Knee Impedance Modulation to Control an Active Orthosis Using Insole Sensors

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
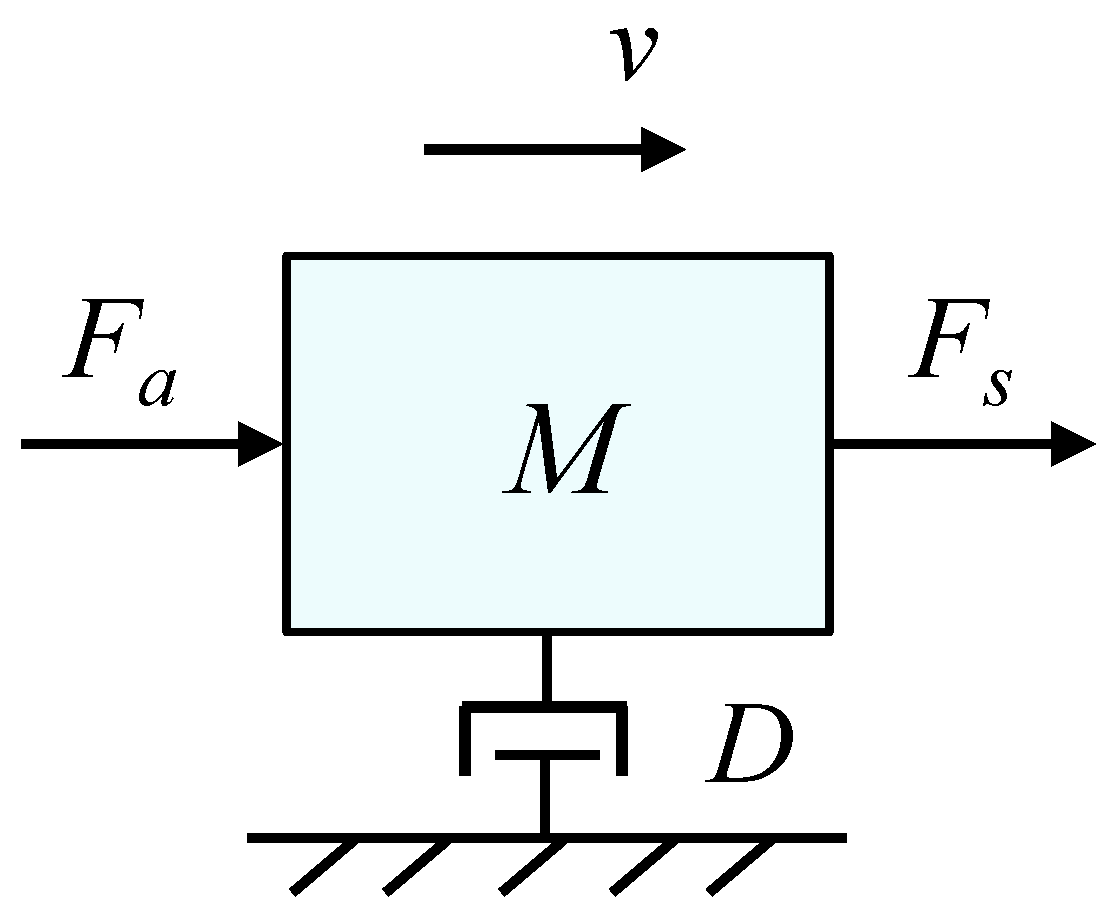
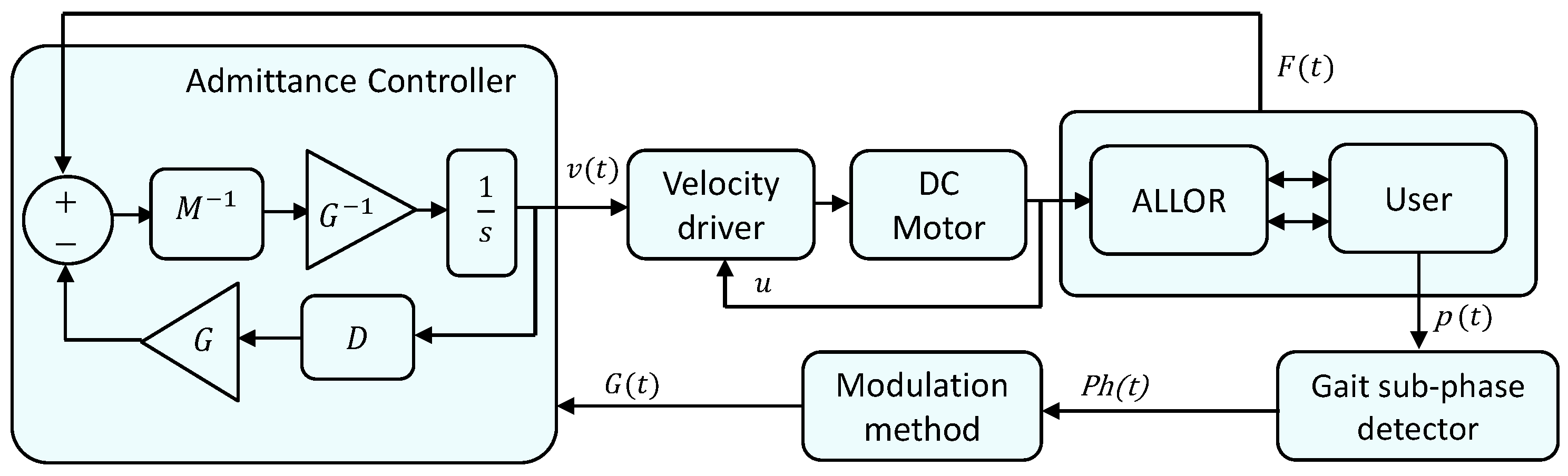
2.1. Admittance Controller
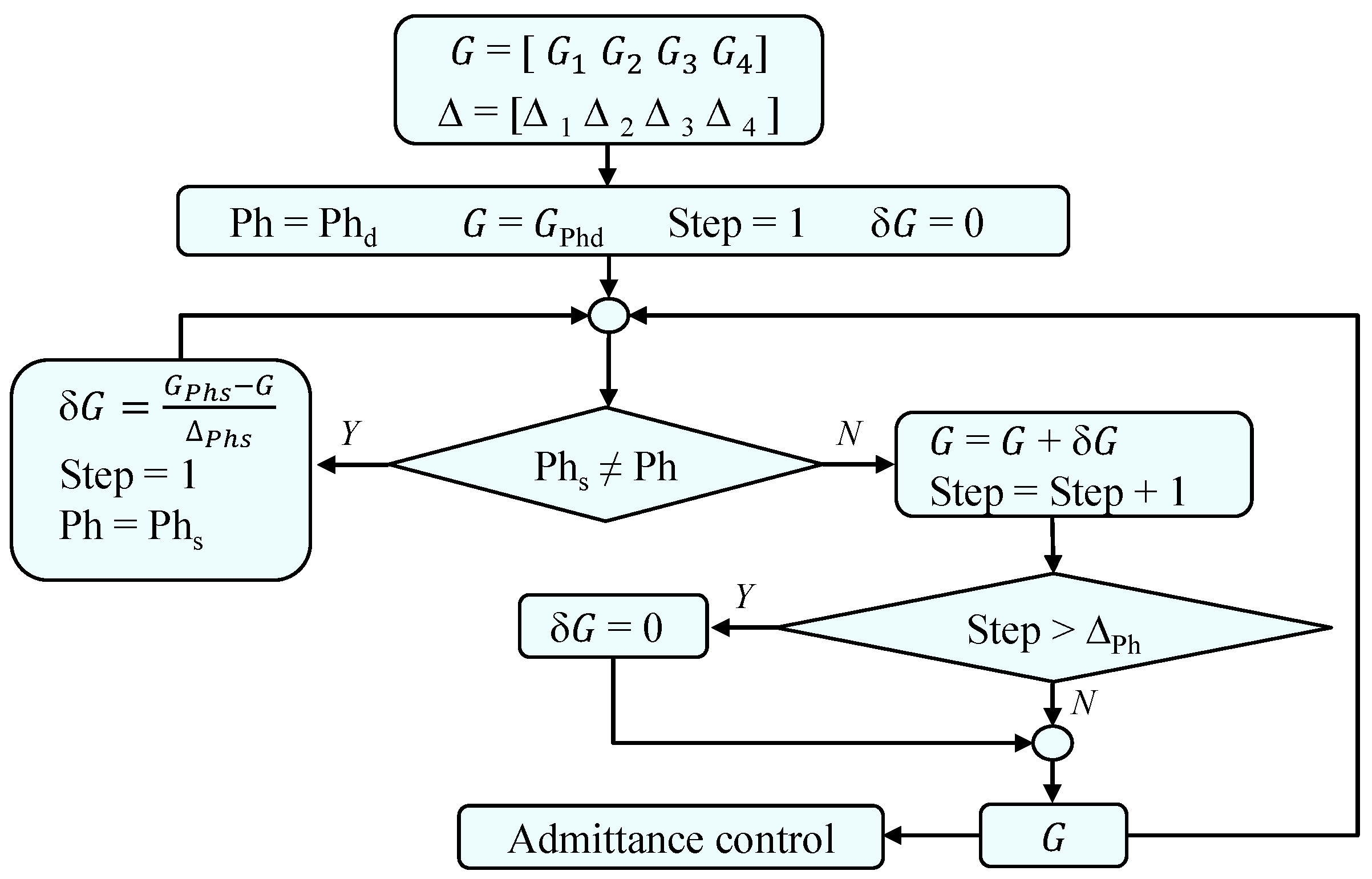
2.2. Knee Impedance Modulation
2.3. Gait Phase Detection
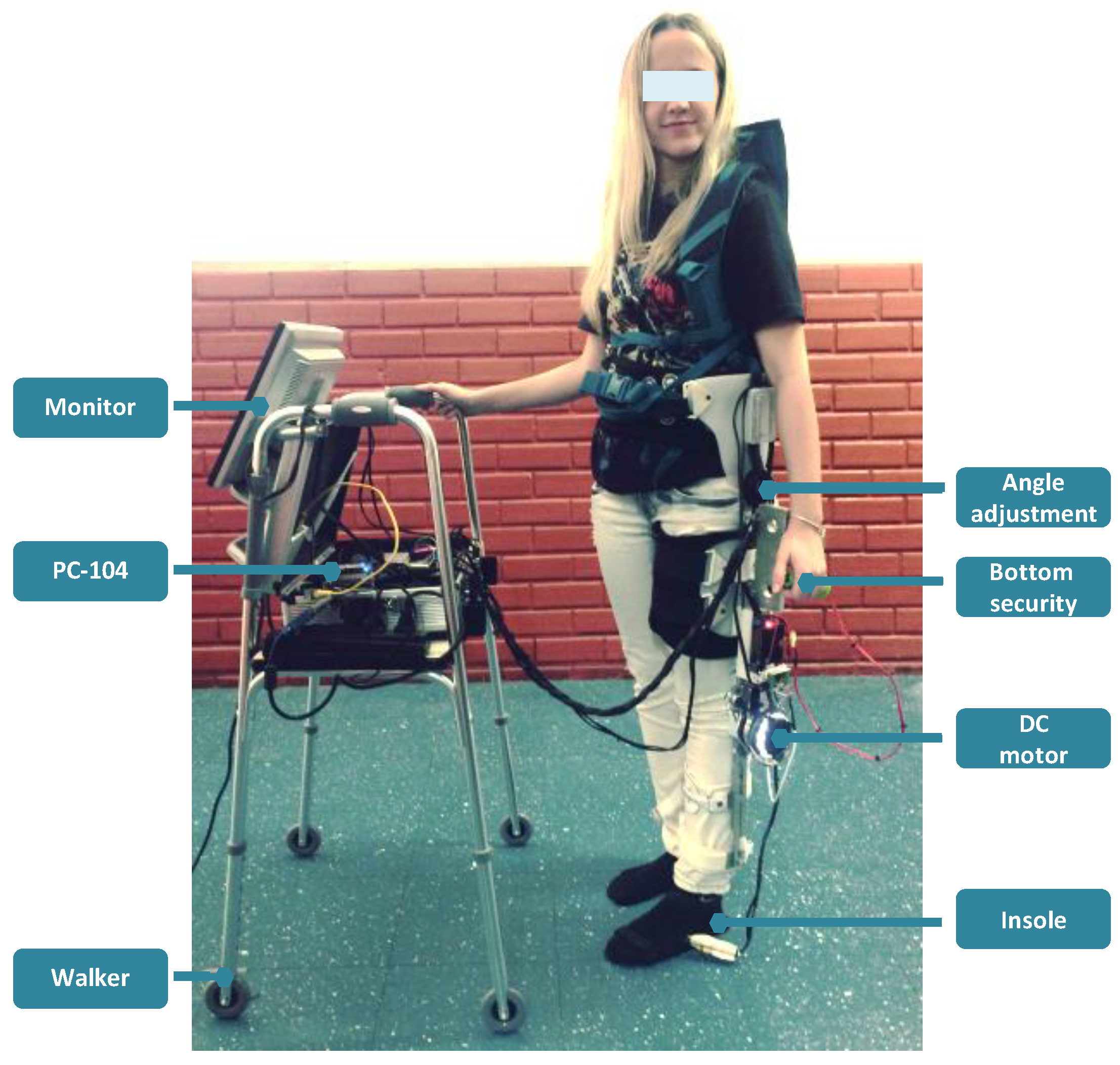
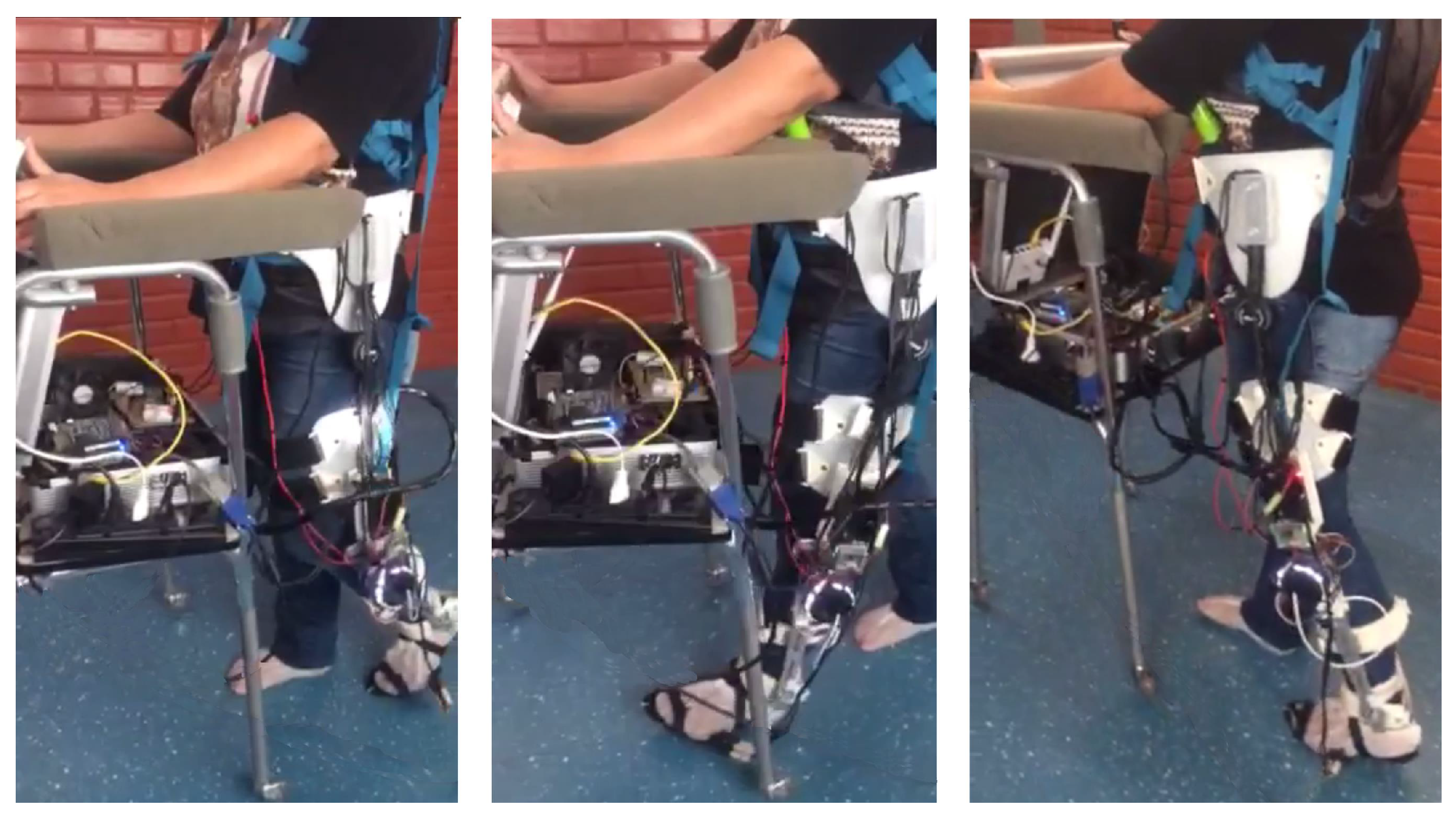
2.4. Active Knee Orthosis
2.5. Experimental Protocol
2.6. Statistical and User’s Satisfaction Analysis
3. Results
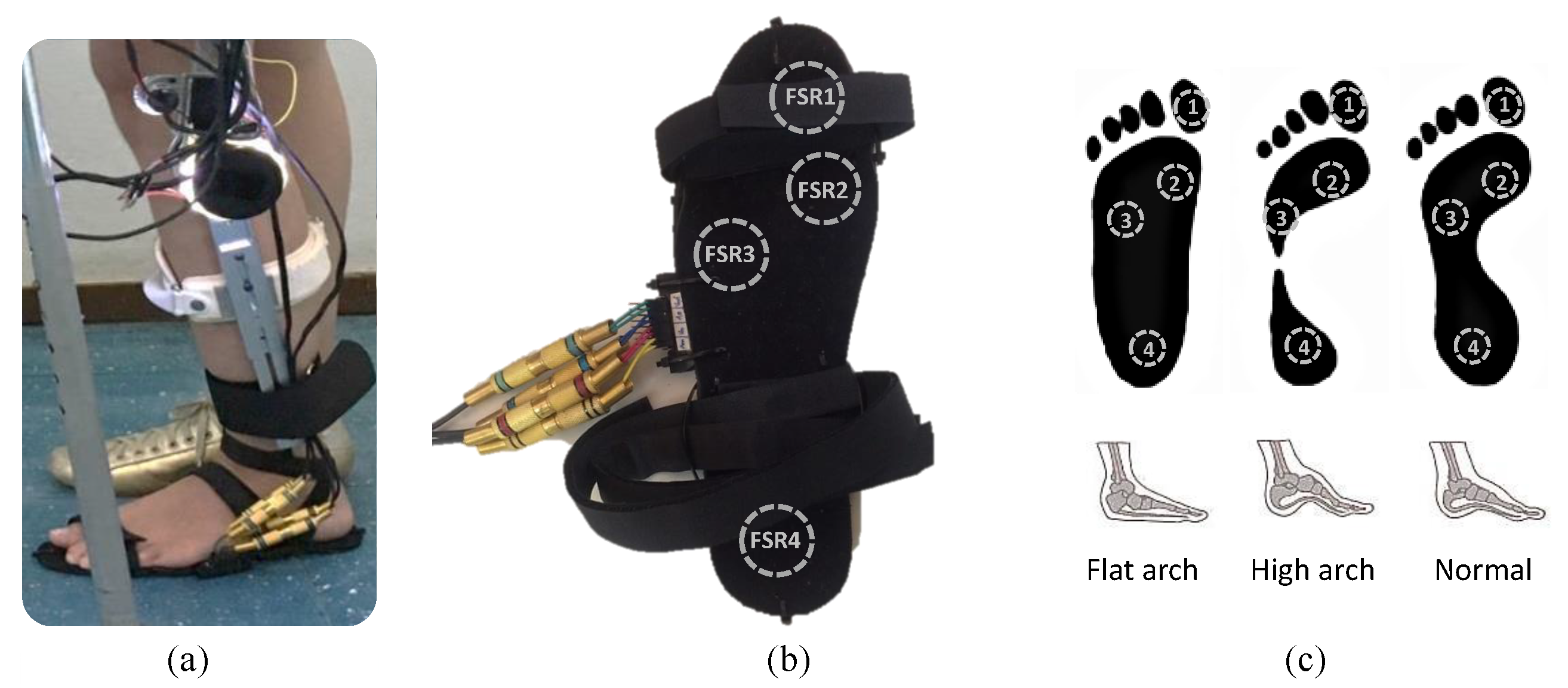
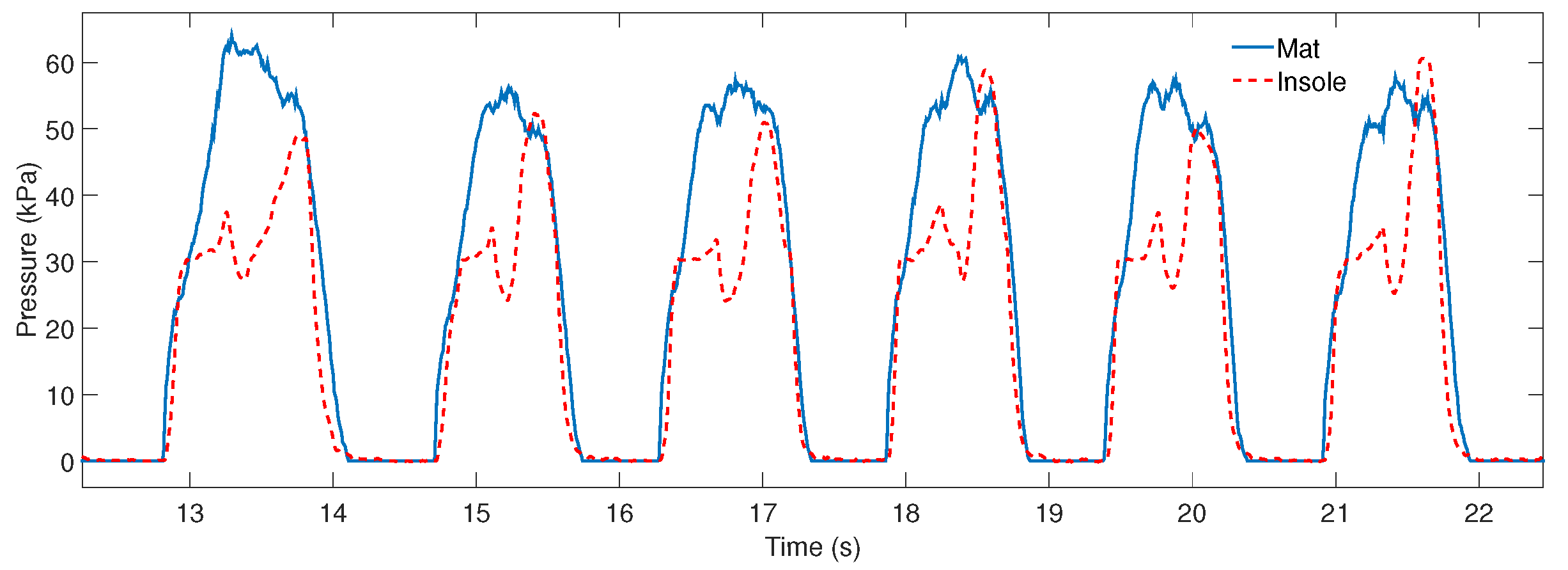
3.1. Instrumented Insole
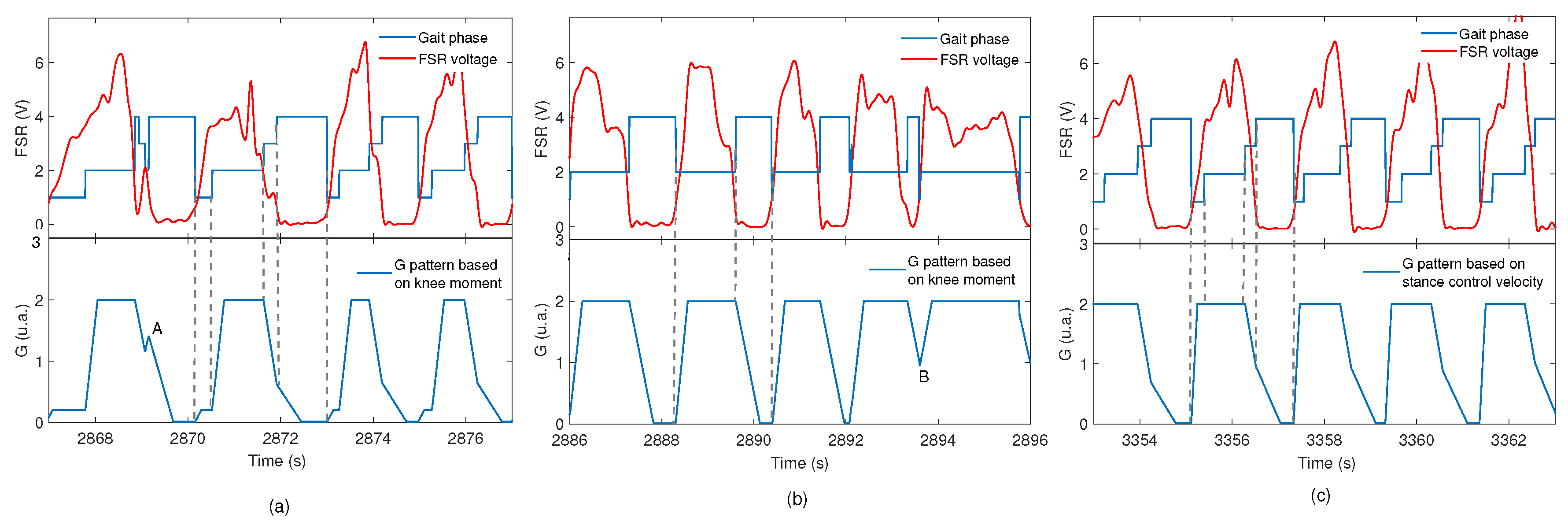
3.2. Knee Impedance Modulation
4. Discussion
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| ALLOR | Advance Lower Limb Orthosis for Rehabilitation |
| D | Damping |
| F | Force |
| FSR | Force sensing resistor |
| G | Gain for impedance modulation |
| H | ALLOR user’s height |
| Initial contact phase | |
| M | Mass |
| p | Plantar pressure |
| Gain pattern for impedance modulation based on knee moment during gait | |
| Gain pattern for impedance modulation based on knee velocity during gait | |
| Gain pattern for impedance modulation to obtain a free movement | |
| Phase | |
| Q | Percentage |
| QUEST | Quebec User Evaluation of Satisfaction with Assistive Technology |
| Stance control | |
| Stance phase | |
| Swing phase | |
| t | Time |
| W | ALLOR user’s weight |
References
- Mahlknecht, P.; Kiechl, S.; Bloem, B.R.; Willeit, J.; Scherfler, C.; Gasperi, A.; Rungger, G.; Poewe, W.; Seppi, K. Prevalence and Burden of Gait Disorders in Elderly Men and Women Aged 60–97 Years: A Population-Based Study. PLoS ONE 2013, 8, e69627. [Google Scholar] [CrossRef] [PubMed]
- Balaban, B.; Tok, F. Gait Disturbances in Patients With Stroke. PM&R 2014, 6, 635–642. [Google Scholar]
- Salzman, B. Gait and balance disorders in older adults. Am. Fam. Physician 2010, 82, 61–68. [Google Scholar] [PubMed]
- Hendrickson, J.; Patterson, K.K.; Inness, E.L.; McIlroy, W.E.; Mansfield, A. Relationship between asymmetry of quiet standing balance control and walking post-stroke. Gait Posture 2014, 39, 177–181. [Google Scholar] [CrossRef] [PubMed]
- Weerdesteyn, V.; de Niet, M.; van Duijnhoven, H.J.R.; Geurts, A.C.H. Falls in individuals with stroke. J. Rehabil. Res. Dev. 2008, 45, 1195–1213. [Google Scholar] [CrossRef] [PubMed]
- Dzahir, M.A.M.; Yamamoto, S.I. Recent trends in lower-limb robotic rehabilitation orthosis: Control scheme and strategy for pneumatic muscle actuated gait trainers. Robotics 2014, 3, 120–148. [Google Scholar] [CrossRef]
- Tucker, M.R.; Olivier, J.; Pagel, A.; Bleuler, H.; Bouri, M.; Lambercy, O.; del R Millán, J.; Riener, R.; Vallery, H.; Gassert, R. Control strategies for active lower extremity prosthetics and orthotics: A review. J. Neuroeng. Rehabilit. 2015, 12, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, B.; Ma, H.; Qin, L.Y.; Gao, F.; Chan, K.M.; Law, S.W.; Qin, L.; Liao, W.H. Recent developments and challenges of lower extremity exoskeletons. J. Orthop. Transl. 2016, 5, 26–37. [Google Scholar] [CrossRef]
- Villa-Parra, A.; Broche, L.; Delisle-Rodríguez, D.; Sagaró, R.; Bastos, T.; Frizera-Neto, A. Design of active orthoses for a robotic gait rehabilitation system. Front. Mech. Eng. 2015, 10, 242–254. [Google Scholar] [CrossRef]
- Louie, D.R.; Eng, J.J. Powered robotic exoskeletons in post-stroke rehabilitation of gait: A scoping review. J. Neuroeng. Rehabilit. 2016, 13, 53. [Google Scholar] [CrossRef] [PubMed]
- Louie, D.R.; Eng, J.J.; Lam, T. Gait speed using powered robotic exoskeletons after spinal cord injury: A systematic review and correlational study. J. Neuroeng. Rehabilit. 2015, 12, 82. [Google Scholar] [CrossRef] [PubMed]
- Cao, J.; Xie, S.Q.; Das, R.; Zhu, G.L. Control strategies for effective robot assisted gait rehabilitation: The state of art and future prospects. Med. Eng. Phys. 2014, 36, 1555–1566. [Google Scholar] [CrossRef] [PubMed]
- Tsuji, T.; Tanaka, Y. Tracking control properties of human-robotic systems based on impedance control. IEEE Trans. Syst. Man Cybern. Part A Syst. Hum. 2005, 35, 523–535. [Google Scholar] [CrossRef]
- Hussain, S.; Xie, S.Q.; Jamwal, P.K. Adaptive impedance control of a robotic orthosis for gait rehabilitation. IEEE Trans. Cybern. 2013, 43, 1025–1034. [Google Scholar] [CrossRef] [PubMed]
- Huo, W.; Mohammed, S.; Moreno, J.C.; Amirat, Y. Lower limb wearable robots for assistance and rehabilitation: A state of the art. IEEE Syst. J. 2016, 10, 1068–1081. [Google Scholar] [CrossRef]
- Bulea, T.C.; Kobetic, R.; To, C.S.; Audu, M.L.; Schnellenberger, J.R.; Triolo, R.J. A variable impedance knee mechanism for controlled stance flexion during pathological gait. IEEE/ASME Trans. Mechatron. 2012, 17, 822–832. [Google Scholar] [CrossRef]
- Ajoudani, A. Transferring Human Impedance Regulation Skills to Robots; Springer: Berlin, Heidelberg, 2016. [Google Scholar]
- Meng, W.; Liu, Q.; Zhou, Z.; Ai, Q.; Sheng, B.; Xie, S.S. Recent development of mechanisms and control strategies for robot-assisted lower limb rehabilitation. Mechatronics 2015, 31, 132–145. [Google Scholar] [CrossRef]
- Figueiredo, J.; Félix, P.; Santos, C.P.; Moreno, J.C. Towards human-knee orthosis interaction based on adaptive impedance control through stiffness adjustment. IEEE Int. Conf. Rehabil. Robot. 2017, 406–411. [Google Scholar] [CrossRef]
- Pfeifer, S.; Vallery, H.; Hardegger, M.; Riener, R.; Perreault, E.J. Model-based estimation of knee stiffness. IEEE Trans. Biomed. Eng. 2012, 59, 2604–2612. [Google Scholar] [CrossRef] [PubMed]
- Sartori, M.; Maculan, M.; Pizzolato, C.; Reggiani, M.; Farina, D. Modeling and simulating the neuromuscular mechanisms regulating ankle and knee joint stiffness during human locomotion. J. Neurophysiol. 2015, 114, 2509–2527. [Google Scholar] [CrossRef] [PubMed]
- Rafiaei, M.; Bahramizadeh, M.; Arazpour, M.; Samadian, M.; Hutchins, S.; Farahmand, F.; Mardani, M. The gait and energy efficiency of stance control knee-ankle-foot orthoses: A literature review. Prosthet. Orthot. Int. 2016, 40, 202–214. [Google Scholar] [CrossRef] [PubMed]
- Zissimopoulos, A.; Fatone, S.; Gard, S.A. Biomechanical and energetic effects of a stance-control orthotic knee joint. J. Rehabilitat. Res. Dev. 2007, 44, 503–513. [Google Scholar] [CrossRef]
- Zacharias, B.; Kannenberg, A. Clinical Benefits of Stance Control Orthosis Systems: An Analysis of the Scientific Literature. J. Prosthet. Orthot. 2012, 24, 2–7. [Google Scholar] [CrossRef]
- Ir, M.; Azuan, N. Stance-Control-Orthoses with Electromechanical Actuation Mechanism: Usefulness, Design Analysis and Directions to Overcome Challenges. J. Neurol. Neurosci. 2015. [Google Scholar] [CrossRef]
- Shamaei, K.; Dollar, A.M. On the mechanics of the knee during the stance phase of the gait. IEEE Int. Conf. Rehabil. Robot. 2011, 2011, 5975478. [Google Scholar] [CrossRef] [PubMed]
- Yakimovich, T.; Lemaire, E.D.; Kofman, J. Engineering design review of stance-control knee-ankle-foot orthoses. J. Rehabilit. Res. Dev. 2009, 46, 257. [Google Scholar] [CrossRef]
- Han, Y.; Cao, Y.; Zhao, J.; Yin, Y.; Ye, L.; Wang, X.; You, Z. A self-powered insole for human motion recognition. Sensors 2016, 16, 1502. [Google Scholar] [CrossRef] [PubMed]
- Agostini, V.; Balestra, G.; Knaflitz, M. Segmentation and classification of gait cycles. IEEE Trans. Neural Syst. Rehabilit. Eng. 2014, 22, 946–952. [Google Scholar] [CrossRef] [PubMed]
- Shahabpoor, E.; Pavic, A. Measurement of walking ground reactions in real-life environments: A systematic review of techniques and technologies. Sensors 2017, 17, 2085. [Google Scholar] [CrossRef] [PubMed]
- Munoz-Organero, M.; Parker, J.; Powell, L.; Mawson, S. Assessing walking strategies using insole pressure sensors for stroke survivors. Sensors 2016, 16, 1631. [Google Scholar] [CrossRef] [PubMed]
- Moufawad El Achkar, C.; Lenoble-Hoskovec, C.; Paraschiv-Ionescu, A.; Major, K.; Büla, C.; Aminian, K. Physical behavior in older persons during daily life: Insights from instrumented shoes. Sensors 2016, 16, 1225. [Google Scholar] [CrossRef] [PubMed]
- Tucker, M.R.; Moser, A.; Lambercy, O.; Sulzer, J.; Gassert, R. Design of a wearable perturbator for human knee impedance estimation during gait. IEEE Int. Conf. Rehabil. Robot. 2013, 2013, 6650372. [Google Scholar] [CrossRef] [PubMed]
- Espinosa, D.A. Hybrid Walking Therapy with Fatigue Management for Spinal Cord Injured Individuals. Ph.D. Thesis, Carlos III University, Madrid, Spain, 2013. [Google Scholar]
- Buerger, S.P.; Hogan, N. Impedance and Interaction Control. In Robotics and Automation Handbook; CRC Press: Boca Raton, FL, USA, 2005. [Google Scholar]
- Newman, W.S. Stability and Performance Limits of Interaction Controllers. J. Dyn. Syst. Meas. Control 1992, 114, 563–570. [Google Scholar] [CrossRef]
- Chen, B.; Zheng, E.; Wang, Q.; Wang, L. A new strategy for parameter optimization to improve phase-dependent locomotion mode recognition. Neurocomputing 2015, 149, 585–593. [Google Scholar] [CrossRef]
- Bulea, T.C.; Kobetic, R.; Triolo, R.J. Restoration of stance phase knee flexion during walking after spinal cord injury using a variable impedance orthosis. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2011, 2011, 608–611. [Google Scholar] [PubMed]
- Yan, T.; Cempini, M.; Oddo, C.M.; Vitiello, N. Review of assistive strategies in powered lower-limb orthoses and exoskeletons. Robot. Auton. Syst. 2015, 64, 120–136. [Google Scholar] [CrossRef]
- Arnos, P. Age-Related Changes in Gait: Influence of Upper-Body Posture. Ph.D. Thesis, University of Toledo, Madrid, Spain, 2007. [Google Scholar]
- Wafai, L.; Zayegh, A.; Woulfe, J.; Aziz, S.M.; Begg, R. Identification of Foot Pathologies Based on Plantar Pressure Asymmetry. Sensors 2015, 15, 20392–20408. [Google Scholar] [CrossRef] [PubMed]
- Callaghan, M.; Whitehouse, S.; Baltzopoulos, V.; Samarji, R. A Comparison of the Effects of First Metatarsophalangeal Joint Arthrodesis and Hemiarthroplasty on Function of Foot Forces using Gait Analysis. Foot Ankle Online J. 2011, 4, 1. [Google Scholar] [CrossRef]
- Lynall, R.C.; Zukowski, L.A.; Plummer, P.; Mihalik, J.P. Reliability and validity of the protokinetics movement analysis software in measuring center of pressure during walking. Gait Posture 2017, 52, 308–311. [Google Scholar] [CrossRef] [PubMed]
- De Carvalho, K.E.C.; Júnior, G.; Bolívar, M.; Sá, K.N. Translation and validation of the Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST 2.0) into Portuguese. Rev. Bras. Reumatol. 2014, 54, 260–267. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.J.; Ryu, J.C.; Moon, I.H.; Kim, K.H.; Mun, M.S. Walker gait analysis of powered gait orthosis for paraplegic. In World Congress on Medical Physics and Biomedical Engineering 2006; Springer: Berlin, Heidelberg, 2007; pp. 2889–2891. [Google Scholar]
- To, C.S.; Kobetic, R.; Bulea, T.C.; Audu, M.L.; Schnellenberger, J.R.; Pinault, G.; Triolo, R.J. Stance control knee mechanism for lower-limb support in hybrid neuroprosthesis. J. Rehabil. Res. Dev. 2011, 48, 839. [Google Scholar] [CrossRef] [PubMed]
- Arazpour, M.; Moradi, A.; Samadian, M.; Bahramizadeh, M.; Joghtaei, M.; Ahmadi Bani, M.; Hutchins, S.W.; Mardani, M.A. The influence of a powered knee–ankle–foot orthosis on walking in poliomyelitis subjects: A pilot study. Prosthet. Orthot. Int. 2016, 40, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Bachschmidt, R.A.; Harris, G.F.; Simoneau, G.G. Walker-assisted gait in rehabilitation: A study of biomechanics and instrumentation. IEEE Trans. Neural Syst. Rehabilit. Eng. 2001, 9, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Loterio, F.A.; Valadão, C.T.; Cardoso, V.F.; Pomer-Escher, A.; Bastos, T.F.; Frizera-Neto, A. Adaptation of a smart walker for stroke individuals: A study on sEMG and accelerometer signals. Res. Biomed. Eng. 2017. [Google Scholar] [CrossRef]
- Li, J.; Zhang, Z.; Tao, C.; Ji, R. Structure design of lower limb exoskeletons for gait training. Chin. J. Mech. Eng. 2015, 28, 878–887. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gait Velocity (m/s) | Cadence (steps/min) | Stance Phase (%gait cycle) | Maximum Flexion in Swing Phase () | |
|---|---|---|---|---|
| P1 | 0.18 (0.07) | 26.76 (6.87) | 49.73 (7.87) | 36.44 (9.56) |
| P2 | 0.14 (0.05) | 22.41 (3.25) | 46.19 (9.04) | 39.92 (12.40) |
| P3 | 0.18 (0.04) | 24.02 (6.22) | 44.51 (7.75) | 39.0 (10.61) |
| p-value | 0.0670 | 0.0032 * | 0.4493 | 0.1534 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Villa-Parra, A.C.; Delisle-Rodriguez, D.; Souza Lima, J.; Frizera-Neto, A.; Bastos, T. Knee Impedance Modulation to Control an Active Orthosis Using Insole Sensors. Sensors 2017, 17, 2751. https://doi.org/10.3390/s17122751
Villa-Parra AC, Delisle-Rodriguez D, Souza Lima J, Frizera-Neto A, Bastos T. Knee Impedance Modulation to Control an Active Orthosis Using Insole Sensors. Sensors. 2017; 17(12):2751. https://doi.org/10.3390/s17122751
Chicago/Turabian StyleVilla-Parra, Ana Cecilia, Denis Delisle-Rodriguez, Jessica Souza Lima, Anselmo Frizera-Neto, and Teodiano Bastos. 2017. "Knee Impedance Modulation to Control an Active Orthosis Using Insole Sensors" Sensors 17, no. 12: 2751. https://doi.org/10.3390/s17122751
APA StyleVilla-Parra, A. C., Delisle-Rodriguez, D., Souza Lima, J., Frizera-Neto, A., & Bastos, T. (2017). Knee Impedance Modulation to Control an Active Orthosis Using Insole Sensors. Sensors, 17(12), 2751. https://doi.org/10.3390/s17122751