossRef]
- Pan, Y.-Q.; Zheng, Q.-X.; Jiang, X.-M.; Chen, X.-Q.; Zhang, X.-Y.; Wu, J.-L. Probiotic Supplements Improve Blood Glucose and Insulin Resistance/Sensitivity among Healthy and GDM Pregnant Women: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Evid.-Based Complement. Altern. Med. 2021, 2021, 9830200. [Google Scholar] [CrossRef]
- Tonucci, L.B.; dos Santos, K.M.O.; de Oliveira, L.L.; Ribeiro, S.M.R.; Martino, H.S.D. Clinical application of probiotics in type 2 diabetes mellitus: A randomized, double-blind, placebo-controlled study. Clin. Nutr. 2017, 36, 85–92. [Google Scholar] [CrossRef]
- Toshimitsu, T.; Gotou, A.; Furuichi, K.; Hachimura, S.; Asami, Y. Effects of 12-wk Lactobacillus plantarum OLL2712 treatment on glucose metabolism and chronic inflammation in prediabetic individuals: A single-arm pilot study. Nutrition 2018, 58, 175–180. [Google Scholar] [CrossRef]
- Samah, S.; Ramasamy, K.; Lim, S.M.; Neoh, C.F. Probiotics for the management of type 2 diabetes mellitus: A systematic review and meta-analysis. Diabetes Res. Clin. Pract. 2016, 118, 172–182. [Google Scholar] [CrossRef]
- Nasri, H.; Rafieian-Kopaei, M. Metformin: Current knowledge. J. Res. Med. Sci. 2014, 19, 658–664. [Google Scholar] [PubMed]
- Top, W.M.C.; Kooy, A.; Stehouwer, C.D.A. Metformin: A Narrative Review of Its Potential Benefits for Cardiovascular Disease, Cancer and Dementia. Pharmaceuticals 2022, 15, 312. [Google Scholar] [CrossRef] [PubMed]
- Gruzman, A.; Babai, G.; Sasson, S. Adenosine Monophosphate-Activated Protein Kinase (AMPK) as a New Target for Antidiabetic Drugs: A Review on Metabolic, Pharmacological and Chemical Considerations. Rev. Diabet. Stud. 2009, 6, 13–36. [Google Scholar] [CrossRef]
- Lee, Y.; Kim, A.H.; Kim, E.; Lee, S.; Yu, K.-S.; Jang, I.-J.; Chung, J.-Y.; Cho, J.-Y. Changes in the gut microbiome influence the hypoglycemic effect of metformin through the altered metabolism of branched-chain and nonessential amino acids. Diabetes Res. Clin. Pract. 2021, 178, 108985. [Google Scholar] [CrossRef] [PubMed]
- Tang, R.; Li, L. Modulation of Short-Chain Fatty Acids as Potential Therapy Method for Type 2 Diabetes Mellitus. Can. J. Infect. Dis. Med. Microbiol. 2021, 2021, 6632266. [Google Scholar] [CrossRef]
- Bin Lee, C.; Chae, S.U.; Jo, S.J.; Jerng, U.M.; Bae, S.K. The Relationship between the Gut Microbiome and Metformin as a Key for Treating Type 2 Diabetes Mellitus. Int. J. Mol. Sci. 2021, 22, 3566. [Google Scholar] [CrossRef]
- Tilves, C.; Yeh, H.-C.; Maruthur, N.; Juraschek, S.P.; Miller, E.R.; Appel, L.J.; Mueller, N.T. A behavioral weight-loss intervention, but not metformin, decreases a marker of gut barrier permeability: Results from the SPIRIT randomized trial. Int. J. Obes. 2022, 46, 655–660. [Google Scholar] [CrossRef] [PubMed]
- Gillard, J.; Leclercq, I.A. Biological tuners to reshape the bile acid pool for therapeutic purposes in non-alcoholic fatty liver disease. Clin. Sci. 2023, 137, 65–85. [Google Scholar] [CrossRef]
- Shin, N.R.; Lee, J.C.; Lee, H.Y.; Kim, M.S.; Whon, T.W.; Lee, M.S.; Bae, J.W. An increase in the Akkermansia spp. population induced by metformin treatment improves glucose homeostasis in diet-induced obese mice. Gut 2014, 63, 727–735. [Google Scholar] [CrossRef]
- Srinivas, N.; Sarnaik, M.K.; Modi, S.; Pisipati, Y.; Vaidya, S.; Gaggatur, N.S.; Sange, A.H.; Sange, I. Sodium-Glucose Cotransporter 2 (SGLT-2) Inhibitors: Delving Into the Potential Benefits of Cardiorenal Protection Beyond the Treatment of Type-2 Diabetes Mellitus. Cureus 2021, 13, e16868. [Google Scholar] [CrossRef]
- Tentolouris, A.; Vlachakis, P.; Tzeravini, E.; Eleftheriadou, I.; Tentolouris, N. SGLT2 Inhibitors: A Review of Their Antidiabetic and Cardioprotective Effects. Int. J. Environ. Res. Public Health 2019, 16, 2965. [Google Scholar] [CrossRef]
- Elbere, I.; Silamikelis, I.; Dindune, I.I.; Kalnina, I.; Ustinova, M.; Zaharenko, L.; Silamikele, L.; Rovite, V.; Gudra, D.; Konrade, I.; et al. Baseline gut microbiome composition predicts metformin therapy short-term efficacy in newly diagnosed type 2 diabetes patients. PLoS ONE 2020, 15, e0241338. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Shi, F.-H.; Liu, W.; Zhang, M.-C.; Feng, R.-L.; Qian, C.; Liu, W.; Ma, J. Dapagliflozin Modulates the Fecal Microbiota in a Type 2 Diabetic Rat Model. Front. Endocrinol. 2020, 11, 635. [Google Scholar] [CrossRef]
- Crudele, L.; Gadaleta, R.M.; Cariello, M.; Moschetta, A. Gut microbiota in the pathogenesis and therapeutic approaches of diabetes. EBioMedicine 2023, 97, 104821. [Google Scholar] [CrossRef]
- Li, J.-M.; Yu, R.; Zhang, L.-P.; Wen, S.-Y.; Wang, S.-J.; Zhang, X.-Y.; Xu, Q.; Kong, L.-D. Dietary fructose-induced gut dysbiosis promotes mouse hippocampal neuroinflammation: A benefit of short-chain fatty acids. Microbiome 2019, 7, 98. [Google Scholar] [CrossRef]
- Martín, M.; Ramos, S. Dietary Flavonoids and Insulin Signaling in Diabetes and Obesity. Cells 2021, 10, 1474. [Google Scholar] [CrossRef] [PubMed]
- Hue, L.; Taegtmeyer, H.; Kasper, J.D.; Meyer, R.A.; Beard, D.A.; Wiseman, R.W.; Wang, T.; Yao, W.; Li, J.; He, Q.; et al. The Randle cycle revisited: A new head for an old hat. Am. J. Physiol. Metab. 2009, 297, E578–E591. [Google Scholar] [CrossRef] [PubMed]
- Singh, A. Dipeptidyl peptidase-4 inhibitors: Novel mechanism of actions. Indian J. Endocrinol. Metab. 2014, 18, 753–759. [Google Scholar] [CrossRef] [PubMed]
- Rahman, S.; Hossain, K.S.; Das, S.; Kundu, S.; Adegoke, E.O.; Rahman, A.; Hannan, A.; Uddin, J.; Pang, M.-G. Role of Insulin in Health and Disease: An Update. Int. J. Mol. Sci. 2021, 22, 6403. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.; Egan, J.M. The role of incretins in glucose homeostasis and diabetes treatment. Pharmacol. Rev. 2008, 60, 470–512. [Google Scholar] [CrossRef] [PubMed]
- Garber, A.J. Incretin effects on β-cell function, replication, and mass. Diabetes Care 2011, 34, S258–S263. [Google Scholar] [CrossRef]
- Razavi, M.; Wei, Y.-Y.; Rao, X.-Q.; Zhong, J.-X. DPP-4 inhibitors and GLP-1RAs: Cardiovascular safety and benefits. Mil. Med. Res. 2022, 9, 45. [Google Scholar] [CrossRef]
- Nadkarni, P.; Chepurny, O.G.; Holz, G.G. Regulation of glucose homeostasis by GLP-1. Prog. Mol. Biol. Transl. Sci. 2014, 121, 23–65. [Google Scholar] [CrossRef]
- Den Besten, G.; van Eunen, K.; Groen, A.K.; Venema, K.; Reijngoud, D.-J.; Bakker, B.M. The role of short-chain fatty acids in the interplay between diet, gut microbiota, and host energy metabolism. J. Lipid Res. 2013, 54, 2325–2340. [Google Scholar] [CrossRef] [PubMed]
- Akmal, M.; Wadhwa, R. Alpha Glucosidase Inhibitors. [Updated 2022 Aug 12]. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK557848/ (accessed on 19 January 2024).
- Dirir, A.M.; Daou, M.; Yousef, A.F.; Yousef, L.F. A review of alpha-glucosidase inhibitors from plants as potential candidates for the treatment of type-2 diabetes. Phytochem. Rev. 2021, 21, 1049–1079. [Google Scholar] [CrossRef]
- Standl, E.; Schnell, O. Alpha-glucosidase inhibitors 2012—Cardiovascular considerations and trial evaluation. Diabetes Vasc. Dis. Res. 2012, 9, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Lu, H.; Xie, T.; Wu, Q.; Hu, Z.; Luo, Y.; Luo, F. Alpha-Glucosidase Inhibitory Peptides: Sources, Preparations, Identifications, and Action Mechanisms. Nutrients 2023, 15, 4267. [Google Scholar] [CrossRef] [PubMed]
- Lebovitz, H.E. alpha-Glucosidase inhibitors. Endocrinol. Metab. Clin. N. Am. 1997, 26, 539–551. [Google Scholar] [CrossRef] [PubMed]
- Ren, F.; Ji, N.; Zhu, Y. Research Progress of α-Glucosidase Inhibitors Produced by Microorganisms and Their Applications. Foods 2023, 12, 3344. [Google Scholar] [CrossRef] [PubMed]
- Thursby, E.; Juge, N. Introduction to the human gut microbiota. Biochem. J. 2017, 474, 1823–1836. [Google Scholar] [CrossRef] [PubMed]
- Berger, S.I.; Iyengar, R. Role of systems pharmacology in understanding drug adverse events. Wiley Interdiscip. Rev. Syst. Biol. Med. 2010, 3, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Miao, M.; Wang, Q.; Wang, X.; Fan, C.; Luan, T.; Yan, L.; Zhang, Y.; Zeng, X.; Dai, Y.; Li, P. The Protective Effects of Inulin-Type Fructans Against High-Fat/Sucrose Diet-Induced Gestational Diabetes Mice in Association With Gut Microbiota Regulation. Front. Microbiol. 2022, 13, 832151. [Google Scholar] [CrossRef]
- Zhao, Q.; Chen, Y.; Huang, W.; Zhou, H.; Zhang, W. Drug-microbiota interactions: An emerging priority for precision medicine. Signal Transduct. Target. Ther. 2023, 8, 386. [Google Scholar] [CrossRef]
- Fu, Y.; Li, S.; Xiao, Y.; Liu, G.; Fang, J. A Metabolite Perspective on the Involvement of the Gut Microbiota in Type 2 Diabetes. Int. J. Mol. Sci. 2023, 24, 14991. [Google Scholar] [CrossRef]
- Farhana, A.; Rehman, A. Metabolic Consequences of Weight Reduction. [Updated 2023 Jul 10]. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK572145/ (accessed on 19 January 2024).
- Garza, M. What Is the Gut Microbiome and How Does It Relate to Diabetes? diaTribe. 9 March 2022. Available online: https://diatribe.org/what-gut-microbiome-and-how-does-it-relate-diabetes (accessed on 19 January 2024).
- Bica, I.-C.; Pietroșel, V.-A.; Salmen, T.; Diaconu, C.-T.; Braticevici, C.F.; Stoica, R.-A.; Suceveanu, A.I.; Stoian, A.P. The Effects of Cardioprotective Antidiabetic Therapy on Microbiota in Patients with Type 2 Diabetes Mellitus—A Systematic Review. Int. J. Mol. Sci. 2023, 24, 7184. [Google Scholar] [CrossRef]
- Bhandari, P. Statistical Power and Why It Matters|A Simple Introduction. Scribbr. Available online: https://www.scribbr.com/statistics/statistical-power/ (accessed on 22 June 2023).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antidiabetic Drugs | Study | PICO Framework | Key Results | Relation to Gut Microbiota |
|---|---|---|---|---|
| METFORMIN | Tong et al. [17] | Participants: 200 patients diagnosed with T2DM and hyperlipidemia. Intervention: individuals were randomized to either the Metformin-treated group or specifically designed herbal formula (AMC-treated) group. Comparison: results after 12 weeks of treatment. Outcome: the impact of the two medicines on the composition of the intestinal microbiota was assessed by analyzing the V3 and V4 regions of the 16S rRNA gene. | Both Metformin and AMC reduced high blood sugar levels and high lipid levels and caused changes in the composition of gut bacteria in individuals with diabetes. The researchers observed a substantial rise in a group of organisms called Blautia spp., which was strongly associated with improvements in glucose and lipid regulation. AMC demonstrated superior effectiveness in enhancing the homeostasis model assessment of insulin resistance and plasma triglyceride levels, while also showing a significant impact on gut flora. Metformin plus the AMC may improve the condition of T2DM with high levels of lipids by increasing the population of good bacteria. | YES for good bacteria: |
| Wu et al. [20] | Participants: 40 patients newly diagnosed with T2DM. Intervention: patients who had not had any medication before were randomly assigned to either receive a placebo (n = 18) or 1700 mg/d of Metformin (n = 22) for a duration of 4 months. Comparison: clinical characteristics of these individuals before and after treatment. Outcome: to identify how Metformin affects the composition of the gut microbiota. | For this study, whole-genome shotgun sequencing of 131 fecal samples was conducted. The taxonomy and gene profiles were determined by aligning the high-quality reads with nonredundant genome and gene catalogues using the metagenomic data-utilization and analysis (MEDUSA) pipeline. During the 4-month trial period, just a single bacterial strain in the placebo group underwent modification. In contrast, the administration of Metformin for 2 and 4 months led to significant changes in the prevalence of 81 and 86 bacterial species, respectively. The majority of these strains were classified as γ-proteobacteria (such as Escherichia coli) and Firmicutes. The results of the study also show a reduction in Intestinibacter in the group treated with Metformin. | YES for bad bacteria:
| |
| Cuesta-Zuluaga et al. [25] | Participants: 112 individuals. Intervention: authors conducted 16S rRNA gene sequencing to examine the formation and arrangement of the gut microbiota. Comparison: 28 T2DM individuals, with 14 of them using Metformin and 84 individuals without diabetes who were selected to match the participants with diabetes in terms of sex, age, and BMI at a ratio of 3 to 1. Outcome: to find out if Metformin is linked to high levels of bacteria that produce short-chain fatty acids and degrade mucin. | A link was discovered between diabetes and gut microbiota, which was influenced by the usage of Metformin. Participants with diabetes who were taking Metformin had a greater occurrence of Akkermansia muciniphila, a type of microbiota that is known for breaking down mucin, as well as several types of gut microbiota that are known for producing SCFAs, including Butyrivibrio, Bifidobacterium bifidum, Megasphaera, and a specific group within the Prevotella taxonomic unit. People with diabetes who were not taking Metformin showed a greater frequency of Clostridiaceae 02d06 and a unique operational taxonomic unit of Prevotella, as well as a reduced abundance of Enterococcus casseliflavus, in comparison to people without diabetes. | YES for good bacteria:
| |
| Sun et al. [32] | Participants: 22 T2DM patients. Intervention: serum and stool samples were collected from the individuals with T2D. Comparison: the microbiota of the participants was analyzed before and after being treated with 1000 mg Metformin twice daily for 3 days. Outcome: to investigate how Metformin controls gut microbiota and metabolites in humans. | The abundance of Bacteroides fragilis was reduced, but the concentration of the bile acid glycoursodeoxycholic acid was higher in the gastrointestinal tract. The alterations were accompanied by the suppression of intestinal farnesoid X receptor signaling. Metformin functions, at least partially, by using a B. fragilis–GUDCA–intestinal FXR axis to enhance metabolic dysfunction, such as in hyperglycemia. | YES for good bacteria:
| |
| Napolitano et al. [34] | Participants: 14 T2DM patients. Intervention: all subjects had to be on a stable dose of Metformin of ≥1000 mg/day for more than 3 months, which was stopped and later resumed. Comparison: subjects were studied at 4 time points: (i) at baseline on Metformin; (ii) 7 days after stopping it; (iii) when fasting blood glucose (FBG) had risen by 25% after stopping Metformin; (iv) when FBG returned to baseline levels after restarting Metformin. Outcome: to characterize the gut-based mechanisms of Metformin. | Discontinuing Metformin led to a decrease in both active and total GLP-1 levels, while causing an increase in serum bile acids, particularly cholic acid and its conjugates. The aforementioned effects were reversed with the resumption of Metformin. The impact on circulating PYY was rather small, but the alterations in GIP were insignificant. The firmicutes phylum microbiota was positively linked with changes in cholic acid. On the other hand, the Bacteroidetes phylum microbiota was negatively correlated with it. The presence of Firmicutes and Bacteroidetes in the gut microbiota was shown to be associated with the levels of serum PYY. Thus, Metformin has intricate effects resulting from its pharmacological actions in the gut. | YES for bad bacteria:
| |
| Wang et al. [36] | Participants: 37 T2DM patients. Intervention: Part B subjects were switched from oral Metformin to subcutaneous once daily injections of Liraglutide began. Part C subjects remained on Metformin. Comparison: the subjects who were stable on Metformin were randomized into two study arms—Part B (n = 19) and Part C (n = 18). Part A comprised only health volunteers. Outcome: to analyze, after 42 days of trial, the effects of these drugs on the composition of the microbiome. | Both before and after the trial, individuals who were taking Metformin experienced a rise in the proportion of the bacterial group Sutterella. Also, Liraglutide had a positive association, leading to an increase in the bacterial group Akkermansia. The relative abundances of Bacteroides and Akkermansia were strongly linked to the duration of diabetes in the subjects. More precisely, those with shorter and medium durations of diabetes had a notably greater prevalence of Akkermansia compared to those with a longer duration of the condition. | YES for bad bacteria:
| |
| Zhang et al. [39] | Participants: 180 individuals with and without T2DM. Intervention: microbiome compositions were analyzed via a 16S ribosomal RNA gene-based sequencing protocol. Comparison: 130 T2DM patients with a specific hypoglycemic treatment and 50 healthy volunteers. Outcome: to identify how the diabetes treatment affects the microbiota. | The use of hypoglycemic drugs resulted in changes to certain species within the gut microbiota, rather than affecting its overall diversity. Metformin boosted the prevalence of Spirochaete, Turicibacter, and Fusobacterium. Insulin further raised the levels of Fusobacterium, whereas α-glucosidase inhibitors (α-GIs) were responsible for the abundance of Bifidobacterium and Lactobacillus. Both Metformin and insulin improved the metabolism of taurine and hypotaurine, whereas α-GI stimulated many amino acid pathways. While there were similarities in the gut microbial community across those using Metformin and insulin, there were notable differences in each diabetic group with hypoglycemia. | YES for bad bacteria: YES for good bacteria: | |
| AGIs and SULFONY-LUREAS | Gu et al. [44] | Participants: 94 treatment-naïve T2DM patients. Intervention: at the start and after 3 months of therapy, samples of feces and blood were collected. Comparison: 1:1 randomized into Acarbose and Glipizide groups. Outcome: to characterize the clinical effects of Acarbose and Glipizide. | After 3-month therapy, there were substantial decreases in HbA1c levels, as well as fasting and postprandial blood glucose levels, in both groups. The Acarbose group showed a higher decrease in body weight and BMI compared to the Glipizide group. Patients who were administered Acarbose, but not Glipizide, displayed a significant improvement in clinical parameters that are risk factors for metabolic comorbidities and cardiovascular complications associated with T2DM (homeostasis model assessment of insulin resistance, total cholesterol, triglyceride levels, and fatty liver index). Both Acarbose and Glipizide therapy resulted in a reduction in plasma FGF19 levels (a crucial factor generated in the gut that plays a significant role in metabolic health). This suggests that the improvement in HbA1c, FBG, and PBG levels was not subject to FGF19. | NO effect on microbial composition. |
| Su et al. [45] | Participants: 140 participants with and without T2DM. Intervention: inflammatory cytokines were determined using either ELISA or RT-PCR. Comparison: 59 participants were assigned to Group A, who received antidiabetic medication (150 mg of Acarbose per day), and 36 participants to Group B (no Acarbose but received the same treatment as Group A). The control group was formed of 45 healthy individuals. Outcome: to analyze trend differences between the two diabetic groups. | After a 4-week treatment, Bifidobacterium longum and Enterococcus faecalis were seen to have grown in both diabetic groups. Group A had a greater abundance of Bifidobacterium longum, along with reduced levels of LPS and prothrombin activator inhibitor-1. Enterococcus faecalis had a negative association with LPS, whereas Bifidobacterium longum presented a favorable connection with Acarbose treatment and HDL cholesterol levels. Acarbose treatment may increase the presence of Bifidobacterium longum in the intestines of people with type 2 diabetes as well as decrease some inflammatory cytokines, independent of its ability to lower blood sugar levels. | YES for good bacteria:
| |
| Kondo et al. [48] | Participants: 497 individuals. Intervention: collection of fecal samples and analysis the makeup of gut bacteria were conducted. Comparison: 383 patients with T2DM and 114 individuals without T2DM were classified into red, blue, green, and yellow groups. Outcome: to compare the proportions of phyla and genera following the grouping of the gut microbiota into four distinct groups. | The red group had higher proportions of the Bifidobacterium and Lactobacillus genera, while demonstrating reduced proportions of the Blautia and Phascolarctobacterium genera. The red group had a greater percentage of individuals with T2DM who used α-glucosidase inhibitors and Glinide medicines and had a reduced consumption of fermented soybean foods, such as miso soup, compared to the other groups. Additionally, these findings indicate that certain medications for diabetes and fermented food products may play a role in this alteration. | YES for good bacteria:
| |
| SGLT2 INHIBITORS | Kusunoki et al. [50] | Participants: 36 patients with T2DM. Intervention: individuals received a SGLT2 inhibitor (Luseogliflozin or Dapagliflozin) for 3 months. Comparison: the presence of germs in the feces of the patients was assessed both before and after treatment with SGLT2 inhibitors. Outcome: to evaluate the incidence rates of microorganisms that regulate and maintain the equilibrium of the microbiota. | Treatment with SGLT2 inhibitors was shown to significantly enhance the total prevalence of the 12 species of bacteria that regulate balance. Furthermore, there were notable increases in the occurrences of bacteria that produce SCFAs among the microorganisms responsible for maintaining balance. Specific examination of the bacteria responsible for maintaining balance in the body showed that treatment with the SGLT2 inhibitor resulted in a notable rise in the occurrence of Ruminococci. Nevertheless, the SGLT2 inhibitor did not have any impact on the bacteria that disrupt the equilibrium. Thus, SGLT2 inhibitors are linked to a rise in the occurrence of bacteria that regulate balance. | YES for good bacteria:
|
| Van Bommel et al. [52] | Participants: 44 T2DM patients. Intervention: 16S rRNA gene sequencing was used to assess the microbiome. Comparison: for 3 months, 44 patients were randomized to either Dapagliflozin or Gliclazide treatment. Outcome: the microbiome of patients who were already receiving Metformin therapy was analyzed after they received either Dapagliflozin or Gliclazide. | Although both Dapagliflozin and Gliclazide improved glycemic management, Dapagliflozin decreased fasting insulin levels and Gliclazide raised them. Dapagliflozin significantly improved the excretion of glucose in urine; however, Gliclazide did not. Dapagliflozin also led to a reduction in BMI, fat mass percentage, and waist circumference, whereas Gliclazide increased them. However, both treatments had no significant impact on either the diversity or composition of the microbiota. | NO effect on microbial composition. | |
| Deng et al. [53] | Participants: 76 treatment-naïve patients with T2DM at risk of cardiovascular diseases (CVDs). Intervention: patients were treated with either Empagliflozin (10 mg/d, n = 40) or Metformin (1700 mg/d, n = 36). Comparison: the clinical parameters of the two groups were compared. Outcome: to evaluate the changes related to glucose metabolism, CVD’s factors, and gut microbiota using 16S rRNA gene sequencing and plasma metabolites. | HbA1c levels decreased in both groups, but only Empagliflozin group showed a change in the microbiome and an increase in CVD risk. The same group showed raised plasma metabolite levels, while having decreasing levels of glycochenodeoxycholate, cis-aconitate, and uric acid. Simultaneously, Empagliflozin increased the abundance of species from Roseburia, Eubacterium, and Faecalibacterium (SCFAs producing bacteria), while decreasing the presence of many hazardous bacteria, including Escherichia-Shigella, Bilophila, and Hungatella. | YES for good bacteria:
| |
| DDP-4 INHIBITORS | Wang et al. [59] | Participants: 90 T2DM patients. Intervention: individuals were treated with Acarbose, Saxagliptin, and Vildagliptin. Comparison: groups of 30 patients for each medicine. Outcome: to evaluate the efficacy of Acarbose, Saxagliptin, and Vildagliptin in the treatment of T2DM. | Patients had examinations at 0, 4, and 12 weeks post-treatment, during which their vital signs were documented. Fecal samples were collected for the purpose of conducting microbial macrogenome sequencing and safety assessments. There was a reduction in blood glucose levels at 4 and 12 weeks after therapy, and there was a notable difference in the total cholesterol and HDL levels at the 12-week mark. Acarbose first raised the amount of Butyricimonas but then reduced it throughout the course of medication administration. Saxagliptin caused a progressive rise in the level of the Megamonas genus. Also, it reduced the level of the Turicibacter genus. The levels of Pseudomonas, Klebsiella, Blautia, Faecalibacterium, and Roseburia varied during Vildagliptin administration, resulting in a larger rise in fasting C-peptide levels compared to the other two medications. Saxagliptin displayed a higher incidence of adverse events compared to Acarbose and Vildagliptin. The combined use of the three medicines may significantly lower the HbA1c level and impact the distribution of intestinal flora in individuals with T2DM. | YES for good bacteria:
|
| Smits et al. [64] | Participants: 51 patients with T2DM. Intervention: individuals received, once a day for 12 weeks, either Liraglutide, Sitagliptin, or placebos. Comparison: fecal samples were analyzed using 16S rRNA gene sequencing at baseline and after 12 weeks. Outcome: to evaluate the impact of Liraglutide, Sitagliptin, or placebos on the composition of the gut microbiota. | Patients who were already taking Metformin or Sulphonylureas were given either Liraglutide or Sitagliptin. When taken as an additional treatment in T2DM patients who are already taking Metformin, the conclusion is that it does not significantly change the composition of the gut microbiota compared to a placebo. | NO effect on microbial composition. |
| Intervention | Control | Correlation | Count | Lower C.I.* | Upper C.I. |
|---|---|---|---|---|---|
| Mean | Mean | 0.997 | 15 | 0.990 | 0.999 |
| SD | 0.692 | 15 | 0.279 | 0.889 | |
| Population | −0.151 | 15 | −0.616 | 0.391 | |
| SD* | Mean | 0.770 | 15 | 0.426 | 0.920 |
| SD | 0.882 | 15 | 0.675 | 0.960 | |
| Population | 0.044 | 15 | −0.479 | 0.544 | |
| Population | Mean | −0.291 | 15 | −0.699 | 0.260 |
| SD | −0.233 | 15 | −0.666 | 0.317 | |
| Population | 0.714 | 15 | 0.318 | 0.898 |
| Bacteria in the Gut | Antihyperglycemic Drugs | ||
|---|---|---|---|
| Blautia | METFORMIN ↑ | ||
| Faecalibacterium | METFORMIN ↑ | ACARBOSE ↑ | VILDAGLIPTIN ↑ |
| Escherichia coli | METFORMIN ↑ | ||
| Firmicutes | METFORMIN ↑ | ||
| Bifidobacterium | METFORMIN ↑ | ACARBOSE ↑ | |
| Intestinibacter | METFORMIN ↓ | ||
| Akkermansia m. | METFORMIN ↑ | ||
| Butyrivibrio | METFORMIN ↑ | ||
| Bifidobacterium b. | METFORMIN ↑ | ||
| Megasphaera | METFORMIN ↑ | ||
| Prevotella | METFORMIN ↑ | ||
| Enterococcus casseliflavus | METFORMIN ↓ | ACARBOSE ↑ | |
| Bacteroides f. | METFORMIN ↑ | ||
| Firmicutes | METFORMIN ↑ | ||
| Bacteroidetes | METFORMIN ↓ | ||
| Sutterella | METFORMIN ↑ | LIRAGLUTIDE ↑ | |
| Akkermansia | METFORMIN ↑ | LIRAGLUTIDE ↑ | |
| Bacteroides | METFORMIN ↑ | LIRAGLUTIDE ↑ | |
| Spirochaete | METFORMIN ↑ | ||
| Turicibacter | METFORMIN ↑ | ACARBOSE ↓ | |
| Fusobacterium | METFORMIN ↑ | ||
| Bifidobacterium | METFORMIN ↑ | AGIs ↑ | |
| Lactobacillus | METFORMIN ↑ | AGIs ↑ | |
| Butyricimonas | ACARBOSE ↑↓ | ||
| Megamonas | SAXAGLIPTIN ↑ | ACARBOSE ↑ | VILDAGLIPTIN ↑ |
| Pseudomonas | SAXAGLIPTIN ↑ | ACARBOSE ↑ | VILDAGLIPTIN ↑ |
| Klebsiella | SAXAGLIPTIN ↑ | ACARBOSE ↑ | VILDAGLIPTIN ↑ |
| Blautia | SAXAGLIPTIN ↑ | ACARBOSE ↓ | VILDAGLIPTIN ↑ |
| Phascolarctobacterium | AGIs ↓ | ||
| Bilophila | SGLT2 ↓ | ||
| Hungatella | SGLT2 ↓ | ||
| Bifidobacterium l. | ACARBOSE ↑ | ||
| Enterococcus f. | AGIs ↑ | ||
| Ruminococci | SGLT2 ↑ | ||
| Roseburia | SGLT2 ↑ | VILDAGLIPTIN ↑ | |
| Eubacterium | SGLT2 ↑ | ||
| Escherichia-Shigella | SGLT2 ↓ | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mindrescu, N.M.; Guja, C.; Jinga, V.; Ispas, S.; Curici, A.; Nelson Twakor, A.; Pantea Stoian, A.M. Interactions between Gut Microbiota and Oral Antihyperglycemic Drugs: A Systematic Review. Int. J. Mol. Sci. 2024, 25, 3540. https://doi.org/10.3390/ijms25063540
Mindrescu NM, Guja C, Jinga V, Ispas S, Curici A, Nelson Twakor A, Pantea Stoian AM. Interactions between Gut Microbiota and Oral Antihyperglycemic Drugs: A Systematic Review. International Journal of Molecular Sciences. 2024; 25(6):3540. https://doi.org/10.3390/ijms25063540
Chicago/Turabian StyleMindrescu, Nicoleta Mihaela, Cristian Guja, Viorel Jinga, Sorina Ispas, Antoanela Curici, Andreea Nelson Twakor, and Anca Mihaela Pantea Stoian. 2024. "Interactions between Gut Microbiota and Oral Antihyperglycemic Drugs: A Systematic Review" International Journal of Molecular Sciences 25, no. 6: 3540. https://doi.org/10.3390/ijms25063540
APA StyleMindrescu, N. M., Guja, C., Jinga, V., Ispas, S., Curici, A., Nelson Twakor, A., & Pantea Stoian, A. M. (2024). Interactions between Gut Microbiota and Oral Antihyperglycemic Drugs: A Systematic Review. International Journal of Molecular Sciences, 25(6), 3540. https://doi.org/10.3390/ijms25063540