
Accuracy of a Custom Physical Activity and Knee Angle Measurement Sensor System for Patients with Neuromuscular Disorders and Gait Abnormalities

 ,
, 
Abstract
:1. Introduction
2. Methods
2.1. Instrumentation

2.2. Software Algorithm
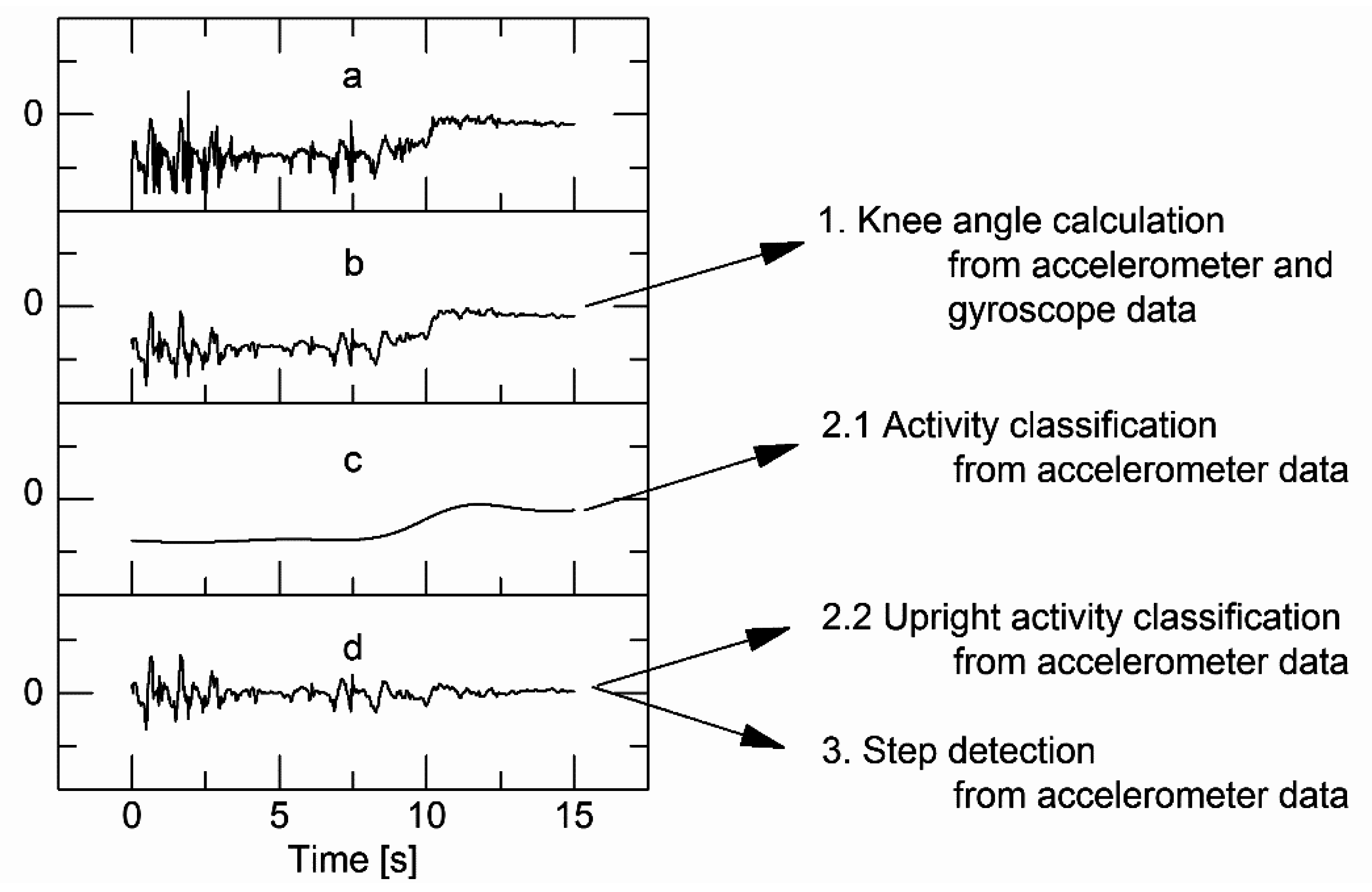
2.2.1. Raw Data Filtering and Frequency Separation

2.2.2. Knee Angle Calculation
2.2.3. Activity Classification

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tibial Sensor | ||||
|---|---|---|---|---|
| Horizontal | Vertical | Sideways | ||
| Femoral Sensor | Horizontal | lying | sitting | lying |
| Vertical | undefined | upright activity | lying | |
| Sideways | lying | lying | lying | |
2.2.4. Step Detection
2.3. Algorithm and Sensor Evaluation
| No. | Exercise | Expected Activities |
|---|---|---|
| (I) | Sensor application | - |
| (II) | Sensor calibration and synchronization | standing |
| (III) | Sensor familiarization | sitting |
| (IV) | Maximum active knee flexion and extension in sitting, standing and lying posture | sitting; standing and lying |
| (V) | Transitions between postures | standing ↔ sitting; standing ↔ lying |
| (VI) | Walking standardized paths marked on the ground | walking |
| (VII) | 25ft walk test | walking |
| (VIII) | Sitting and resting | sitting |
| (IX) | Eating a snack | sitting → walking → standing and opening a cupboard → walking → sitting while eating → walking → standing and washing hands → walking → sitting |
| (X) | Opening a window | sitting → walking → standing and opening window → walking → sitting |
| (XI) | Watching TV | sitting |
| (XII) | Interview | sitting → walking → standing → sitting |
| (XIII) | Maximum active knee flexion and extension | lying; sitting; standing |
| (XIV) | Sensor removal | - |
2.3.1. Excluded Data
2.3.2. Statistical Analysis
3. Results
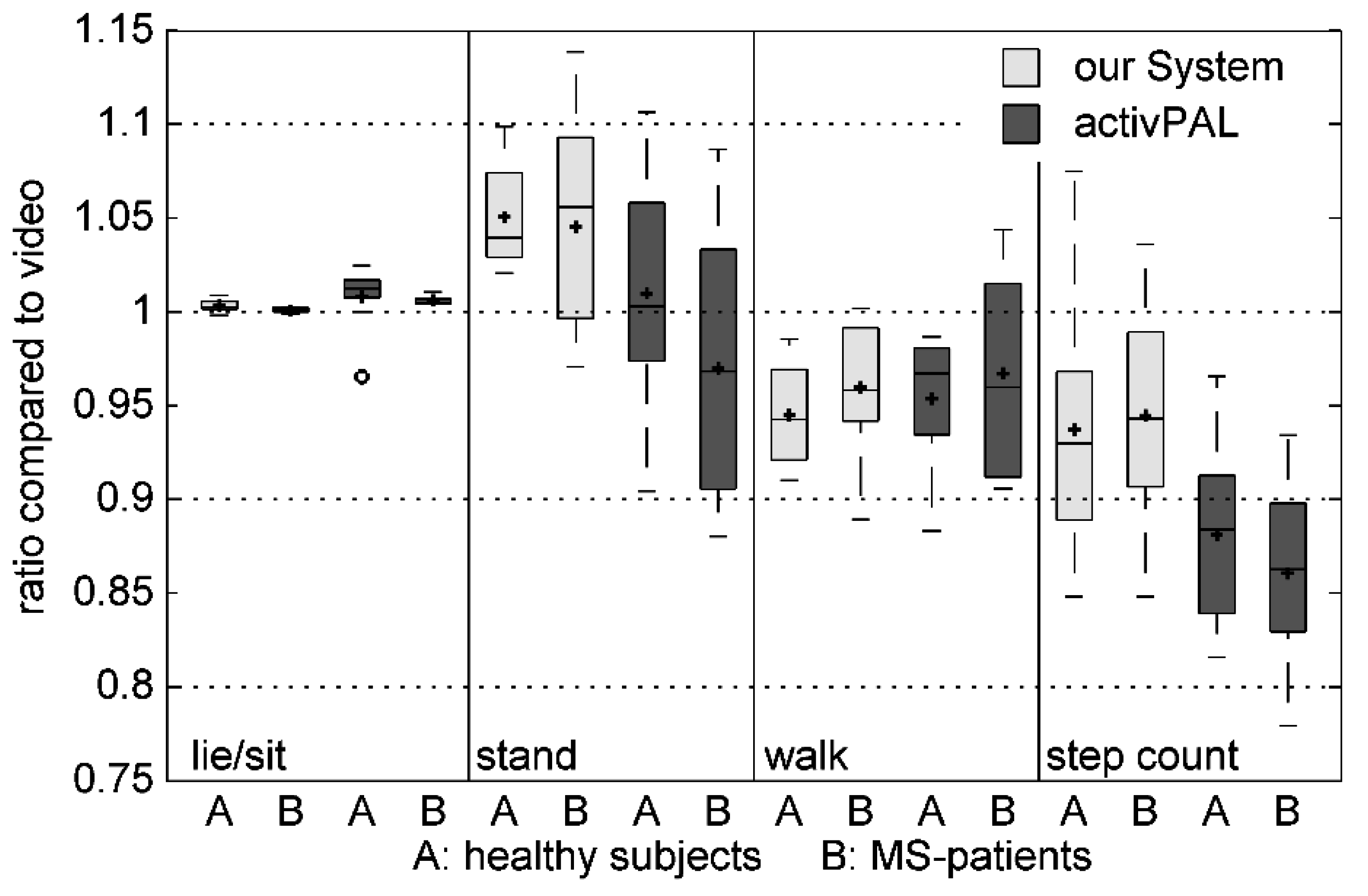
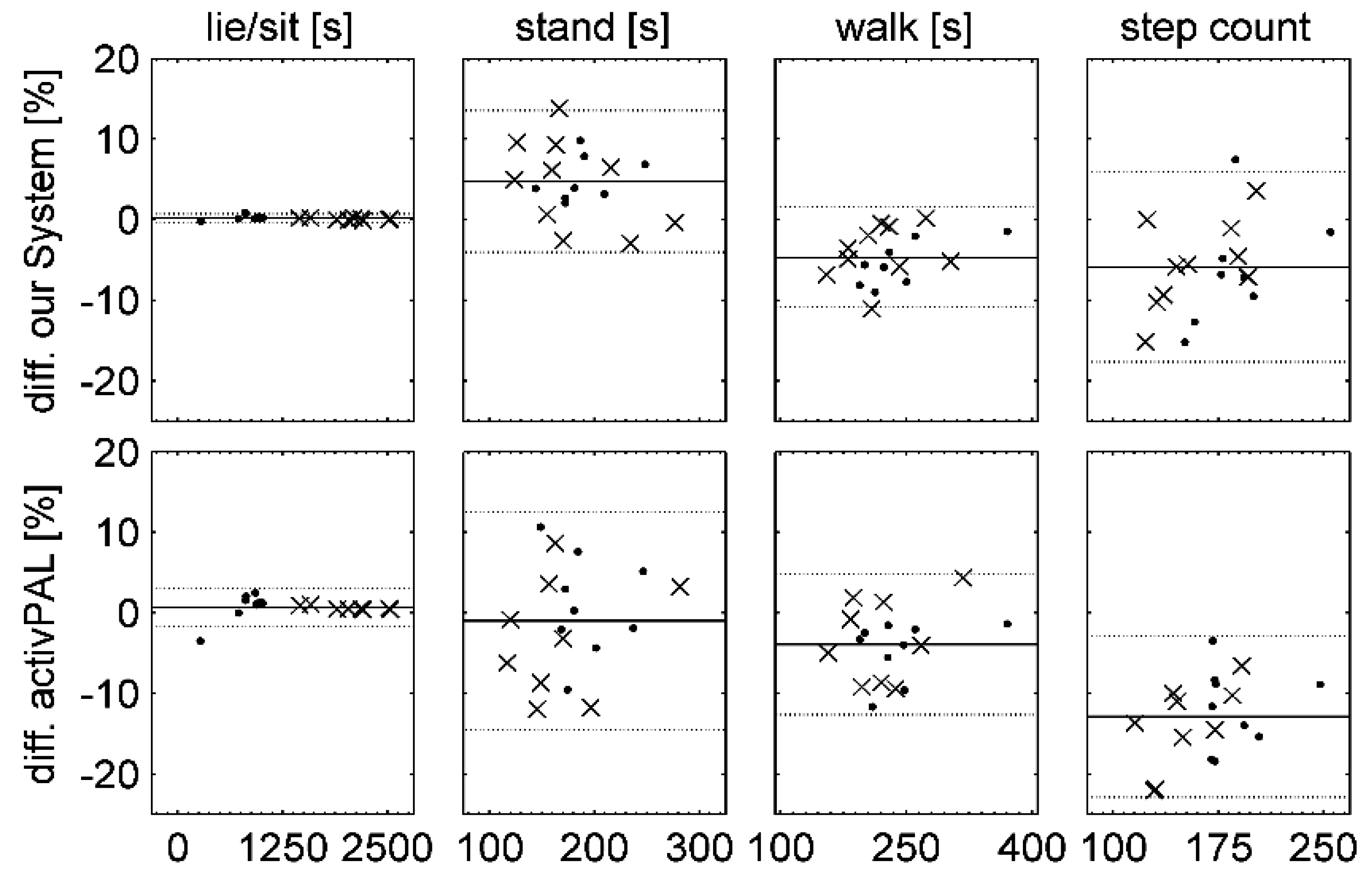
3.1. Activity Classification and Step Counting
| Video Annotation-Researcher 2 | ||||||||
| Lie | Sit | Stand | Walk | N/D | ||||
| (a) | Video Annotation - Researcher 1 | A (n = 10) | Lie | 99.50 | 0.50 | |||
| Sit | 0.11 | 99.08 | 0.02 | 0.01 | 0.78 | |||
| Stand | 0.31 | 90.62 | 5.34 | 3.73 | ||||
| Walk | 1.88 | 97.70 | 0.42 | |||||
| B (n = 10) | Lie | 99.07 | 0.93 | |||||
| Sit | 0.20 | 99.39 | 0.01 | 0.41 | ||||
| Stand | 0.32 | 85.95 | 8.13 | 5.60 | ||||
| Walk | 1.77 | 98.01 | 0.22 | |||||
| Our Algorithm | ||||||||
| Lie | Sit | Stand | Walk | N/D | ||||
| (b) | Merged Video Annotation (ground truth) | A (n = 8) | Lie | 96.94 | 3.06 | |||
| Sit | 0.07 | 99.88 | 0.01 | 0.04 | ||||
| Stand | 0.82 | 96.45 | 2.73 | |||||
| Walk | 0.70 | 6.37 | 92.87 | 0.05 | ||||
| B (n = 10) | Lie | 92.68 | 7.32 | |||||
| Sit | 0.11 | 99.71 | 0.12 | 0.01 | 0.04 | |||
| Stand | 2.08 | 92.63 | 5.21 | 0.09 | ||||
| Walk | 0.56 | 7.57 | 91.88 | |||||
| activPAL | ||||||||
| Lie/sit | Stand | Walk | N/D | |||||
| (c) | Merged Video Annotation (ground truth) | A (n = 9) | Lie | 100.00 | ||||
| Sit | 99.70 | 0.30 | 0.01 | |||||
| Stand | 5.22 | 89.24 | 5.54 | |||||
| Walk | 0.83 | 7.87 | 91.30 | |||||
| B (n = 9) | Lie | 100.00 | ||||||
| Sit | 99.98 | 0.02 | ||||||
| Stand | 6.78 | 87.36 | 5.86 | |||||
| Walk | 0.32 | 7.20 | 92.48 | |||||
| Our Algorithm | activPAL | ||||
|---|---|---|---|---|---|
| A | B | A | B | ||
| Lying | Precision | 0.99 | 0.97 | not applicable, distinction between lying and sitting posture is not possible due to functionality | |
| Sensitivity | 0.97 | 0.93 | |||
| Specificity | 1 | 1 | |||
| Accuracy | 1 | 1 | |||
| Sitting | Precision | 0.99 | 0.99 | ||
| Sensitivity | 1 | 1 | |||
| Specificity | 0.99 | 0.98 | |||
| Accuracy | 0.99 | 0.99 | |||
| Lying + Sitting | Precision | 1 | 1 | 0.99 | 0.99 |
| Sensitivity | 1 | 1 | 1 | 1 | |
| Specificity | 0.99 | 0.99 | 0.97 | 0.97 | |
| Accuracy | 1 | 1 | 0.99 | 0.99 | |
| Standing | Precision | 0.92 | 0.89 | 0.89 | 0.90 |
| Sensitivity | 0.96 | 0.93 | 0.89 | 0.87 | |
| Specificity | 0.98 | 0.99 | 0.98 | 0.99 | |
| Accuracy | 0.98 | 0.99 | 0.97 | 0.98 | |
| Walking | Precision | 0.98 | 0.96 | 0.96 | 0.95 |
| Sensitivity | 0.93 | 0.92 | 0.91 | 0.92 | |
| Specificity | 0.99 | 1 | 0.99 | 1 | |
| Accuracy | 0.98 | 0.99 | 0.97 | 0.99 | |


| Difference [%] Mean (SD) | ||
|---|---|---|
| Our System | activPAL | |
| Lie/Sit | 0.18 (0.27) | 0.70 (1.21) |
| Stand | 4.75 (4.50) | −1.02 (6.91) |
| Walk | −4.68 (3.17) | −3.95 (4.44) |
| Step Count | −5.87 (6.02) | −12.92 (5.11) |
3.2. Knee Angle Measurement
| Quality of Knee Angle Measurement | ||||
|---|---|---|---|---|
| n | RMSE [°] Mean (SD) | PCC Mean (SD) | ||
| Activity | ROM lying | 34 | 4.86 (1.97) | 0.999 (0.000) |
| ROM sitting | 33 | 2.91 (1.09) | 0.999 (0.001) | |
| ROM Standing | 32 | 2.37 (0.78) | 0.999 (0.001) | |
| Walking | 36 | 3.63 (1.23) | 0.975 (0.026) | |
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Caspersen, C.J.; Powell, K.E.; Christenson, G.M. Physical Activity, Exercise, and Physical Fitness: Definitions and Distinctions for Health-Related Research. Public Health Rep. 1985, 100, 126–131. [Google Scholar] [PubMed]
- Gorman, E.; Hanson, H.M.; Yang, P.H.; Khan, K.M.; Liu-Ambrose, T.; Ashe, M.C. Accelerometry Analysis of Physical Activity and Sedentary Behavior in Older Adults: A Systematic Review and Data Analysis. Eur. Rev. Aging. Phys. Activ. 2014, 11, 35–49. [Google Scholar] [CrossRef]
- Lin, L.L.; Brown, J.C.; Segal, S.; Schmitz, K.H. Quality of Life, Body Mass Index, and Physical Activity among Uterine Cancer Patients. Int. J. Gynecol. Cancer 2014, 24, 1027–1032. [Google Scholar] [CrossRef] [PubMed]
- Marck, C.H.; Hadgkiss, E.J.; Weiland, T.J.; van der Meer, D.M.; Pereira, N.G.; Jelinek, G.A. Physical Activity and Associated Levels of Disability and Quality of Life in People with Multiple Sclerosis: A Large International Survey. BMC Neurol. 2014, 14, 143–153. [Google Scholar]
- Kieseier, B.C.; Pozzilli, C. Assessing Walking Disability in Multiple Sclerosis. Mult. Scler. 2012, 18, 914–924. [Google Scholar] [CrossRef] [PubMed]
- Song, M.; Carroll, D.D.; Lee, S.M.; Fulton, J.E. Physical Activities of U.S. High School Students, National Youth Physical Activity and Nutrition Survey, 2010. Phys. Act. Health 2014. [Google Scholar] [CrossRef]
- Vanhees, L.; Lefevre, J.; Philippaerts, R.; Martens, M.; Huygens, W.; Troosters, T.; Beunen, G. How to Assess Physical Activity? How to Assess Physical Fitness? Eur. J. Cardiovasc. Prev. Rehabil. 2005, 12, 102–114. [Google Scholar] [CrossRef]
- Müller, C.; Winter, C.; Rosenbaum, D. Current Objective Techniques for Physical Activity Assessment in Comparison with Subjective Methods. Dtsch. Z. Sportmed. 2010, 61, 11–18. (In German) [Google Scholar]
- Broderick, J.M.; Ryan, J.; O’Donnell, D.M.; Hussey, J. A Guide to Assessing Physical Activity Using Accelerometry in Cancer Patients. Support Care Cancer 2014, 22, 1121–1130. [Google Scholar] [CrossRef] [PubMed]
- Bassett, D.R. Device-Based Monitoring in Physical Activity and Public Health Research. Physiol. Meas. 2012, 33, 1769–1783. [Google Scholar] [CrossRef] [PubMed]
- Reilly, J.J.; Penpraze, V.; Hislop, J.; Davies, G.; Grant, S.; Paton, J.Y. Objective Measurement of Physical Activity and Sedentary Behaviour: Review with New Data. Arch. Dis. Child. 2008, 93, 614–619. [Google Scholar] [CrossRef] [PubMed]
- Ward, D.S.; Evenson, K.R.; Vaughn, A.; Rodgers, A.B.; Troiano, R.P. Accelerometer Use in Physical Activity: Best Practices and Research Recommendations. Med. Sci. Sports Exerc. 2005, 37, S582–S588. [Google Scholar] [CrossRef] [PubMed]
- Harding, P.; Holland, A.E.; Delany, C.; Hinman, R.S. Do Activity Levels Increase after Total Hip and Knee Arthroplasty? Clin. Orthop. Relat. Res. 2014, 472, 1502–1511. [Google Scholar] [CrossRef] [PubMed]
- Kaushal, N.; Rhodes, R.E. The Home Physical Environment and its Relationship with Physical Activity and Sedentary Behavior: A Systematic Review. Prev. Med. 2014, 67, 221–237. [Google Scholar] [CrossRef] [PubMed]
- Tan, V.P.; Macdonald, H.M.; Kim, S.; Nettlefold, L.; Gabel, L.; Ashe, M.C.; McKay, H.A. Influence of Physical Activity on Bone Strength in Children and Adolescents: A Systematic Review and Narrative Synthesis. J. Bone. Miner. Res. 2014, 29, 2061–2081. [Google Scholar] [CrossRef]
- Benedetti, M.G.; Berti, L.; Frizziero, A.; Ferrarese, D.; Giannini, S. Functional Recovery after Hip Resurfacing and Rehabilitation. J. Sport Rehabil. 2012, 21, 167–174. [Google Scholar] [PubMed]
- Weber, T.; Dendorfer, S.; Dullien, S.; Grifka, J.; Verkerke, G.J.; Renkawitz, T. Measuring Functional Outcome after Total Hip Replacement with Subject-Specific Hip Joint Loading. Proc. Inst. Mech. Eng. H. 2012, 226, 939–946. [Google Scholar] [CrossRef] [PubMed]
- Sinha, A.; Twycross-Lewis, R.; Small, C.; Morrissey, D.; Maffulli, N. Motion Analysis as an Outcome Measure for Hip Arthroplasty. Surgeon 2011, 9, 284–291. [Google Scholar] [CrossRef] [PubMed]
- Djurić-Jovičić, M.D.; Jovičić, N.S.; Popović, D.B. Kinematics of Gait: New Method for Angle Estimation Based on Accelerometers. Sensors 2011, 11, 10571–10585. [Google Scholar] [CrossRef] [PubMed]
- Favre, J.; Jolles, B.M.; Aissaoui, R.; Aminian, K. Ambulatory Measurement of 3D Knee Joint Angle. J. Biomech. 2008, 41, 1029–1035. [Google Scholar] [CrossRef] [PubMed]
- Schulze, M.; Calliess, T.; Gietzelt, M.; Wolf, K.H.; Liu, T.H.; Seehaus, F.; Bocklage, R.; Windhagen, H.; Marschollek, M. Development and Clinical Validation of an Unobtrusive Ambulatory Knee Function Monitoring System with Inertial 9DoF Sensors. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2012, 2012, 1968–1971. [Google Scholar] [PubMed]
- Seel, T.; Raisch, J.; Schauer, T. IMU-Based Joint Angle Measurement for Gait Analysis. Sensors 2014, 14, 6891–6909. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Inoue, Y.; Shibata, K. Development of a Wearable Sensor System for Quantitative Gait Analysis. Measurement 2009, 42, 978–988. [Google Scholar] [CrossRef]
- Liu, T.; Inoue, Y.; Shibata, K. A Wearable Ground Reaction Force Sensor System and its Application to the Measurement of Extrinsic Gait Variability. Sensors 2010, 10, 10240–10255. [Google Scholar] [CrossRef] [PubMed]
- Schepers, H.M.; van Asseldonk, E.; Chris, T.M.B.; Peter, H.V. Ambulatory Estimation of Foot Placement during Walking Using Inertial Sensors. J. Biomech. 2010, 43, 3138–3143. [Google Scholar] [CrossRef] [PubMed]
- Bamberg, S.J.M.; Benbasat, A.Y.; Scarborough, D.M.; Krebs, D.E.; Paradiso, J.A. Gait Analysis Using a Shoe-Integrated Wireless Sensor System. IEEE Trans. Inf. Technol. Biomed. 2008, 12, 413–423. [Google Scholar] [CrossRef] [PubMed]
- Tao, W.; Liu, T.; Zheng, R.; Feng, H. Gait Analysis Using Wearable Sensors. Sensors 2012, 12, 2255–2283. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, D.F.; Gaston, P.; Simpson, A.H. Is Patient Reporting of Physical Function Accurate Following Total Knee Replacement? J. Bone. Joint. Surg. Br. 2012, 94, 1506–1510. [Google Scholar] [CrossRef] [PubMed]
- Lord, S.; Galna, B.; Rochester, L. Moving Forward on Gait Measurement: Toward a More Refined Approach. Mov. Disord. 2013, 28, 1534–1543. [Google Scholar] [CrossRef] [PubMed]
- Holm, B.; Bandholm, T.; Lunn, T.H.; Husted, H.; Aalund, P.K.; Hansen, T.B.; Kehlet, H. Role of Preoperative Pain, Muscle Function, and Activity Level in Discharge Readiness after Fast-Track Hip and Knee Arthroplasty. Acta Orthop. 2014, 85, 488–492. [Google Scholar] [CrossRef] [PubMed]
- Karantonis, D.M.; Narayanan, M.R.; Mathie, M.; Lovell, N.H.; Celler, B.G. Implementation of a Real-Time Human Movement Classifier Using a Triaxial Accelerometer for Ambulatory Monitoring. IEEE Trans. Inf. Technol. Biomed. 2006, 10, 156–167. [Google Scholar] [CrossRef] [PubMed]
- Antonsson, E.K.; Mann, R.W. The Frequency Content of Gait. J. Biomech. 1985, 18, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Godfrey, A.; Bourke, A.K.; Ólaighin, G.M.; van de Ven, P.; Nelson, J. Activity Classification Using a Single Chest Mounted Tri-Axial Accelerometer. Med. Eng. Phys. 2011, 33, 1127–1135. [Google Scholar] [CrossRef] [PubMed]
- Higgins, W.T. A Comparison of Complementary and Kalman Filtering. IEEE Trans. Aerosp. Electron. Syst. 1975, 11, 321–325. [Google Scholar] [CrossRef]
- Lyons, G.M.; Culhane, K.M.; Hilton, D.; Grace, P.A.; Lyons, D. A Description of an Accelerometer-Based Mobility Monitoring Technique. Med. Eng. Phys. 2005, 27, 497–504. [Google Scholar] [CrossRef] [PubMed]
- Culhane, K.M.; Lyons, G.M.; Hilton, D.; Grace, P.A.; Lyons, D. Long-Term Mobility Monitoring of Older Adults Using Accelerometers in a Clinical Environment. Clin. Rehabil. 2004, 18, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Noh, Y.H.; Jeong, D.U. Implementation of Fuzzy-Rule Based Activity Classification and Optimized Adaptive Filter-Set for Wearable ECG Recording. IJMUE 2012, 7, 59–72. [Google Scholar]
- Ying, H.; Silex, C.; Schnitzer, A.; Leonhardt, S.; Schiek, M. Automatic Step Detection in the Accelerometer Signal. In 4th International Workshop on Wearable and Implantable Body Sensor Networks (BSN 2007); Springer: Berlin/Heidelberg, Germany; pp. 80–85.
- Pan, J.; Tompkins, W.J. A Real-Time QRS Detection Algorithm. IEEE Trans. Biomed. Eng. 1985, 32, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Marschollek, M.; Goevercin, M.; Wolf, K.-H.; Song, B.; Gietzelt, M.; Haux, R.; Steinhagen-Thiessen, E. A Performance Comparison of Accelerometry-Based Step Detection Algorithms on a Large, Non-Laboratory Sample of Healthy and Mobility-Impaired Persons. IEEE Eng. Med. Biol. Soc. Conf. Proc. 2008, 2008, 1319–1322. [Google Scholar]
- Cohen, J. A Coefficient of Agreement for Nominal Scales. Educ. Psychol. Meas. 1960, 20, 37–46. [Google Scholar] [CrossRef]
- Congalton, R.G. A Review of Assessing the Accuracy of Classifications of Remotely Sensed Data. Remote Sens. Environ. 1991, 37, 35–46. [Google Scholar] [CrossRef]
- Hein, A.; Kirste, T. Generic Performance Metrics for Continuous Activity Recognition. In KI 2011: Advances in Artificial Intelligence; Hutchison, D., Kanade, T., Kittler, J., Kleinberg, J.M., Mattern, F., Mitchell, J.C., Naor, M., Nierstrasz, O., Pandu, R.C., Steffen, B., et al., Eds.; Springer: Berlin/Heidelberg, Germany, 2011; pp. 139–143. [Google Scholar]
- Grant, P.M.; Ryan, C.G.; Tigbe, W.W.; Granat, M.H. The Validation of a Novel Activity Monitor in the Measurement of Posture and Motion during Everyday Activities. Br. J. Sports Med. 2006, 40, 992–997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kozey-Keadle, S.; Libertine, A.; Lyden, K.; Staudenmayer, J.; Freedson, P.S. Validation of Wearable Monitors for Assessing Sedentary Behavior. Med. Sci. Sports Exerc. 2011, 43, 1561–1567. [Google Scholar] [CrossRef] [PubMed]
- Ryan, C.G.; Grant, P.M.; Tigbe, W.W.; Granat, M.H. The Validity and Reliability of a Novel Activity Monitor as a Measure of Walking. Br. J. Sports Med. 2006, 40, 779–784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrington, D.M.; Welk, G.J.; Donnelly, A.E. Validation of MET Estimates and Step Measurement Using the ActivPAL Physical Activity Logger. J. Sports Sci. 2011, 29, 627–633. [Google Scholar] [CrossRef] [PubMed]
- Stief, F.; Bohm, H.; Michel, K.; Schwirtz, A.; Doderlein, L. Reliability and Accuracy in Three-Dimensional Gait Analysis: A Comparison of Two Lower Body Protocols. J. Appl. Biomech. 2013, 29, 105–111. [Google Scholar] [PubMed]
- Zheng, H.; Black, N.D.; Harris, N.D. Position-Sensing Technologies for Movement Analysis in Stroke Rehabilitation. Med. Biol. Eng. Comput. 2005, 43, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Nägerl, H.; Kubein-Meesenburg, D.; Cotta, H.; Fanghänel, J. Biomechanische Prinzipien in Diarthrosen und Synarthrosen. Teil III: Mechanik des Tibiofemoralgelenkes und Rolle der Kreuzbänder. Z. Orthop. Ihre. Grenzgeb. 1993, 131, 385–396. (In German) [Google Scholar] [CrossRef]
- Lafortune, M.A.; Cavanagh, P.R.; Sommer, H.J.; Kalenak, A. Three-Dimensional Kinematics of the Human Knee during Walking. J. Biomech. 1992, 25, 347–357. [Google Scholar] [CrossRef] [PubMed]
- Ramsey, D.K.; Wretenberg, P.F. Biomechanics of the Knee: Methodological Considerations in the in Vivo Kinematic Analysis of the Tibiofemoral and Patellofemoral Joint. Clin. Biomech. 1999, 14, 595–611. [Google Scholar] [CrossRef]
- Reinschmidt, C.; van den Bogert, A.J.; Nigg, B.M.; Lundberg, A.; Murphy, N. Effect of Skin Movement on the Analysis of Skeletal Knee Joint Motion during Running. J. Biomech. 1997, 30, 729–732. [Google Scholar] [CrossRef] [PubMed]
- Benoit, D.L.; Ramsey, D.K.; Lamontagne, M.; Xu, L.; Wretenberg, P.; Renström, P. Effect of Skin Movement Artifact on Knee Kinematics during Gait and Cutting Motions Measured in Vivo. Gait Posture 2006, 24, 152–164. [Google Scholar] [CrossRef] [PubMed]
- Benedetti, M.G.; Di Gioia, A.; Conti, L.; Berti, L.; Degli Esposti, L.; Tarrini, G.; Melchionda, N.; Giannini, S. Physical Activity Monitoring in Obese People in the Real Life Environment. J. Neuroeng. Rehabil. 2009, 6, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Morlock, M.; Schneider, E.; Bluhm, A.; Vollmer, M.; Bergmann, G.; Müller, V.; Honl, M. Duration and Frequency of Every Day Activities in Total Hip Patients. J. Biomech. 2001, 34, 873–881. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feldhege, F.; Mau-Moeller, A.; Lindner, T.; Hein, A.; Markschies, A.; Zettl, U.K.; Bader, R. Accuracy of a Custom Physical Activity and Knee Angle Measurement Sensor System for Patients with Neuromuscular Disorders and Gait Abnormalities. Sensors 2015, 15, 10734-10752. https://doi.org/10.3390/s150510734
Feldhege F, Mau-Moeller A, Lindner T, Hein A, Markschies A, Zettl UK, Bader R. Accuracy of a Custom Physical Activity and Knee Angle Measurement Sensor System for Patients with Neuromuscular Disorders and Gait Abnormalities. Sensors. 2015; 15(5):10734-10752. https://doi.org/10.3390/s150510734
Chicago/Turabian StyleFeldhege, Frank, Anett Mau-Moeller, Tobias Lindner, Albert Hein, Andreas Markschies, Uwe Klaus Zettl, and Rainer Bader. 2015. "Accuracy of a Custom Physical Activity and Knee Angle Measurement Sensor System for Patients with Neuromuscular Disorders and Gait Abnormalities" Sensors 15, no. 5: 10734-10752. https://doi.org/10.3390/s150510734
APA StyleFeldhege, F., Mau-Moeller, A., Lindner, T., Hein, A., Markschies, A., Zettl, U. K., & Bader, R. (2015). Accuracy of a Custom Physical Activity and Knee Angle Measurement Sensor System for Patients with Neuromuscular Disorders and Gait Abnormalities. Sensors, 15(5), 10734-10752. https://doi.org/10.3390/s150510734