A Novel Sensorized Heart Valve Prosthesis: Preliminary In Vitro Evaluation



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. IVI Sensor—The Concept
2.2. The Proof-of-Concept Prototype
2.3. In Vitro Tests
2.3.1. In Vitro Test Bench
2.3.2. Tests for Selection of the Optimal IVI Measurement Configuration
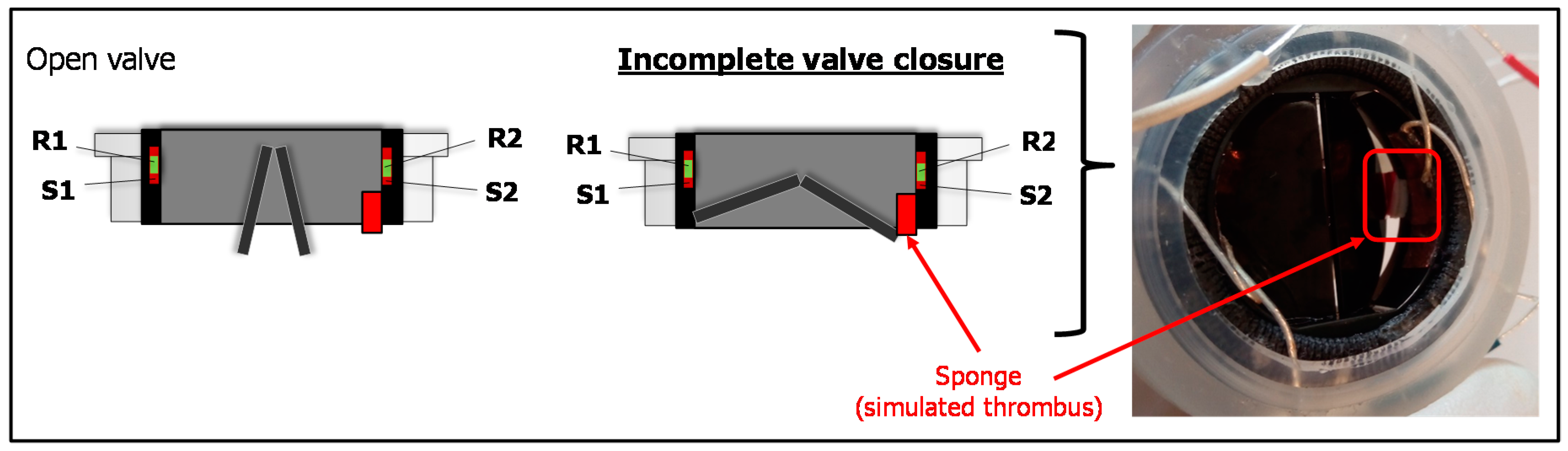
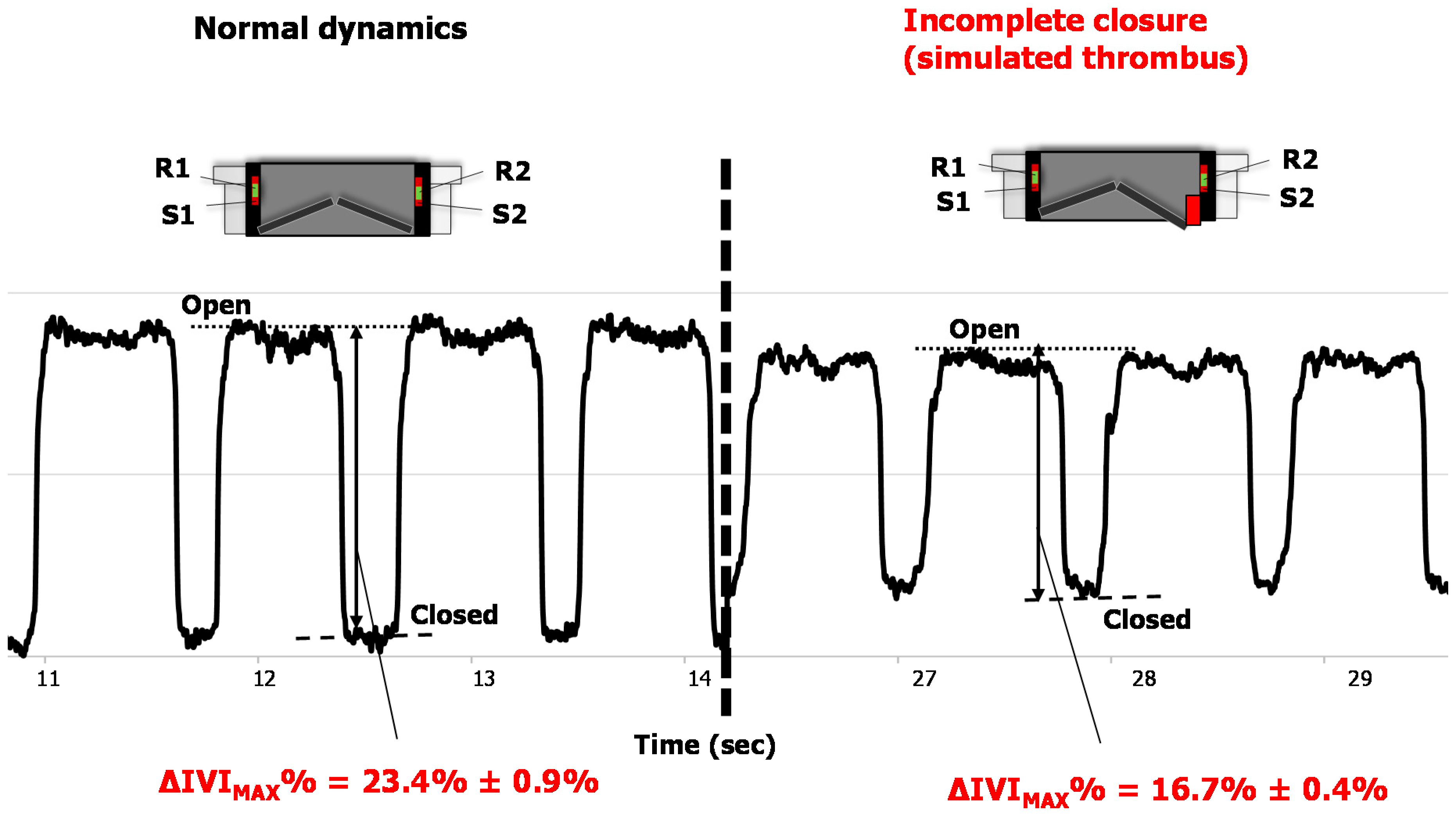
2.3.3. Tests with Altered Leaflet Dynamics
2.4. Data Analysis and Statistics
3. Results
3.1. Results of Tests for Selection of IVI Measurement Configuration
3.2. Results of Tests with Altered Leaflet Dynamics
4. Discussion
Study Limitations and Future Directions
5. Conclusions
6. Patents
- WO2015EP58201 20150415. Heart valve prosthesis with integrated electronic circuit for measuring intravalvular electrical impedance, and system for monitoring functionality of the prosthesis. E. Marcelli (Inventor); Alma Mater Studiorum (Applicant). Filed: 15 April 2015.
- Also published as: EP3131502 (A1); CN106456043 (A); US9987129 (B2)—Issued: 5 June 2018.
- N. 0001423344 Protesi valvolare cardiaca con circuito elettronico integrato per effettuare misure di impedenza elettrica intravalvolare e sistema per monitorare la funzionalità di tale protesi—E. Marcelli (Inventor); Alma Mater Studiorum (Applicant). Filed: 16 April 2014. Issued: 22 July 2016.
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Iung, B.; Vahanian, A. Epidemiology of valvular heart disease in the adult. Nat. Rev. Cardiol. 2011, 8, 162–172. [Google Scholar] [CrossRef] [PubMed]
- Coffey, S.; Cairns, B.J.; Iung, B. The modern epidemiology of heart valve disease. Heart Br. Card. Soc. 2016, 102, 75–85. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, H.; Falk, V.; Bax, J.J.; De Bonis, M.; Hamm, C.; Holm, P.J.; Iung, B.; Lancellotti, P.; Lansac, E.; Rodriguez Munoz, D.; et al. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2017, 38, 2739–2791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, J.C.J.; Davidson, M.J.; Lamy, A.; Eikelboom, J.W. Antithrombotic management of patients with prosthetic heart valves: current evidence and future trends. Lancet 2009, 374, 565–576. [Google Scholar] [CrossRef]
- Pibarot, P.; Dumesnil, J.G. Prosthetic heart valves: Selection of the optimal prosthesis and long-term management. Circulation 2009, 119, 1034–1048. [Google Scholar] [CrossRef] [PubMed]
- Roudaut, R.; Serri, K.; Lafitte, S. Thrombosis of prosthetic heart valves: Diagnosis and therapeutic considerations. Heart 2007, 93, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Puri, R.; Auffret, V.; Rodés-Cabau, J. Bioprosthetic Valve Thrombosis. J. Am. Coll. Cardiol. 2017, 69, 2193–2211. [Google Scholar] [CrossRef] [PubMed]
- Dangas, G.D.; Weitz, J.I.; Giustino, G.; Makkar, R.; Mehran, R. Prosthetic Heart Valve Thrombosis. J. Am. Coll. Cardiol. 2016, 68, 2670–2689. [Google Scholar] [CrossRef] [PubMed]
- Makkar, R.R.; Fontana, G.; Søndergaard, L. Possible Subclinical Leaflet Thrombosis in Bioprosthetic Aortic Valves. N. Engl. J. Med. 2016, 374, 1591–1592. [Google Scholar] [CrossRef] [PubMed]
- Chakravarty, T.; Søndergaard, L.; Friedman, J.; De Backer, O.; Berman, D.; Kofoed, K.F.; Jilaihawi, H.; Shiota, T.; Abramowitz, Y.; Jørgensen, T.H.; et al. Subclinical leaflet thrombosis in surgical and transcatheter bioprosthetic aortic valves: An observational study. Lancet 2017, 389, 2383–2392. [Google Scholar] [CrossRef]
- Egbe, A.C.; Pislaru, S.V.; Pellikka, P.A.; Poterucha, J.T.; Schaff, H.V.; Maleszewski, J.J.; Connolly, H.M. Bioprosthetic Valve Thrombosis Versus Structural Failure: Clinical and Echocardiographic Predictors. J. Am. Coll. Cardiol. 2015, 66, 2285–2294. [Google Scholar] [CrossRef] [PubMed]
- Holmes, D.R.; Mack, M.J. Aortic Valve Bioprostheses: Leaflet Immobility and Valve Thrombosis. Circulation 2017, 135, 1749–1756. [Google Scholar] [CrossRef] [PubMed]
- Pislaru, S.V.; Hussain, I.; Pellikka, P.A.; Maleszewski, J.J.; Hanna, R.D.; Schaff, H.V.; Connolly, H.M. Misconceptions, diagnostic challenges and treatment opportunities in bioprosthetic valve thrombosis: Lessons from a case series. Eur. J. Cardio-Thorac. Surg. Off. J. Eur. Assoc. Cardio-Thorac. Surg. 2015, 47, 725–732. [Google Scholar] [CrossRef] [PubMed]
- Yanagawa, B.; Mazine, A.; Bhatt, D.L.; Clavel, M.A.; Côté, N.; Cheema, A.N.; Philippe, P.; Verma, S. Subclinical bioprosthetic aortic valve thrombosis: Clinical and translational implications. Curr. Opin. Cardiol. 2017, 32, 137–146. [Google Scholar] [CrossRef] [PubMed]
- Rashid, H.N.; Brown, A.J.; McCormick, L.M.; Amiruddin, A.S.; Kim, K.B.; Cameron, J.D.; Nasis, A.; Gooley, R.P. Subclinical Leaflet Thrombosis in Transcatheter Aortic Valve Replacement Detected by Multidetector Computed Tomography—A Review of Current Evidence. Circ. J. Off. J. Jpn. Circ. Soc. 2018, 82, 1735–1742. [Google Scholar] [CrossRef] [PubMed]
- Marwan, M.; Mekkhala, N.; Göller, M.; Röther, J.; Bittner, D.; Schuhbaeck, A.; Hell, M.; Muschiol, G.; Kolwelter, J.; Feyrer, R.; et al. Leaflet thrombosis following transcatheter aortic valve implantation. J. Cardiovasc. Comput. Tomogr. 2018, 12, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Pache, G.; Schoechlin, S.; Blanke, P.; Dorfs, S.; Jander, N.; Arepalli, C.D.; Gick, M.; Buettner, H.-J.; Leipsic, J.; Langer, M.; et al. Early hypo-attenuated leaflet thickening in balloon-expandable transcatheter aortic heart valves. Eur. Heart J. 2016, 37, 2263–2271. [Google Scholar] [CrossRef] [PubMed]
- Habets, J.; Budde, R.P.; Symersky, P.; Van Den Brink, R.B.; Bas, A.; Mali, W.P.; van Herwerden, L.A.; Chamuleau, S.A. Diagnostic evaluation of left-sided prosthetic heart valve dysfunction. Nat. Rev. Cardiol. 2011, 8, 466–478. [Google Scholar] [CrossRef] [PubMed]
- Hansson, N.C.; Grove, E.L.; Andersen, H.R.; Leipsic, J.; Mathiassen, O.N.; Jensen, J.M.; Jensen, K.T.; Blanke, P.; Leetmaa, T.; Tang, M.; et al. Transcatheter Aortic Valve Thrombosis: Incidence, Predisposing Factors, and Clinical Implications. J. Am. Coll. Cardiol. 2016, 68, 2059–2069. [Google Scholar] [CrossRef] [PubMed]
- Marcelli, E. Protesi Valvolare Cardiaca con Circuito Elettronico Integrato per Effettuare Misure di Impedenza Elettrica Intravalvolare e Sistema per Monitorare la Funzionalità di tale Protesi. IT Patent IT2014BO00217, 22 July 2016. [Google Scholar]
- Marcelli, E. Heart Valve Prosthesis with Integrated Electronic Circuit for Measuring Intravalvular Electrical Impedance, and System for Monitoring Functionality of the Prosthesis. WO Patent WO2015158789 (A1), 22 October 2015. CN Patent CN106456043 (A), 22 February 2017; U.S. Patent US9987129 (B2), 5 June 2018. [Google Scholar]
- Marcelli, E.; Cercenelli, L. Intravalvular impedance sensor for next-generation smart prosthetic heart valves. Int. J. Artif. Organ. 2015, 38, 399. [Google Scholar]
- Mond, H.; Strathmore, N.; Kertes, P.; Hunt, D.; Baker, G. Rate responsive pacing using a minute ventilation sensor. Pacing Clin. Electrophysiol. PACE 1988, 11, 1866–1874. [Google Scholar] [CrossRef] [PubMed]
- Bonnet, J.L.; Ritter, P.; Pioger, G. Measurement of minute ventilation with different DDDR pacemaker electrode configurations. Investigators of a Multicenter Study Evaluating the Chorus RM and Opus RM Pacemakers. Pacing Clin. Electrophysiol. PACE 1998, 21, 4–10. [Google Scholar] [CrossRef] [PubMed]
- Rivero, G.; García-Páez, J.; Alvarez-Ayuso, L. Magnetic Sensor for Early Detection of Heart Valve Bioprostheses Failure. Sens. Lett. 2007, 5, 263–266. [Google Scholar] [CrossRef] [Green Version]
- Lanning, C.; Shandas, R. Development and validation of implantable sensors for monitoring function of prosthetic heart valves: In vitro studies. Med. Biol. Eng. Comput. 2003, 41, 416–424. [Google Scholar] [CrossRef] [PubMed]
- Martinsen, O.G.; Grimnes, S. Bioimpedance and Bioelectricity Basics, 3rd ed.; Elsevier: Amsterdam, The Netherlands, 2011. [Google Scholar]
- Marcelli, E.; Cercenelli, L. Cardiorespiratory Mechanical Simulator for In Vitro Testing of Impedance Minute Ventilation Sensors in Cardiac Pacemakers. ASAIO J. Am. Soc. Artif. Int. Organs 1992, 2016, 62, 150–156. [Google Scholar]
- Corazza, I.; Casadei, L.; Bonafè, E.; Cercenelli, L.; Marcelli, E.; Zannoli, E.R. How to transform a fixed stroke alternating syringe ventricle into an adjustable elastance ventricle. Rev. Sci. Instrum. 2018, 89, 074301. [Google Scholar] [CrossRef] [PubMed]







© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marcelli, E.; Bortolani, B.; Corazza, I.; Cercenelli, L. A Novel Sensorized Heart Valve Prosthesis: Preliminary In Vitro Evaluation. Sensors 2018, 18, 3905. https://doi.org/10.3390/s18113905
Marcelli E, Bortolani B, Corazza I, Cercenelli L. A Novel Sensorized Heart Valve Prosthesis: Preliminary In Vitro Evaluation. Sensors. 2018; 18(11):3905. https://doi.org/10.3390/s18113905
Chicago/Turabian StyleMarcelli, Emanuela, Barbara Bortolani, Ivan Corazza, and Laura Cercenelli. 2018. "A Novel Sensorized Heart Valve Prosthesis: Preliminary In Vitro Evaluation" Sensors 18, no. 11: 3905. https://doi.org/10.3390/s18113905
APA StyleMarcelli, E., Bortolani, B., Corazza, I., & Cercenelli, L. (2018). A Novel Sensorized Heart Valve Prosthesis: Preliminary In Vitro Evaluation. Sensors, 18(11), 3905. https://doi.org/10.3390/s18113905