


Alpha 7 Nicotinic Acetylcholine Receptor Agonist PHA 568487 Reduces Acute Inflammation but Does Not Affect Cardiac Function or Myocardial Infarct Size in the Permanent Occlusion Model
 ,
,
Abstract
:
1. Introduction
2. Results
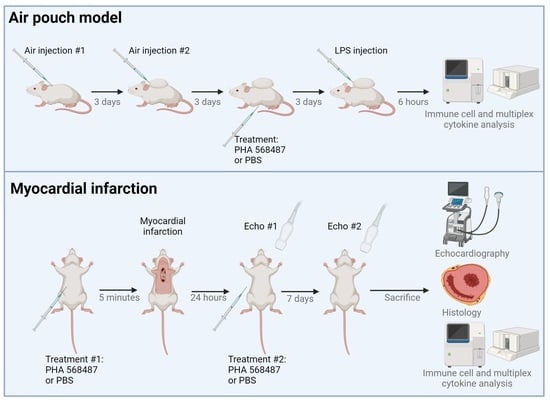
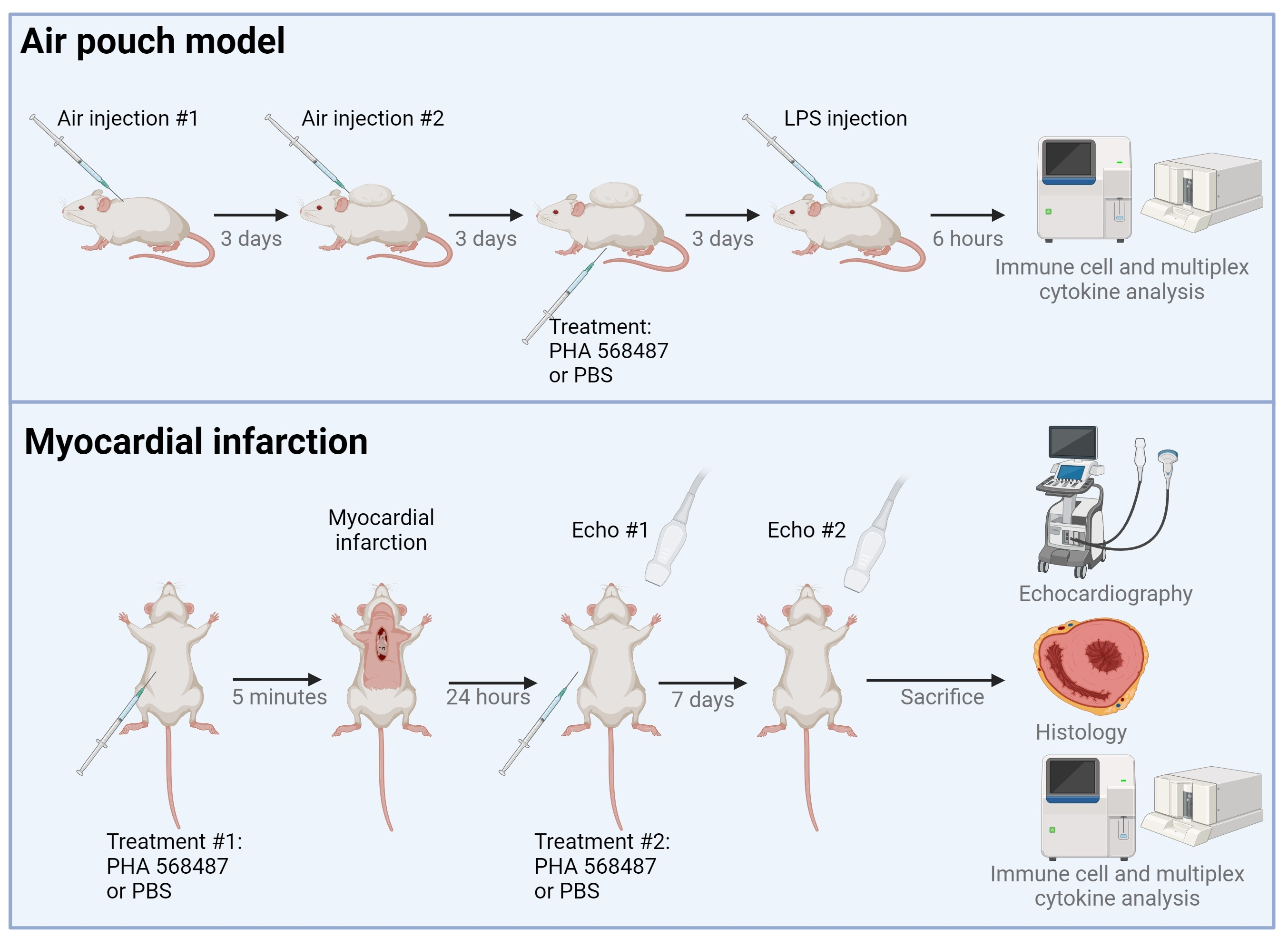
2.1. α7nAChR Agonist PHA 568487 Dampens Inflammation in the Air Pouch Model
2.2. α7nAChR Is Expressed in Primary Cardiomyocytes
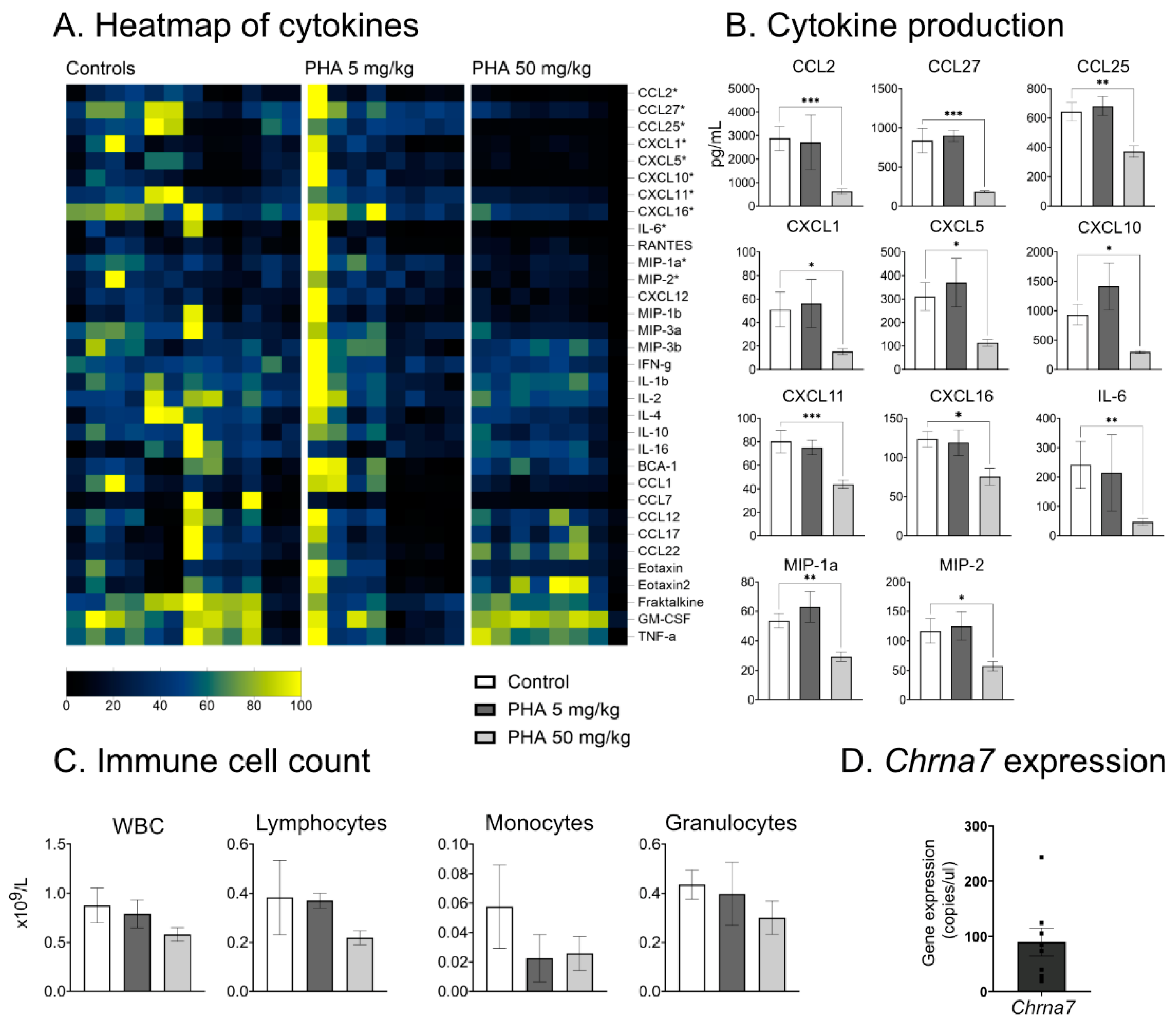
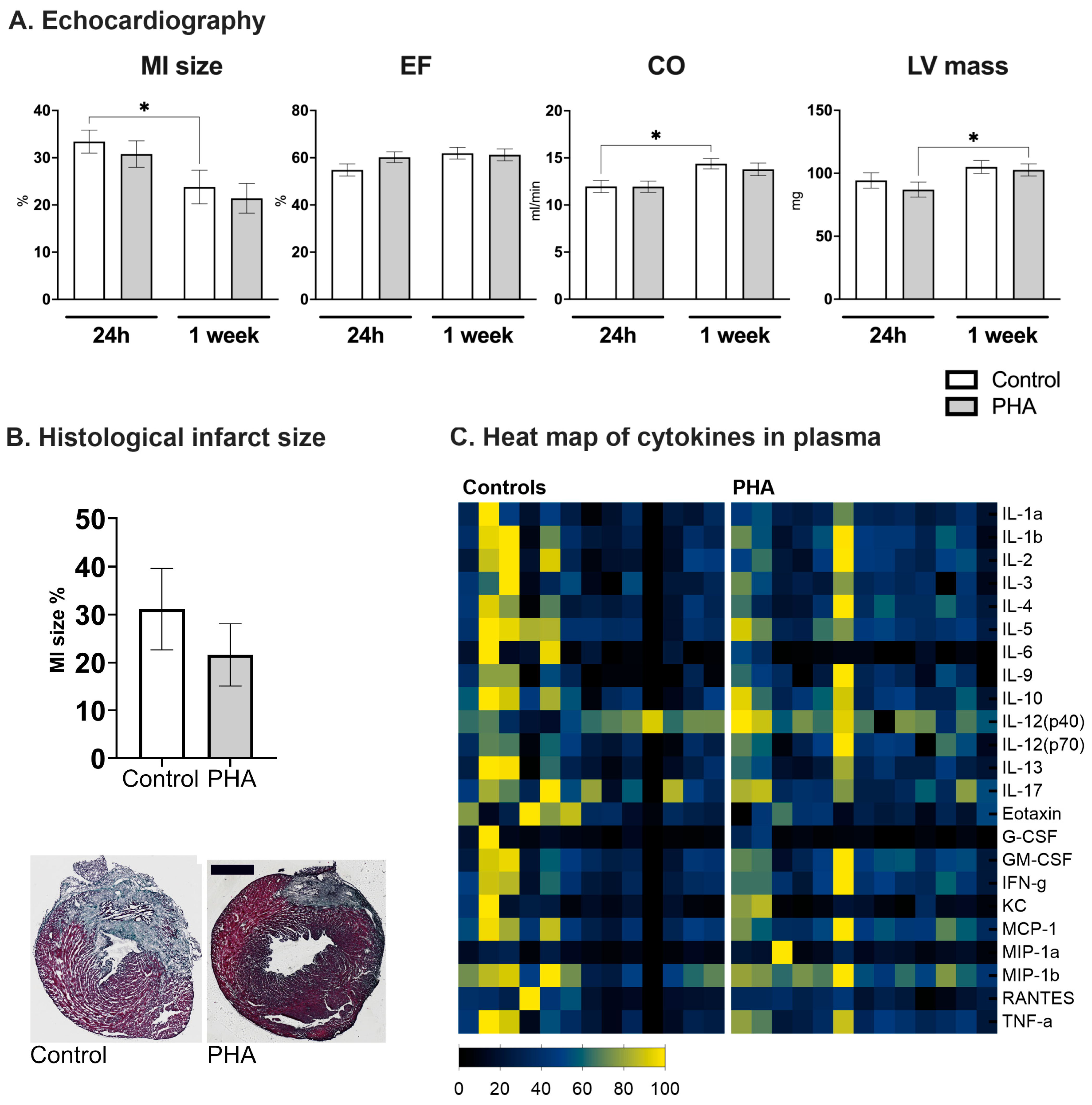
2.3. No Effect of the α7nAChR Agonist PHA 568487 in the Permanent Occlusion Model of Myocardial Infarction
3. Discussion
4. Materials and Methods
4.1. Isolation of Primary Cardiomyocytes and Droplet Digital PCR (ddPCR) Analysis
4.2. Air Pouch Model
4.3. Myocardial Infarction Study
4.4. Echocardiographic Measurements in Mice
4.5. Histological Analysis of Myocardial Infarction Size
4.6. Multiplex Analysis
4.7. Viability
4.8. Ethical Considerations
4.9. Statistics
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D.; Mickley, H.; Crea, F.; Van De Werf, F.; et al. Fourth universal definition of myocardial infarction (2018). Eur. Heart J. 2019, 40, 237–269. [Google Scholar] [CrossRef]
- Anderson, J.L.; Morrow, D.A. Acute Myocardial Infarction. N. Engl. J. Med. 2017, 376, 2053–2064. [Google Scholar] [CrossRef]
- Frangogiannis, N.G. Cardiac fibrosis: Cell biological mechanisms, molecular pathways and therapeutic opportunities. Mol. Asp. Med. 2019, 65, 70–99. [Google Scholar] [CrossRef]
- Dick, S.A.; Macklin, J.A.; Nejat, S.; Momen, A.; Clemente-Casares, X.; Althagafi, M.G.; Chen, J.; Kantores, C.; Hosseinzadeh, S.; Aronoff, L.; et al. Self-renewing resident cardiac macrophages limit adverse remodeling following myocardial infarction. Nat. Immunol. 2019, 20, 29–39. [Google Scholar] [CrossRef]
- van Hout, G.P.; Bosch, L.; Ellenbroek, G.H.; de Haan, J.J.; van Solinge, W.W.; Cooper, M.A.; Arslan, F.; de Jager, S.C.; Robertson, A.A.; Pasterkamp, G.; et al. The selective NLRP3-inflammasome inhibitor MCC950 reduces infarct size and preserves cardiac function in a pig model of myocardial infarction. Eur. Heart J. 2017, 38, 828–836. [Google Scholar] [CrossRef]
- Frangogiannis, N.G. The inflammatory response in myocardial injury, repair, and remodelling. Nat. Rev. Cardiol. 2014, 11, 255–265. [Google Scholar] [CrossRef]
- Tracey, K.J. Reflex control of immunity. Nat. Rev. Immunol. 2009, 9, 418–428. [Google Scholar] [CrossRef]
- Wang, H.; Yu, M.; Ochani, M.; Amelia, C.A.; Tanovic, M.; Susarla, S.; Li, J.H.; Wang, H.; Yang, N.; Ulloa, L.; et al. Nicotinic acetylcholine receptor α7 subunit is an essential regulator of inflammation. Nature 2003, 421, 384–388. [Google Scholar] [CrossRef]
- Borovikova, L.V.; Ivanova, S.; Zhang, M.; Yang, H.; Botchkina, G.I.; Watkins, L.R.; Wang, H.; Abumrad, N.; Eaton, J.W.; Tracey, K.J. Vagus nerve stimulation attenuates the systemic inflammatory response to endotoxin. Nature 2000, 405, 458–462. [Google Scholar] [CrossRef] [PubMed]
- Roy, A.; Fields, W.C.; Rocha-Resende, C.; Resende, R.R.; Guatimosim, S.; Prado, V.F.; Gros, R.; Prado, M.A. Cardiomyocyte-secreted acetylcholine is required for maintenance of homeostasis in the heart. FASEB J. 2013, 27, 5072–5082. [Google Scholar] [CrossRef] [PubMed]
- de Jonge, W.J.; Ulloa, L. The alpha7 nicotinic acetylcholine receptor as a pharmacological target for inflammation. Br. J. Pharmacol. 2007, 151, 915–929. [Google Scholar] [CrossRef]
- Ulleryd, M.A.; Mjornstedt, F.; Panagaki, D.; Yang, L.J.; Engevall, K.; Gutierrez, S.; Wang, Y.; Gan, L.M.; Nilsson, H.; Michaelsson, E.; et al. Stimulation of alpha 7 nicotinic acetylcholine receptor (α7nAChR) inhibits atherosclerosis via immunomodulatory effects on myeloid cells. Atherosclerosis 2019, 287, 122–133. [Google Scholar] [CrossRef]
- Li, H.; Zhang, Z.Z.; Zhan, J.; He, X.H.; Song, X.M.; Wang, Y.L. Protective effect of PNU-120596, a selective alpha7 nicotinic acetylcholine receptor-positive allosteric modulator, on myocardial ischemia-reperfusion injury in rats. J. Cardiovasc. Pharmacol. 2012, 59, 507–513. [Google Scholar] [CrossRef]
- Xiong, J.; Yuan, Y.J.; Xue, F.S.; Wang, Q.; Cheng, Y.; Li, R.P.; Liao, X.; Liu, J.H. Postconditioning with α7nAChR agonist attenuates systemic inflammatory response to myocardial ischemia—Reperfusion injury in rats. Inflammation 2012, 35, 1357–1364. [Google Scholar] [CrossRef]
- Fang, J.; Wang, J.; Chen, F.; Xu, Y.; Zhang, H.; Wang, Y. α7nAChR Deletion Aggravates Myocardial Infarction and Enhances Systemic Inflammatory Reaction via mTOR-Signaling-Related Autophagy. Inflammation 2019, 42, 1190–1202. [Google Scholar] [CrossRef]
- Walker, D.P.; Wishka, D.G.; Piotrowski, D.W.; Jia, S.; Reitz, S.C.; Yates, K.M.; Myers, J.K.; Vetman, T.N.; Margolis, B.J.; Jacobsen, E.J.; et al. Design, synthesis, structure-activity relationship, and in vivo activity of azabicyclic aryl amides as alpha7 nicotinic acetylcholine receptor agonists. Bioorg. Med. Chem. 2006, 14, 8219–8248. [Google Scholar] [CrossRef]
- Smith, C.J.; Zhang, Y.; Koboldt, C.M.; Muhammad, J.; Zweifel, B.S.; Shaffer, A.; Talley, J.J.; Masferrer, J.L.; Seibert, K.; Isakson, P.C. Pharmacological analysis of cyclooxygenase-1 in inflammation. Proc. Natl. Acad. Sci. USA 1998, 95, 13313–13318. [Google Scholar] [CrossRef]
- Hou, Z.; Zhou, Y.; Yang, H.; Liu, Y.; Mao, X.; Qin, X.; Li, X.; Zhang, X.; Hu, Y. Alpha7 nicotinic acetylcholine receptor activation protects against myocardial reperfusion injury through modulation of autophagy. Biochem. Biophys. Res. Commun. 2018, 500, 357–364. [Google Scholar] [CrossRef]
- Mavropoulos, S.A.; Khan, N.S.; Levy, A.C.; Faliks, B.T.; Sison, C.P.; Pavlov, V.A.; Zhang, Y.; Ojamaa, K. Nicotinic acetylcholine receptor-mediated protection of the rat heart exposed to ischemia reperfusion. Mol. Med. 2017, 23, 120–133. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Li, J.; Zhang, L.; Li, N.; Su, S.; Ye, Z.; Xu, Y. Decreased α7nAChR mRNA levels in peripheral blood monocytes are associated with enhanced inflammatory cytokine production in patients with lupus nephritis. Biomed. Pharmacother. 2019, 111, 359–366. [Google Scholar] [CrossRef] [PubMed]
- Lindsey, M.L.; Bolli, R.; Canty, J.M., Jr.; Du, X.J.; Frangogiannis, N.G.; Frantz, S.; Gourdie, R.G.; Holmes, J.W.; Jones, S.P.; Kloner, R.A.; et al. Guidelines for experimental models of myocardial ischemia and infarction. Am. J. Physiol. Heart Circ. Physiol. 2018, 314, H812–H838. [Google Scholar] [CrossRef] [PubMed]
- Lin, Z.H.; Li, Y.C.; Wu, S.J.; Zheng, C.; Lin, Y.Z.; Lian, H.; Lin, W.Q.; Lin, J.F. Eliciting α7-nAChR exerts cardioprotective effects on ischemic cardiomyopathy via activation of AMPK signalling. J. Cell. Mol. Med. 2019, 23, 4746–4758. [Google Scholar] [CrossRef] [PubMed]
- Romano, M.; Diomede, L.; Sironi, M.; Massimiliano, L.; Sottocorno, M.; Polentarutti, N.; Guglielmotti, A.; Albani, D.; Bruno, A.; Fruscella, P.; et al. Inhibition of monocyte chemotactic protein-1 sysnthesis by statins. Lab. Investig. 2000, 80, 1095–1100. [Google Scholar] [CrossRef] [PubMed]
- Cronstein, B.N.; Naime, D.; Ostad, E. The antiinflammatory mechanism of methotrexate: Increased adenosine release at inflamed sites diminishes leukocyte accumulation in an in vivo model of inflammation. J. Clin. Investig. 1993, 92, 2675–2682. [Google Scholar] [CrossRef] [PubMed]
- Edwards, J.C.; Sedgwick, A.D.; Willoughby, D.A. The formation of a structure with the features of synovial lining by subcutaneous injection of air: An in vivo tissue culture system. J. Pathol. 1981, 134, 147–156. [Google Scholar] [CrossRef] [PubMed]
- Sawant, K.V.; Sepuru, K.M.; Penaranda, B.; Lowry, E.; Garofalo, R.P.; Rajarathnam, K. Chemokine Cxcl1-Cxcl2 heterodimer is a potent neutrophil chemoattractant. J. Leukoc. Biol. 2023, 114, 666–671. [Google Scholar] [CrossRef] [PubMed]
- David, B.A.; Kubes, P. Exploring the complex role of chemokines and chemoattractants in vivo on leukocyte dynamics. Immunol. Rev. 2019, 289, 9–30. [Google Scholar] [CrossRef] [PubMed]
- Mardani, I.; Tomas Dalen, K.; Drevinge, C.; Miljanovic, A.; Ståhlman, M.; Klevstig, M.; Scharin Täng, M.; Fogelstrand, P.; Levin, M.; Ekstrand, M.; et al. Plin2-deficiency reduces lipophagy and results in increased lipid accumulation in the heart. Sci. Rep. 2019, 9, 6909. [Google Scholar] [CrossRef] [PubMed]
- Pattanaik, B.; Hammarlund, M.; Mjörnstedt, F.; Ulleryd, M.A.; Zhong, W.; Uhlén, M.; Gummesson, A.; Bergström, G.; Johansson, M.E. Polymorphisms in alpha 7 nicotinic acetylcholine receptor gene, CHRNA7, and its partially duplicated gene, CHRFAM7A, associate with increased inflammatory response in human peripheral mononuclear cells. FASEB J. 2022, 36, e22271. [Google Scholar] [CrossRef]
- Drevinge, C.; Dalen, K.T.; Mannila, M.N.; Täng, M.S.; Ståhlman, M.; Klevstig, M.; Lundqvist, A.; Mardani, I.; Haugen, F.; Fogelstrand, P.; et al. Perilipin 5 is protective in the ischemic heart. Int. J. Cardiol. 2016, 219, 446–454. [Google Scholar] [CrossRef]
- Zhang, Y.; Takagawa, J.; Sievers, R.E.; Khan, M.F.; Viswanathan, M.N.; Springer, M.L.; Foster, E.; Yeghiazarians, Y. Validation of the wall motion score and myocardial performance indexes as novel techniques to assess cardiac function in mice after myocardial infarction. Am. J. Physiol. Heart Circ. Physiol. 2007, 292, H1187–H1192. [Google Scholar] [CrossRef]
- Claycomb, W.C.; Lanson, N.A., Jr.; Stallworth, B.S.; Egeland, D.B.; Delcarpio, J.B.; Bahinski, A.; Izzo, N.J., Jr. HL-1 cells: A cardiac muscle cell line that contracts and retains phenotypic characteristics of the adult cardiomyocyte. Proc. Natl. Acad. Sci. USA 1998, 95, 2979–2984. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| 24 h Post MI | One Week Post MI | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Control | PHA | Sham Control | Sham PHA | p | Control | PHA | Sham Control | Sham PHA | p | |
| n | 13 | 13 | 3 | 3 | 13 | 13 | 3 | 3 | ||
| BW, g | 24.2 ± 2.5 | 23.5 ± 2.5 | 23.8 ± 2.2 | 21.2 ± 1.9 | 0.52 | 25.1 ± 2.7 | 24.6 ± 2.6 | 24.9 ± 2.2 | 23.7 ± 2.8 | 0.65 |
| HR, bpm | 437 ± 55 | 440 ± 50 | 453 ± 24 | 394 ± 79 | 0.92 | 435 ± 51 | 421 ± 39 | 464 ± 54 | 365 ± 49 | 0.51 |
| SV, μL | 27.2 ± 4.6 | 27.1 ± 4 | 29.1 ± 2.1 | 31.9 ± 1.9 | >0.99 | 33.4 ± 4.4 | 33.5 ± 5.4 | 34.3 ± 4 | 33.4 ± 8.9 | 0.92 |
| FS, % | 8.4 ± 4.8 | 10.8 ± 3.9 | 18.4 ± 5.9 | 10.7 ± 5.6 | 0.22 | 11.7 ± 6 | 11.5 ± 4.2 | 16.9 ± 7.3 | 13.1 ± 7.1 | 0.96 |
| FAC, % | 50.6 ± 8.2 | 55.9 ± 11.2 | 66.8 ± 6.3 | 53.9 ± 22.3 | 0.08 | 55.7 ± 9.8 | 56.4 ± 11.8 | 69 ± 8.5 | 52.1 ± 10.3 | 0.92 |
| LV V(d), μL | 50.3 ± 8.1 | 45.6 ± 8.7 | 41.8 ± 1.1 | 55.1 ± 11.2 | 0.13 | 55.0 ± 10 | 56.1 ± 12.7 | 47.8 ± 0.5 | 57.1 ± 8.1 | 0.92 |
| LV V(s), μL | 23.1 ± 7.7 | 18.5 ± 7.2 | 12.6 ± 3.1 | 23.2 ± 13.2 | 0.06 | 21.6 ± 8.7 | 22.5 ± 9.6 | 13.5 ± 3.5 | 23.8 ± 7.9 | 0.80 |
| WBC, ×109/L | NA | NA | NA | NA | 3.7 ± 1.3 | 3.2 ± 1.1 | 5.1 ± 0.6 | 4.3 ± 0.1 | 0.38 | |
| Lym, ×109/L | NA | NA | NA | NA | 1.6 ± 0.7 | 1.8 ± 0.5 | 3.3 ± 0.8 | 2.6 ± 0.2 | 0.58 | |
| Gran, ×109/L | NA | NA | NA | NA | 1.9 ± 1.3 | 1.3 ± 1 | 1.7 ± 0.5 | 1.4 ± 0.3 | 0.19 | |
| Mon, ×109/L | NA | NA | NA | NA | 0.2 ± 0.2 | 0.2 ± 0.1 | 0.2 ± 0.2 | 0.3 ± 0.04 | 0.18 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mjörnstedt, F.; Miljanovic, A.; Wilhelmsson, R.; Levin, M.; Johansson, M.E. Alpha 7 Nicotinic Acetylcholine Receptor Agonist PHA 568487 Reduces Acute Inflammation but Does Not Affect Cardiac Function or Myocardial Infarct Size in the Permanent Occlusion Model. Int. J. Mol. Sci. 2024, 25, 4414. https://doi.org/10.3390/ijms25084414
Mjörnstedt F, Miljanovic A, Wilhelmsson R, Levin M, Johansson ME. Alpha 7 Nicotinic Acetylcholine Receptor Agonist PHA 568487 Reduces Acute Inflammation but Does Not Affect Cardiac Function or Myocardial Infarct Size in the Permanent Occlusion Model. International Journal of Molecular Sciences. 2024; 25(8):4414. https://doi.org/10.3390/ijms25084414
Chicago/Turabian StyleMjörnstedt, Filip, Azra Miljanovic, Rebecka Wilhelmsson, Malin Levin, and Maria E. Johansson. 2024. "Alpha 7 Nicotinic Acetylcholine Receptor Agonist PHA 568487 Reduces Acute Inflammation but Does Not Affect Cardiac Function or Myocardial Infarct Size in the Permanent Occlusion Model" International Journal of Molecular Sciences 25, no. 8: 4414. https://doi.org/10.3390/ijms25084414
APA StyleMjörnstedt, F., Miljanovic, A., Wilhelmsson, R., Levin, M., & Johansson, M. E. (2024). Alpha 7 Nicotinic Acetylcholine Receptor Agonist PHA 568487 Reduces Acute Inflammation but Does Not Affect Cardiac Function or Myocardial Infarct Size in the Permanent Occlusion Model. International Journal of Molecular Sciences, 25(8), 4414. https://doi.org/10.3390/ijms25084414