
Predicting Response to Immunotargeted Therapy in Endometrial Cancer via Tumor Immune Microenvironment: A Multicenter, Observational Study

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
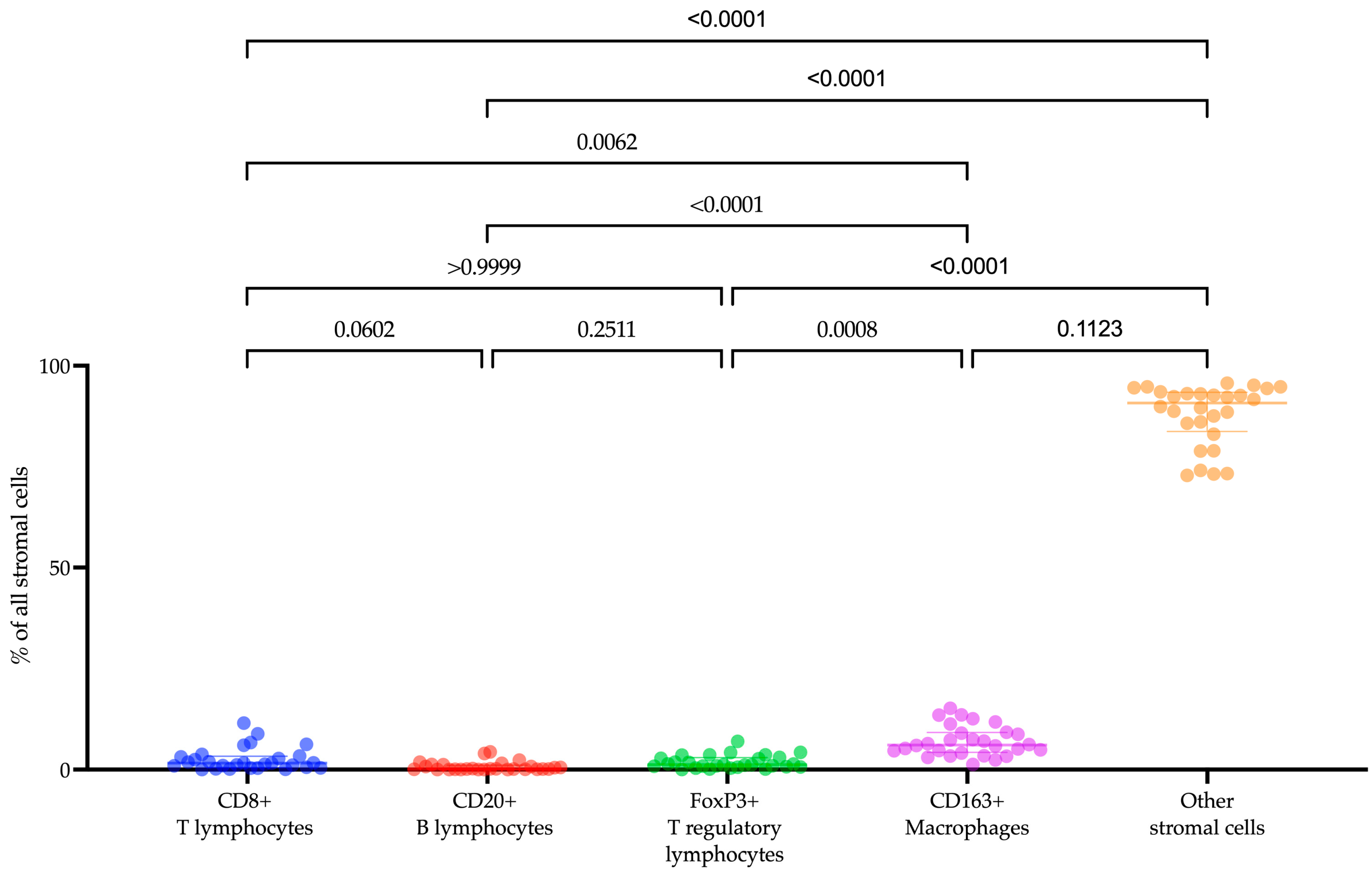
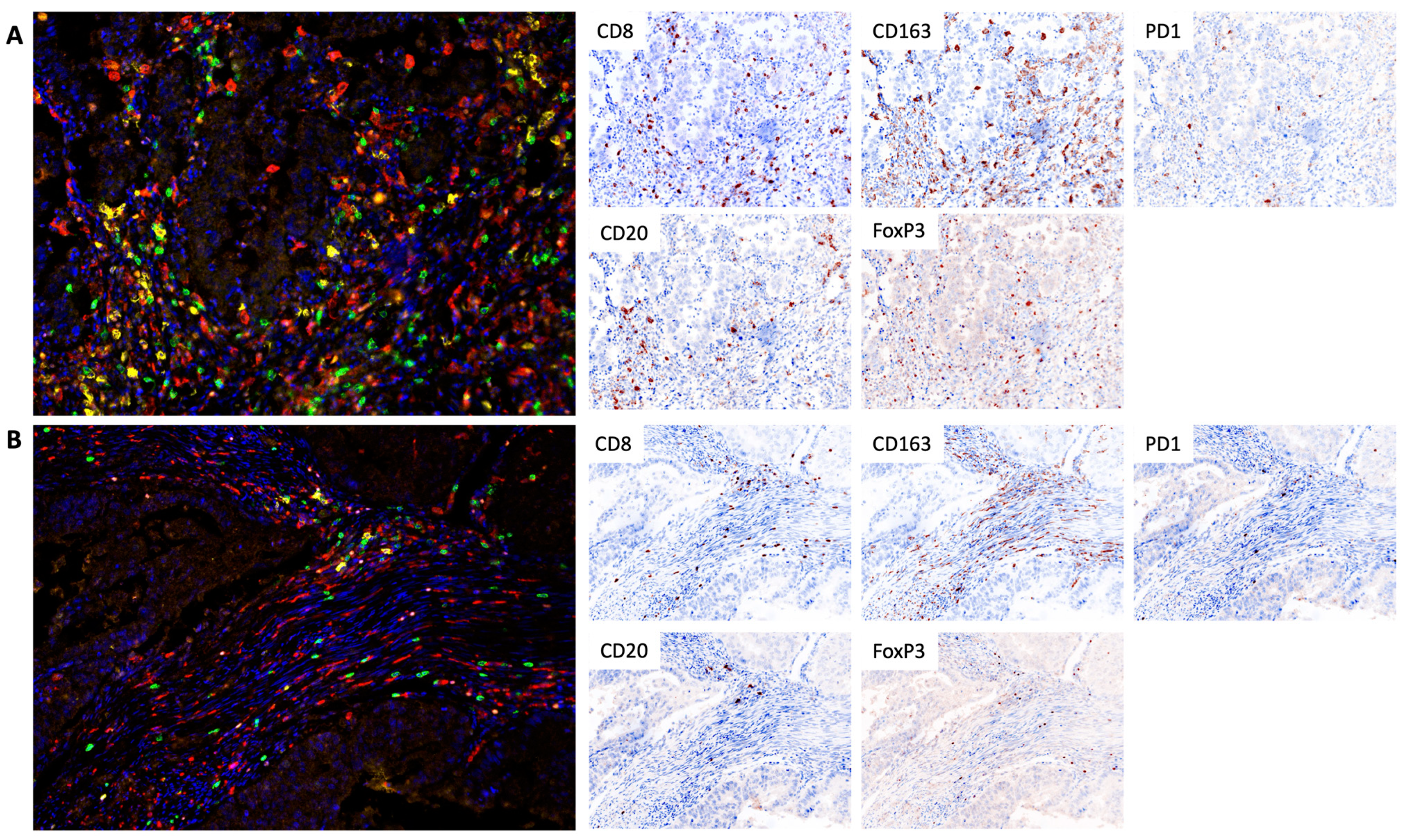
2.2. Immune Cells Composition of Tumor Microenvironment of Recurrent or Metastatic Endometrial Cancer
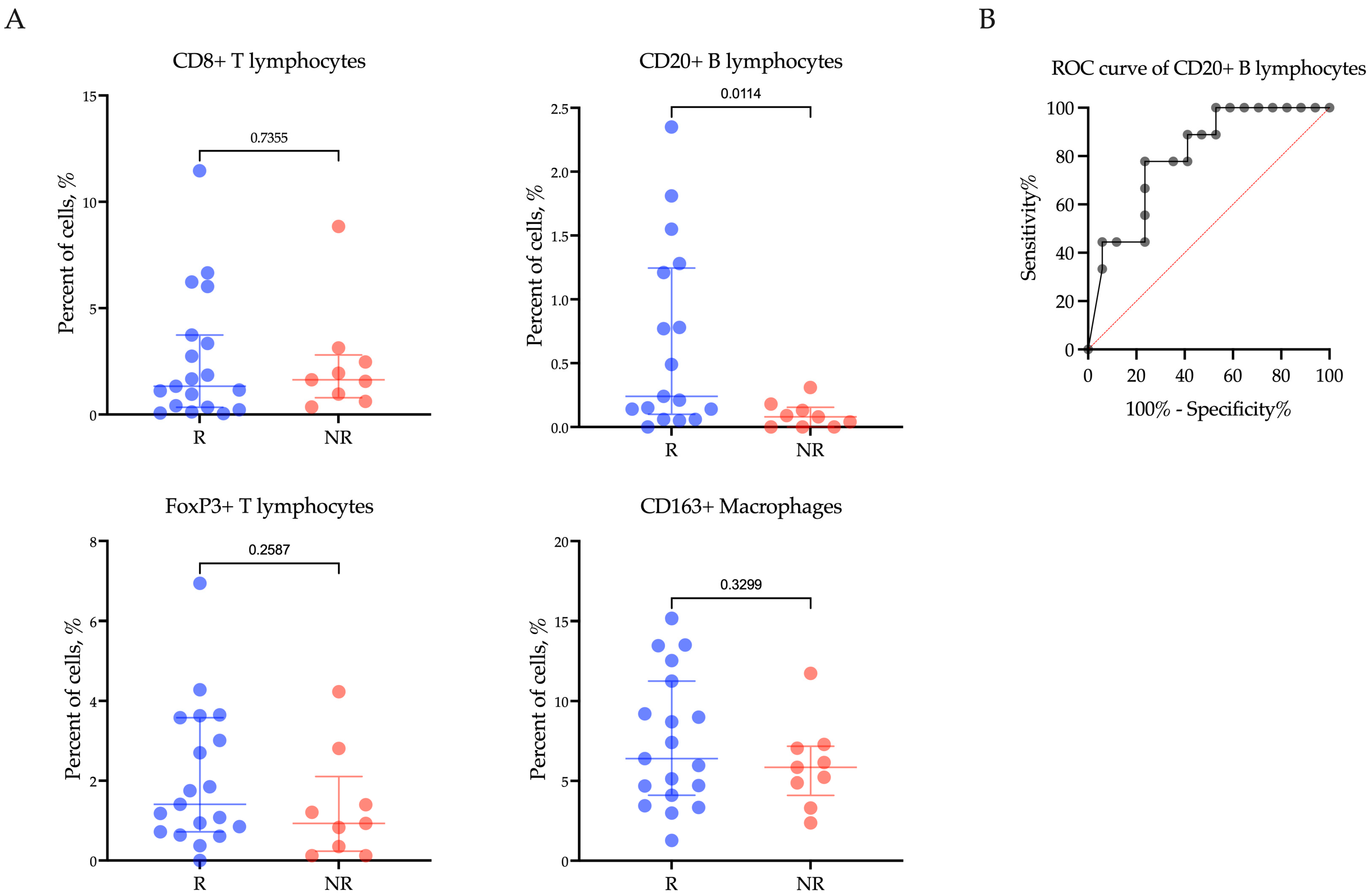
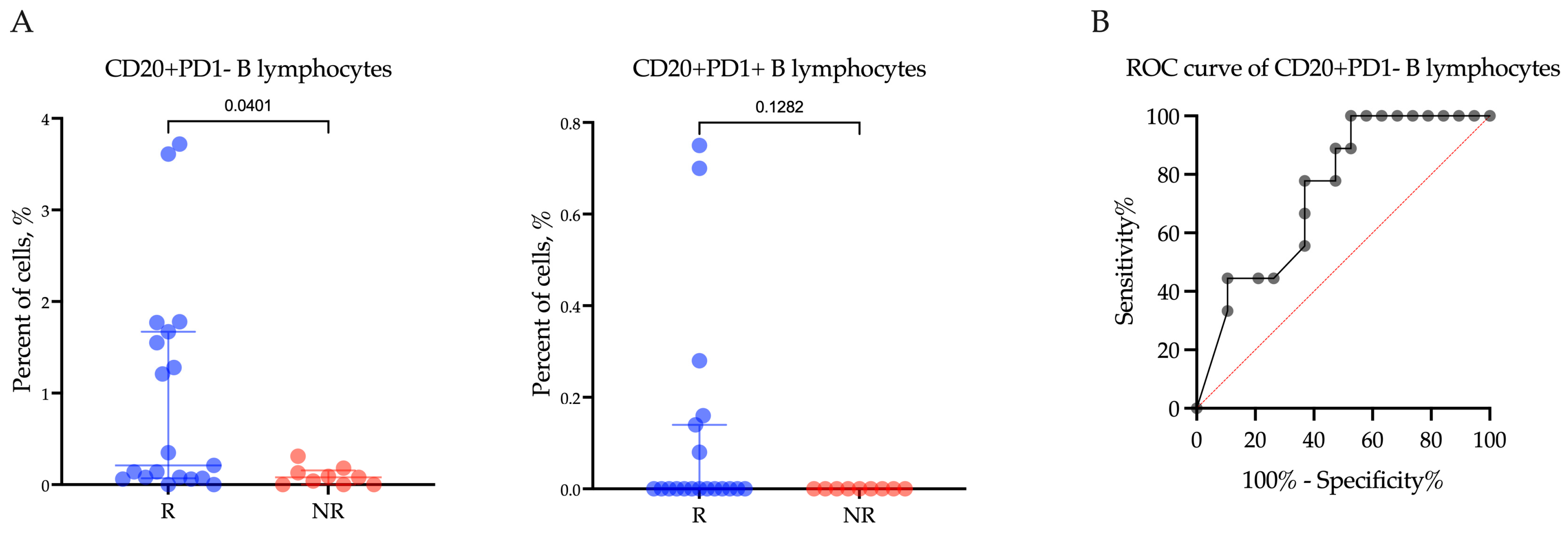
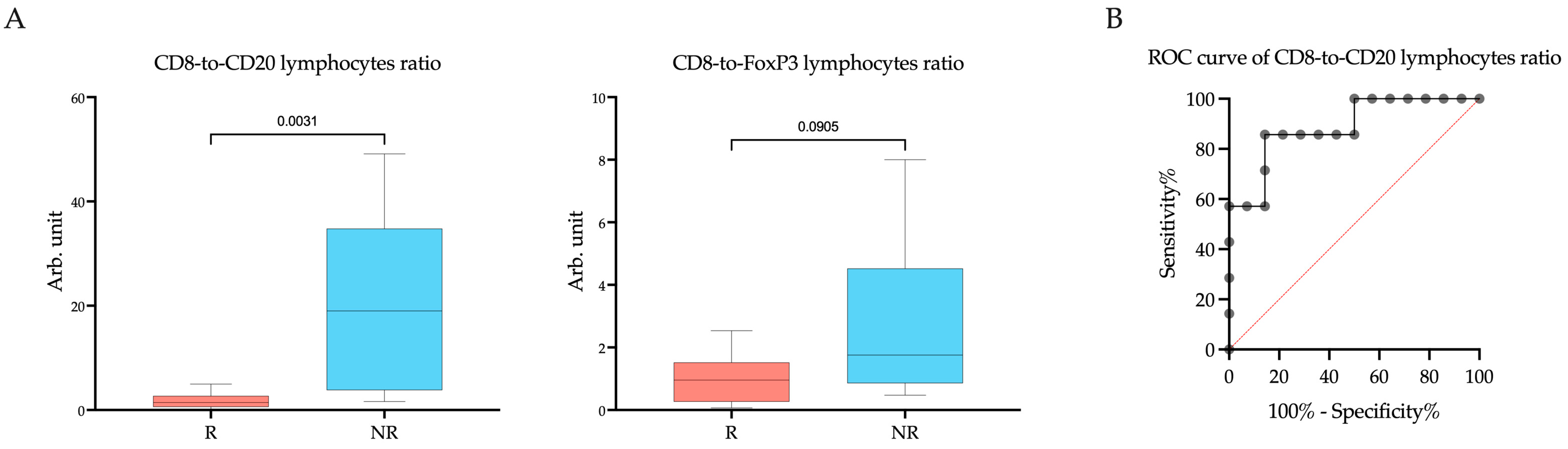
2.3. Levels of CD20+ B Lymphocytes and the CD8-to-CD20 Lymphocyte Ratio Are Associated with Response to Pembrolizumab plus Lenvatinib Treatment
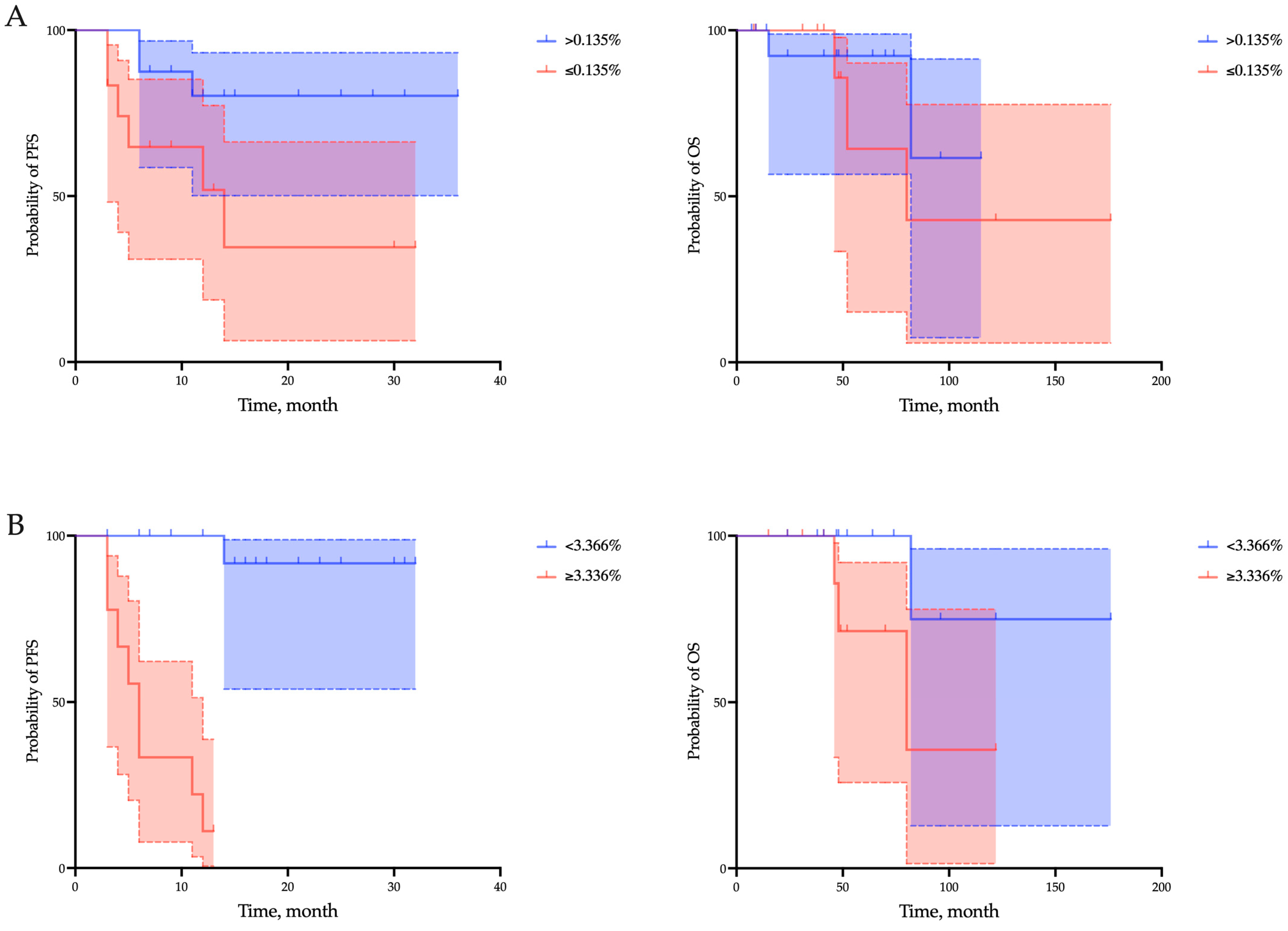
2.4. CD20+ B Lymphocytes and the CD8-to-CD20 Lymphocytes Ratio as Prognostic Factors of PFS, but Not OS, in (R/M) EC Patients
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. TSA-Associated Multiplex Immunofluorescence
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Oaknin, A.; Bosse, T.J.; Creutzberg, C.L.; Giornelli, G.; Harter, P.; Joly, F.; Lorusso, D.; Marth, C.; Marth, C.; Mirza, M.R.; et al. Endometrial cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol. 2022, 33, 860–877. [Google Scholar] [CrossRef] [PubMed]
- Marcus, L.; Lemery, S.J.; Keegan, P.; Pazdur, R. FDA Approval Summary: Pembrolizumab for the Treatment of Microsatellite Instability-High Solid Tumors. Clin. Cancer Res. 2019, 25, 3753–3758. [Google Scholar] [CrossRef] [PubMed]
- Green, A.K.; Feinberg, J.; Makker, V. A Review of Immune Checkpoint Blockade Therapy in Endometrial Cancer. Am. Soc. Clin. Oncol. Educ. Book 2020, 40, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Makker, V.; Colombo, N.; Casado Herráez, A.; Santin, A.D.; Colomba, E.; Miller, D.S.; Fujiwara, K.; Pignata, S.; Baron-Hay, S.; Ray-Coquard, I.; et al. Lenvatinib plus Pembrolizumab for Advanced Endometrial Cancer. N. Engl. J. Med. 2022, 386, 437–448. [Google Scholar] [CrossRef] [PubMed]
- Marth, C.; Tarnawski, R.; Tyulyandina, A.; Pignata, S.; Gilbert, L.; Kaen, D.; Rubio, M.J.; Frentzas, S.; Beiner, M.; Magallanes-Maciel, M.; et al. Phase 3, randomized, open-label study of pembrolizumab plus lenvatinib versus chemotherapy for first-line treatment of advanced or recurrent endometrial cancer: ENGOT-en9/LEAP-001. Int. J. Gynecol. Cancer 2022, 32, 93–100. [Google Scholar] [CrossRef]
- Maiorano, B.A.; Maiorano, M.F.P.; Cormio, G.; Maglione, A.; Lorusso, D.; Maiello, E. How Immunotherapy Modified the Therapeutic Scenario of Endometrial Cancer: A Systematic Review. Front. Oncol. 2022, 12, 844801. [Google Scholar] [CrossRef]
- Yamamoto, Y.; Matsui, J.; Matsushima, T.; Obaishi, H.; Miyazaki, K.; Nakamura, K.; Tohyama, O.; Semba, T.; Yamaguchi, A.; Hoshi, S.S.; et al. Lenvatinib, an angiogenesis inhibitor targeting VEGFR/FGFR, shows broad antitumor activity in human tumor xenograft models associated with microvessel density and pericyte coverage. Vasc. Cell 2014, 6, 18. [Google Scholar] [CrossRef] [PubMed]
- Kato, Y.; Tabata, K.; Kimura, T.; Yachie-Kinoshita, A.; Ozawa, Y.; Yamada, K.; Ito, J.; Tachino, S.; Hori, Y.; Matsuki, M.; et al. Lenvatinib plus anti-PD-1 antibody combination treatment activates CD8+ T cells through reduction of tumor-associated macrophage and activation of the interferon pathway. PLoS ONE 2019, 14, e0212513. [Google Scholar] [CrossRef]
- Kimura, T.; Kato, Y.; Ozawa, Y.; Kodama, K.; Ito, J.; Ichikawa, K.; Yamada, K.; Hori, Y.; Tabata, K.; Takase, K.; et al. Immunomodulatory activity of lenvatinib contributes to antitumor activity in the Hepa1-6 hepatocellular carcinoma model. Cancer Sci. 2018, 109, 3993–4002. [Google Scholar] [CrossRef]
- Yi, C.; Chen, L.; Lin, Z.; Liu, L.; Shao, W.; Zhang, R.; Lin, J.; Zhang, J.; Zhu, W.; Jia, H.; et al. Lenvatinib Targets FGF Receptor 4 to Enhance Antitumor Immune Response of Anti-Programmed Cell Death-1 in HCC. Hepatology 2021, 74, 2544–2560. [Google Scholar] [CrossRef] [PubMed]
- Delgado, A.; Guddati, A.K. Clinical endpoints in oncology—A primer. Am. J. Cancer Res. 2021, 11, 1121–1131. [Google Scholar] [PubMed]
- de Visser, K.E.; Korets, L.V.; Coussens, L.M. De novo carcinogenesis promoted by chronic inflammation is B lymphocyte dependent. Cancer Cell 2005, 7, 411–423. [Google Scholar] [CrossRef] [PubMed]
- Affara, N.I.; Ruffell, B.; Medler, T.R.; Gunderson, A.J.; Johansson, M.; Bornstein, S.; Bergsland, E.; Steinhoff, M.; Li, Y.; Gong, Q.; et al. B cells regulate macrophage phenotype and response to chemotherapy in squamous carcinomas. Cancer Cell 2014, 25, 809–821. [Google Scholar] [CrossRef]
- Riaz, N.; Havel, J.J.; Makarov, V.; Desrichard, A.; Urba, W.J.; Sims, J.S.; Hodi, F.S.; Martín-Algarra, S.; Mandal, R.; Sharfman, W.H.; et al. Tumor and Microenvironment Evolution during Immunotherapy with Nivolumab. Cell 2017, 171, 934–949.e16. [Google Scholar] [CrossRef] [PubMed]
- Willsmore, Z.N.; Coumbe, B.G.T.; Crescioli, S.; Reci, S.; Gupta, A.; Harris, R.J.; Chenoweth, A.; Chauhan, J.; Bax, H.J.; McCraw, A.; et al. Combined anti-PD-1 and anti-CTLA-4 checkpoint blockade: Treatment of melanoma and immune mechanisms of action. Eur. J. Immunol. 2021, 51, 544–556. [Google Scholar] [CrossRef]
- Shen, M.; O’Donnell, E.; Leon, G.; Kisovar, A.; Melo, P.; Zondervan, K.; Granne, I.; Southcombe, J. The role of endometrial B cells in normal endometrium and benign female reproductive pathologies: A systematic review. Hum. Reprod. Open 2021, 2022, hoab043. [Google Scholar] [CrossRef] [PubMed]
- Shen, M.; Child, T.; Mittal, M.; Sarodey, G.; Salim, R.; Granne, I.; Southcombe, J.H. B Cell Subset Analysis and Gene Expression Characterization in Mid-Luteal Endometrium. Front. Cell Dev. Biol. 2021, 9, 709280. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Zhou, J.; Xiao, Y.; Ming, J.; Zhou, J.; Dong, F.; Zhou, X.; Xu, Z.; Xu, Z.; Lei, P.; et al. CD20+CD22+ADAM28+ B Cells in Tertiary Lymphoid Structures Promote Immunotherapy Response. Front Immunol. 2022, 13, 865596. [Google Scholar] [CrossRef]
- Cowan, M.; Xie, P.; Chen, S.; Cardenas, H.; Kocherginsky, M.; Zhang, B.; Matei, D. Immune markers of response to pembrolizumab and guadecitabine in platinum resistant ovarian cancer utilizing multiplex immunohistochemistry (mIHC). Gynecol. Oncol. 2021, 162, S28–S29. [Google Scholar] [CrossRef]
- Sharonov, G.V.; Serebrovskaya, E.O.; Yuzhakova, D.V.; Britanova, O.V.; Chudakov, D.M. B cells, plasma cells and antibody repertoires in the tumour microenvironment. Nat. Rev. Immunol. 2020, 20, 294–307. [Google Scholar] [CrossRef] [PubMed]
- Lu, M.; Zhang, X.; Gao, X.; Sun, S.; Wei, X.; Hu, X.; Huang, C.; Xu, H.; Wang, B.; Zhang, W.; et al. Lenvatinib enhances T cell immunity and the efficacy of adoptive chimeric antigen receptor-modified T cells by decreasing myeloid-derived suppressor cells in cancer. Pharmacol. Res. 2021, 174, 105829. [Google Scholar] [CrossRef]
- Xu, W.; Joo, H.; Clayton, S.; Dullaers, M.; Herve, M.C.; Blankenship, D.; De La Morena, M.T.; Balderas, R.; Picard, C.; Casanova, J.L.; et al. Macrophages induce differentiation of plasma cells through CXCL10/IP-10. J. Exp. Med. 2012, 209, 1813–1823. [Google Scholar] [CrossRef] [PubMed]
- Horeweg, N.; Workel, H.H.; Loiero, D.; Church, D.N.; Vermij, L.; Léon-Castillo, A.; Krog, R.T.; de Boer, S.M.; Nout, R.A.; Powell, M.E.; et al. Tertiary lymphoid structures critical for prognosis in endometrial cancer patients. Nat. Commun. 2022, 13, 1373. [Google Scholar] [CrossRef] [PubMed]
- Zheng, W. Molecular Classification of Endometrial Cancer and the 2023 FIGO Staging: Exploring the Challenges and Opportunities for Pathologists. Cancers 2023, 15, 4101. [Google Scholar] [CrossRef]
- Levine, D.A.; The Cancer Genome Atlas Research Network. Integrated genomic characterization of endometrial carcinoma. Nature 2013, 497, 67–73. [Google Scholar] [CrossRef]
- Zhao, Z.; Zheng, B.; Zheng, J.; Zhang, Y.; Jiang, C.; Nie, C.; Jiang, X.; Yao, D.; Zhao, H. Integrative Analysis of Inflammatory Response-Related Gene for Predicting Prognosis and Immunotherapy in Glioma. J. Mol. Neurosci. 2023, 73, 608–627. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter, Abs. (%) | ||
|---|---|---|
| Age (years) | ||
| FIGO | IA | 3/28 (10.7) |
| IB | 5/28 (17.8) | |
| II | 7/28 (25.0) | |
| IIIA | 5/28 (17.8) | |
| IIIC | 3/28(10.7) | |
| IVB | 5/28 (17.8) | |
| Histological type | Endometrioid | 21/28 (75.0) |
| Papillary serous | 7/28 (25.0) | |
| Grade | I | 6/28 (21.4) |
| II | 11/28 (39.3) | |
| III | 8/28 (28.6) | |
| No data | 3/28 (10.7) | |
| Myometrium involvement | None | 1/28 (3.6) |
| <50% | 11/28 (39.3) | |
| >50% | 16/28 (57.1) | |
| Lymphovascular invasion (LVI) | No | 16/28 (57.1) |
| Yes | 12/28 (42.8) | |
| Metastasis | No | 7/28 (25.0) |
| Yes | 21/28 (75.0) | |
| Variables | Univariate Analysis | Bootstrap | |
|---|---|---|---|
| OR (95%CI) | p Value | Bias | |
| FIGO (I–II vs. III–IV) | 1.11 (0.57 to 3.67) | 0.29 | 0.02 |
| Histological type (Endometrioid vs. Papillary serous) | 1.66 (0.50 to 8.32) | 0.44 | 0.05 |
| Metastasis (Yes vs. No) | 0.96 (0.46 to 1.63) | 0.59 | 0.34 |
| Grade (1–2 vs. 3) | 1.97 (0.84 to 6.76) | 0.36 | 0.09 |
| Myometrial invasion (Yes vs. No) | 1.09 (0.05 to 1.38) | 0.93 | 0.42 |
| Lymphovascular invasion (Yes vs. No) | 1.55 (0.29 to 2.19) | 0.74 | 0.55 |
| Proportion of CD20+ (>0.135 vs. ≤0.135) | 2.56 (1.12 to 6.80) | 0.004 | 0.001 |
| CD8-to-CD20 lymphocytes ratio (<3.366 vs. ≥3.366) | 8.21 (2.76 to 23.10) | 0.0001 | 0.001 |
| Variables | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| HR (95%CI) | p Value | HR (95%CI) | p Value | |
| FIGO (I–II vs. III–IV) | 1.32 (0.64 to 15.23) | 0.45 | 1.27 (0.36 to 10.90) | 0.56 |
| Histological type (Endometrioid vs. Papillary serous) | 0.79 (0.45 to 1.73) | 0.78 | 1.08 (0.12 to 3.97) | 0.53 |
| Metastasis (Yes vs. No) | 1.45 (0.34 to 9.83) | 0.64 | 1.62 (0.33 to 17.25) | 0.57 |
| Grade (1–2 vs. 3) | 3.26 (0.84 to 13.41) | 0.08 | 4.94 (0.79 to 11.42) | 0.14 |
| Myometrial invasion (Yes vs. No) | 0.78 (0.21 to 3.18) | 0.72 | 0.47 (0.15 to 3.28) | 0.75 |
| Lymphovascular invasion (Yes vs. No) | 1.27 (0.31 to 4.84) | 0.71 | 0.61 (0.10 to 2.84) | 0.53 |
| Proportion of CD20+ (>0.135 vs. ≤0.135) | 4.01 (1.10 to 19.1) | 0.04 | 6.09 (1.31 to 63.12) | 0.03 |
| CD8-to-CD20 lymphocytes ratio (<3.366 vs. ≥3.366) | 26.84 (5.67 to 126.9) | 0.0001 | 17.82 (3.93 to 117.11) | 0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maltseva, A.; Kalinchuk, A.; Chernorubashkina, N.; Sisakyan, V.; Lots, I.; Gofman, A.; Anzhiganova, Y.; Martynova, E.; Zukov, R.; Aleksandrova, E.; et al. Predicting Response to Immunotargeted Therapy in Endometrial Cancer via Tumor Immune Microenvironment: A Multicenter, Observational Study. Int. J. Mol. Sci. 2024, 25, 3933. https://doi.org/10.3390/ijms25073933
Maltseva A, Kalinchuk A, Chernorubashkina N, Sisakyan V, Lots I, Gofman A, Anzhiganova Y, Martynova E, Zukov R, Aleksandrova E, et al. Predicting Response to Immunotargeted Therapy in Endometrial Cancer via Tumor Immune Microenvironment: A Multicenter, Observational Study. International Journal of Molecular Sciences. 2024; 25(7):3933. https://doi.org/10.3390/ijms25073933
Chicago/Turabian StyleMaltseva, Anastasia, Anna Kalinchuk, Nataliya Chernorubashkina, Virab Sisakyan, Igor Lots, Alina Gofman, Yulia Anzhiganova, Elizaveta Martynova, Ruslan Zukov, Elena Aleksandrova, and et al. 2024. "Predicting Response to Immunotargeted Therapy in Endometrial Cancer via Tumor Immune Microenvironment: A Multicenter, Observational Study" International Journal of Molecular Sciences 25, no. 7: 3933. https://doi.org/10.3390/ijms25073933
APA StyleMaltseva, A., Kalinchuk, A., Chernorubashkina, N., Sisakyan, V., Lots, I., Gofman, A., Anzhiganova, Y., Martynova, E., Zukov, R., Aleksandrova, E., Kolomiets, L., & Tashireva, L. (2024). Predicting Response to Immunotargeted Therapy in Endometrial Cancer via Tumor Immune Microenvironment: A Multicenter, Observational Study. International Journal of Molecular Sciences, 25(7), 3933. https://doi.org/10.3390/ijms25073933