
Influence of Individual Differences on the Calculation Method for FBG-Type Blood Pressure Sensors


Abstract
:1. Introduction
2. Measurement Principle
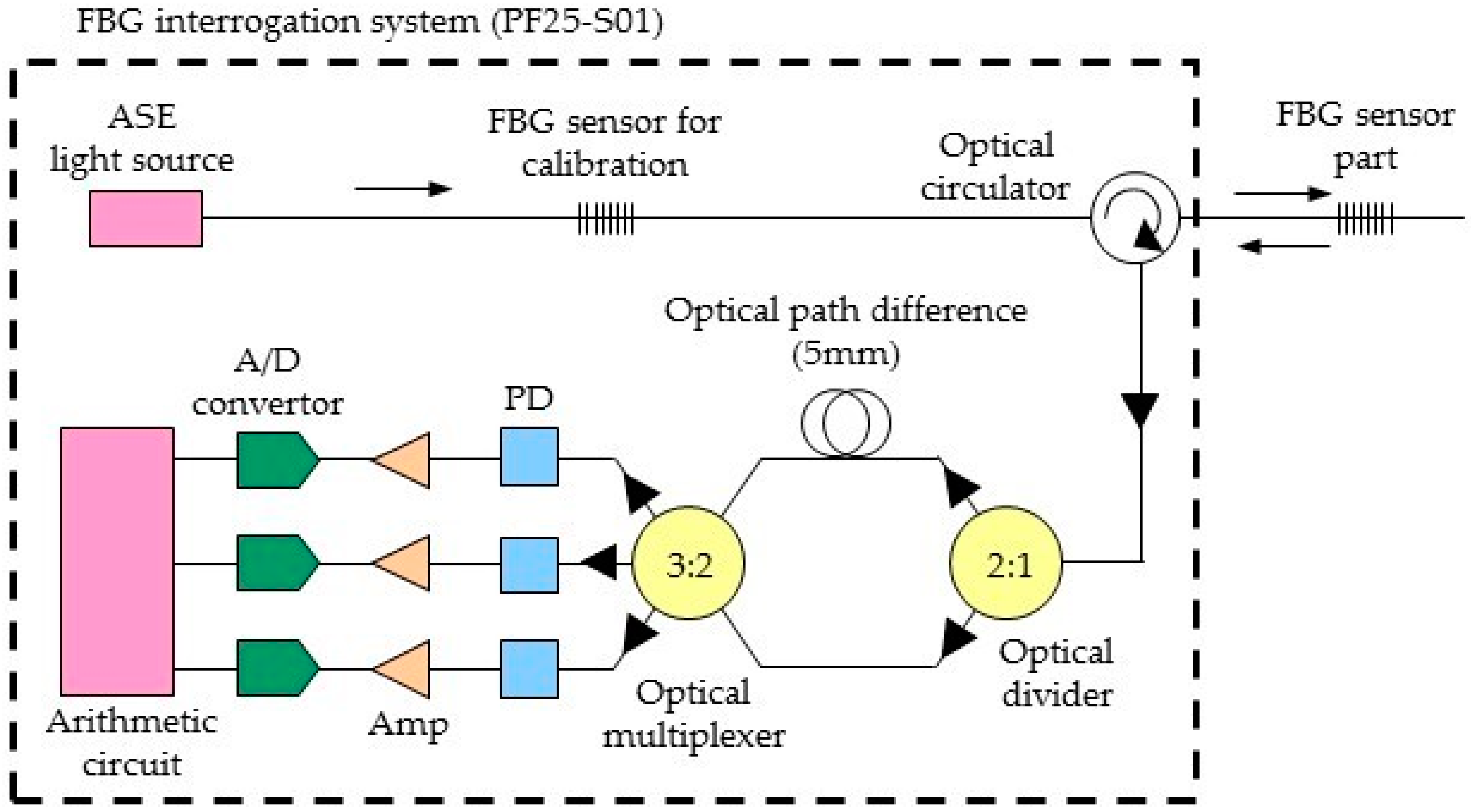
2.1. Measurement System of the FBG Sensor
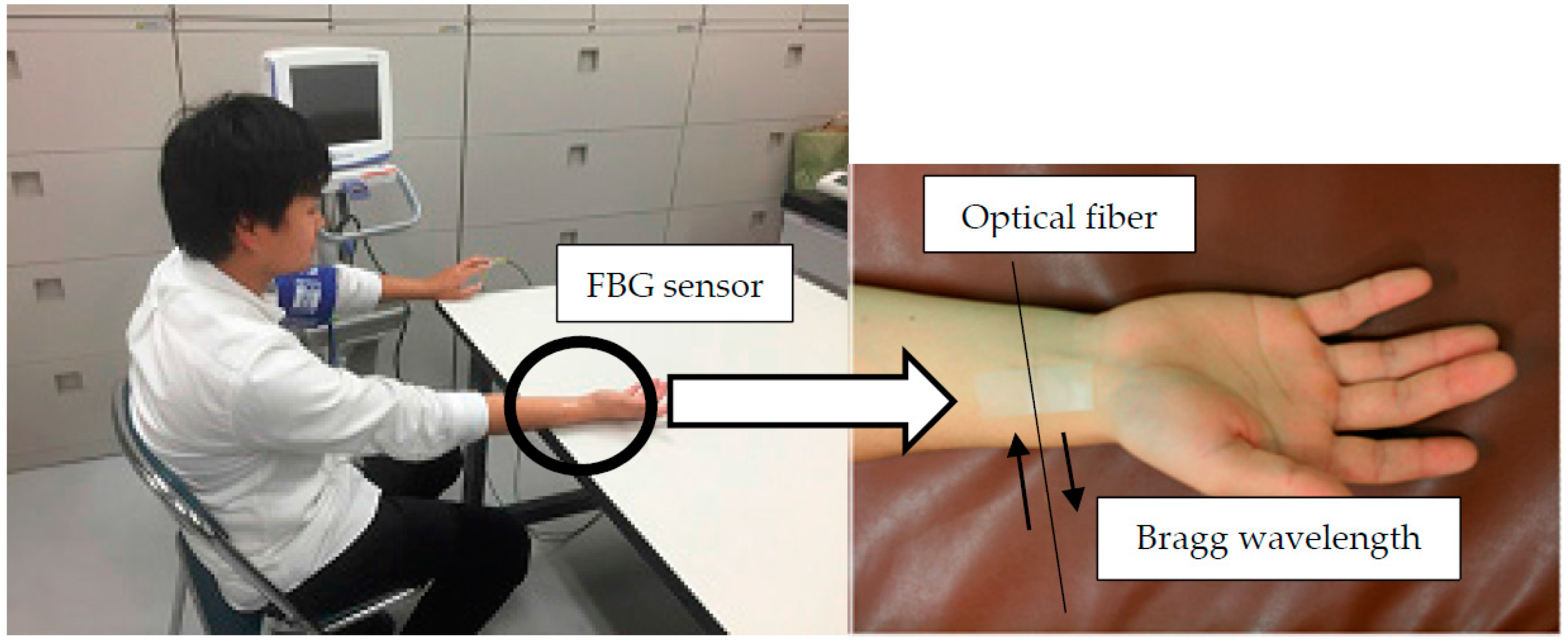
2.2. Measurement of the Pulse Wave Signal by the FBG Sensor
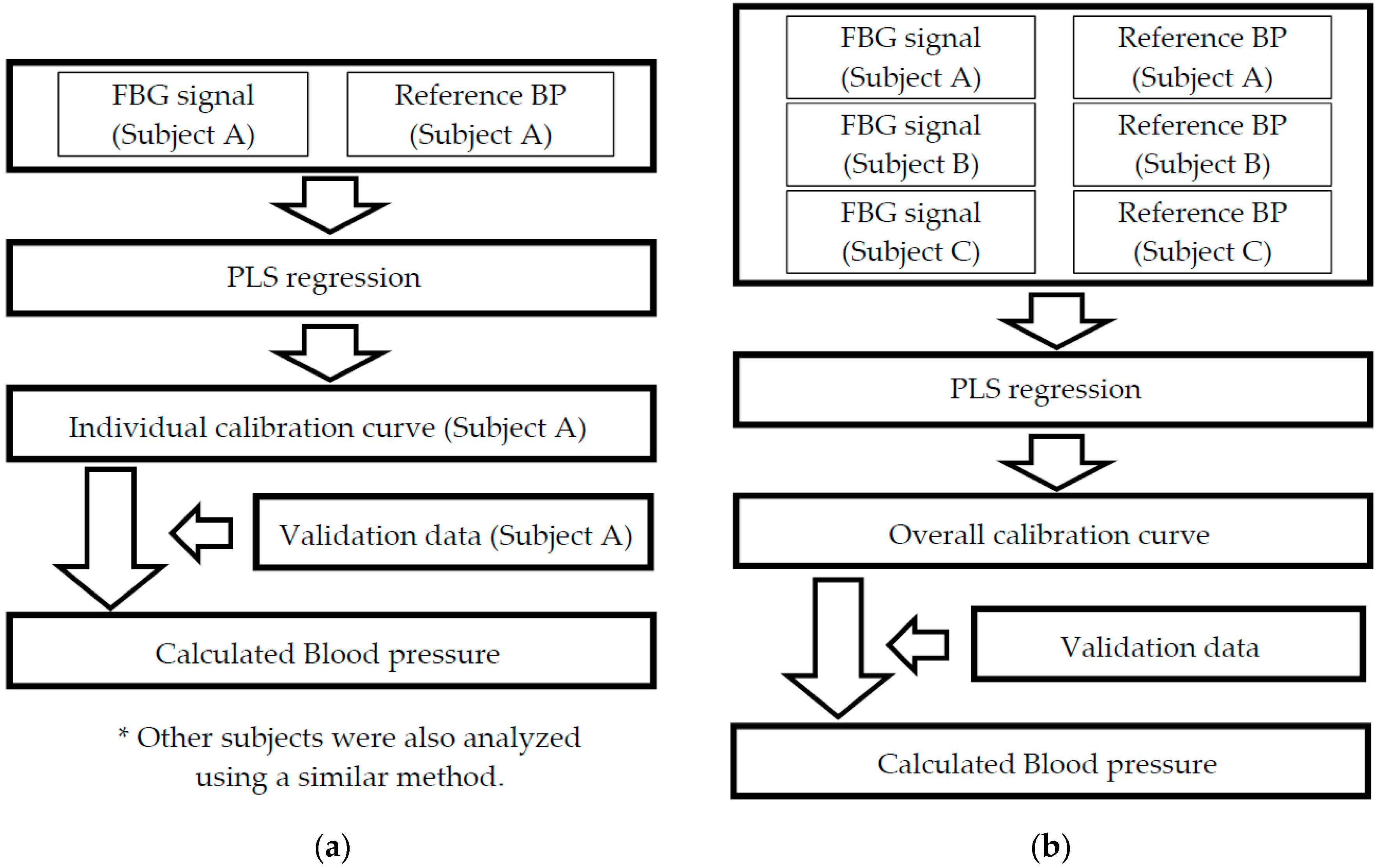
2.3. Blood Pressure Measurement Calculation Method
3. Measurement Results
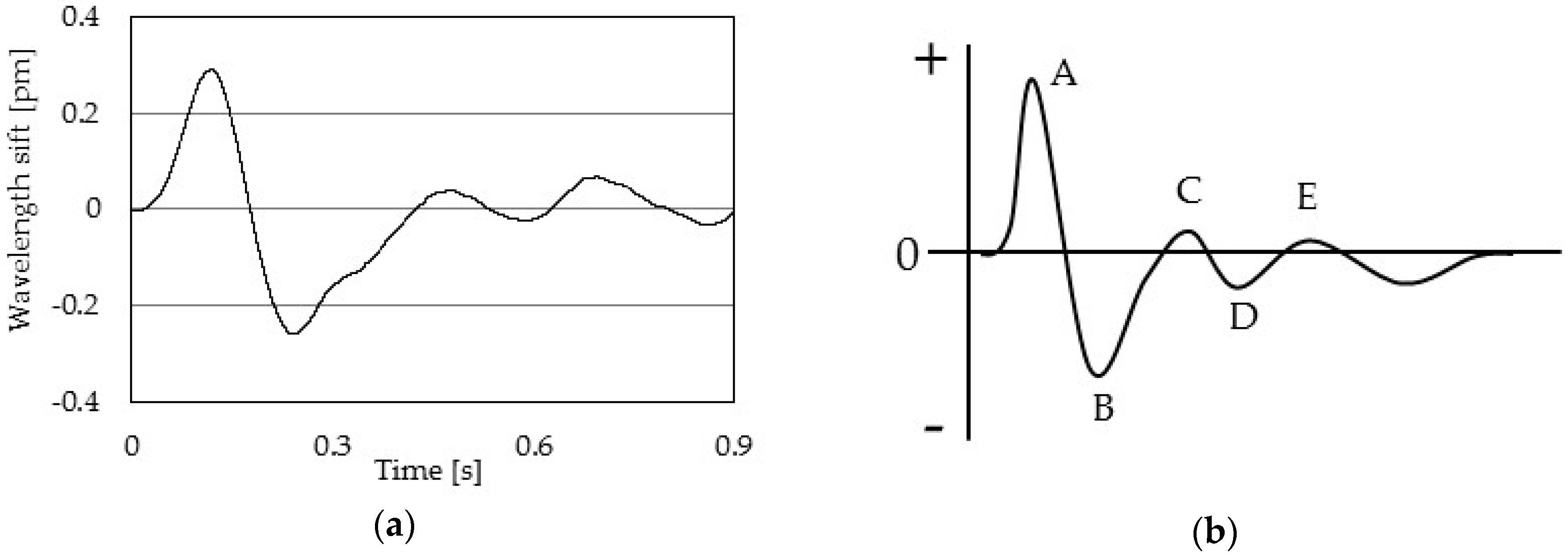
3.1. Results of Pulse Wave Signal Measurement by the FBG Sensor
3.2. The Influence of Individual Differences in the Blood Pressure Calculated Using the Calibration Curve Method
4. Conclusions
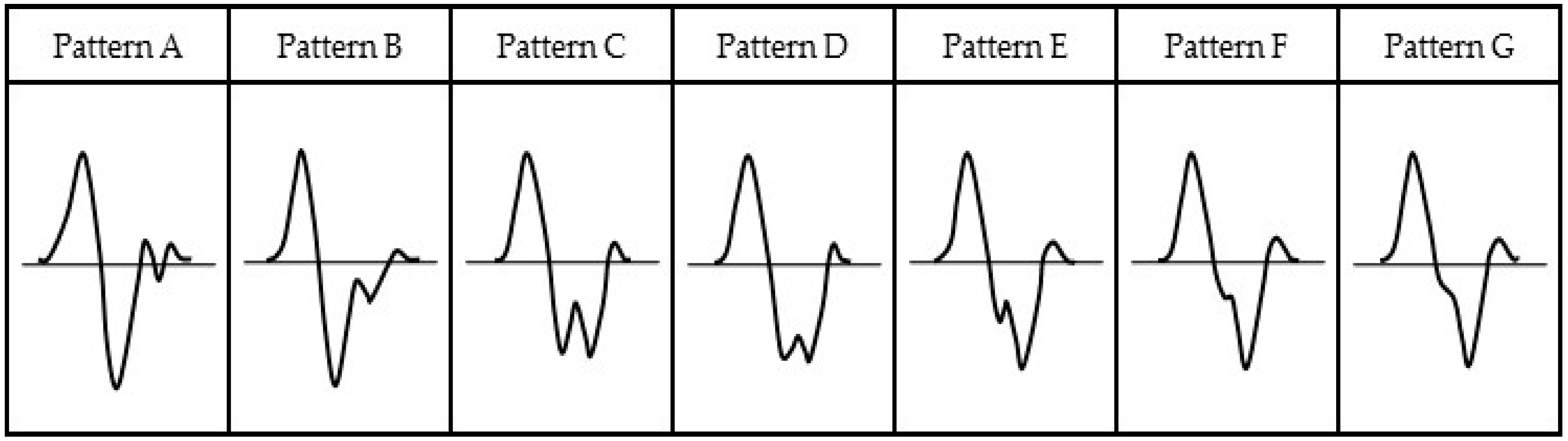
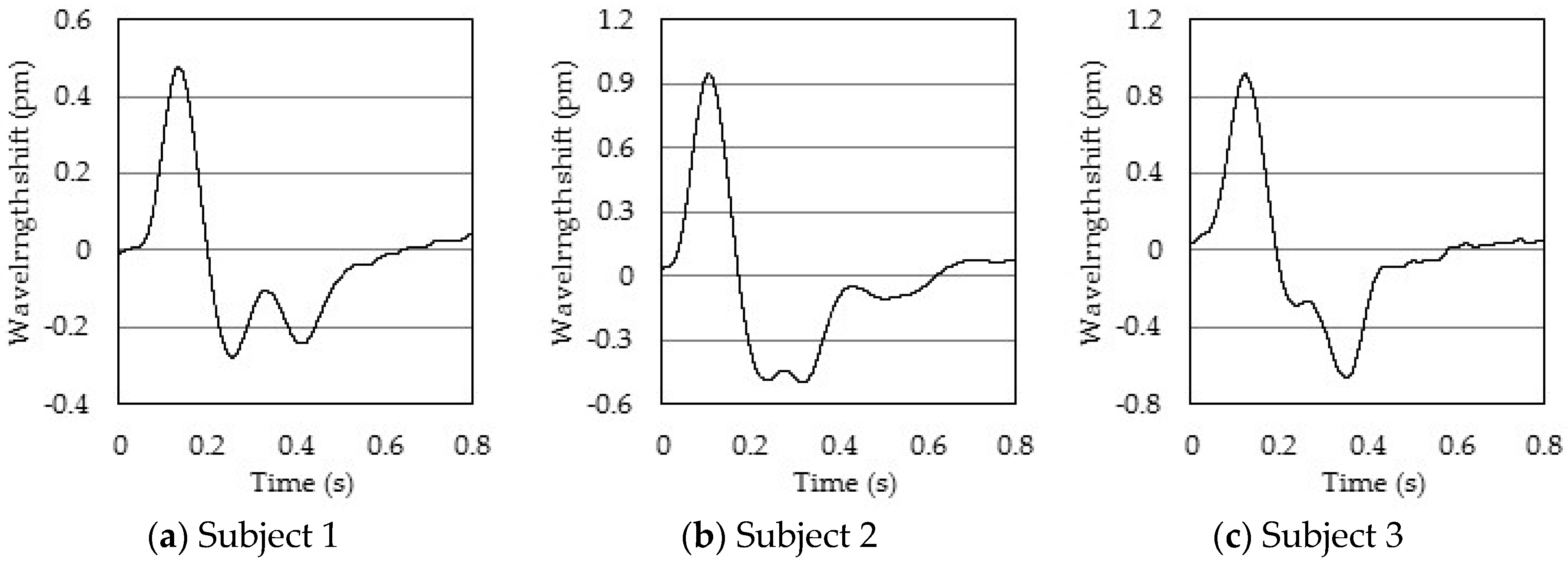
- The pulse wave signal measured by the FBG sensor is similar to the acceleration pulse wave signal.
- The waveform of the measured pulse wave signal differs between healthy and elderly individuals.
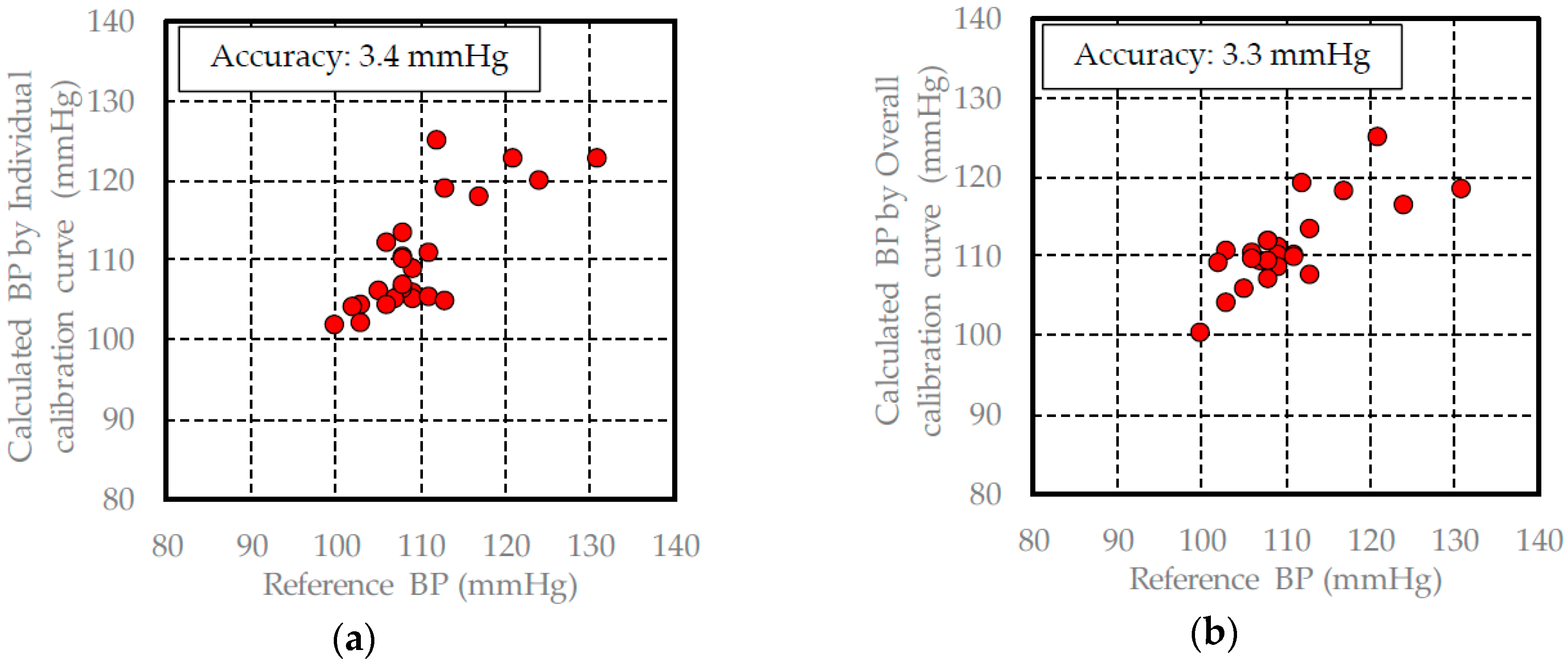
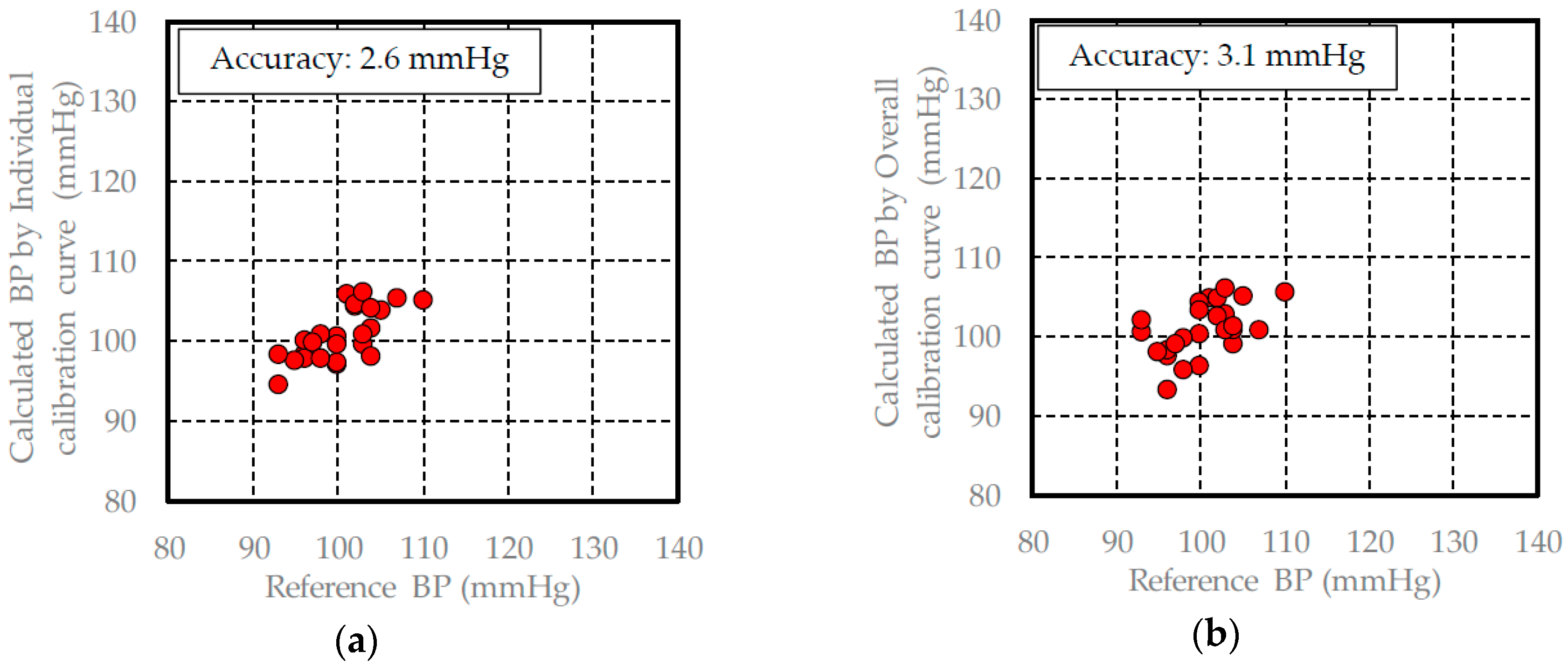
- The overall calibration curve has the influence of individual differences, because the measurement accuracy of the calculated blood pressure was lower than the measurement accuracy using the individual calibration method.
- The measurement accuracy of the calculated blood pressure using the overall calibration curve is approximately 3 mmHg.
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Cabinet Office, Government of Japan. Situation on Aging, Annual Report on the Aging Society 2015. Available online: http://www8.cao.go.jp/kourei/english/annualreport/2015/pdf/c1-1.pdf (accessed on 3 October 2016).
- Tam, H.Y.; Liu, S.Y.; Guan, B.O.; Chung, W.H.; Chan, T.H.; Cheng, L.K. Fiber bragg grating sensors for structural and railway applications. Proc. SPIE 2005, 5634. [Google Scholar] [CrossRef] [Green Version]
- Wei, C.L.; Lai, C.C.; Liu, S.Y.; Chung, W.H.; Ho, T.K.; Tam, H.Y.; Ho, S.L.; McCusker, A.; Kam, J.; Lee, K.Y. A fiber bragg grating sensor system for train axle counting. IEEE Sens. J. 2014, 10, 1905–1912. [Google Scholar]
- Wei, C.L.; Xin, Q.; Chung, W.H.; Liu, S.Y.; Tam, H.Y.; Ho, S.L. Real-time train wheel condition monitoring by fiber bragg grating sensors. Int. J. Distrib. Sens. Netw. 2012. [Google Scholar] [CrossRef]
- Hao, J.; Jayachandran, M.; Kng, P.L.; Foo, S.F.; Aung, P.W.; Cai, Z. FBG-based smart bed system for healthcare applications. Front. Optoelectron. 2010, 1, 78–83. [Google Scholar] [CrossRef]
- Spillman, W.B., Jr.; Mayer, M.; Bennett, J.; Gong, J.; Meissner, K.E.; Davis, B.; Claus, R.O.; Muelenaer, A.A., Jr.; Xu, X. A ‘smart’ bed for non-intrusive monitoring of patient physiological factors. Meas. Sci. Technol. 2004, 15, 1614–1620. [Google Scholar] [CrossRef]
- Elsarnagawy, T.; Haueisen, J.; Farrag, M.; Ansari, S.G.; Fouad, H. Embedded fiber bragg grating based strain sensor as smart costume for vital signal sensing. Sens. Lett. 2014, 12, 1669–1674. [Google Scholar] [CrossRef]
- Kawamura, M.; Ishizawa, H.; Sato, S.; Koyama, S. Application to vital signs by fiber bragg grating sensing. In Proceedings of the SICE Annual Conference 2011 Final Program and Papers, Tokyo, Japan, 13–18 September 2011; pp. 2702–2704.
- Miyauchi, Y.; Ishizawa, H.; Koyama, S. The pulse rate measuring system which use FBG sensors. In Proceedings of the 13th International Symposium on the Science and Technology of Lighting, New York, NY, USA, 24–29 June 2012; pp. 415–416.
- Sato, S.; Ishizawa, H.; Hattori, A.; Miyauchi, Y. Study of fixed points in pulse rate measurement by FBG sensor. In Proceedings of the SICE Annual Conference 2012 Final Program and Papers, Akita, Japan, 20–23 August 2012; pp. 1849–1851.
- Miyauchi, Y.; Ishizawa, H.; Koyama, S.; Sato, S. Verification of the systolic blood-pressure measurement principle by FBG Sensors. In Proceedings of the SICE Annual Conference 2012 Final Program and Papers, Akita, Japan, 20–23 August 2012; pp. 619–622.
- Takagi, T.; Ishizawa, H.; Niimura, M.; Koyama, S.; Miyauchi, Y.; Katsuragawa, Y. Basis study on systolic blood pressure measurement by using FBG sensors. In Proceedings of the International Symposium on Fiber Science and Technology 2014, Tokyo, Japan, 28 September–1 October 2014.
- Yoshino, T.; Sano, Y.; Ota, D.; Fujita, K.; Ikui, T. Fiber-Bragg-grating based single axial mode Fabry-Perot interferometer and its strain and acceleration sensing applications. J. Lightwave Tech. 2016, 34, 2240–2250. [Google Scholar] [CrossRef]
- Todd, M.D.; Johnson, G.A.; Chang, C.C. Passive, light intensity-independent interferometric method for fiber Bragg grating interrogation. Electron. Lett. 1999, 35, 1970–1971. [Google Scholar] [CrossRef]
- Chino, S.; Ishizawa, H.; Hosoya, S.; Koyama, S.; Fujimoto, K. Non-invasive blood pressure measurement—The study of measuring points. In Proceedings of the SICE Annual Conference 2016, Tsukuba, Japan, 20–23 September 2016; pp. 1706–1709.
- Katsuragawa, Y.; Ishizawa, H. Non-invasive blood pressure measurement by pulse wave analysis using FBG sensor. In Proceedings of the 2015 IEEE International Instrumentation and Measurement Technology Conference (I2MTC), Pisa, Italy, 11–14 May 2015; pp. 511–515.
- Hall, J.W.; Pollard, A. Near-infrared spectroscopic determination of serum total proteins, albumin, globulins, and urea. Clin. Biochem. 1993, 26, 483–490. [Google Scholar] [CrossRef]
- Heise, H.M.; Bittner, A.; Marbach, R. Clinical chemistry and near infrared spectroscopy: Technology for non-invasive glucose monitoring. J. Near Infrared Spectrosc. 1998, 6, 349–359. [Google Scholar] [CrossRef]
- Malin, S.F.; Ruchti, T.L.; Blank, T.B.; Thennadil, S.N.; Monfre, S.L. Noninvasive prediction of glucose by near-infrared diffuse reflectance spectroscopy. Clin. Chem. 1999, 45, 1651–1658. [Google Scholar] [PubMed]
- Kasemsumran, S.; Du, Y.; Maruo, K.; Ozaki, Y. Improvement of partial least squares models for in vitro and in vivo glucose quantifications by using near-infrared spectroscopy and searching combination moving window partial least squares. Chemom. Intel. Lab. Syst. 2006, 82, 97–103. [Google Scholar] [CrossRef]
- Koyama, S.; Morishima, M.; Miyauchi, Y.; Ishizawa, H. Non-destructive identification and mixture ratio analysis of cotton-polyester blended textile products by IR spectroscopy. Text. Light Ind. Sci. Technol. 2013, 2, 153–160. [Google Scholar]
- Wold, S.; Ruhe, A.; Wold, H.; Dunn, W.J. The collinearity problem in linear regression, The partial least squares (PLS) approach to generalized inverses. SIAM. J. Sci. Stat. Comput. 1984, 5, 735–743. [Google Scholar] [CrossRef]
- Wold, S.; Sjostrom, M.; Ericksson, L. PLS-regression, a basic tool of chemometrics. Chemom. Intel. Lab. Syst. 2001, 58, 109–130. [Google Scholar] [CrossRef]
- Lorber, A.; Wangen, L.E.; Kowalski, B.R. A theoretical foundation for the PLS algorithm. J. Chemom. 1987, 1, 19–31. [Google Scholar] [CrossRef]
- Martens, H.; Neas, T. Multivariate Calibration; John Wiley & Sons: Hoboken, NJ, USA, 1989; pp. 116–165. [Google Scholar]
- Ahn, J.M. Wave detection in acceleration plethysmogram. Healthc. Inf. Res. 2015, 21, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Elgendi, M.; Norton, I.; Brearley, M.; Abbott, D.; Schuurmans, D. Detection of a and b waves in the acceleration photoplethysmogram. BioMed. Eng. Online 2014, 13, 139–158. [Google Scholar] [CrossRef] [PubMed]
- Sano, Y.; Kataoka, Y.; Ikuyama, T.; Wada, M.; Imano, H.; Kawamura, K.; Watanabe, T.; Nishida, A.; Osanai, H. Evaluation of peripheral circulation with accelerated plethysmography and its practical applications report 2. Quantification of inflection points of a waveform. Bull. Phys. Fit. Res. Inst. 1988, 68, 17–25. [Google Scholar]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject | Samples | Max (mmHg) | Min (mmHg) | Avg (mmHg) |
|---|---|---|---|---|
| A | 50 | 125 | 100 | 111.3 |
| B | 50 | 136 | 113 | 123.1 |
| C | 50 | 111 | 93 | 100.9 |
| Overall | 150 | 136 | 93 | 111.8 |
| Subject | Samples | Max (mmHg) | Min (mmHg) | Avg (mmHg) |
|---|---|---|---|---|
| A | 25 | 131 | 100 | 110.1 |
| B | 25 | 138 | 112 | 122.2 |
| C | 25 | 110 | 93 | 100.4 |
| Calibration curve | R | Accuracy (mmHg) |
|---|---|---|
| Individual Subject A | 0.82 | 4.2 |
| Individual Subject B | 0.89 | 3.0 |
| Individual Subject C | 0.67 | 3.1 |
| Overall | 0.93 | 4.1 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koyama, S.; Ishizawa, H.; Fujimoto, K.; Chino, S.; Kobayashi, Y. Influence of Individual Differences on the Calculation Method for FBG-Type Blood Pressure Sensors. Sensors 2017, 17, 48. https://doi.org/10.3390/s17010048
Koyama S, Ishizawa H, Fujimoto K, Chino S, Kobayashi Y. Influence of Individual Differences on the Calculation Method for FBG-Type Blood Pressure Sensors. Sensors. 2017; 17(1):48. https://doi.org/10.3390/s17010048
Chicago/Turabian StyleKoyama, Shouhei, Hiroaki Ishizawa, Keisaku Fujimoto, Shun Chino, and Yuka Kobayashi. 2017. "Influence of Individual Differences on the Calculation Method for FBG-Type Blood Pressure Sensors" Sensors 17, no. 1: 48. https://doi.org/10.3390/s17010048
APA StyleKoyama, S., Ishizawa, H., Fujimoto, K., Chino, S., & Kobayashi, Y. (2017). Influence of Individual Differences on the Calculation Method for FBG-Type Blood Pressure Sensors. Sensors, 17(1), 48. https://doi.org/10.3390/s17010048