1. Introduction
Ultrasound systems are widely used in non-destructive testing, medical imaging, and therapeutic ultrasound applications [
1,
2,
3]. Recently, the therapeutic ultrasound has been developed based on the advanced ultrasonic transducer and semiconductor technology [
4]. The therapeutic ultrasound can be divided into two major categories: low-level (<3 W/cm
2) and high-level (≥3 W/cm
2) therapeutic ultrasounds [
5]. The high-level therapeutic ultrasound, which is also called high-intensity focused ultrasound (HIFU), is used to treat solid cancer tissues (>1 cm
2), considering all safety regulations [
6]. In this type of therapeutic ultrasound, acoustic waves that are produced due to mechanical effects and acoustic cavitation are focused into the target, causing the thermal evaporation of the target, and thus destroying the tumors [
7]. Compared to the high-level therapeutic ultrasound, the low-level therapeutic ultrasound causes mechanical effects that can be easily applied to produce functional changes in tissues or cells without much consideration of safety regulations [
5]. Briefly, ultrasonic stimulus by the low-level intensity initiated the process of cavitation that causes cell damage [
5]. The process of cavitation can directly cause cell lysis or the disruption of cell attachment for cell proliferation. Most cancer cells have a more rigid membrane compared to normal cells that is more sensitive to ultrasonic stimulus. In addition, the cavitation often forms free-radicals able to disrupt cellular membranes. Therefore, it can be used to suppress cancer cell proliferation, which is one of the functional changes, and thus improve the anticancer chemicals [
8]. In particular, the low-level therapeutic ultrasound typically works in nonlinear acoustic ranges, which cannot effectively predict various behavior models in tissue or cell levels [
9]. Additionally, a certain power or voltage level triggered ultrasonic transducers in the low-level therapeutic ultrasound have relatively limited ranges as compared to the ones in the high-level therapeutic ultrasound. This restricts the application of effective solutions even though the low-level ultrasound can be easily regulated [
5]. Therefore, the design of an ultrasound system for low-level therapeutic ultrasounds to improve the therapeutic effects is an important issue to be considered.
Ultrasound systems are typically composed of ultrasonic transmitters, transducers, and receivers [
10,
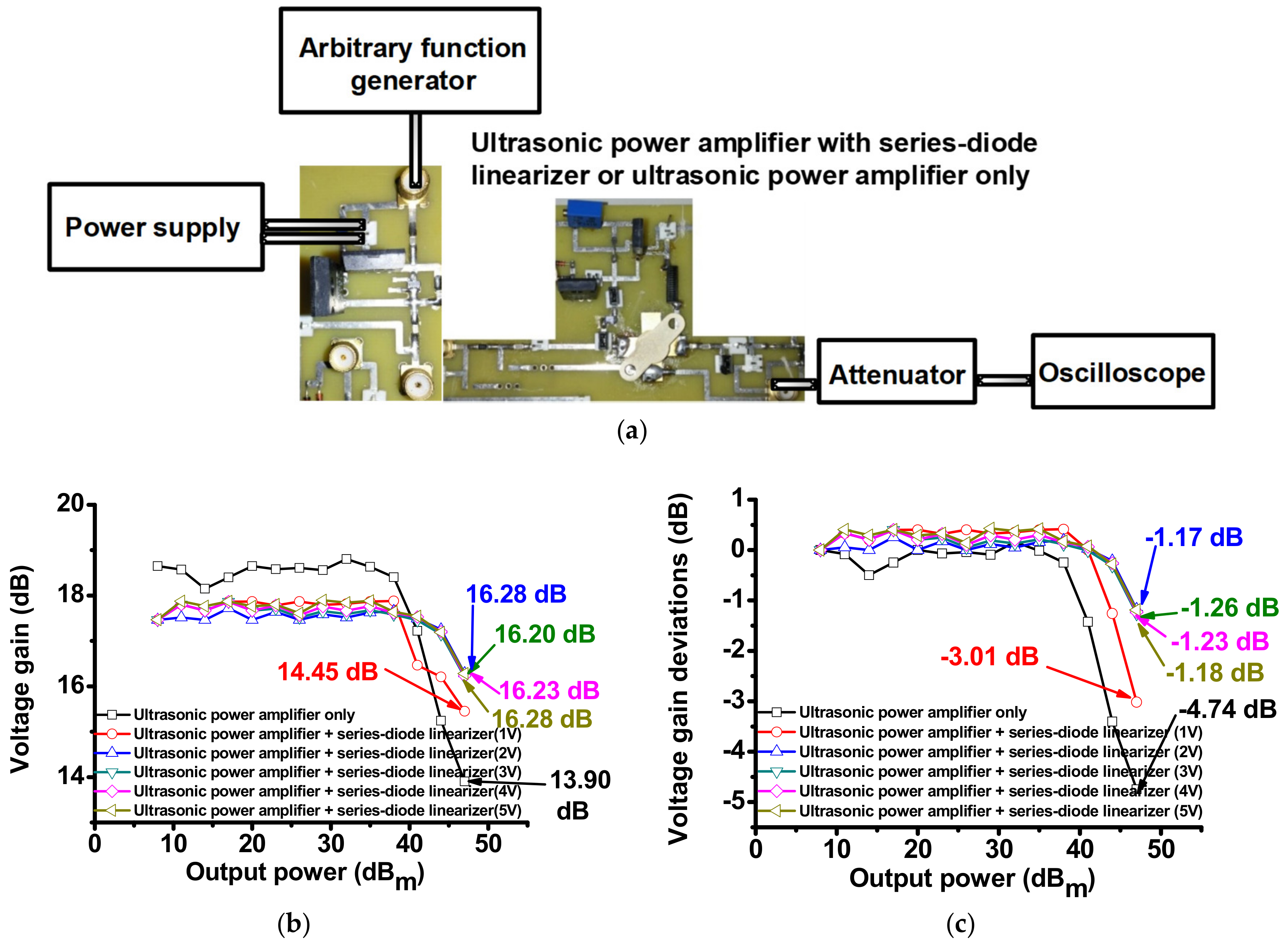
11]. The ultrasonic power amplifiers are the last stage ultrasonic transmitter components and are one of the most critical electronic components, which directly transfer the electrical signals or power the ultrasonic transducers [
2,
12]. Parameters such as harmonic distortions, voltage gains, and bandwidths affect the performance of ultrasonic transducers in ultrasonic transmitters [
4,
10]. Recently, linearizer schemes have been introduced in the ultrasound systems to improve the image quality of the received echo signals by minimizing the harmonic distortions of triggering transmit signals of the ultrasonic power amplifiers [
13,
14]. The previous approach reduces the harmonic distortions of the echo signals for ultrasonic imaging applications. However, our proposed approach could rather increase the transmitted power gains for therapeutic applications. Therefore, we propose a series-diode linearizer scheme developed to serve therapeutic purposes so that it can help an ultrasonic power amplifier effectively transfer the signals at a certain frequency. The electrical impedances of the series-diode linearizer, controlled by external DC voltage, can change the electrical impedances of an ultrasonic power amplifier, thus matching the electrical impedances of an ultrasonic transducer with more freedom. Consequently, ultrasonic power amplifiers can produce high-voltage signals to drive higher power to the ultrasonic transducers, thus effectively transferring the higher ultrasonic waves into the target.
An electrical impedance matching circuit, which is placed between ultrasonic power amplifiers and ultrasonic transducers, can be used to improve the performance parameters, such as voltage gains and bandwidths, of ultrasonic transducers [
4]. An impedance transformer has been used to obtain electrical matching to improve the voltage gains or bandwidths of an air-coupled type ultrasonic transducer that has a high value of the electrical impedances [
15]. A low-pass filter has also been used to obtain electrical matching with an ultrasonic transducer to improve the bandwidths [
16]. These techniques involve the use of electrical components that are relatively high-voltage tolerant and might affect the center frequency of ultrasonic transducers owing to the high values of the inductances. These techniques also might affect the ring down of the transmit ultrasonic pulses for ultrasonic transducers [
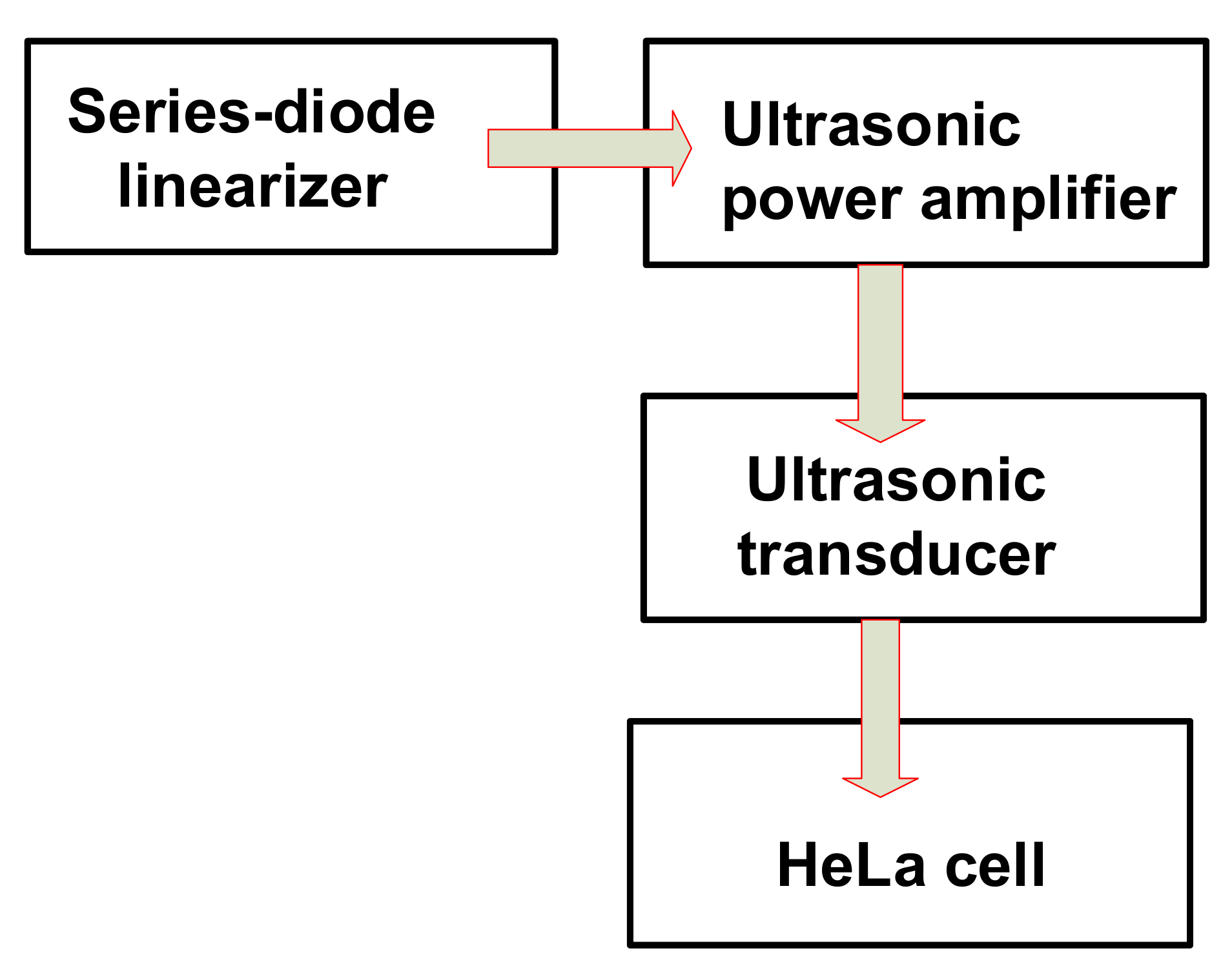
17]. Since the proposed series-diode linearizer is placed in the front of the ultrasonic power amplifier, as shown in
Figure 1, it does not require high-voltage tolerant components and does not critically affect the center frequency of the ultrasonic transducers. Additionally, an external DC voltage in the proposed series-diode linearizer can change the electrical impedances of the ultrasonic power amplifiers with more freedom, thus being matched with the electrical impedances of the ultrasonic transducer. Therefore, higher transmitted voltages from the ultrasonic transducers could be transferred into the desired target.
2. Materials and Methods
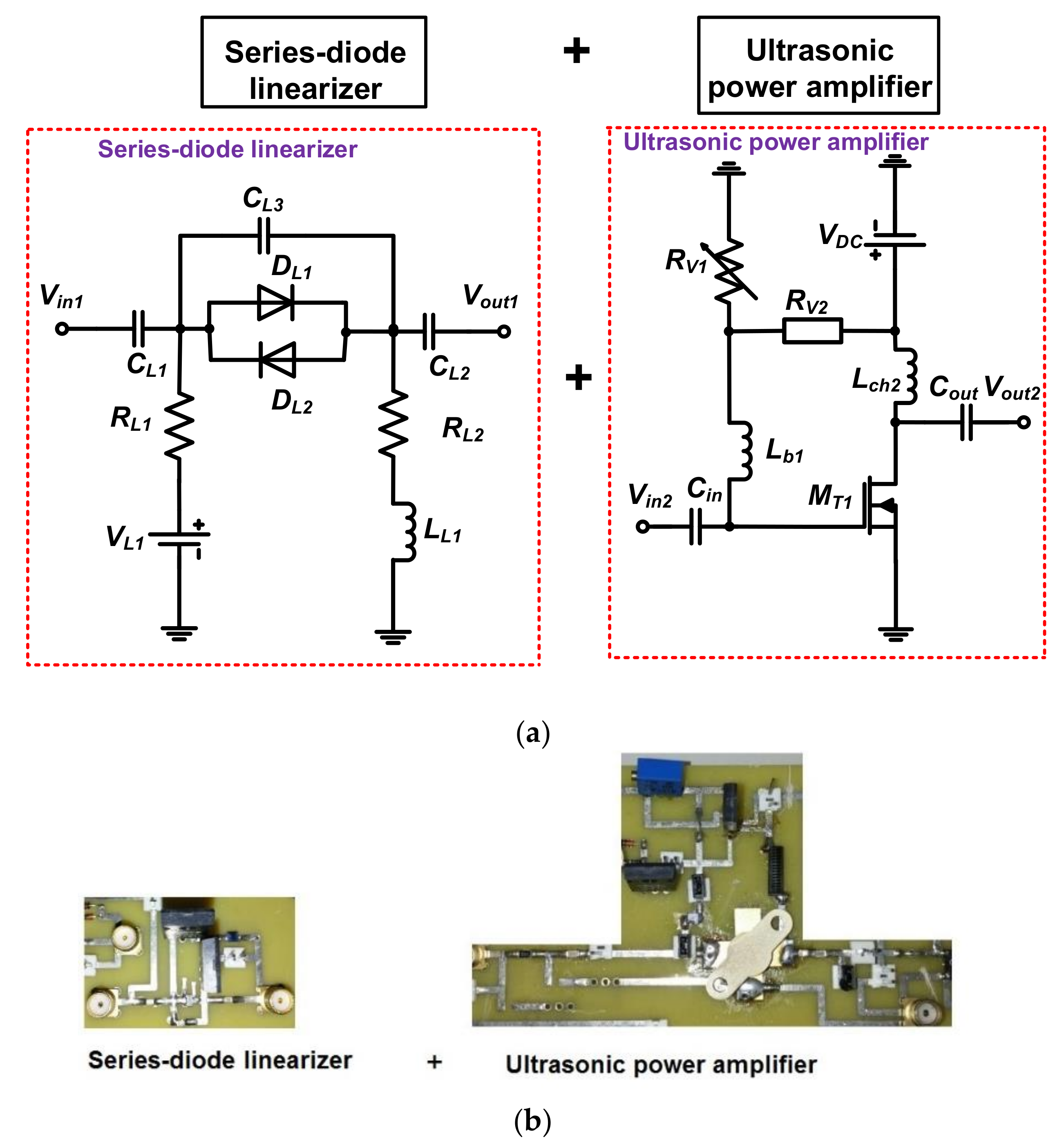
Figure 2a shows the schematic diagrams of the DC voltage driven series-diode linearizer and ultrasonic power amplifier. The ultrasonic power amplifier is a typical power amplifier [
18]. In the series-diode linearizer circuit, single cross-coupled diodes (
D1 and
D2) were used to transmit bipolar, multicycle pulse waveforms into the ultrasonic power amplifier. The cross-coupled diode impedances can be changed depending on the applied DC bias voltages. Three capacitors (
CL1,
CL2, and
CL3) and two resistors (
RL1 and
RL2) were used to minimize the pulse fluctuation at the input port (
Vin1). An additional inductor (
LL1) was used to compensate the capacitances (
CL1,
CL2, and
CL3).
In the ultrasonic power amplifier, two input and output coupling capacitors (
Cin and
Cout) were used because high-voltage DC can generate long discharged pulses when receiving the echo signals from the ultrasonic transducers. The choke inductor (
Lch2) was used to reduce DC voltage variances. The variable and fixed resistors (
Rv1 and
Rv2) were used to provide gate bias voltage to the primary transistor (
MT1) from the DC power supply (
VDC).
Figure 2b shows the implemented series-diode linearizer and ultrasonic power amplifier, which were connected through a short SMA coaxial cable of 20 cm in length to minimize the signal distortions between them. A heat sink is attached at the bottom of the transistor in the printed circuit board to dissipate heat when operating the high-voltage pulses for therapeutic applications.
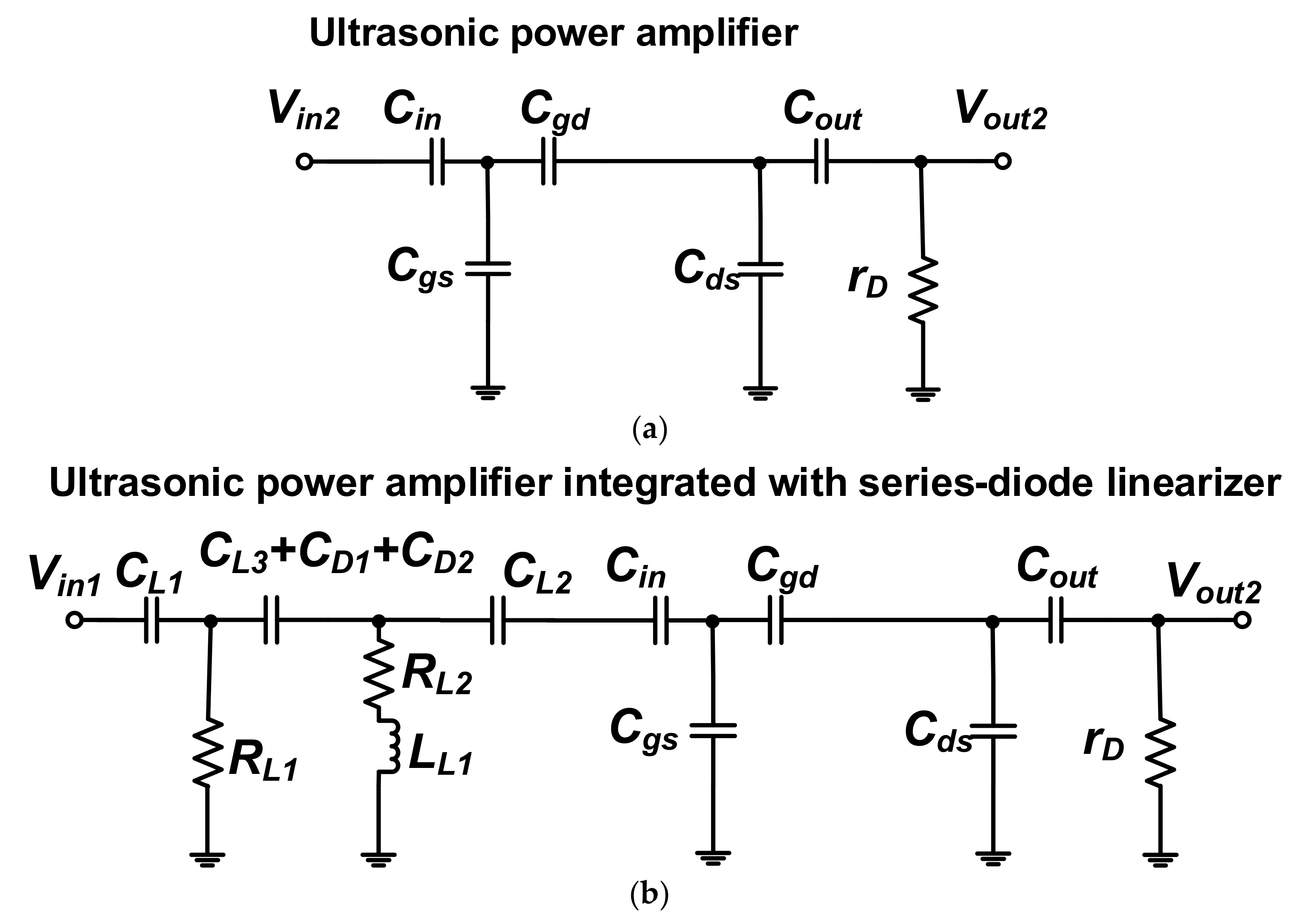
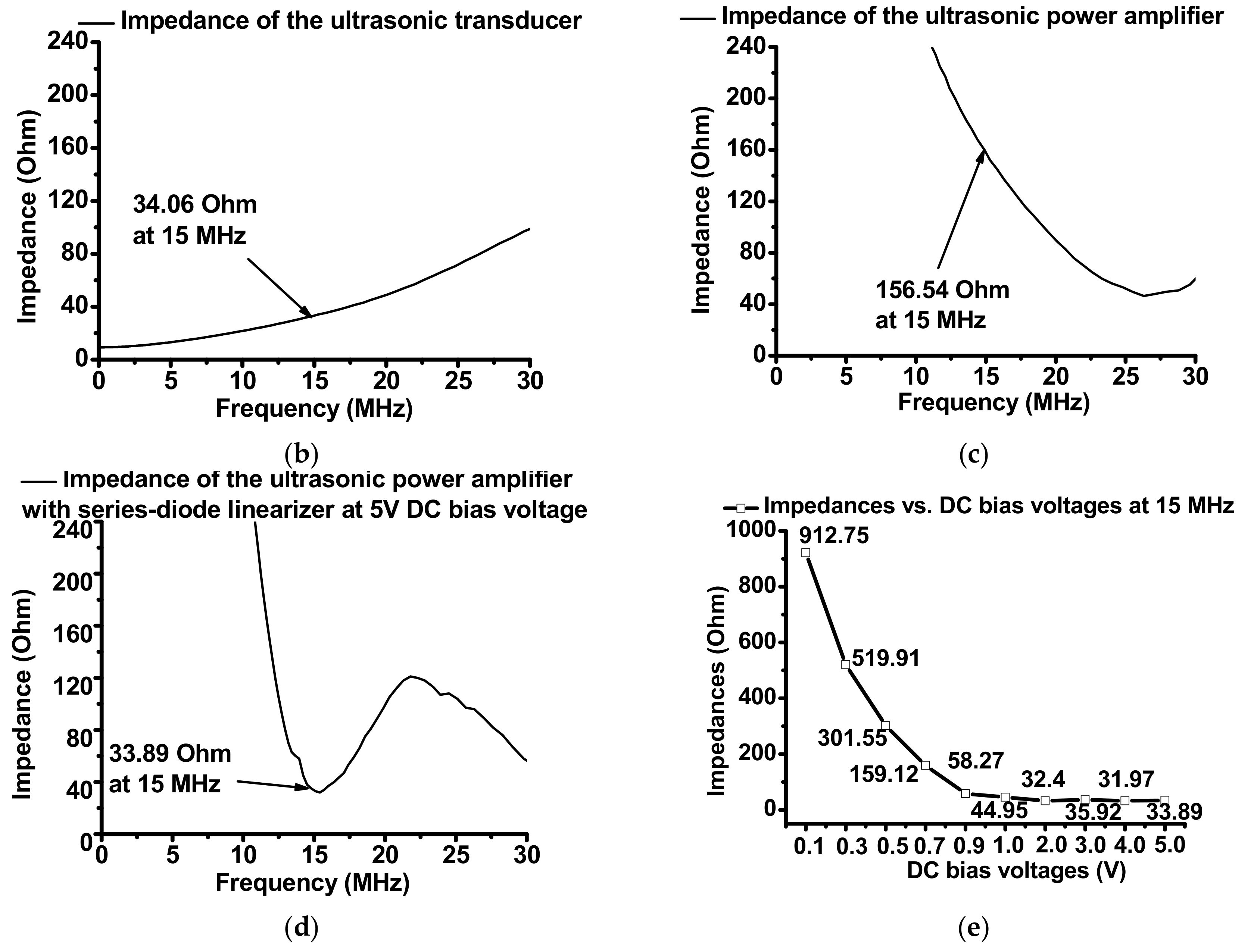
Figure 3 shows the equivalent circuit models of the isolated ultrasonic power amplifier and the ultrasonic power amplifier integrated with the series-diode linearizer to show electrical impedance variances after consolidating the series-diode linearizer circuit.
The electrical impedances of the ultrasonic power amplifier (
Ztran) and the ultrasonic power amplifier integrated with the series-diode linearizer (
Ztran+lin) were expressed in Equations (1) and (2).
where
rD,
Cgs,
Cgd, and
Cds are parasitic drain resistance, gate-source, gate-drain, and drain-source capacitances, respectively, of the primary transistor (
MT1),
C1 is the combined capacitance of the diode parasitic capacitances (C
D1 and C
D2) with capacitor (
CL3), and
fc is the operating frequency of the ultrasonic power amplifier.
As already mentioned, an inductor (LL1) and two resistors (RL1 and RL2) were used to compensate the capacitances of the cross-coupled diodes in the series-diode linearizer, and parasitic resistances and capacitances of the ultrasonic power amplifier at a certain frequency. Therefore, electrical impedances of the ultrasonic power amplifier integrated with the series-diode linearizer can be changed further as compared to those of the isolated ultrasonic power amplifier. According to Equation (2), the electrical impedances could be adjustable because the electrical impedances of the ultrasonic power amplifier integrated with series-diode linearizer (Ztran+lin) could be varied depending on the fc and C1 if the fixed resistors (RL1 and RL2), capacitors (CL1, CL2, and CL3), and inductor (LL1) in the series-diode linearizer were selected. At the fixed operating frequency (fc), the electrical impedances are dependent on the diode capacitance (C1) due to fixed resistances, capacitances, and inductance. Therefore, we can confirm that additional DC voltage (VL1) in the series-diode linearizer could change the electrical impedances of the ultrasonic power amplifier. Next, the measured electrical impedances are compared with the ultrasonic power amplifier with and without series-diode linearizer.
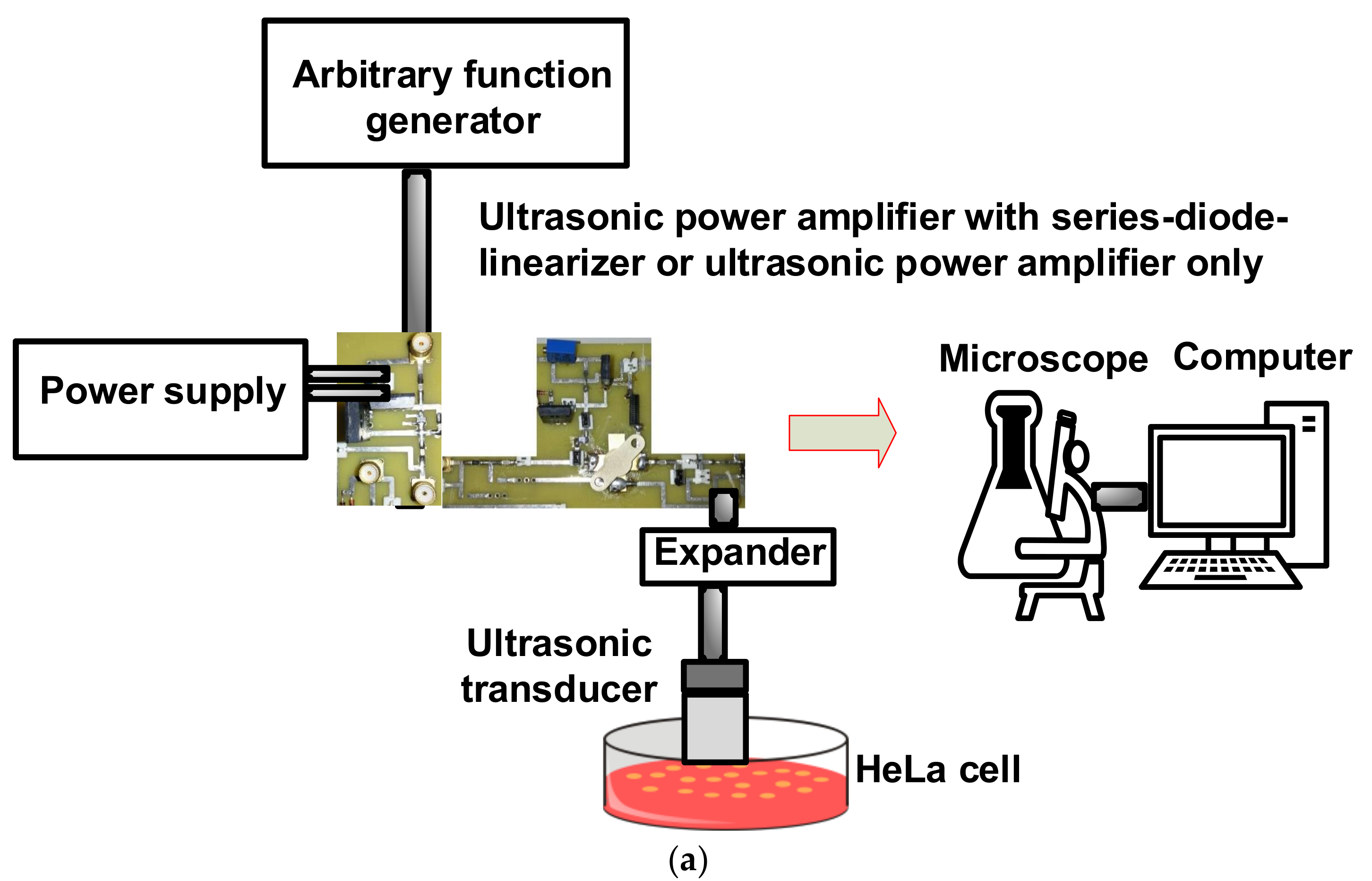
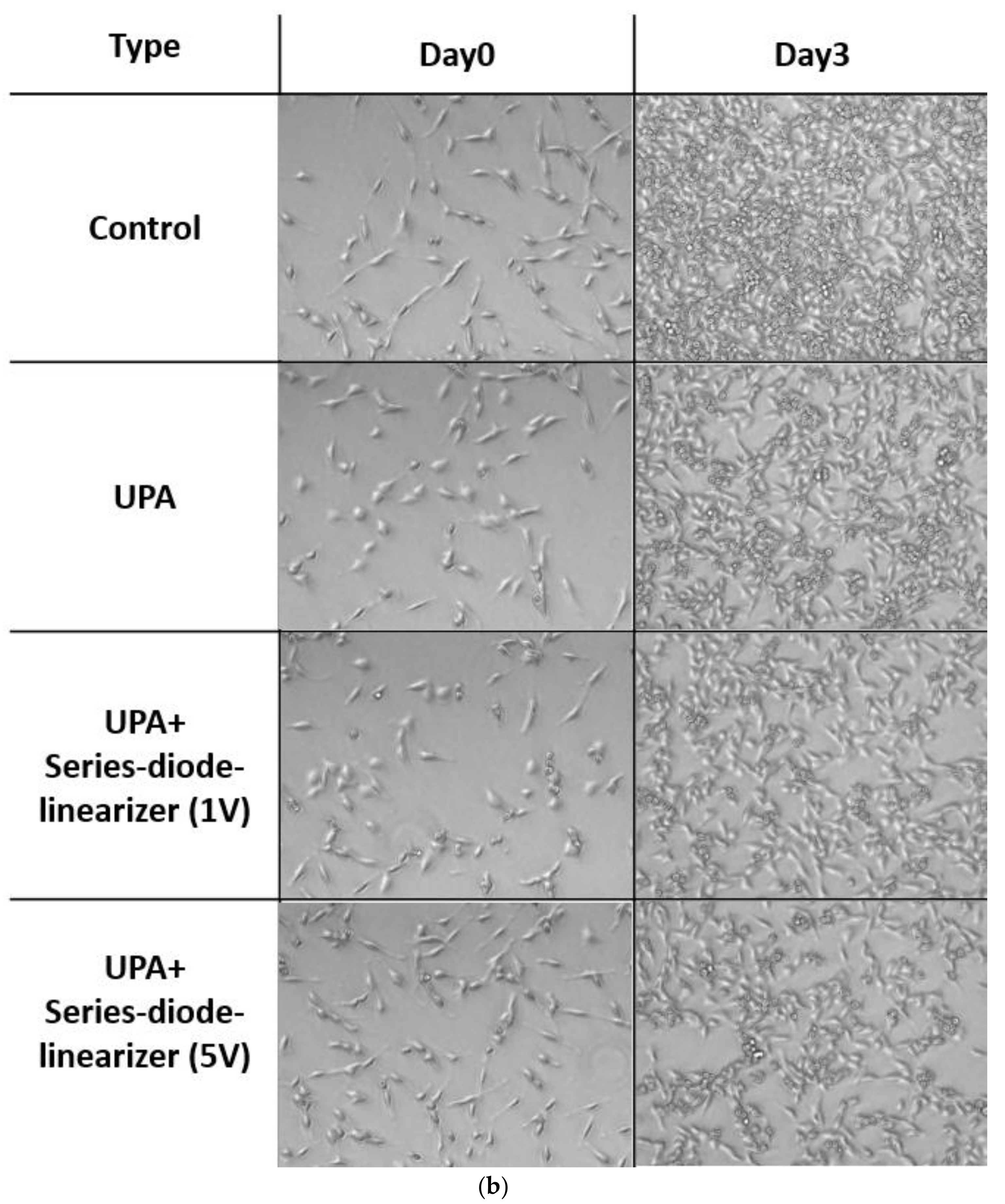
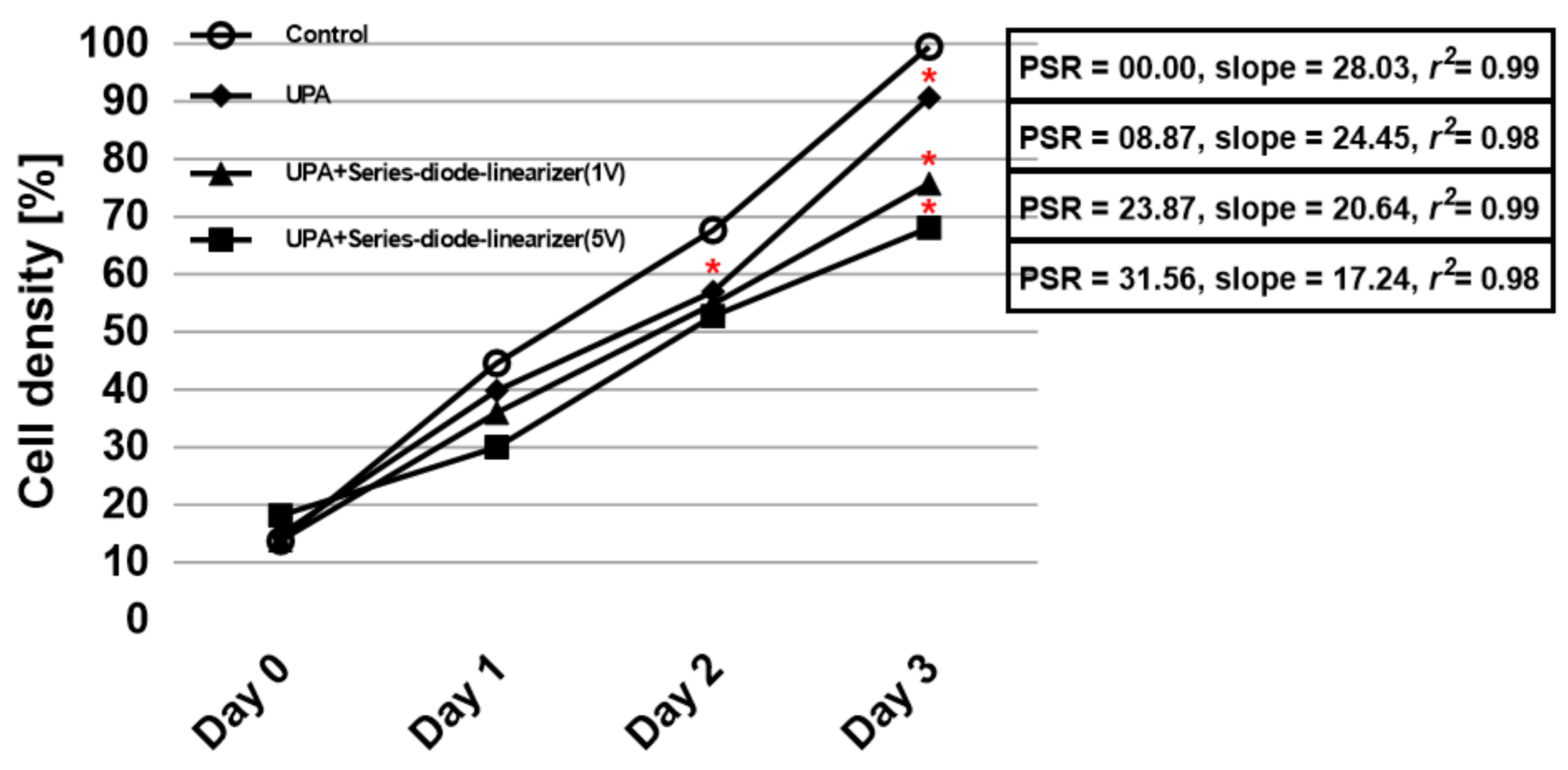
To study the therapeutic effects of the proposed ultrasonic power amplifier with and without the series-diode linearizer, the cell densities and proliferation suppressing ratios (PSRs) were measured on the human cervical cancer cell (HeLa cells, Korean Cell Line Bank) in vitro. HeLa cells were maintained in a high-glucose Dulbecco’s Modified Eagle Medium containing 10% Fetal Bovine Serum with 1% penicillin streptomycin and incubated at 37 °C in a humidified benchtop incubator with 5% CO
2. The prepared cells were trypsinized when the growing cells reached confluence at 70% and then washed three times with phosphate-buffered saline to isolate them in the media. Next, they were resuspended to prepare an approximate concentration of
cells/mL. When the cell confluence reached 40%, the ultrasonic stimulus was induced and consequently counted as Day 0. To avoid thermal damages, the ambient temperature was adjusted to 26 °C during the preparation and experimental procedures. A probe container printed using a commercial 3D printer (Cubicon 3DP-310F, Cubicon Inc., Gyeonggi-do, Korea), was designed to hold the ultrasound transducer. It stimulated the same previous spot on the prepared culture dish. The ultrasonic transducer was placed in the surface of the growth media in the cell culture dish, and its position was retained until Day 3. All prepared samples were divided into four groups: control group (no ultrasonic induction,
n = 6), ultrasonic power amplifier group (ultrasonic induction with ultrasonic power amplifier,
n = 6), ultrasonic power amplifier integrated with series-diode linearizer 1 V (when 1 V DC bias voltage is applied,
n = 6), and ultrasonic power amplifier integrated with series-diode linearizer 5 V (when 5 V DC bias voltage is applied,
n = 6). The ultrasonic stimulus was induced daily for about 30 min. To quantify cell densities and PSRs, the microscopic images of the ultrasound signal-focused area in the cell culture dish were taken instantly after ultrasound signal induction by an inverted fluorescent microscope (IX73 with DP80, Olympus Corp., Tokyo, Japan). Various image processing procedures and statistical analyses using ANOVA with Scheffe’s post-hoc test were performed using the MATLAB software (MathWorks, Natick, MA, USA) to identify the quantitative characteristics of each group [
19]. The cell density was determined by dividing the pixel number of the cell grown area by the acquired microscopic pixel number. The PSR was calculated by dividing the variance of cell density of the experimental group and the control group by the cell density of the control group on Day 3. A
p value of less than 0.05 was considered statistically significant as compared to the control group.














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}