

Redox Homeostasis Alteration Is Restored through Melatonin Treatment in COVID-19 Patients: A Preliminary Study
 , , ,
, , ,
Abstract
:1. Introduction
2. Results
2.1. Demographic Characteristics of the COVID-19 Patients
2.2. Blood Biochemical Characteristics of the Healthy Subjects
2.3. Activities of the Enzymes That Use Glutathione
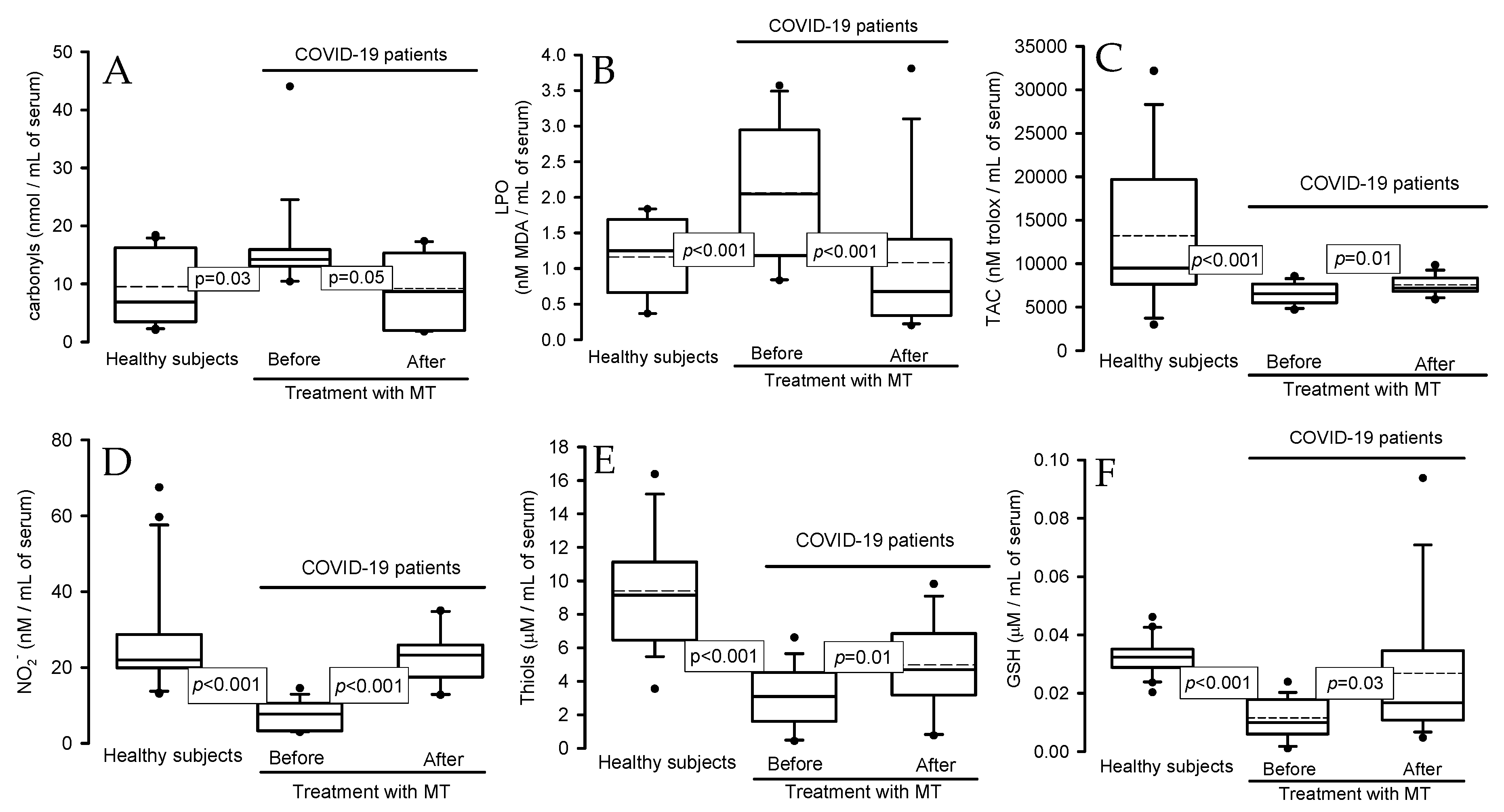
2.4. Oxidative Stress Markers
2.5. Activities of Enzymes: Peroxidases and ecSOD in Native Gels
2.6. Electron Microscopy
3. Discussion
4. Materials and Methods
4.1. Population That Comprised the Study
4.2. Detection of SARS-CoV-2 via Real-Time Reverse Transcriptase Polymerase Chain Reaction
4.3. Healthy Subjects
4.4. Therapeutic Management
4.5. Peripheral Blood Samples
4.6. Oxidative Stress Markers
4.6.1. Carbonyl Proteins
4.6.2. Evaluation of Total Antioxidant Capacity
4.6.3. Determination of the Lipid Peroxidation Marker
4.6.4. Nitrite Determination
4.6.5. Thiol and Glutathione Levels
4.6.6. Determinations of Antioxidant Enzymes That Use GSH
4.6.7. Interleukin-6 Concentration
4.6.8. Obtainment of the Postmortem Biopsies
4.6.9. Immune Colloidal Gold Technique
4.7. Statistical Analysis
5. Conclusions
5.1. Perspectives
5.2. Study Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Soto, M.E.; Guarner-Lans, V.; Soria-Castro, E.; Manzano-Pech, L.; Pérez-Torres, I. Is antioxidant therapy a useful complementary measure for COVID-19 treatment? An algorithm for its application. Medicina 2020, 56, 386–415. [Google Scholar] [CrossRef] [PubMed]
- Soria-Castro, E.; Soto, M.E.; Guarner-Lans, V.; Rojas, G.; Perezpeña-Diazconti, M.; Críales-Vera, S.A.; Manzano-Pech, L.; Pérez-Torres, I. The kidnapping of mitochondrial function associated with the SARS-CoV-2 infection. Histol. Histopathol. 2021, 36, 947–965. [Google Scholar] [PubMed]
- Zhang, D.; Kukkar, D.; Kim, K.H.; Bhatt, P. A comprehensive review on immunogen and immune-response proteins of SARS-CoV-2 and their applications in prevention, diagnosis, and treatment of COVID-19. Int. J. Biol. Macromol. 2024, 259, 129284. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Torres, I.; Guarner-Lans, V.; Soria-Castro, E.; Manzano-Pech, L.; Palacios-Chavarría, A.; Valdez-Vázquez, R.R.; Domínguez-Cherit, J.G.; Herrera-Bello, H.; Castillejos-Suastegui, H.; Moreno-Castañeda, L.; et al. Alteration in the lipid profile and the desaturases activity in patients with severe pneumonia by SARS-CoV-2. Front. Physiol. 2021, 12, 667024. [Google Scholar] [CrossRef] [PubMed]
- Negru, P.A.; Radu, A.F.; Vesa, C.M.; Behl, T.; Abdel-Daim, M.M.; Nechifor, A.C.; Endres, L.; Stoicescu, M.; Pasca, B.; Tit, D.M.; et al. Therapeutic dilemmas in addressing SARS-CoV-2 infection: Favipiravir versus Remdesivir. Biomed. Pharmacother. 2022, 147, 112700. [Google Scholar] [CrossRef] [PubMed]
- Molina-Carballo, A.; Palacios-López, R.; Jerez-Calero, A.; Augustín-Morales, M.C.; Agil, A.; Muñoz-Hoyos, A.; Muñoz-Gallego, A. Protective effect of melatonin administration against SARS-CoV-2 infection: A systematic review. Curr. Issues. Mol. Biol. 2022, 44, 31–45. [Google Scholar] [CrossRef] [PubMed]
- Boutin, J.A.; Liberelle, M.; Yous, S.; Ferry, G.; Nepveu, F. Melatonin facts: Lack of evidence that melatonin is a radical scavenger in living systems. J. Pineal. Res. 2023, 76, e12926. [Google Scholar] [CrossRef] [PubMed]
- Reppert, S.M. Melatonin receptors: Molecular biology of a new family of G protein-coupled receptors. J. Biol. Rhythm. 1997, 12, 528–531. [Google Scholar] [CrossRef] [PubMed]
- Mehrzadi, S.; Karimi, M.Y.; Fatemi, A.; Reiter, R.J.; Hosseinzadeh, A. SARS-CoV-2 and other coronaviruses negatively influence mitochondrial quality control: Beneficial effects of melatonin. Pharmacol. Ther. 2021, 224, 107825. [Google Scholar] [CrossRef]
- Pontes, G.N.; Cardoso, E.C.; Carneiro-Sampaio, M.M.; Markus, R.P. Pineal melatonin and the innate immune response: The TNF-alpha increase after cesarean section suppresses nocturnal melatonin production. J. Pineal. Res. 2007, 43, 365–371. [Google Scholar] [CrossRef]
- Markus, R.P.; Fernandes, P.A.; Kinker, G.S.; da Silveira, C.M.S.; Marçola, M. Immune-pineal axis—Acute inflammatory responses coordinate melatonin synthesis by pinealocytes and phagocytes. Br. J. Pharmacol. 2018, 175, 3239–3250. [Google Scholar] [CrossRef]
- Pablos, M.I.; Guerrero, J.M.; Ortiz, G.G.; Agapito, M.T.; Reiter, R.J. Both melatonin and a putative nuclear melatonin receptor agonist CGP 52608 stimulate glutathione peroxidase and glutathione reductase activities in mouse brain in vivo. Neuroendocrinol. Lett. 1997, 18, 49–58. [Google Scholar]
- Terron, M.P.; Flores, L.J.; Czarnocki, Z. Melatonin and its metabolites: New findings regarding their production and their radical scavenging actions. Acta. Biochim. Pol. 2007, 54, 1–9. [Google Scholar]
- Gulcin, I.; Buyukokuroglu, M.E.; Kufrevioglu, O.I. Metal chelating and hydrogen peroxide scavenging effects of melatonin. J. Pineal. Res. 2003, 34, 278–281. [Google Scholar] [CrossRef] [PubMed]
- Galano, A.; Tan, D.X.; Reiter, R.J. Melatonin and related compounds: Chemical insights into their protective effects against oxidative stress. Curr. Org. Chem. 2017, 21, 2077–2095. [Google Scholar] [CrossRef]
- Yao, Y.; Zhu, W.; Han, D.; Shi, X.; Xu, S. New insights into how melatonin ameliorates bisphenol A-induced colon damage: Inhibition of NADPH oxidase. J. Agric. Food. Chem. 2023, 71, 2566–2578. [Google Scholar] [CrossRef] [PubMed]
- Hardeland, R. Antioxidant protection by melatonin: Multiplicity of mechanisms from radical detoxification to radical avoidance. Endocrine. 2005, 27, 119–130. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.M.; Zhang, Y. Melatonin: A well-documented antioxidant with conditional pro-oxidant actions. J. Pineal. Res. 2014, 57, 131–146. [Google Scholar] [CrossRef] [PubMed]
- Budkowska, M.; Cecerska-Heryć, E.; Marcinowska, Z.; Siennicka, A.; Dołęgowska, B. The influence of circadian rhythm on the activity of oxidative stress enzymes. Int. J. Mol. Sci. 2022, 23, 14275. [Google Scholar] [CrossRef]
- Soto, M.E.; Guarner-Lans, V.; Díaz-Díaz, E.; Manzano-Pech, L.; Palacios-Chavarría, A.; Valdez-Vázquez, R.R.; Aisa-Álvarez, A.; Saucedo-Orozco, H.; Pérez-Torres, I. Hyperglycemia and loss of redox homeostasis in COVID-19 Patients. Cells. 2022, 11, 932. [Google Scholar] [CrossRef]
- Nakao, T.; Morita, H.; Maemura, K.; Amiya, E.; Inajima, T.; Saito, Y.; Watanabe, M.; Manabe, I.; Kurabayashi, M.; Nagai, R.; et al. Melatonin ameliorates Angiotensin II-induced vascular endothelial damage via its antioxidative properties. J. Pineal. Res. 2013, 55, 287–293. [Google Scholar] [CrossRef]
- Feitosa, E.L.; Júnior, F.T.D.S.S.; NeryNeto, J.A.O.; Matos, L.F.L.; Moura, M.H.S.; Rosales, T.O.; De Freitas, G.B.L. COVID-19: Rational discovery of the therapeutic potential of melatonin as a SARS-CoV-2 main protease inhibitor. Int. J. Med. Sci. 2020, 17, 2133–2146. [Google Scholar] [CrossRef] [PubMed]
- Boga, J.A.; Coto-Montes, A.; Rosales-Corral, S.A.; Tan, D.X.; Reiter, R.J. Beneficial actions of melatonin in the management of viral infections: A new use for this molecular handyman. Rev. Med. Virol. 2012, 22, 323–338. [Google Scholar] [CrossRef]
- Anderson, G.; Reiter, R.J. Melatonin: Roles in influenza, COVID-19, and other viral infections. Rev. Med. Virol. 2020, 30, e2109. [Google Scholar] [CrossRef]
- Bahrampour, J.K.; Pourhanifeh, M.H.; Hosseinzadeh, A.; Hemati, K.; Mehrzadi, S. Melatonin potentials against viral infections including COVID-19: Current evidence and new findings. Virus. Res. 2020, 287, 198108. [Google Scholar] [CrossRef]
- Soto, M.E.; Manzano-Pech, L.; Palacios-Chavarría, A.; Valdez-Vázquez, R.R.; Guarner-Lans, V.; Pérez-Torres, I. N-acetyl cysteine restores the diminished activity of the antioxidant enzymatic system caused by SARS-CoV-2 infection: Preliminary findings. Pharmaceuticals 2023, 16, 591. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, C.; Mayo, J.C.; Sainz, R.M.; Antolín, I.; Herrera, F. Regulation of antioxidant enzymes: A significant role for melatonin. J. Pineal. Res. 2004, 36, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Öztürk, G.; Akbulut, G.K.; Güney, S.; Acuna-Castroviejo, D. Age-related changes in the rat brain mitochondrial antioxidative enzyme ratios: Modulation by melatonin. Exp. Gerontol. 2012, 47, 706–711. [Google Scholar] [CrossRef]
- Sezgin, G.; Özturk, G.; Güney, S.; Sinanoğlu, O.; Tunçdemir, M. Protective effect of melatonin and 1,25-dihydroxyvitamin D3 on renal ischemia-reperfusion injury in rats. Ren. Fail. 2013, 35, 374–379. [Google Scholar] [CrossRef]
- Crespo, I.; Miguel, B.S.; Laliena, A.; Alvarez, M.; Culebras, J.M.; González-Gallego, J.; Tuñón, M.J. Melatonin prevents the decreased activity of antioxidant enzymes and activates nuclear erythroid 2-related factor 2 signaling in an animal model of fulminant hepatic failure of viral origin. J. Pineal. Res. 2010, 49, 193–200. [Google Scholar] [CrossRef]
- Muhammad, Y.; Kani, Y.A.; Iliya, S.; Muhammad, J.B.; Binji, A.; El-Fulaty, A.A.; Kabir, M.B.; Bindawa, K.U.; Ahmed, A. Deficiency of antioxidants and increased oxidative stress in COVID-19 patients: A cross-sectional comparative study in Jigawa, Northwestern Nigeria. SAGE. Open. Med. 2021, 9, 2050312121991246. [Google Scholar] [CrossRef] [PubMed]
- Tang, D.; Comish, P.; Kang, R. The hallmarks of COVID-19 disease. PLoS. Pathog. 2020, 16, e1008536. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Kim, C.H.; Ryu, J.H.; Kim, M.J.; Park, C.Y.; Lee, J.M.; Holtzman, M.J.; Joo-Heon, Y. Reactive oxygen species induce antiviral innate immune response through IFN-lambda regulation in human nasal epithelial cells. Am. J. Respir. Cell. Mol. Biol. 2013, 49, 855–865. [Google Scholar] [CrossRef] [PubMed]
- Vlasova, I.I. Peroxidase activity of human hemoproteins: Keeping the fire under control. Molecules. 2018, 23, 2561. [Google Scholar] [CrossRef] [PubMed]
- Cao, Z.; Cheng, G. Recombinant myeloperoxidase as a New class of antimicrobial agents. Microbiol. Spectr. 2022, 10, e0052221. [Google Scholar] [CrossRef] [PubMed]
- Camp, O.G.; Bai, D.; Gonullu, D.C.; Nayak, N.; Abu-Soud, H.M. Melatonin interferes with COVID-19 at several distinct ROS-related steps. J. Inorg. Biochem. 2021, 223, 111546. [Google Scholar] [CrossRef] [PubMed]
- Goud, P.T.; Bai, D.; Abu-Soud, H.M. A Multiple-hit hypothesis involving reactive oxygen species and myeloperoxidase explains clinical deterioration and fatality in COVID-19. Int. J. Biol. Sci. 2021, 17, 62–72. [Google Scholar] [CrossRef] [PubMed]
- Abu-Soud, H.M.; Hazen, S.L. Nitric oxide is a physiological substrate for mammalian peroxidases. J. Biol. Chem. 2000, 275, 37524–37532. [Google Scholar] [CrossRef] [PubMed]
- Yamasaki, H. Blood nitrate and nitrite modulating nitric oxide bioavailability: Potential therapeutic functions in COVID-19. Nitric. Oxide. 2020, 103, 29–30. [Google Scholar] [CrossRef]
- Kouhpayeh, S.; Shariati, L.; Boshtam, M.; Rahimmanesh, I.; Mirian, M.; Esmaeili, Y.; Najaflu, M.; Khanahmad, N.; Zeinalian, M.; Trovato, M.; et al. The molecular basis of COVID-19 pathogenesis, conventional and nanomedicine therapy. Int. J. Mol. Sci. 2021, 22, 5438. [Google Scholar] [CrossRef]
- Wang, J.; Mei, F.; Bai, L.; Zhou, S.; Liu, D.; Yao, L.; Ahluwalia, A.; Ghiladi, R.A.; Su, L.; Shu, T.; et al. Serum nitrite and nitrate: A potential biomarker for post-COVID-19 complications? Free Radic. Biol. Med. 2021, 175, 216–225. [Google Scholar] [CrossRef] [PubMed]
- Corrao, S.; Bocchio, M.R.; Monaco, M.L.; Natoli, G.; Cavezzi, A.; Troiani, E.; Argano, C. Does evidence exist to blunt inflammatory response by nutraceutical supplementation during COVID-19 pandemic? An overview of systematic reviews of vitamin D, vitamin C, melatonin, and Zinc. Nutrients 2021, 13, 1261. [Google Scholar] [CrossRef] [PubMed]
- Ghaleh, H.E.G.; Hosseini, A.; Aghamollaei, H.; Fasihi-Ramandi, M.; Alishiri, G.; Saeedi-Boroujeni, A.; Hassanpour, K.; Mahmoudian-Sani, M.R.; Farnoosh, G. NLRP3 inflammasome activation and oxidative stress status in the mild and moderate SARS-CoV-2 infected patients: Impact of melatonin as a medicinal supplement. Z. Naturforsch. C J. Biosci. 2022, 77, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Zarezadeh, M.; Khorshidi, M.; Emami, M.; Janmohammadi, P.; Kord-Varkaneh, H.; Mousavi, S.M.; Mohammed, S.H.; Saedisomeolia, A.; Alizadeh, S. Melatonin supplementation and pro-inflammatory mediators: A systematic review and meta-analysis of clinical trials. Eur. J. Nutr. 2020, 59, 1803–1813. [Google Scholar] [CrossRef] [PubMed]
- Farnoosh, G.; Akbariqomi, M.; Badri, T.; Bagheri, M.; Izadi, M.; Saeedi-Boroujeni, A.; Rezaie, E.; Ghaleh, H.E.G.; Aghamollaei, H.; Fasihi-Ramandi, M.; et al. Efficacy of a low dose of melatonin as an adjunctive therapy in hospitalized patients with COVID-19: A randomized, double-blind clinical Trial. Arch. Med. Res. 2021, 53, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Alizadeh, N.; Dianatkhah, M.; Alimohamadi, Y.; Moradi, H.; Akbarpour, S.; Akrami, M.; Mansouri, F.; Faraji, N.; Rezaie, Z.; Alizadeh, M.; et al. High dose melatonin as an adjuvant therapy in intubated patients with COVID-19: A randomized clinical trial. J. Taibah Univ. Med. Sci. 2022, 17, 454–460. [Google Scholar] [CrossRef] [PubMed]
- Cardinali, D.P.; Brown, G.M.; Pandi-Perumal, S.R. Can Melatonin be a potential “Silver Bullet” in treating COVID-19 patients? Diseases 2020, 8, 44. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.M.; Zhao, C.C.; Xie, Q.M.; Xu, J.; Fei, G.H. TLR2-melatonin feedback loop regulates the activation of NLRP3 inflammasome in murine allergic airway inflammation. Front. Immunol. 2020, 11, 172. [Google Scholar] [CrossRef] [PubMed]
- Serdengeçti, N.; Tarakçıoğlu, M.C. COVID-19-related brief insomnia in a 13-year-old adolescent girl. Sleep. Sci. 2024, 17, e112–e114. [Google Scholar] [CrossRef]
- Taha, M.A.; Abdelkader, S.A.S.; Hossam-Eldin, M.M.; El-Tawab, M.W.; Al-Hejazi, T.; Mousa, Y.; Sharma, R.; Reiter, R.J. Safety and efficacy of melatonin as an adjuvant therapy in COVID-19 patients: Systematic review and meta-analysis. Adv. Med. Sci. 2023, 68, 341–352. [Google Scholar] [CrossRef]
- Mahjoub, L.; Youssef, R.; Yaakoubi, H.; Salah, H.B.; Jaballah, R.; Mejri, M.; Sekma, A.; Trabelsi, I.; Nouira, S.; Khrouf, M.; et al. Melatonin, vitamins and minerals supplements for the treatment of COVID-19 and Covid-like illness: A prospective, randomized, double-blind multicenter study. Explore 2024, 20, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Abbas-Mousavi, S.; Heydari, K.; Mehravaran, H.; Saeedi, M.; Alizadeh-Navaei, R.; Hedayatizadeh-Omran, A.; Amir Shamshirian, A. Melatonin effects on sleep quality and outcomes of COVID-19 patients: An open-label, randomized, controlled trial. J. Med. Virol. 2022, 94, 263–271. [Google Scholar] [CrossRef]
- Hasan, Z.T.; Atrakji, M.Q.Y.M.A.A.; Mehuaiden, K.A. The effect of melatonin on thrombosis, sepsis and mortality rate in COVID-19 patients. Int. J. Infect. Dis. 2022, 114, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Alizadeh, Z.; Keyhanian, N.; Ghaderkhani, S.; Dashti-Khavidaki, S.; Shoormasti, R.S.; Pourpak, Z. A pilot study on controlling coronavirus disease 2019 (COVID-19) inflammation using melatonin supplement. Iran. J. Allergy. Asthma. Immunol. 2021, 20, 494–499. [Google Scholar] [CrossRef] [PubMed]
- Hasan, Z.; Al-Atrakji, M.; Alsaaty, M.; Abdulnafa, Z.; Mehuaiden, A. The effect of melatonin on C-reactive protein, serum ferritin and D-dimer in COVID-19 patients. Int. J. Drug. Delivery. Technol. 2022, 12, 108–112. [Google Scholar] [CrossRef]
- Ameri, A.; Asadi, F.; Ziaei, A.; Vatankhah, M.; Safa, O.; Kamali, M.; Fathalipour, M.; Mahmoodi, M.; Hassanipour, S. Efficacy and safety of oral melatonin in patients with severe COVID-19: A randomized controlled trial. Inflammopharmacology 2023, 1, 265–274. [Google Scholar] [CrossRef] [PubMed]
- Fogleman, C.; Cohen, D.; Mercier, A.; Farrell, D.; Rutz, J.; Bresz, K.; Vernon, T. A pilot of a randomized control trial of melatonin and vitamin C for mild-to-moderate COVID-19. J. Am. Board. Fam. Med. 2022, 35, 695–707. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Rico, M.; de la Muela, P.; Herrera-Morueco, J.J.; Geoffroy, P.A.; Limosin, F.; Hoertel, N. Melatonin does not reduce mortality in adult hospitalized patients with COVID-19: A multicenter retrospective observational study. J. Travel. Med. 2022, 29, taab195. [Google Scholar] [CrossRef] [PubMed]
- Bologna, C.; Madonna, P.; Pone, E. Efficacy of prolonged-release melatonin 2 mg (PRM 2 mg) prescribed for insomnia in hospitalized patients for COVID-19: A retrospective observational study. J. Clin. Med. 2021, 10, 5857. [Google Scholar] [CrossRef]
- Hosseini, A.; Ghaleh, H.E.; Aghamollaei, H.; Ramandi, M.F.; Alishiri, G.; Shahriary, A.; Hassanpour, K.; Tat, M.; Farnoosh, G. Evaluation of Th1 and Th2 mediated cellular and humoral immunity in patients with COVID-19 following the use of melatonin as an adjunctive treatment. Eur. J. Pharmacol. 2021, 904, 174193. [Google Scholar] [CrossRef]
- Owino, S.; Buonfiglio, D.D.C.; Tchio, C.; Tosini, G. Melatonin signaling a key regulator of glucose homeostasis and energy metabolism. Front. Endocrinol. 2019, 10, 488. [Google Scholar] [CrossRef] [PubMed]
- Reiter, R.J.; Sharma, R.; Rosales-Corral, S. Anti-Warburg effect of melatonin: A proposed mechanism to explain its inhibition of multiple diseases. Int. J. Mol. Sci. 2021, 22, 764. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Pastora, J.; Weigand, M.; Kim, J.; Wu, X.; Strayer, J.; Palmer, A.F.; Zborowski, M.; Yazer, M.; Chalmers, J.J. Hyperferritinemia in critically ill COVID-19 patients—Is ferritin the product of inflammation or a pathogenic mediator? Clin. Chim. Acta. 2020, 509, 249–251. [Google Scholar] [CrossRef] [PubMed]
- Sayed, R.K.; Fernández-Ortiz, M.; Diaz-Casado, M.E.; Rusanova, I.; Rahim, I.; Escames, G.; López, L.C.; Mokhtar, D.M.; Acuña-Castroviejo, D. The protective effect of melatonin against age-associated, sarcopenia-dependent tubular aggregate formation, lactate depletion, and mitochondrial changes. J. Gerontol. A Biol. Sci. Med. Sci. 2018, 73, 1330–1338. [Google Scholar] [CrossRef] [PubMed]
- Tan, D.X.; Manchester, L.C.; Esteban-Zubero, E.; Zhou, Z.; Reiter, R.J. Melatonin as a potent and inducible endogenous antioxidant: Synthesis and metabolism. Molecules 2015, 20, 18886–18906. [Google Scholar] [CrossRef]
- Tarocco, A.; Caroccia, N.; Morciano, G.; Wieckowski, M.R.; Ancora, G.; Garani, G.; Pinton, P. Melatonin as a master regulator of cell death and inflammation: Molecular mechanisms and clinical implications for newborn care. Cell Death. Dis. 2019, 10, 317. [Google Scholar] [CrossRef]
- Ramos, E.; López-Muñoz, F.; Gil-Martín, E.; Egea, J.; Álvarez-Merz, I.; Painuli, S.; Semwal, P.; Martins, N.; Hernández-Guijo, J.M.; Romero, A. The coronavirus disease 2019 (COVID-19): Key emphasis on melatonin safety and therapeutic efficacy. Antioxidants 2021, 10, 1152. [Google Scholar] [CrossRef]
- Olson, G.; Andrew, M.D. Diagnosis and treatment of adults with community-acquired pneumonia. JAMA 2020, 323, 885–886. [Google Scholar] [CrossRef]
- Lambden, S.; Laterre, P.F.; Levy, M.M.; Francois, B. The SOFA score-development, utility, and challenges of accurate assessment in clinical trials. Crit. Care 2019, 23, 374. [Google Scholar] [CrossRef]
- Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E. Acute respiratory distress syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar]
- Chavarría, A.P.; Vázquez, R.R.V.; Cherit, J.G.D.; Bello, H.H.; Suastegui, H.C.; Moreno-Castañeda, L.; Estrada, A.G.; Hernández, F.; González-Marcos, O.; Saucedo-Orozco, H.; et al. Antioxidants and pentoxifylline as coadjuvant measures to standard therapy to improve prognosis of patients with pneumonia by COVID-19. Comput. Struct. Biotechnol. J. 2021, 19, 1379–1390. [Google Scholar] [CrossRef] [PubMed]
- Brower, R.G.; Lanken, P.N.; MacIntyre, N.; Matthay, M.A.; Morris, A.; Marek, A. National heart, lung, and blood institute ARDS clinical trials network higher versus lower positive end-expiratory pressures in patients with the acute respiratory distress syndrome. N. Engl. J. Med. 2004, 351, 327–336. [Google Scholar] [PubMed]
- Thachil, J.; Tang, N.; Gando, S.; Falanga, A.; Cattaneo, M.; Levi, M. ISTH interim guidance on recognition and management of coagulopathy in COVID-19. J. Thromb. Haemost. 2020, 18, 1023–1026. [Google Scholar] [CrossRef] [PubMed]
- Guimarães, H.P.; Timerman, S.; Rodrigues, R.D.R.; Corrêa, T.D.; Schubert, D.U.C.; Freitas, A.P. Position statement: Cardiopulmonary resuscitation of patients with confirmed or suspected COVID-19-2020. Arq. Bras. Cardiol. 2020, 114, 1078–1087. [Google Scholar] [CrossRef] [PubMed]
- Soto, M.E.; Pérez-Torres, I.; Manzano-Pech, L.; Soria-Castro, E.; Morales-Marín, A.; Ramírez-Marroquín, E.S.; Martínez-Hernández, H.; Herrera-Alarcón, V.; Guarner-Lans, V. Reduced levels of selenium and thioredoxin reductase in the thoracic aorta could contribute to aneurysm formation in patients with Marfan syndrome. Int. J. Mol. Sci. 2023, 24, 10429. [Google Scholar] [CrossRef]
- Erel, O.; Neşelioğlu, S.; Tunçay, M.E.; Oğuz, E.F.; Eren, F.; Akkuş, M.S.; Güner, H.R.; Ateş, İ. A sensitive indicator for the severity of COVID-19: Thiol. Turk. J. Med. Sci. 2021, 51, 921–928. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Median and Min–Max Range |
|---|---|
| Age years | 62 (34–84) |
| Body mass index | 30 (20–37) |
| Comorbidities (%) | |
| Diabetes Mellitus | 11 (65) |
| Hypertension | 7 (41) |
| Dyslipidemia | 10 (59) |
| Chronic obstructive pulmonary disease | 1 (6) |
| Normal Weight | 6 (35) |
| Overweight | 3 (18) |
| Obesity | 8 (47) |
| Gasometry and blood biochemistry median and min–max range | |
| PaO2 (mmHg) | 79 (58–152) |
| PCO2 (mmHg) | 31 (27–36) |
| PaO2/FiO2 (mmHg) | 145 (49–243) |
| SPO2/FiO2 (mmHg) | 160 (50–280) |
| Heart Rate bpm | 84 (58–106) |
| Mean arterial pressure (mmHg) | 82 (65–99) |
| Temperature °C | 36.5 (35.9–37.2) |
| Creatinine in serum mg/dL | 0.80 (0.60–2.5) |
| Blood urea nitrogen mg/dL | 18.6 (5.8–77.7) |
| Leukocytes 103/µL | 10.1 (5.3–22.6) |
| Lymphocytes 103/µL | 0.66 (0.39–1.29) |
| Platelets 103/µL | 275 (180–576) |
| Ferritin ng/mL | 665.7 (175–2354) |
| D-dimer ng/dL | 655 (27–35,200) |
| C-reactive protein mg/dL | 145 (37–308) |
| Procalcitonin ng/dL | 0.40 (0.06–34.7) |
| Score median and Min–Max range | |
| SOFA | 2 (1–8) |
| APACHE | 5 (4–7) |
| SAPS | 26.5 (13–31) |
| Days with mechanic ventilation | 2 (1–2) |
| Days in ICU | 14.5 (6–20) |
| Variable | Before Q1, Q2, Q3 | After Q1, Q2, Q3 |
|---|---|---|
| Glucose (mg/dL) | 157.8, 204.3, 266.6 * | 100.8, 139.4, 227.1 |
| Insulin (ng/mL) | 0.7, 1.30, 2.0 | 0.4, 1.3, 2.5 |
| HOMA index | 5.8, 9.7, 20.4 | 4.7, 8.6, 23.2 |
| IL-6 (pg/mL) | 16.2, 43.2, 84.1 ** | 7.8, 7.8, 22.0 |
| HDL (mg/dL) | 23.8, 29.0, 42.1 † | 29.3, 35.3, 40.0 |
| LDL (mg/dL) | 51.6, 62.5, 80.2 | 54.1, 86.1, 86.8 |
| Total cholesterol (mg/dL) | 23, 141, 162 | 100, 146, 160 |
| TG (mg/dL) | 96, 140, 185 | 178, 205, 742 |
| Gender | 15 Men, 5 Female |
|---|---|
| Variable | Q1, Q2, Q3 |
| Age | 49.0, 60.0, 63.2 |
| Glucose (mg/dL) | 67.7, 100.0, 114.0 |
| Uric acid (mg/dL) | 5.0, 6.6, 7.4 |
| Cholesterol (mg/dL) | 142.5, 166.5, 191.5 |
| HDL (mg/dL) | 33.3, 37.0, 41.2 |
| LDL (mg/dL) | 78.7, 93.3, 111.0 |
| TG (mg/dL) | 98.1, 113.5, 191.2 |
| C-reactive protein (mg/dL) | 1.0, 1.8, 3.6 |
| Atherogenic index | 2.0, 2.6, 3.0 |
| Patients | Gender | Treatment with MT | Variable Determination |
|---|---|---|---|
| 1 | Female | 3 mg/day/2 weeks | Insomnia ↓ [49] |
| 67 | 43 men, 24 women | 21 mg/day/no data | CRP, Platelets ↓ [50] |
| 82 | 32 men, 50 women | 2 mg/day/1 month | Symptoms related to COVID-19 ↓ [51] |
| 58 | 25 men, 23 women | 3 mg/day/1 week | No changes in CRP, lymphocytes, and leukocytes, but oxygen saturation ↓ [52] |
| 82 | 58 men, 24 women | 10 mg/day/2 weeks | General symptoms of COVID-19 ↓ [53] |
| 272 | 120 men, 152 women | 2.6 mg/day/2 weeks | No change in mortality [54] |
| 40 | 23 men, 17 women | 2 mg/day/12 days | Sleep ↑ and delirium ↓ [45] |
| 40 | No data | 9 mg/day/2 weeks | CRP ↓, IL-4,-2 ↓ [55] |
| 82 | 58 men, 24 women | 10 mg/day/2 weeks | Thrombosis ↓ [56] |
| 40 | 26 men, 14 women | 6 mg/day/2 weeks | CRP ↓ [57] |
| 24 | 14 men, 10 women | 3 mg/day/2 weeks | CRP ↓, and breathing improved [58] |
| 82 | 58 men, 24 women | 10 mg/day/2 weeks | CRP ↓, Ferritin ↓, and D-Dimer ↓ [59] |
| 100 | 50 men, 50 women | 5 mg/day/1 week | Fewer days without mechanical ventilation [60] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soto, M.E.; Pérez-Torres, I.; Manzano-Pech, L.; Palacios-Chavarría, A.; Valdez-Vázquez, R.R.; Guarner-Lans, V.; Soria-Castro, E.; Díaz-Díaz, E.; Castrejón-Tellez, V. Redox Homeostasis Alteration Is Restored through Melatonin Treatment in COVID-19 Patients: A Preliminary Study. Int. J. Mol. Sci. 2024, 25, 4543. https://doi.org/10.3390/ijms25084543
Soto ME, Pérez-Torres I, Manzano-Pech L, Palacios-Chavarría A, Valdez-Vázquez RR, Guarner-Lans V, Soria-Castro E, Díaz-Díaz E, Castrejón-Tellez V. Redox Homeostasis Alteration Is Restored through Melatonin Treatment in COVID-19 Patients: A Preliminary Study. International Journal of Molecular Sciences. 2024; 25(8):4543. https://doi.org/10.3390/ijms25084543
Chicago/Turabian StyleSoto, María Elena, Israel Pérez-Torres, Linaloe Manzano-Pech, Adrían Palacios-Chavarría, Rafael Ricardo Valdez-Vázquez, Verónica Guarner-Lans, Elizabeth Soria-Castro, Eulises Díaz-Díaz, and Vicente Castrejón-Tellez. 2024. "Redox Homeostasis Alteration Is Restored through Melatonin Treatment in COVID-19 Patients: A Preliminary Study" International Journal of Molecular Sciences 25, no. 8: 4543. https://doi.org/10.3390/ijms25084543
APA StyleSoto, M. E., Pérez-Torres, I., Manzano-Pech, L., Palacios-Chavarría, A., Valdez-Vázquez, R. R., Guarner-Lans, V., Soria-Castro, E., Díaz-Díaz, E., & Castrejón-Tellez, V. (2024). Redox Homeostasis Alteration Is Restored through Melatonin Treatment in COVID-19 Patients: A Preliminary Study. International Journal of Molecular Sciences, 25(8), 4543. https://doi.org/10.3390/ijms25084543