The Design and Application of Simplified Insole-Based Prototypes with Plantar Pressure Measurement for Fast Screening of Flat-Foot


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subject
2.2. Equipment
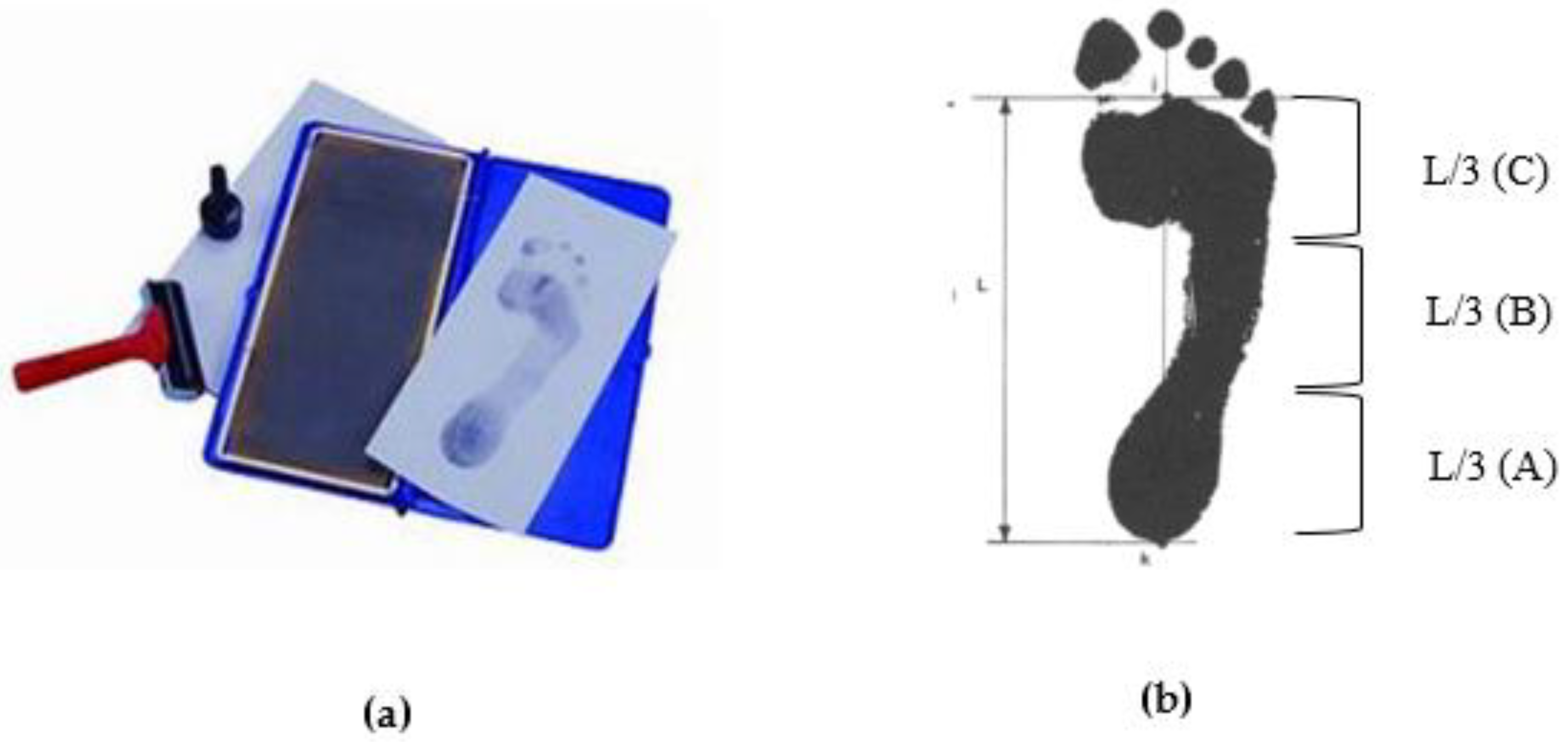
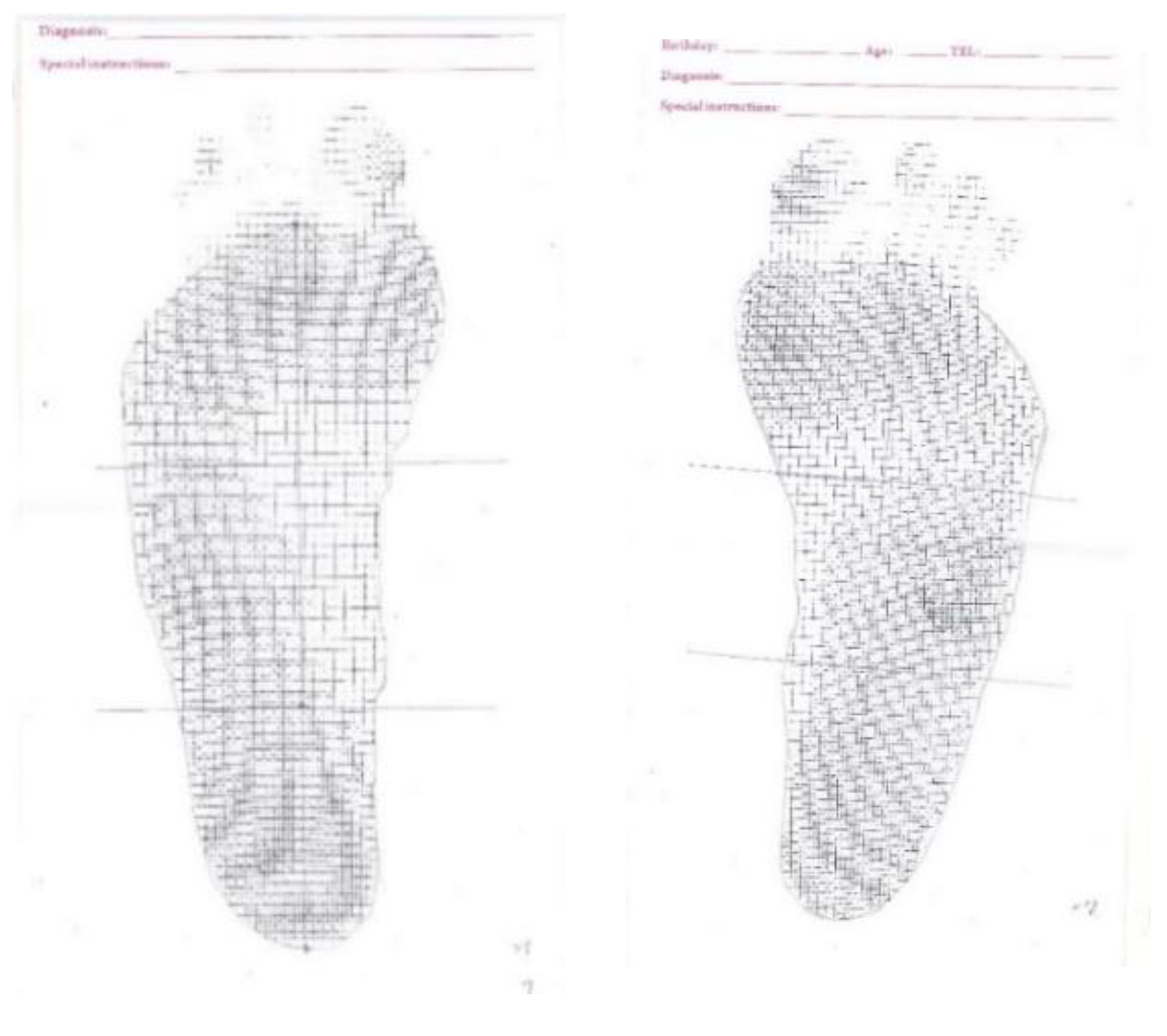
2.2.1. Ink-Type Footprint Printer
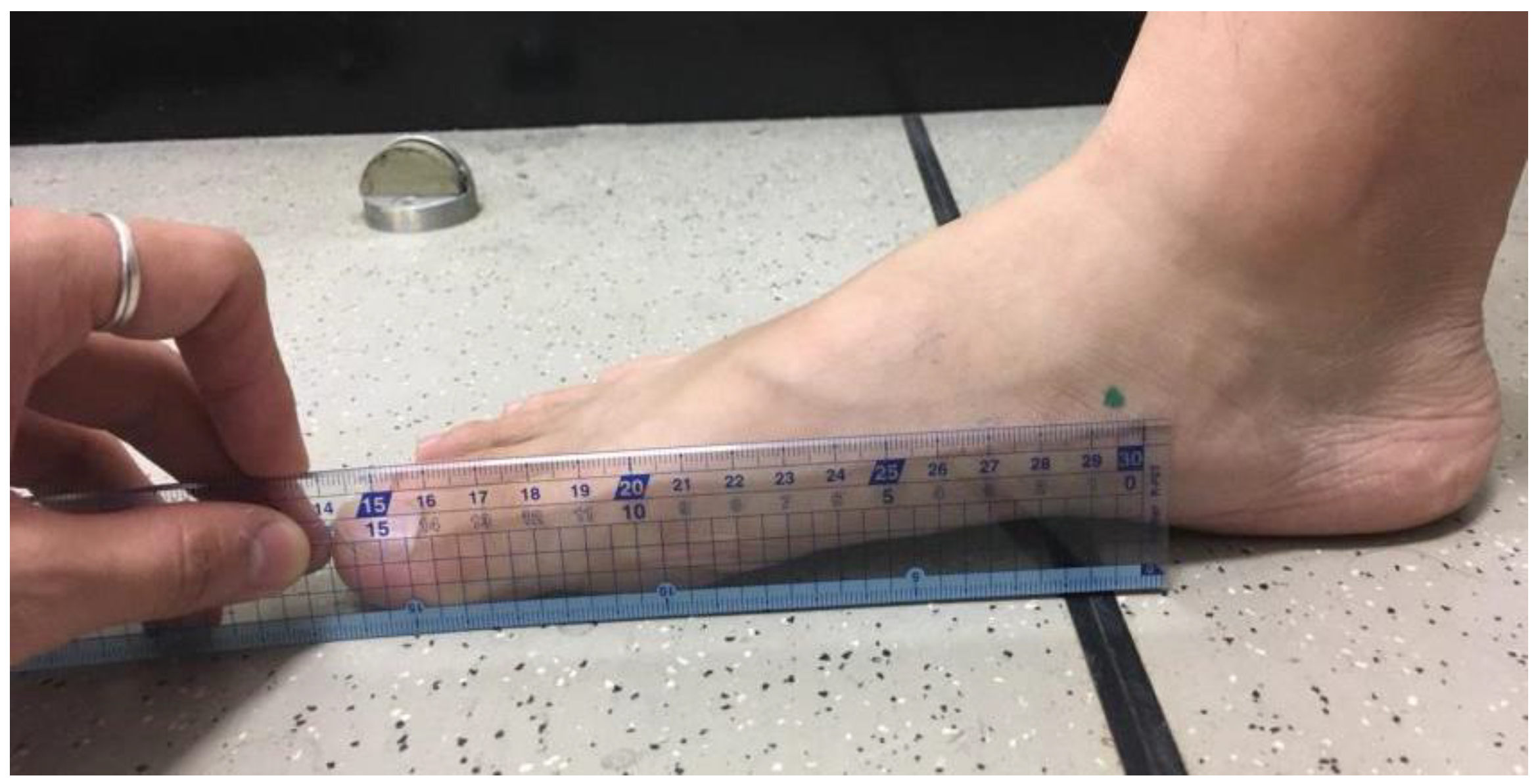
2.2.2. Self-Made Simplified Instrument
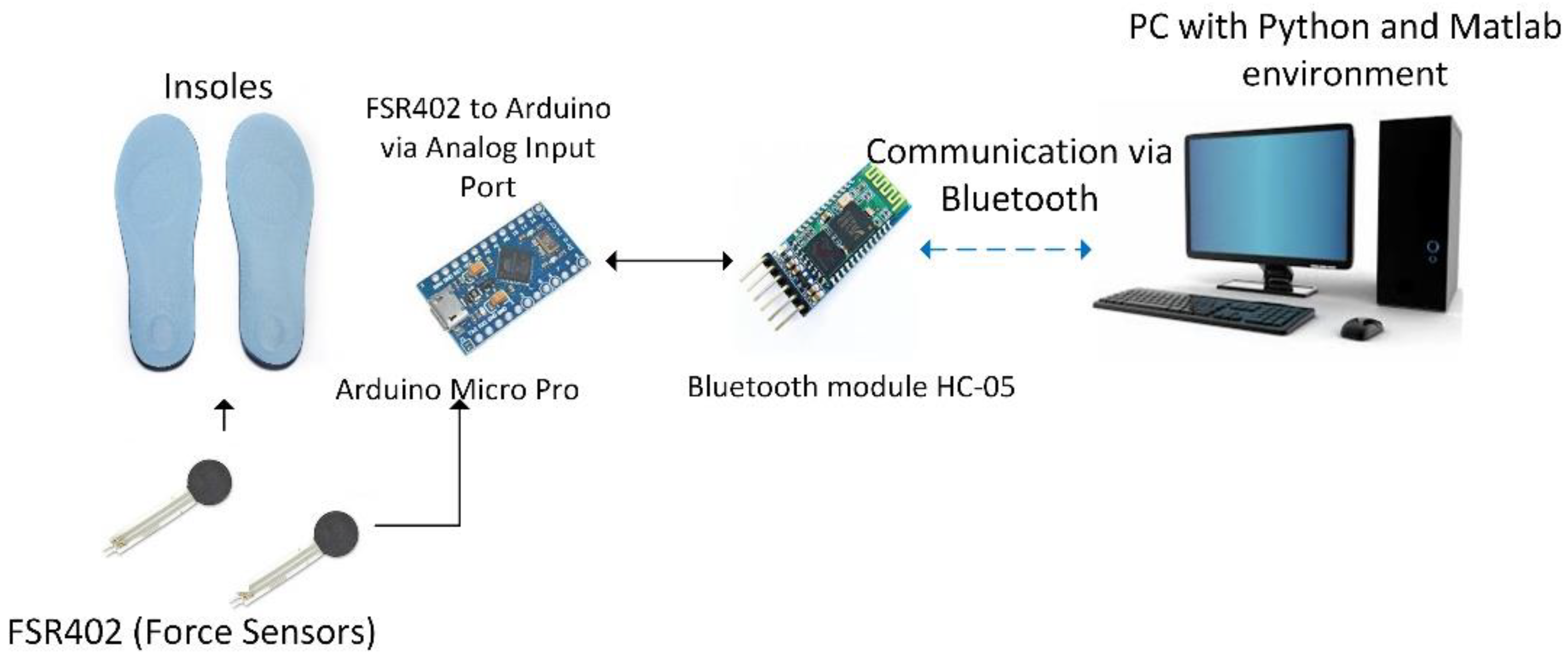
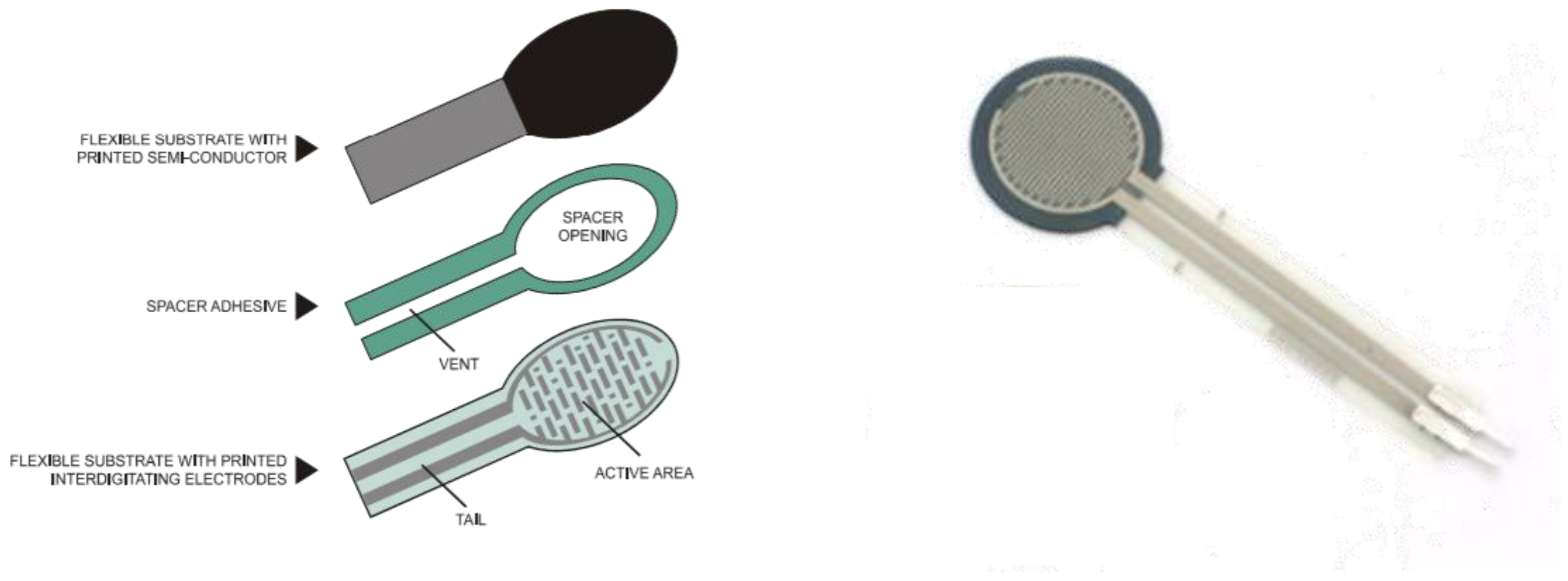
2.2.3. Hardware System Design
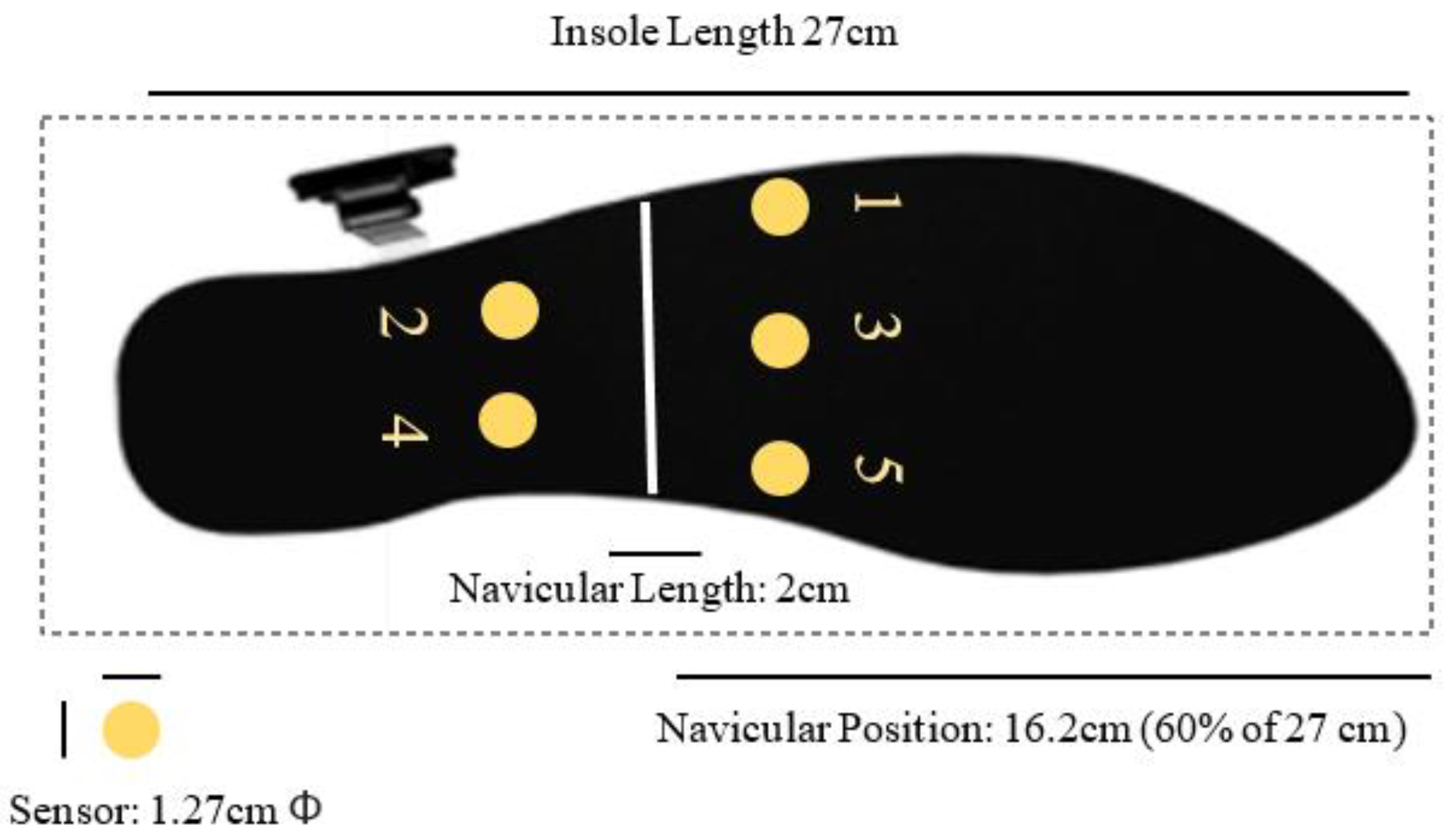
2.2.4. Sensor Placement Design
2.2.5. Experimental Procedure
2.2.6. Static Standing Insole-Type Plantar Pressure Measurement
2.2.7. Dynamic Insole-Type Plantar Pressure Measurement
2.3. Data Analysis
2.4. Statistical Analysis
3. Results
3.1. Static Standing Trials
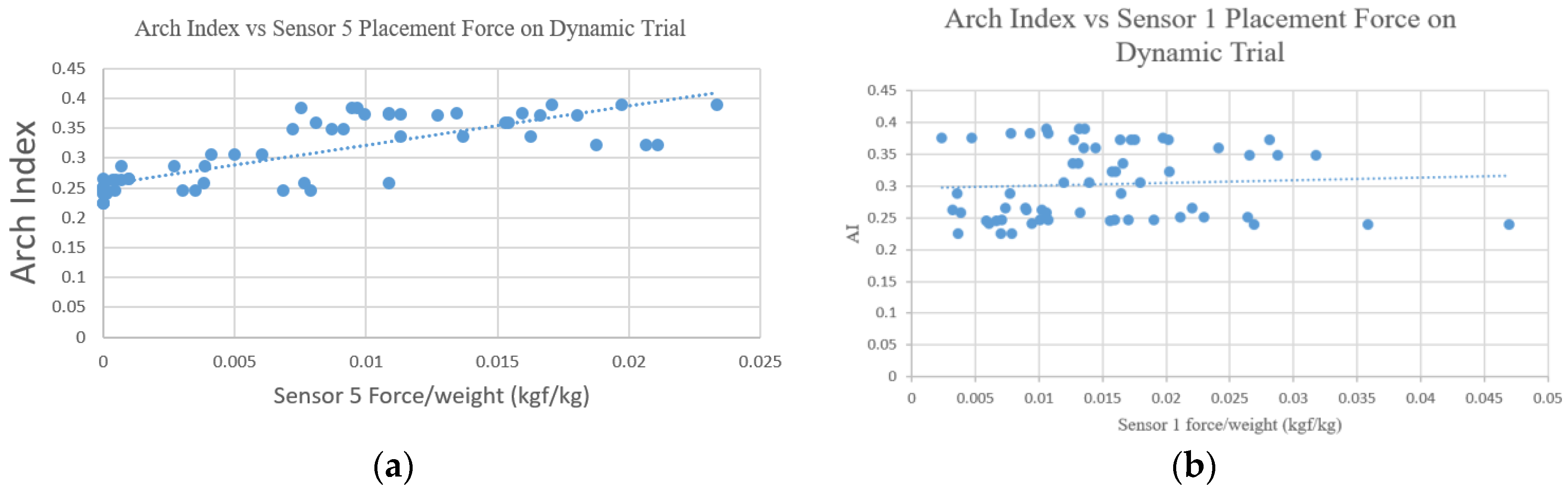
3.2. Dynamic Trials
4. Discussion
4.1. Placements of the Sensors
4.2. Static Trials
4.3. Dynamic Trials
4.4. Research Limitation and Future Works
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Ethical Statements
References
- Jack, E.A. Naviculo-cuneiform fusion in the treatment of flat foot. J. Bone Jt. Surg. Br. Vol. 1953, 35, 75–82. [Google Scholar] [CrossRef]
- Carr, J.B.; Yang, S.; Lather, L.A. Pediatric pes planus: A state-of-the-art review. Pediatrics 2016, 137, e20151230. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.S.; Vanore, J.V.; Thomas, J.L.; Catanzariti, A.R.; Kogler, G.; Kravitz, S.R.; Miller, S.J.; Gassen, S.C. Diagnosis and treatment of adult flatfoot. J. Foot Ankle Surg. 2005, 44, 78–113. [Google Scholar] [CrossRef] [PubMed]
- Aenumulapalli, A.; Kulkarni, M.M.; Gandotra, A.R. Prevalence of flexible flat foot in adults: A cross-sectional study. J. Clin. Diagn. Res. 2017, 11, AC17–AC20. [Google Scholar] [CrossRef] [PubMed]
- Brody, D.M. Techniques in the evaluation and treatment of the injured runner. Orthop. Clin. N. Am. 1982, 13, 541–558. [Google Scholar]
- Cavanagh, P.R.; Rodgers, M.M. The arch index: A useful measure from footprints. J. Biomech. 1987, 20, 547–551. [Google Scholar] [CrossRef]
- Rao, U.B.; Joseph, B. The influence of footwear on the prevalence of flat foot. A survey of 2300 children. Bone Jt. J. 1992, 74, 525–527. [Google Scholar] [CrossRef]
- Riddiford-Harland, D.; Steele, J.; Storlien, L. Does obesity influence foot structure in prepubescent children? Int. J. Obes. 2000, 24, 541. [Google Scholar] [CrossRef]
- Hernandez, A.J.; Kimura, L.K.; Laraya, M.H.F.; Fávaro, E. Calculation of staheli’s plantar arch index and prevalence of flat feet: A study with 100 children aged 5–9 years. Acta Ortopédica Brasileira 2007, 15, 68–71. [Google Scholar] [CrossRef]
- Chen, C.-H.; Huang, M.-H.; Chen, T.-W.; Weng, M.-C.; Lee, C.-L.; Wang, G.-J. The correlation between selected measurements from footprint and radiograph of flatfoot. Arch. Phys. Med. Rehabil. 2006, 87, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Hawes, M.R.; Nachbauer, W.; Sovak, D.; Nigg, B.M. Footprint parameters as a measure of arch height. Foot Ankle 1992, 13, 22–26. [Google Scholar] [CrossRef] [PubMed]
- Vauhnik, R.; Turk, Z.; Pilih, I.A.; Mičetić-Turk, D. Intra-rater reliability of using the navicular drop test for measuring foot pronation. Hrvatski Športskomedicinski Vjesnik 2006, 21, 8–11. [Google Scholar]
- Menz, H.B.; Munteanu, S.E. Validity of 3 clinical techniques for the measurement of static foot posture in older people. J. Orthop. Sports Phys. Ther. 2005, 35, 479–486. [Google Scholar] [CrossRef] [PubMed]
- Queen, R.M.; Mall, N.A.; Hardaker, W.M.; Nunley, J.A. Describing the medial longitudinal arch using footprint indices and a clinical grading system. Foot Ankle Int. 2007, 28, 456–462. [Google Scholar] [CrossRef] [PubMed]
- Cavanagh, P.R.; Rodgers, M.M.; Liboshi, A. Pressure distribution under symptom-free feet during barefoot standing. Foot Ankle 1987, 7, 262–278. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, D.G.; Peters, E.J.; Athanasiou, K.A.; Lavery, L.A. Is there a critical level of plantar foot pressure to identify patients at risk for neuropathic foot ulceration? J. Foot Ankle Surg. 1998, 37, 303–307. [Google Scholar] [CrossRef]
- Lavery, L.A.; Vela, S.A.; Fleischli, J.G.; Armstrong, D.G.; Lavery, D.C. Reducing plantar pressure in the neuropathic foot: A comparison of footwear. Diabetes Care 1997, 20, 1706–1710. [Google Scholar] [CrossRef] [PubMed]
- Saito, M.; Nakajima, K.; Takano, C.; Ohta, Y.; Sugimoto, C.; Ezoe, R.; Sasaki, K.; Hosaka, H.; Ifukube, T.; Ino, S. An in-shoe device to measure plantar pressure during daily human activity. Med. Eng. Phys. 2011, 33, 638–645. [Google Scholar] [CrossRef] [PubMed]
- Shu, L.; Hua, T.; Wang, Y.; Li, Q.; Feng, D.D.; Tao, X. In-shoe plantar pressure measurement and analysis system based on fabric pressure sensing array. IEEE Trans. Inf. Technol. Biomed. 2010, 14, 767–775. [Google Scholar] [PubMed]
- Eguchi, R.; Yorozu, A.; Fukumoto, T.; Takahashi, M. Ground Reaction Force Estimation Using Insole Plantar Pressure Measurement System from Single-Leg Standing. In Proceedings of the 2016 IEEE International Conference on Multisensor Fusion and Integration for Intelligent Systems (MFI), Baden-Baden, Germany, 19–21 September 2016; pp. 109–113. [Google Scholar]
- Howell, A.M.; Kobayashi, T.; Hayes, H.A.; Foreman, K.B.; Bamberg, S.J.M. Kinetic gait analysis using a low-cost insole. IEEE Trans. Biomed. Eng. 2013, 60, 3284–3290. [Google Scholar] [CrossRef] [PubMed]
- Liang, T.-C.; Lin, J.-J.; Guo, L.-Y. Plantar pressure detection with fiber bragg gratings sensing system. Sensors 2016, 16, 1766. [Google Scholar] [CrossRef] [PubMed]
- Navarro, L.A.; García, D.O.; Villavicencio, E.A.; Torres, M.A.; Nakamura, O.K.; Huamaní, R.; Yabar, L.F. Opto-electronic system for detection of flat foot by using estimation techniques: Study and approach of design. In Proceedings of the 2010 Annual International Conference of the Engineering in Medicine and Biology Society (EMBC), Buenos Aires, Argentina, 31 August–4 September 2010; pp. 5768–5771. [Google Scholar]
- Flórez, J.; Velasquez, A. Calibration of force sensing resistors (fsr) for static and dynamic applications. In Proceedings of the 2010 IEEE ANDESCON, Bogota, Colombia, 15–17 September 2010; pp. 1–6. [Google Scholar]
- McCrory, J.; Young, M.; Boulton, A.; Cavanagh, P. Arch index as a predictor of arch height. Foot 1997, 7, 79–81. [Google Scholar] [CrossRef]
- Kanatli, U.; Yetkin, H.; Cila, E. Footprint and radiographic analysis of the feet. J. Pediatr. Orthop. 2001, 21, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Yalcin, N.; Esen, E.; Kanatli, U.; Yetkin, H. Evaluation of the medial longitudinal arch: A comparison between the dynamic plantar pressure measurement system and radiographic analysis. Acta Orthop. Traumatol. Turc. 2010, 44, 241–245. [Google Scholar] [CrossRef] [PubMed]
- Menz, H.B.; Morris, M.E. Clinical determinants of plantar forces and pressures during walking in older people. Gait Posture 2006, 24, 229–236. [Google Scholar] [CrossRef] [PubMed]
- Jonely, H.; Brismée, J.-M.; Sizer, P.S., Jr.; James, C.R. Relationships between clinical measures of static foot posture and plantar pressure during static standing and walking. Clin. Biomech. 2011, 26, 873–879. [Google Scholar] [CrossRef] [PubMed]
- Xiong, S.; Goonetilleke, R.S.; Witana, C.P.; Weerasinghe, T.W.; Au, E.Y.L. Foot arch characterization: A review, a new metric, and a comparison. J. Am. Podiat. Med. Assoc. 2010, 100, 14–24. [Google Scholar] [CrossRef]
- Kernozek, T.W.; Ricard, M.D. Foot placement angle and arch type: Effect on rearfoot motion. Arch. Phys. Med. Rehabil. 1990, 71, 988–991. [Google Scholar] [PubMed]
- Elvira, J.; Vera-Garcia, F.; Meana, M. Subtalar joint kinematic correlations with footprint arch index in race walkers. J. Sports Med. Phys. Fitness 2008, 48, 225. [Google Scholar] [PubMed]
- Shrader, J.A.; Popovich, J.M., Jr.; Gracey, G.C.; Danoff, J.V. Navicular drop measurement in people with rheumatoid arthritis: Interrater and intrarater reliability. Phys. Ther. 2005, 85, 656–664. [Google Scholar] [PubMed]
- Murley, G.S.; Menz, H.B.; Landorf, K.B. A protocol for classifying normal-and flat-arched foot posture for research studies using clinical and radiographic measurements. J. Foot Ankle Res. 2009, 2, 22. [Google Scholar] [CrossRef] [PubMed]
- Wearing, S.C.; Hills, A.P.; Byrne, N.M.; Hennig, E.M.; McDonald, M. The arch index: A measure of flat or fat feet? Foot Ankle Int. 2004, 25, 575–581. [Google Scholar] [CrossRef] [PubMed]
- Aurichio, T.R.; Rebelatto, J.R.; De Castro, A.P. The relationship between the body mass index (bmi) and foot posture in elderly people. Arch. Gerontol. Geriatr. 2011, 52, e89–e92. [Google Scholar] [CrossRef] [PubMed]
- Levinger, P.; Menz, H.B.; Fotoohabadi, M.R.; Feller, J.A.; Bartlett, J.R.; Bergman, N.R. Foot posture in people with medial compartment knee osteoarthritis. J. Foot Ankle Res. 2010, 3, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pohl, M.B.; Hamill, J.; Davis, I.S. Biomechanical and anatomic factors associated with a history of plantar fasciitis in female runners. Clin. J. Sport Med. 2009, 19, 372–376. [Google Scholar] [CrossRef] [PubMed]
- Menz, H.B.; Munteanu, S.E.; Zammit, G.V.; Landorf, K.B. Foot structure and function in older people with radiographic osteoarthritis of the medial midfoot. Osteoarthr. Cartil. 2010, 18, 317–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject Information | Normal Foot (N = 11) | Flatfoot (N = 10) | ||
|---|---|---|---|---|
| Mean | ±Std | Mean | ±Std | |
| Age (year) | 23.4 | 1.0 | 23.1 | 2.2 |
| Height (cm) | 176.6 | 3.0 | 173.1 | 5.6 |
| Weight (kg) | 70.5 | 6.9 | 72.2 | 7.8 |
| BMI (kg/m2) | 22.6 | 2.1 | 24.0 | 2.5 |
| Arch Index | 0.251 | 0.016 | 0.356 | 0.027 |
| Shoe Size (US Size) | 9.6 | 0.4 | 9.5 | 0.43 |
| Ratio of foot length and navicular-to-toe length | 0.63 | 0.01 | 0.64 | 0.01 |
| Parameters | r | p Value | ||
|---|---|---|---|---|
| Mean (kgf/kg) | Standard Deviation | |||
| Sensor 1 | 0.00688 | 0.00424 | 0.406 | 0.001 ** |
| Sensor 2 | 0.01081 | 0.00346 | 0.336 | 0.008 * |
| Sensor 3 | 0.00602 | 0.00397 | 0.678 | 0.000 ** |
| Sensor 4 | 0.01562 | 0.0045 | 0.417 | 0.001 ** |
| Sensor 5 | 0.00339 | 0.00471 | 0.0707 | 0.000 ** |
| 3 Sensors Point (1, 3, 5) | 0.01629 | 0.01138 | 0.680 | 0.000 ** |
| 5 Sensors Point (1–5) | 0.04272 | 0.01613 | 0.668 | 0.000 ** |
| Medial Arch (5 + 4 + 3/2) | 0.02202 | 0.00917 | 0.715 | 0.000 ** |
| Lateral Arch (1 + 2 + 3/2) | 0.02069 | 0.00868 | 0.487 | 0.000 ** |
| Parameters | Normal Foot | Flatfoot | p Value | ||
|---|---|---|---|---|---|
| Mean | Standard Deviation | Mean | Standard Deviation | ||
| Sensor 1 | 0.00462 | 0.00205 | 0.00929 | 0.00456 | 0.009 * |
| Sensor 2 | 0.00931 | 0.00261 | 0.0124 | 0.00347 | 0.029 * |
| Sensor 3 | 0.00342 | 0.00108 | 0.0088 | 0.00397 | 0.003 ** |
| Sensor 4 | 0.01371 | 0.00469 | 0.01765 | 0.00311 | 0.049 * |
| Sensor 5 | 0.00024 | 0.00059 | 0.00676 | 0.00477 | 0.000 ** |
| 3 Sensors Point (1, 3, 5) | 0.00827 | 0.00223 | 0.02485 | 0.01078 | 0.000 ** |
| 5 Sensors Point (1–5) | 0.03129 | 0.00648 | 0.05491 | 0.01401 | 0.001 ** |
| Medial Arch (5 + 4 + 3/2) | 0.01566 | 0.00519 | 0.02881 | 0.00728 | 0.000 ** |
| Lateral Arch (1 + 2 + 3/2) | 0.01563 | 0.00412 | 0.02609 | 0.00886 | 0.006 ** |
| Parameters | r | p Value | ||
|---|---|---|---|---|
| Mean (kgf/kg) | Standard Deviation | |||
| Sensor 1 | 0.03655 | 0.00861 | 0.063 | 0.627 |
| Sensor 2 | 0.03127 | 0.00543 | 0.343 | 0.006 * |
| Sensor 3 | 0.02922 | 0.00692 | 0.541 | 0.000 ** |
| Sensor 4 | 0.04123 | 0.00747 | 0.505 | 0.000 ** |
| Sensor 5 | 0.02017 | 0.00695 | 0.801 | 0.000 ** |
| 3 Sensors Point (1, 3, 5) | 0.056 | 0.01529 | 0.604 | 0.000 ** |
| 5 Sensors Point (1–5) | 0.11451 | 0.02282 | 0.587 | 0.000 ** |
| Medial Arch (5 + 4 + 3/2) | 0.06643 | 0.01319 | 0.784 | 0.000 ** |
| Lateral Arch (1 + 2 + 3/2) | 0.06069 | 0.01374 | 0.319 | 0.011 * |
| Parameters | Normal Foot | Flatfoot | p Value | ||
|---|---|---|---|---|---|
| Mean | Standard Deviation | Mean | Standard Deviation | ||
| Sensor 1 | 0.01351 | 0.00859 | 0.01605 | 0.00555 | 0.105 |
| Sensor 2 | 0.01883 | 0.00374 | 0.02223 | 0.00529 | 0.139 |
| Sensor 3 | 0.01104 | 0.00421 | 0.01798 | 0.00633 | 0.007 * |
| Sensor 4 | 0.02304 | 0.00727 | 0.02906 | 0.00558 | 0.035 * |
| Sensor 5 | 0.00168 | 0.00249 | 0.01291 | 0.00466 | 0.000 ** |
| 3 Sensors Point (1, 3, 5) | 0.02574 | 0.00967 | 0.04532 | 0.01071 | 0.000 ** |
| 5 Sensors Point (1–5) | 0.06191 | 0.01307 | 0.08878 | 0.01926 | 0.067 |
| Medial Arch (5 + 4 + 3/2) | 0.02812 | 0.00758 | 0.04735 | 0.00912 | 0.001 ** |
| Lateral Arch (1 + 2 + 3/2) | 0.03461 | 0.0111 | 0.04401 | 0.00961 | 0.006 * |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, W.-C.; Sugiarto, T.; Chen, J.-W.; Lin, Y.-J. The Design and Application of Simplified Insole-Based Prototypes with Plantar Pressure Measurement for Fast Screening of Flat-Foot. Sensors 2018, 18, 3617. https://doi.org/10.3390/s18113617
Hsu W-C, Sugiarto T, Chen J-W, Lin Y-J. The Design and Application of Simplified Insole-Based Prototypes with Plantar Pressure Measurement for Fast Screening of Flat-Foot. Sensors. 2018; 18(11):3617. https://doi.org/10.3390/s18113617
Chicago/Turabian StyleHsu, Wei-Chun, Tommy Sugiarto, Jun-Wen Chen, and Yi-Jia Lin. 2018. "The Design and Application of Simplified Insole-Based Prototypes with Plantar Pressure Measurement for Fast Screening of Flat-Foot" Sensors 18, no. 11: 3617. https://doi.org/10.3390/s18113617
APA StyleHsu, W. -C., Sugiarto, T., Chen, J. -W., & Lin, Y. -J. (2018). The Design and Application of Simplified Insole-Based Prototypes with Plantar Pressure Measurement for Fast Screening of Flat-Foot. Sensors, 18(11), 3617. https://doi.org/10.3390/s18113617