1. Introduction
Extracorporeal Shock Wave Lithotriptors (ESWLs) have been widely utilized in the urology departments of hospitals all over the world. Their use in noninvasive treatment [
1] has gained credit from the majority of doctors and patients in urology. Most of the currently operational ESWLs locate stones (calculi) manually with a C-arm (X-ray) or ultrasound (US) scanner. When the stone location is done, the lithotriptor thereafter strikes with thousands of shock waves focusing at a spatially fixed focal area (F2) where the stone presumably exists and is subsequently shattered into pieces. After treatment, the patient excretes those fragments as a matter of course during the following months [
2].
The prognoses by ESWLs vary in different studies. In 2010 a large-scale research studied more than 8,500 patients and concluded that the overall stone free rates using an electromagnetic and an electrohydraulic lithotriptors were 61.1% and 64.5%, respectively [
3]. A more recent study reported that the stone-free rate after 3 months was 69.4% after assessing the 3-year treatment results [
4]. The above stone-free rates of the traditional lithotriptors are no more than 70%. It is because the stone moves due to the patient's respiration which causes organs to travel, sometimes by as much as 7 cm [
5]. An
in vitro study showed that the percentage of SWs hitting the stone were 70% and 39% as demonstrated by a model stone driven by a motorized positioner undergoing 10 and 18 mm of motion, respectively [
6]. Those missed shots delivering the compressive and tensile forces were consequently directed at the surrounding tissues and caused cavitation around the cells, which produces renal trauma side effects [
7].
The drawbacks of the existing ESWLs include several aspects. First of all, the stone location procedure is tedious and needs a proficient operator to shorten the fluorescence exposure time. Secondly, a urinary stone moves due to the patient's respiration. Shock waves restricted to a fixed point not only reduce the effectiveness of the treatment, but may also damage nearby tissues. Finally, the operator needs to check the stone's location and reactivate the X-ray fluoroscopy so often that the patient is exposed to even higher doses of radiation. There were some efforts to increase the coincidence ratio between the stone and F2. An Anti-misshot Control Device (AMCD) has been installed in a piezoelectric lithotriptor to prevent misshots to renal tissue. It functions in such a manner that shock waves were generated only when the US echo of a stone was in the focal region [
8]. Another software called Echotrack was also developed to calculate the average position of the stone in US images. It automatically adjusted the SW generator to coincide with the stone's location once every certain amount of time [
9]. A genuine automatic stone tracking system was developed by the authors' research team and functioned to use US to sense the stone and servo motors to track it in real time. The system could reduce by more than half the number of SWs needed [
10,
11].
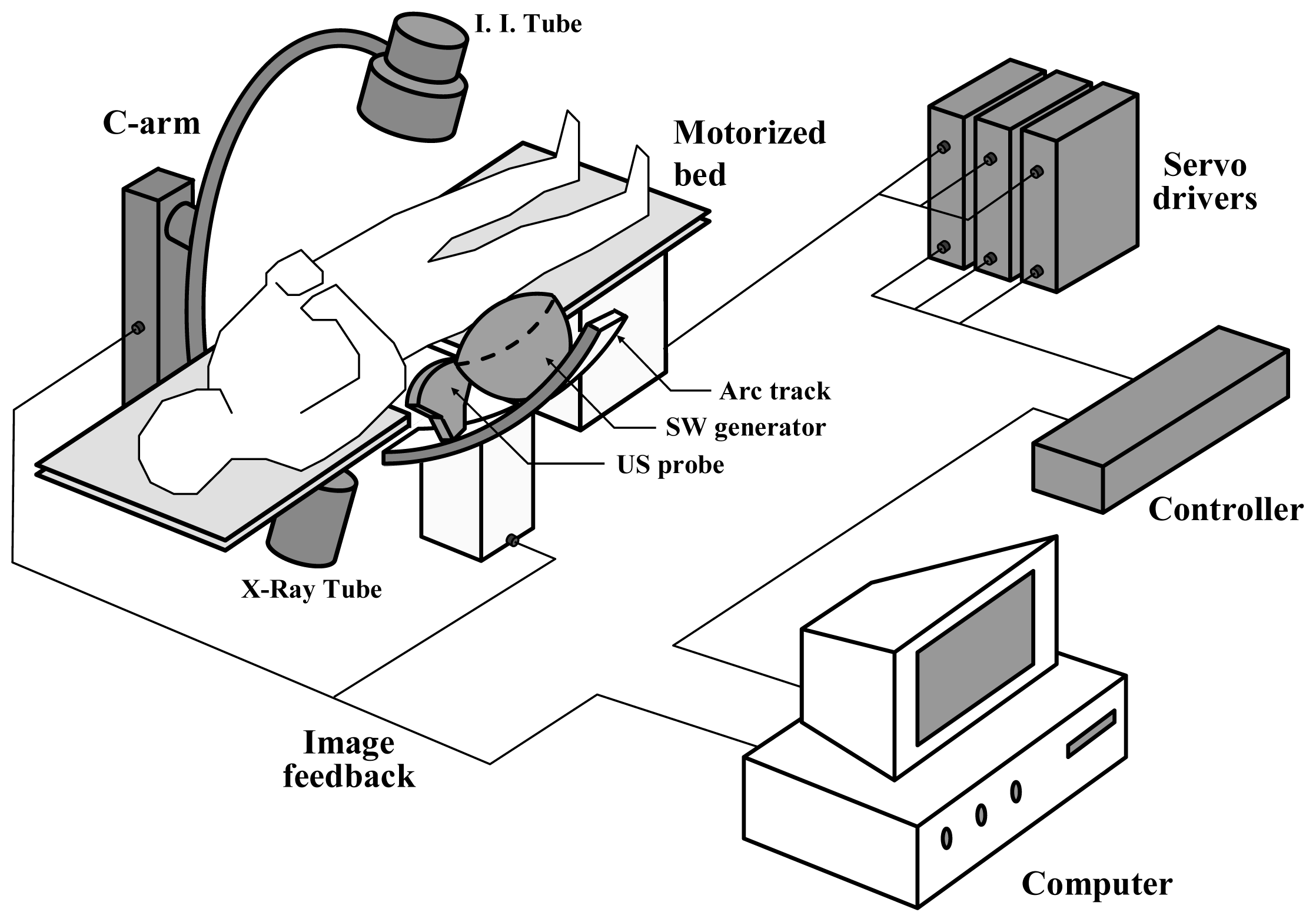
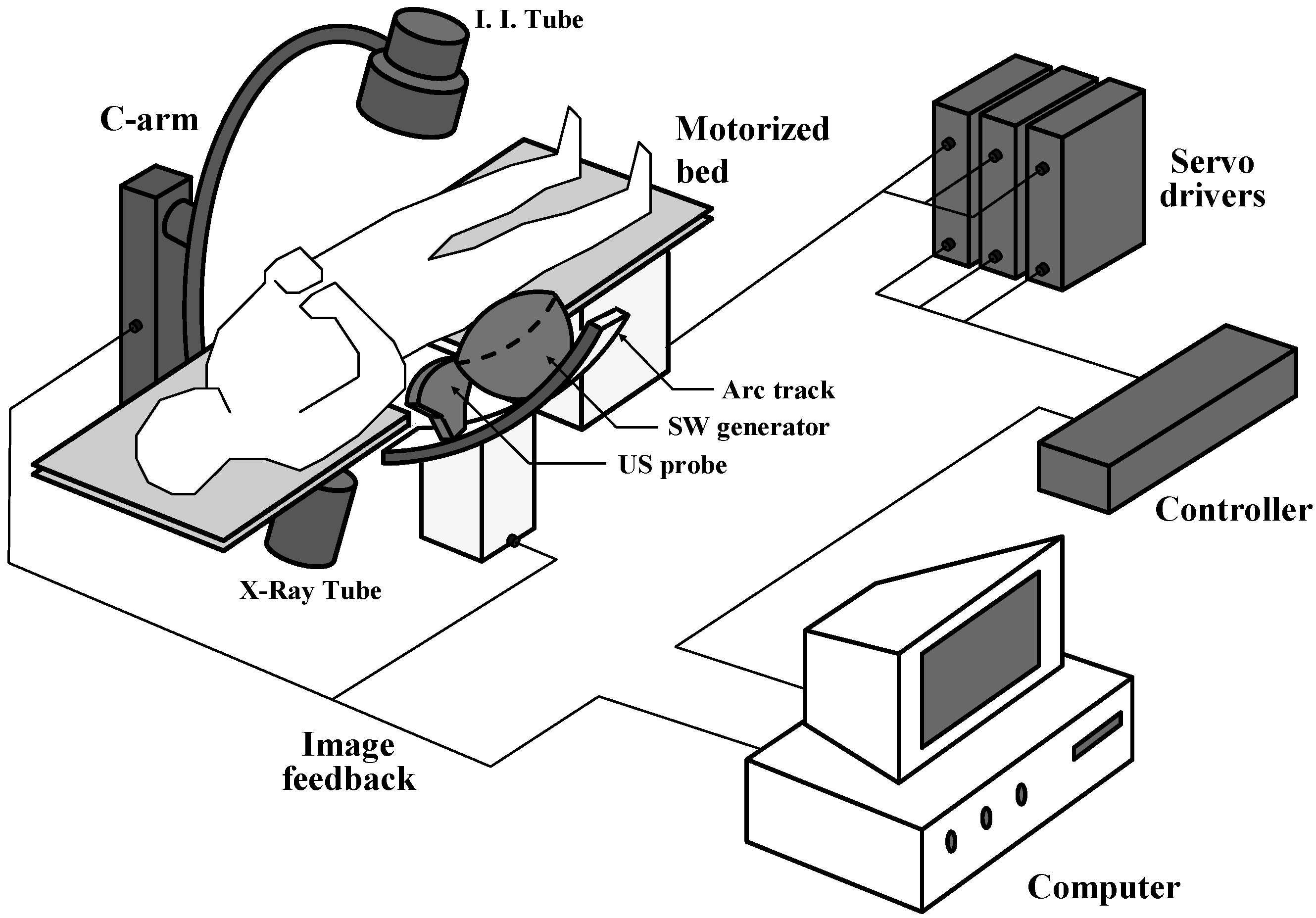
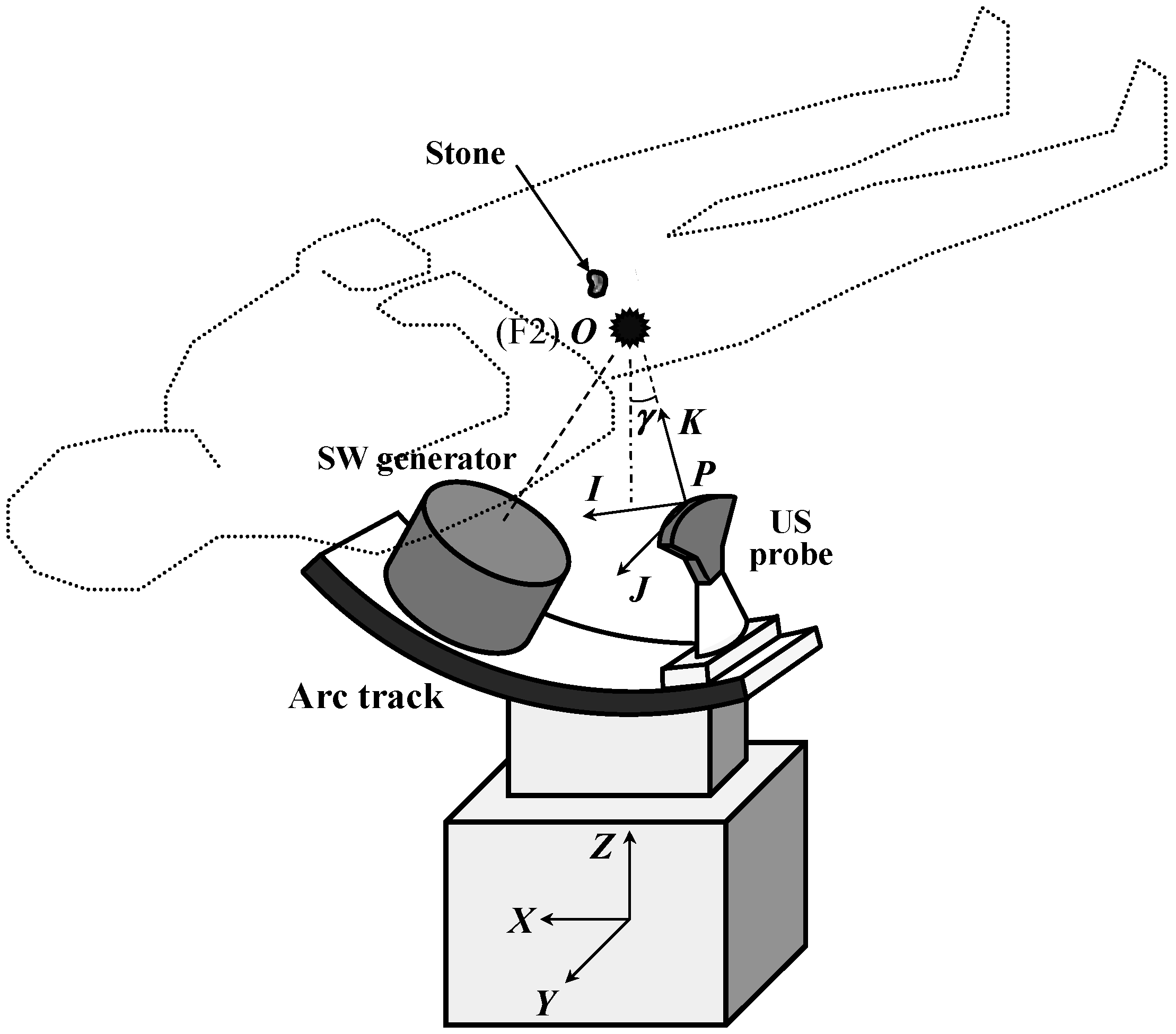
This study takes advantage of both X-ray and US to develop a dual stone locating system on a domestic ESWL here in Taiwan. It is capable of initially locating a urinary stone and then tracking it down automatically. The work includes the image processing on both pieces of equipment, the derivations of stone location equations, the programming of the control panel, and the integration of mechatronic components. It is noted that, in fact, some of the technologies developed in this study are not new. Few of them are even in clinical use already. Our job is to accommodate the frameworks of an existing lithotriptor and integrate these technologies for the new model to achieve our design goals.
3. Results and Discussion
We performed two
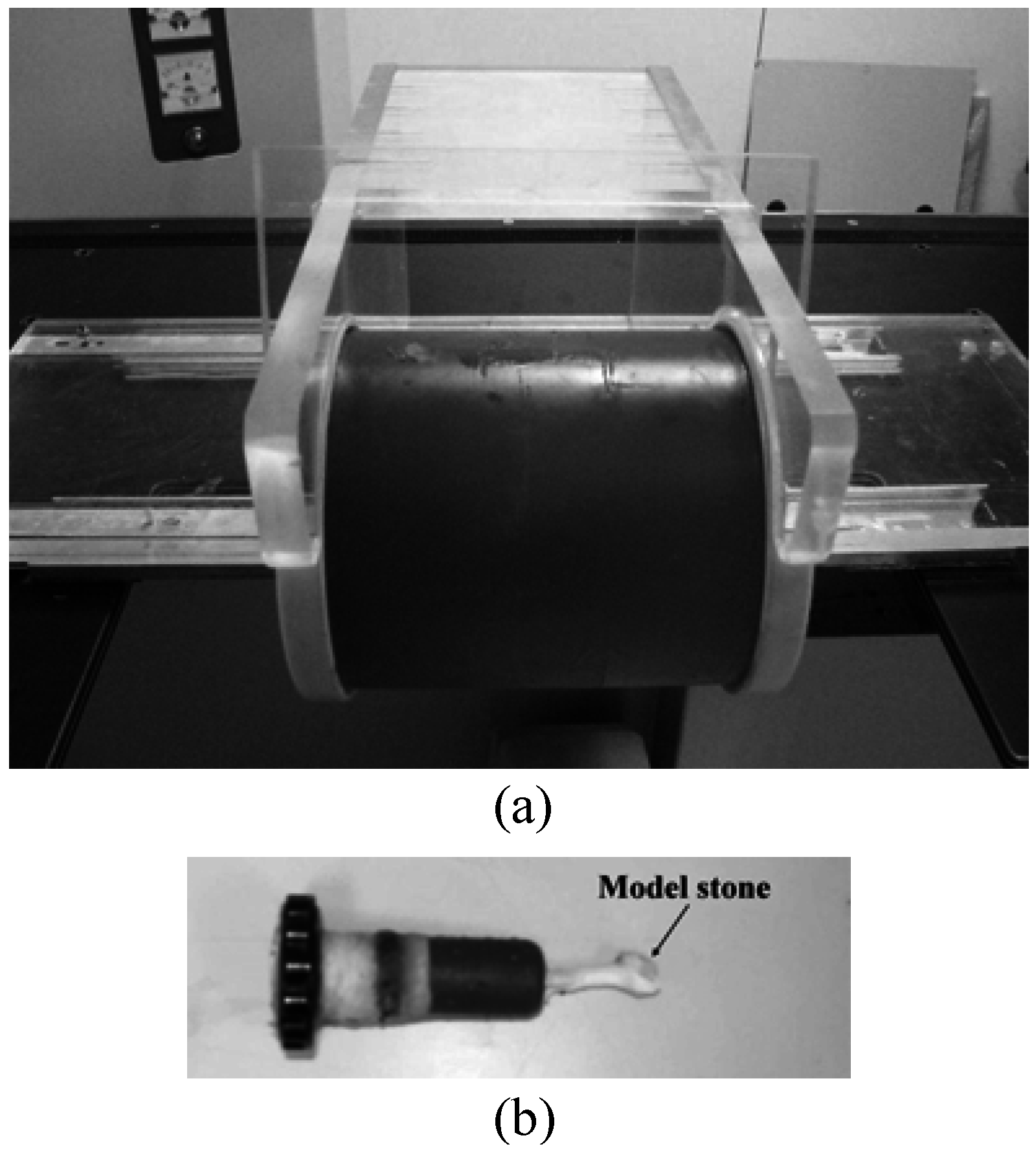
in vitro experiments to demonstrate the ability of the dual stone locating system. The first was the initial stone location inside a phantom (LTK-5, ATS Lab., Inc., Bridgeport, CT, USA, see
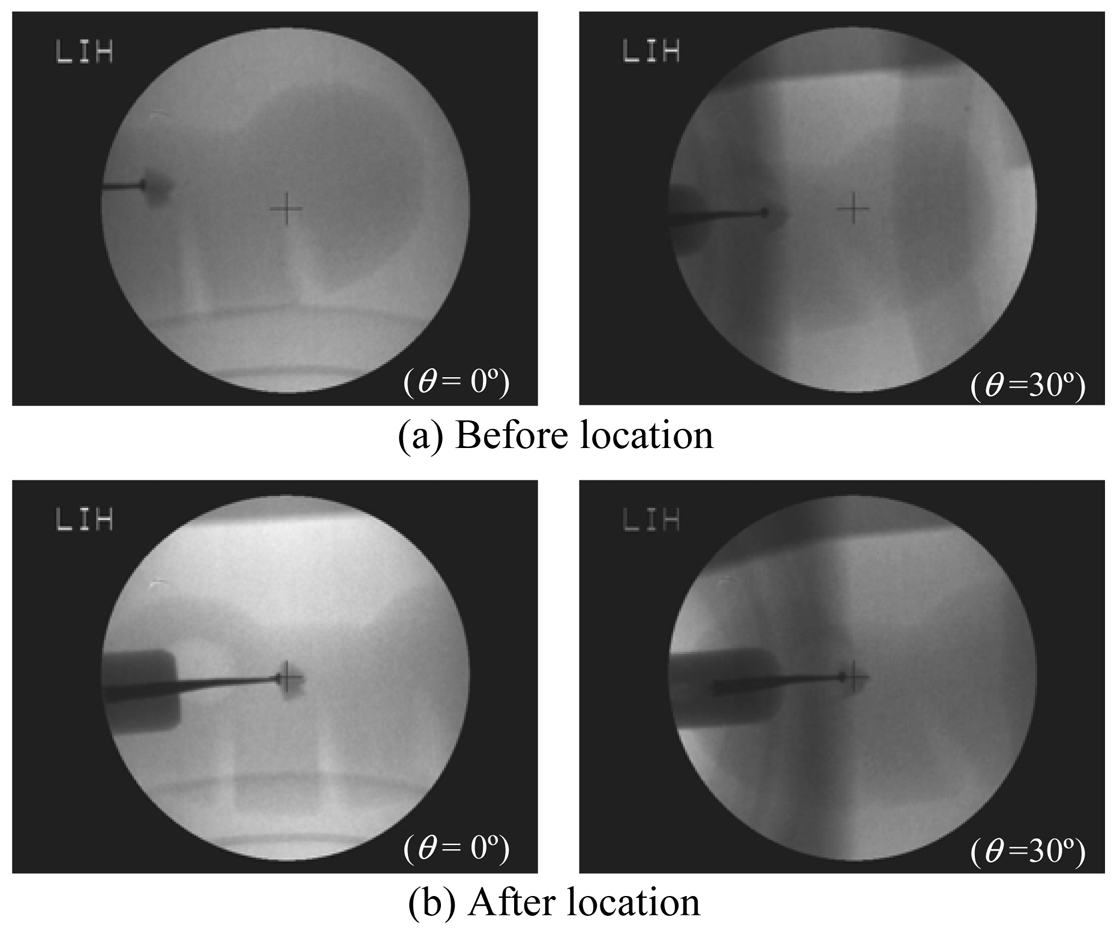
Figure 6). A model stone attached to the tip of the phantom cap was plugged inside the kidney-shaped cavity of the phantom. The phantom was mounted on the ESWL bed and placed inside the exposure range of the X-ray.
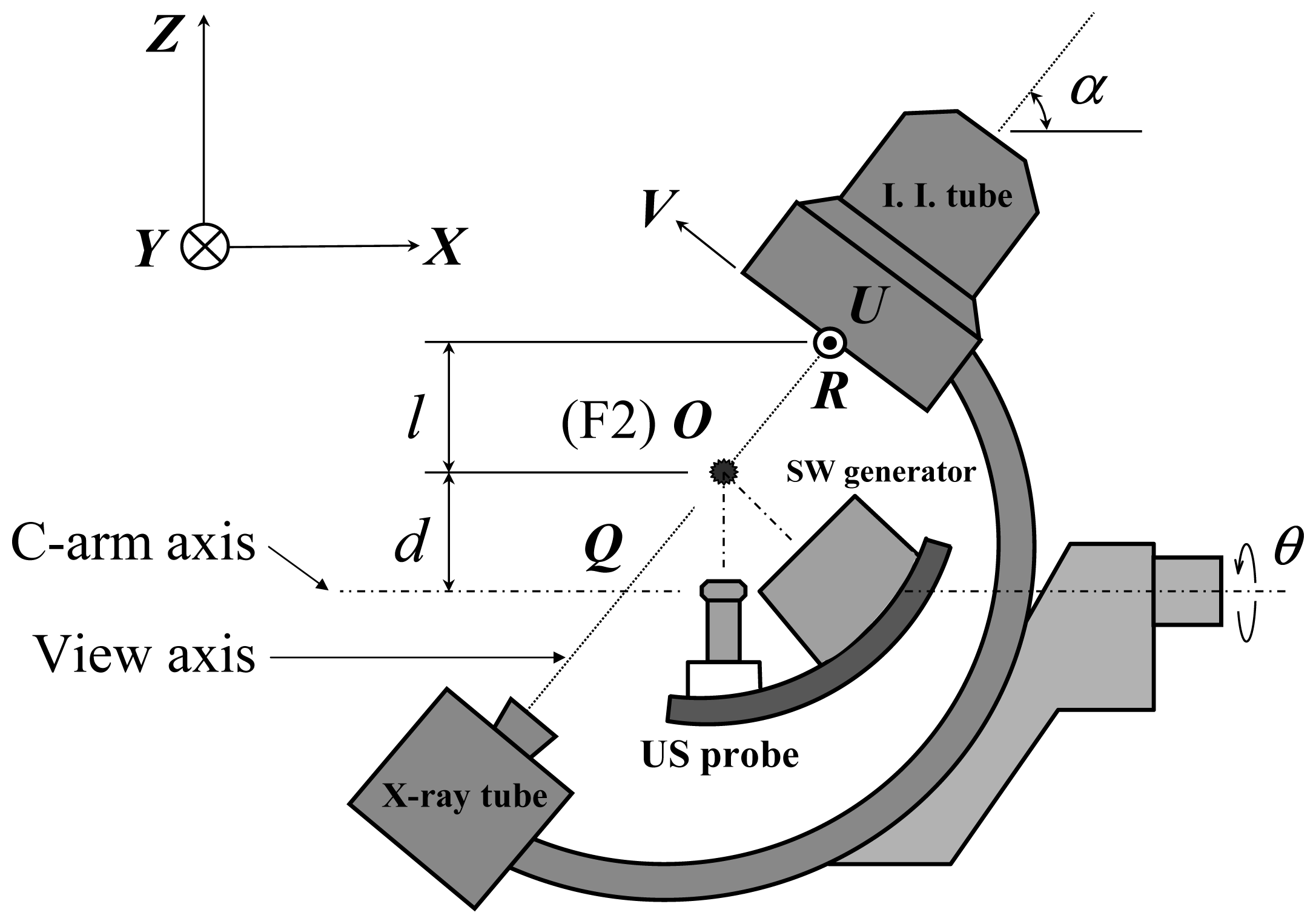
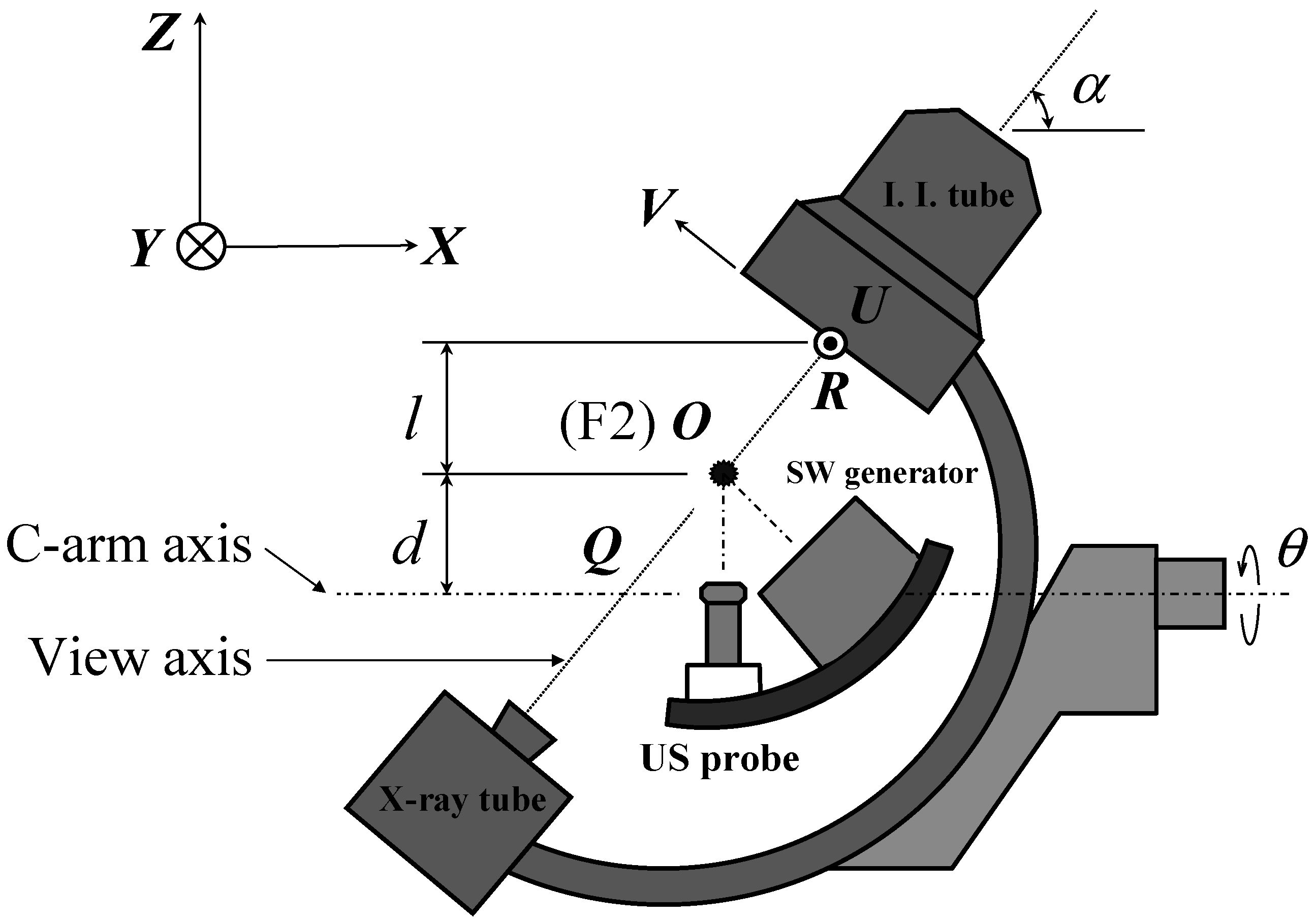
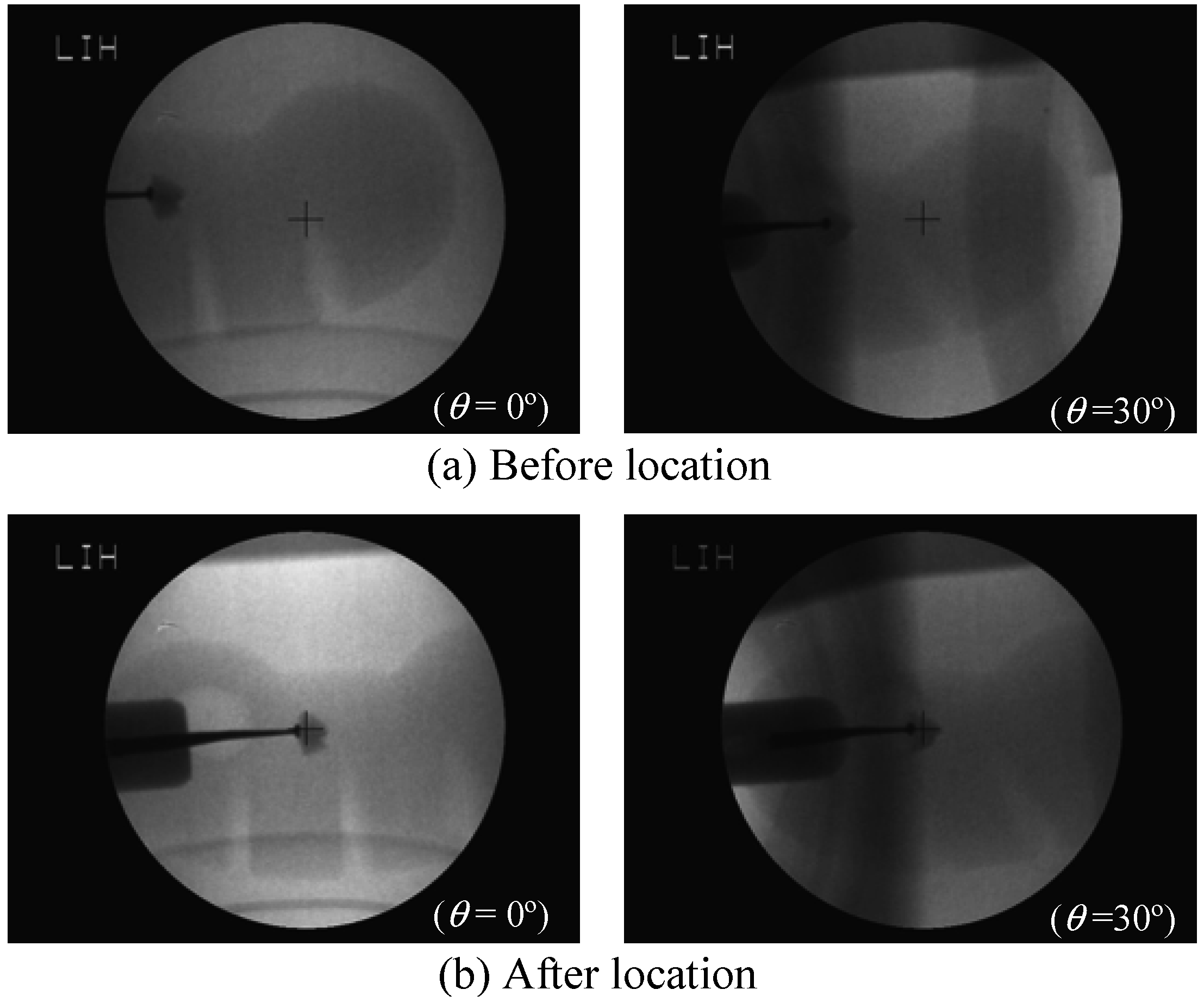
Since there was not any obstructing factor along the view axis, no pitch angle was needed (
α = 0°). Two consecutive fluorescent images (
θ = 0° and
θ = 30°) were taken and displayed on the monitor to let the operator point at the stone. According to
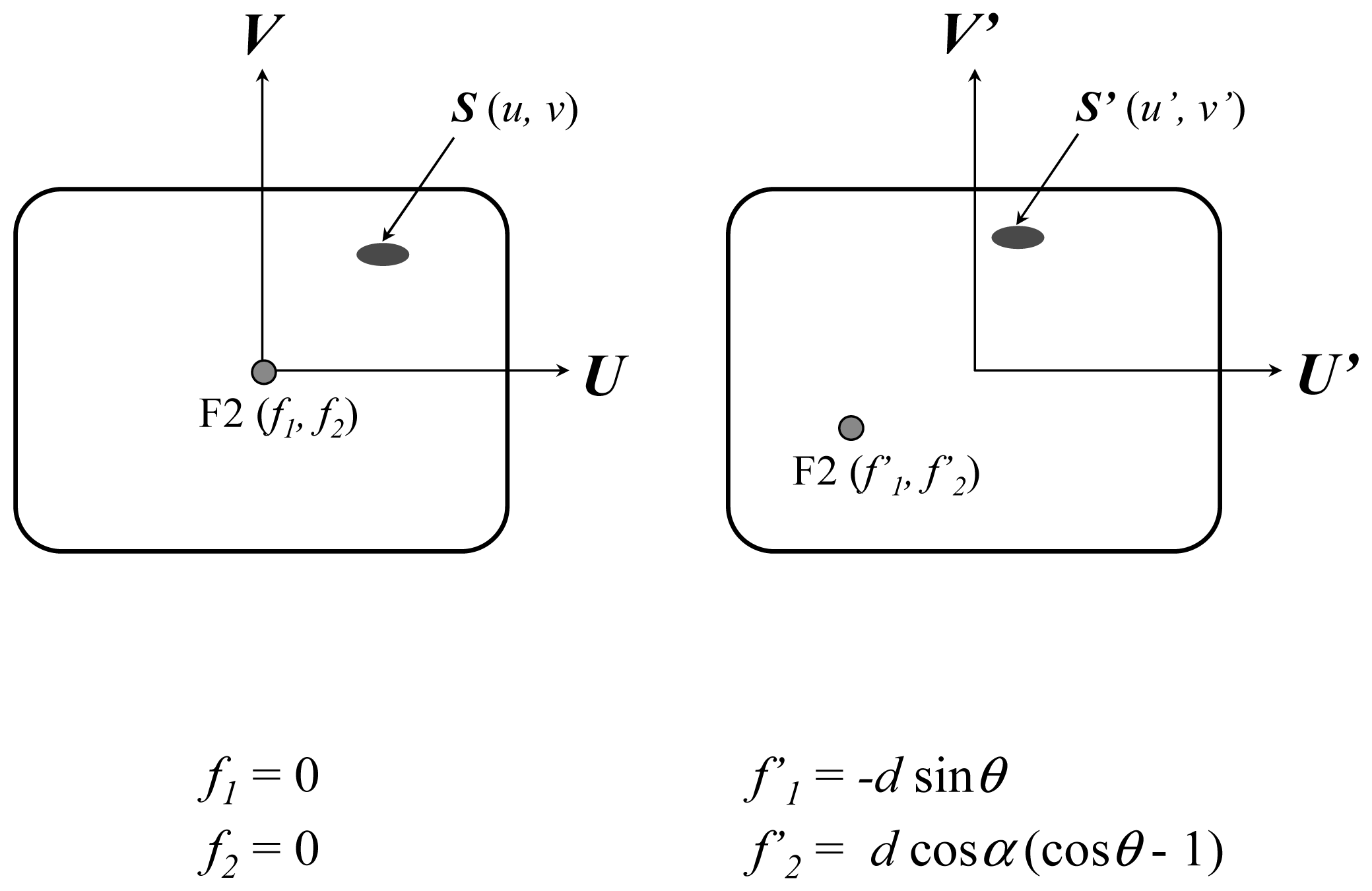
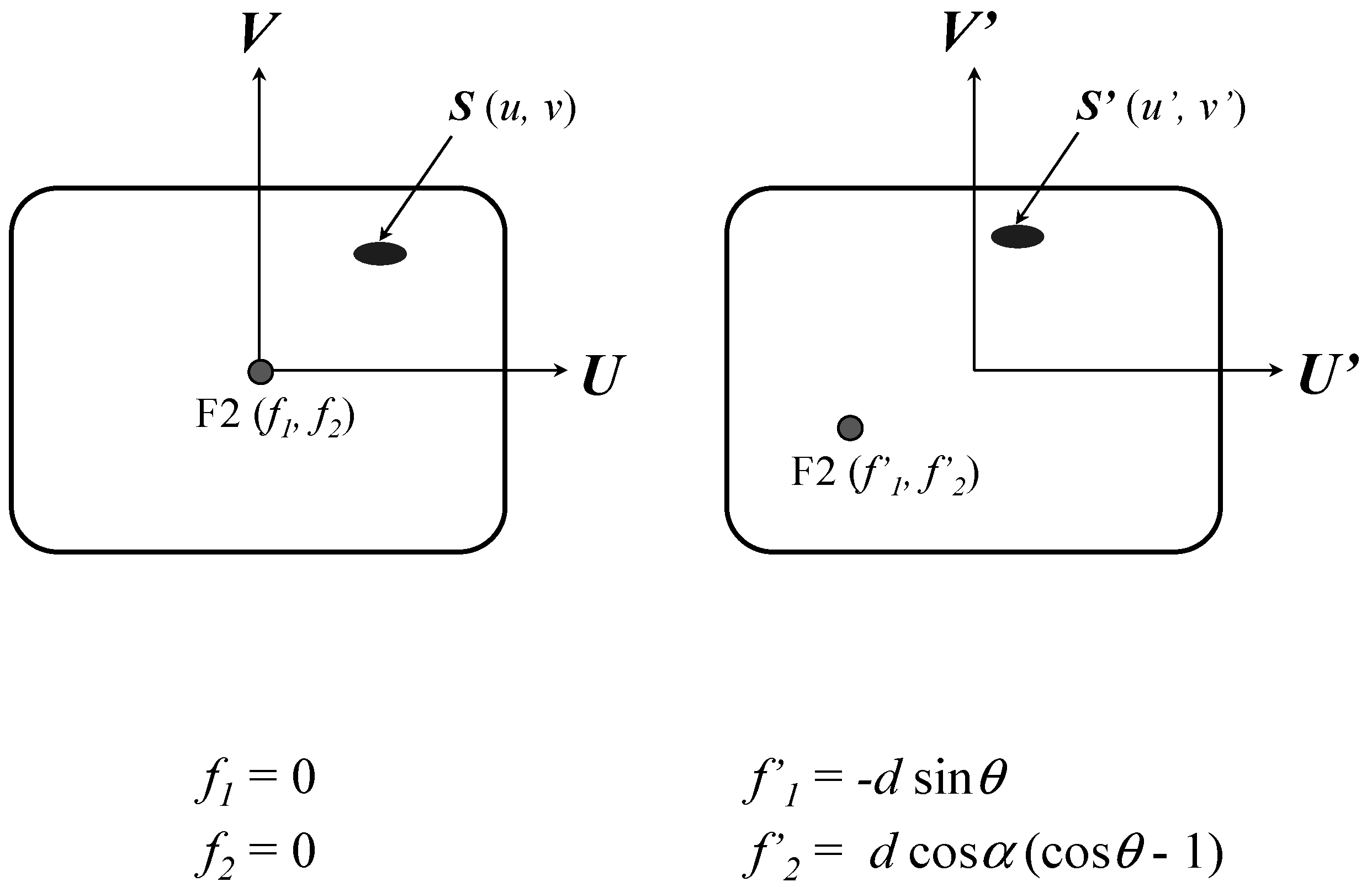
Equations (1)–
(3), the system actuated the servo mechanisms to move the bed briefly. Afterward, another two consecutive fluorescent images with the same angles were taken to verify the accuracy of the stone location, as shown in
Figure 7. As one can see, the initial stone location mode did successively bring the modal stone to F2 (cross mark).
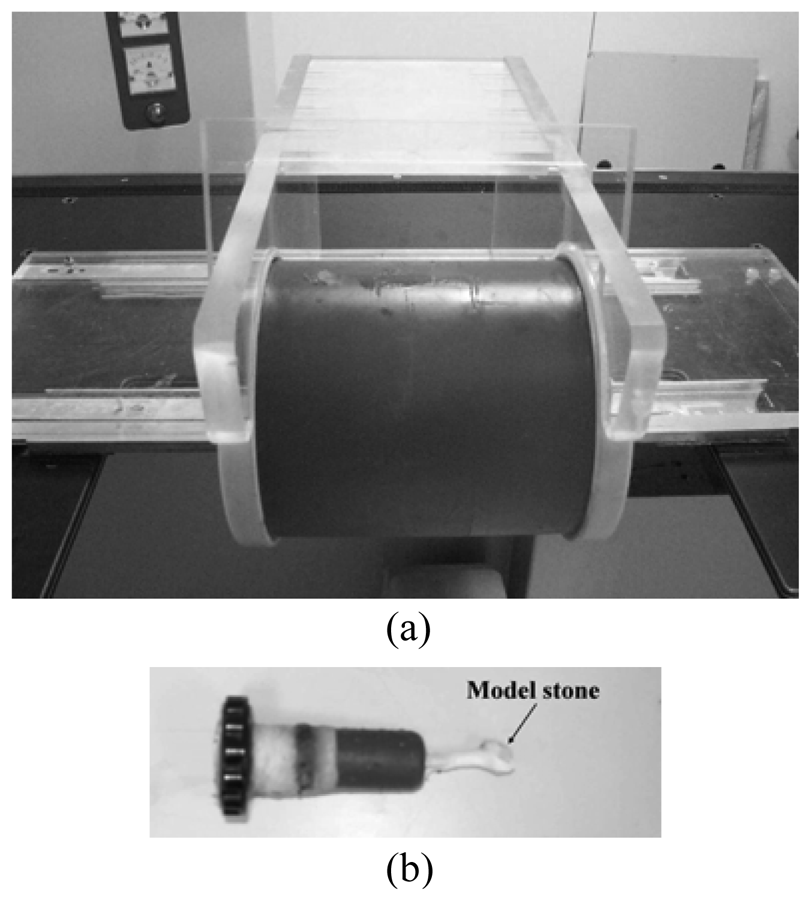
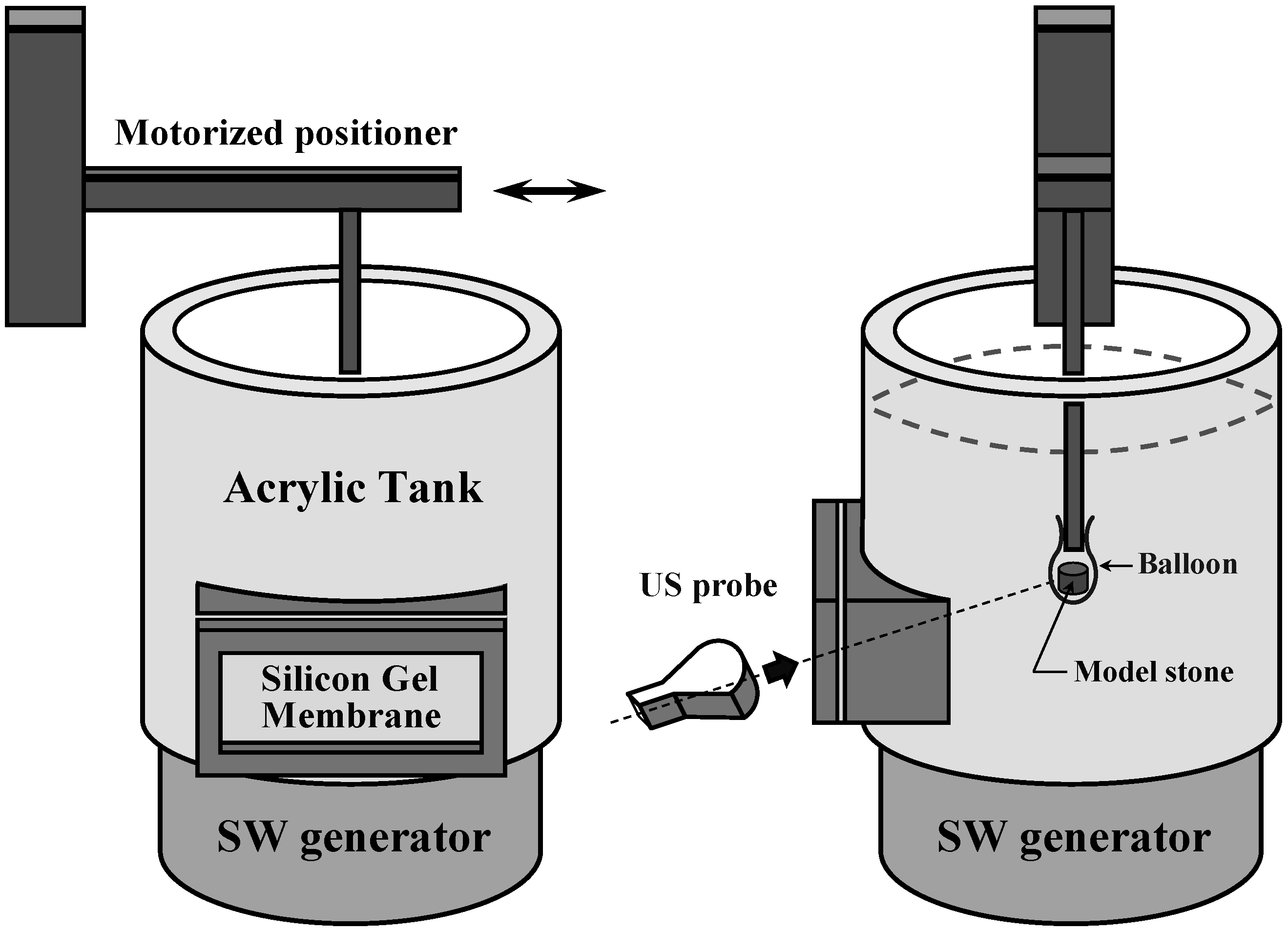
The second experiment was to demonstrate the automatic stone tracking ability as the system switched to the stone tracking mode. To simulate the stone moving inside a patient, we customized a set of devices to let the US be able to scan a model stone.
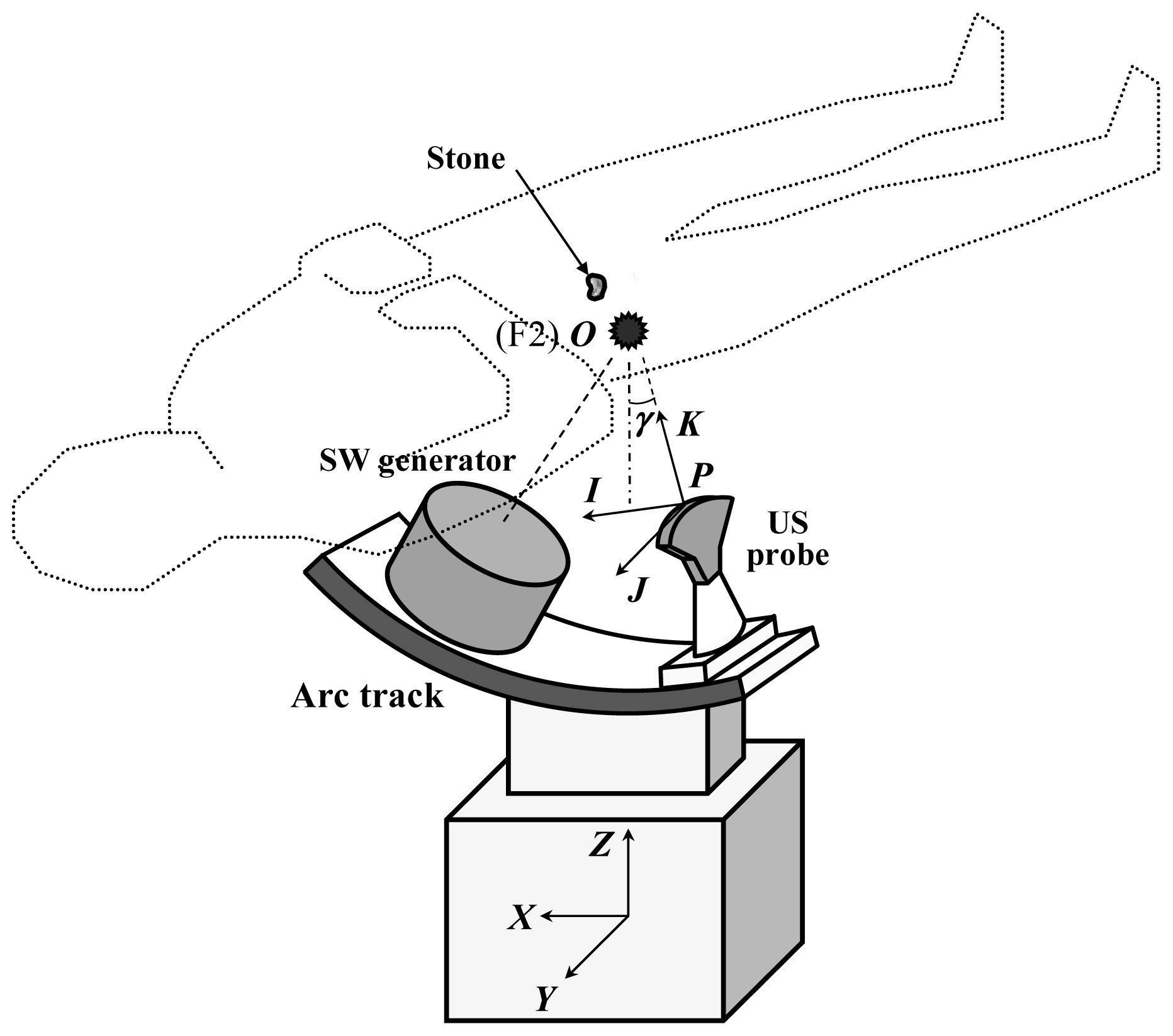
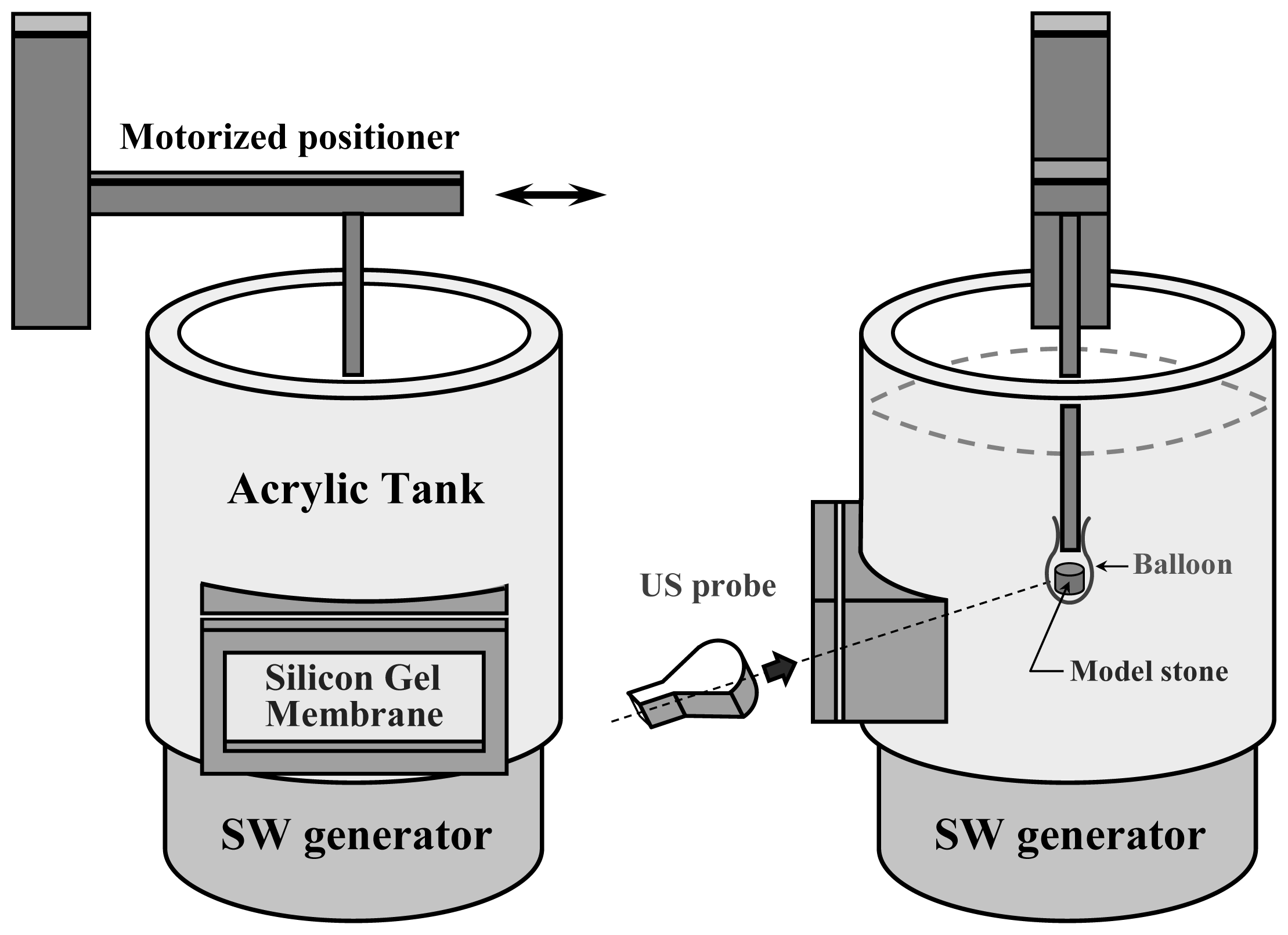
Figure 8 shows an acrylic tank mounted on the SW generator that included a side window. The US probe could make contact with the silicone gel membrane fixed to the window frames and scan inside the water tank. A motorized positioner immersed a stick whose tip was fastened with a water-filled balloon containing a cylindrical model stone (6 × 6 mm, diameter × height.) A previously recorded trajectory of a kidney stone was introduced to the positioner that moved the stone to simulate a situation perturbed by respiration. When the automatic tracking mode was turned on, the software continuously processed the US images in real time (∼10 fps) and simultaneously commanded the servo mechanisms to move the bed along with the positioner. We recorded the US images all the way for tracking and non-tracking conditions, and later on analyzed their coincidence rates between the stone and F2 along the time axis.
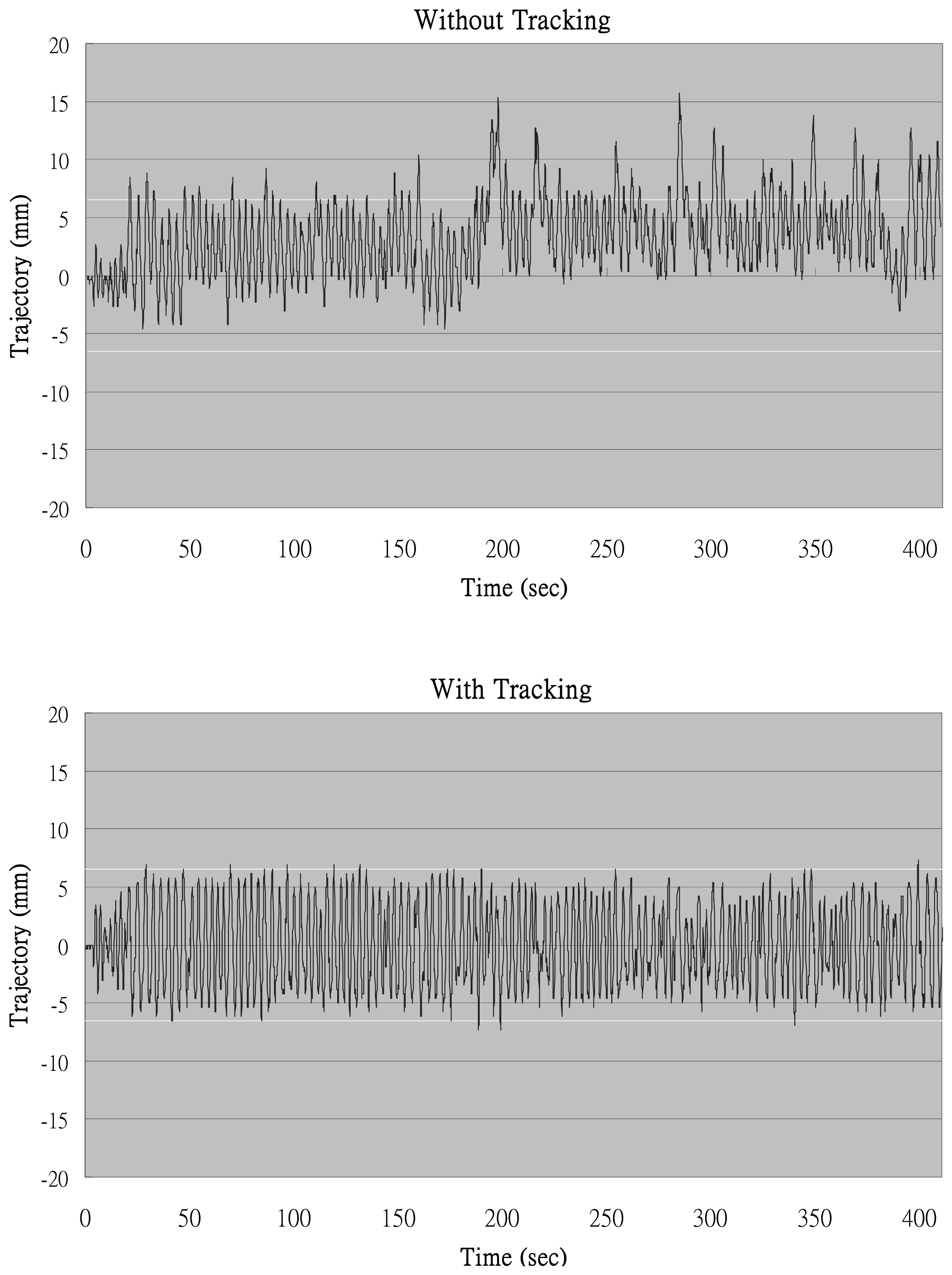
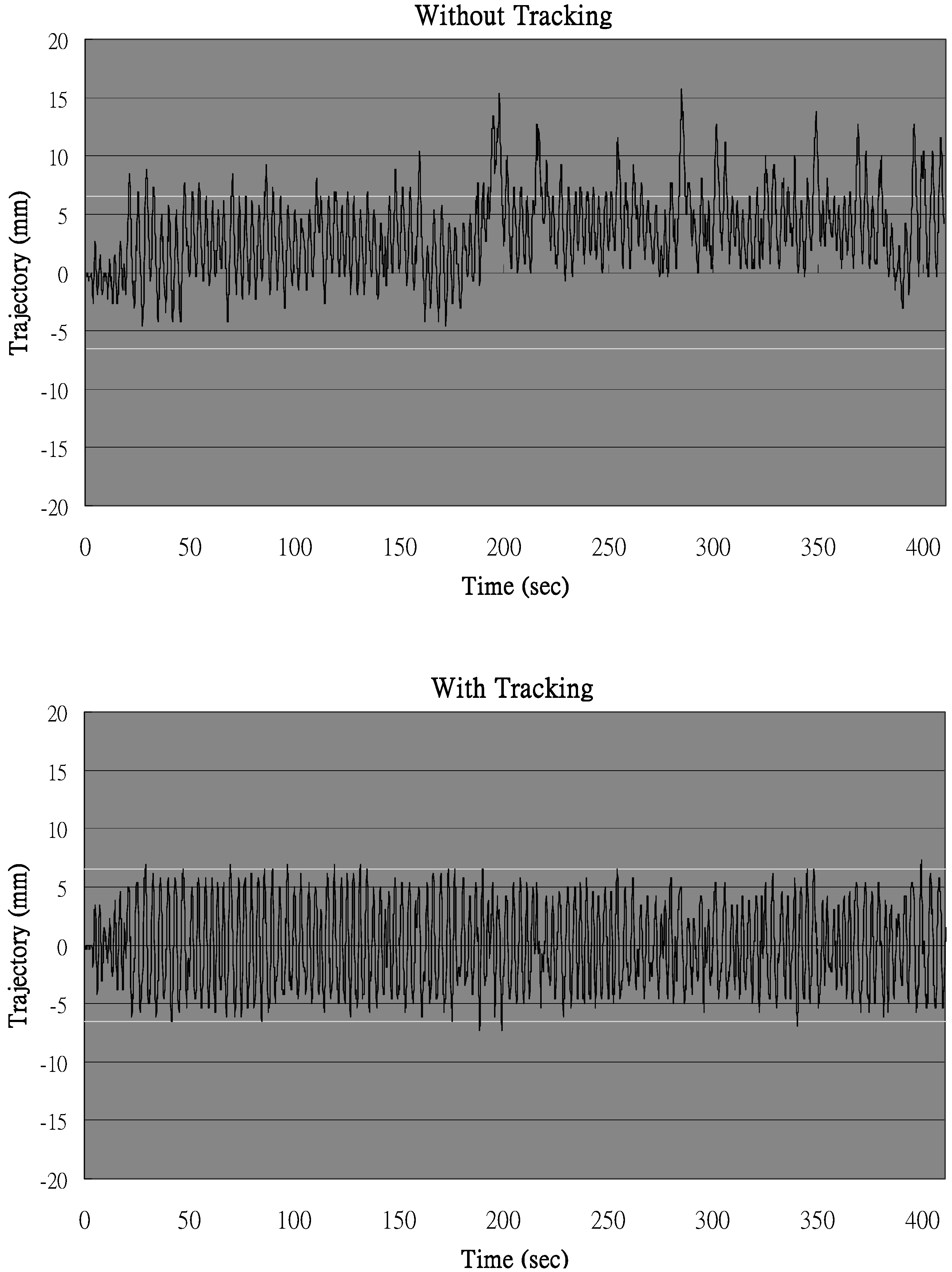
Figure 9 shows the trajectories of the stone's center in the US images with and without tracking. The horizontal dashed lines indicated that the portion of the stone is in the focal zone. This was set between ±6.5 mm where the effective range of the focal zone was ±3.5 mm and the half size of the stone was approximately 3 mm. As the stone's center went inside the dashed lines, the SW would be considered able to successfully hit the stone.
Without tracking, the patient's breathing slowly shifted the average position of the stone, which accounted for the lower coincidence rate of only 82.6%. In the automatic stone tracking mode, on the other hand, the trajectory stayed mostly inside the focal zone and reached 98.5% of the coincidence rate. This means that in this case the application of nearly 20% of the SWs could be saved by using the stone tracking function.
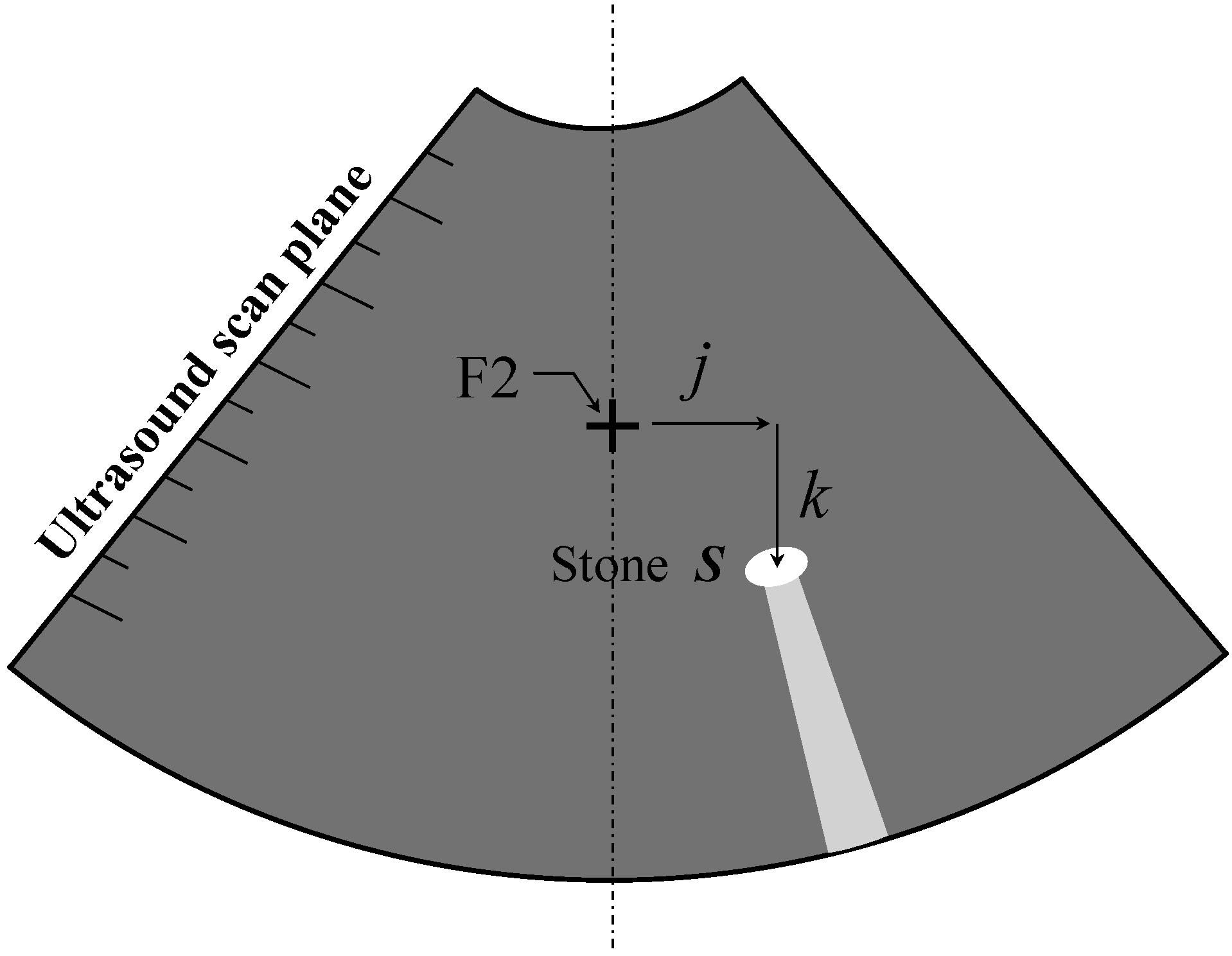
It is noted that, as mentioned in the last paragraph of Section 2, the system cannot track the stone if it moves out of the ultrasound scan plane. The software has to stop tracking, reposition the stone by X ray, and start tracking all over again. Although missing the stone is annoying, it seldom happens in the current ex vivo simulation setting without shock wave application. Besides, re-targeting on the stone does not take long and does no more harm to the patient, compared to the traditional X-ray ESWLs. If the stone breaks and its fragments distribute in various calices during treatment, as long as the ultrasound can identify one of the fragments and the contrast between the fragment and the surrounding tissue is clear, i.e., it can lock on it. The tracking mode can still be activated. If continuously recognizing or tracking the stone through US is not possible, this system still can remain to target by X ray only on a fixed point without using tracking function. Just like the old way, it is better for one to target on the stone fragments piece by piece.
It needs to be mentioned that this in vitro experiment is used to test the tracking ability of the revised system in a simplified environment. In ex vivo or even in vivo situations the surrounding tissues of the stone might greatly change the gray level characteristics in the ultrasound images which may affect the success of recognizing and tracking the stone. These need to be assessed in the future studies. In addition, some feature in the US image, such as the anechoic shadow beneath the stone, will be implemented in the stone recognition process in future endeavors.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}








