Induction of Inflammation In Vivo by Electrocardiogram Sensor Operation Using Wireless Power Transmission



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
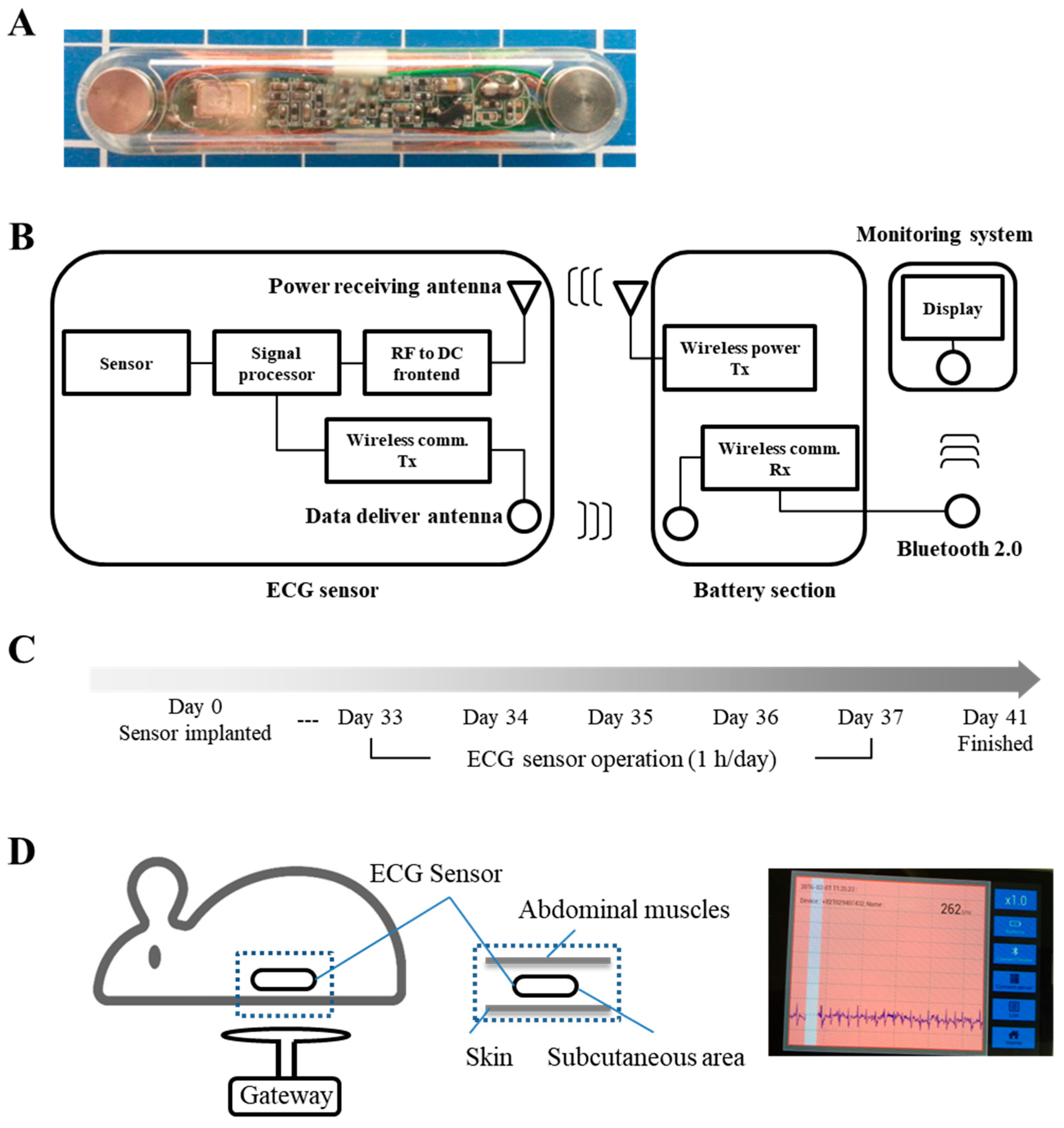
2.1. Insertion and Measurement of the ECG Sensor
2.2. Histological Analysis
2.3. Reverse Transcription-Polymerase Chain Reaction (RT-PCR) Analysis of Gene Expression
2.4. Statistical Analysis
3. Results
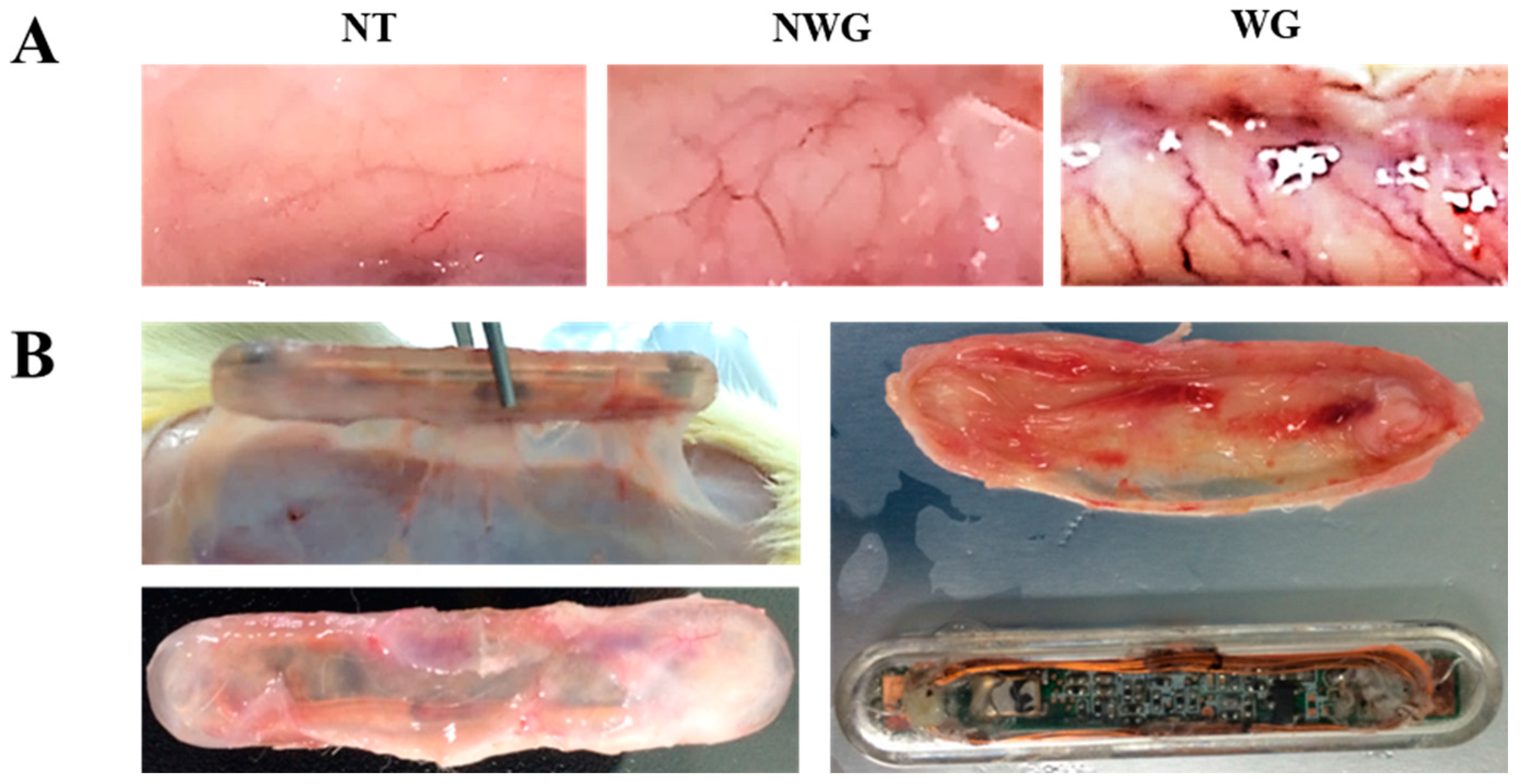
3.1. The Wireless ECG Sensor Affected the Biocompatibility of the Surrounding Tissue
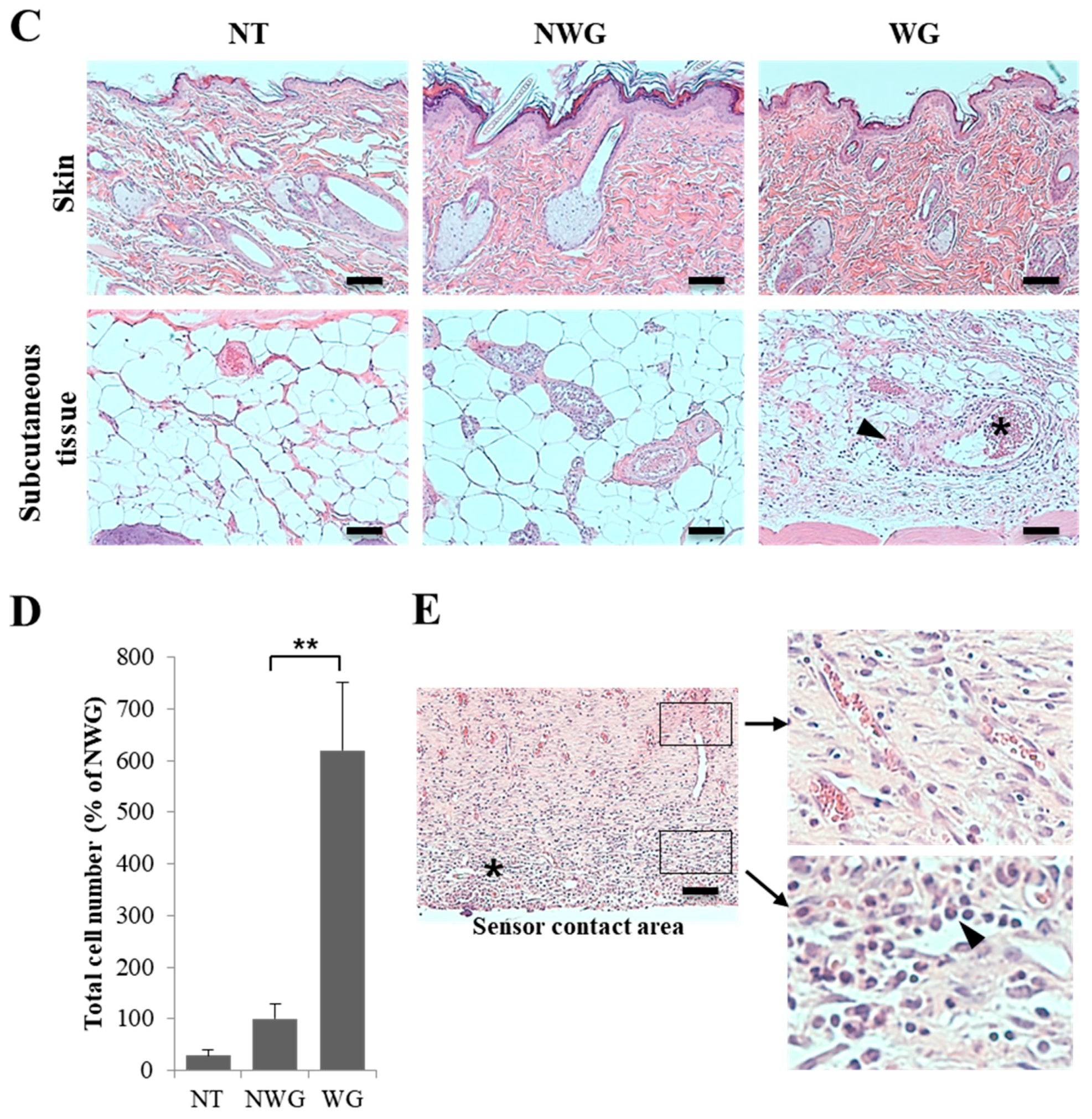
3.2. Wireless-Powered Transmission Induced Inflammatory Cell Infiltration
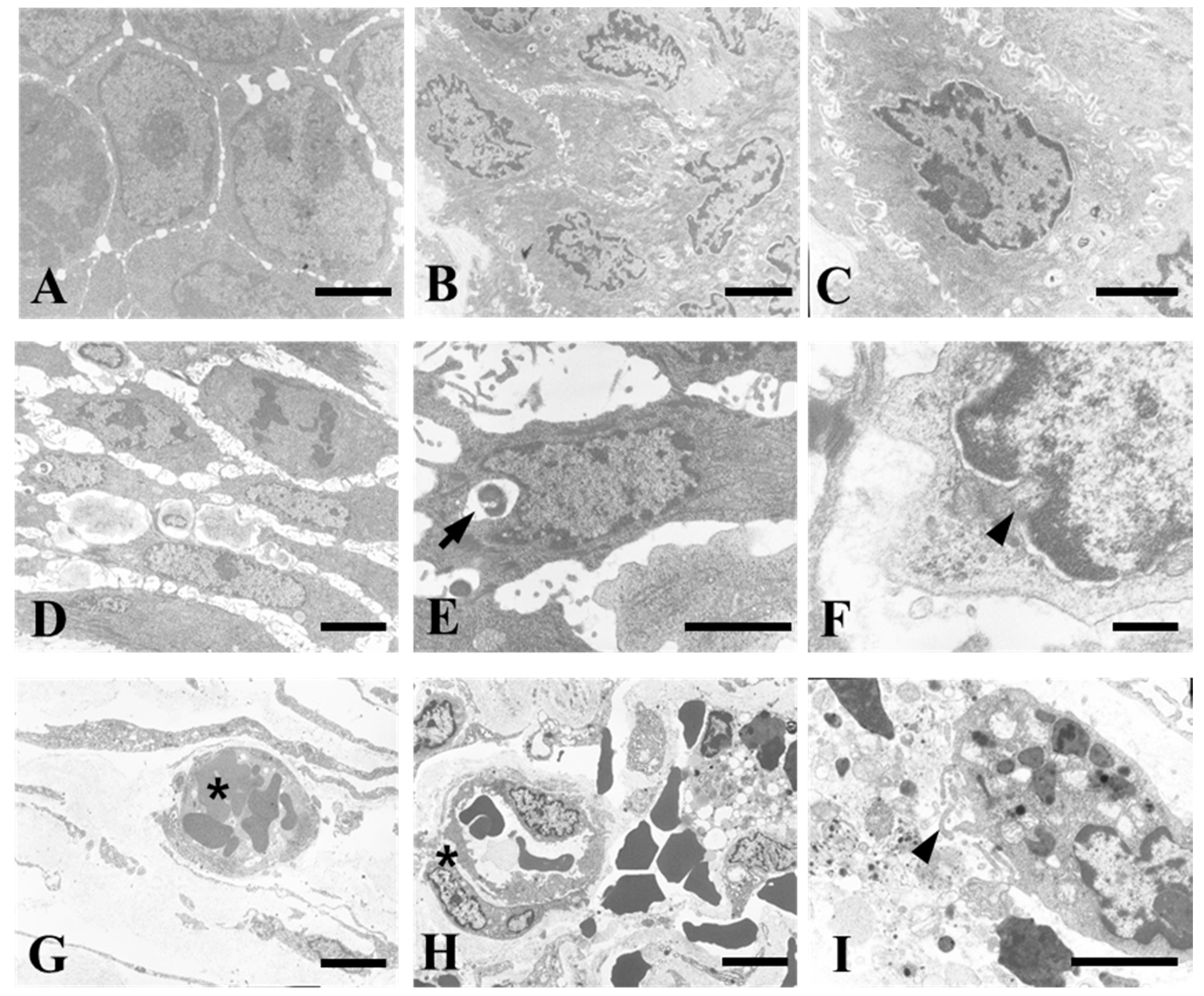
3.3. Operation of the Wireless Power Transmission Sensor Induced Cell Death by Inflammatory Reaction
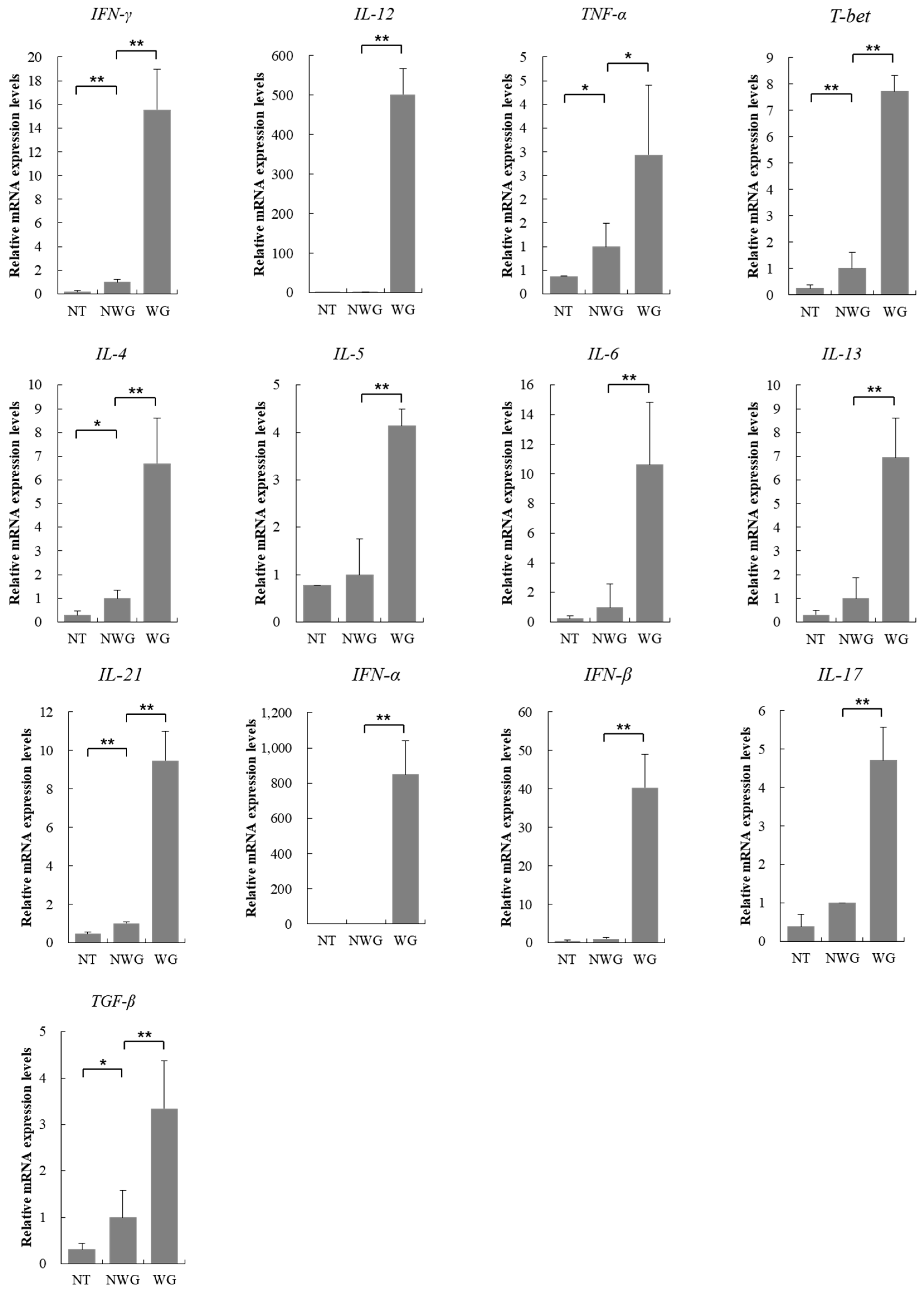
3.4. Inflammatory Markers were Upregulated Due to the Operation of the Wireless Power Transmission System
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Muller, A.J.; Knuth, M.; Nikolaus, K.S.; Krivanek, R.; Kuster, F.; Hasslacher, C.; Auffarth, G.U. Blood glucose self-monitoring with a long-term subconjunctival glucose sensor. J. Diabetes Sci. Technol. 2013, 7, 24–34. [Google Scholar] [CrossRef] [PubMed]
- Abraham, W.T.; Adamson, P.B.; Hasan, A.; Bourge, R.C.; Pamboukian, S.V.; Aaron, M.F.; Raval, N.Y. Safety and accuracy of a wireless pulmonary artery pressure monitoring system in patients with heart failure. Am. Heart J. 2011, 161, 558–566. [Google Scholar] [CrossRef] [PubMed]
- Vallejo-Heligon, S.G.; Brown, N.L.; Reichert, W.M.; Klitzman, B. Porous, Dexamethasone-loaded polyurethane coatings extend performance window of implantable glucose sensors in vivo. Acta Biomater. 2016, 30, 106–115. [Google Scholar] [CrossRef] [PubMed]
- Ruhhammer, J.; Ruh, D.; Foerster, K.; Heilmann, C.; Beyersdorf, F.; Barker, A.; Jung, B.; Seifert, A.; Goldschmidtboeing, F.; Woias, P. Arterial strain measurement by implantable capacitive sensor without vessel constriction. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2012, 2012, 535–538. [Google Scholar] [PubMed]
- Bentkover, S.H. The biology of facial fillers. Facial Plast. Surg. 2009, 25, 73–85. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.M.; Rodriguez, A.; Chang, D.T. Foreign body reaction to biomaterials. Semin. Immunol. 2008, 20, 86–100. [Google Scholar] [CrossRef] [PubMed]
- Koh, A.; Nichols, S.P.; Schoenfisch, M.H. Glucose sensor membranes for mitigating the foreign body response. J. Diabetes Sci. Technol. 2011, 5, 1052–1059. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.S.; Liu, Y.H.; Lin, C.R. A wireless sensor enabled by wireless power. Sensors 2012, 12, 16116–16143. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, M.N.; Colacci, A.; Louekari, K.; Luijten, M.; Hakkert, B.C.; Paparella, M.; Vasseur, P. International regulatory needs for development of an IATA for non-genotoxic carcinogenic chemical substances. ALTEX 2016, 33, 359–392. [Google Scholar] [CrossRef] [PubMed]
- Ho, J.S.; Yeh, A.J.; Neofytou, E.; Kim, S.; Tanabe, Y.; Patlolla, B.; Beygui, R.E.; Poon, A.S. Wireless power transfer to deep-tissue microimplants. Proc. Natl. Acad. Sci. USA 2014, 111, 7974–7979. [Google Scholar] [CrossRef] [PubMed]
- Radziemski, L.; Makin, I.R. In vivo demonstration of ultrasound power delivery to charge implanted medical devices via acute and survival porcine studies. Ultrasonics 2016, 64, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Schunck, T.; Bieth, F.; Pinguet, S.; Delmote, P. Penetration and propagation into biological matter and biological effects of high-power ultra-wideband pulses: A review. Electromagn. Biol. Med. 2016, 35, 84–101. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-H. Human implantable arrhythmia monitoring sensor with wireless power and data transmission technique. Austin J. Biosens. Bioelectron. 2015, 1, 1008. [Google Scholar]
- Heo, J.C.; Lee, S.H. Alleviation of asthma-related symptoms by a derivative of L-allo threonine. Int. J. Mol. Med. 2013, 31, 881–887. [Google Scholar] [CrossRef] [PubMed]
- Miyatake, Y.; Ikeda, H.; Ishizu, A.; Baba, T.; Ichihashi, T.; Suzuki, A.; Tomaru, U.; Kasahara, M.; Yoshiki, T. Role of neuronal interferon-γ in the development of myelopathy in rats infected with human T-Cell leukemia virus type 1. Am. J. Pathol. 2006, 169, 189–199. [Google Scholar] [CrossRef] [PubMed]
- Banos, O.; Villalonga, C.; Damas, M.; Gloesekoetter, P.; Pomares, H.; Rojas, I. PhysioDroid: Combining wearable health sensors and mobile devices for a ubiquitous, continuous, and personal monitoring. Sci. World J. 2014, 2014, 490824. [Google Scholar] [CrossRef] [PubMed]
- Bosgra, S.; Westerhout, J. Interpreting in vitro developmental toxicity test battery results: The consideration of toxicokinetics. Reprod. Toxicol. 2015, 55, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Jin, Z.; Zong, C.; Jiang, B.; Zhou, Z.; Tong, J.; Cao, Y. The effect of combined exposure of 900 MHz radiofrequency fields and doxorubicin in HL-60 cells. PLoS ONE 2012, 7, e46102. [Google Scholar] [CrossRef] [PubMed]
- Tanis, E.; Spliethoff, J.W.; Evers, D.J.; Langhout, G.C.; Snaebjornsson, P.; Prevoo, W.; Hendriks, B.H.; Ruers, T.J. Real-time in vivo assessment of radiofrequency ablation of human colorectal liver metastases using diffuse reflectance spectroscopy. Eur. J. Surg. Oncol. 2016, 42, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Lucke, L.; Bluvshtein, V. Safety considerations for wireless delivery of continuous power to implanted medical devices. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2014, 2014, 286–289. [Google Scholar] [PubMed]
- Chen, S.; Li, Q.; Wang, W.; Ma, B.; Hao, H.; Li, L. In vivo experimental study of thermal problems for rechargeable neurostimulators. Neuromodulation 2013, 16, 436–441. [Google Scholar] [CrossRef] [PubMed]
- Ha, S.; Khraiche, M.L.; Silva, G.A.; Cauwenberghs, G. Direct inductive stimulation for energy-efficient wireless neural interfaces. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2012, 2012, 883–886. [Google Scholar] [PubMed]
- Romagnani, S. T-cell subsets (Th1 versus Th2). Ann. Allergy Asthma Immunol. 2000, 85, 9–18. [Google Scholar] [CrossRef]
- Guilmot, A.; Bosse, J.; Carlier, Y.; Truyens, C. Monocytes play an IL-12-dependent crucial role in driving cord blood NK cells to produce IFN-g in response to Trypanosoma cruzi. PLoS Negl. Trop. Dis. 2013, 7, e2291. [Google Scholar] [CrossRef] [PubMed]
- Gracie, J.A.; Bradley, J.A. Interleukin-12 induces interferon-gamma-dependent switching of IgG alloantibody subclass. E. J. Immunol. 1996, 26, 1217–1221. [Google Scholar] [CrossRef] [PubMed]
- Baj-Rossi, C.; Kilinc, E.G.; Ghoreishizadeh, S.S.; Casarino, D.; Jost, T.R.; Dehollain, C.; Grassi, F.; Pastorino, L.; De Micheli, G.; Carrara, S. Full fabrication and packaging of an implantable multi-panel device for monitoring of metabolites in small animals. IEEE Trans. Biomed. Circuits Syst. 2014, 8, 636–647. [Google Scholar] [CrossRef] [PubMed]





© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heo, J.-C.; Kim, B.; Kim, Y.-N.; Kim, D.-K.; Lee, J.-H. Induction of Inflammation In Vivo by Electrocardiogram Sensor Operation Using Wireless Power Transmission. Sensors 2017, 17, 2905. https://doi.org/10.3390/s17122905
Heo J-C, Kim B, Kim Y-N, Kim D-K, Lee J-H. Induction of Inflammation In Vivo by Electrocardiogram Sensor Operation Using Wireless Power Transmission. Sensors. 2017; 17(12):2905. https://doi.org/10.3390/s17122905
Chicago/Turabian StyleHeo, Jin-Chul, Beomjoon Kim, Yoon-Nyun Kim, Dae-Kwang Kim, and Jong-Ha Lee. 2017. "Induction of Inflammation In Vivo by Electrocardiogram Sensor Operation Using Wireless Power Transmission" Sensors 17, no. 12: 2905. https://doi.org/10.3390/s17122905
APA StyleHeo, J. -C., Kim, B., Kim, Y. -N., Kim, D. -K., & Lee, J. -H. (2017). Induction of Inflammation In Vivo by Electrocardiogram Sensor Operation Using Wireless Power Transmission. Sensors, 17(12), 2905. https://doi.org/10.3390/s17122905