Three-Dimensional Registration of Freehand-Tracked Ultrasound to CT Images of the Talocrural Joint


Abstract
:1. Introduction
2. Materials and Methods
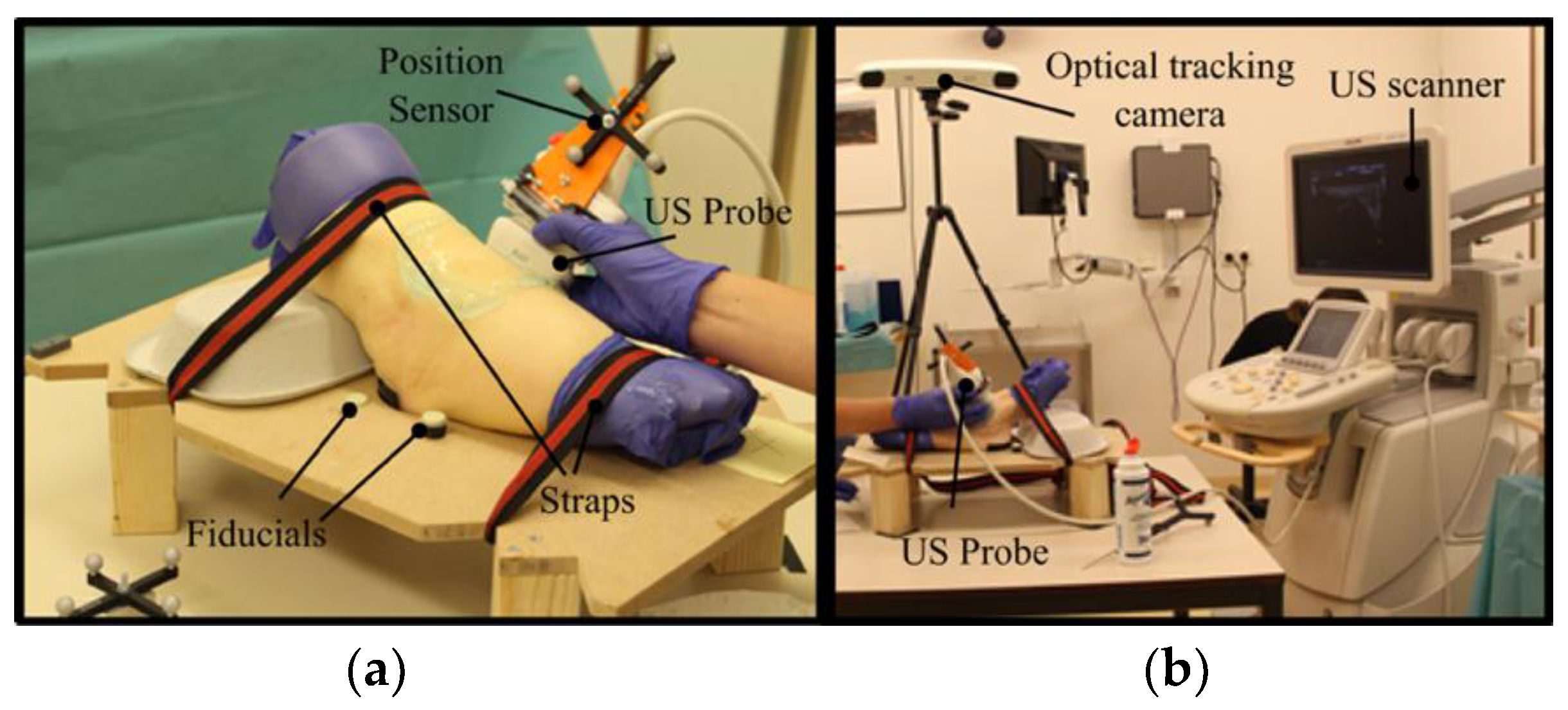
2.1. Test Data Acquisition
2.1.1. CT Scans
2.1.2. Freehand Tracked 2D US Images
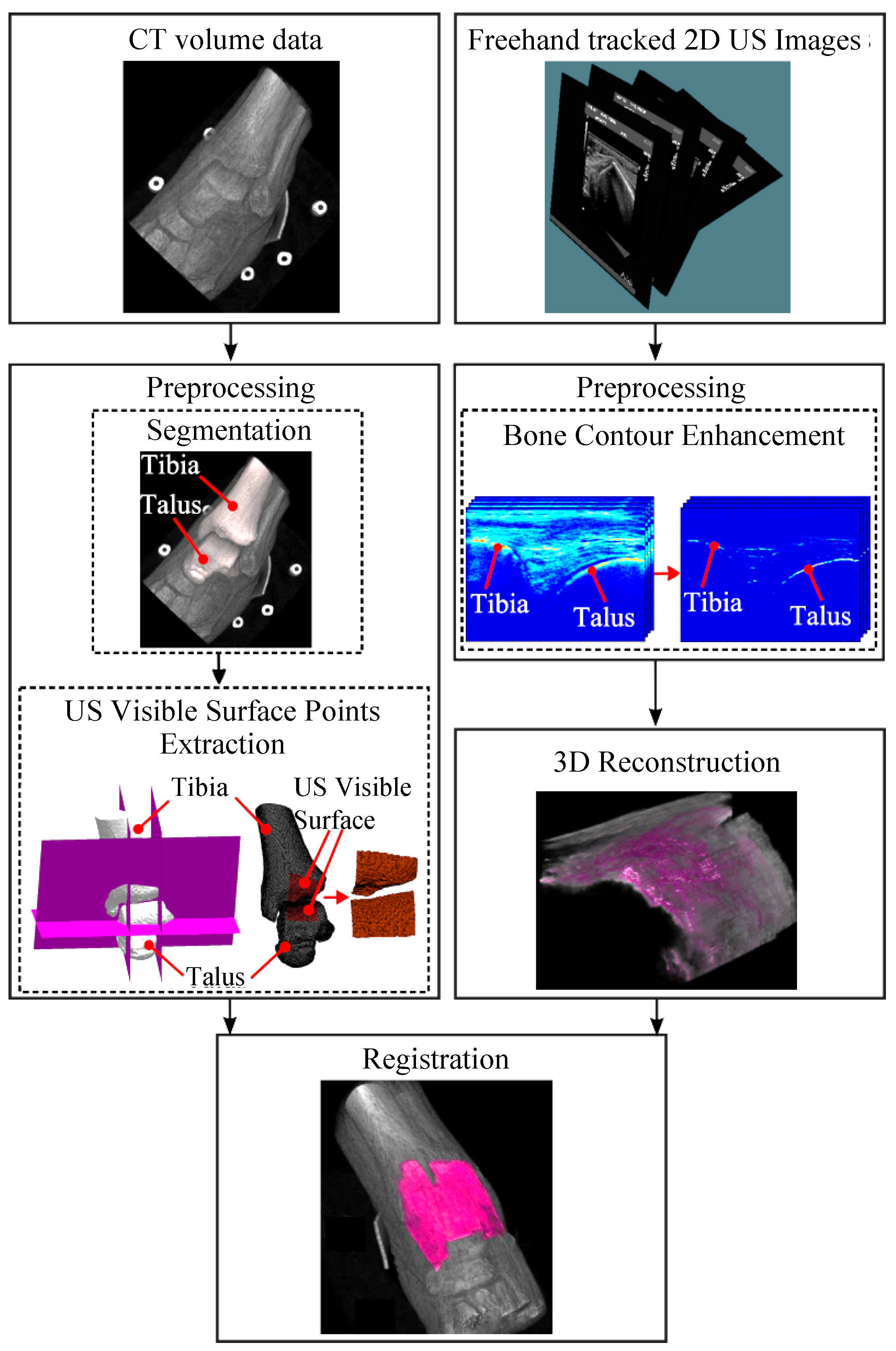
2.2. Data Preprocessing
2.2.1. Surface Point Extraction from CT Data
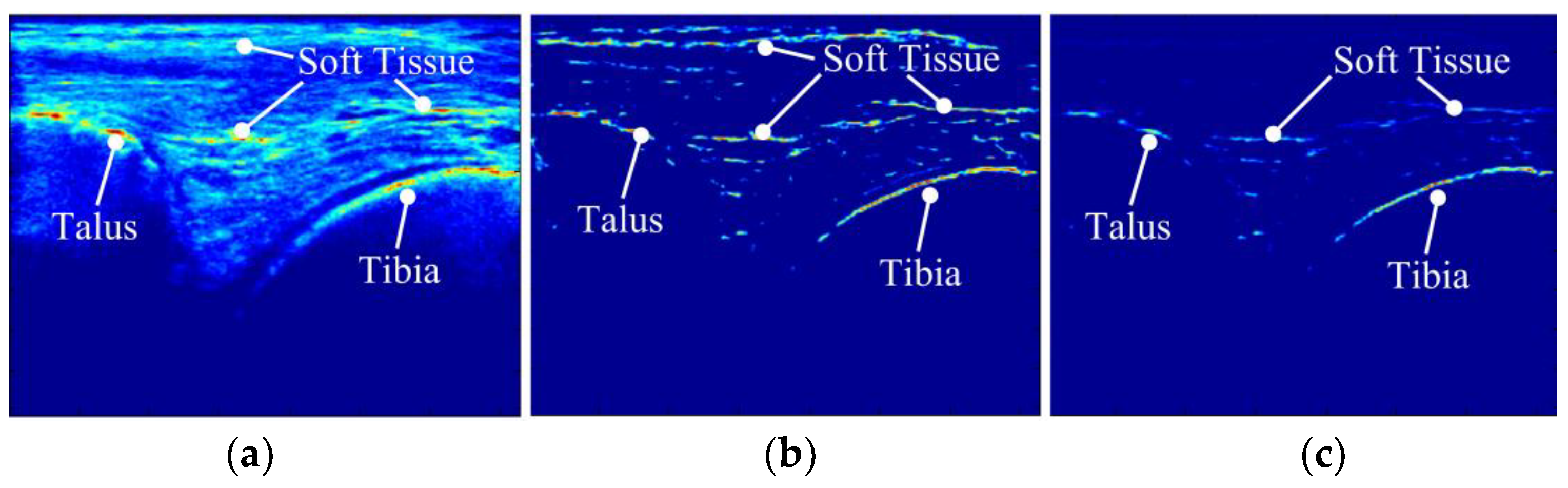
2.2.2. Bone Surface Enhancement in Ultrasound
2.3. 3D Bone Response Data and US to CT Registration
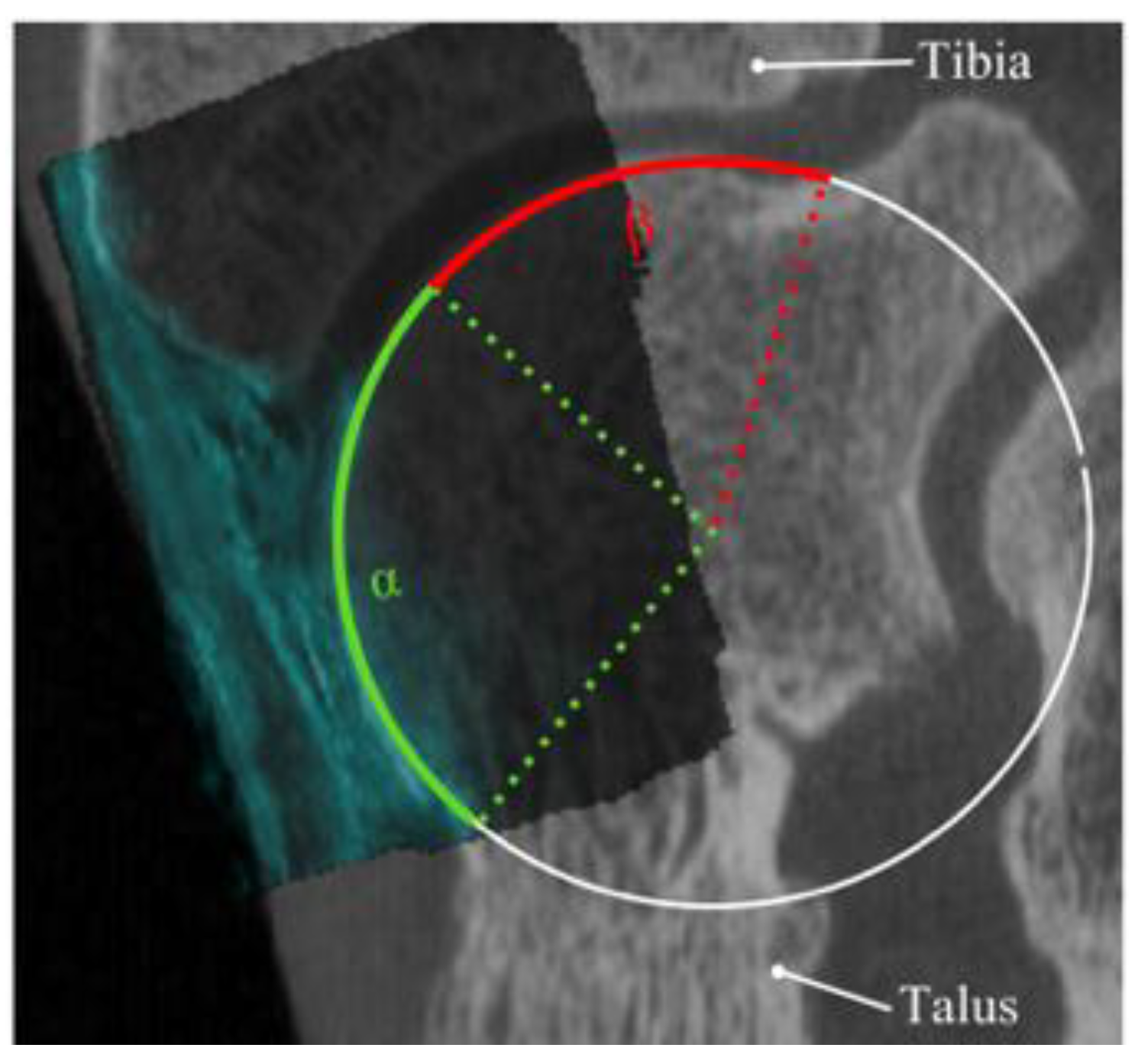
2.4. Evaluation of the Registrations
2.5. Clinical Study
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Raikin, S.M.; Elias, I.; Zoga, A.C.; Morrison, W.B.; Besser, M.P.; Schweitzer, M.E. Osteochondral Lesions of the Talus: Localization and Morphologic Data from 424 Patients Using a Novel Anatomical Grid Scheme. Foot Ankle Int. 2007, 28, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Heijink, A.; Vanhees, M.; van den Ende, K.; van den Bekerom, M.P.; van Riet, R.P.; Van Dijk, C.N.; Eygendaal, D. Biomechanical Considerations in the Pathogenesis of Osteoarthritis of the Elbow. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 2313–2318. [Google Scholar] [CrossRef] [PubMed]
- Orr, J.D.; Dawson, L.K.; Garcia, E.J.; Kirk, K.L. Incidence of Osteochondral Lesions of the Talus in the United States Military. Foot Ankle Int. 2011, 32, 948–954. [Google Scholar] [CrossRef] [PubMed]
- Zengerink, M.; Struijs, P.A.A.; Tol, J.L.; van Dijk, C.N. Treatment of Osteochondral Lesions of the Talus: A Systematic Review. Knee Surg. Sports Traumatol. Arthrosc. 2010, 18, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Verhagen, R.A.; Struijs, P.A.; Bossuyt, P.M.; van Dijk, C.N. Systematic Review of Treatment Strategies for Osteochondral Defects of the Talar Dome. Foot Ankle Clin. 2003, 8, 233–242. [Google Scholar] [CrossRef]
- Farr, J.; Cole, B.; Dhawan, A.; Kercher, J.; Sherman, S. Clinical Cartilage Restoration: Evolution and Overview. Clin. Orthop. Relat. Res. 2011, 469, 2696–2705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kok, A.C.; Terra, M.P.; Muller, S.; Askeland, C.; van Dijk, C.N.; Kerkhoffs, G.M.M.J.; Tuijthof, G.J.M. Feasibility of Ultrasound Imaging of Osteochondral Defects Inthe Ankle: A Clinical Pilot Study. Ultrasound Med. Biol. 2014, 40, 2530–2536. [Google Scholar] [CrossRef] [PubMed]
- Tuijthof, G.J.M.; Kok, A.C.; Terra, M.P.; Aaftink, J.F.A.; Streekstra, G.J.; van Dijk, C.N.; Kerkhoffs, G.M.M.J. Sensitivity and Specificity of Ultrasound in Detecting (Osteo)chondral Defects: A Cadaveric Study. Ultrasound Med. Biol. 2013, 39, 1368–1375. [Google Scholar] [CrossRef] [PubMed]
- Möller, I.; Bong, D.; Naredo, E.; Filippucci, E.; Carrasco, I.; Moragues, C.; Iagnocco, A. Ultrasound in the Study and Monitoring of Osteoarthritis. Osteoarthr. Cartil. 2008, 16, 4–7. [Google Scholar] [CrossRef] [PubMed]
- Spannow, A.H.; Pfeiffer-Jensen, M.; Andersen, N.T.; Stenbøg, E.; Herlin, T.; Rheumatology, P.; Spannow, A.H.; Pfeiffer-Jensen, M.; Andersen, N.T.; Stenbøg, E.; et al. Inter -and Intraobserver Variation of Ultrasonographic Cartilage Thickness Assessments in Small and Large Joints in Healthy Children. Pediatr. Rheumatol. Online J. 2009, 7, 12. [Google Scholar] [CrossRef] [PubMed]
- Van Bergen, C.J.; Gerards, R.M.; Opdam, K.T.; Terra, M.P.; Kerkhoffs, G.M. Diagnosing, Planning and Evaluating Osteochondral Ankle Defects with Imaging Modalities. World J. Orthop. 2015, 6, 944–953. [Google Scholar] [CrossRef] [PubMed]
- Barratt, D.C.; Penney, G.P.; Chan, C.S.K.; Slomczykowski, M.; Carter, T.J.; Edwards, P.J.; Hawkes, D.J. Self-Calibrating 3D-Ultrasound-Based Bone Registration for Minimally Invasive Orthopedic Surgery. IEEE Trans. Med. Imaging 2006, 25, 312–323. [Google Scholar] [CrossRef] [PubMed]
- Brounstein, A.; Hacihaliloglu, I.; Guy, P.; Hodgson, A.; Abugharbieh, R. Towards Real-Time 3D US to CT Bone Image Registration Using Phase and Curvature Feature Based GMM Matching. In International Conference on Medical Image Computing and Computer-Assisted Intervention; Springer: Berlin/Heidelberg, Germany, 2011; Volume 6891, pp. 235–242. [Google Scholar]
- Hacihaliloglu, I.; Brounstein, A.; Guy, P.; Hodgson, A.; Abugharbieh, R. 3D Ultrasound-CT Registration in Orthopaedic Trauma Using GMM Registration with Optimized Particle Simulation-Based Data Reduction. In International Conference on Medical Image Computing and Computer-Assisted Intervention; Springer: Berlin/Heidelberg, Germany, 2012; Volume 15, pp. 82–89. [Google Scholar]
- Lang, A.; Mousavi, P.; Gill, S.; Fichtinger, G.; Abolmaesumi, P. Multi-Modal Registration of Speckle-Tracked Freehand 3D Ultrasound to CT in the Lumbar Spine. Med. Image Anal. 2012, 16, 675–686. [Google Scholar] [CrossRef] [PubMed]
- Moghari, M.H.; Abolmaesumi, P. Point-Based Rigid-Body Registration Using an Unscented Kalman Filter. IEEE Trans. Med. Imaging 2007, 26, 1708–1728. [Google Scholar] [CrossRef] [PubMed]
- Penney, G.P.; Barratt, D.C.; Chan, C.S.K.; Slomczykowski, M.; Carter, T.J.; Edwards, P.J.; Hawkes, D.J. Cadaver Validation of Intensity-Based Ultrasound to CT Registration. In International Conference on Medical Image Computing and Computer-Assisted Intervention; Springer: Berlin/Heidelberg, Germany, 2005; Volume 3750, pp. 1000–1007. [Google Scholar]
- Muratore, D.M.; Russ, J.H.; Dawant, B.M.; Galloway, R.L. Three-Dimensional Image Registration of Phantom Vertebrae for Image-Guided Surgery: A Preliminary Study. Comput. Aided Surg. 2002, 7, 342–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winter, S.; Pechlivanis, I.; Dekomien, C.; Igel, C.; Schmieder, K. Toward Registration of 3D Ultrasound and CT Images of the Spine in Clinical Praxis: Design and Evaluation of a Data Acquisition Protocol. Ultrasound Med. Biol. 2009, 35, 1773–1782. [Google Scholar] [CrossRef] [PubMed]
- Yan, C.X.B.; Goulet, B.; Pelletier, J.; Chen, S.J.S.; Tampieri, D.; Collins, D.L. Towards Accurate, Robust and Practical Ultrasound-CT Registration of Vertebrae for Image-Guided Spine Surgery. Int. J. Comput. Assist. Radiol. Surg. 2011, 6, 523–537. [Google Scholar] [CrossRef] [PubMed]
- Brendel, B.; Winter, S.; Rick, A.; Stockheim, M.; Ermert, H. Bone Registration with 3D CT and Ultrasound Data Sets. Int. Congr. Ser. 2003, 1256, 426–432. [Google Scholar] [CrossRef]
- Nagpal, S.; Abolmaesumi, P.; Rasoulian, A.; Hacihaliloglu, I.; Ungi, T.; Osborn, J.; Lessoway, V.A.; Rudan, J.; Jaeger, M.; Rohling, R.N.; et al. A Multi-Vertebrae CT to US Registration of the Lumbar Spine in Clinical Data. Int. J. Comput. Assist. Radiol. Surg. 2015, 10, 1371–1381. [Google Scholar] [CrossRef] [PubMed]
- Rasoulian, A.; Mousavi, P.; Hedjazi Moghari, M.; Foroughi, P.; Abolmaesumi, P. Group-Wise Feature-Based Registration of CT and Ultrasound Images of Spine. In Medical Imaging 2010: Visualization, Image-Guided Procedures, and Modeling; International Society for Optics and Photonics: Bellingham, WA, USA, 2010; Volume 7625, p. 76250R. [Google Scholar]
- Amin, D.V.; Kanade, T.; DiGioia, A.M.; Jaramaz, B. Ultrasound Registration of the Bone Surface for Surgical Navigation. Comput. Aided Surg. 2003, 8, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Besl, P.J.; McKay, N.D. Method for Registration of 3-D Shapes. In Sensor Fusion IV: Control Paradigms and Data Structures; International Society for Optics and Photonics: Bellingham, WA, USA, 1992; Volume 1611, pp. 586–607. [Google Scholar]
- Winter, S.; Brendel, B.; Pechlivanis, I.; Schmieder, K.; Igel, C. Registration of CT and Intraoperative 3-D Ultrasound Images of the Spine Using Evolutionary and Gradient-Based Methods. IEEE Trans. Evol. Comput. 2008, 12, 284–296. [Google Scholar] [CrossRef]
- Van Bergen, C.J.A.; Tuijthof, G.J.M.; Blankevoort, L.; Maas, M.; Kerkhoffs, G.M.M.J.; Van Dijk, C.N. Computed Tomography of the Ankle in Full Plantar Flexion: A Reliable Method for Preoperative Planning of Arthroscopic Access to Osteochondral Defects of the Talus. Arthrosc. J. Arthrosc. Relat. Surg. 2012, 28, 985–992. [Google Scholar] [CrossRef] [PubMed]
- Hacihaliloglu, I.; Rasoulian, A.; Rohling, R.N.; Abolmaesumi, P. Local Phase Tensor Features for 3-D Ultrasound to Statistical Shape+pose Spine Model Registration. IEEE Trans. Med. Imaging 2014, 33, 2167–2179. [Google Scholar] [CrossRef] [PubMed]
- Askeland, C.; Solberg, O.V.; Bakeng, J.B.L.; Reinertsen, I.; Tangen, G.A.; Hofstad, E.F.; Iversen, D.H.; Våpenstad, C.; Selbekk, T.; Langø, T.; et al. CustusX: An Open-Source Research Platform for Image-Guided Therapy. Int. J. Comput. Assist. Radiol. Surg. 2016, 11, 505–519. [Google Scholar] [CrossRef] [PubMed]
- Bø, L.E.; Hofstad, E.F.; Lindseth, F.; Hernes, T.A.N. Versatile Robotic Probe Calibration for Position Tracking in Ultrasound Imaging. Phys. Med. Biol. 2015, 60, 3499–3513. [Google Scholar] [CrossRef] [PubMed]
- Tümer, N.; Blankevoort, L.; Giessen, M.; Van De Terra, M.P.; Jong, P.A. De Weinans, H.; Tuijthof, G.J.M.; Zadpoor, A.A. Bone Shape Difference between Control and Osteochondral Defect Groups of the Ankle Joint. Osteoarthr. Cartil. 2016, 24, 2108–2115. [Google Scholar] [CrossRef] [PubMed]
- Anas, E.M.A.; Seitel, A.; Rasoulian, A.; John, P.S.; Ungi, T.; Lasso, A.; Darras, K.; Wilson, D.; Lessoway, V.A.; Fichtinger, G.; et al. Registration of a Statistical Model to Intraoperative Ultrasound for Scaphoid Screw Fixation. Int. J. Comput. Assist. Radiol. Surg. 2016, 11, 957–965. [Google Scholar] [CrossRef] [PubMed]
- Belaid, A.; Boukerroui, D.; Maingourd, Y.; Lerallut, J.; Member, S. Phase Based Level Set Segmentation of Ultrasound Images. IEEE Trans. Inf. Technol. Biomed. 2009, 15, 138–147. [Google Scholar] [CrossRef] [PubMed]
- Hacihaliloglu, I.; Abugharbieh, R.; Hodgson, A.J.; Rohling, R.N. Bone Surface Localization in Ultrasound Using Image Phase-Based Features. Ultrasound Med. Biol. 2009, 35, 1475–1487. [Google Scholar] [CrossRef] [PubMed]
- Shojaeilangari, S.; Yau, W.-Y.; Li, J.; Teoh, E.-K. Multi-Scale Analysis of Local Phase and Local Orientation for Dynamic Facial Expression Recognition. J. Multimed. Theory Appl. 2014, 1, 1–10. [Google Scholar] [CrossRef]
- Felsberg, M.; Sommer, G.; Felsberg, M.; Sommer, G. The Monogenic Signal. IEEE Trans. Image Process. 2001, 49, 3136–3144. [Google Scholar] [CrossRef]
- Anas, E.M.A.; Seitel, A.; Rasoulian, A.; John, P.S.; Pichora, D.; Darras, K.; Wilson, D.; Lessoway, V.A.; Hacihaliloglu, I.; Mousavi, P.; et al. Bone Enhancement in Ultrasound Using Local Spectrum Variations for Guiding Percutaneous Scaphoid Fracture Fixation Procedures. Int. J. Comput. Assist. Radiol. Surg. 2015, 10, 959–969. [Google Scholar] [CrossRef] [PubMed]
- Hansen, N.; Ostermeier, A. Completely Derandomized Self-Adaptation in Evolution Strategies. Evol. Comput. 2001, 9, 159–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kagadis, G.C.; Delibasis, K.K.; Matsopoulos, G.K.; Mouravliansky, N.A.; Asvestas, P.A.; Nikiforidis, G.C. A Comparative Study of Surface- and Volume-Based Techniques for the Automatic Registration between CT and SPECT Brain Images. Med. Phys. 2002, 29, 201–213. [Google Scholar] [CrossRef] [PubMed]
- Silva, L.; Bellon, O.R.P.; Boyer, K.L. Precision Range Image Registration Using a Robust Surface Interpenetration Measure and Enhanced Genetic Algorithms. IEEE Trans. Pattern Anal. Mach. Intell. 2005, 27, 762–776. [Google Scholar] [CrossRef] [PubMed]
- Van Bergen, C.J.A.; Tuijthof, G.J.M.; Maas, M.; Sierevelt, I.N.; van Dijk, C.N. Arthroscopic Accessibility of the Talus Quantified by Computed Tomography Simulation. Am. J. Sports Med. 2012, 40, 2318–2324. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| US Sweep | Number of Successful | Mean (and STD) (mm) | |
|---|---|---|---|
| Type | Registrations | diRMS | dfRMS |
| I | 99 | 6.96 (3.27) | 0.46 (0.17) |
| 80 | 7.50 (2.87) | 1.24 (0.62) | |
| 71 | 6.99 (2.49) | 1.80 (0.18) | |
| 65 | 8.72 (3.78) | 0.62 (0.28) | |
| 46 | 9.66 (4.66) | 0.51 (0.17) | |
| 39 | 7.43 (2.46) | 0.57 (0.35) | |
| 37 | 10.60 (3.79) | 0.70 (0.54) | |
| 35 | 6.97 (2.12) | 0.76 (0.68) | |
| 29 | 6.95 (2.73) | 0.57 (0.36) | |
| 24 | 10.04 (3.64) | 0.65 (0.67) | |
| 20 | 8.09 (2.66) | 0.81 (0.62) | |
| 1 | 7.04 (0.00) | 1.69 (0.00) | |
| II | 99 | 7.28 (3.06) | 0.66 (0.32) |
| 97 | 8.04 (3.45) | 0.93 (0.30) | |
| 91 | 8.55 (3.30) | 0.26 (0.41) | |
| 89 | 8.33 (3.42) | 1.21 (0.57) | |
| 78 | 8.55 (3.88) | 0.95 (0.36) | |
| 77 | 8.67 (3.66) | 0.43 (0.44) | |
| 76 | 7.35 (3.01) | 1.33 (0.14) | |
| 35 | 9.50 (2.95) | 0.82 (0.43) | |
| 28 | 7.97 (2.84) | 0.62 (0.45) | |
| 24 | 9.73 (3.96) | 0.64 (0.43) | |
| 16 | 9.41 (4.03) | 0.68 (0.35) | |
| 0 | - | - | |
| US Sweep | Number of Successful | Mean (and STD) (mm) |
|---|---|---|
| Type | Registrations | dfRMS |
| I | 100 | 0.31 (0.19) |
| 100 | 1.38 (0.28) | |
| 99 | 0.62 (0.33) | |
| 98 | 0.63 (0.26) | |
| 90 | 0.94 (0.47) | |
| 77 | 0.75 (0.29) | |
| 2 | 0.40 (0.33) | |
| 0 | - | |
| 0 | - | |
| 0 | - | |
| 0 | - | |
| 0 | - | |
| II | 100 | 0.35 (0.27) |
| 100 | 0.47 (0.29) | |
| 100 | 0.56 (0.20) | |
| 100 | 0.60 (0.25) | |
| 99 | 0.61 (0.32) | |
| 62 | 0.47 (0.36) | |
| 52 | 1.63 (0.18) | |
| 31 | 1.42 (0.41) | |
| 26 | 1.05 (0.32) | |
| 22 | 1.91 (0.08) | |
| 3 | 1.88 (0.06) | |
| 0 | - |
| Visible Talar Surface (% of the Total Talar Surface) | |||
|---|---|---|---|
| Lateral | Central | Medial | |
| Observer 1(1) | 55.3 (47.2–69.1) | 47.9 (42.3–58.2) | 51.7 (42.0–62.7) |
| Observer 1(2) | 55.4 (46.3–68.1) | 47.3 (38.2–59.0) | 52.4 (42.2–61.6) |
| Observer 2 | 53.6 (42.8–66.1) | 47.3 (36.8–60.0) | 51.4 (42.5–59.0) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tümer, N.; Kok, A.C.; Vos, F.M.; Streekstra, G.J.; Askeland, C.; Tuijthof, G.J.M.; Zadpoor, A.A. Three-Dimensional Registration of Freehand-Tracked Ultrasound to CT Images of the Talocrural Joint. Sensors 2018, 18, 2375. https://doi.org/10.3390/s18072375
Tümer N, Kok AC, Vos FM, Streekstra GJ, Askeland C, Tuijthof GJM, Zadpoor AA. Three-Dimensional Registration of Freehand-Tracked Ultrasound to CT Images of the Talocrural Joint. Sensors. 2018; 18(7):2375. https://doi.org/10.3390/s18072375
Chicago/Turabian StyleTümer, Nazlı, Aimee C. Kok, Frans M. Vos, Geert J. Streekstra, Christian Askeland, Gabrielle J. M. Tuijthof, and Amir A. Zadpoor. 2018. "Three-Dimensional Registration of Freehand-Tracked Ultrasound to CT Images of the Talocrural Joint" Sensors 18, no. 7: 2375. https://doi.org/10.3390/s18072375
APA StyleTümer, N., Kok, A. C., Vos, F. M., Streekstra, G. J., Askeland, C., Tuijthof, G. J. M., & Zadpoor, A. A. (2018). Three-Dimensional Registration of Freehand-Tracked Ultrasound to CT Images of the Talocrural Joint. Sensors, 18(7), 2375. https://doi.org/10.3390/s18072375