Non-Invasive Electromagnetic Skin Patch Sensor to Measure Intracranial Fluid–Volume Shifts

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Jessica Aldrich 1
1. Introduction
State of the Art in Intracranial Pressure Measurement
2. Materials and Methods
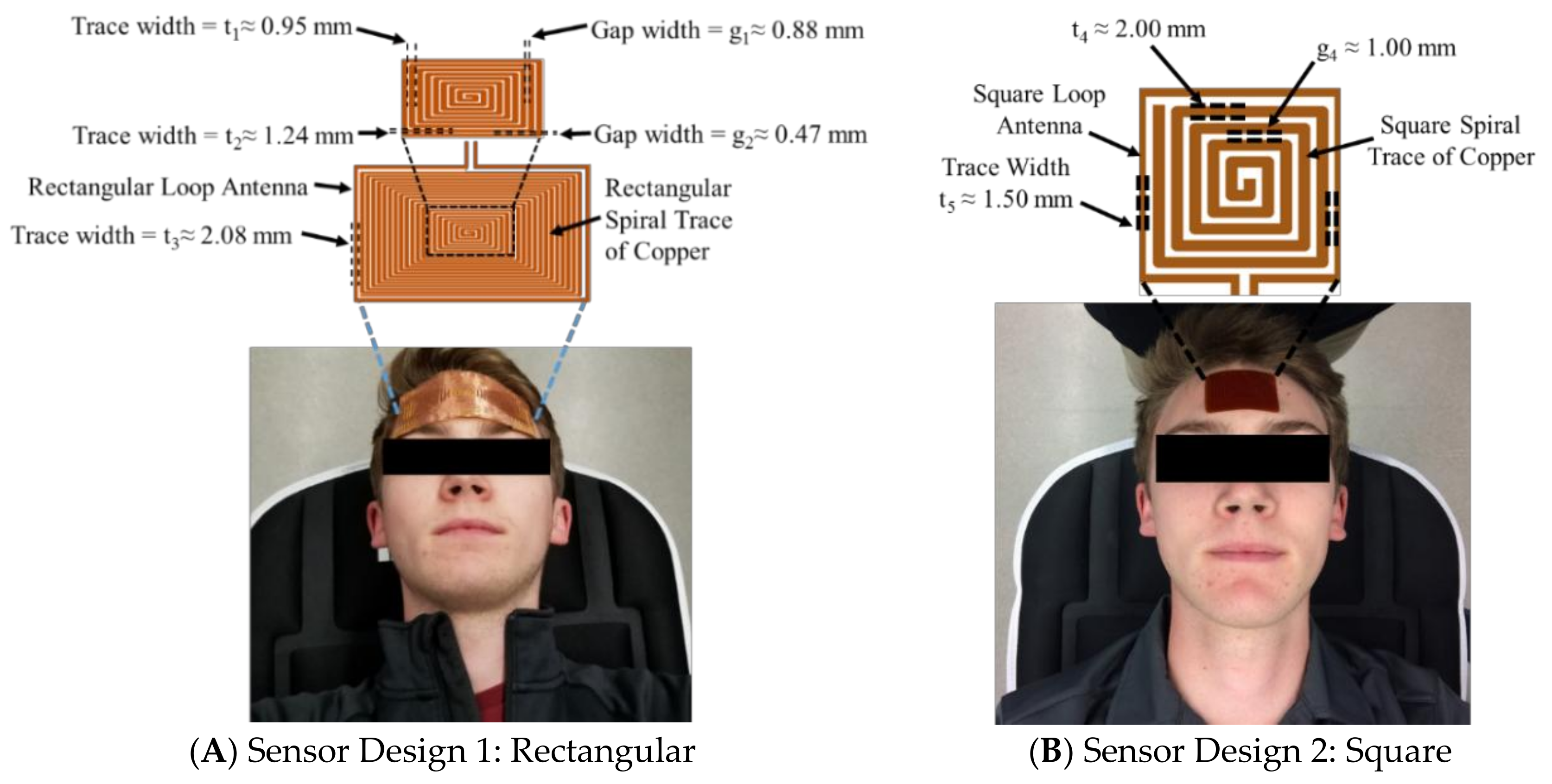
2.1. Sensor Design and Data Collection Setup
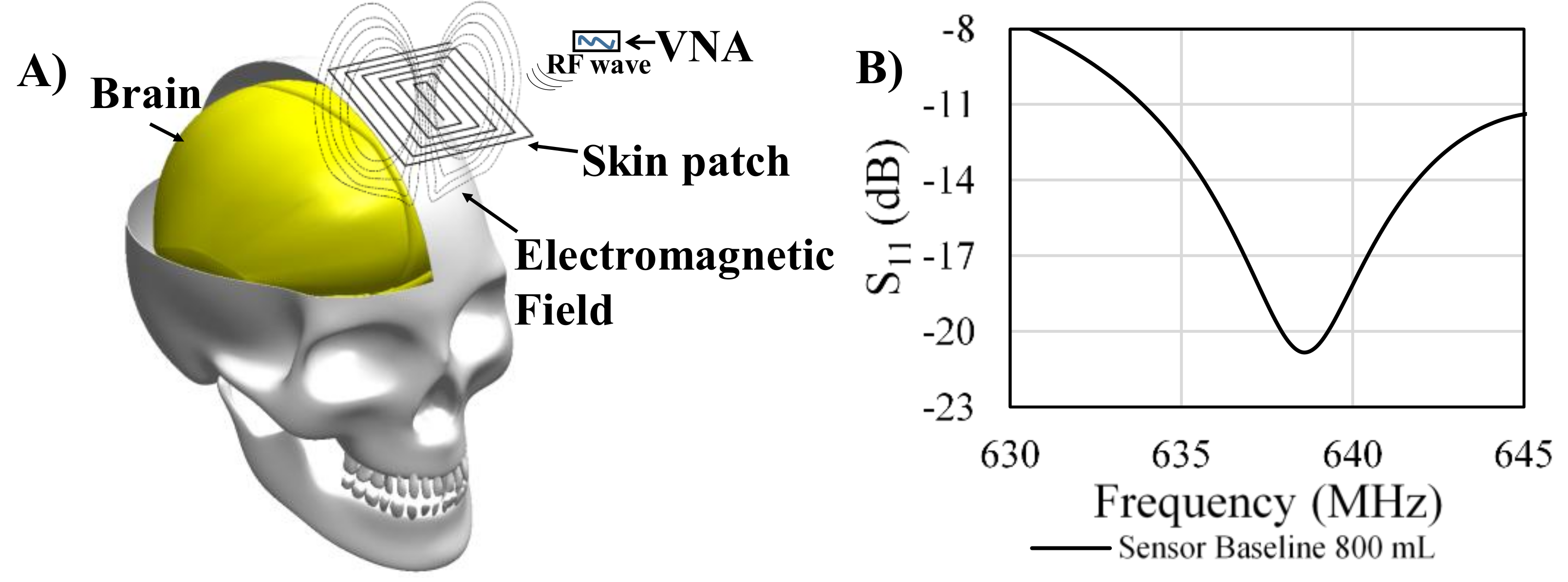
2.2. Theory and Operating Principle
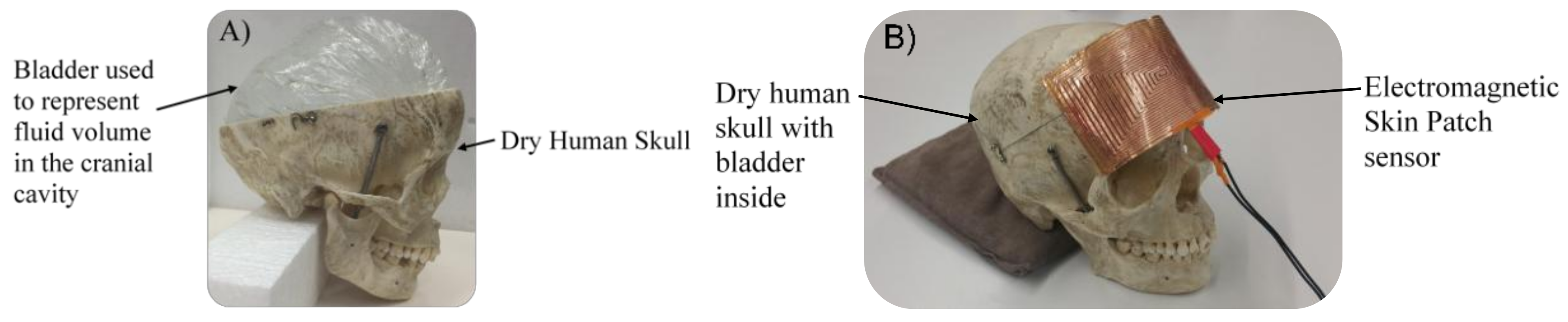
2.3. Dry Human Skull Model
2.4. Preliminary Proof-of-Concept Human Tests
2.4.1. Human Subjects
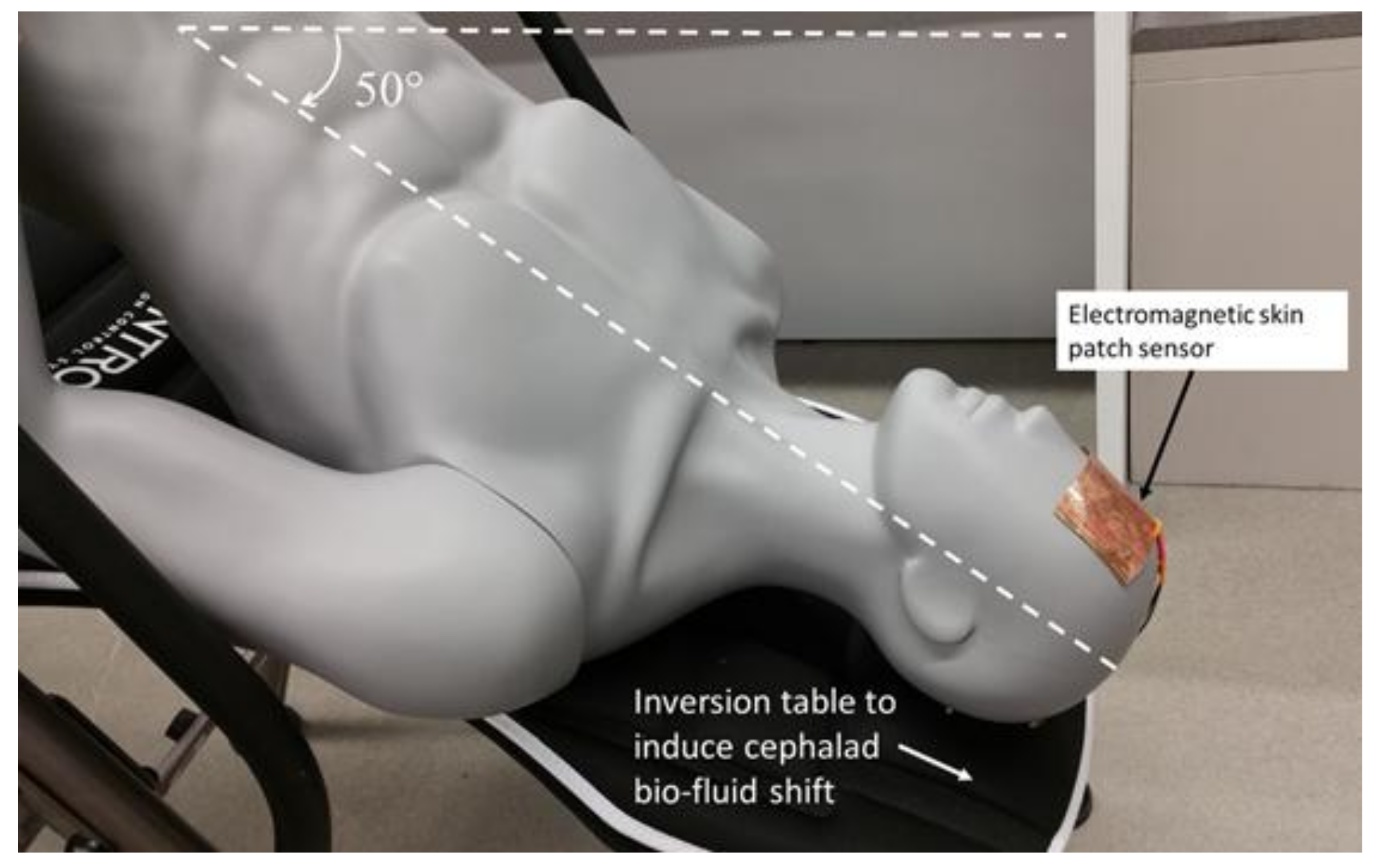
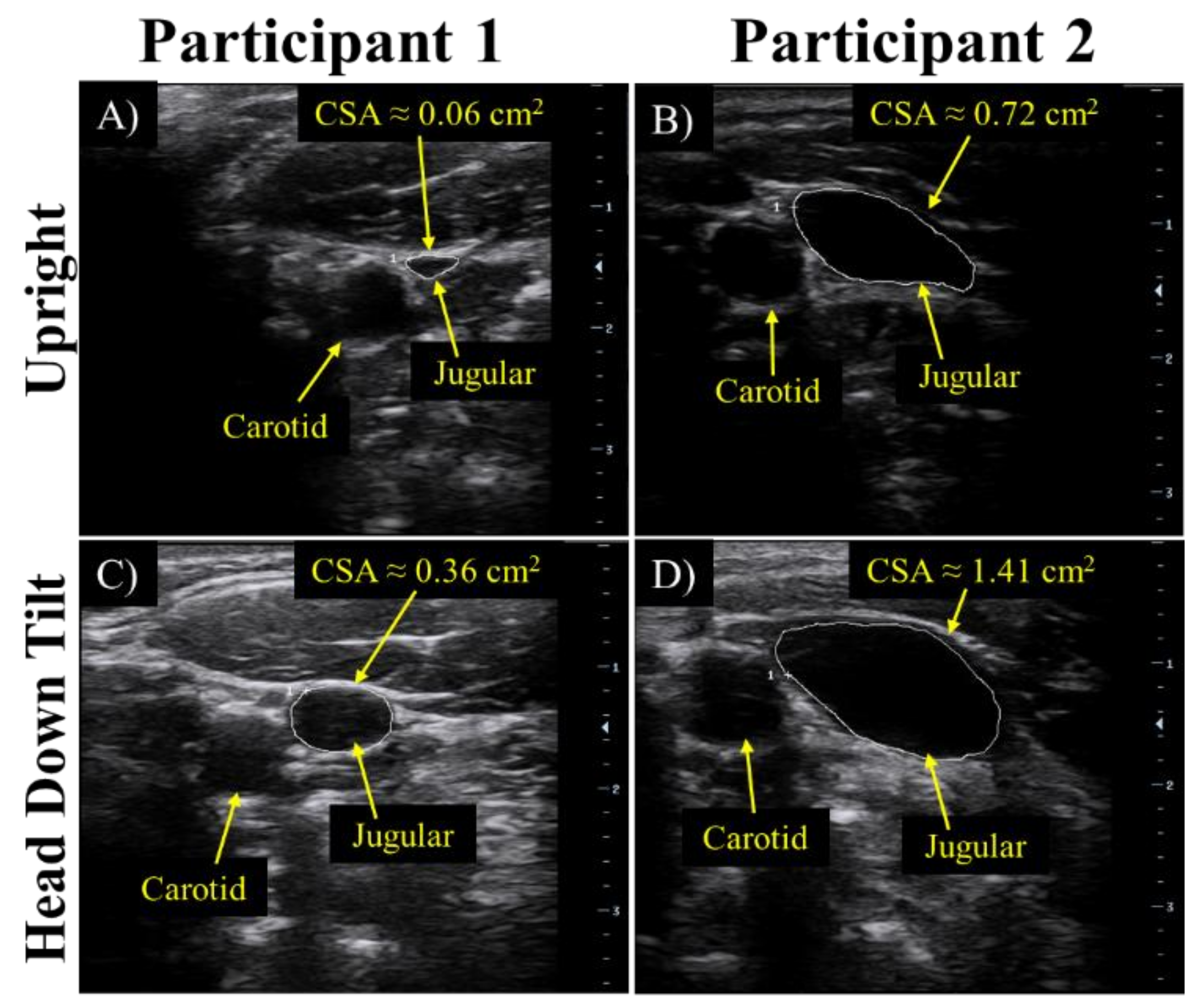
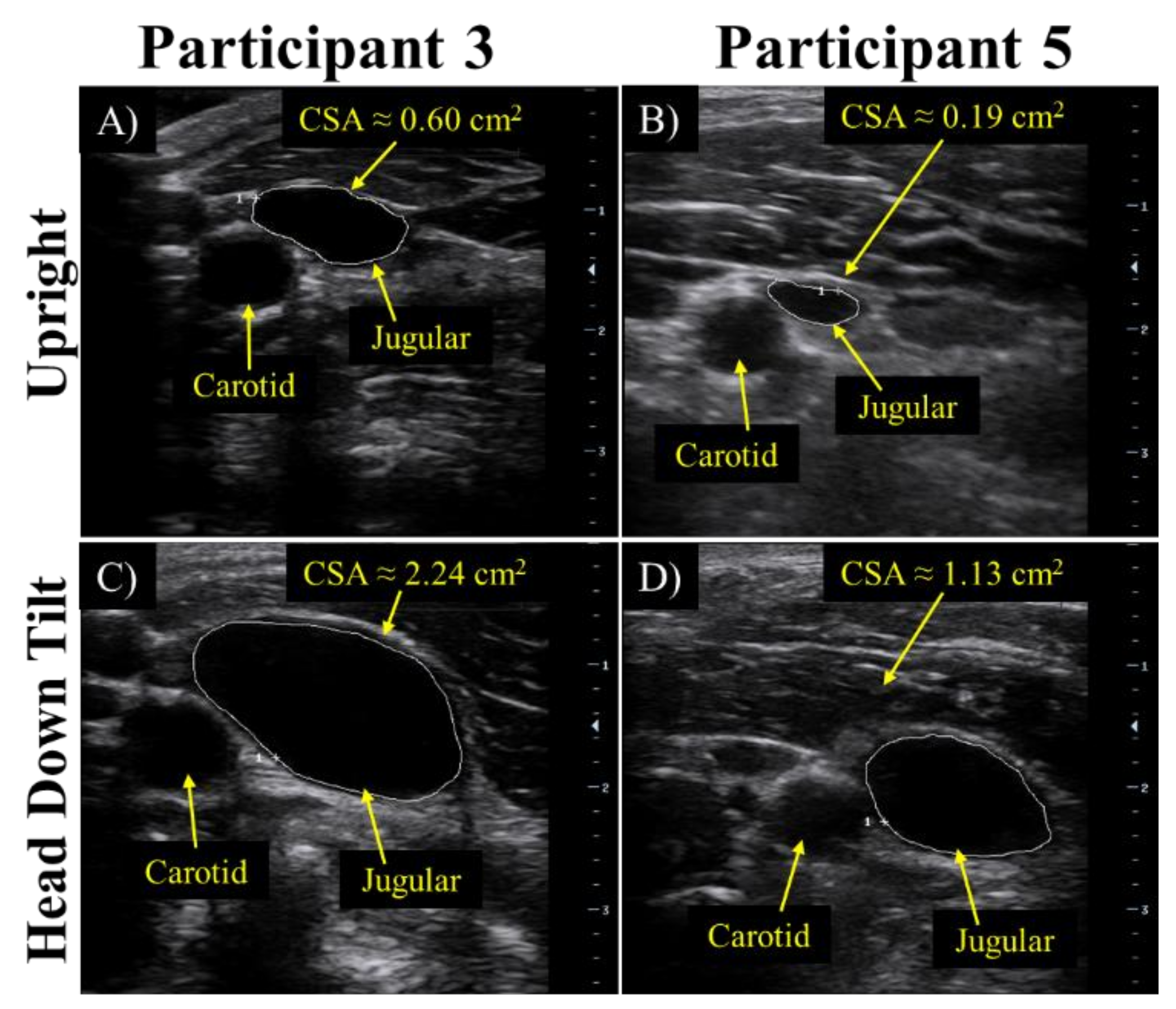
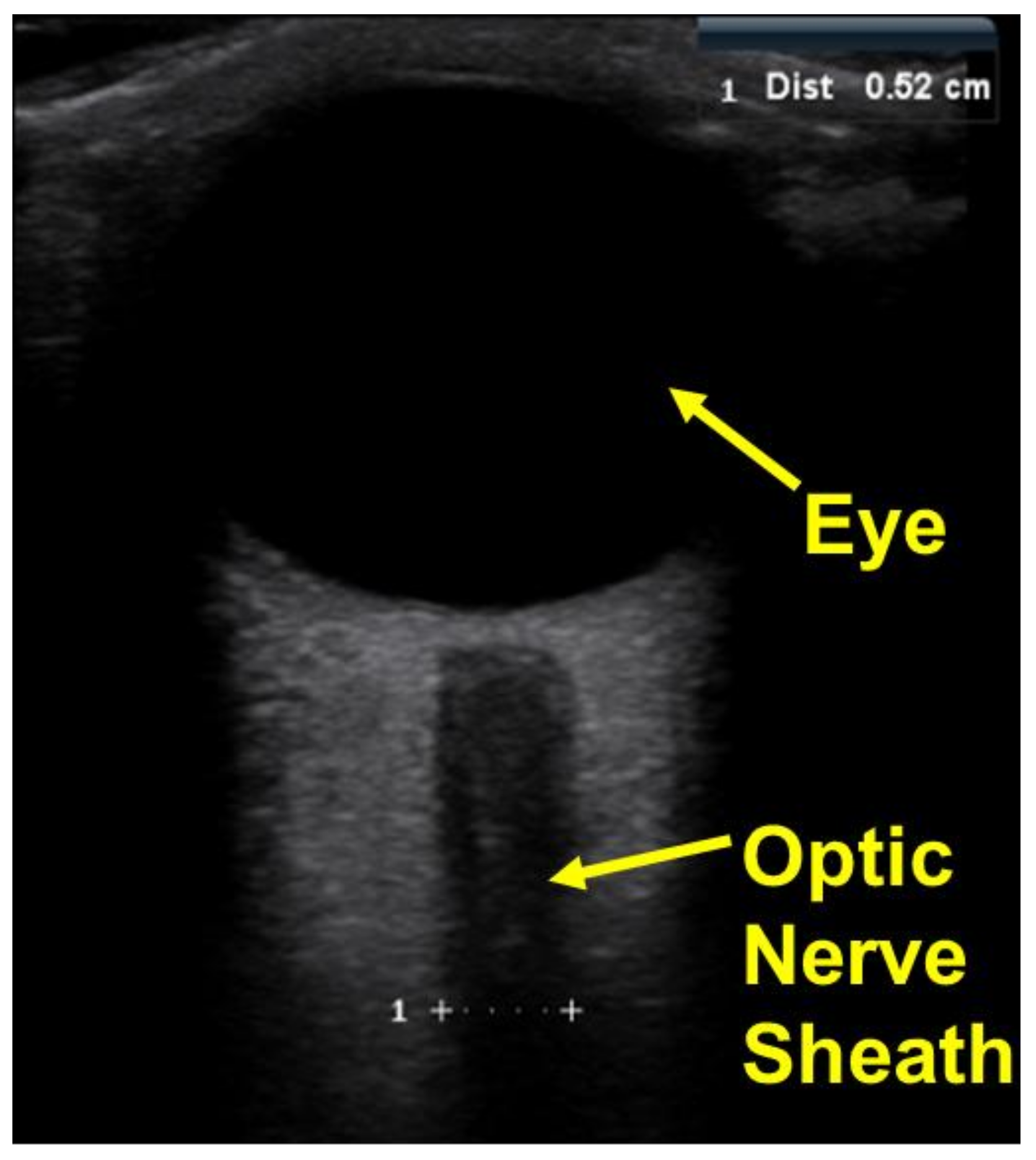
2.4.2. Validation of Bio-Fluid Shift
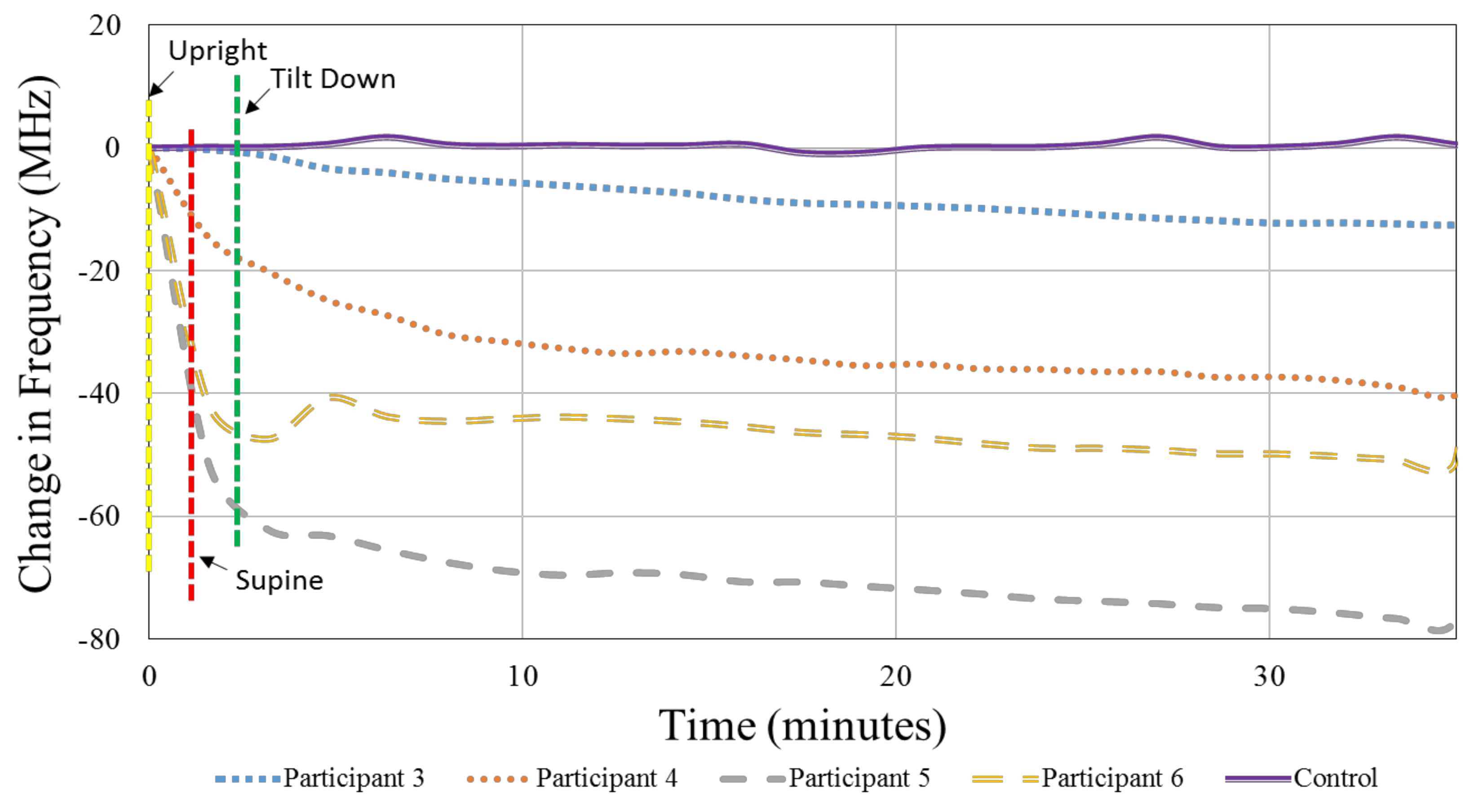
2.4.3. Data Collection for Human Testing—Head Down Tilt Study
2.4.4. Repeatability of Measurements
3. Results
3.1. Electromagnetic Resonant Sensor
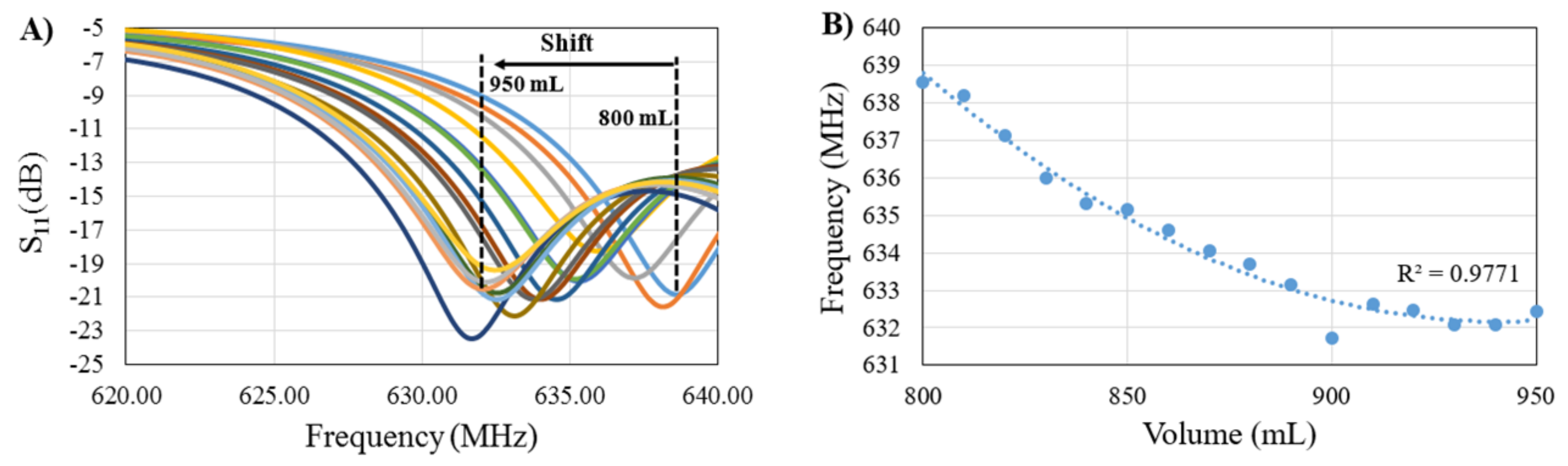
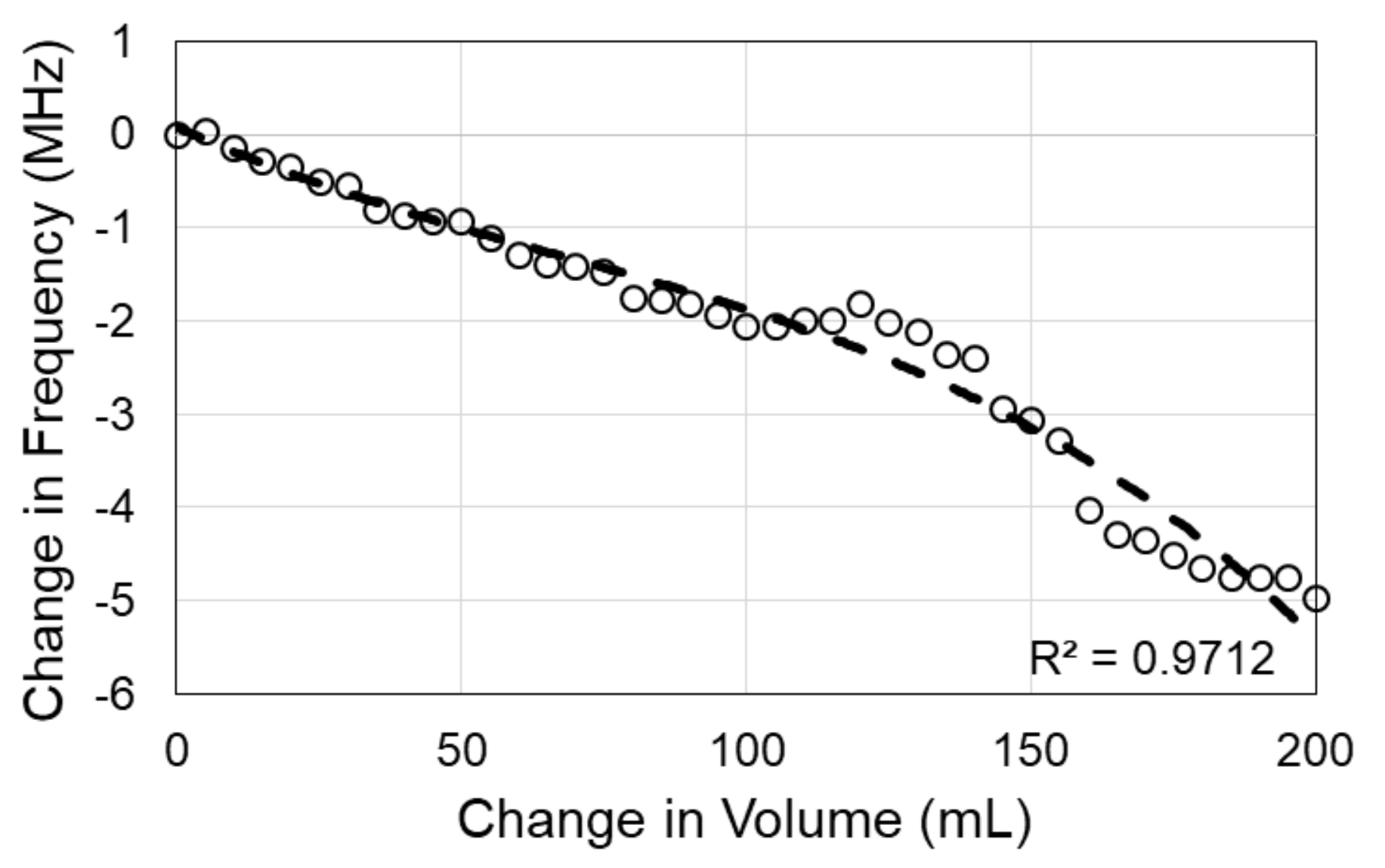
3.2. Sensor Signal Response Due to Volumetric Changes in Skull Model
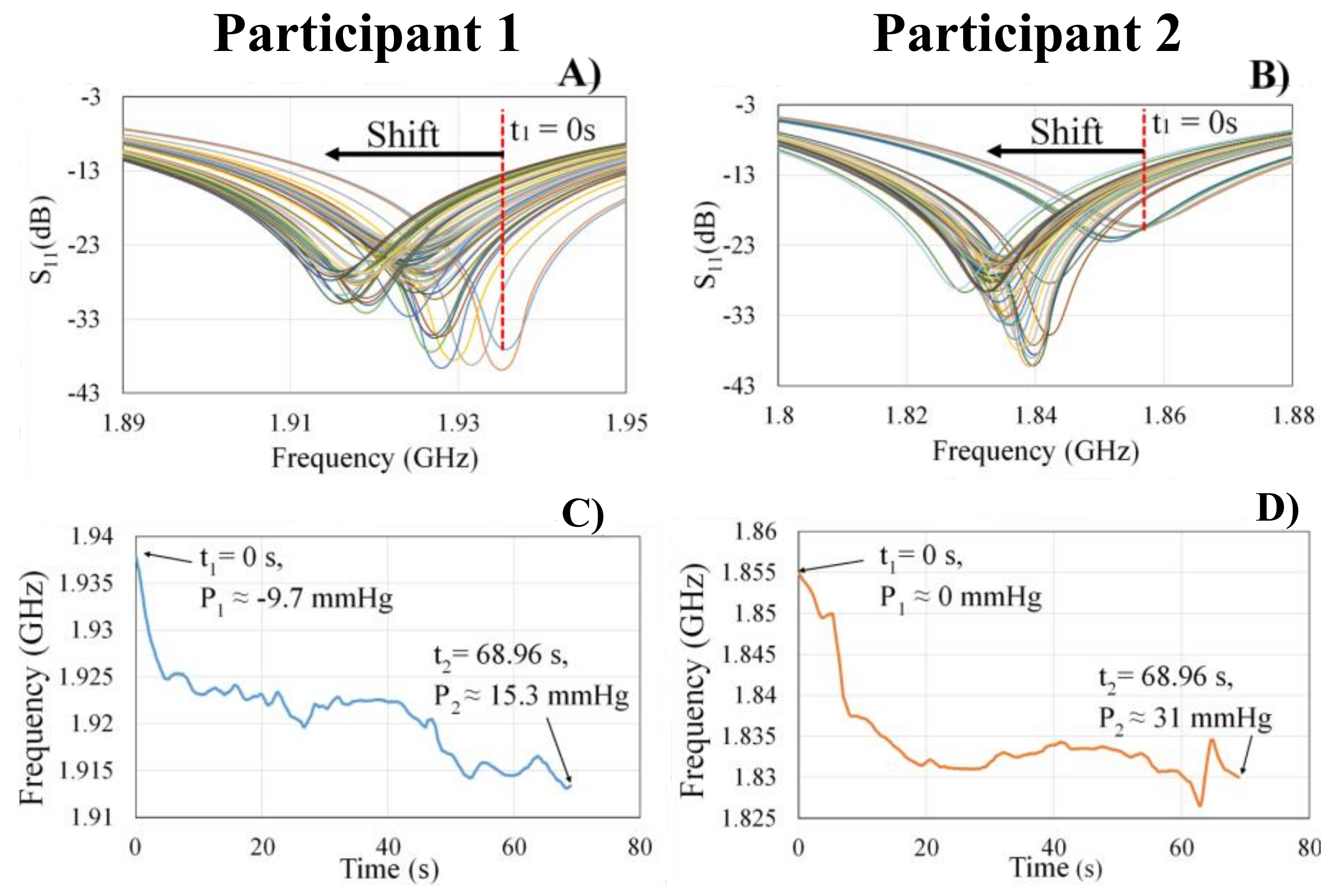
3.3. Preliminary Human Tests
4. Discussion
Potential Clinical Applications
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Raboel, P.; Bartek, J.; Andresen, M.; Bellander, B.; Romner, B. Intracranial pressure monitoring: Invasive versus non-invasive methods—A review. Crit. Care Res. Pract. 2012, 2012. [Google Scholar] [CrossRef] [PubMed]
- Steiner, L.; Andrews, P. Monitoring the injured brain: ICP and CBF. Br. J. Anaesth. 2006, 97, 26–38. [Google Scholar] [CrossRef] [PubMed]
- Abraham, M.; Singhal, V. Intracranial pressure monitoring. J. Neuroanaesthesiol. Crit. Care 2015, 2, 193–203. [Google Scholar] [CrossRef]
- Avezaat, C.J.; van Eijndhoven, J.H.; Wyper, D.J. Cerebrospinal fluid pulse pressure and intracranial volume-pressure relationships. J. Neurol. Neurosurg. Psychiatry 1979, 42, 687–700. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, J.B.; Shiloh, A.L.; Savel, R.H.; Eisen, L.A. Non-invasive methods of estimating intracranial pressure. Neurocrit. Care 2011, 15, 599–608. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Scalzo, F.; Bergsneider, M.; Vespa, P.; Martin, N.; Hu, X. Noninvasive Intracranial Pressure Assessment based on Data Mining Approach using Nonlinear Mapping Function. IEEE Trans. Biomed. Eng. 2012, 59, 619–626. [Google Scholar] [PubMed]
- Harmon, K.G.; Drezner, J.A.; Gammons, M.; Guskiewicz, K.M.; Halstead, M.; Herring, S.A.; Kutcher, J.S.; Pana, A.; Putukian, M.; Roberts, W.O. American Medical Society for Sports Medicine position statement: Concussion in sport. Br. J. Sports Med. 2013, 47, 15–26. [Google Scholar] [CrossRef]
- Nelson, E.; Mulugeta, L.; Myers, J. Microgravity-Induced Fluid Shift and Ophthalmic Changes. Life 2014, 4, 621–665. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.-F.; Hargens, A.R. Intraocular/Intracranial pressure mismatch hypothesis for visual impairment syndrome in space. Aviat. Space Environ. Med. 2014, 85, 78–80. [Google Scholar] [CrossRef] [PubMed]
- Flores, O.; Rubinsky, B.; González, C.A. Experimental sensitivity study of inductive phase shift spectroscopy as non-invasive method for hypoperfusion vs bleeding volumetric detection in brain. In Proceedings of the 30th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Vancouver, BC, Canada, 20–25 August 2008; pp. 678–681. [Google Scholar]
- González, C.A.; Blumrosen, G.; Rubinsky, B. Remote Monitoring of Internal Bleeding Based on Magnetic Induction and Cellular Phone Technology: A Potential Application in Poor Regions in México. Comput. Sist. 2010, 14, 187–195. [Google Scholar]
- González, C.A.; Horowitz, L.; Rubinsky, B. In vivo inductive phase shift measurements to detect intraperitoneal fluid. IEEE Trans. Biomed. Eng. 2007, 54, 953–956. [Google Scholar] [CrossRef] [PubMed]
- González, C.A.; Rojas, R.; Villanueva, C.; Rubinsky, B. Inductive phase shift spectroscopy for volumetric brain edema detection: An experimental simulation. In Proceedings of the 29th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Lyon, France, 22–29 August 2007; pp. 2346–2349. [Google Scholar]
- González, C.A.; Rubinsky, B. Frequency dependence of phase shift in edema: A theoretical study with magnetic induction. In Proceedings of the 27th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Shanghai, China, 17–18 January 2006; pp. 3518–3521. [Google Scholar]
- Mobashsher, A.T.; Bialkowski, K.S.; Abbosh, A.M.; Crozier, S. Design and Experimental Evaluation of a Non-Invasive Microwave Head Imaging System for Intracranial Haemorrhage Detection. PLoS ONE 2016, 11, e0152351. [Google Scholar] [CrossRef] [PubMed]
- Rojas, R.; Rubinsky, B.; Gonzalez, C. The effect of brain hematoma location on volumetric inductive phase shift spectroscopy of the brain with circular and magnetron sensor coils: A numerical simulation study. Physiol. Meas. 2008, 29, S255–S266. [Google Scholar] [CrossRef] [PubMed]
- Scharfetter, H.; Casañas, R.; Rosell, J. Biological tissue characterization by magnetic induction spectroscopy (MIS): Requirements and limitations. IEEE Trans. Biomed. Eng. 2003, 50, 870–880. [Google Scholar] [CrossRef] [PubMed]
- Watson, S.; Williams, R.J.; Gough, W.; Griffiths, H. A magnetic induction tomography system for samples with conductivities below 10 S m−1. Meas. Sci. Technol. 2008, 19, 1–11. [Google Scholar] [CrossRef]
- Zhang, Z.; Liu, P.; Zhou, D.; Zhang, L.; Lei, H. Intracerebral hemorrhage (ICH) evaluation with a novel magnetic induction sensor: A preliminary study using the Chinese head model. Biomed. Mater. Eng. 2014, 24, 3579–3587. [Google Scholar] [PubMed]
- Griffith, J.L.; Andre’A, W.; Moore-Jansen, P.; Cluff, K. Non-invasive biomedical patch sensor to measure intracranial pressure. In Proceedings of the 2016 IEEE 13th International Conference on Wearable and Implantable Body Sensor Networks (BSN), San Francisco, CA, USA, 14–17 June 2016; p. 211. [Google Scholar]
- Cluff, K.; Becker, R.; Jayakumar, B.; Han, K.; Condon, E.; Dudley, K.; Szatkowski, G.; Pipinos, I.I.; Amick, R.Z.; Patterson, J. Passive Wearable Skin Patch Sensor Measures Limb Hemodynamics Based on Electromagnetic Resonance. IEEE Trans. Biomed. Eng. 2018, 65, 847–856. [Google Scholar] [CrossRef] [PubMed]
- Onorio, I.; Michele, M. A spiral passive electromagnetic sensor (SPES) for wireless and wired structural health monitoring. Meas. Sci. Technol. 2016, 27, 045601. [Google Scholar]
- Szatkowski, G.N.; Dudley, K.L.; Smith, L.J.; Wang, C.; Ticatch, L.A. Open Circuit Resonant (SansEC) Sensor Technology for Lightning Mitigation and Damage Detection and Diagnosis for Composite Aircraft Applications; Technical Report: NASA/TP-2014-218554; NASA: Washington, DC, USA, 2014. [Google Scholar]
- Woodard, S.E. SansEC sensing technology—A new tool for designing space systems and components. In Proceedings of the 2011 IEEE Aerospace Conference, Big Sky, MT, USA, 5–12 March 2011; pp. 1–11. [Google Scholar]
- Alruwaili, F.H.; Griffith, J.L.; Cluff, K.; Patterson, J.A. Non-invasive point-of-care method for measuring left-ventricular stroke-volume using a passive electromagnetic skin patch sensor. J. Am. Coll. Cardiol. 2017, 69, 1068. [Google Scholar] [CrossRef]
- Rogers, J.; Jayakumar, B.; Patterson, J.; Cluff, K. Abstract 516: Electromagnetic Properties of Blood-flow for Screening of Peripheral Artery Disease. Arterioscler. Thromb. Vasc. Biol. 2016, 36 (Suppl. 1), A516. [Google Scholar]
- Griffith, J.; Eckerman, B.; Becker, R.; Richardson, A.; Cluff, K. Non-invasive Method for Monitoring Microgravity Induced Bio-fluid shifts in Lower Limbs. In Proceedings of the American Society for Gravitational and Space Research (ASGSR) Conference, Seattle, WA, USA, 25–28 October 2017. [Google Scholar]
- Woodard, S.E. Functional electrical sensors as single component electrically open circuits having no electrical connections. IEEE Trans. Instrum. Meas. 2010, 59, 3206–3213. [Google Scholar] [CrossRef]
- Herczyński, A. Bound charges and currents. Am. J. Phys. 2013, 81, 202–205. [Google Scholar] [CrossRef]
- Mobashsher, A.T.; Mahmoud, A.; Abbosh, A.M. Portable Wideband Microwave Imaging System for Intracranial Hemmorhage Detection Using Improved Back-projection Algorithm with Model of Effective Head Permittivity. Sci. Rep. 2016, 6, 20459. [Google Scholar] [CrossRef] [PubMed]
- Kumari, S.; Gupta, V.R. Measurement of specific absorption rate of monopole patch antenna on human arm. Int. J. Microw. Opt. Technol. 2015, 10, 190–194. [Google Scholar]
- Mohammed, B.A.J.; Abbosh, A.M. Realistic head phantom to test microwave systems for brain imaging. Microw. Opt. Technol. Lett. 2014, 56, 979–982. [Google Scholar] [CrossRef]
- Watkins, W.; Hargens, A.R.; Baird, S.; Clary, E.M.; Macias, B.R. Lower-body negative pressure decreases non-invasively measured intracranial pressure and internal jugular vein cross-sectional area during head-down tilt. J. Appl. Physiol. 2017, 123, 260–266. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.J.; Yao, Y.; Feng, L.S.; Wang, Y.Z.; Zheng, N.N.; Feng, J.C.; Xing, Y.Q. Noninvasive and quantitative intracranial pressure estimation using ultrasonographic measurement of optic nerve sheath diamter. Sci. Rep. 2017, 7, 42063. [Google Scholar] [CrossRef] [PubMed]
- Bolouri, H.; Säljö, A.; Viano, D.C.; Hamberger, A. Animal model for sport-related concussion; ICP and cognitive function. Acta Neurol. Scand. 2012, 125, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Engelborghs, K.; Verlooy, J.; Van Deuren, B.; Van Reempts, J.; Borgers, M. Intracranial pressure in a modified experimental model of closed head injury. In Brain Edema X; Springer: Berlin/Heidelberg, Germany, 1997; pp. 123–125. [Google Scholar]
- Bey, T.; Ostick, B. Second impact syndrome. West. J. Emerg. Med. 2009, 10, 6–10. [Google Scholar] [PubMed]
- Wetjen, N.M.; Pichelmann, M.A.; Atkinson, J.L. Second impact syndrome: Concussion and second injury brain complications. J. Am. Coll. Surg. 2010, 211, 553–557. [Google Scholar] [CrossRef] [PubMed]













© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Griffith, J.; Cluff, K.; Eckerman, B.; Aldrich, J.; Becker, R.; Moore-Jansen, P.; Patterson, J. Non-Invasive Electromagnetic Skin Patch Sensor to Measure Intracranial Fluid–Volume Shifts. Sensors 2018, 18, 1022. https://doi.org/10.3390/s18041022
Griffith J, Cluff K, Eckerman B, Aldrich J, Becker R, Moore-Jansen P, Patterson J. Non-Invasive Electromagnetic Skin Patch Sensor to Measure Intracranial Fluid–Volume Shifts. Sensors. 2018; 18(4):1022. https://doi.org/10.3390/s18041022
Chicago/Turabian StyleGriffith, Jacob, Kim Cluff, Brandon Eckerman, Jessica Aldrich, Ryan Becker, Peer Moore-Jansen, and Jeremy Patterson. 2018. "Non-Invasive Electromagnetic Skin Patch Sensor to Measure Intracranial Fluid–Volume Shifts" Sensors 18, no. 4: 1022. https://doi.org/10.3390/s18041022
APA StyleGriffith, J., Cluff, K., Eckerman, B., Aldrich, J., Becker, R., Moore-Jansen, P., & Patterson, J. (2018). Non-Invasive Electromagnetic Skin Patch Sensor to Measure Intracranial Fluid–Volume Shifts. Sensors, 18(4), 1022. https://doi.org/10.3390/s18041022