
Continuous Glucose Monitoring Sensors: Past, Present and Future Algorithmic Challenges


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. The Past: The “Smart” CGM Sensor
3. The Present: The Nonadjunctive CGM Use
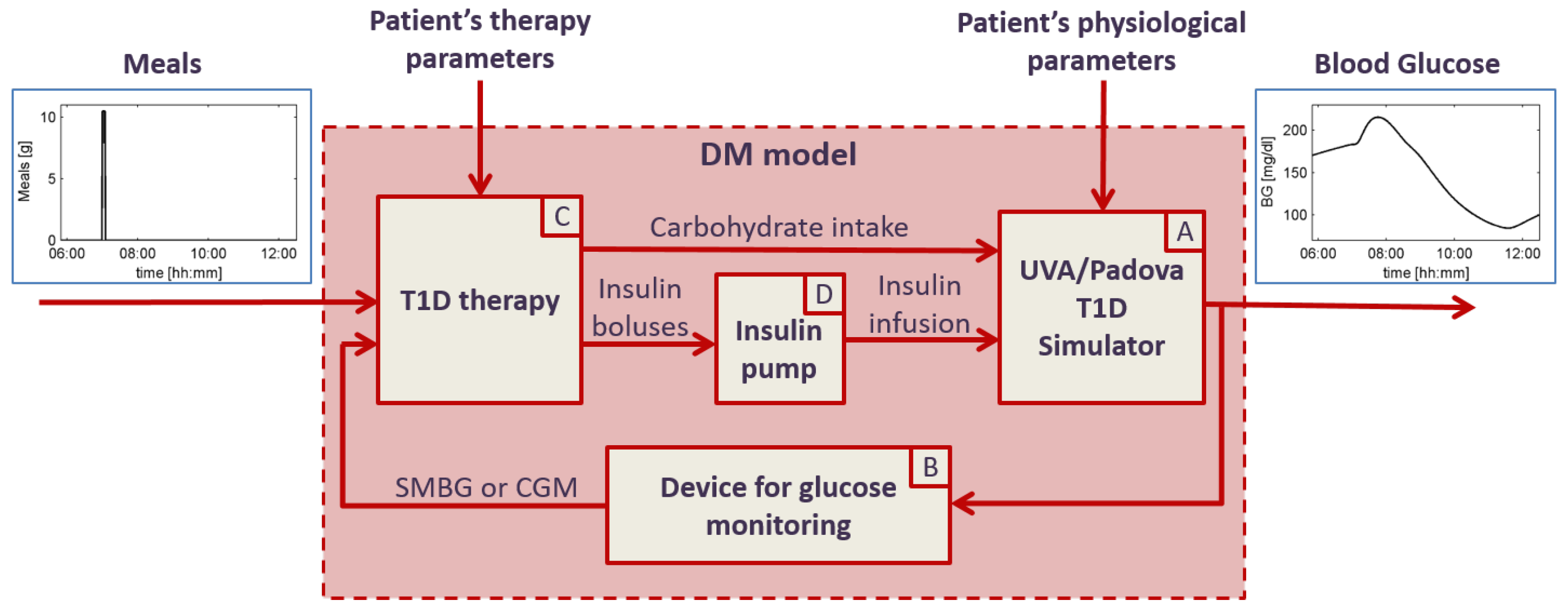
- (A)
- the UVA/Padova T1D simulator, which receives for input the physiological parameters of the specific virtual patient, the CHO intake and insulin infusion, and outputs the BG concentration profile. The UVA/Padova T1D simulator is a large-scale maximal computer model of glucose, insulin and glucagon dynamics in patients with T1D, described by 13 differential equations and provided with three different populations: 100 adult, 100 pediatric and 100 adolescent virtual subjects [52,53]. Each virtual subject is characterized by 36 physiological parameters, able to describe the inter-individual variability observed in the T1D population. The UVA/Padova T1D simulator was originally designed to generate single-meal scenarios and was accepted by the U.S. Food and Drug Administration (FDA) to substitute the pre-clinical for certain insulin treatments in 2008. Recently, thanks to the development and embedding of inter- and intra-day variability of the insulin sensitivity, the new version of the UVA/Padova T1D simulator allows for generating physiological glucose profiles of T1D on multiple-day scenarios [54,55];
- (B)
- models of SMBG and CGM devices, able to reliably reproduce all the technological variability (in terms of accuracy) that can be observed in real life. These models receive for input the BG concentration from the UVA/Padova T1D simulator and outputs the CGM and SMBG values, respectively. The SMBG measurement error is sampled from a composite distribution obtained combining a skew-normal density function, to describe the central part of the distribution, the exponential functions, and the tails [56]. The CGM sensor model is able to describe all of the key components of the sensor error, i.e., the variability of the time delay due to the BG-to-IG diffusion process, the variability of the calibration error, and the variability of the random noise component by sampling from appropriate distributions as described in depth in [57,58,59];
- (C)
- a model of treatment rules and subject behavior, able to reproduce all the variability in the habits of the diabetic patients and in their use of BG monitoring technologies [51]. Specifically, this module simulates the patient behavior in using SMBG and/or CGM information to make treatment decisions like tuning meal insulin doses and triggering correction boluses and CHO hypo rescues. The inputs of the model the SMBG and/or the CGM measurements (which includes not only the glucose readings, but also trend arrows, alerts and alarms), the meal scheduling and patient’s therapy parameters, like the CHO-to-insulin ratio (CR) and the correction factor (CF). The model outputs are insulin boluses, obtained as the sum of meal boluses and correction boluses, and CHO intake, obtained as the sum of meals’ CHO and hypotreatments;
- (D)
- the insulin pump model, which is simply an actuator receiving for input the dose of insulin boluses and outputting the insulin delivery pattern containing the minute by minute dose of insulin injected [51].
4. The Future: New Challenges
5. Conclusions
Conflicts of Interest
Abbreviations
| AP | artificial pancreas |
| BG | blood glucose |
| CF | correcton factor |
| CR | carbohydrate-to-insulin ratio |
| CGM | continuous glucose monitoring |
| CHO | carbohydrate |
| IG | interstitial glucose |
| ISCT | in silico clinical trial |
| MARD | mean absolute relative difference |
| SMBG | self-monitoring blood glucose |
| T1D | Type 1 diabetes |
| T1D-DM | Type 1 diabetes-decision making |
| UVA | University of Virginia |
References
- Gross, T.M.; Bode, B.W.; Einhorn, D.; Kayne, D.M.; Reed, J.H.; White, N.H.; Mastrototaro, J.J. Performance evaluation of the MiniMed continuous glucose monitoring system during patient home use. Diabetes Technol. Ther. 2000, 2, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Feldman, B.; Brazg, R.; Schwartz, S.; Weinstein, R. A continuous glucose sensor based on wired enzyme technology—Results from a 3-day trial in patients with type 1 diabetes. Diabetes Technol. Ther. 2003, 5, 769–779. [Google Scholar] [CrossRef] [PubMed]
- Bode, B.; Gross, K.; Rikalo, N.; Schwartz, S.; Wahl, T.; Page, C.; Gross, T.; Mastrototaro, J. Alarms based on real-time sensor glucose values alert patients to hypo- and hyperglycemia: the guardian continuous monitoring system. Diabetes Technol. Ther. 2004, 6, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Bailey, T.; Zisser, H.; Chang, A. New features and performance of a next-generation SEVEN-day continuous glucose monitoring system with short lag time. Diabetes Technol. Ther. 2009, 11, 749–755. [Google Scholar] [CrossRef] [PubMed]
- Christiansen, M.; Bailey, T.; Watkins, E.; Liljenquist, D.; Price, D.; Nakamura, K.; Boock, R.; Peyser, T. A new-generation continuous glucose monitoring system: Improved accuracy and reliability compared with a previous-generation system. Diabetes Technol. Ther. 2013, 15, 881–888. [Google Scholar] [CrossRef] [PubMed]
- Dexcom G5 Mobile. Available online: https://www.dexcom.com/g5-mobile-cgm (accessed on 23 June 2016).
- Mastrototaro, J.; Shin, J.; Marcus, A.; Sulur, G.; Abelseth, J.; Bode, B.W.; Buckingham, B.A.; Hirsch, I.B.; Kaufman, F.R.; Schwartz, S.L.; et al. The accuracy and efficacy of real-time continuous glucose monitoring sensor in patients with type 1 diabetes. Diabetes Technol. Ther. 2008, 10, 385–390. [Google Scholar] [CrossRef] [PubMed]
- Tamborlane, W.V.; Beck, R.W.; Bode, B.W.; Buckingham, B.; Chase, H.P.; Clemons, R.; Fiallo-Scharer, R.; Fox, L.A.; Gilliam, L.K.; Hirsch, I.B.; et al. Continuous glucose monitoring and intensive treatment of type 1 diabetes. N. Engl. J. Med. 2008, 359, 1464–1476. [Google Scholar] [PubMed]
- Zhao, C.; Dassau, E.; Jovanovi, L.; Zisser, H.C.; Doyle, F.J.; Seborg, D.E. Predicting subcutaneous glucose concentration using a latent-variable-based statistical method for type 1 diabetes mellitus. J. Diabetes Sci. Technol. 2012, 6, 617–633. [Google Scholar] [CrossRef] [PubMed]
- Turksoy, K.; Bayrak, E.S.; Quinn, L.; Littlejohn, E.; Rollins, D.; Cinar, A. Hypoglycemia Early Alarm Systems Based On Multivariable Models. Ind. Eng. Chem. Res. 2013, 52, 12329–12336. [Google Scholar] [CrossRef] [PubMed]
- Zarkogianni, K.; Mitsis, K.; Litsa, E.; Arredondo, M.T.; Fico, G.; Fioravanti, A.; Nikita, K.S. Comparative assessment of glucose prediction models for patients with type 1 diabetes mellitus applying sensors for glucose and physical activity monitoring. Med. Biol. Eng. Comput. 2015, 53, 1333–1343. [Google Scholar] [CrossRef] [PubMed]
- Zhao, C.; Yu, C. Rapid model identification for online subcutaneous glucose concentration prediction for new subjects with type I diabetes. IEEE Trans. Biomed. Eng. 2015, 62, 1333–1344. [Google Scholar] [CrossRef] [PubMed]
- Zecchin, C.; Facchinetti, A.; Sparacino, G.; Cobelli, C. How Much Is Short-Term Glucose Prediction in Type 1 Diabetes Improved by Adding Insulin Delivery and Meal Content Information to CGM Data? A Proof-of-Concept Study. J. Diabetes Sci. Technol. 2016, 10, 1149–1160. [Google Scholar] [CrossRef] [PubMed]
- Hughes, C.S.; Patek, S.D.; Breton, M.D.; Kovatchev, B.P. Hypoglycemia prevention via pump attenuation and red-yellow-green “traffic” lights using continuous glucose monitoring and insulin pump data. J. Diabetes Sci. Technol. 2010, 4, 1146–1155. [Google Scholar] [CrossRef] [PubMed]
- Cameron, F.; Wilson, D.M.; Buckingham, B.A.; Arzumanyan, H.; Clinton, P.; Chase, H.P.; Lum, J.; Maahs, D.M.; Calhoun, P.M.; Bequette, B.W. Inpatient studies of a Kalman-filter-based predictive pump shutoff algorithm. J. Diabetes Sci. Technol. 2012, 6, 1142–1147. [Google Scholar] [CrossRef] [PubMed]
- Weiss, R.; Garg, S.K.; Bergenstal, R.M.; Klonoff, D.C.; Bode, B.W.; Bailey, T.S.; Thrasher, J.; Schwartz, F.; Welsh, J.B.; Kaufman, F.R.; et al. Predictors of Hypoglycemia in the ASPIRE In-Home Study and Effects of Automatic Suspension of Insulin Delivery. J. Diabetes Sci. Technol. 2015, 9, 1016–1020. [Google Scholar] [CrossRef] [PubMed]
- Herrero, P.; Calm, R.; Vehi, J.; Armengol, J.; Georgiou, P.; Oliver, N.; Tomazou, C. Robust fault detection system for insulin pump therapy using continuous glucose monitoring. J. Diabetes Sci. Technol. 2012, 6, 1131–1141. [Google Scholar] [CrossRef] [PubMed]
- Facchinetti, A.; Del Favero, S.; Sparacino, G.; Cobelli, C. An online failure detection method of the glucose sensor-insulin pump system: Improved overnight safety of type-1 diabetic subjects. IEEE Trans. Biomed. Eng. 2013, 60, 406–416. [Google Scholar] [CrossRef] [PubMed]
- Baysal, N.; Cameron, F.; Buckingham, B.A.; Wilson, D.M.; Chase, H.P.; Maahs, D.M.; Bequette, B.W.; Buckingham, B.A.; Wilson, D.M.; Aye, T.; et al. A novel method to detect pressure-induced sensor attenuations (PISA) in an artificial pancreas. J. Diabetes Sci. Technol. 2014, 8, 1091–1096. [Google Scholar] [CrossRef] [PubMed]
- Turksoy, K.; Roy, A.; Cinar, A. Real-Time Model-Based Fault Detection of Continuous Glucose Sensor Measurements. IEEE Trans. Biomed. Eng. 2016. [Google Scholar] [CrossRef] [PubMed]
- Cescon, M.; DeSalvo, D.J.; Ly, T.T.; Maahs, D.M.; Messer, L.H.; Buckingham, B.A.; Doyle, F.J.; Dassau, E. Early Detection of Infusion Set Failure During Insulin Pump Therapy in Type 1 Diabetes. J. Diabetes Sci. Technol. 2016, 10, 1268–1276. [Google Scholar] [CrossRef] [PubMed]
- Bequette, B.W. Challenges and Recent Progress in the Development of a Closed-loop Artificial Pancreas. Annu. Rev. Control. 2012, 36, 255–266. [Google Scholar] [CrossRef] [PubMed]
- Peyser, T.; Dassau, E.; Breton, M.; Skyler, J.S. The artificial pancreas: Current status and future prospects in the management of diabetes. Ann. N. Y. Acad. Sci. 2014, 1311, 102–123. [Google Scholar] [CrossRef] [PubMed]
- Cobelli, C.; Renard, E.; Kovatchev, B. The artificial pancreas: A digital-age treatment for diabetes. Lancet Diabetes Endocrinol. 2014, 2, 679–681. [Google Scholar] [CrossRef]
- Thabit, H.; Hovorka, R. Coming of age: The artificial pancreas for type 1 diabetes. Diabetologia 2016, 59, 1795–1805. [Google Scholar] [CrossRef] [PubMed]
- Sparacino, G.; Facchinetti, A.; Cobelli, C. “Smart” continuous glucose monitoring sensors: On-line signal processing issues. Sensors 2010, 10, 6751–6772. [Google Scholar] [CrossRef] [PubMed]
- Facchinetti, A.; Sparacino, G.; Guerra, S.; Luijf, Y.M.; DeVries, J.H.; Mader, J.K.; Ellmerer, M.; Benesch, C.; Heinemann, L.; Bruttomesso, D.; et al. Real-time improvement of continuous glucose monitoring accuracy: the smart sensor concept. Diabetes Care 2013, 36, 793–800. [Google Scholar] [CrossRef] [PubMed]
- Facchinetti, A.; Sparacino, G.; Cobelli, C. Signal processing algorithms implementing the “smart sensor” concept to improve continuous glucose monitoring in diabetes. J. Diabetes Sci. Technol. 2013, 7, 1308–1318. [Google Scholar] [CrossRef] [PubMed]
- Facchinetti, A.; Sparacino, G.; Cobelli, C. An online self-tunable method to denoise CGM sensor data. IEEE Trans. Biomed. Eng. 2010, 57, 634–641. [Google Scholar] [CrossRef] [PubMed]
- Facchinetti, A.; Sparacino, G.; Cobelli, C. Online denoising method to handle intraindividual variability of signal-to-noise ratio in continuous glucose monitoring. IEEE Trans. Biomed. Eng. 2011, 58, 2664–2671. [Google Scholar] [CrossRef] [PubMed]
- Chase, J.G.; Hann, C.E.; Jackson, M.; Lin, J.; Lotz, T.; Wong, X.W.; Shaw, G.M. Integral-based filtering of continuous glucose sensor measurements for glycaemic control in critical care. Comput. Methods Programs Biomed. 2006, 82, 238–247. [Google Scholar] [CrossRef] [PubMed]
- Palerm, C.C.; Bequette, B.W. Hypoglycemia detection and prediction using continuous glucose monitoring-a study on hypoglycemic clamp data. J. Diabetes Sci. Technol. 2007, 1, 624–629. [Google Scholar] [CrossRef] [PubMed]
- Kuure-Kinsey, M.; Palerm, C.C.; Bequette, B.W. A dual-rate Kalman filter for continuous glucose monitoring. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2006, 1, 63–66. [Google Scholar] [PubMed]
- Mahmoudi, Z.; Dencker Johansen, M.; Christiansen, J.S.; Hejlesen, O.K. A multistep algorithm for processing and calibration of microdialysis continuous glucose monitoring data. Diabetes Technol. Ther. 2013, 15, 825–835. [Google Scholar] [CrossRef] [PubMed]
- Guerra, S.; Facchinetti, A.; Sparacino, G.; Nicolao, G.D.; Cobelli, C. Enhancing the accuracy of subcutaneous glucose sensors: A real-time deconvolution-based approach. IEEE Trans. Biomed. Eng. 2012, 59, 1658–1669. [Google Scholar] [CrossRef] [PubMed]
- Vettoretti, M.; Facchinetti, A.; Del Favero, S.; Sparacino, G.; Cobelli, C. On-line calibration of glucose sensors from the measured current by a time-varying calibration function and Bayesian priors. IEEE Trans. Biomed. Eng. 2015, 63, 1631–1641. [Google Scholar] [CrossRef] [PubMed]
- Barcelo-Rico, F.; Bondia, J.; Diez, J.L.; Rossetti, P. A multiple local models approach to accuracy improvement in continuous glucose monitoring. Diabetes Technol. Ther. 2012, 14, 74–82. [Google Scholar] [CrossRef] [PubMed]
- Barcelo-Rico, F.; Diez, J.L.; Rossetti, P.; Vehi, J.; Bondia, J. Adaptive calibration algorithm for plasma glucose estimation in continuous glucose monitoring. IEEE J. Biomed. Health Inform. 2013, 17, 530–538. [Google Scholar] [CrossRef] [PubMed]
- Kirchsteiger, H.; Zaccarian, L.; Renard, E.; del Re, L. LMI-Based Approaches for the Calibration of Continuous Glucose Measurement Sensors. IEEE J. Biomed. Health Inform. 2015, 19, 1697–1706. [Google Scholar] [CrossRef] [PubMed]
- Sparacino, G.; Zanderigo, F.; Corazza, S.; Maran, A.; Facchinetti, A.; Cobelli, C. Glucose concentration can be predicted ahead in time from continuous glucose monitoring sensor time-series. IEEE Trans. Biomed. Eng. 2007, 54, 931–937. [Google Scholar] [CrossRef] [PubMed]
- Zecchin, C.; Facchinetti, A.; Sparacino, G.; Cobelli, C. Jump neural network for online short-time prediction of blood glucose from continuous monitoring sensors and meal information. Comput. Methods Programs Biomed. 2014, 113, 144–152. [Google Scholar] [CrossRef] [PubMed]
- Georga, E.I.; Protopappas, V.C.; Ardigo, D.; Marina, M.; Zavaroni, I.; Polyzos, D.; Fotiadis, D.I. Multivariate prediction of subcutaneous glucose concentration in type 1 diabetes patients based on support vector regression. IEEE J. Biomed. Health Inform. 2013, 17, 71–81. [Google Scholar] [CrossRef] [PubMed]
- Georga, E.I.; Protopappas, V.C.; Polyzos, D.; Fotiadis, D.I. Evaluation of short-term predictors of glucose concentration in type 1 diabetes combining feature ranking with regression models. Med. Biol. Eng. Comput. 2015, 53, 1305–1318. [Google Scholar] [CrossRef] [PubMed]
- Garcia, A.; Rack-Gomer, A.L.; Bhavaraju, N.C.; Hampapuram, H.; Kamath, A.; Peyser, T.; Facchinetti, A.; Zecchin, C.; Sparacino, G.; Cobelli, C. Dexcom G4AP: An advanced continuous glucose monitor for the artificial pancreas. J. Diabetes Sci. Technol. 2013, 7, 1436–1445. [Google Scholar] [CrossRef] [PubMed]
- Bailey, T.S.; Chang, A.; Christiansen, M. Clinical accuracy of a continuous glucose monitoring system with an advanced algorithm. J. Diabetes Sci. Technol. 2015, 9, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Castle, J.R.; Jacobs, P.G. Nonadjunctive Use of Continuous Glucose Monitoring for Diabetes Treatment Decisions. J. Diabetes Sci. Technol. 2016. [Google Scholar] [CrossRef] [PubMed]
- Kovatchev, B.P.; Patek, S.D.; Ortiz, E.A.; Breton, M.D. Assessing sensor accuracy for non-adjunct use of continuous glucose monitoring. Diabetes Technol. Ther. 2015, 17, 177–186. [Google Scholar] [CrossRef] [PubMed]
- Patek, S.D.; Lv, D.; Ortiz, E.A.; Hughes-Karvetski, C.; Kulkarni, S.; Zhang, Q.; Breton, M.D. Empirical Representation of Blood Glucose Variability in a Compartmental Model. In Prediction Methods for Blood Glucose Concentration: Design, Use and Evaluation; Kirchsteiger, H., Jørgensen, B.J., Renard, E., del Re, L., Eds.; Springer: Cham, Switzerland, 2016; pp. 133–157. [Google Scholar]
- Viceconti, M.; Cobelli, C.; Haddad, T.; Kovatchev, B.; Palmer, M. In silico assessment of biomedical products: The conundrum of rare but not so rare events. J. Eng. Med. 2016. submitted. [Google Scholar]
- Vettoretti, M.; Facchinetti, A.; Sparacino, G.; Cobelli, C. Predicting insulin treatment scenarios with the net effect method: Domain of validity. Diabetes Technol. Ther. 2016, 18, 694–704. [Google Scholar] [CrossRef] [PubMed]
- Vettoretti, M.; Facchinetti, A.; Sparacino, G.; Cobelli, C. Patient decision-making of CGM sensor driven insulin therapies in type 1 diabetes: In silico assessment. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2015, 2015, 2363–2366. [Google Scholar] [PubMed]
- Kovatchev, B.P.; Breton, M.; Man, C.D.; Cobelli, C. In silico preclinical trials: A proof of concept in closed-loop control of type 1 diabetes. J. Diabetes Sci. Technol. 2009, 3, 44–55. [Google Scholar] [CrossRef] [PubMed]
- Man, C.D.; Micheletto, F.; Lv, D.; Breton, M.; Kovatchev, B.; Cobelli, C. The UVA/PADOVA Type 1 Diabetes Simulator: New Features. J. Diabetes Sci. Technol. 2014, 8, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Visentin, R.; Dalla Man, C.; Kudva, Y.C.; Basu, A.; Cobelli, C. Circadian variability of insulin sensitivity: Physiological input for in silico artificial pancreas. Diabetes Technol. Ther. 2015, 17, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Visentin, R.; Man, C.; Cobelli, C. One-Day Bayesian Cloning of Type 1 Diabetes Subjects: Towards a Single-Day UVA/Padova Type 1 Diabetes Simulator. IEEE Trans. Biomed. Eng. 2016, 63, 2416–2424. [Google Scholar] [CrossRef] [PubMed]
- Vettoretti, M.; Facchinetti, A.; Sparacino, G.; Cobelli, C. Accuracy of devices for self-monitoring of blood glucose: A stochastic error model. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2015, 2015, 2359–2362. [Google Scholar] [PubMed]
- Facchinetti, A.; Del Favero, S.; Sparacino, G.; Castle, J.R.; Ward, W.K.; Cobelli, C. Modeling the glucose sensor error. IEEE Trans. Biomed. Eng. 2014, 61, 620–629. [Google Scholar] [CrossRef] [PubMed]
- Facchinetti, A.; Del Favero, S.; Sparacino, G.; Cobelli, C. Model of glucose sensor error components: Identification and assessment for new Dexcom G4 generation devices. Med. Biol. Eng. Comput. 2015, 53, 1259–1269. [Google Scholar] [CrossRef] [PubMed]
- Facchinetti, A.; Del Favero, S.; Sparacino, G.; Cobelli, C. Modeling Transient Disconnections and Compression Artifacts of Continuous Glucose Sensors. Diabetes Technol. Ther. 2016, 18, 264–272. [Google Scholar] [CrossRef] [PubMed]
- FDA Advisory Panel Votes to Recommend Non-Adjunctive Use of Dexcom G5 Mobile CGM. Diabetes Technol. Ther. 2016, 18, 512–516.
- Edelman, S.V. Regulation Catches Up to Reality: Nonadjunctive Use of Continuous Glucose Monitoring Data. J. Diabetes Sci. Technol. 2016. [Google Scholar] [CrossRef] [PubMed]
- Bailey, T.; Bode, B.W.; Christiansen, M.P.; Klaff, L.J.; Alva, S. The Performance and Usability of a Factory-Calibrated Flash Glucose Monitoring System. Diabetes Technol. Ther. 2015, 17, 787–794. [Google Scholar] [CrossRef] [PubMed]
- Bolinder, J.; Antuna, R.; Geelhoed-Duijvestijn, P.; Kroger, J.; Weitgasser, R. Novel glucose-sensing technology and hypoglycaemia in type 1 diabetes: A multicentre, non-masked, randomised controlled trial. Lancet 2016, 388, 2254–2263. [Google Scholar] [CrossRef]
- Acciaroli, G.; Vettoretti, M.; Facchinetti, A.; Sparacino, G.; Cobelli, C. From Two to One Per Day Calibration of Dexcom G4 Platinum by a Time-Varying Day-Specific Bayesian Prior. Diabetes Technol. Ther. 2016, 18, 472–479. [Google Scholar] [CrossRef] [PubMed]
- Bequette, B.W. Fault detection and safety in closed-loop artificial pancreas systems. J. Diabetes Sci. Technol. 2014, 8, 1204–1214. [Google Scholar] [CrossRef] [PubMed]



© 2016 by the author; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Facchinetti, A. Continuous Glucose Monitoring Sensors: Past, Present and Future Algorithmic Challenges. Sensors 2016, 16, 2093. https://doi.org/10.3390/s16122093
Facchinetti A. Continuous Glucose Monitoring Sensors: Past, Present and Future Algorithmic Challenges. Sensors. 2016; 16(12):2093. https://doi.org/10.3390/s16122093
Chicago/Turabian StyleFacchinetti, Andrea. 2016. "Continuous Glucose Monitoring Sensors: Past, Present and Future Algorithmic Challenges" Sensors 16, no. 12: 2093. https://doi.org/10.3390/s16122093
APA StyleFacchinetti, A. (2016). Continuous Glucose Monitoring Sensors: Past, Present and Future Algorithmic Challenges. Sensors, 16(12), 2093. https://doi.org/10.3390/s16122093