
A Cardiac Early Warning System with Multi Channel SCG and ECG Monitoring for Mobile Health




Abstract
:1. Introduction
2. Related Works
2.1. Motivation and Goals
- Design ECG and multi channel SCG data acquisition and communication framework for mobile health monitoring.
- Develop efficient mechanisms for feature point-based abnormality detection of ECG data.
- Develop efficient mechanisms for feature point-based abnormality detection of multi channel SCG data.
- Joint analysis of ECG and multi channel SCG data for cardiac monitoring.
- Implement the data acquisition and early warning module to collect and visualize the activities of cardiac data.
- Accuracy assessment of the early warning system for the ECG data is conducted as a case study.
3. System Model
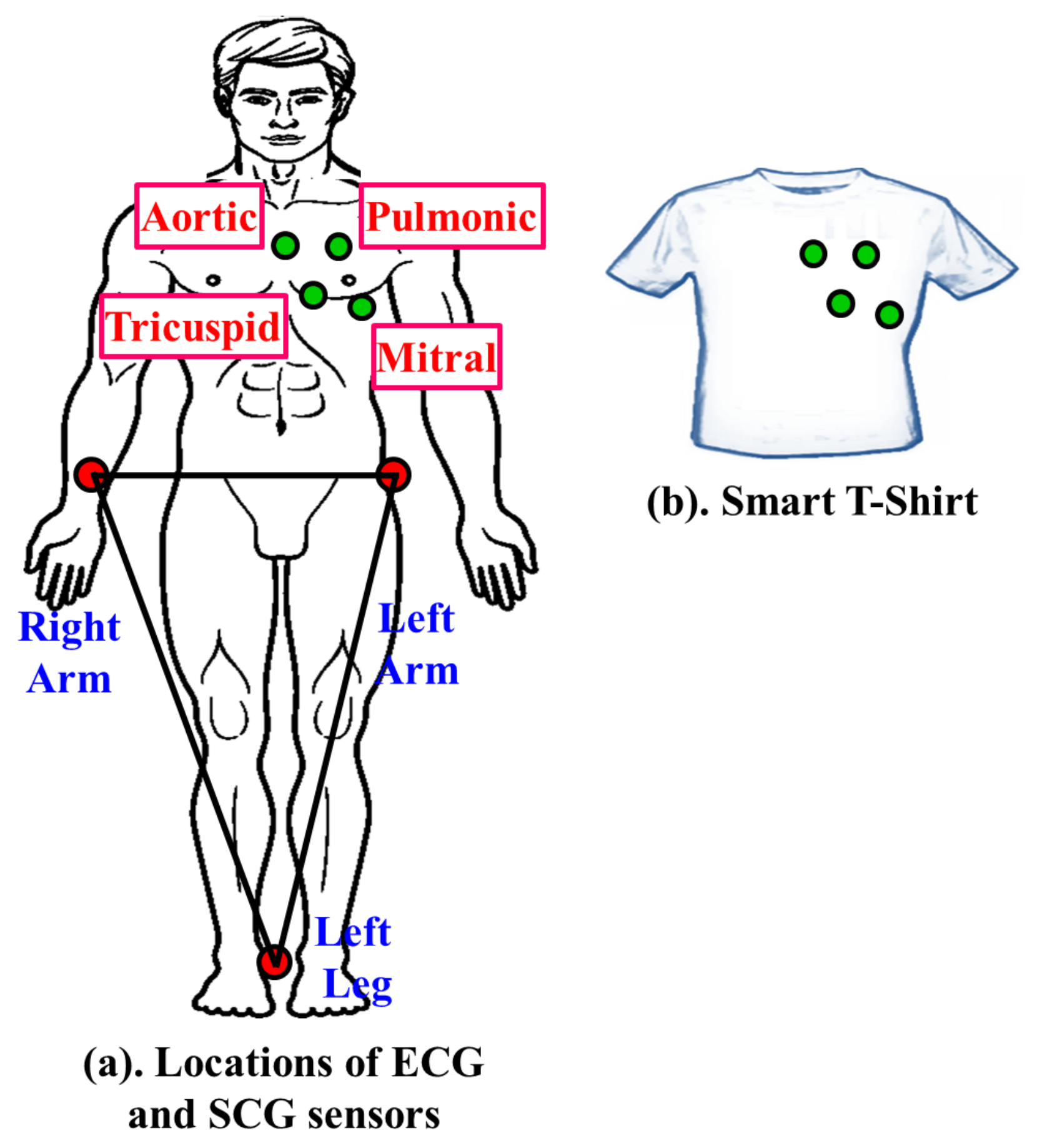
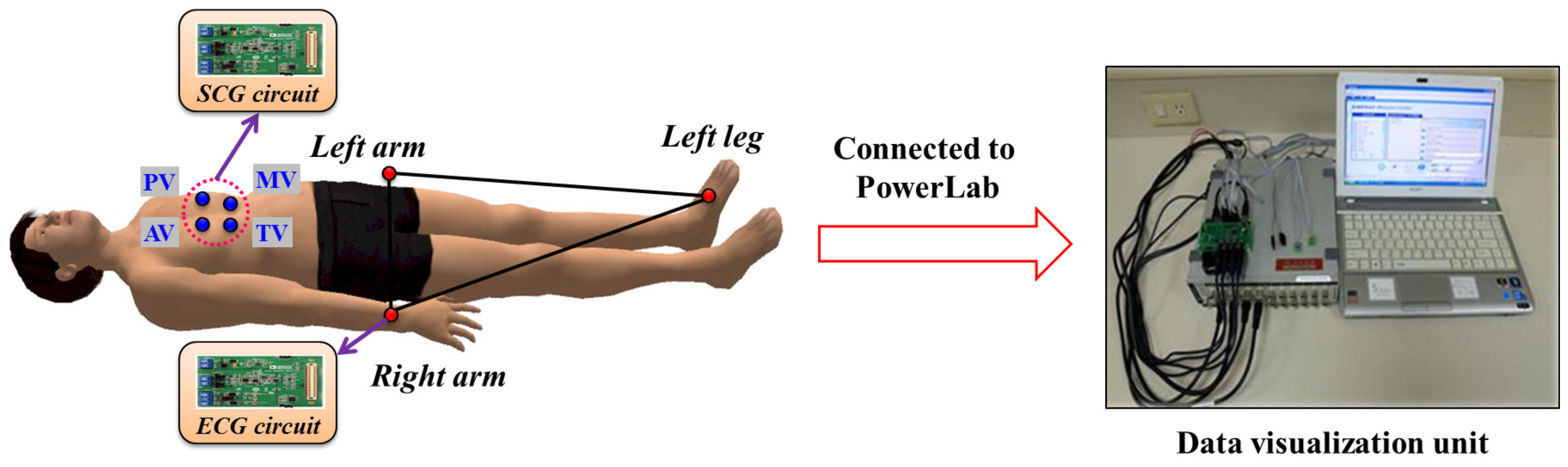
3.1. Data Acquisition Module
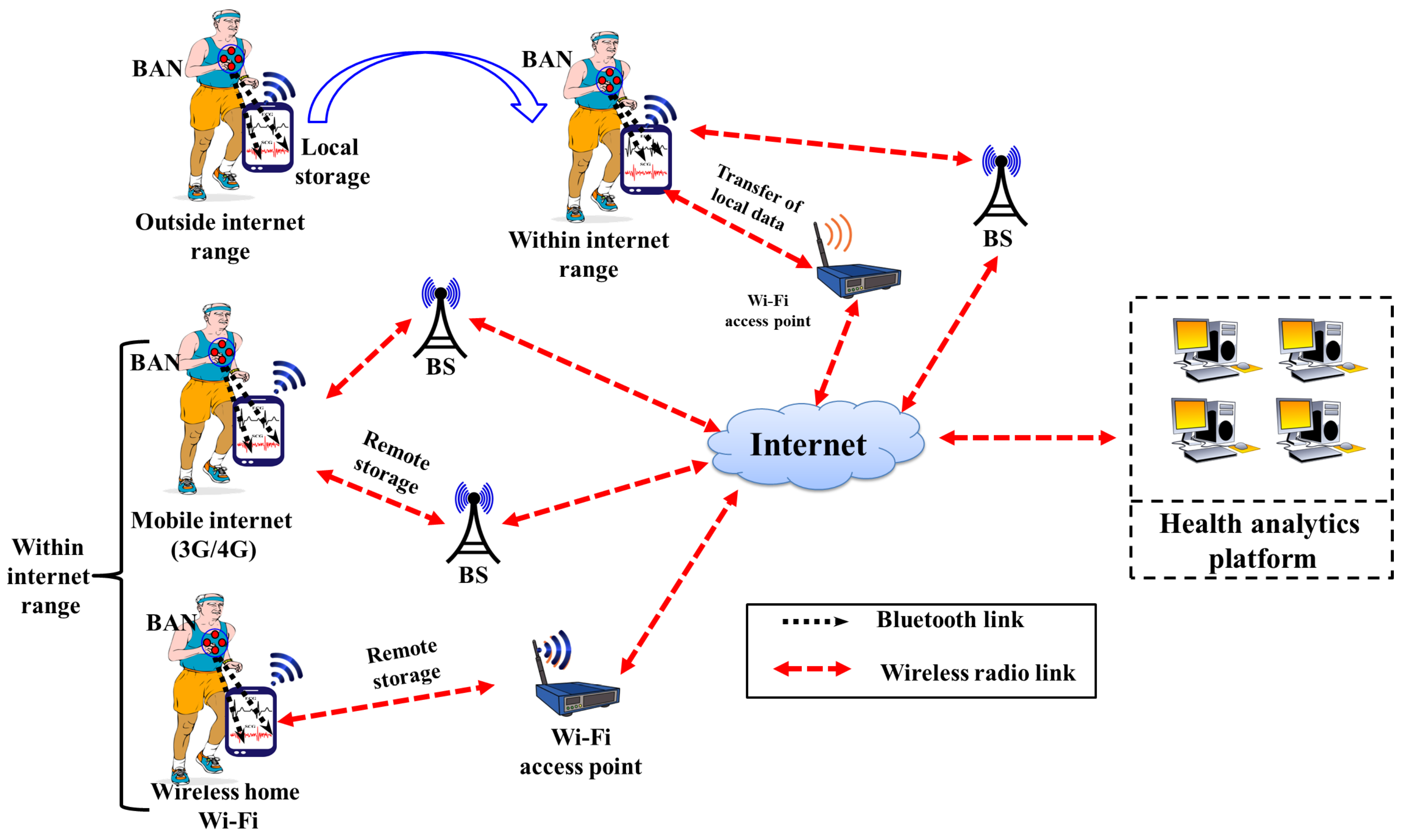
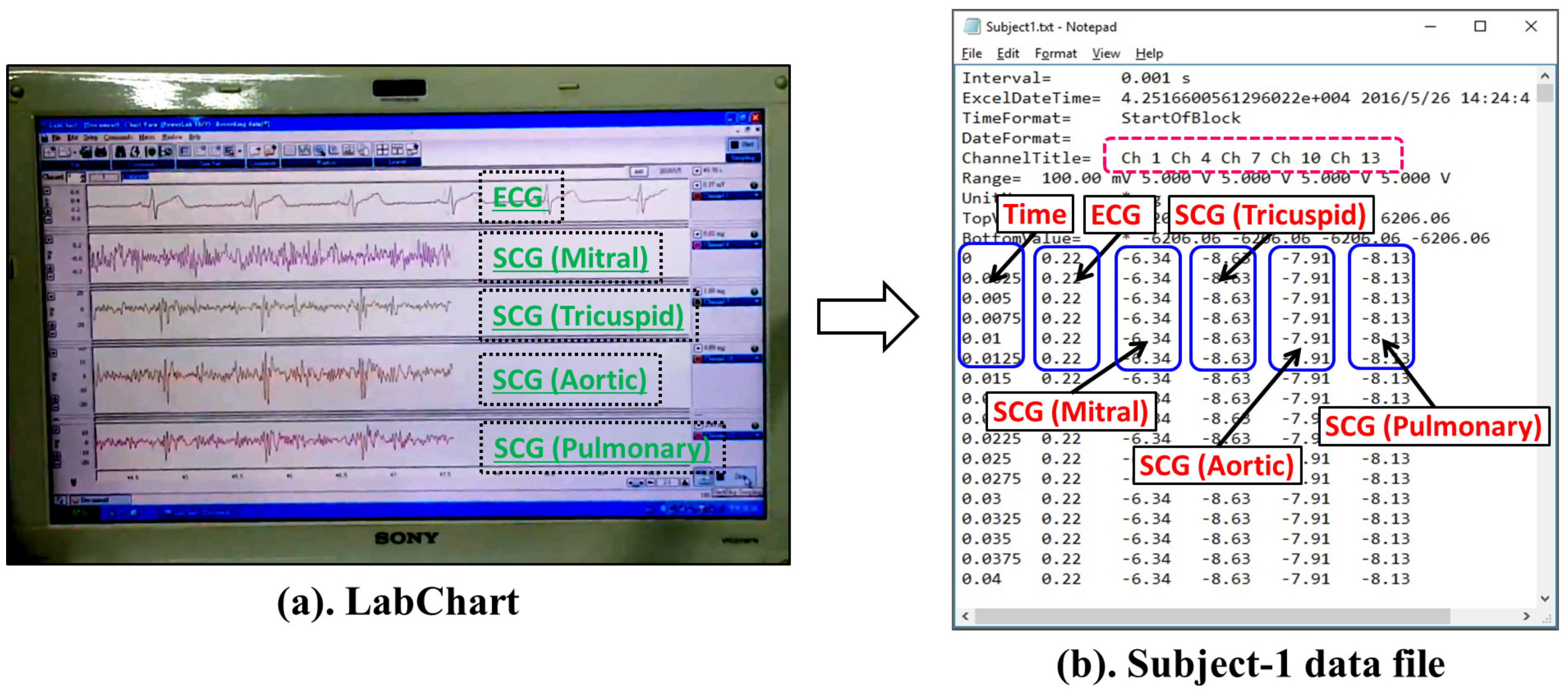
3.2. Data Communication Module
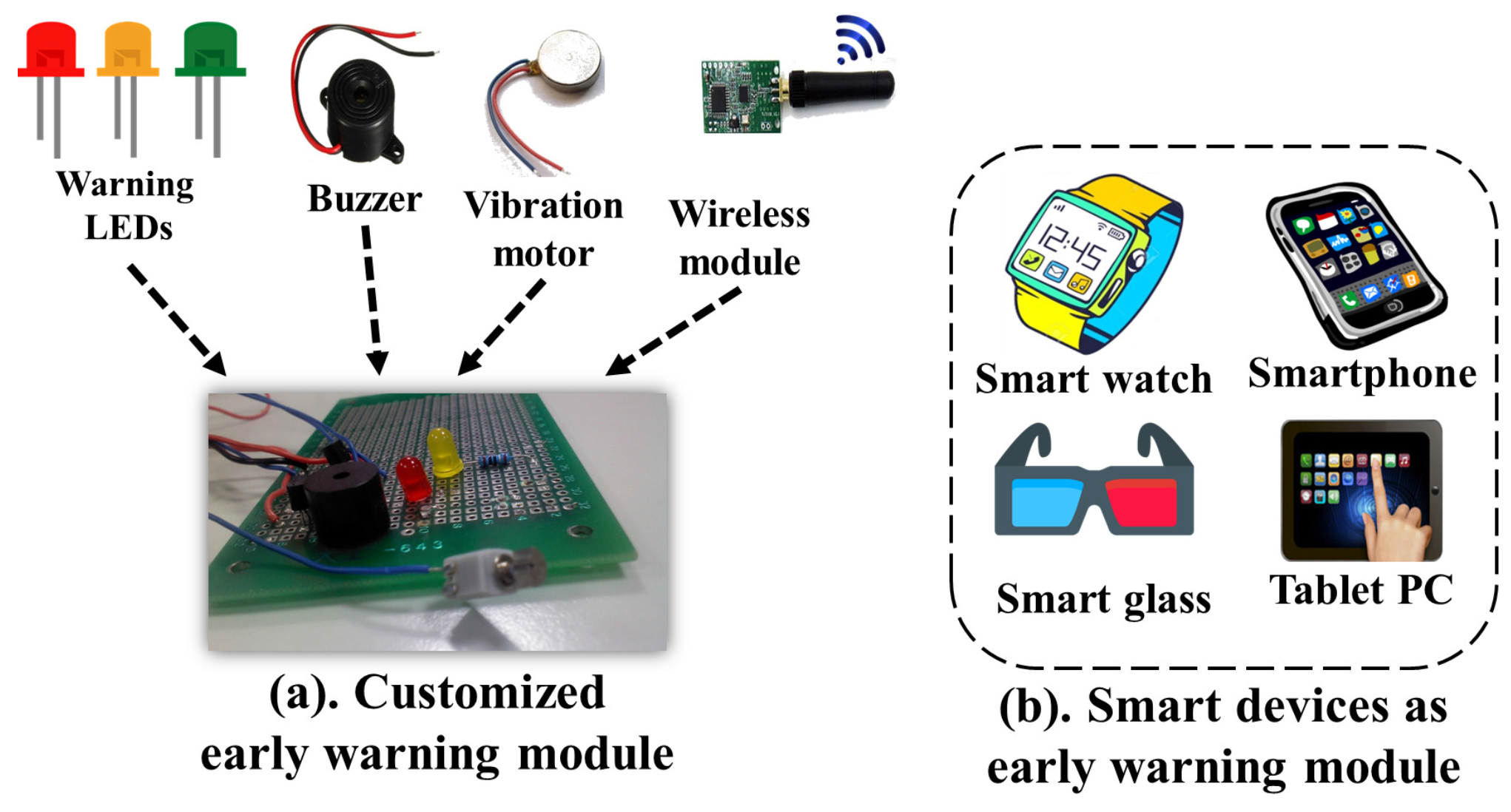
3.3. Early Warning Module
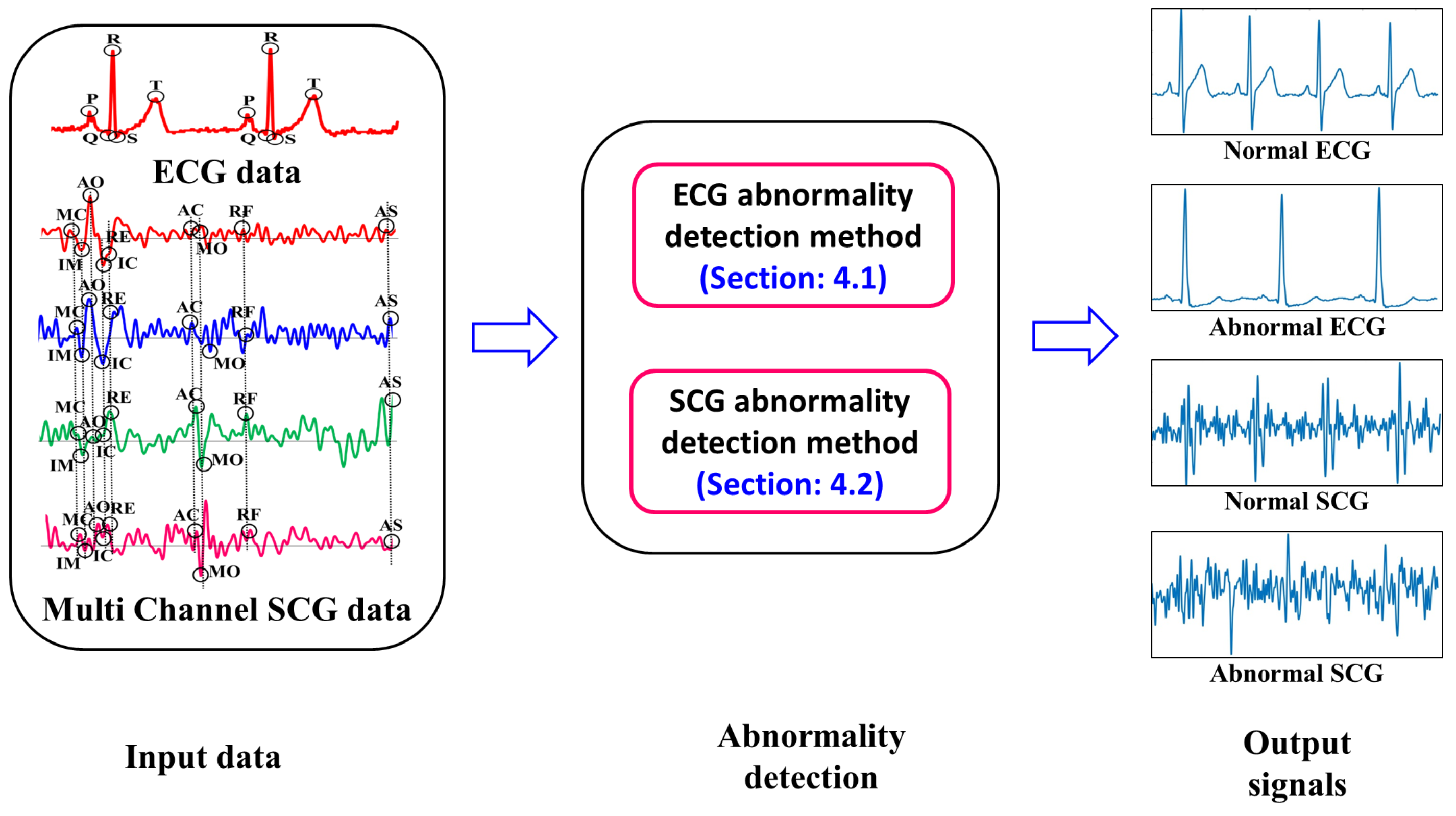
4. Cardiological Data Analysis
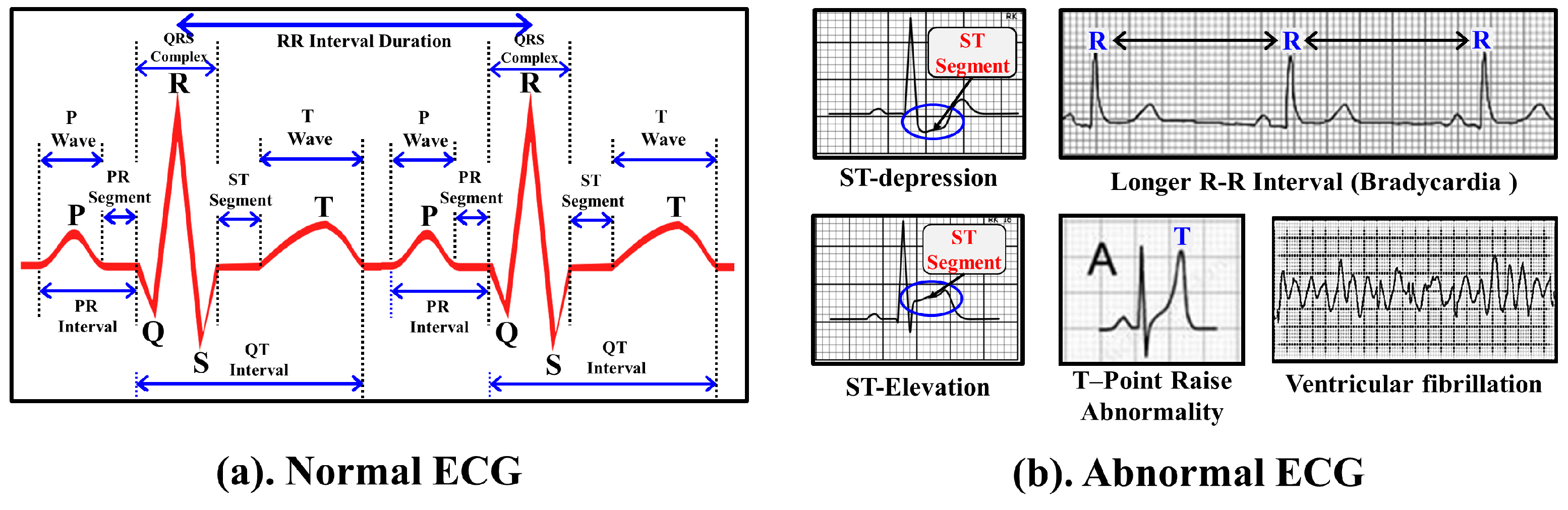
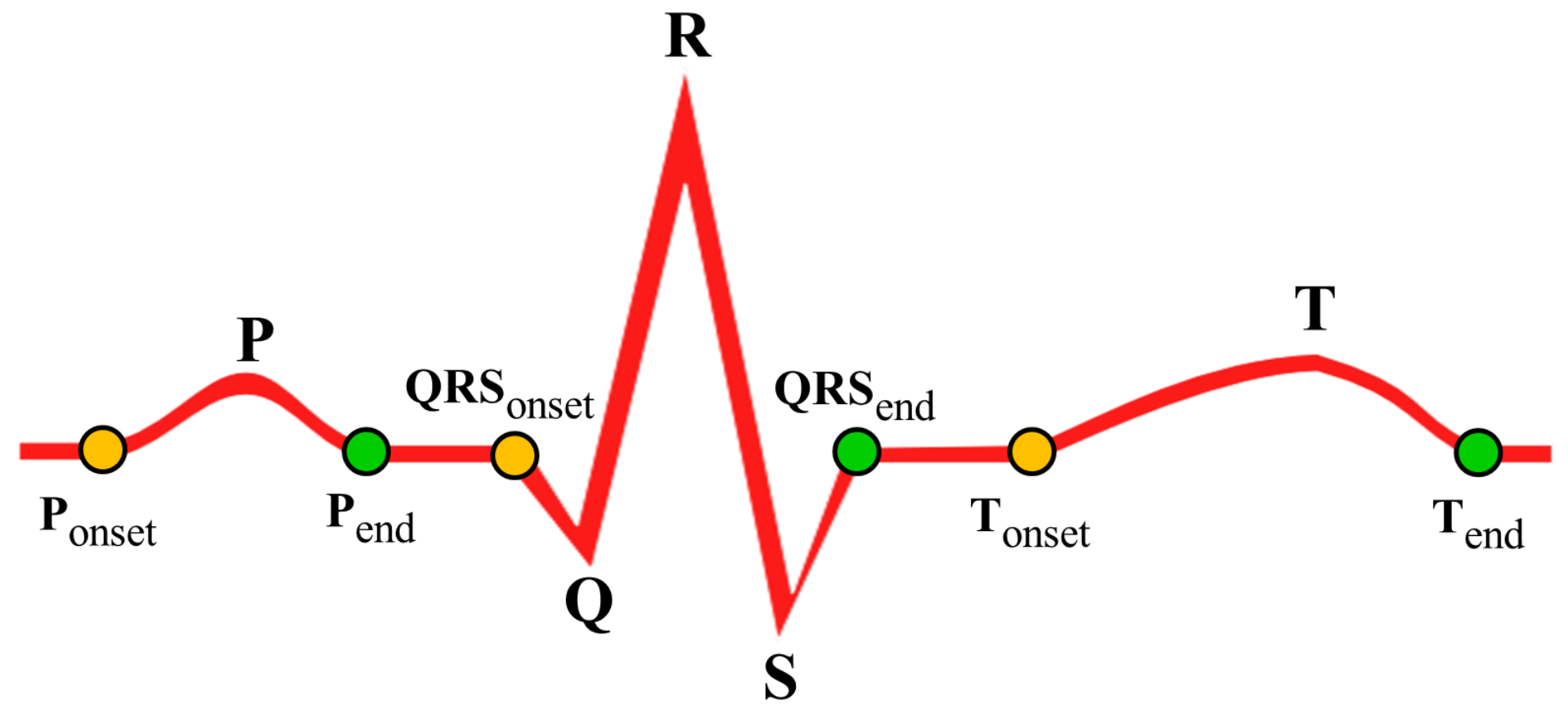
4.1. Abnormality Detection of ECG Data
| Algorithm 1: Selection of important points in ECG. |
 |
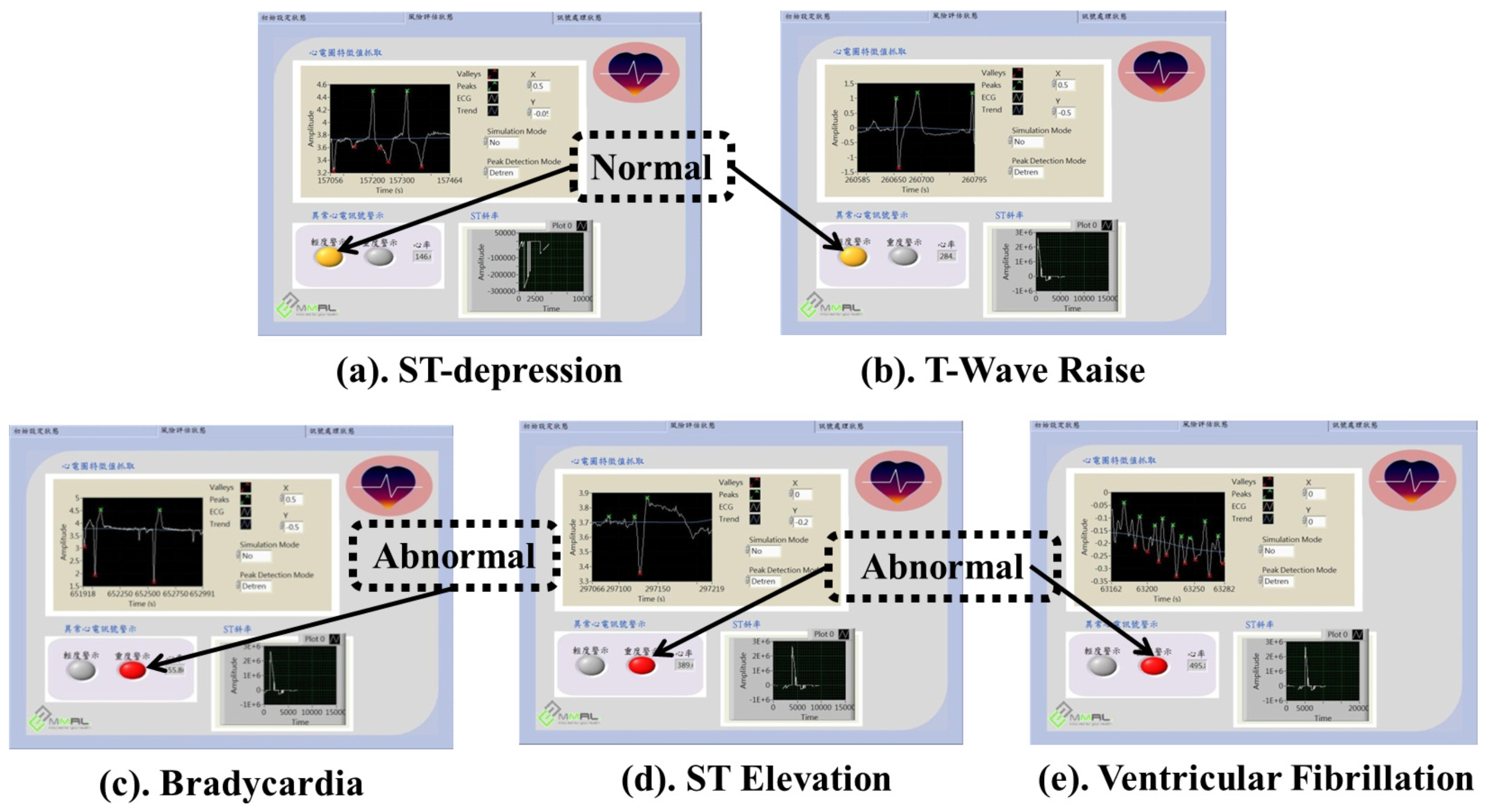
4.1.1. ST Segment Abnormality Detection
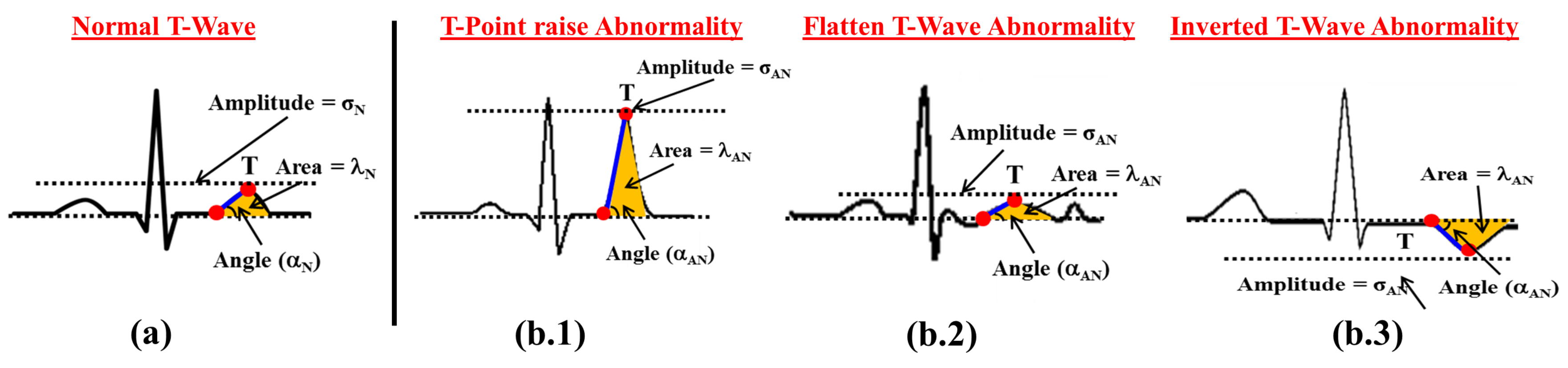
4.1.2. T-Wave Abnormality Detection
4.1.3. RR Interval Abnormality Detection
4.1.4. Other ECG Abnormalities
4.2. Abnormality Detection of SCG Data
| Algorithm 2: Selection of important points of SCG. |
 |
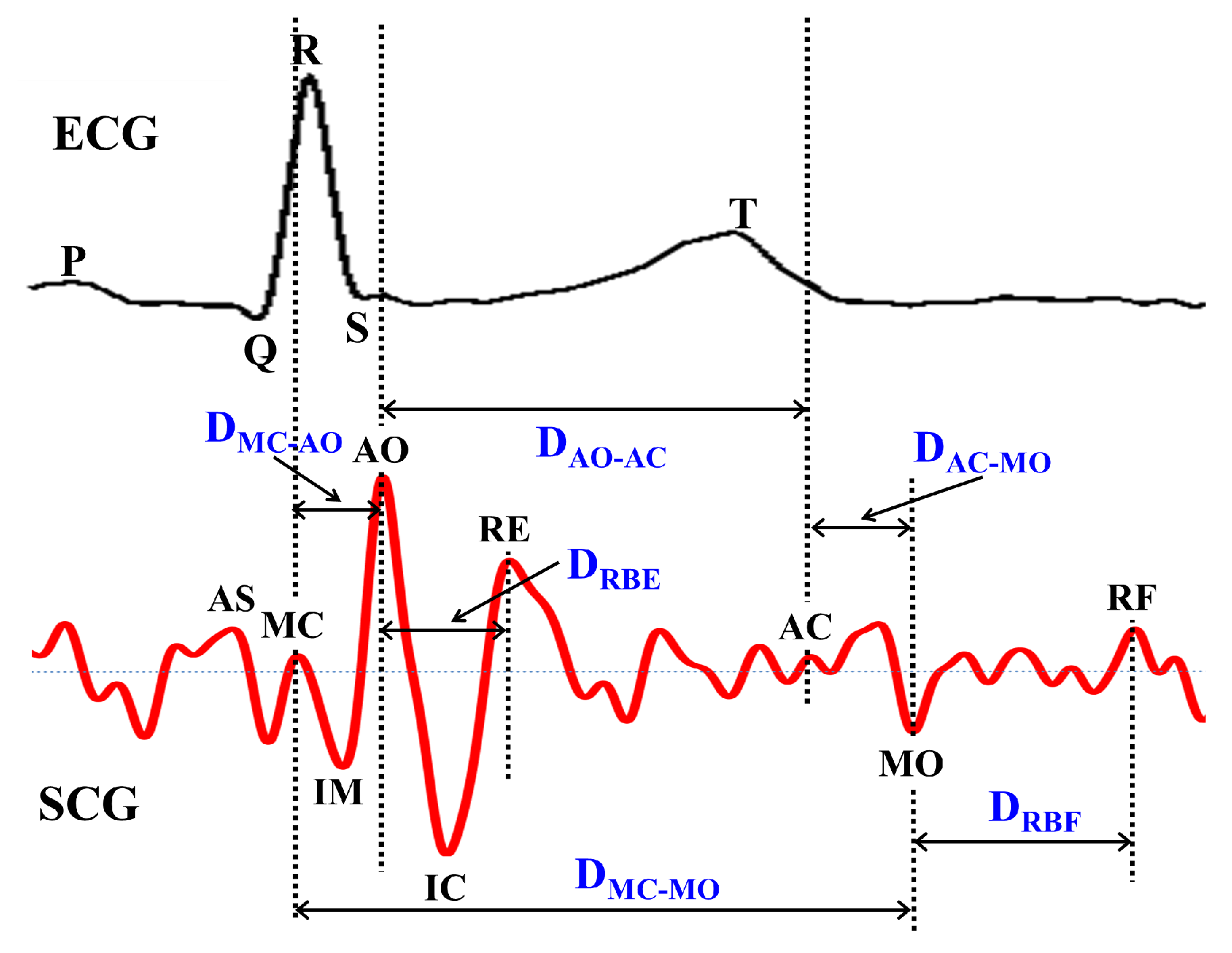
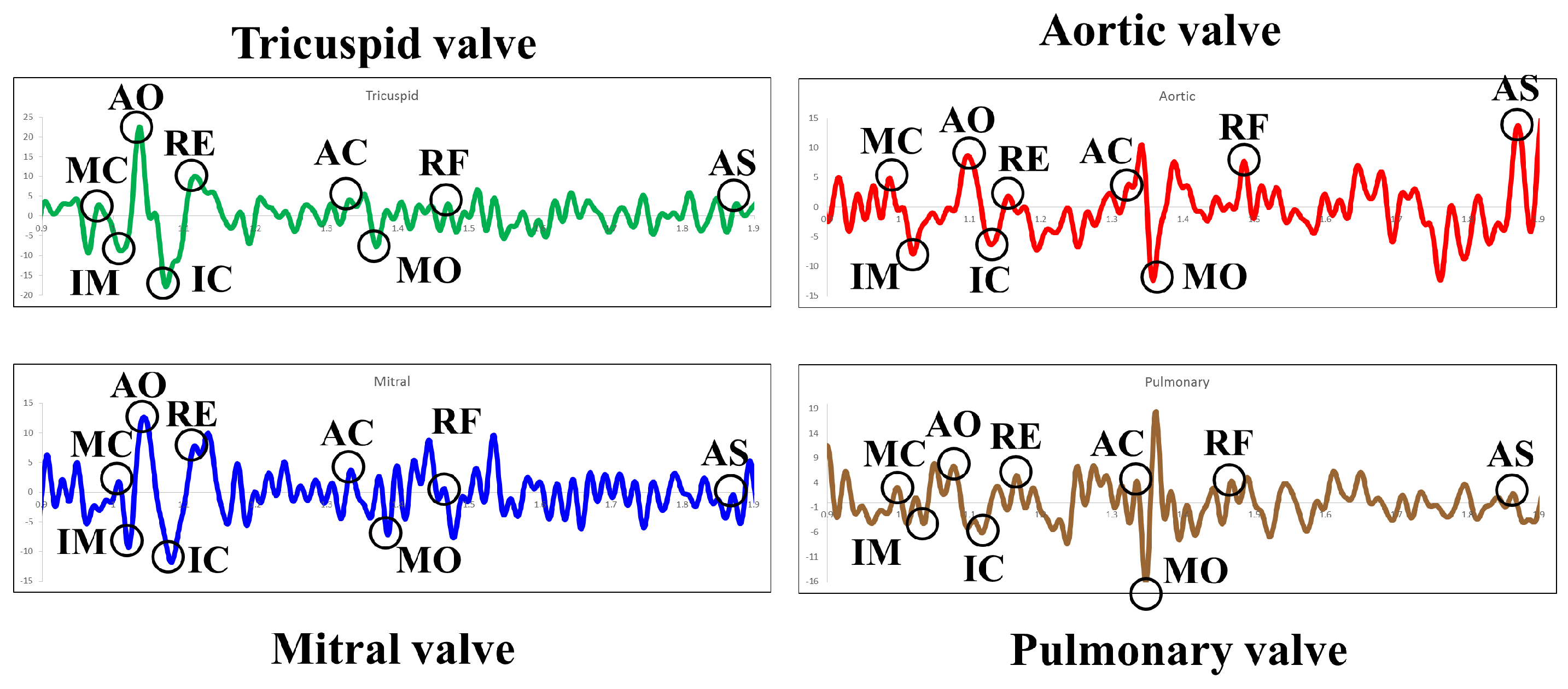
4.2.1. SCG Features Derivation
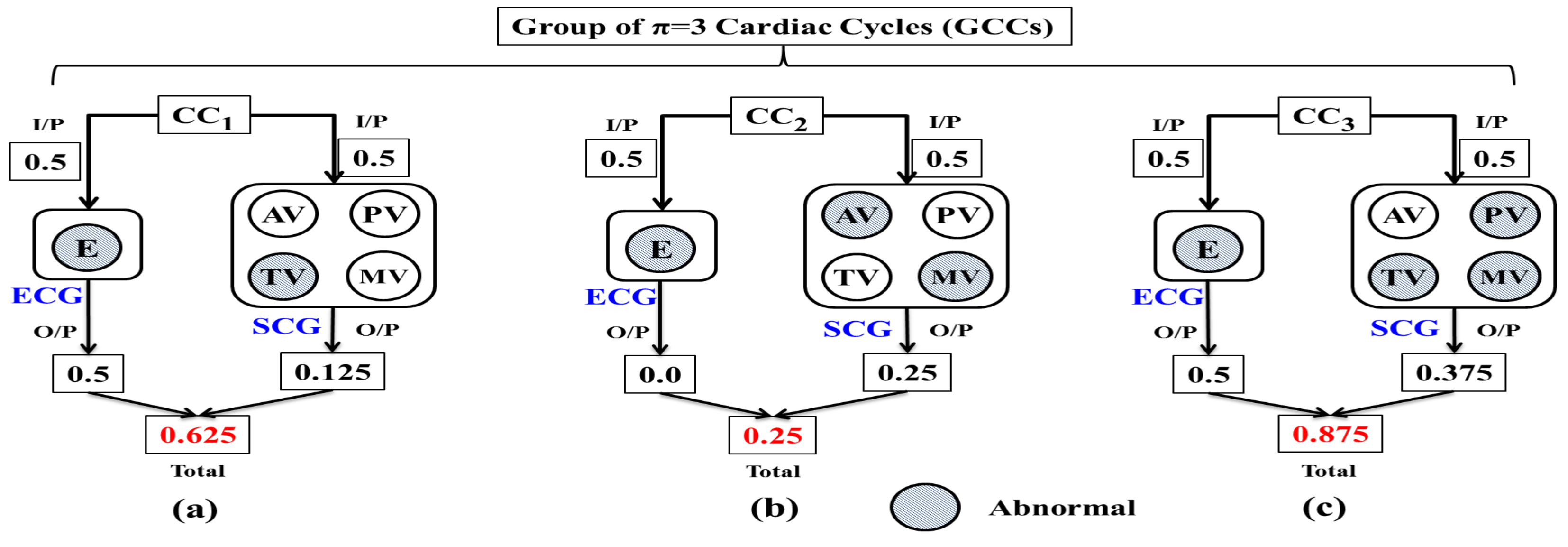
4.3. Combined Analysis of Multi Channel SCG and ECG Data
5. Implementation
5.1. Implementation of Data Acquisition Module
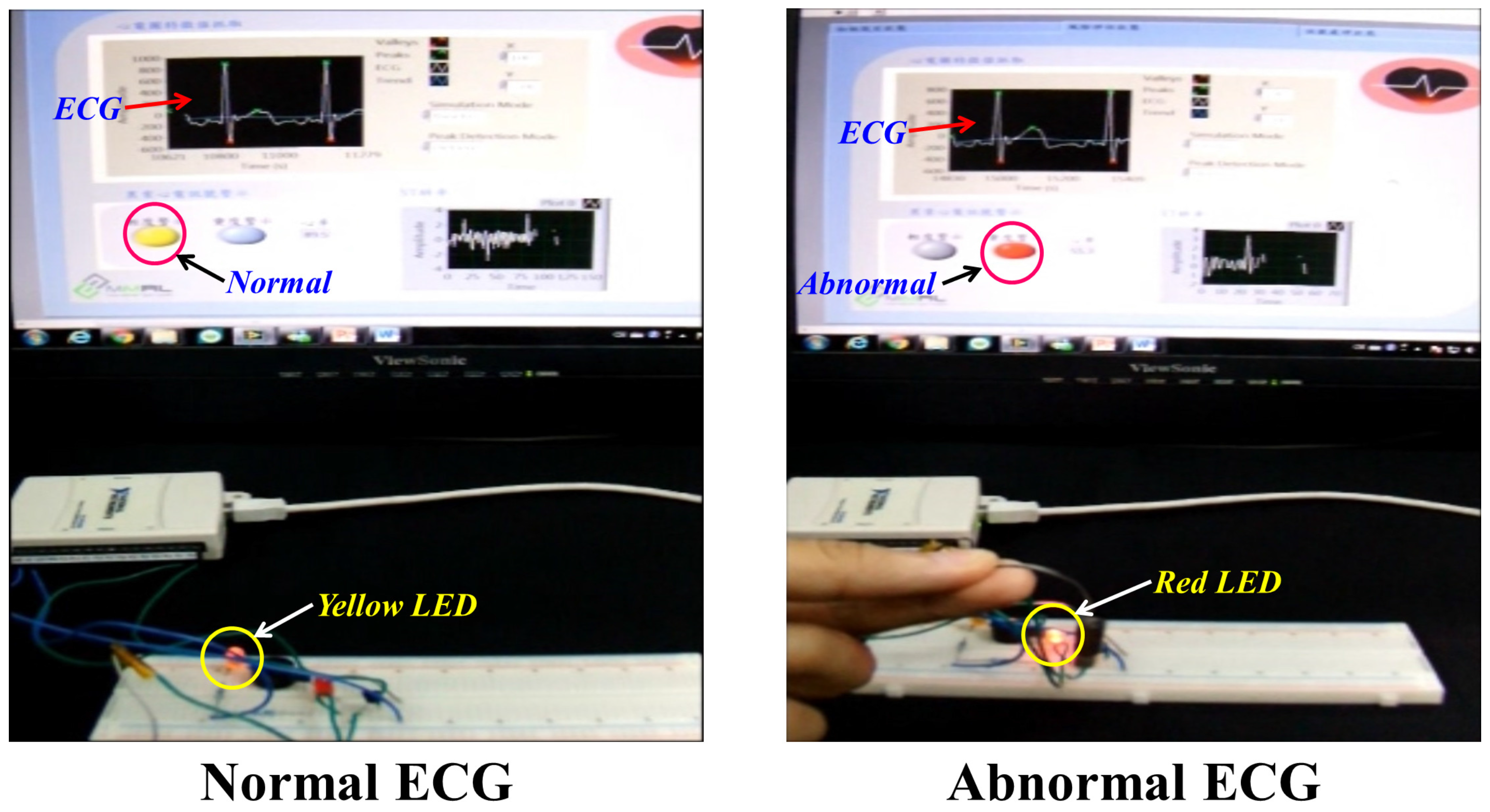
5.2. Implementation of Early Warning Module
5.3. Accuracy Assessment of Early Warning Module
5.4. Performance Evaluation of Important Points (ECG and SCG)
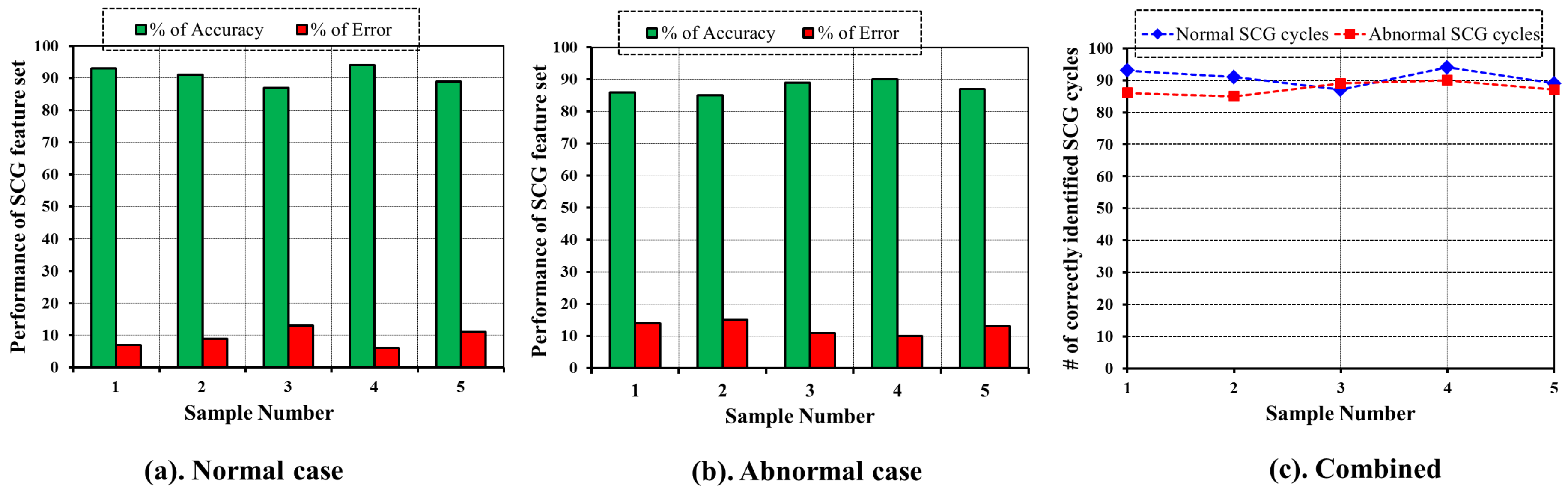
5.5. Performance Evaluation of SCG Features
6. Conclusions and Future Works
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| TPR | True Positive Rate |
| TP | True Positive |
| TN | True Negative |
| FP | False Positive |
| FN | False Negative |
References
- Hu, M.X.; Lamers, F.; de Geus, E.J.; Penninx, B.W. Influences of lifestyle factors on cardiac autonomic nervous system activity over time. Prev. Med. 2017, 94, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Townsend, N.; Nichols, M.; Scarborough, P.; Rayner, M. Cardiovascular disease in Europe—Epidemiological update 2015. Eur. Heart J. 2015, 36, 2696–2705. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; De Ferranti, S.; Després, J.P.; Fullerton, H.J.; Howard, V.J.; et al. Executive summary. Circulation 2015, 131, 434–441. [Google Scholar] [CrossRef]
- Picano, E. Economic and biological costs of cardiac imaging. Cardiovasc. Ultrasound 2005, 3, 13. [Google Scholar] [CrossRef] [PubMed]
- Mayer, F.; Stahrenberg, R.; Gröschel, K.; Mostardt, S.; Biermann, J.; Edelmann, F.; Liman, J.; Wasem, J.; Goehler, A.; Wachter, R.; et al. Cost-effectiveness of 7-day-Holter monitoring alone or in combination with transthoracic echocardiography in patients with cerebral ischemia. Clin. Res. Cardiol. 2013, 102, 875–884. [Google Scholar] [CrossRef] [PubMed]
- Majumder, S.; Mondal, T.; Deen, M.J. Wearable Sensors for Remote Health Monitoring. Sensors 2017, 17, 130. [Google Scholar] [CrossRef] [PubMed]
- Sahoo, P.K. Efficient security mechanisms for mHealth applications using wireless body sensor networks. Sensors 2012, 12, 12606–12633. [Google Scholar] [CrossRef] [PubMed]
- Kumari, P.; Mathew, L.; Syal, P. Increasing trend of wearables and multimodal interface for human activity monitoring: A review. Biosens. Bioelectron. 2017, 90, 298–307. [Google Scholar] [CrossRef] [PubMed]
- Griss, R.; Schena, A.; Reymond, L.; Patiny, L.; Werner, D.; Tinberg, C.E.; Baker, D.; Johnsson, K. Bioluminescent sensor proteins for point-of-care therapeutic drug monitoring. Nat. Chem. Biol. 2014, 10, 598–603. [Google Scholar] [CrossRef] [PubMed]
- Prioleau, T.; Moore, E.; Ghovanloo, M. Unobtrusive and Wearable Systems for Automatic Dietary Monitoring. IEEE Trans. Bio-Med. Eng. 2017. [Google Scholar] [CrossRef] [PubMed]
- Miao, F.; Cheng, Y.; He, Y.; He, Q.; Li, Y. A wearable context-aware ECG monitoring system integrated with built-in kinematic sensors of the smartphone. Sensors 2015, 15, 11465–11484. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.Y.; Chou, W.C.; Chang, P.C.; Chou, C.C.; Wen, M.S.; Ho, M.Y.; Lee, W.C.; Hsieh, M.J.; Tsai, T.H.; Lee, M.Y. Identification of Location Specific Feature Points in a Cardiac Cycle Using a Novel Seismocardiogram Spectrum System. IEEE J. Biomed. Health Informat. 2016. [Google Scholar] [CrossRef] [PubMed]
- Nemati, E.; Deen, M.J.; Mondal, T. A wireless wearable ECG sensor for long-term applications. IEEE Commun. Mag. 2012, 50. [Google Scholar] [CrossRef]
- Moyer, V.A. Screening for coronary heart disease with electrocardiography: US Preventive Services Task Force recommendation statement. Ann. Intern. Med. 2012, 157, 512–518. [Google Scholar] [CrossRef] [PubMed]
- Inan, O.T.; Migeotte, P.F.; Park, K.S.; Etemadi, M.; Tavakolian, K.; Casanella, R.; Zanetti, J.; Tank, J.; Funtova, I.; Prisk, G.K.; et al. Ballistocardiography and seismocardiography: A review of recent advances. IEEE J. Biomed. Health Inform. 2015, 19, 1414–1427. [Google Scholar] [CrossRef] [PubMed]
- Crow, R.S.; Hannan, P.; Jacobs, D.; Hedquist, L.; Salerno, D.M. Relationship between seismocardiogram and echocardiogram for events in the cardiac cycle. Am. J. Noninvasive Cardiol. 1994, 8, 39–46. [Google Scholar]
- Zanetti, J. Seismocardiography: A new technique for recording cardiac vibrations concept, method, and initial observations. J. Cardiovasc. Technol. 1990, 9, 111–118. [Google Scholar]
- Tavakolian, K.; Blaber, A.P.; Ngai, B.; Kaminska, B. Estimation of hemodynamic parameters from seismocardiogram. In Proceedings of the 2010 Computing in Cardiology, Belfast, UK, 26–29 September 2010; pp. 1055–1058. [Google Scholar]
- Di Rienzo, M.; Vaini, E.; Castiglioni, P.; Merati, G.; Meriggi, P.; Parati, G.; Faini, A.; Rizzo, F. Wearable seismocardiography: Towards a beat-by-beat assessment of cardiac mechanics in ambulant subjects. Auton. Neurosci. 2013, 178, 50–59. [Google Scholar] [CrossRef] [PubMed]
- Etemadi, M.; Inan, O.T.; Heller, J.A.; Hersek, S.; Klein, L.; Roy, S. A wearable patch to enable long-term monitoring of environmental, activity and hemodynamics variables. IEEE Trans. Biomed. Circuits Syst. 2016, 10, 280–288. [Google Scholar] [CrossRef] [PubMed]
- Annus, P.; Samieipour, A.; Rist, M.; Ruiso, I.; Krivoshei, A.; Land, R.; Parve, T.; Min, M. Wearable Data Acquisition System of Multimodal Physiological Signal for Personal Health Care. In PHealth 2013: Proceedings of the 10th International Conference on Wearable Micro and Nano Technologies for Personalized Health; IOS Press: Amsterdam, The Netherlands, 2013; Volume 189, p. 107. [Google Scholar]
- Huang, Y.M.; Hsieh, M.Y.; Chao, H.C.; Hung, S.H.; Park, J.H. Pervasive, secure access to a hierarchical sensor-based healthcare monitoring architecture in wireless heterogeneous networks. IEEE J. Sel. Areas Commun. 2009, 27, 400–411. [Google Scholar] [CrossRef]
- He, H.; Du, Z.; Zhang, W.; Chen, A. Optimization strategy of Hadoop small file storage for big data in healthcare. J. Supercomput. 2016, 72, 3696–3707. [Google Scholar] [CrossRef]
- Sahoo, P.K.; Mohapatra, S.K.; Wu, S.L. Analyzing Healthcare Big Data with Prediction for Future Health Condition. IEEE Access 2017, 4, 9786–9799. [Google Scholar] [CrossRef]
- Hon, C.P.; Pereira, M.; Sushmita, S.; Teredesai, A.; De Cock, M. Risk Stratification for Hospital Readmission of Heart Failure Patients: A Machine Learning Approach. In Proceedings of the 7th ACM International Conference on Bioinformatics, Computational Biology, and Health Informatics, Seattle, WA, USA, 2–5 October 2016; pp. 491–492. [Google Scholar]
- Pandey, S.; Voorsluys, W.; Niu, S.; Khandoker, A.; Buyya, R. An autonomic cloud environment for hosting ECG data analysis services. Future Gener. Comput. Syst. 2012, 28, 147–154. [Google Scholar] [CrossRef]
- Gia, T.N.; Jiang, M.; Rahmani, A.M.; Westerlund, T.; Liljeberg, P.; Tenhunen, H. Fog computing in healthcare internet of things: A case study on ecg feature extraction. In Proceedings of the 2015 IEEE International Conference on Computer and Information Technology; Ubiquitous Computing and Communications; Dependable, Autonomic and Secure Computing; Pervasive Intelligence and Computing (CIT/IUCC/DASC/PICOM), Liverpool, UK, 26–28 October 2015; pp. 356–363. [Google Scholar]
- Wolgast, G.; Ehrenborg, C.; Israelsson, A.; Helander, J.; Johansson, E.; Manefjord, H. Wireless Body Area Network for Heart Attack Detection [Education Corner]. IEEE Antennas Propag. Mag. 2016, 58, 84–92. [Google Scholar] [CrossRef]
- Gyselinckx, B.; Penders, J.; Vullers, R. Potential and challenges of body area networks for cardiac monitoring. J. Electrocardiol. 2007, 40, S165–S168. [Google Scholar] [CrossRef] [PubMed]
- Mundt, C.W.; Montgomery, K.N.; Udoh, U.E.; Barker, V.N.; Thonier, G.C.; Tellier, A.M.; Ricks, R.D.; Darling, R.B.; Cagle, Y.D.; Cabrol, N.A.; et al. A multiparameter wearable physiologic monitoring system for space and terrestrial applications. IEEE Trans. Inf. Technol. Biomed. 2005, 9, 382–391. [Google Scholar] [CrossRef] [PubMed]
- Mitra, U.; Emken, B.A.; Lee, S.; Li, M.; Rozgic, V.; Thatte, G.; Vathsangam, H.; Zois, D.S.; Annavaram, M.; Narayanan, S.; et al. KNOWME: A case study in wireless body area sensor network design. IEEE Commun. Mag. 2012, 50, 116–125. [Google Scholar] [CrossRef]
- Von Rosenberg, W.; Chanwimalueang, T.; Goverdovsky, V.; Looney, D.; Sharp, D.; Mandic, D.P. Smart Helmet: Wearable Multichannel ECG and EEG. IEEE J. Transl. Eng. Health Med. 2016, 4. [Google Scholar] [CrossRef] [PubMed]
- Page, A.; Soyata, T.; Couderc, J.P.; Aktas, M. An open source ECG clock generator for visualization of long-term cardiac monitoring data. IEEE Access 2015, 3, 2704–2714. [Google Scholar] [CrossRef]
- Morrison, T.; Silver, J.; Otis, B. A single-chip encrypted wireless 12-lead ECG smart shirt for continuous health monitoring. In Proceedings of the 2014 Symposium on VLSI Circuits Digest of Technical Papers, Honolulu, HI, USA, 10–13 June 2014; pp. 1–2. [Google Scholar]
- Pandian, P.; Mohanavelu, K.; Safeer, K.; Kotresh, T.; Shakunthala, D.; Gopal, P.; Padaki, V. Smart Vest: Wearable multi-parameter remote physiological monitoring system. Med. Eng. Phys. 2008, 30, 466–477. [Google Scholar] [CrossRef] [PubMed]
- Miramontes, R.; Aquino, R.; Flores, A.; Rodríguez, G.; Anguiano, R.; Ríos, A.; Edwards, A. PlaIMoS: A Remote Mobile Healthcare Platform to Monitor Cardiovascular and Respiratory Variables. Sensors 2017, 17, 176. [Google Scholar] [CrossRef] [PubMed]
- Tavakolian, K.; Portacio, G.; Tamddondoust, N.R.; Jahns, G.; Ngai, B.; Dumont, G.A.; Blaber, A.P. Myocardial contractility: A seismocardiography approach. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August–1 September 2012; pp. 3801–3804. [Google Scholar]
- Shimmer, Discovery in Motion. Available online: http://www.shimmersensing.com/products/shimmer3-ecg-unit (accessed on 18 March 2017).
- Pani, D.; Dessì, A.; Saenz-Cogollo, J.F.; Barabino, G.; Fraboni, B.; Bonfiglio, A. Fully textile, PEDOT: PSS based electrodes for wearable ECG monitoring systems. IEEE Trans. Biomed. Eng. 2016, 63, 540–549. [Google Scholar] [CrossRef] [PubMed]
- Spano, E.; Di Pascoli, S.; Iannaccone, G. Low-power wearable ECG monitoring system for multiple-patient remote monitoring. IEEE Sens. J. 2016, 16, 5452–5462. [Google Scholar]
- Righter, W.H.; Nicoll, A.J.; Kennedy, H.L. Portable, Multi-Channel ECG Data Monitor/Recorder. U.S. Patent 5,365,935, 22 November 1994. [Google Scholar]
- Peng, M.; Wang, T.; Hu, G.; Zhang, H. A wearable heart rate belt for ambulant ECG monitoring. In Proceedings of the 2012 IEEE 14th International Conference on e-Health Networking, Applications and Services (Healthcom), Beijing, China, 10–13 October 2012; pp. 371–374. [Google Scholar]
- Di Rienzo, M.; Meriggi, P.; Rizzo, F.; Castiglioni, P.; Lombardi, C.; Ferratini, M.; Parati, G. Textile technology for the vital signs monitoring in telemedicine and extreme environments. IEEE Trans. Inf. Technol. Biomed. 2010, 14, 711–717. [Google Scholar] [CrossRef] [PubMed]
- Baronti, P.; Pillai, P.; Chook, V.W.; Chessa, S.; Gotta, A.; Hu, Y.F. Wireless sensor networks: A survey on the state of the art and the 802.15. 4 and ZigBee standards. Comput. Commun. 2007, 30, 1655–1695. [Google Scholar] [CrossRef]
- Braojos, R.; Ansaloni, G.; Atienza, D.; Rincón, F.J. Embedded real-time ECG delineation methods: A comparative evaluation. In Proceedings of the 2012 IEEE 12th International Conference on Bioinformatics & Bioengineering (BIBE), Larnaca, Cyprus, 11–13 November 2012; pp. 99–104. [Google Scholar]
- Rijnbeek, P.R.; van Herpen, G.; Bots, M.L.; Man, S.; Verweij, N.; Hofman, A.; Hillege, H.; Numans, M.E.; Swenne, C.A.; Witteman, J.C.; et al. Normal values of the electrocardiogram for ages 16–90 years. J. Electrocardiol. 2014, 47, 914–921. [Google Scholar] [CrossRef] [PubMed]
- Normal Electrocardiography (ECG) Intervals. 2014. Available online: http://emedicine.medscape.com/article/2172196-overview (accessed on 26 April 2016).
- Johnston, F.; Boyland, J.; Meadows, M.; Shale, E. Some properties of a simple moving average when applied to forecasting a time series. J. Oper. Res. Soc. 1999, 50, 1267–1271. [Google Scholar] [CrossRef]
- Welford, B. Note on a method for calculating corrected sums of squares and products. Technometrics 1962, 4, 419–420. [Google Scholar]
- Knuth, D.E. The Art of Computer Programming, 2: Seminumerical Algorithms; Addision Wesley: Reading, MA, USA, 1998. [Google Scholar]
- Grubbs, F.E. Procedures for detecting outlying observations in samples. Technometrics 1969, 11, 53. [Google Scholar] [CrossRef]
- MEMS Motion Sensor: Ultra Low Power High Performance 3-Axis Digital Accelerometer. Available online: http://www.st.com/en/mems-and-sensors/lis331dlh.html (accessed on 10 January 2017).
- ADUC7020 Precision Analog Microcontroller. Available online: http://www.analog.com/en/products/processors-dsp/microcontrollers/arm7-core-products/aduc7020.html (accessed on 16 January 2017).
- PowerLab Data with Integrity. Available online: https://www.adinstruments.com/products/powerlab (accessed on 12 January 2017).
- LabChart Enabling Discovery. Available online: https://www.adinstruments.com/products/labchart (accessed on 19 January 2017).




















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Notation | Meaning |
|---|---|
| Normal P wave Duration (80 ms) | |
| Normal P wave amplitude (0.1 mm, 0.2 mm) | |
| Normal wave Duration (80 ms, 100 ms) | |
| Normal wave amplitude (≤1 mm) |
| Notation | Meaning |
|---|---|
| Time duration from closing of mitral valve to opening of aortic valve. | |
| Time duration between opening and closing of aortic valve. | |
| Time duration between closing and opening of mitral valve. | |
| Time duration from closing of aortic valve to opening of mitral valve. | |
| Time duration of systolic blood ejection. | |
| Time duration of diastolic blood filling. |
| Subject No. | Gender | Age | Height (m) | Weight (Kg) | BMI | ECG (mV) | SCG Mitral (mV) | SCG Tricuspid (mV) | SCG Aortic (mV) | SCG Pulmonary (mV) |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Male | 23 | 1.71 | 62 | 21.2 | 0.23 | −2.01 | −1.08 | −1.33 | −3.27 |
| 2 | Female | 27 | 1.66 | 57 | 20.7 | 0.22 | −6.34 | −8.63 | −7.91 | −8.13 |
| 3 | Male | 24 | 1.8 | 78 | 24.1 | 0.62 | −0.95 | −0.16 | −2.68 | 3.08 |
| … | … | … | … | … | … | … | … | … | … | … |
| 50 | Female | 28 | 1.69 | 66 | 23.1 | 0.33 | −2.73 | −4.98 | 2.73 | −3.12 |
| Component | Specification |
|---|---|
| Yellow LED | Wavelength = 585 nm–595 nm, Emission luminance = 3000–5000 mcd, Voltage = 1.8–2.2 V. |
| Red LED | Wavelength = 620 nm–625 nm, Emission luminance = 1000–1500 mcd, Voltage = 1.9–2.2 V. |
| Buzzer | 15 Vp-p 3 mA 80 dB. |
| Vibration Motor | Rate voltage = 3.0 V, Rated current = 60 mA Max, Rated speed = 1400 ± 2500 rpm, |
| Stall current = 70 mA Max, Terminal impedance = 40 ± 20%. Stall current = 70 mA Max, | |
| Terminal impedance = 40 ± 20%. |
| Average Heart Beat Rate | Total # of Data Points | # of ECG Important Points | # of SCG Important Points | |
|---|---|---|---|---|
| 82 | 5854 | 100 | 180 | |
| 63 | 7619 | 100 | 180 | |
| 71 | 6761 | 100 | 180 | |
| 54 | 8889 | 91 | 166 | |
| 74 | 6486 | 94 | 171 |
| For ECG | For SCG | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| TP | TN | FP | FN | Accuracy | TPR | TP | TN | FP | FN | Accuracy | TPR | |
| 92 | 5709 | 45 | 8 | 0.991 | 0.92 | 153 | 5602 | 72 | 27 | 0.983 | 0.85 | |
| 86 | 7470 | 49 | 14 | 0.992 | 0.86 | 159 | 7356 | 83 | 21 | 0.986 | 0.88 | |
| 89 | 6624 | 37 | 11 | 0.993 | 0.89 | 148 | 6488 | 93 | 32 | 0.982 | 0.82 | |
| 76 | 8741 | 67 | 15 | 0.991 | 0.83 | 134 | 8642 | 86 | 32 | 0.987 | 0.80 | |
| 81 | 6334 | 58 | 13 | 0.989 | 0.86 | 136 | 6236 | 79 | 35 | 0.982 | 0.79 | |
| Average | 0.991 | 0.87 | Average | 0.984 | 0.83 | |||||||
| SCG Features | Mean | Standard Deviation (SD) |
|---|---|---|
| 0.06 | 0.012 | |
| 0.21 | 0.021 | |
| 0.30 | 0.032 | |
| 0.04 | 0.010 | |
| 0.09 | 0.011 | |
| 0.09 | 0.019 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sahoo, P.K.; Thakkar, H.K.; Lee, M.-Y. A Cardiac Early Warning System with Multi Channel SCG and ECG Monitoring for Mobile Health. Sensors 2017, 17, 711. https://doi.org/10.3390/s17040711
Sahoo PK, Thakkar HK, Lee M-Y. A Cardiac Early Warning System with Multi Channel SCG and ECG Monitoring for Mobile Health. Sensors. 2017; 17(4):711. https://doi.org/10.3390/s17040711
Chicago/Turabian StyleSahoo, Prasan Kumar, Hiren Kumar Thakkar, and Ming-Yih Lee. 2017. "A Cardiac Early Warning System with Multi Channel SCG and ECG Monitoring for Mobile Health" Sensors 17, no. 4: 711. https://doi.org/10.3390/s17040711
APA StyleSahoo, P. K., Thakkar, H. K., & Lee, M. -Y. (2017). A Cardiac Early Warning System with Multi Channel SCG and ECG Monitoring for Mobile Health. Sensors, 17(4), 711. https://doi.org/10.3390/s17040711