
A Molecular Approach for Detecting Bacteria and Fungi in Healthcare Environment Aerosols: A Systematic Review

 ,
,  , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Focused Question
2.2. Protocol
2.3. Eligibility Criteria
- Studies that focused on aerosols in healthcare environments (dental clinics, rehabilitation centers, nursing centers, sanatoriums, different hospital areas);
- Presence of bacteria and fungi;
- Application of molecular methods to recognize the bacteria;
- In vivo studies;
- In vitro studies;
- Full-text articles;
- Studies in English.
- Aerosols not focused on aerosols in healthcare environments;
- Studies not including the presence of bacteria and fungi;
- Studies without molecular analysis;
- Non-English studies;
- Systematic review articles;
- Reviews;
- Meta-analysis.
2.4. Information Sources, Search Strategy, and Study Selection
2.5. Data Collection Process, Data Items
2.6. Risk of Bias in Individual Studies
2.7. Quality Assessment
2.8. Risk of Bias across Studies
3. Results
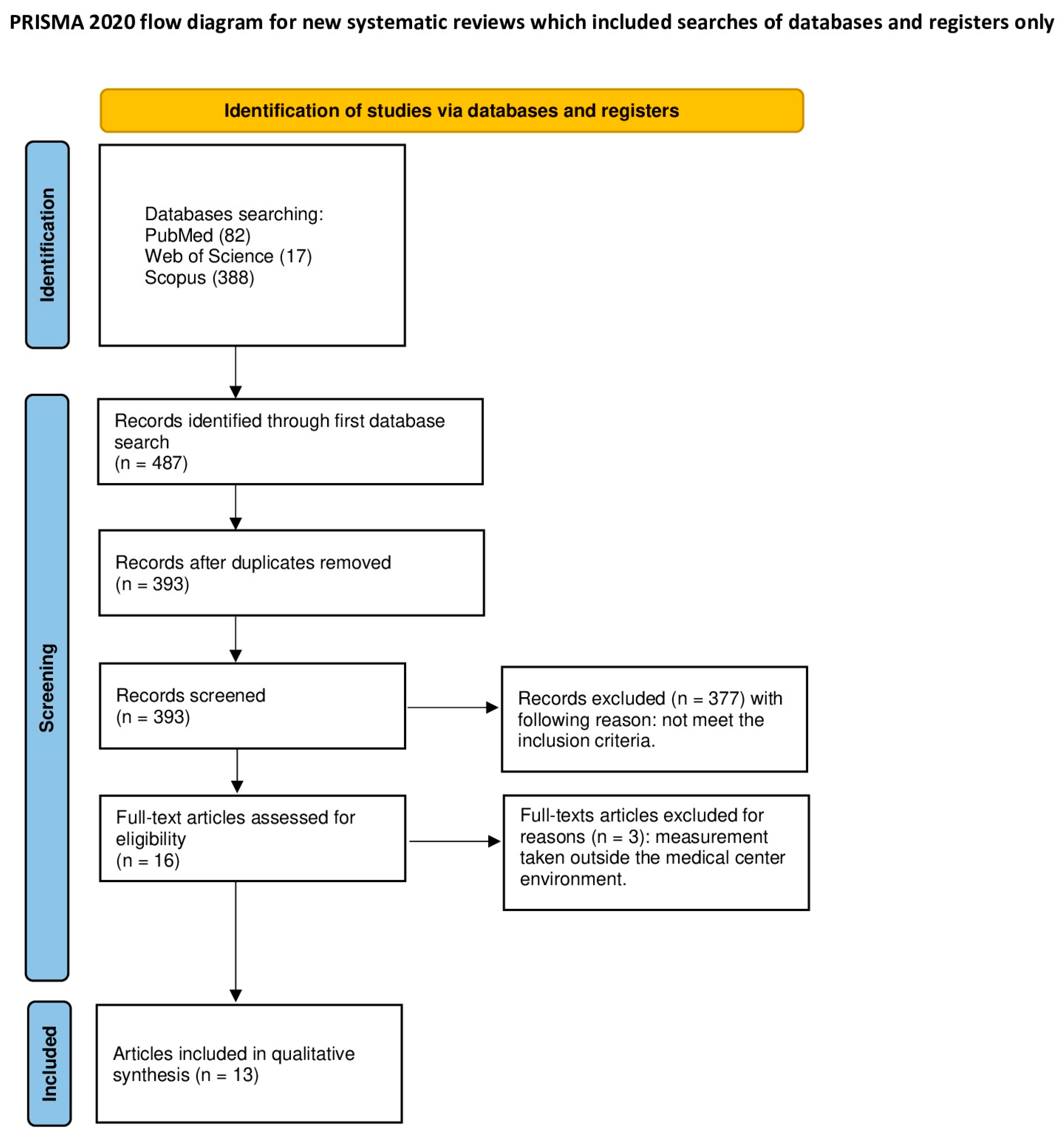
3.1. Study Selection
3.2. General Characteristics of the Included Studies
3.3. Main Study Outcomes
3.4. Quality Assessment of the Included Studies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jones, R.M.; Brosseau, L.M. Aerosol Transmission of Infectious Disease. J. Occup. Environ. Med. 2015, 57, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Pathak, B.; Khataniar, A.; Das, B.; Upadhyaya, S.; Medhi, A.; Bhuyan, P.K.; Buragohain, A.K.; Borah, D. Spatio-Temporal Diversity of Biological Aerosols over Northeast India: A Metagenomic Approach. Environ. Sci. Pollut. Res. 2022, 29, 64096–64111. [Google Scholar] [CrossRef] [PubMed]
- Angenent, L.T.; Kelley, S.T.; Amand, A.S.; Pace, N.R.; Hernandez, M.T. Molecular Identification of Potential Pathogens in Water and Air of a Hospital Therapy Pool. Proc. Natl. Acad. Sci. USA 2005, 29, 4860–4865. [Google Scholar] [CrossRef] [PubMed]
- Grydaki, N.; Colbeck, I.; Mendes, L.; Eleftheriadis, K.; Whitby, C. Bioaerosols in the Athens Metro: Metagenetic Insights into the PM10 Microbiome in a Naturally Ventilated Subway Station. Environ. Int. 2021, 146, 106186. [Google Scholar] [CrossRef] [PubMed]
- Matys, J.; Grzech-Leśniak, K. Dental Aerosol as a Hazard Risk for Dental Workers. Materials 2020, 13, 5109. [Google Scholar] [CrossRef] [PubMed]
- Grzech-Leśniak, K.; Matys, J. The Effect of Er:Yag Lasers on the Reduction of Aerosol Formation for Dental Workers. Materials 2021, 14, 2857. [Google Scholar] [CrossRef] [PubMed]
- Santarpia, J.L.; Rivera, D.N.; Herrera, V.L.; Morwitzer, M.J.; Creager, H.M.; Santarpia, G.W.; Crown, K.K.; Brett-Major, D.M.; Schnaubelt, E.R.; Broadhurst, M.J.; et al. Aerosol and Surface Contamination of SARS-CoV-2 Observed in Quarantine and Isolation Care. Sci. Rep. 2020, 10, 12732. [Google Scholar] [CrossRef] [PubMed]
- Austin, B. The Value of Cultures to Modern Microbiology. Antonie Leeuwenhoek Int. J. Gen. Mol. Microbiol. 2017, 110, 1247–1256. [Google Scholar] [CrossRef]
- Perkins, S.D.; Angenent, L.T. Potential Pathogenic Bacteria in Metalworking Fluids and Aerosols from a Machining Facility. FEMS Microbiol. Ecol. 2010, 74, 643–654. [Google Scholar] [CrossRef]
- Matys, J.; Gedrange, T.; Dominiak, M.; Grzech-Leśniak, K. Quantitative Evaluation of Aerosols Produced in the Dental Office during Caries Treatment: A Randomized Clinical Trial. J. Clin. Med. 2023, 12, 4597. [Google Scholar] [CrossRef]
- Lagier, J.C.; Edouard, S.; Pagnier, I.; Mediannikov, O.; Drancourt, M.; Raoult, D. Current and Past Strategies for Bacterial Culture in Clinical Microbiology. Clin. Microbiol. Rev. 2015, 28, 208–236. [Google Scholar] [CrossRef]
- Nammour, S.; El Mobadder, M.; Maalouf, E.; Namour, M.; Namour, A.; Rey, G.; Matamba, P.; Matys, J.; Zeinoun, T.; Grzech-Leśniak, K. Clinical Evaluation of Diode (980 Nm) Laser-Assisted Nonsurgical Periodontal Pocket Therapy: A Randomized Comparative Clinical Trial and Bacteriological Study. Photobiomodulation Photomed. Laser Surg. 2021, 39, 10–22. [Google Scholar] [CrossRef]
- Mbareche, H.; Brisebois, E.; Veillette, M.; Duchaine, C. Bioaerosol Sampling and Detection Methods Based on Molecular Approaches: No Pain No Gain. Sci. Total Environ. 2017, 599–600, 2095–2104. [Google Scholar] [CrossRef] [PubMed]
- Riley, L.W. Laboratory Methods in Molecular Epidemiology: Bacterial Infections. Microbiol. Spectr. 2018, 6, 10-1128. [Google Scholar] [CrossRef] [PubMed]
- Thornton, B.; Basu, C. Rapid and Simple Method of QPCR Primer Design. Methods Mol. Biol. 2015, 1275, 173–179. [Google Scholar] [CrossRef]
- Aly, S.M.; Sabri, D.M. Next Generation Sequencing (NGS): A Golden Tool in Forensic Toolkit. Arch. Med. Sądowej Kryminol. 2015, 65, 260–271. [Google Scholar] [CrossRef]
- Heid, C.A.; Stevens, J.; Livak, K.J.; Williams, P.M. Real Time Quantitative PCR. Genome Res. 1996, 6, 986–994. [Google Scholar] [CrossRef] [PubMed]
- Chrzanowska, N.M.; Kowalewski, J.; Lewandowska, M.A. Use of Fluorescence in Situ Hybridization (FISH) in Diagnosis and Tailored Therapies in Solid Tumors. Molecules 2020, 25, 1864. [Google Scholar] [CrossRef]
- Campos, R.; Borme, J.; Guerreiro, J.R.; Machado, G.; Cerqueira, M.F.; Petrovykh, D.Y.; Alpuim, P. Attomolar Label-Free Detection of Dna Hybridization with Electrolyte-Gated Graphene Field-Effect Transistors. ACS Sens. 2019, 4, 286–293. [Google Scholar] [CrossRef]
- Oueslati, A.; Hassen, W.; Ellafi, A.; Alibi, S.; Jaziri, A.; Bachkouel, S.; Oueslati, I.; Snoussi, M.; Adnan, M.; Patel, M.; et al. Assessment of Bacterial Diversity of Industrial Poultry Wastewater by Denaturing Gradient Gel Electrophoresis (DGGE) and the Cultivation Method in Order to Inform Its Reuse in Agriculture. BioMed Res. Int. 2022, 2022, 12. [Google Scholar] [CrossRef]
- Malhotra, S.; Sharma, S.; Bhatia, N.; Kumar, P.; Hans, C. Molecular Methods in Microbiology and Their Clinical Application. J. Mol. Genet. Med. 2014, 8. [Google Scholar] [CrossRef]
- Sleator, R.D.; Shortall, C.; Hill, C. Metagenomics. Lett. Appl. Microbiol. 2008, 47, 361–366. [Google Scholar] [CrossRef]
- Zhao, Y.; Chen, F.; Li, Q.; Wang, L.; Fan, C. Isothermal Amplification of Nucleic Acids. Chem. Rev. 2015, 115, 12491–12545. [Google Scholar] [CrossRef] [PubMed]
- Bumgarner, R. Overview of DNA microarrays: Types, applications, and their future. Curr. Protoc. Mol. Biol. 2013, 101, 22.1.1–22.1.11. [Google Scholar] [CrossRef] [PubMed]
- Tamminga, G.G.; Jansen, G.J.; Wiersma, M. Evaluation of a Fluorescence in Situ Hybridization (FISH)-Based Method for Detection of SARS-CoV-2 in Saliva. PLoS ONE 2022, 17, e0277367. [Google Scholar] [CrossRef]
- Yousefzadeh, A.; Maleki, A.; Athar, S.D.; Darvishi, E.; Ahmadi, M.; Mohammadi, E.; Tang, V.T.; Kalmarzi, R.N.; Kashefi, H. Evaluation of bio-aerosols type, density, and modeling of dispersion in inside and outside of different wards of educational hospital. Environ. Sci. Pollut. Res. 2022, 29, 14143–14157. [Google Scholar] [CrossRef]
- Johnson, J.S.; Spakowicz, D.J.; Hong, B.Y.; Petersen, L.M.; Demkowicz, P.; Chen, L.; Leopold, S.R.; Hanson, B.M.; Agresta, H.O.; Gerstein, M.; et al. Evaluation of 16S RRNA Gene Sequencing for Species and Strain-Level Microbiome Analysis. Nat. Commun. 2019, 10, 5029. [Google Scholar] [CrossRef] [PubMed]
- Núñez, A.; de Paz, G.A.; Rastrojo, A.; García, A.M.; Alcamí, A.; Montserrat Gutiérrez-Bustillo, A.; Moreno, D.A. Monitoring of Airborne Biological Particles in Outdoor Atmosphere. Part 2: Metagenomics Applied to Urban Environments. Int. Microbiol. 2016, 19, 69–80. [Google Scholar] [CrossRef]
- Soroka, M.; Wasowicz, B.; Rymaszewska, A. Loop-Mediated Isothermal Amplification (Lamp): The Better Sibling of PCR? Cells 2021, 10, 1931. [Google Scholar] [CrossRef]
- Cordero, F.; Botta, M.; Calogero, R.A. Microarray Data Analysis and Mining Approaches. Brief. Funct. Genom. Proteom. 2007, 6, 265–281. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 Explanation and Elaboration: Updated Guidance and Exemplars for Reporting Systematic Reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef] [PubMed]
- Watson, P.F.; Petrie, A. Method Agreement Analysis: A Review of Correct Methodology. Theriogenology 2010, 73, 1167–1179. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J. Cochrane Handbook for Systematic Reviews of Interventions; Cochrane Training; Cochrane: London, UK, 2021. [Google Scholar]
- Núñez, A.; García, A.M. The aerobiome in a hospital environment: Characterization, seasonal tendencies and the effect of window opening ventilation. Build. Environ. 2023, 230, 110024. [Google Scholar] [CrossRef]
- Nimra, A.; Ali, Z.; Sultan, S.; Nasir, Z.A.; Sidra, S.; Hussain, A. Molecular sequencing and phylogenetic analysis of bioaerosols in hospital wards with different ventilation conditions. J. Infect. Dev. Ctries. 2022, 16, 157–165. [Google Scholar] [CrossRef] [PubMed]
- Wu, B.; Qi, C.; Wang, L.; Yang, W.; Zhou, D.; Wang, M.; Dong, Y.; Weng, H.; Li, C.; Hou, X.; et al. Detection of Microbial Aerosols in Hospital Wards and Molecular Identification and Dissemination of Drug Resistance of Escherichia coli. Environ. Int. 2020, 137, 105479. [Google Scholar] [CrossRef] [PubMed]
- Handorean, A.; Robertson, C.E.; Harris, J.K.; Frank, D.; Hull, N.; Kotter, C.; Stevens, M.J.; Baumgardner, D.; Pace, N.R.; Hernandez, M. Microbial Aerosol Liberation from Soiled Textiles Isolated during Routine Residuals Handling in a Modern Health Care Setting. Microbiome 2015, 3, 72. [Google Scholar] [CrossRef] [PubMed]
- Habibi, N.; Uddin, S.; Behbehani, M.; Al Salameen, F.; Razzack, N.A.; Zakir, F.; Shajan, A.; Alam, F. Bacterial and fungal communities in indoor aerosols from two Kuwaiti hospitals. Front. Microbiol. 2022, 13, 955913. [Google Scholar] [CrossRef]
- Perkins, S.D.; Mayfield, J.; Fraser, V.; Angenent, L.T. Potentially Pathogenic Bacteria in Shower Water and Air of a Stem Cell Transplant Unit. Appl. Environ. Microbiol. 2009, 75, 5363–5372. [Google Scholar] [CrossRef] [PubMed]
- Montagna, M.T.; Cristina, M.L.; De Giglio, O.; Spagnolo, A.M.; Napoli, C.; Cannova, L.; Deriu, M.G.; Delia, S.A.; Giuliano, A.; Guida, M.; et al. Serological and molecular identification of Legionella spp. in water and surrounding air samples in Italian healthcare facilities. Environ. Res. 2016, 146, 47–50. [Google Scholar] [CrossRef]
- Jiang, X.; Liu, Y.; Liu, Q.; Jing, W.; Qin, K.; Sui, G. Rapid Capture and Analysis of Airborne Staphylococcus aureus in the Hospital Using a Microfluidic Chip. Micromachines 2016, 7, 169. [Google Scholar] [CrossRef]
- Chen, P.-S.; Lin, C.K.; Tsai, F.T.; Yang, C.-Y.; Lee, C.-H.; Liao, Y.-S.; Yeh, C.-Y.; King, C.-C.; Wu, J.-L.; Wang, Y.-C.; et al. Quantification of Airborne Influenza and Avian Influenza Virus in a Wet Poultry Market using a Filter/Real-time qPCR Method. Aerosol Sci. Technol. 2009, 43, 290–297. [Google Scholar] [CrossRef]
- Gilbert, Y.; Veillette, M.; Duchaine, C. Airborne bacteria and antibiotic resistance genes in hospital rooms. Aerobiologia 2010, 26, 185–194. [Google Scholar] [CrossRef]
- Retamal-Valdes, B.; Soares, G.M.; Stewart, B.; Figueiredo, L.C.; Faveri, M.; Miller, S.; Zhang, Y.P.; Feres, M. Effectiveness of a Pre-Procedural Mouthwash in Reducing Bacteria in Dental Aerosols: Randomized Clinical Trial. Braz. Oral Res. 2017, 31, e21. [Google Scholar] [CrossRef] [PubMed]
- Clarridge, J.E. Impact of 16S RRNA Gene Sequence Analysis for Identification of Bacteria on Clinical Microbiology and Infectious Diseases. Clin. Microbiol. Rev. 2004, 17, 840–862. [Google Scholar] [CrossRef]
- Başpınar, E.Ö.; Dayan, S.; Bekçibaşı, M.; Tekin, R.; Ayaz, C.; Deveci, Ö.; Hoşoğlu, S. Comparison of Culture and PCR Methods in the Diagnosis of Bacterial Meningitis. Braz. J. Microbiol. 2017, 48, 232–236. [Google Scholar] [CrossRef]
- Ku, D.N.; Ku, S.K.; Helfman, B.; McCarty, N.A.; Wolff, B.J.; Winchell, J.M.; Anderson, L.J. Ability of Device to Collect Bacteria from Cough Aerosols Generated by Adults with Cystic Fibrosis [Version 1; Referees: 2 Approved]. F1000Research 2016, 5, 1920. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, M.; Ramsheh, M.Y.; Williams, C.M.L.; Auty, J.; Haldar, K.; Abdulwhhab, M.; Brightling, C.E.; Barer, M.R. Face Mask Sampling Reveals Antimicrobial Resistance Genes in Exhaled Aerosols from Patients with Chronic Obstructive Pulmonary Disease and Healthy Volunteers. BMJ Open Respir. Res. 2018, 5, e000321. [Google Scholar] [CrossRef]
- Shu, Q.; Rajagopal, M.; Fan, J.; Zhan, L.; Kong, X.; He, Y.; Rotcheewaphan, S.; Lyon, C.J.; Sha, W.; Zelazny, A.M.; et al. Peptidomic analysis of mycobacterial secreted proteins enables species identification. View 2022, 3, 20210019. [Google Scholar] [CrossRef]
- Innes, N.; Johnson, I.G.; Al-Yaseen, W.; Harris, R.; Jones, R.; KC, S.; McGregor, S.; Robertson, M.; Wade, W.G.; Gallagher, J.E. A Systematic Review of Droplet and Aerosol Generation in Dentistry. J. Dent. 2021, 105, 103556. [Google Scholar] [CrossRef]
- Lahdentausta, L.; Sanmark, E.; Lauretsalo, S.; Korkee, V.; Nyman, S.; Atanasova, N.; Oksanen, L.; Zhao, J.; Hussein, T.; Hyvärinen, A.; et al. Aerosol Concentrations and Size Distributions during Clinical Dental Procedures. Heliyon 2022, 8, e11074. [Google Scholar] [CrossRef]
- Stockwell, R.E.; Chin, M.; Johnson, G.R.; Wood, M.E.; Sherrard, L.J.; Ballard, E.; O’Rourke, P.; Ramsay, K.A.; Kidd, T.J.; Jabbour, N.; et al. Transmission of Bacteria in Bronchiectasis and Chronic Obstructive Pulmonary Disease: Low Burden of Cough Aerosols. Respirology 2019, 24, 980–987. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Guo, G.; Wang, H.; Yang, X.; Shao, F.; Yang, C.; Gao, W.; Shao, Z.; Zhang, J.; Luo, J.; et al. Comparative study of bacteriological culture and real-time fluorescence quantitative PCR (RT-PCR) and multiplex PCR-based reverse line blot (mPCR/RLB) hybridization assay in the diagnosis of bacterial neonatal meningitis. BMC Pediatr. 2014, 14, 224. [Google Scholar] [CrossRef] [PubMed]
- Pandya, S.; Ravi, K.; Srinivas, V.; Jadhav, S.; Khan, A.; Arun, A.; Riley, L.W.; Madhivanan, P. Comparison of culture-dependent and culture-independent molecular methods for characterization of vaginal microflora. J Med. Microbiol. 2017, 66, 149–153. [Google Scholar] [CrossRef] [PubMed]
- Das, S.; Dash, H.R.; Mangwani, N.; Chakraborty, J.; Kumari, S. Understanding molecular identification and polyphasic taxonomic approaches for genetic relatedness and phylogenetic relationships of microorganisms. J. Microbiol. Methods 2014, 103, 80–100. [Google Scholar] [CrossRef] [PubMed]
- López-Pérez, M.; Aguirre-Garrido, F.; Herrera-Zúñiga, L.; Fernández, F.J. Gene as a Dynamical Notion: An Extensive and Integrative Vision. Redefining the Gene Concept, from Traditional to Genic-Interaction, as a New Dynamical Version. BioSystems 2023, 234, 105060. [Google Scholar] [CrossRef] [PubMed]
- Antunes, L.C.S.; Imperi, F.; Carattoli, A.; Visca, P. Deciphering the Multifactorial Nature of Acinetobacter Baumannii Pathogenicity. PLoS ONE 2011, 6, e22674. [Google Scholar] [CrossRef] [PubMed]
- Xie, M.; Fussenegger, M. Designing Cell Function: Assembly of Synthetic Gene Circuits for Cell Biology Applications. Nat. Rev. Mol. Cell Biol. 2018, 19, 507–525. [Google Scholar] [CrossRef] [PubMed]
- Martínez, J.L.; Baquero, F. Interactions among Strategies Associated with Bacterial Infection: Pathogenicity, Epidemicity, and Antibiotic Resistance. Clin. Microbiol. Rev. 2002, 15, 647–679. [Google Scholar] [CrossRef]
- Kurkela, S.; Brown, D.W.G. Molecular diagnostic techniques. Medicine 2009, 37, 535–540. [Google Scholar] [CrossRef]
- Ari, Ş.; Arikan, M. Next-generation sequencing: Advantages, disadvantages, and future. In Plant Omics: Trends and Applications; Springer: Berlin/Heidelberg, Germany, 2016; pp. 109–135. [Google Scholar]


{kind=link}
| Study | Aim of the Study | Material and Methods | Results | Conclusions |
|---|---|---|---|---|
| Yousefzadeh A. et al. [26] | To establish the concentration and identify bacteria and fungi in bioaerosol present in indoor and outdoor air of a hospital | The air samples were taken from 10 different hospital wards using an Andersen one-stage sampler. Samples were taken from outside the hospital as well. Then, the aerosol was subjected to further culture identification, evaluation of antibiotic resistance, and PCR identification. | The study resulted in the identification of 14 bacterial and 12 fungi species. lowest concentrations of bacteria load were found in the operating room and the highest in the internal men’s ward. The biggest number of fungal species was found in the lung ward. Staphylococcus hemolyticus and Penicillium were the most abundant. S. hemolyticus showed resistance to five types of antibiotics. | The air quality in some wards exceeded the WHO standards despite good ventilation systems. |
| Núñez, A. et al. [34] | Comparison of hospital indoor and outdoor aerosols at two different seasons to evaluate the influence of the urban atmosphere, determine the presence of pathogens, and to evaluate the effectiveness of ventilation. | A total of 45 samples were collected in summer and wintertime from indoors and outdoors of the hospital. The samples were taken using the Petri dishes and then subjected to DNA extraction and sequencing- targeting the bacterial and fungal DNA. | The results showed a striking microbial variability associated with the year season. In summer, the predominant bacterial and fungal taxa were Proteobacteria and Ascomycota, while in winter, Basidiomycota showed the highest abundance. Opening the window to ventilate the room showed minor variations in air composition. | The indoor air is highly influenced by outdoor conditions. Changes in bacterial composition depending on the season |
| Nimra, A et al. [35] | To explore microbial diversity in differentially ventilated orthopedic wards (OW) and emergency rooms (OER) via the application of molecular techniques and biochemical testing. | The samples were taken from two different hospitals- one with central air conditioning (group I) and the other with non-central air conditioning (group II). Both the indoor and outdoor air was sampled. The samples were subjected to culture identification and quantification and phylogenic analysis involving 16S rRNA sequencing. | The molecular analysis observed the most abundant species, such as B. cereus, B. subtilis, C. perfringens, E. coli, K. pneumoniae, S. aureus and M. luteus. The indoor bacteria load was lower in the case of hospitals with central air-conditioning. The fungal analysis showed A.flavus and A. niger as the most abundant species in both OW, Penicillium, and A. niger in OER in group I and A. flavusand A. niger in group II. | Effective air circulation is crucial for maintaining air cleanliness in healthcare facilities. Moreover, molecular testing allowed for the detection of specific bacterial strains. In the case of bacterial strains, identification based on culture alone was sufficient to identify the most common strains. |
| Wu B et al. [36] | The aim of the study was to examine the load of E. coli in the air located in different parts of the hospital ward and to check its genetic similarity in terms of antibiotic resistance. | Samples from different ward environments were collected using Andersen-6 impact type and RCS centrifugal air microbial samplers. Air samples were also taken from the corridor 5 and 10 m far from the ward. Collected bacteria were cultured on media and subjected to PFGE testing. The PCR method was employed to examine antibiotic-resistance genes, specifically TEM, SHV, and CTX-M. | The concentration of airborne aerobic bacteria varied between each ward. E. coli was present in each ward and showed the highest concentration in ward A. The results showed a presence of E. coli also in spaces outside the ward. The tests allowed us to determine the antibiotic resistance of the strain found in each ward and after. | This study allowed us to isolate and identify the E. coli strains in different parts of the hospital. The study also assesses the antimicrobial resistance profiles. Molecular PFGE showed that E. coli can be spread through the air into parts outside of the ward possessing a potential threat to the health of patients. |
| Handorean A et al. [37] | Examination of airborne bacteria contained in the air in hospital textile storage rooms during the period between its storage and removal for laundry. | The aerosol was collected from different textile rooms, filtered by special filters, and subjected to PCR testing. | The research did not show any differences in the composition of the air when bed linen was delivered and taken away. The PCR technique allowed us to distinguish the bacteria found in the samples. | Handling hospital textiles may expose health workers to infections. |
| Habibi, N. et al. [38] | The aim of this study was to investigate indoor aerosols in two hospitals and to identify bacterial and fungal identification. | The samples were collected from two hospitals involved in COVID-19 treatment and from non-hospitalized settings. The samples were then subjected to 16S rDNA and ITS sequencing and PCR amplification. | The molecular investigation allowed us to determine the exact taxonomic composition of both bacterial and fungal communities. The bacteria composition differed between hospitals and non-hospital facilities while the fungal community was more homogenous. | The molecular methods were effective in the identification of bacterial species present in examined facilities. |
| Angenent LT et al. [3] | General molecular analysis of bioaerosol in public pools and public health facilities. | Samples of the pool air, the air just above the pool, pool water and the air from the outside of the pool building were collected. Then, they were subjected to colony and microscopy count. Later, the DNA sequencing was conducted (PCR). | Regardless of the sample, bacterial counts were significantly higher than in routine samples. Moreover, you managed to determine the phylogenetic origin of the bacteria contained in the samples. A high percentage of bacteria turned out to be M. avium clones. | The results of the study confirm the transmission of bacteria, which means the transmission of diseases. Furthermore, the protocols responsible for removing potential pathogens are clearly inadequate. |
| Perkins SD et al. [39] | To investigate if shower stalls in a stem cell transplant unit in a hospital can be a source of pathogens by analyzing the bacterial load, colony count, and bacterial DNA. | Samples were collected from the shower stall in a hospital with a stem cell transplant unit. Samples were collected for 6 days from the shower stall with and without membrane-integrated showerheads prior to turning on the shower, and then shower aerosol samples were collected from the same location as the water was running. Lastly, one liter of shower water was collected. Then, the samples were subjected to quantitative and molecular (PCR) analysis. | There were more pathogenic bacteria detected in collected water than in shower aerosol samples. Most notable was the presence of M. mucogenicum in water and P. aeruginosa in aerosol samples. However, in the samples collected from the shower stall where the membrane-integrated showerhead was installed, a reduced number of bacteria was observed. | Using membrane-integrated showerheads in shower stalls in a stem cell transplant unit can help to reduce the microbial load in water and surrounding aerosol, which can prevent infections in patient populations. |
| Montagna, M.T et al. [40] | To compare the Legionella pneumophila serogroups present in water and air samples collected from 10 healthcare facilities. | The hot water from the tap was sampled as well as the air from around the tap. Colonies classified as Legionella were subjected to a latex agglutination test with polyvalent antisera. Then, a molecular analysis was conducted on 17 strains. | The most prevalent Lgn serogroup was serogroup 6, followed by 9, 1, 7, and 12. In water samples, only Lgn serogroup 6 was detected. | The study does not show a correlation between water and surrounding air contamination. However, it shows the significance of serotyping, enabling a more precise evaluation of the dissemination of Legionella serogroups in the environment. |
| Jiang, X et el. [41] | The use of microfluidic chip for the rapid detection of Staphylococcus aureus. | An S. aureus culture was diluted to different concentrations of bioaerosol and then captured by a specially fabricated microchip. A clinical airborne sample was also collected from six different settings of a hospital, including surgery rooms, ICU, surgical wards, outpatients’ service hall and doctor’s office. The samples were then subjected to a LAMP reaction. | Fluorescent detection was used to evaluate the concentrations of S. aureus. The in vitro samples showed high fluorescence when many bacterial cells were present. Fluorescence decreased as the number of cells in the sample decreased. In the case of clinical samples, the fluorescence was very low, which means that S. aureus concentrations did not exceed the detection limit. | The presented technique is a promising method that can be applied in disease control due to significant time savings compared to other methods. |
| Chen, P.-S et al. [42] | The use of RT-PCR to assess the concentration profiles of airborne M. tuberculosis in a hospital, encompassing both patient-related and non-patient-related areas. | In total, 24 samples were taken from non-tuberculosis areas and 34 from tuberculosis areas. The DNA was extracted from the samples, and M. tuberculosis was detected using RT-qPCR. | The TB area M. tuberculosis concentrations were significantly higher than in non-TB areas. The highest airborne M. tuberculosis was detected in waiting and consulting rooms, emergency departments and medical wards. | The study emphasizes the significance of identifying high-risk areas and implementing tuberculosis control strategies to protect healthcare workers and patients within hospital environments. |
| Gilbert, Y et al. [43] | Analysis of bacterial diversity in a newly occupied hospital and assessment of whether sinks may be a potential reservoir of bioaerosols and a reservoir of opportunistic bacteria and antibiotic-resistant genes | The sink biofilm samples and air samples were taken from empty patients’ rooms. Extra cubic meters of air were collected to assess the presence of antibiotic-resistance genes. The tap water was also sampled. The collected material was subjected to molecular identification using 16S rRNA amplification and PCR. The biodiversity was analyzed using DGGE. | The results showed slightly higher concentrations of airborne microorganisms in patients’ rooms than in control rooms. The predominant bacteria species were S. epidermidis, S. hominis, Bacillus sp., and M. luteus. The most prevalent fungal species were Cladosporium sp. and Penicillium sp. The molecular methods showed the presence of many antibiotic-resistance genes. | Actions should be taken to minimize the presence of opportunistic pathogens in the air and water to avoid potential infections of patients present on the hospital premises. |
| Retamal-Valdes B et al. [44] | To evaluate the effect of a pre-procedural mouthwash containing sodium fluoride (F), zinc lactate (Zn), or cetylpyridinium chloride (CPC). | Three plates were placed on a support board attached to the reflector, on the bracket tray, and on the office bench to test the dental office environment. Four groups of 15 people were invited to the study. The first group rinsed the mouth with the mixture of CPC+Zn+F, the second group rinsed with water, the third group with chlorhexidine, and the fourth group did not rinse the mouth. Then, each patient was seated on the chair, and three new plates were placed on the support board, on the patient’s chest, and on the dentist’s forehead. The dentist processes the full-mouth dental prophylaxis. Then, the plates were incubated and analyzed using DNA hybridization. | No bacteria growth was detected on the plates located in the office before the procedure. The bacterial count was significantly lower in patients from group number 1 than group number 2, 3, or 4. When all locations were considered together, the results showed that the number of bacteria in the case of CPC+Zn+F or chlorhexidine rinse was lower than in patients who rinsed only with water or did not rinse at all. The DNA-DNA hybridization showed the presence of 40 subgingival species. | The mouthwash containing CPC+Zn+F was an effective way to reduce bacterial species present in oral aerosols during prophylaxis using ultrasonic instruments. |
| Authors | Aerosol Collection Method | Place of Aerosol Collection | Microbiological Culture Method | Molecular Method | Results (Microbiological Culture) | Results (Molecular Analysis) |
|---|---|---|---|---|---|---|
| Yousefzadeh A et al. [26] | -Andersen one-stage sampler -Bacteria collecting time: 20 min -Fungi collecting time: 5 min | -Inside the hospital (men’s ward, women’s ward, lung, neurology, infectious and burns wards, ICU, operating and emergency room) -Outside the hospital | -Collected samples were incubated for ~48 h in 35–37 °C -Biochemical tests for microscopic and morphologic examination -The Kirby–Bauer disk diffusion method for antibiotic resistance evaluation | -DNA extraction by phenol–chloroform method -PCR method (16S rRNA amplification) | -Bacteria: the emergency room showed the highest concentrations; bacteria concentrations depended on many factors like bed number or ventilation; the most abundant species: Staphylococcus hemolyticus -Fungi: the highest concentration was detected on the long ward, the lowest in the operating room; the most abundant species Penicillium and cranosporium and yeasts and scopolariopsis | -Performed on two samples that showed the highest abundance and resistance -Sample one: resistance to ciprofloxacin, gentamicin, azithromycin, amoxicillin, cefixime -Sample two: resistance to gentamicin, azithromycin, amoxicillin, cefixime |
| Núñez, A et al. [34] | -Impactor-type device (DUO SAS Super 360 (VWR)) -Air sampling between 9:00 a.m. and 14:00 p.m. | -Inside de hospital (a room next to the inpatient wing on the 4th floor) -Outside the hospital on the roof of the hospital wing) | -Petri dishes with Nutrient Agar supplemented with amphotericin to prevent fungal growth -Incubation of collected samples for 3 days at 35 °C | -DNA extraction using DNeasy Powersoil Kit (Quiagen) -16S rRNA amplification for bacteria -ITS sequencing for fungi | -Bacteria concentration indoors was lower than outdoors | -The bacteria composition differs between summer and winter -Opening and closing the window had an influence on air composition inside the hospital -The prodominant bacteria species: Sphingomonas, Streptomyces, Massilia, Hymenobacter and Methylobacterium-Methylorubrum -The predominant fungi species: Cladosporium, Alternaria, Filobasidium and Penicillium |
| Nimra, A et al. [35] | -Volumetric pump sampler -Sampling time 15 min | -Orthopedic wards (OW) and emergency rooms (OER) -Two hospitals- one centrally air-conditioned and the other without central air-conditioning. | -Nutrient agar plates: incubated for 24 h at 37 °C -Sabouraud dextrose agar: incubated for 6 to 7 days at 28 °C. | -PCR (16S rRNA amplification) -Flow cytometry analysis | -Bacteria: the culture study showed a lower bacterial count in OW and OER in an air-conditioned hospital -Fungi: the fungal count showed no significant difference between the two OW, but in OER in a non-air conditioned hospital, the fungal load was higher; the examination allowed to identify: A. flavus and A. Niger in both OW and higher amounts of Penicillium and A. niger in OER in air-conditioned hospital compared to non-air conditioned hospital where A. flavus and A. Niger were more abundant. | -The most observed colonies were identified by PCR, which showed Gram(+) rods: Bacillus cereus, Bacillus subtilis, and Clostridium perfringens, Gram(−) rods: Escherichia coli and Klebsiella pneumonia, and the Gram(+) cocci Staphylococcus aureus and Micrococcus luteus |
| Wu B et al. [36] | -Andersen-6 impact-type sampler -RCS centrifugal air microbial -Sampling time 1 to 5 min | -Samples were taken from 3 different wards (wards A, B, and C) from 3 different points -Samples were also taken from the corridors 5 m and 10 m away from the wards | -Agar supplemented with 5% ram blood and 1% glucose. -Incubation for 24–48 h at 37 °C -Antibiotic resistance test by determining the zone of bacterial growth inhibition. | -Pulsed-field gel electrophoresis (PFGE) | -The highest bacterial count was observed in Ward A, while the lowest count was found in Ward B, with a notable difference. -This trend was similarly reflected in the specific concentration of E. coli. -The E. coli isolated from ward A showed a complete resistance to ampicillin. | -The PFGE analysis revealed a genetic polymorphism among the isolated species. -The test facilitated the comparison of E. coli strains obtained from three distinct wards. -Samples collected from the corridor outside the ward exhibited high similarity to ward samples, suggesting the possible airborne transmission beyond the ward. |
| Handorean A et al. [37] | -Liquid impingers modified for ultra-clean DNA recovery -Liquid impingers modified for ultra-clean DNA recovery -Liquid impingers modified for ultra-clean DNA recovery -Sampling time: 48 h periods in February (prior to patients’ occupation) and June (initial patients’ occupation) | -Hospital holding textile rooms | - | -PCR (16S rRNA sequencing) | - | Higher concentrations of Staphylococcus, Propionibacteria, Corynebacteria, Lactobacillus, and Streptococcus spp. were found, significantly surpassing levels in patient rooms with clean bedding. Seasonal variations influenced bacterial content, with Propionibacterium species dominating in winter while other species remained relatively stable. |
| Habibi, N. et al. [38] | -A customized sampler -Sampling time: 2 h | -Hospital I: near the main entrance, reception, pediatric consualty, central laboratories, pharmacy, and COVID ward -Hospital II: COVID isolation areas and ward, virology, and cytology laboratories -Non-hospitalized setting | - | -Bacteria: PCR (16S rRNA amplification) -Fungi: PCR (18S rRNA amplification) | - | -The molecular testing provided the information about fungal and bacteria taxa -The tests allowed to identify of the most abundant species present in each examined place in both hospitals and non-hospitalized settings |
| Angenent LT et al. [3] | -γ-radiated filter cassette -Swirling aerosol collectors (SACs) -Sampling time 1h or 2 h 40 min depending on the season. | -Hospital therapy pool with independent ventilation system -Air from the outside of the hospital | -Tryptic soy agar -Incubated for 2–3 weeks at 37 °C. | -PCR -Cloning -Restriction fragment length polymorphism (RFLP) -Sequencing | -The number of colonies in all samples was always higher inside the therapy pool area than outside. -The number of colonies did not represent the real bacterial load in the samples; therefore, the test requires more specialized methods than the culture method. | -Seventy-seven mycobacterial rRNA genes were identified in the air samples, with some closely related to pathogenic species like M. avium. -Prevotella melaninogenica, associated with vaginitis, periodontal disease, and sinusitis, was detected in the air. -Additionally, Staphylococcus spp. and Streptococcus spp. or Alloiococcus otitis, responsible for ear infections, were present in the pool air. |
| Perkins SD et al. [39] | -Swirling aerosol collector -Sampling time: 90 min | -Hospital shower prior to turning on the water and while the shower was turned on -The samples were taken while using a conventional shower head and with a Pall-Aquasafe water filter -Shower water | -Microbiological analysis was carried out only for the sample of collected water, which is irrelevant to this review. | -PCR (16S rRNA amplification) | - | -The DNA concentration in the winter samples and in all samples collected under the water filter conditions were too low for successful sequencing. -Samples collected under ordinary showerhead conditions detected the presence of bacteria from Proteobacteria genera. -Detailed phylogenetic analysis detected 444 operational taxonomic units. -The most pathogenic bacteria detected in air samples was P. aeruginosa. |
| Montagna, M.T et al. [40] | -Surface Air System -Petri dishes -Total sampling time: 8 h | -Air from around the tap from ten hospitals | -Petri dishes with Glycine-Vancomycin-Polymyxin-Cycloheximide medium | -Sequence-based typing (SBT) | -As the Legionella pneumophilia 6 serotype was the most abundant, the culture method allowed to establish the bacteria concentrations in collected samples (CFU/L) | -The SBT investigated the allelic profiles of the detected Legionella strains. -A more exact spread of Lgn serotypes could be established |
| Jiang, X et al. [41] | -A fabricated microfluid chip | -Cultured S. aureus -Intensive care unit, surgery room, emergency room, surgical ward, outpatient service hall and doctor’s office | - | -Loop-mediated isothermal amplification (LAMP) | - | -The LAMP results of the samples from the hospital were negative because the collected number of bacteria was lower than the limit of detection (LOD) |
| Chen, P.-S et al. [42] | -Nuclepore filter -Sampling time: 8 h (4 h in consulting rooms) | -Tuberculosis (TB) positive patients’ areas -Suspected TB patients’ areas -Non-TB patients’ areas | - | -RT-qPCR | - | -The Mycobacterium tuberculosis concentrations in TB-positive areas were significantly higher than in non-TB areas. -The increased concentrations of M. tuberculosis implicate a high risk of nosominal infections in health workers or other patients |
| Gilbert, Y et al. [43] | -Six stage Andersen impactor -Bacteria sampling time: 20 min -Fungi sampling time: 5 min | -Ten pulmonology ward rooms with recently gone patients -Control room | -Bacteria: tryptic soy agar and blood agar incubated for 48 h at 25 °C and 37 °C, respectively -Fungi: rose Bengal agar, incubated for 7 days at 25 °C | -PCR (16s rRNA sequencing) -Denaturing gradient gel electrophoresis (DGGE) | -Bacteria: the concentrations in hospital rooms did not show a significant difference compared to the concentrations in the control room -Fungi: the fungal concentrations were significantly higher than in control samples | -Dominant bacteria identified: Staphylococcus epidermidis, Staphylococcus. hominis, Bacillus spp. and Micrococcus luteus -Dominant fungi identified: Cladosporium sp. and Penicillium sp. -The molecular tests detected antibiotic resistance in many strains, like vancomycin resistance in S. paucimobilis |
| Retamal-Valdes B et al. [44] | -Agar plates | -Before the dental procedure: support board attached to the reflector, the bracket tray, and the office bench -During the dental procedure: the support board, volunteer’s chest, and clinician’s forehead. | -Tryptic Soy Agar with Yeast Extract enriched with 5% menadione, 5% sheep blood, and 1% N-Acetylmuramic acid -Incubated for 72 h at 37 °C. | -DNA hybridization | -No bacterial growth was detected in the samples collected from the dental office before the procedure. -The colony-forming units (CFU) of the bacteria gathered from the patient’s chest and operator’s forehead were significantly lower in groups who rinsed with CPC+Zn+F and CHX compared to groups with water or no rinse. | -The DNA hybridization technique identified 40 species of subgingival bacteria species -In groups rinsing with CPC+Zn+F or CHX, the aerosol generated during full-mouth dental prophylaxis contained a smaller quantity of orange complex bacteria compared to the group rinsing with water or not rinsing. |
| Criteria | Study | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Yousefzadeh A et al. [26] | Núñez, A et al. [34] | Nimra, A et al. [35] | Wu B et al. [36] | Handorean A et al. [37] | Habibi, N et al. [38] | Angenent LT et al. [3] | Perkins SD et al. [39] | Montagna, M.T et al. [40] | Jiang, X et al. [41] | Chen, P.-S et al. [42] | Gilbert, Y et al. [43] | Retamal-Valdes B. et al. [44] | |
| Origin of the aerosol | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Method of collecting the aerosol | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Method and type of molecular test performed | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Presence of a control group | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 1 |
| Sample size calculation | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 1 |
| Number of samples in the group of more than 10 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| Total | 4 | 5 | 4 | 4 | 4 | 4 | 3 | 3 | 3 | 4 | 5 | 3 | 6 |
| Risk of bias | moderate | low | moderate | moderate | moderate | moderate | moderate | moderate | moderate | moderate | low | moderate | low |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matys, J.; Kensy, J.; Gedrange, T.; Zawiślak, I.; Grzech-Leśniak, K.; Dobrzyński, M. A Molecular Approach for Detecting Bacteria and Fungi in Healthcare Environment Aerosols: A Systematic Review. Int. J. Mol. Sci. 2024, 25, 4154. https://doi.org/10.3390/ijms25084154
Matys J, Kensy J, Gedrange T, Zawiślak I, Grzech-Leśniak K, Dobrzyński M. A Molecular Approach for Detecting Bacteria and Fungi in Healthcare Environment Aerosols: A Systematic Review. International Journal of Molecular Sciences. 2024; 25(8):4154. https://doi.org/10.3390/ijms25084154
Chicago/Turabian StyleMatys, Jacek, Julia Kensy, Tomasz Gedrange, Ireneusz Zawiślak, Kinga Grzech-Leśniak, and Maciej Dobrzyński. 2024. "A Molecular Approach for Detecting Bacteria and Fungi in Healthcare Environment Aerosols: A Systematic Review" International Journal of Molecular Sciences 25, no. 8: 4154. https://doi.org/10.3390/ijms25084154
APA StyleMatys, J., Kensy, J., Gedrange, T., Zawiślak, I., Grzech-Leśniak, K., & Dobrzyński, M. (2024). A Molecular Approach for Detecting Bacteria and Fungi in Healthcare Environment Aerosols: A Systematic Review. International Journal of Molecular Sciences, 25(8), 4154. https://doi.org/10.3390/ijms25084154