1. Introduction
Access control systems using fingerprint, face, and iris biometric authentications [
1] are extensively applied, but some issues, such as privacy and cost, still need to be addressed. Recently, security-related studies have shown a tendency to focus on realistic electrocardiogram (ECG or EKG) identifications/verifications for access control.
An ECG is a voltage variation signal that detects the electrical changes of the heart on the skin which are caused when the heart muscle depolarizes during each heartbeat.
The purpose of this paper is to propose a statistical-based algorithm using the reduced binary pattern (RBP) for human identity recognition. The suggested algorithm meets the accuracy and cost requirements in an ECG verification system. Any ECG signal will first be converted into concise binary patterns and then statistical counting and ranking processes follow for verification purposes. Its advantages will be illustrated as follows:
Signal preprocessing, such as de-noising, adjusting signal means, and so on, can be totally neglected. The noise can simply be viewed as one verification feature.
Unlike other published methods, ECG QRS (Quantitative Regression Swedish) detection can be waived completely in our scheme. The algorithm can be performed directly and still maintains robustness to dynamic variation of ECG signals.
Variations in length and sampling rates of matching signals are absolutely allowed.
The algorithm requires less ECG information content and performs in a timely manner with low computational complexity. It does not need ECG information content like R-R intervals, mean and variation of ECG signals, and so on.
The remaining parts of the paper are organized as follows. An overview of related works on ECG verification is presented in
Section 2; the outline of the proposed algorithm is introduced in
Section 3, followed by a detailed description; the experimental results are shown and discussed in Section IV; and some concluding remarks are drawn in Section V.
2. Related Studies
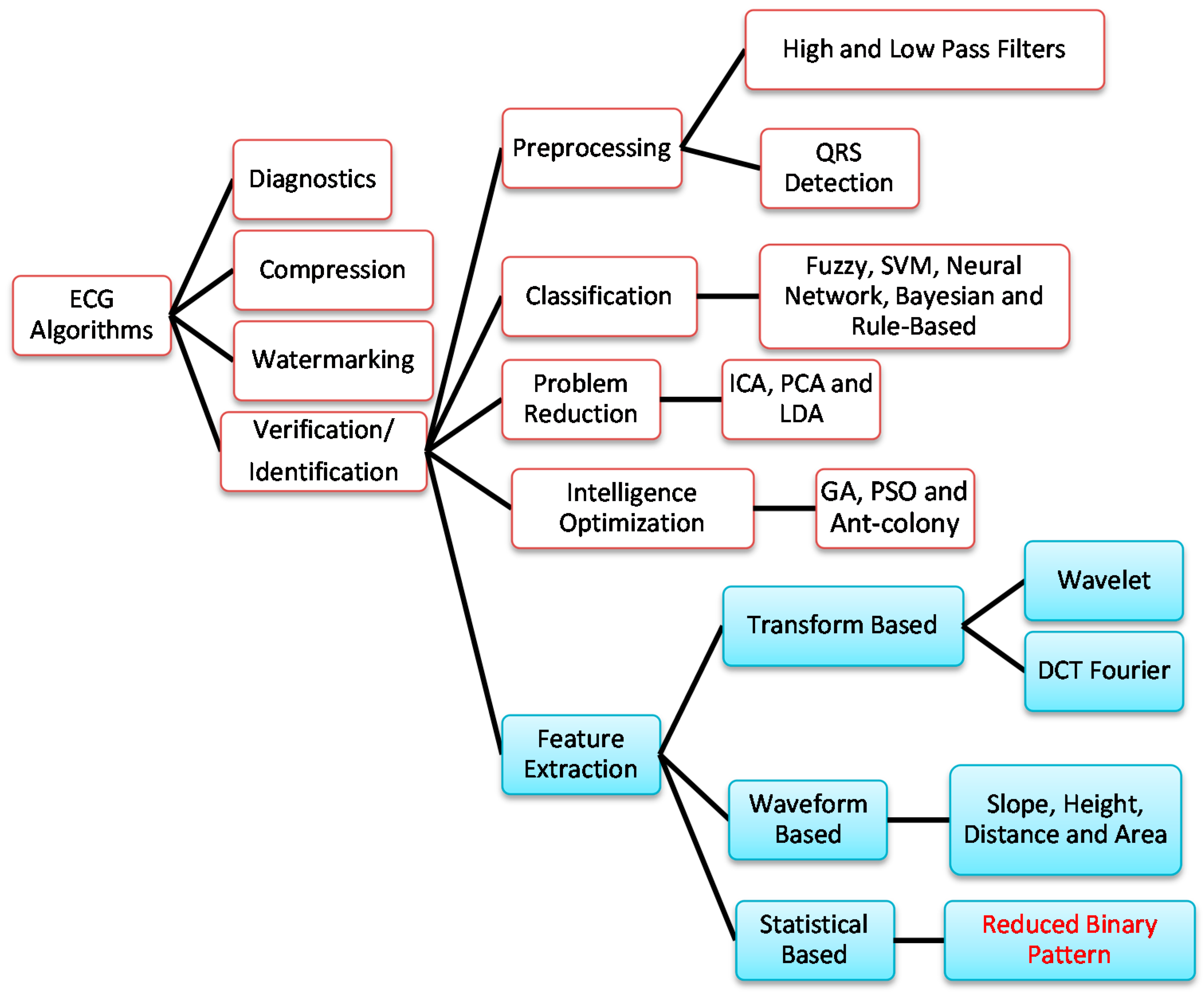
The classification of ECG algorithms is shown in
Figure 1. In this figure, FFT and DCT denote the fast Fourier transform and discrete cosine transform, respectively; SVM denotes the support vector machine; ICA, PCA, and LDA denote independent component analysis, principal component analysis, and linear discriminant analysis, respectively; GA and PSO denote genetic algorithm and particle swarm optimization, respectively. In addition to ECG-based diagnostics for heart diseases [
2,
3], ECG has also been applied to data compression [
4,
5,
6], information watermarking [
7,
8], and human verification/identification [
9,
10,
11,
12,
13,
14,
15,
16,
17,
18,
19,
20,
21,
22,
23].
Signal pre-processing, feature extraction, data classification, data reduction, and intelligence optimization are the key research focuses in human identification/verification. High- and low-pass filters and QRS detection are the main schemes employed in signal preprocessing, while fuzzy rule [
24], SVM [
13], neural network [
2], Bayesian [
25], and rule-based [
26] algorithms are frequently adopted in data classification. For data reduction, ICA [
27], PCA [
17], and LDA [
28] have been used in ECG signal processing. Intelligence optimization techniques such as GA [
29], PSO, ant-colony, and so on are commonly utilized for tuning the parameters of the aforementioned algorithms.
Figure 1.
The classification of ECG algorithms.
Figure 1.
The classification of ECG algorithms.
Most ECG-based human identification/verification methods rely on feature extraction derived from the ECG signals. The features are usually extracted according to three models: transform-based, waveform-based, and statistical-based.
The transform-based algorithms consist of wavelet transforms [
9,
10,
11,
12,
13,
14] and frequency domain transforms, including Fourier transform [
15] or DCT [
16]. Since the wavelet transform contains information in the time and frequency domain, it is more popular than the frequency domain transform.
Correlation coefficients and measurements of wavelet distances have been used in matching acquired ECG signals and modules [
9]. Since this identification/verification method requires heavy calculation, its implementation is restricted in the statistical sense. The feature selection algorithm in [
12] applied the feature set evaluation (FSE) k-nearest neighbor (k-NN) algorithm to improve low recognition rates and used the eigenspace method to reduce data dimensions; however, this approach is both complicated and time-consuming. In [
13], morphological characteristics are first extracted through the wavelet transform and the independent component analysis; SVM follows for identification/verification purposes. Although a high identification rate could be reached, a lengthy feature extraction process seems unavoidable.
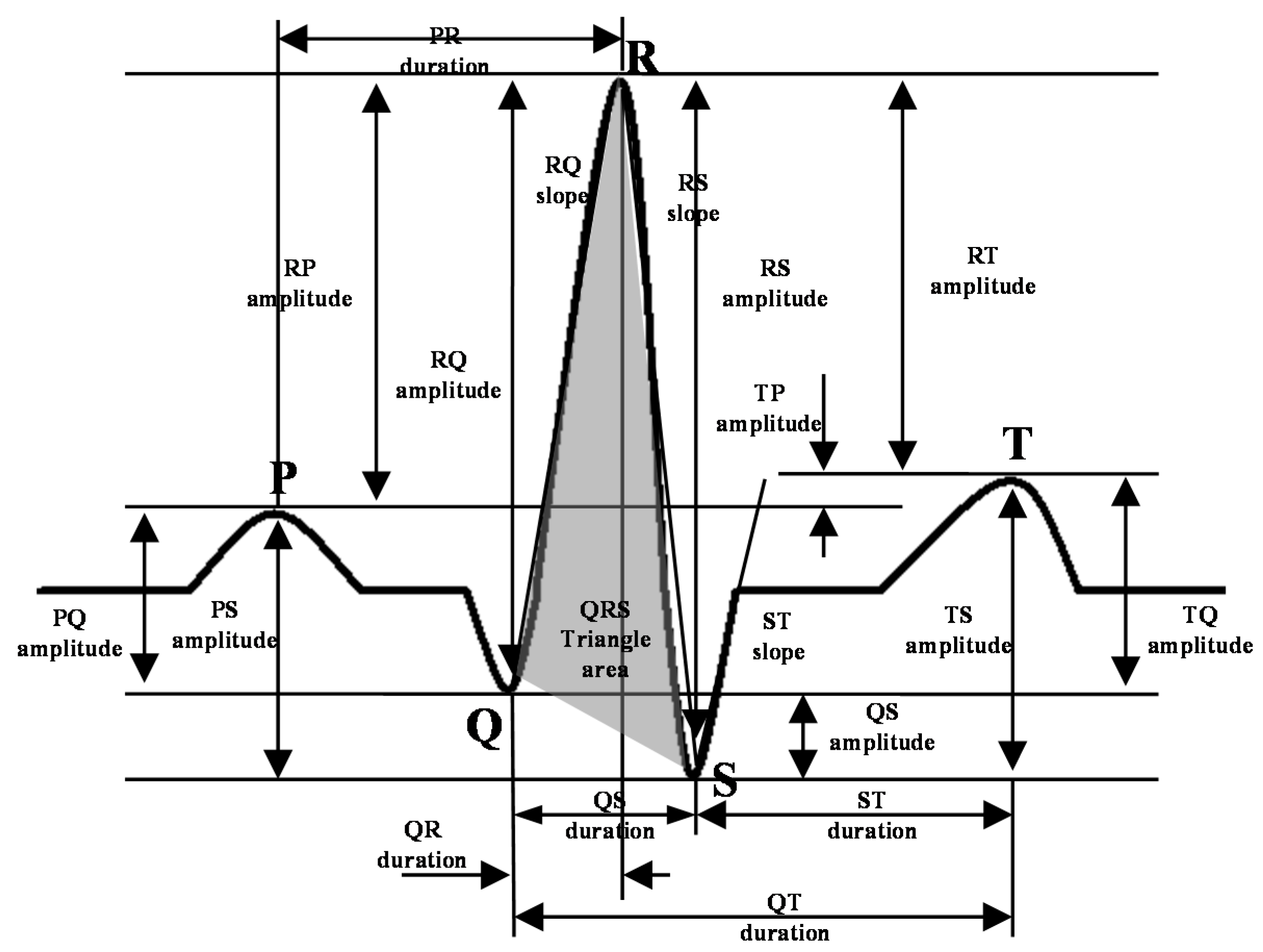
Waveform-based algorithms [
17,
18,
19,
20,
21,
22,
23] extract different time domain characteristics (distance, height, and area) from fiducial points inside the ECG waveform. These waveform descriptors will be used to match or classify ECG signals in the identification/verification process. These algorithms usually have good accuracy in recognizing regular ECG signals but show opposite results for irregular data.
Some researchers combined a precision-matched result with a waveform neural network in the signal preprocessing stage [
18]. This model extracted seven features from the ECG signals based on their amplitude and the interval to be analyzed by the decision-based neural network. The computational complexity depends heavily on the forms of those time-domain ECG signals and the level of difficulty of the matching process carried out by the neural network. Nineteen characteristics are extracted from the time interval, amplitude, and angle of deflection and studied [
22]; the identification is examined using Euclidian distances and an adaptive threshold. The eigenvectors used in feature-matching take time but are necessary for all band waves in the ECG signals.
An ECG signal can be described as a non-stationary time series that presents some irregularities in the waveform. Unlike the waveform-based algorithms, the transform-based algorithms analyze the non-stationary information based on the signal’s presentation in the frequency domain. Not only is this process slow, but it is also difficult to extract good features for the purpose of identification.
Statistical-based algorithms usually depend on statistical evaluations (count, mean, and variance) of human identification. They are usually less time-consuming but definitely need a well-designed statistical model to assure high-quality accuracy. A method based on rank order statistics was presented to analyze the human heart beat [
30].
The non-stationary behavior of ECG has been utilized in many studies. The fetal ECG was reconstructed with higher-order statistical tools exploiting ECG non-stationary properties associated with post-de-noising wavelets [
27]. A de-trended fluctuation analysis to quantify the correlation property in the non-stationary physiological time series was presented [
31]. Our previous work for an ECG card access control system [
32] focused on the architecture in ECG human identification.
Compared with algorithms presented in the literature, our proposed scheme is capable of providing secure and accurate results with a user-possessed controller. Moreover, it can be easily embedded into the field application structure to ensure the implementation of a feasible ECG identification hardware.
3. System Architecture and Application Example
Even though some ECG biometric identifications have been demonstrated, there is a serious issue regarding the use of a centralized ECG database. Due to implementation cost and accuracy issues, there is not yet a feasible application. In our previous work [
32], we put this idea into practice and introduced a portable ECG card for access control. This small ECG card provides a cheap and convenient way to enhance door access security.
An ECG access control system consists of a personal ECG sensor card and an access control device. An ECG card is a small device for storing personal ECG data and will be useful for identity recognition. As suggested in
Figure 2, applications of ECG cards include secure personal keys to open cars, houses, deposit boxes, and mobile phones.
Figure 2.
Application diagram of ECG sensor card for human verification.
Figure 2.
Application diagram of ECG sensor card for human verification.
The following advantages mean that the ECG approach outperforms the most popular fingerprint approach.
The ECG signal is not visible and photo-copying is impossible. Replication of ECG signals is more difficult.
ECG data can be measured only by a smaller, low-power-consumption, low-cost, simple circuit.
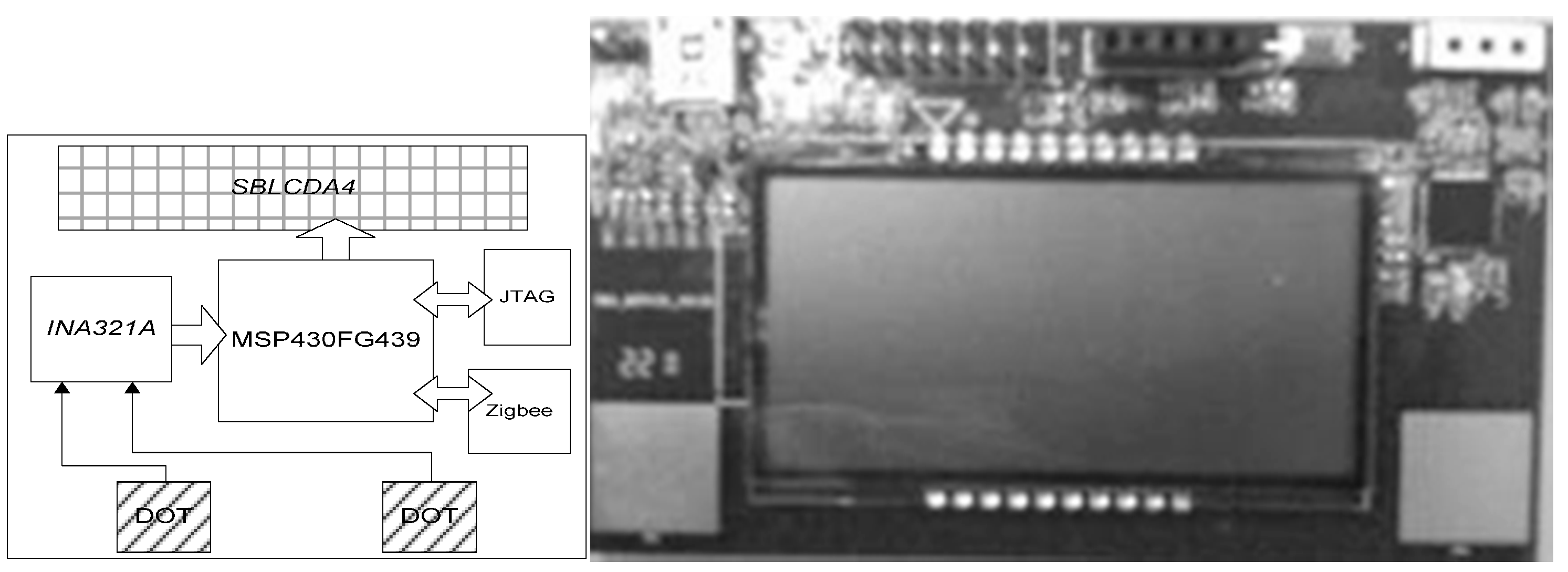
The blueprint of the architecture of an ECG sensor card is shown on the left of
Figure 3. Data are obtained through a contact pad (denoted by “DOT”), and the processing unit, the integrated chip “INA321A”, is in charge of common mode noise removal from the original signal. The main processing unit, the integrated microprocessor “MSP430FG439”, controls and transmits all data to the ZigBee module, a short-range wireless transmission module that communicates with the access control device. The other modules include “SBLCDA4” and “JTAG”, which will be used for LCD (Liquid Crystal Display) display and debugging the microprocessor, respectively.
Figure 3.
Architecture and hardware implementation of ECG sensor card.
Figure 3.
Architecture and hardware implementation of ECG sensor card.
One real implementation of the ECG sensor card is shown on the right of
Figure 3. An ECG card contains two voltage-sensitive contacts, noise filter modules, a microprocessor, and a wireless transmission module. This small and low-cost device allows practical ECG identification in real life.
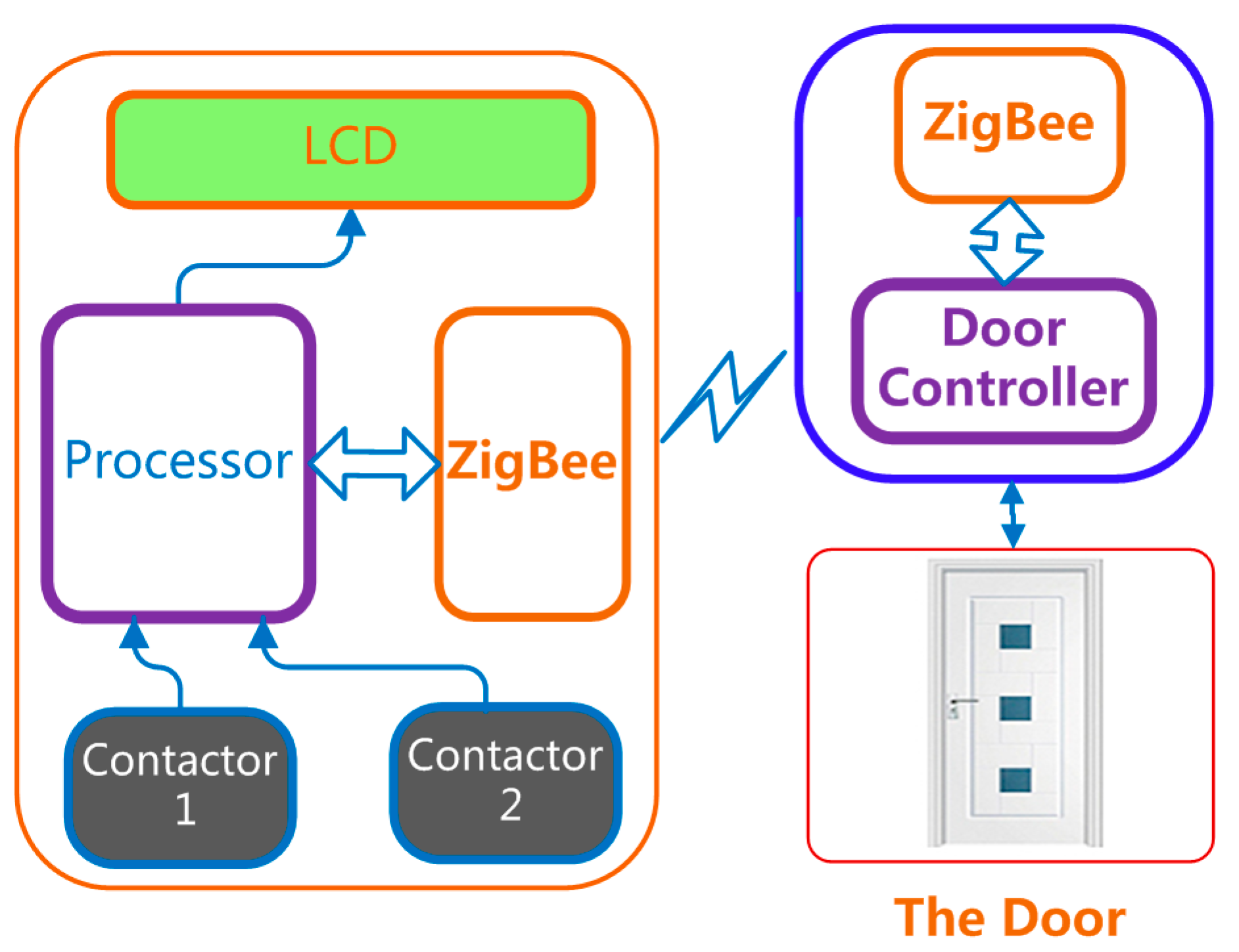
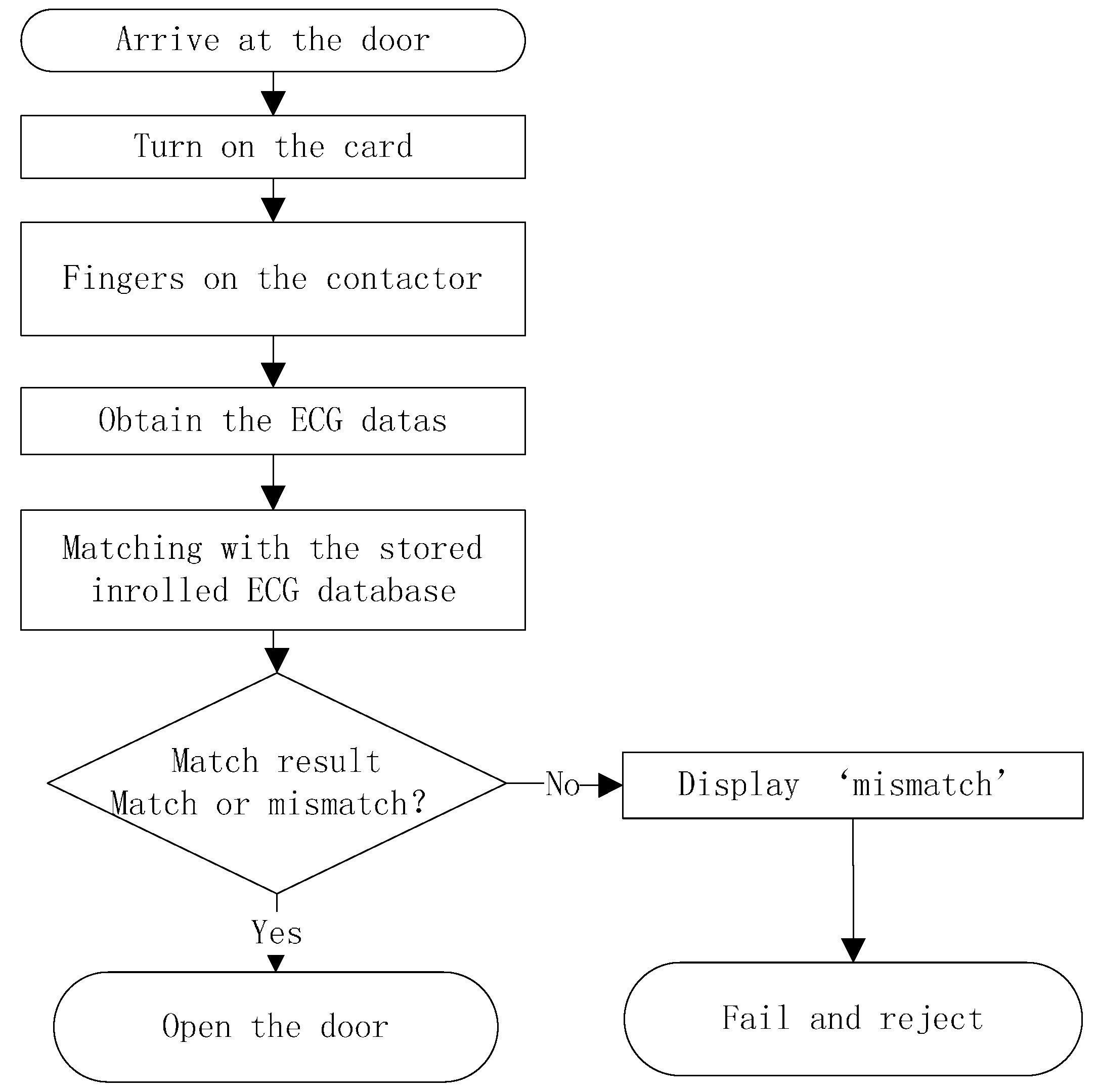
A door access control, as shown in
Figure 4, serves as one real application of ECG access cards. This card checks whether an ECG signal provided by the user matches that stored inside the card. The controller is an embedded system or personal computer connected with an ECG card via the wireless transmission module. The flowchart in
Figure 5 shows the ECG verification process in the door access control.
Figure 4.
Door access control: Application of ECG sensor card.
Figure 4.
Door access control: Application of ECG sensor card.
Figure 5.
Flow chart of ECG verification processing.
Figure 5.
Flow chart of ECG verification processing.
4. Algorithm
4.1. The Basic RBP Algorithm
The idea of our proposed algorithm, RBP for ECG verification, is related to Yang’s [
30] and Kumar’s [
33] works, but we expand it to a different field of application. The differences between Yang’s model and our model are as follows:
Their approach focuses on the human heartbeats; ours focuses on just the bare ECG signals.
They convert, count, and rank P waves in the ECG signals only; we perform these procedures on every sample of ECG data to obtain the reduced binary pattern.
They aim for heart disease classification; we focus on human identity recognition through ECG signals.
The processing in our design can be roughly divided into three necessary steps that will be illustrated as follows.
All ECG signals are non-stationary. Consider an ECG signal as
, where the real-valued
corresponds to the
input datum. Each pair of consecutive input signals is compared and the data are categorized into one of the two cases: a decrease or increase in
. A preliminary reduced function then maps these two cases to 0 or 1, respectively, according to the rule:
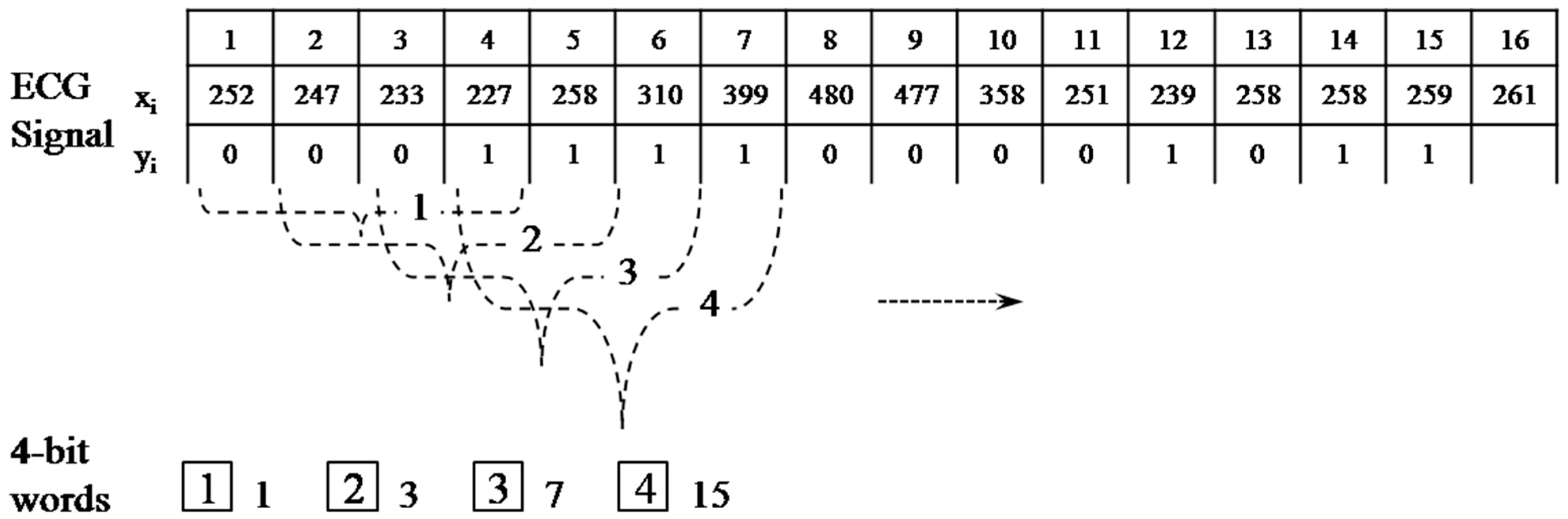
This procedure converts the ECG signal of length
to a binary sequence
of length
. Every
bits in
are grouped to construct a reduced binary sequence of length
, referred to as an m-bit word, and then all such words are collected to form a reduced binary pattern
where
. We then convert each m-bit word
to its decimal expansion
.
An example of the reduced binary pattern conversion for
is depicted in
Figure 6. For instance, the first four-bit word
is labeled as
, which equates to
.
Figure 6.
Process of the reduced binary pattern conversion.
Figure 6.
Process of the reduced binary pattern conversion.
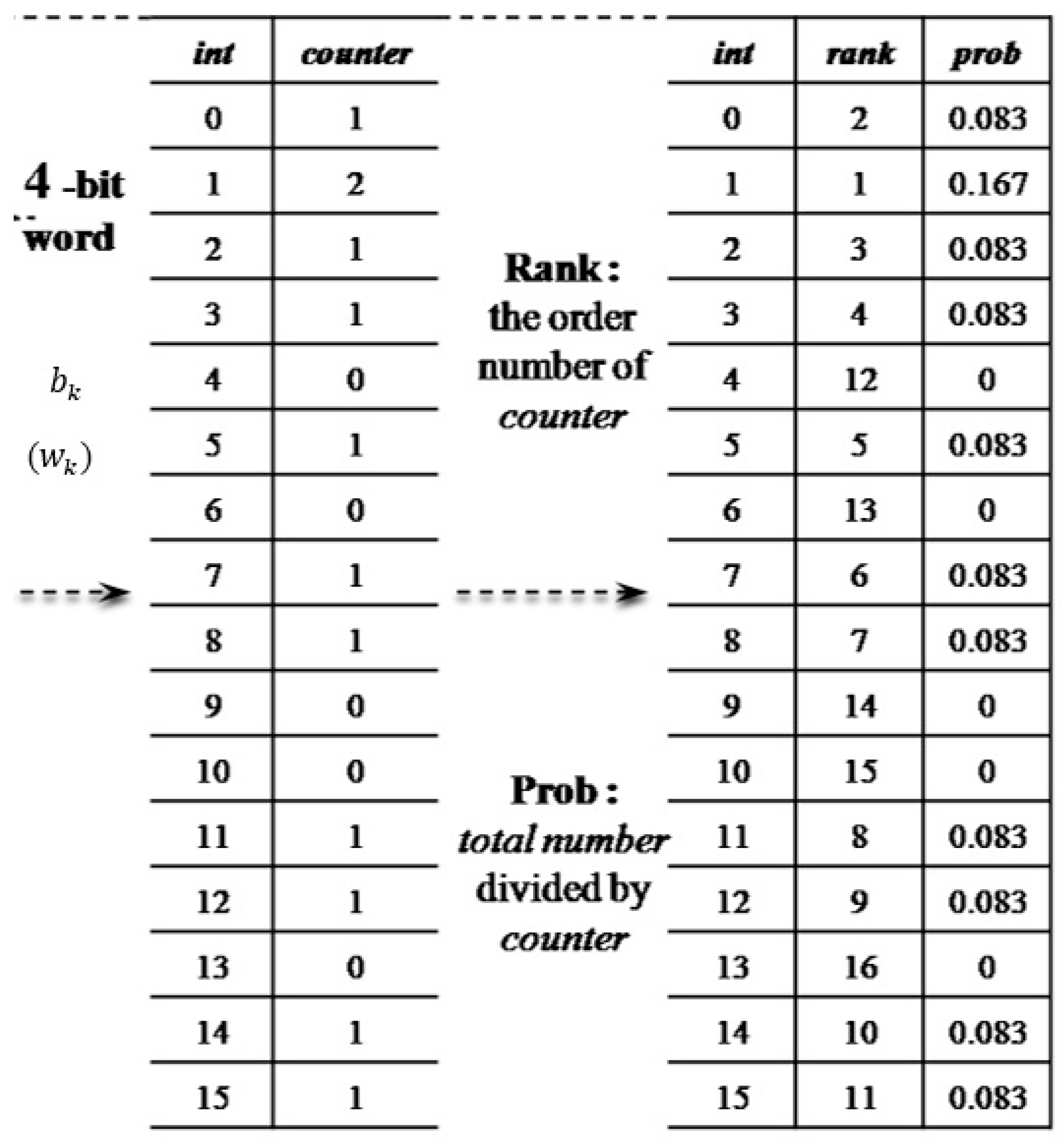
The main theme in this step, as shown in
Figure 7, is to count the occurrences of all
and sort them in order of descending frequency.
Let
be an integer for
. It is obvious that values of
range from 0 to
. Let integer
, and let
and
be the corresponding relative frequency and occurrence of
. To be exact,
and
. Next,
is ranked according to its frequency
from the largest to the smallest. For example,
means the
-bit words
, which converts to the same
as those that appear the most frequently in the reduced binary pattern.
Figure 7.
The counting and ranking process.
Figure 7.
The counting and ranking process.
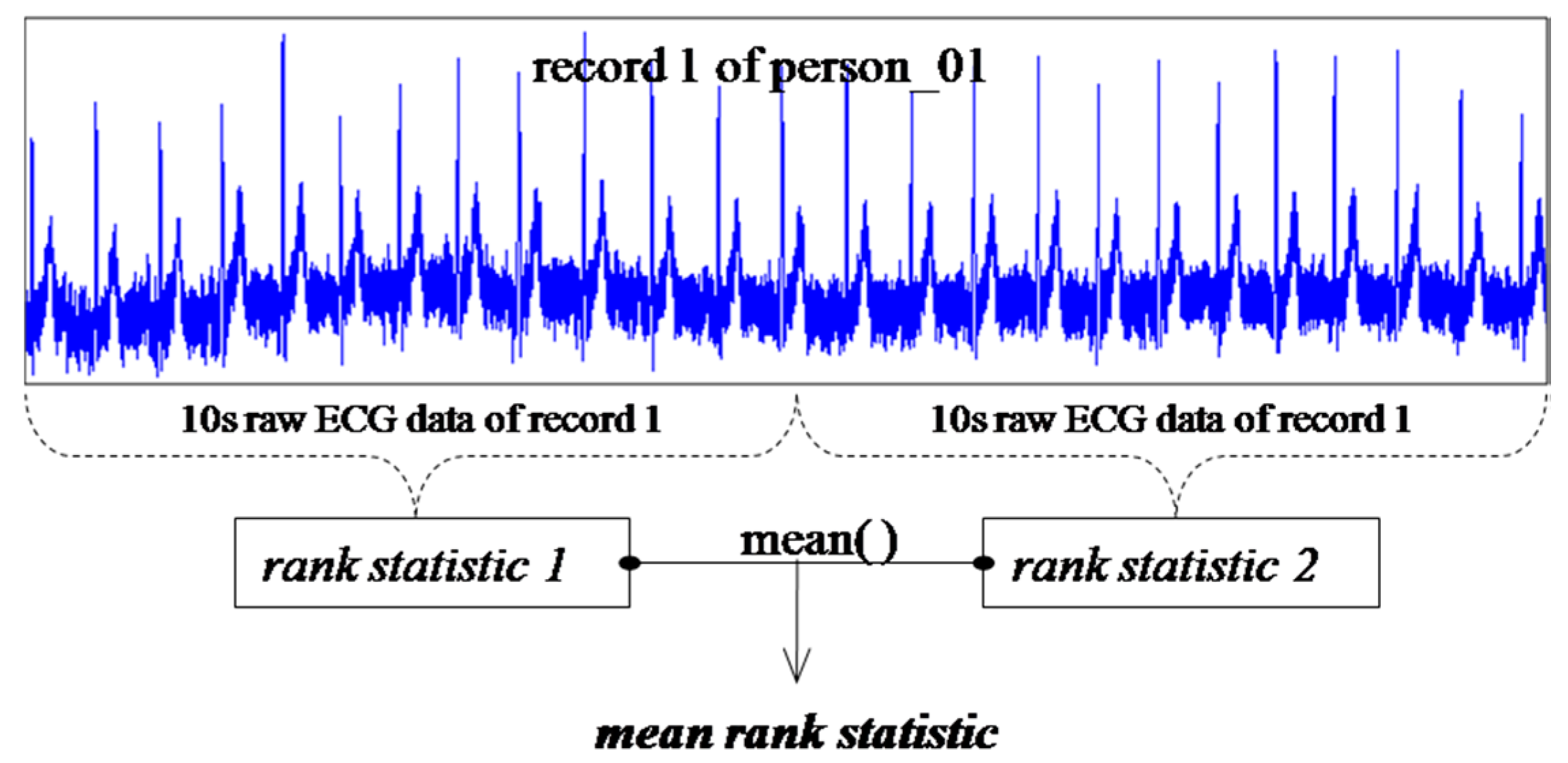
Consider two segments of ECG data
and
, which may belong to two distinct subjects. To understand how closely they are related, the measurement of similarity needs to be defined. We incorporate a weighted distance formula [
30] to measure the similarity between
and
:
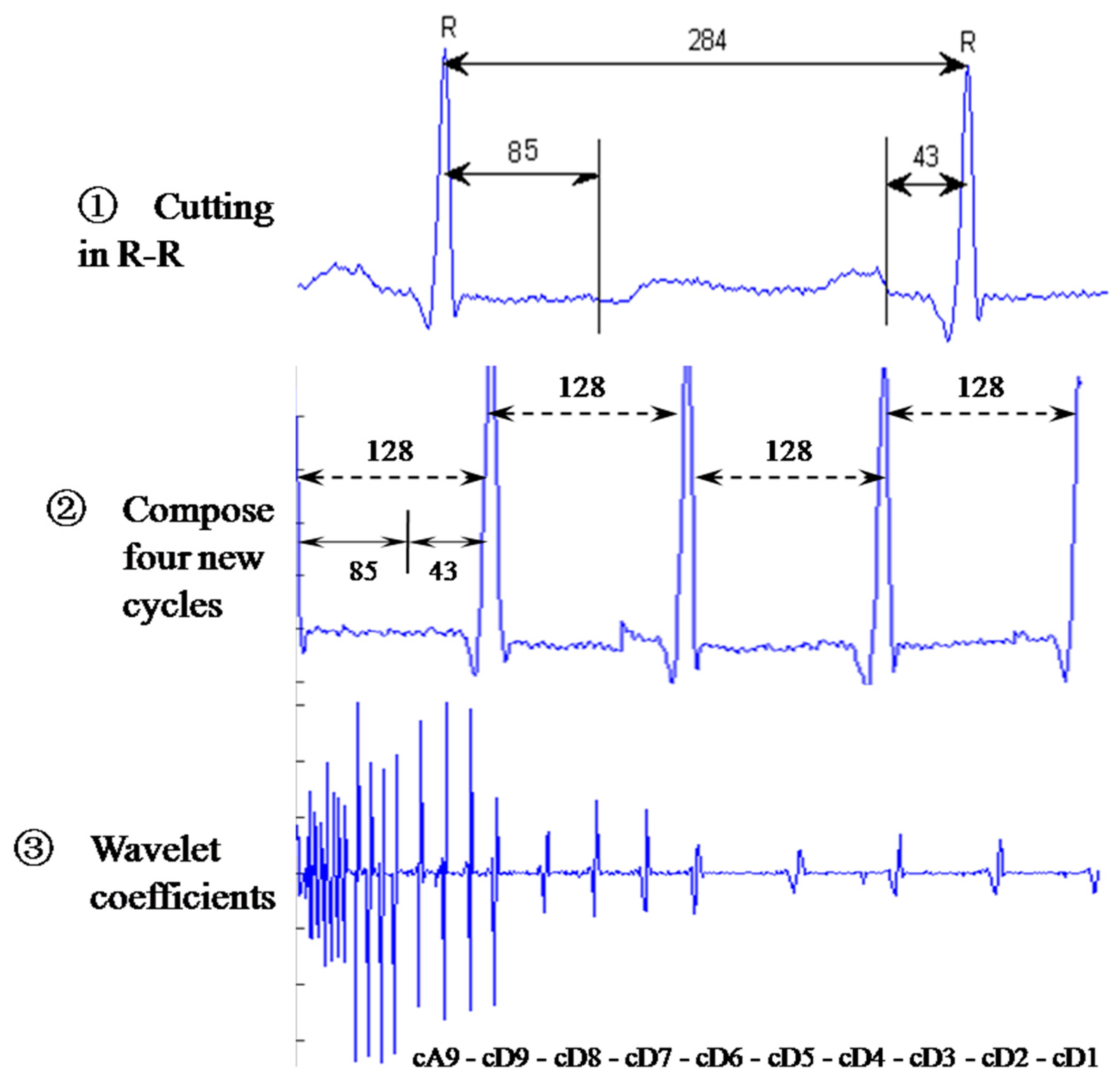
where the segment means a sequence of sampled ECG data of 10 sample periods which serves as a basic unit for our analysis. Each sample period denotes the ECG signal in an R-R interval.
and
represent the relative frequency and rank of
in the sequence
. The absolute difference between two ranks is multiplied by the normalized probabilities as a weighted sum; the factor
assures that all values of measurements lie within the scope of (0, 1).
Consider two groups of ECG data,
and
, each containing
and
segments, respectively. We define the measurement of similarity between these two groups:
where
and
are the corresponding segments from
and
, respectively;
denotes the associated distance between these segments.
is the average distance of all segments from
and
. If
,
is referred to as the intra-group distance; otherwise it is the inter-group distance.
4.2. The Advanced RBP Algorithm
Next, we consider a new scaling factor
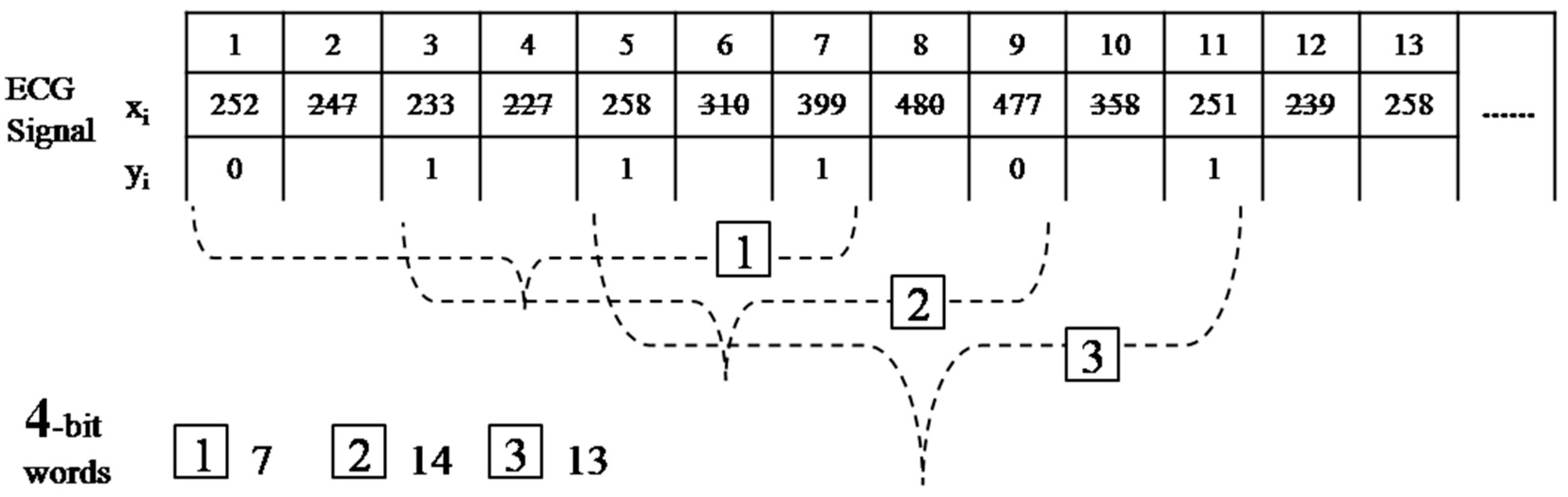
, which is an increment in the length of the interval, in the RBP algorithm. All steps in this algorithm are similar to those performed in the basic design, except that the binary sequence will be obtained from the comparison of
and
instead of
and
, where
represents the raw ECG data. The reduced function (1) is now replaced with:
Figure 8 represents the process of the modified RBP conversion of
and
. The first four-bit word
is now labeled as
.
Figure 8.
Process of the modified reduced binary pattern conversion.
Figure 8.
Process of the modified reduced binary pattern conversion.
If we are concerned with the effect of the size of variations in amplitude, the reduced function will be:
where
denotes the jump in amplitude. This model allows variation (noises) from two consecutive data points to differ by
units, which in turn reduces a small variation in amplitude by requiring a large rise in amplitude. In the case where variations in time and amplitude are allowed, the general reduced function can be set as:
A proper choice of
may reduce impacts from noises and a suitable scaling factor
could result in an ideal reduced binary pattern. Therefore, appropriate tuning of either parameter will improve the verification accuracy.
Table 1 and Algorithm 1 include notations and the main pseudo code of the advanced RBP algorithm. The main pseudo code consists of two code segments: an ECG datum
is converted to the statistical counter
and the rank values are sorted to obtain
. To expedite our computation process, an unsigned
of length
is created and each bit of σ stores the corresponding value of
. We also set
, of length
, to accumulate the repeated number of
-bit words in the reduced binary pattern.
Table 1.
Notation for the advanced RBP (Reduced Binary Pattern) pseudo code.
Table 1.
Notation for the advanced RBP (Reduced Binary Pattern) pseudo code.
| Symbols | Description |
|---|
| CT | m-bit word counter of size 2m for the reduced binary patterns |
| N | Maximum length of the ECG segment for verification |
| p | Relative frequency array |
| RK | Rank array |
| m | Number of bits in a word for the reduced binary pattern |
| x | Input ECG data |
| α | Scaling factor of interval for the reduced binary sequence |
| β | Granularity of amplitude for reduced binary function |
| θCT | The total number of m-bit words for counting |
| σ | Unsigned integer with m-bits for the purpose of shifting |
| τ | Position variable |
| Algorithm 1 Main Pseudo Code of the Advanced RBP Algorithm |
| 1: LOOP UNTIL BY |
| 2: |
| 3: IF - > |
| 4: |
| 5: IF |
| 6: ++ |
| 7: |
| 8: LOOP UNTIL |
| 9: |
| 10: LOOP UNTIL |
| 11: IF |
| 12: IF |
| 13: |
4.3. The Evolving RBP Algorithm
Since ECG signals change slightly day by day, modifying our algorithm to handle this issue seems crucial. This model utilizes an incremental learning process to improve the advanced version. The advanced RBP algorithm evolves an incremental-update mechanism for the rank order of the
-bit word
. If both ECG signals, the obtained one and the original one, come from the same individual, the identity match passes. The original relative frequency
is now replaced by the new relative frequency
from the new input ECG.
where
is the weighted factor controlling the degree of impact from the new frequency
,
. The value of
is affected by the degree of non-stationarity in the old and new ECG signals. A larger
indicates that the new data are more non-stationary and the rank
,
will then be recalculated and updated. This non-stationary behavior can be modeled by verifying the cross-correlation between these two ECG signals in the future.












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}




