

Serum Levels of miR-122-5p and miR-125a-5p Predict Hepatotoxicity Occurrence in Patients Undergoing Autologous Hematopoietic Stem Cell Transplantation

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Results
2.1. Study Group Characteristics
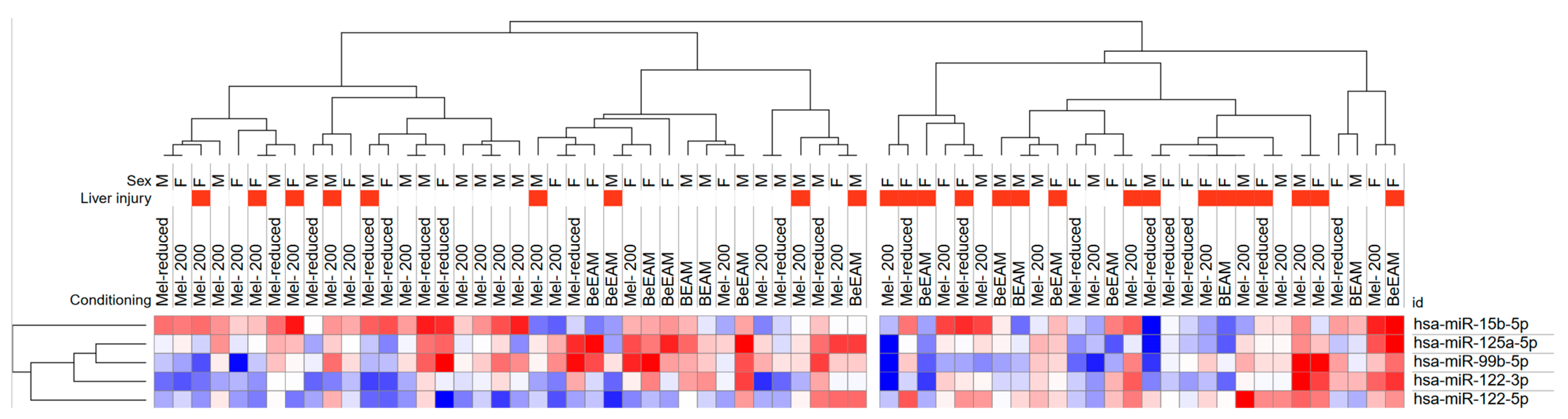
2.2. miRNAs Expression Levels in ASCT Patients in Relation to Liver Injury
2.3. Factors Associated with Liver Injury
2.4. Prediction of miRNAs Target Genes and KEGG Pathway Analysis
3. Discussion
4. Materials and Methods
4.1. Patients and Treatment
4.2. Hepatotoxicity Assessment and miRNAs Selection
4.3. Samples Collection and RT-qPCR
4.4. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Niederwieser, D.; Baldomero, H.; Bazuaye, N.; Bupp, C.; Chaudhri, N.; Corbacioglu, S.; Elhaddad, A.; Frutos, C.; Galeano, S.; Hamad, N.; et al. One and a Half Million Hematopoietic Stem Cell Transplants: Continuous and Differential Improvement in Worldwide Access with the Use of Non-Identical Family Donors. Haematologica 2022, 107, 1045. [Google Scholar] [CrossRef]
- Kodad, S.G.; Sutherland, H.; Limvorapitak, W.; Abou Mourad, Y.; Barnett, M.J.; Forrest, D.; Gerrie, A.; Hogge, D.E.; Nantel, S.H.; Narayanan, S.; et al. Outpatient Autologous Stem Cell Transplants for Multiple Myeloma: Analysis of Safety and Outcomes in a Tertiary Care Center. Clin. Lymphoma Myeloma Leuk. 2019, 19, 784–790. [Google Scholar] [CrossRef] [PubMed]
- Shah, N.; Cornelison, A.M.; Saliba, R.; Ahmed, S.; Nieto, Y.L.; Bashir, Q.; Parmar, S.; Hosing, C.; Popat, U.; Shpall, E.J.; et al. Inpatient vs Outpatient Autologous Hematopoietic Stem Cell Transplantation for Multiple Myeloma. Eur. J. Haematol. 2017, 99, 532–535. [Google Scholar] [CrossRef] [PubMed]
- Dytfeld, D.; Łojko-Dankowska, A.; Nowicki, A.; Matuszak, M.; Wache, A.; Gil, L. Safety and Cost Effectiveness of Outpatient Autologous Hematopoietic Stem Cell Transplantation for Multiple Myeloma—Single-Center Experience of a Pilot Early Discharge Program. Acta Haematol. Pol. 2021, 52, 178–181. [Google Scholar] [CrossRef]
- Patel, R.D.; Klumpp, T.R.; Martin, M.E.; Kropf, P.; Fasan, O.O.; Mangan, K.F. A Retrospective Analysis of The Association Between Common Myeloablative Conditioning Regimens and Hepatotoxicity. Blood 2013, 122, 5515. [Google Scholar] [CrossRef]
- de Moura Almeida, A.; Cotrim, H.P.; Fonseca, D.C.; Alencar, D.M.; Dutra, D.D.; de Melo Santos, H.H.; Botura, M.; Salvino, M.A.; Arruda, M. da G.B. Liver Injury after Autologous Hematopoietic Stem Cell Transplant: DILI and SOS. Blood 2018, 132, 2161. [Google Scholar] [CrossRef]
- Abdelbary, H.; Magdy, R.; Moussa, M.; Abdelmoaty, I. Liver Disease during and after Hematopoietic Stem Cell Transplantation in Adults: A Single-Center Egyptian Experience. J. Egypt. Natl. Canc. Inst. 2020, 32, 1–8. [Google Scholar] [CrossRef]
- Modi, D.; Ye, J.C.; Surapaneni, M.; Singh, V.; Chen, W.; Jang, H.; Deol, A.; Ayash, L.; Alavi, A.; Ratanatharathorn, V.; et al. Liver Graft-Versus-Host Disease Is Associated with Poor Survival among Allogeneic Hematopoietic Stem Cell Transplant Recipients. Am. J. Hematol. 2019, 94, 1072–1080. [Google Scholar] [CrossRef]
- Condrat, C.E.; Thompson, D.C.; Barbu, M.G.; Bugnar, O.L.; Boboc, A.; Cretoiu, D.; Suciu, N.; Cretoiu, S.M.; Voinea, S.C. MiRNAs as Biomarkers in Disease: Latest Findings Regarding Their Role in Diagnosis and Prognosis. Cells 2020, 9, 276. [Google Scholar] [CrossRef]
- SMitchell, P.S.; Parkin, R.K.; Kroh, E.M.; Fritz, B.R.; Wyman, S.K.; Pogosova-Agadjanyan, E.L.; Peterson, A.; Noteboom, J.; O’Briant, K.C.; Allen, A.; et al. Circulating MicroRNAs as Stable Blood-Based Markers for Cancer Detection. Proc. Natl. Acad. Sci. USA 2008, 105, 10513–10518. [Google Scholar] [CrossRef]
- Wang, K.; Zhang, S.; Marzolf, B.; Troisch, P.; Brightman, A.; Hu, Z.; Hood, L.E.; Galas, D.J. Circulating MicroRNAs, Potential Biomarkers for Drug-Induced Liver Injury. Proc. Natl. Acad. Sci. USA 2009, 106, 4402–4407. [Google Scholar] [CrossRef] [PubMed]
- Russo, M.W.; Steuerwald, N.; Norton, H.J.; Anderson, W.E.; Foureau, D.; Chalasani, N.; Fontana, R.J.; Watkins, P.B.; Serrano, J.; Bonkovsky, H.L. Profiles of MiRNAs in Serum in Severe Acute Drug Induced Liver Injury and Their Prognostic Significance. Liver Int. 2017, 37, 757–764. [Google Scholar] [CrossRef] [PubMed]
- Cione, E.; Abrego Guandique, D.M.; Caroleo, M.C.; Luciani, F.; Colosimo, M.; Cannataro, R. Liver Damage and MicroRNAs: An Update. Curr. Issues Mol. Biol. 2023, 45, 78–91. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Cheng, X.; Lu, Z.; Wang, J.; Chen, H.; Fan, W.; Gao, X.; Lu, D. Upregulation of miR-15b in NAFLD models and in the serum of patients with fatty liver disease. Diabetes Res. Clin. Pract. 2013, 99, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Chen, J.; Liu, Y.; Li, S.; Huang, P. Plasma miR-15b-5p, miR-338-5p, and miR-764 as Biomarkers for Hepatocellular Carcinoma. Med. Sci. Monit. 2015, 21, 1864–1871. [Google Scholar] [CrossRef] [PubMed]
- Cisilotto, J.; do Amaral, A.E.; Rosolen, D.; Rode, M.P.; Silva, A.H.; Winter, E.; da Silva, T.E.; Fischer, J.; Matiollo, C.; Rateke, E.C.D.M.; et al. MicroRNA profiles in serum samples from Acute-On-Chronic Liver Failure patients and miR-25-3p as a potential biomarker for survival prediction. Sci. Rep. 2020, 10, 100. [Google Scholar] [CrossRef] [PubMed]
- Messner, C.J.; Schmidt, S.; Özkul, D.; Gaiser, C.; Terracciano, L.; Krähenbühl, S.; Suter-Dick, L. Identification of mir-199a-5p, mir-214-3p and mir-99b-5p as fibrosis-specific extracellular biomarkers and promoters of hsc activation. Int. J. Mol. Sci. 2021, 22, 9799. [Google Scholar] [CrossRef] [PubMed]
- Tuncer, H.H.; Rana, N.; Milani, C.; Darko, A.; Al-Homsi, S.A. Gastrointestinal and Hepatic Complications of Hematopoietic Stem Cell Transplantation. World J. Gastroenterol. 2012, 18, 1851–1860. [Google Scholar] [CrossRef]
- Hogan, W.J.; Maris, M.; Storer, B.; Sandmaier, B.M.; Maloney, D.G.; Schoch, H.G.; Woolfrey, A.E.; Shulman, H.M.; Storb, R.; McDonald, G.B. Hepatic Injury after Nonmyeloablative Conditioning Followed by Allogeneic Hematopoietic Cell Transplantation: A Study of 193 Patients. Blood 2004, 103, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.; Nicolas, E.; Marks, D.; Sander, C.; Lerro, A.; Buendia, M.A.; Xu, C.; Mason, W.S.; Moloshok, T.; Bort, R.; et al. MiR-122, a Mammalian Liver-Specific MicroRNA, Is Processed from Hcr MRNA and May Downregulate the High Affinity Cationic Amino Acid Transporter CAT-1. RNA Biol. 2004, 1, 106–113. [Google Scholar] [CrossRef]
- Lagos-Quintana, M.; Rauhut, R.; Yalcin, A.; Meyer, J.; Lendeckel, W.; Tuschl, T. Identification of Tissue-Specific MicroRNAs from Mouse. Curr. Biol. 2002, 12, 735–739. [Google Scholar] [CrossRef] [PubMed]
- Jopling, C.L. Liver-Specific MicroRNA-122: Biogenesis and Function. RNA Biol. 2012, 9, 137. [Google Scholar] [CrossRef] [PubMed]
- Krauskopf, J.; De Kok, T.M.; Schomaker, S.J.; Gosink, M.; Burt, D.A.; Chandler, P.; Warner, R.L.; Johnson, K.J.; Caiment, F.; Kleinjans, J.C.; et al. Serum MicroRNA Signatures as “Liquid Biopsies” for Interrogating Hepatotoxic Mechanisms and Liver Pathogenesis in Human. PLoS ONE 2017, 12, e0177928. [Google Scholar] [CrossRef] [PubMed]
- Vliegenthart, A.D.B.; Shaffer, J.M.; Clarke, J.I.; Peeters, L.E.J.; Caporali, A.; Bateman, D.N.; Wood, D.M.; Dargan, P.I.; Craig, D.G.; Moore, J.K.; et al. Comprehensive MicroRNA Profiling in Acetaminophen Toxicity Identifies Novel Circulating Biomarkers for Human Liver and Kidney Injury. Sci. Rep. 2015, 5, 15501. [Google Scholar] [CrossRef] [PubMed]
- Jopling, C.L.; Yi, M.K.; Lancaster, A.M.; Lemon, S.M.; Sarnow, P. Modulation of Hepatitis C Virus RNA Abundance by a Liver-Specific MicroRNA. Science 2005, 309, 1577–1581. [Google Scholar] [CrossRef] [PubMed]
- Shimakami, T.; Yamane, D.; Jangra, R.K.; Kempf, B.J.; Spaniel, C.; Barton, D.J.; Lemon, S.M. Stabilization of Hepatitis C Virus RNA by an Ago2-MiR-122 Complex. Proc. Natl. Acad. Sci. USA 2012, 109, 941–946. [Google Scholar] [CrossRef]
- Murray, D.D.; Suzuki, K.; Law, M.; Trebicka, J.; Neuhaus Nordwall, J.; Johnson, M.; Vjecha, M.J.; Kelleher, A.D.; Emery, S. Circulating MiR-122 and MiR-200a as Biomarkers for Fatal Liver Disease in ART-Treated, HIV-1-Infected Individuals. Sci. Rep. 2017, 7, 10934. [Google Scholar] [CrossRef] [PubMed]
- Moosa, M.S.; Russomanno, G.; Dorfman, J.R.; Gunter, H.; Patel, C.; Costello, E.; Carr, D.; Maartens, G.; Pirmohamed, M.; Goldring, C.; et al. Analysis of Serum MicroRNA-122 in a Randomized Controlled Trial of N-Acetylcysteine for Treatment of Antituberculosis Drug-Induced Liver Injury. Br. J. Clin. Pharmacol. 2023, 89, 1844–1851. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.; Zhou, Z.; Xu, Z.; Li, G.; Dong, P.; Chen, Z.; Lin, D.; Chen, B.; Yu, F. Serum MicroRNA-125a-5p, a Useful Biomarker in Liver Diseases, Correlates with Disease Progression. Mol. Med. Rep. 2015, 12, 1584–1590. [Google Scholar] [CrossRef]
- Coppola, N.; Potenza, N.; Pisaturo, M.; Mosca, N.; Tonziello, G.; Signoriello, G.; Messina, V.; Sagnelli, C.; Russo, A.; Sagnelli, E. Liver MicroRNA Hsa-MiR-125a-5p in HBV Chronic Infection: Correlation with HBV Replication and Disease Progression. PLoS ONE 2013, 8, e65336. [Google Scholar] [CrossRef]
- Zhang, C.; Zhao, Y.; Wang, Q.; Qin, J.; Ye, B.; Xu, C.; Yu, G. Overexpression of MiR-125a-5p Inhibits Hepatocyte Proliferation through the STAT3 Regulation In Vivo and In Vitro. Int. J. Mol. Sci. 2022, 23, 8661. [Google Scholar] [CrossRef] [PubMed]
- Berasain, C.; Castillo, J.; Prieto, J.; Avila, M.A. New Molecular Targets for Hepatocellular Carcinoma: The ErbB1 Signaling System. Liver Int. 2007, 27, 174–185. [Google Scholar] [CrossRef]
- Berasain, C.; Avila, M.A. The EGFR Signalling System in the Liver: From Hepatoprotection to Hepatocarcinogenesis. J. Gastroenterol. 2014, 49, 9–23. [Google Scholar] [CrossRef] [PubMed]
- Oakley, F.; Trim, N.; Constandinou, C.M.; Ye, W.; Gray, A.M.; Frantz, G.; Hillan, K.; Kendall, T.; Benyon, R.C.; Mann, D.A.; et al. Hepatocytes Express Nerve Growth Factor during Liver Injury: Evidence for Paracrine Regulation of Hepatic Stellate Cell Apoptosis. Am. J. Pathol. 2003, 163, 1849. [Google Scholar] [CrossRef]
- Rasi, G.; Serafino, A.; Bellis, L.; Lonardo, M.T.; Andreola, F.; Zonfrillo, M.; Vennarecci, G.; Pierimarchi, P.; Vallebona, P.S.; Ettorre, G.M.; et al. Nerve Growth Factor Involvement in Liver Cirrhosis and Hepatocellular Carcinoma. World J. Gastroenterol. WJG 2007, 13, 4986. [Google Scholar] [CrossRef]
- Amir, M.; Yu, M.; He, P.; Srinivasan, S. Hepatic Autonomic Nervous System and Neurotrophic Factors Regulate the Pathogenesis and Progression of Non-Alcoholic Fatty Liver Disease. Front. Med. 2020, 7, 62. [Google Scholar] [CrossRef] [PubMed]
- Fabregat, I.; Moreno-Càceres, J.; Sánchez, A.; Dooley, S.; Dewidar, B.; Giannelli, G.; ten Dijke, P. TGF-β Signalling and Liver Disease. FEBS J. 2016, 283, 2219–2232. [Google Scholar] [CrossRef]
- Dooley, S.; Ten Dijke, P. TGF-β in Progression of Liver Disease. Cell Tissue Res. 2012, 347, 245. [Google Scholar] [CrossRef]
- Zhang, C.; Sun, C.; Zhao, Y.; Ye, B.; Yu, G.Y. Signaling Pathways of Liver Regeneration: Biological Mechanisms and Implications. iScience 2024, 27, 108683. [Google Scholar] [CrossRef]
- Drug-Induced Liver Injury: Premarketing Clinical Evaluation|FDA. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/drug-induced-liver-injury-premarketing-clinical-evaluation (accessed on 6 April 2024).
- Stutchfield, B.M.; Antoine, D.J.; Mackinnon, A.C.; Gow, D.J.; Bain, C.C.; Hawley, C.A.; Hughes, M.J.; Francis, B.; Wojtacha, D.; Man, T.Y.; et al. CSF1 Restores Innate Immunity After Liver Injury in Mice and Serum Levels Indicate Outcomes of Patients With Acute Liver Failure. Gastroenterology 2015, 149, 1896–1909.e14. [Google Scholar] [CrossRef]
- Church, R.J.; Kullak-Ublick, G.A.; Aubrecht, J.; Bonkovsky, H.L.; Chalasani, N.; Fontana, R.J.; Goepfert, J.C.; Hackman, F.; King, N.M.P.; Kirby, S.; et al. Candidate Biomarkers for the Diagnosis and Prognosis of Drug-Induced Liver Injury: An International Collaborative Effort. Hepatology 2019, 69, 760–773. [Google Scholar] [CrossRef] [PubMed]
- Humphries, C.; Dear, J.W. Novel Biomarkers for Drug-Induced Liver Injury. Clin. Toxicol. 2023, 61, 567–572. [Google Scholar] [CrossRef] [PubMed]
- Ye, H.; Nelson, L.J.; Del Moral, M.G.; Martínez-Naves, E.; Cubero, F.J. Dissecting the Molecular Pathophysiology of Drug-Induced Liver Injury. World J. Gastroenterol. 2018, 24, 1373. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos, T.N.; Duarte, F.B.; Filho, P.A.M.; De Jesus Dos Santos, T.E.; Barbosa, M.C.; De Almeida Filho, T.P.; Cavalcanti, B.C.; De Vasconcelos, P.R.L.; Dutra, L.L.; Lopes, G.S.; et al. Association of Oxidative Stress and DNA Damage with Grafting Time in Patients with Multiple Myeloma and Lymphoma Submitted to Autologous Hematopoietic Stem Cell Transplantation. Rev. Assoc. Med. Bras. 2016, 62, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, T.L.; Benvegnú, D.M.; Bonfanti, G.; Frediani, A.V.; Rocha, J.B.T. δ-ALA-D Activity Is a Reliable Marker for Oxidative Stress in Bone Marrow Transplant Patients. BMC Cancer 2009, 9, 138. [Google Scholar] [CrossRef] [PubMed]
- Nakazato, T.; Ito, C.; Shimazaki, K.; Arakaki, H.; Aisa, Y. Evaluation of Oxidative Stress Markers in Hematopoietic Stem Cell Transplantation Patients. Blood 2015, 126, 1925. [Google Scholar] [CrossRef]
- Saeed, H.; Alstott, M.C.; Mitov, M.; Butterfield, D.A.; Van Meter Dressler, E.; Yalamanchi, S.; Hayslip, J.; Monohan, G. Oxidative Stress Following High Dose Chemotherapy with Autologous Stem Cell Transplant. Biol. Blood Marrow Transplant. 2016, 22, S131–S132. [Google Scholar] [CrossRef]
- Mikulski, D.; Nowicki, M.; Dróźdż, I.; Misiewicz, M.; Kościelny, K.P.; Okoński, K.; Krawiec, K.; Perdas, E.; Wierzbowska, A.; Fendler, W. High Serum MiR-223-3p Expression Level Predicts Complete Response and Prolonged Overall Survival in Multiple Myeloma Patients Undergoing Autologous Hematopoietic Stem Cell Transplantation. Front. Oncol. 2023, 13, 1250355. [Google Scholar] [CrossRef]
- Navarro, A.; Díaz, T.; Tovar, N.; Pedrosa, F.; Tejero, R.; Cibeira, M.T.; Magnano, L.; Rosiñol, L.; Monzó, M.; Bladé, J.; et al. A Serum MicroRNA Signature Associated with Complete Remission and Progression after Autologous Stem-Cell Transplantation in Patients with Multiple Myeloma. Oncotarget 2015, 6, 1874–1883. [Google Scholar] [CrossRef]
- Sevcikova, A.; Fridrichova, I.; Nikolaieva, N.; Kalinkova, L.; Omelka, R.; Martiniakova, M.; Ciernikova, S. Clinical Significance of MicroRNAs in Hematologic Malignancies and Hematopoietic Stem Cell Transplantation. Cancers 2023, 15, 2658. [Google Scholar] [CrossRef]
- Reikvam, H.; Vo, A.K.; Johansen, S.; Hemsing, A.L.; Solheim, M.H.; Mosevoll, K.A.; Tvedt, T.H.A.; Hatfield, K.J. MicroRNA Serum Profiles and Chronic Graft-versus-Host Disease. Blood Adv. 2022, 6, 5295. [Google Scholar] [CrossRef] [PubMed]
- Bearman, S.I.; Appelbaum, F.R.; Buckner, C.D.; Petersen, F.B.; Fisher, L.D.; Clift, R.A.; Thomas, E.D. Regimen-Related Toxicity in Patients Undergoing Bone Marrow Transplantation. J. Clin. Oncol. 2016, 6, 1562–1568. [Google Scholar] [CrossRef] [PubMed]
- Labonté, L.; Iqbal, T.; Zaidi, M.A.; McDiarmid, S.A.; Huebsch, L.B.; Tay, J.; Atkins, H.; Allan, D.S. Utility of Comorbidity Assessment in Predicting Transplantation-Related Toxicity Following Autologous Hematopoietic Stem Cell Transplantation for Multiple Myeloma. Biol. Blood Marrow Transplant. 2008, 14, 1039–1044. [Google Scholar] [CrossRef] [PubMed]
- Grabia, S.; Smyczynska, U.; Pagacz, K.; Fendler, W. NormiRazor: Tool Applying GPU-Accelerated Computing for Determination of Internal References in MicroRNA Transcription Studies. BMC Bioinform. 2020, 21, 425. [Google Scholar] [CrossRef] [PubMed]
- Mikulski, D.; Dróżdż, I.; Perdas, E.; Stawiski, K.; Nowicki, M.; Misiewicz, M.; Strzałka, P.; Wierzbowska, A.; Fendler, W. Changes in the Microrna Expression Profile in Patients Undergoing Autologous Steam Cell Transplantation. Blood 2021, 138, 4789. [Google Scholar] [CrossRef]
- Chang, L.; Zhou, G.; Soufan, O.; Xia, J. miRNet 2.0: Network-based visual analytics for miRNA functional analysis and systems biology. Nucleic Acids Res. 2020, 48, W244–W251. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total N (%) |
|---|---|
| Number of patients | 66 (100) |
| Sex | F: 34 (51.5) |
| M: 3 2 (48.5) | |
| Age at ASCT | 59 |
| Median (IQR) | (49–65) |
| Diagnosis | |
| Multiple Myeloma | 50 (75.8) |
| Hodgkin Lymphoma | 8 (12.1) |
| Mantle Cell Lymphoma | 4 (6.1) |
| Diffuse Large B-cell Lymphoma | 2 (3.0) |
| Angioimmunoblastic T-cell Lymphoma | 1 (1.5) |
| Anaplastic Large Cell Lymphoma | 1 (1.5) |
| Myeloma stage | |
| ISS I | 17 (34.0) |
| ISS II | 10 (20.0) |
| ISS III | 15 (30.0) |
| Missing | 8 (16.0) |
| Ann Arbor | |
| I | 1 (8.3) |
| II | 2 (16.7) |
| III | 4 (33.3) |
| IV | 5 (41.7) |
| Conditioning | |
| Mel-200 | 32 (48.5) |
| Mel-reduced | 18 (27.3) |
| BeEAM | 11 (16.7) |
| BEAM | 5 (7.6) |
| HBV/HCV infection | |
| Without HBV/HCV | 58 (87.9) |
| HBV | 7 (10.6) |
| HCV | 1 (1.5) |
| Markers of liver injury preASCT | |
| Median (IQR) | |
| AST (U/L) | 19 (16–22) |
| ALT (U/L) | 20 (14–28) |
| Bilirubin (mg/dL) | 0.36 (0.3–0.5) |
| Albumins (mg/dL) | 41.25 (38.3–44.4) |
| GGTP (U/L) | 18 (13–33) |
| ALP (U/L) | 79.5 (59.5–105.5) |
| Antifungal treatment after ASCT | |
| No | 34 (51.5) |
| Yes | 30 (45.5) |
| Missing | 2 (3) |
| Abnormal ALT and/or AST at admission | |
| No | 64 (97.0) |
| Yes | 2 (3.0) |
| Variable | Value | OR | 95% CI Lower | 95% CI Upper | p-Value |
|---|---|---|---|---|---|
| HBV/HCV | No | Reference | |||
| Yes | 0.20 | 0.02 | 1.75 | 0.1471 | |
| Diagnosis | Lymphoma | Reference | |||
| Myeloma | 0.52 | 0.16 | 1.61 | 0.2547 | |
| Sex | Male | Reference | |||
| Female | 1.34 | 0.49 | 3.63 | 0.5696 | |
| Age at ASCT | <60 years | Reference | |||
| ≥60 years | 0.37 | 0.13 | 1.08 | 0.0679 | |
| Albumin | g/L | 1.09 | 0.92 | 1.29 | 0.3244 |
| AST | IU/L | 1.00 | 0.93 | 1.07 | 0.9978 |
| ALT | IU/L | 1.01 | 0.97 | 1.05 | 0.7740 |
| Bilirubin | Above median | 0.44 | 0.14 | 1.39 | 0.1636 |
| ALP | IU/L | 1.00 | 0.98 | 1.02 | 0.7331 |
| GGTP | IU/L | 1.02 | 0.98 | 1.07 | 0.2316 |
| Stage | ISS ≤ 2 or Ann Arbor ≤ III | Reference | |||
| ISS 3 or Ann Arbor IV | 0.61 | 0.20 | 1.87 | 0.3864 | |
| Antifungal treatment | No | Reference | |||
| Yes | 0.71 | 0.26 | 1.95 | 0.5112 | |
| Previous lines of treatment | <2 | Reference | |||
| ≥2 | 1.44 | 0.53 | 3.94 | 0.4749 | |
| Conditioning regimen | Mel-200 | Reference | |||
| Mel-reduced | 0.66 | 0.19 | 2.35 | 0.5207 | |
| B(e)EAM | 1.58 | 0.47 | 5.35 | 0.4595 | |
| hsa-miR-15b-5p | 1 dCt | 0.49 | 0.18 | 1.36 | 0.1717 |
| hsa-miR-125a-5p | 1 dCt | 0.56 | 0.30 | 1.05 | 0.0686 |
| hsa-miR-99b-5p | 1 dCt | 0.69 | 0.37 | 1.28 | 0.2442 |
| hsa-miR-122-5p | 1 dCt | 1.59 | 1.09 | 2.32 | 0.0164 |
| hsa-miR-122-3p | 1 dCt | 0.86 | 0.60 | 1.23 | 0.3990 |
| Variable | Value | OR | 95% CI Lower | 95% CI Upper | p-Value |
|---|---|---|---|---|---|
| Sex | Male | Reference | |||
| Female | 1.91 | 0.56 | 6.50 | 0.3029 | |
| Age at ASCT | <60 years | Reference | |||
| ≥60 years | 0.29 | 0.07 | 1.24 | 0.0941 | |
| hsa-miR-122-5p | 1 dCt | 2.10 | 1.29 | 3.42 | 0.0029 |
| hsa-miR-125a-5p | 1 dCt | 0.27 | 0.11 | 0.71 | 0.0079 |
| Conditioning regimen | Mel-200 | Reference | |||
| Mel-reduced | 0.64 | 0.13 | 3.15 | 0.5832 | |
| B(e)EAM | 1.79 | 0.37 | 8.63 | 0.4699 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mikulski, D.; Kościelny, K.; Dróżdż, I.; Mirocha, G.; Nowicki, M.; Misiewicz, M.; Perdas, E.; Strzałka, P.; Wierzbowska, A.; Fendler, W. Serum Levels of miR-122-5p and miR-125a-5p Predict Hepatotoxicity Occurrence in Patients Undergoing Autologous Hematopoietic Stem Cell Transplantation. Int. J. Mol. Sci. 2024, 25, 4355. https://doi.org/10.3390/ijms25084355
Mikulski D, Kościelny K, Dróżdż I, Mirocha G, Nowicki M, Misiewicz M, Perdas E, Strzałka P, Wierzbowska A, Fendler W. Serum Levels of miR-122-5p and miR-125a-5p Predict Hepatotoxicity Occurrence in Patients Undergoing Autologous Hematopoietic Stem Cell Transplantation. International Journal of Molecular Sciences. 2024; 25(8):4355. https://doi.org/10.3390/ijms25084355
Chicago/Turabian StyleMikulski, Damian, Kacper Kościelny, Izabela Dróżdż, Grzegorz Mirocha, Mateusz Nowicki, Małgorzata Misiewicz, Ewelina Perdas, Piotr Strzałka, Agnieszka Wierzbowska, and Wojciech Fendler. 2024. "Serum Levels of miR-122-5p and miR-125a-5p Predict Hepatotoxicity Occurrence in Patients Undergoing Autologous Hematopoietic Stem Cell Transplantation" International Journal of Molecular Sciences 25, no. 8: 4355. https://doi.org/10.3390/ijms25084355
APA StyleMikulski, D., Kościelny, K., Dróżdż, I., Mirocha, G., Nowicki, M., Misiewicz, M., Perdas, E., Strzałka, P., Wierzbowska, A., & Fendler, W. (2024). Serum Levels of miR-122-5p and miR-125a-5p Predict Hepatotoxicity Occurrence in Patients Undergoing Autologous Hematopoietic Stem Cell Transplantation. International Journal of Molecular Sciences, 25(8), 4355. https://doi.org/10.3390/ijms25084355