Myoelectric Signal Classification of Targeted Muscles Using Dictionary Learning


Abstract
:1. Introduction
2. Methods
2.1. Subjects
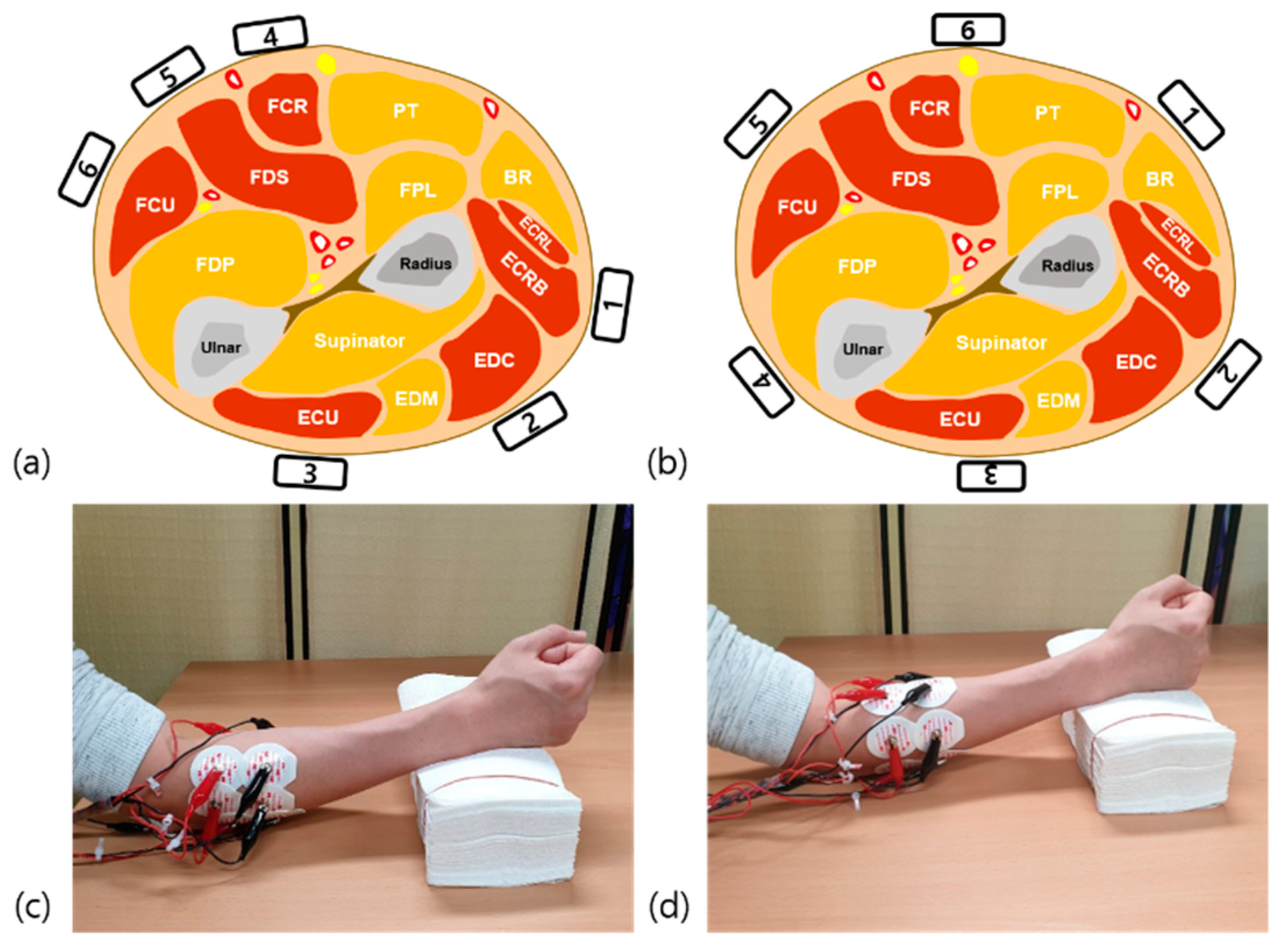
2.2. Electrode Configuration
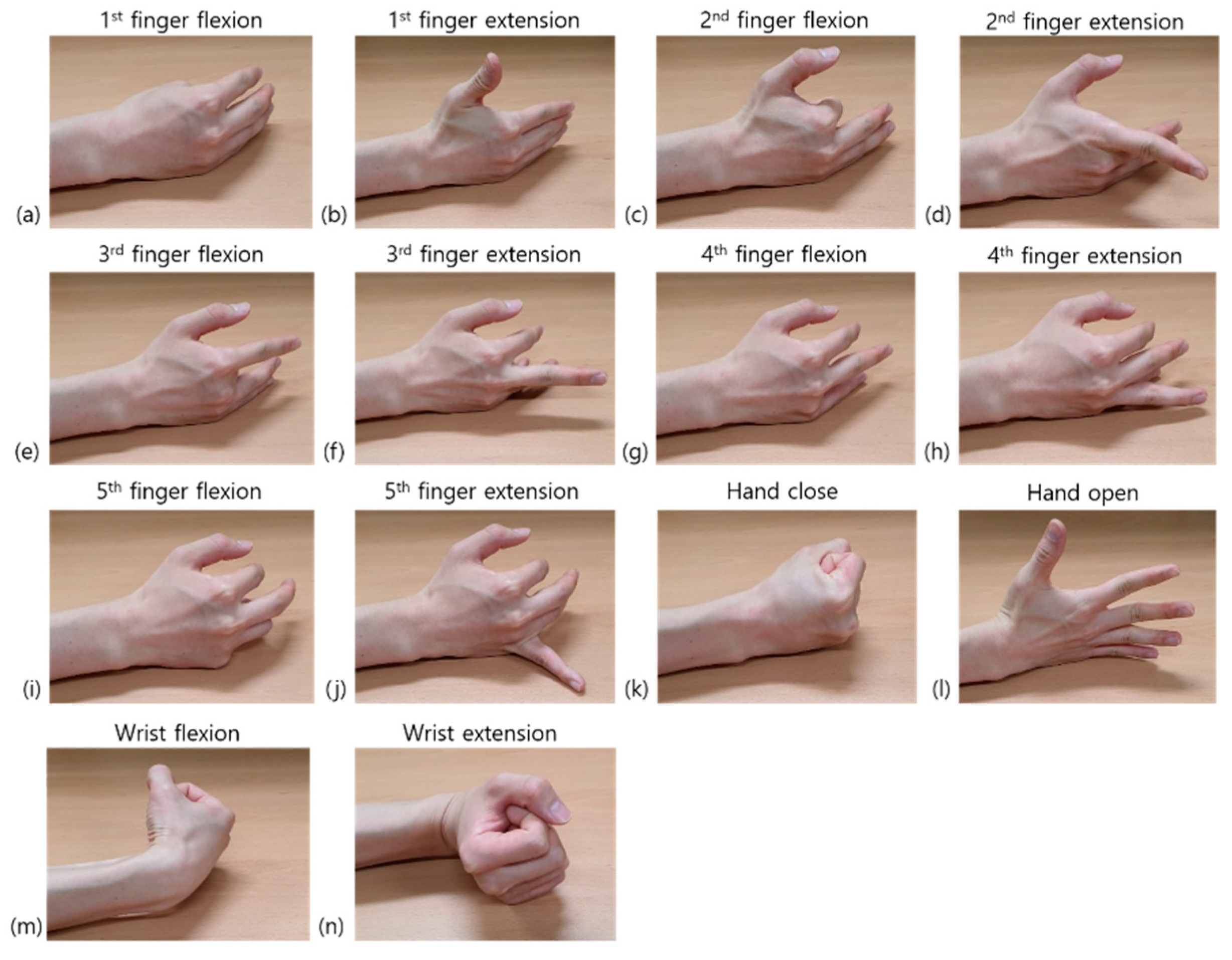
2.3. Experimental Protocol
2.4. Other Database
2.5. Acquisition Setup
2.6. EMG Signal Processing and Feature Extraction
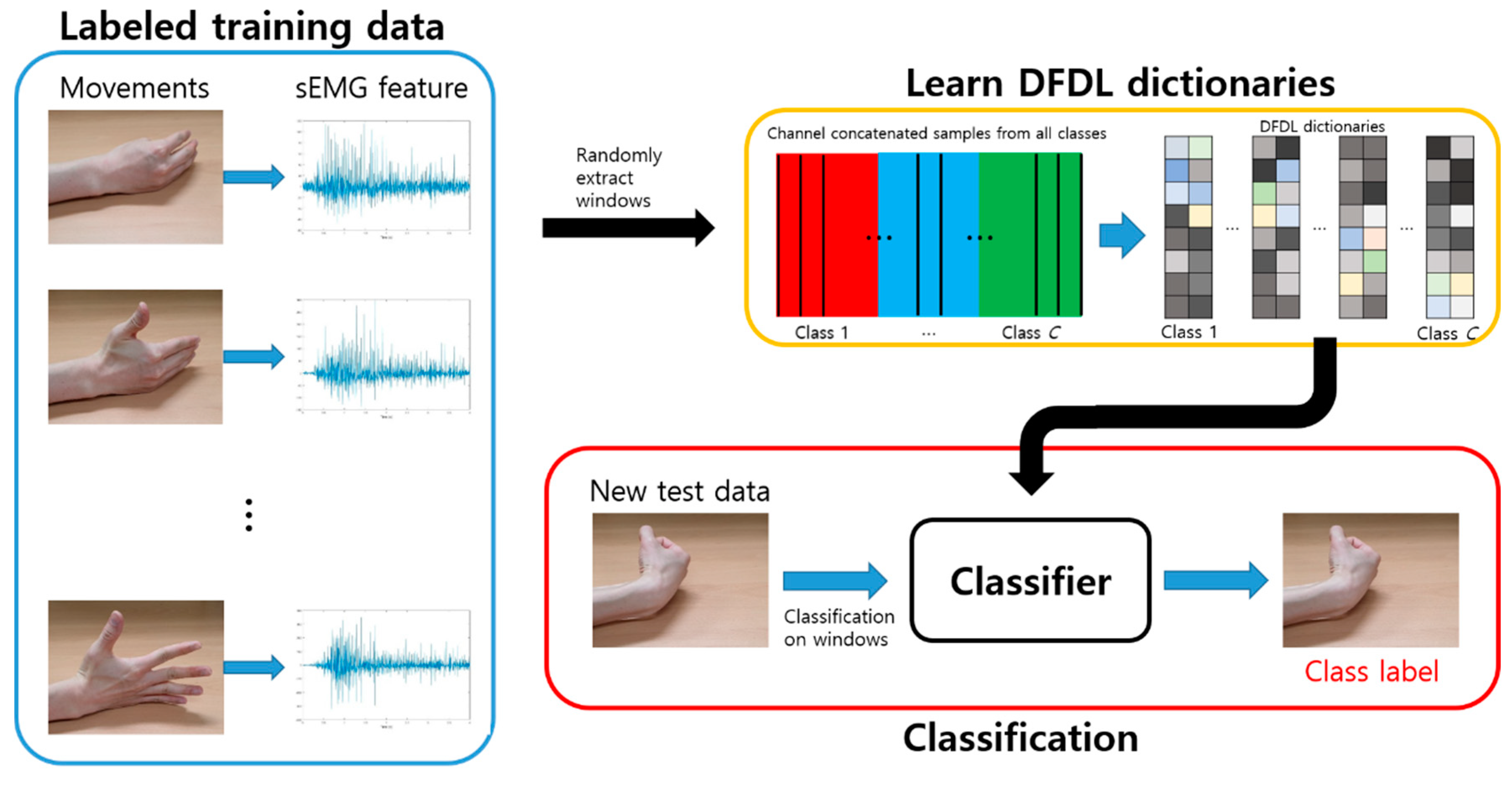
2.7. Classification
2.7.1. Discriminative Feature-Oriented Dictionary Learning
2.7.2. Classical Classifiers
2.8. Statistics
3. Results
3.1. Classification Results for the Healthy Volunteers
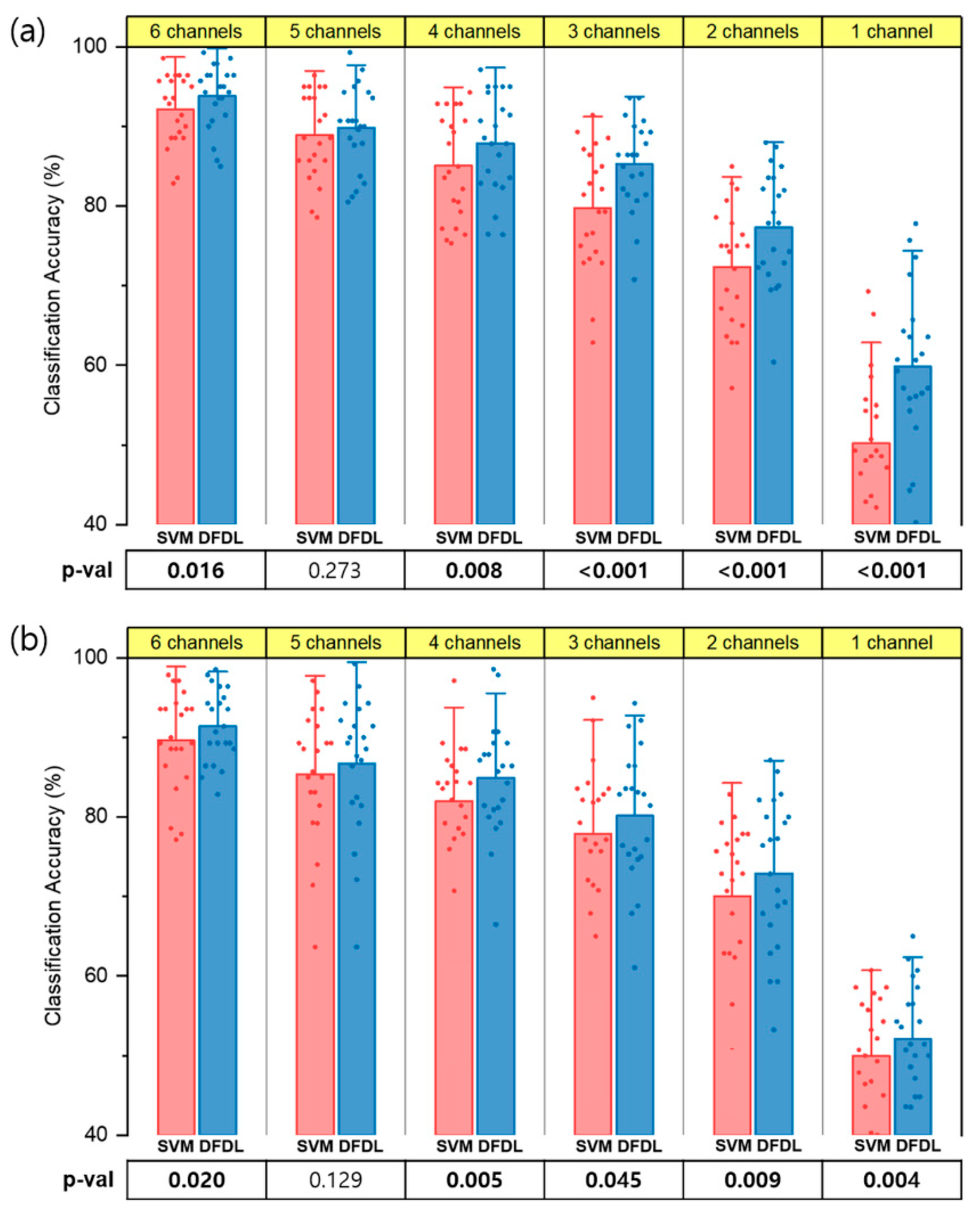
3.2. Comparison between DFDL and SVM
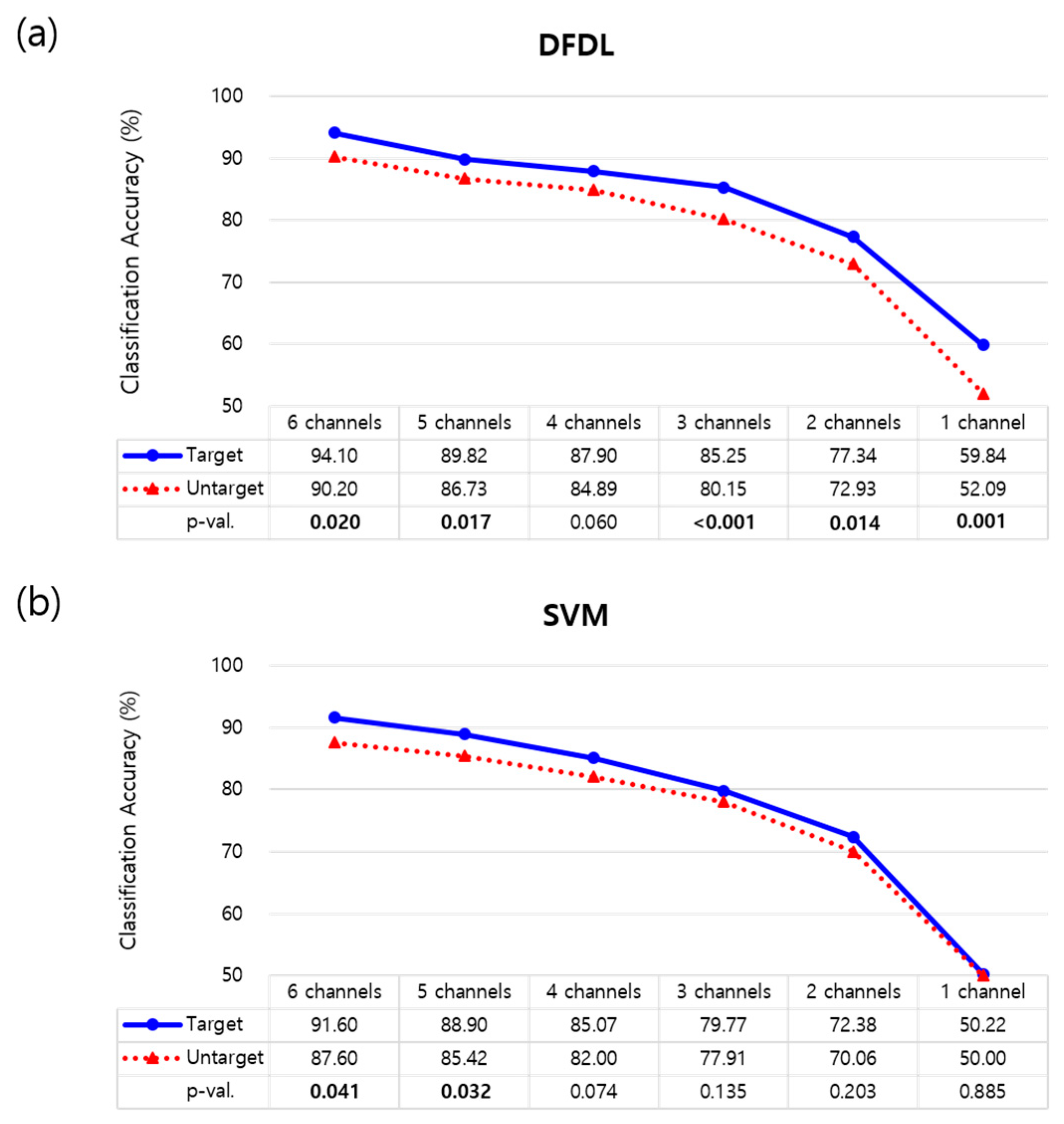
3.3. Effects of Number and Location of Electrodes
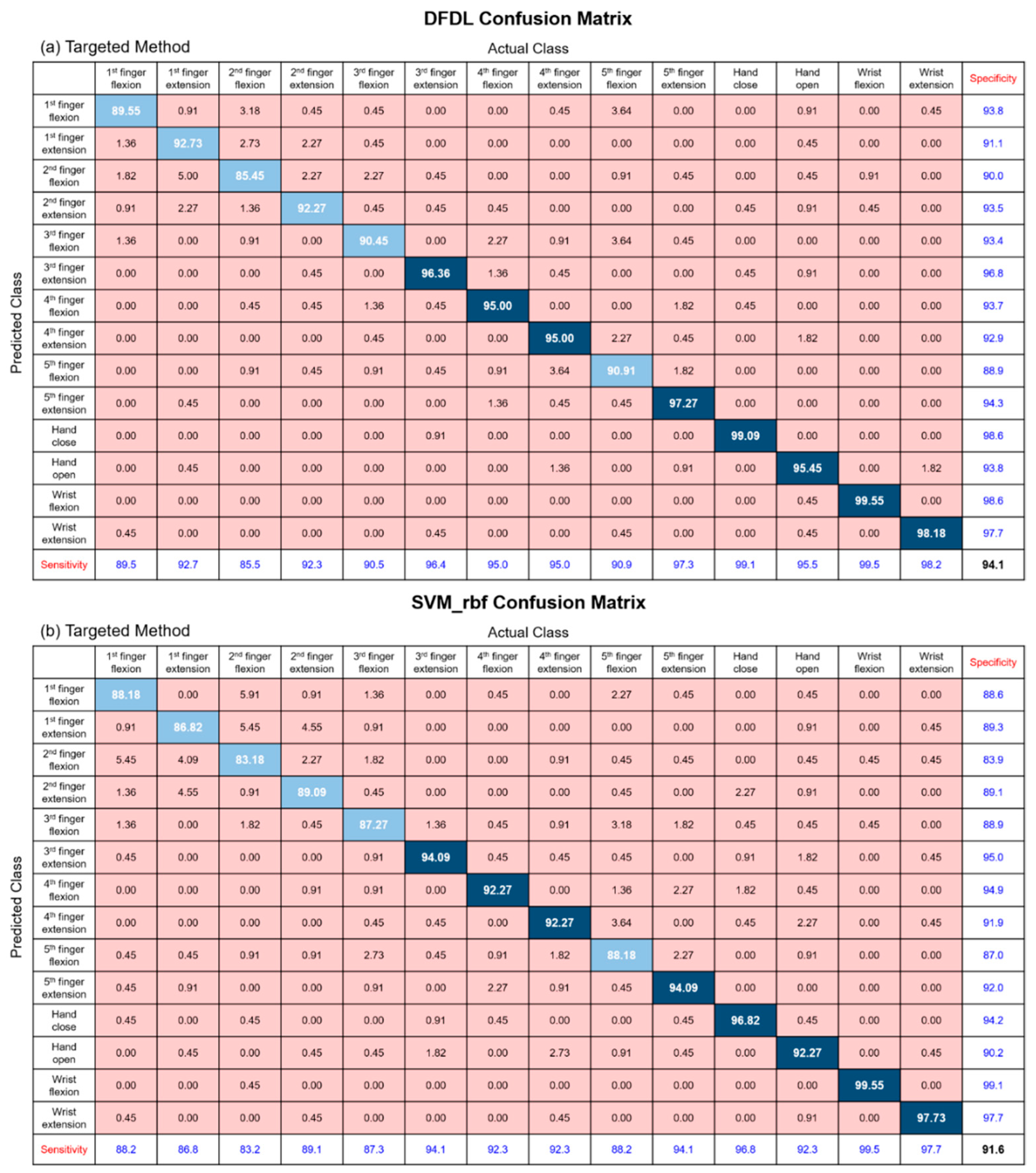
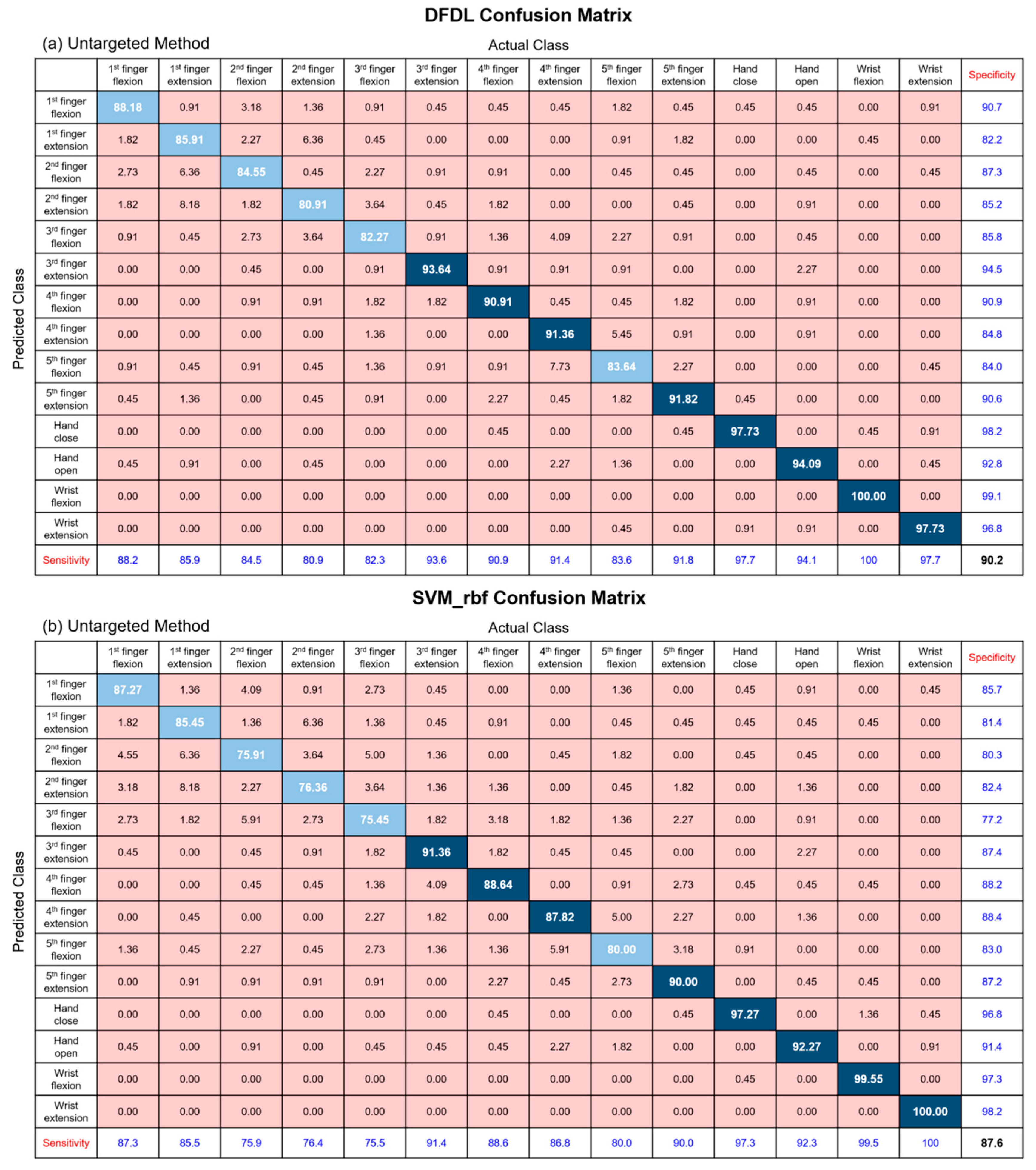
3.4. Classification Results of Each Class
3.5. Classification Results for Amputees
3.6. Classification Accuracy of Fewer Hand Movements
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| sEMG | Surface electromyography |
| DFDL | Discriminative feature-oriented dictionary learning |
| LDA | Linear discriminant analysis |
| SVM | Support vector machine |
| K-SVD | K-singular value decomposition |
| EEG | Electroencephalogram |
| LC-KSVD | Label consistent K-SVD |
| ECRL/B | Extensor carpi radialis longus and brevis |
| EDC | Extensor digitorum communis |
| ECU | Extensor carpi ulnaris |
| FCR | Flexor carpi radialis |
| FDS | Flexor digitorum superficialis |
| FDP | Flexor digitorum profundus |
| FCU | Flexor carpi ulnaris |
| NINAPRO | Non-Invasive Adaptive Prosthetics |
| DASH | Disabilities of the arm, shoulder, and hand |
| SVM_lin | Support vector machine with linear kernel |
| SVM_rbf | Support vector machine with radial basis function kernel |
| NB | Naïve Bayes classifier |
| RF | Random forests |
| KNN | k-nearest Neighbors |
| ANOVA | Analysis of variance |
References
- Myers, K.P.; VanDamme, T.; Pasquina, P.F. Rehabilitation of the Blast Injury Casualty with Amputation. In Managing Dismounted Complex Blast Injuries in Military & Civilian Settings; Springer: Berlin, Germany, 2018; pp. 225–239. [Google Scholar]
- Jensen, S.E.; Butt, Z.; Bill, A.; Baker, T.; Abecassis, M.M.; Heinemann, A.W.; Cella, D.; Dumanian, G.A. Quality of life considerations in upper limb transplantation: Review and future directions. J. Hand Surg. 2012, 37, 2126–2135. [Google Scholar] [CrossRef]
- Biddiss, E.A.; Chau, T.T. Upper limb prosthesis use and abandonment: A survey of the last 25 years. Prosthet. Orthot. Int. 2007, 31, 236–257. [Google Scholar] [CrossRef] [PubMed]
- Cifu, D.X. Braddom’s Physical Medicine and Rehabilitation, 5th ed.; Elsevier: Amsterdam, The Netherlands, 2016; pp. 167–189. [Google Scholar]
- Haig, A.; Gelblum, J.; Rechtien, J.; Gitter, A. Technology review: The use of surface EMG in the diagnosis and treatment of nerve and muscle disorders. Am. Assoc. Neuromuscul. Electrodiagn. Med. (AANEM) 1999, S239–S242. [Google Scholar]
- Hudgins, B.; Parker, P.; Scott, R.N. A new strategy for multifunction myoelectric control. IEEE Trans. Biomed. Eng. 1993, 40, 82–94. [Google Scholar] [CrossRef] [PubMed]
- Belter, J.T.; Segil, J.L.; Dollar, A.M.; Weir, R.F. Mechanical design and performance specifications of anthropomorphic prosthetic hands: A review. J. Rehabil. Res. Dev. 2013, 50, 599–618. [Google Scholar] [CrossRef]
- Lorrain, T.; Jiang, N.; Farina, D. Influence of the training set on the accuracy of surface EMG classification in dynamic contractions for the control of multifunction prostheses. J. Neuroeng. Rehabil. 2011, 8, 25. [Google Scholar] [CrossRef]
- Phinyomark, A.; Phukpattaranont, P.; Limsakul, C. Investigating long-term effects of feature extraction methods for continuous EMG pattern classification. Fluct. Noise Lett. 2012, 11, 1250028. [Google Scholar] [CrossRef]
- Ajiboye, A.B.; Weir, R.F. A heuristic fuzzy logic approach to EMG pattern recognition for multifunctional prosthesis control. IEEE Trans. Neural Syst. Rehabil. Eng. 2005, 13, 280–291. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Englehart, K.B.; Hudgins, B.; Chan, A.D. A Gaussian mixture model based classification scheme for myoelectric control of powered upper limb prostheses. IEEE Trans. Biomed. Eng. 2005, 52, 1801–1811. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.D.; Englehart, K.B. Continuous myoelectric control for powered prostheses using hidden Markov models. IEEE Trans. Biomed. Eng. 2005, 52, 121–124. [Google Scholar] [CrossRef]
- Geng, W.; Du, Y.; Jin, W.; Wei, W.; Hu, Y.; Li, J. Gesture recognition by instantaneous surface EMG images. Sci. Rep. 2016, 6, 36571. [Google Scholar] [CrossRef]
- Ison, M.; Vujaklija, I.; Whitsell, B.; Farina, D.; Artemiadis, P. High-density electromyography and motor skill learning for robust long-term control of a 7-DoF robot arm. IEEE Trans. Neural Syst. Rehabil. Eng. 2016, 24, 424–433. [Google Scholar] [CrossRef]
- Hargrove, L.J.; Englehart, K.; Hudgins, B. A comparison of surface and intramuscular myoelectric signal classification. IEEE Trans. Biomed. Eng. 2007, 54, 847–853. [Google Scholar] [CrossRef]
- Farrell, T.R. A comparison of the effects of electrode implantation and targeting on pattern classification accuracy for prosthesis control. IEEE Trans. Bio-Med. Eng. 2008, 55, 2198. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Li, B. Discriminative K-SVD for dictionary learning in face recognition. In Proceedings of the Computer Vision and Pattern Recognition (CVPR), San Francisco, CA, USA, 13–18 June 2010; pp. 2691–2698. [Google Scholar]
- Ma, L.; Wang, C.; Xiao, B.; Zhou, W. Sparse representation for face recognition based on discriminative low-rank dictionary learning. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Providence, RI, USA, 16–21 June 2012; pp. 2586–2593. [Google Scholar]
- Yang, M.; Zhang, L.; Feng, X.; Zhang, D. Fisher discrimination dictionary learning for sparse representation. In Proceedings of the IEEE International Conference on Computer Vision (ICCV), Barcelona, Spain, 6–13 November 2011; pp. 543–550. [Google Scholar]
- Vu, T.H.; Mousavi, H.S.; Monga, V.; Rao, G.; Rao, U.A. Histopathological image classification using discriminative feature-oriented dictionary learning. IEEE Trans. Med. Imaging 2016, 35, 738–751. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Zhang, L.; Feng, X.; Zhang, D. Sparse representation based fisher discrimination dictionary learning for image classification. Int. J. Comput. Vis. 2014, 109, 209–232. [Google Scholar] [CrossRef]
- Shin, Y.; Lee, S.; Ahn, M.; Cho, H.; Jun, S.C.; Lee, H.-N. Noise robustness analysis of sparse representation based classification method for non-stationary EEG signal classification. Biomed. Signal Process. Control 2015, 21, 8–18. [Google Scholar] [CrossRef]
- Zhou, W.; Yang, Y.; Yu, Z. Discriminative dictionary learning for EEG signal classification in Brain-computer interface. In Proceedings of the 12th International Conference on Control Automation Robotics & Vision (ICARCV), Guangzhou, China, 5–7 December 2012; pp. 1582–1585. [Google Scholar]
- Ameri, R.; Pouyan, A.; Abolghasemi, V. Projective dictionary pair learning for EEG signal classification in brain computer interface applications. Neurocomputing 2016, 218, 382–389. [Google Scholar] [CrossRef]
- Liu, T.; Si, Y.; Wen, D.; Zang, M.; Lang, L. Dictionary learning for VQ feature extraction in ECG beats classification. Expert Syst. Appl. 2016, 53, 129–137. [Google Scholar] [CrossRef]
- Al-Timemy, A.H.; Bugmann, G.; Escudero, J.; Outram, N. Classification of finger movements for the dexterous hand prosthesis control with surface electromyography. IEEE J. Biomed. Health Inform. 2013, 17, 608–618. [Google Scholar] [CrossRef]
- Stegeman, D.; Hermens, H. Standards for Surface Electromyography: The European Project Surface EMG for Non-Invasive Assessment of Muscles (SENIAM); Roessingh Research and Development: Enschede, The Netherlands, 2007; pp. 108–112. [Google Scholar]
- Hang, J.; Lee, J.A.D. Manual of Nerve Conduction Study and Surface Anatomy for Needle Electromyography; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2005. [Google Scholar]
- Pylatiuk, C.; Schulz, S.; Döderlein, L. Results of an Internet survey of myoelectric prosthetic hand users. Prosthet. Orthot. Int. 2007, 31, 362–370. [Google Scholar] [CrossRef]
- Atzori, M.; Gijsberts, A.; Kuzborskij, I.; Elsig, S.; Hager, A.-G.M.; Deriaz, O.; Castellini, C.; Müller, H.; Caputo, B. Characterization of a benchmark database for myoelectric movement classification. IEEE Trans. Neural Syst. Rehabil. Eng. 2015, 23, 73–83. [Google Scholar] [CrossRef]
- Zhai, X.; Jelfs, B.; Chan, R.H.; Tin, C. Self-recalibrating surface EMG pattern recognition for neuroprosthesis control based on convolutional neural network. Front. Neurosci. 2017, 11, 379. [Google Scholar] [CrossRef]
- Atzori, M.; Gijsberts, A.; Castellini, C.; Caputo, B.; Mittaz Hager, A.-G.; Elsig, S.; Giatsidis, G.; Bassetto, F.; Müller, H. Effect of clinical parameters on the control of myoelectric robotic prosthetic hands. J. Rehabil. Res. Dev. 2016, 53, 345–358. [Google Scholar] [CrossRef]
- Chen, X.; Wang, Z.J. Pattern recognition of number gestures based on a wireless surface EMG system. Biomed. Signal Process. Control 2013, 8, 184–192. [Google Scholar] [CrossRef]
- Zardoshti-Kermani, M.; Wheeler, B.C.; Badie, K.; Hashemi, R.M. EMG feature evaluation for movement control of upper extremity prostheses. IEEE Trans. Rehabil. Eng. 1995, 3, 324–333. [Google Scholar] [CrossRef]
- Phinyomark, A.; Phukpattaranont, P.; Limsakul, C. Feature reduction and selection for EMG signal classification. Expert Syst. Appl. 2012, 39, 7420–7431. [Google Scholar] [CrossRef]
- Khushaba, R.N.; Al-Jumaily, A.; Al-Ani, A. Novel feature extraction method based on fuzzy entropy and wavelet packet transform for myoelectric Control. In Proceedings of the International Symposium on Communications and Information Technologies, Sydney, NSW, Australia, 17–19 October 2007; pp. 352–357. [Google Scholar]
- Khushaba, R.N.; Kodagoda, S.; Lal, S.; Dissanayake, G. Driver drowsiness classification using fuzzy wavelet-packet-based feature-extraction algorithm. IEEE Trans. Biomed. Eng. 2011, 58, 121–131. [Google Scholar] [CrossRef]
- Yuan, X.-T.; Liu, X.; Yan, S. Visual classification with multitask joint sparse representation. IEEE Trans. Image Process. 2012, 21, 4349–4360. [Google Scholar] [CrossRef]
- Dong, W.; Zhang, L.; Shi, G.; Li, X. Nonlocally centralized sparse representation for image restoration. IEEE Trans. Image Process. 2013, 22, 1620–1630. [Google Scholar] [CrossRef]
- Mairal, J.; Bach, F.; Ponce, J.; Sapiro, G. Online learning for matrix factorization and sparse coding. J. Mach. Learn. Res. 2010, 11, 19–60. [Google Scholar]
- Mairal, J.; Bach, F.; Ponce, J.; Sapiro, G.; Jenatton, R.; Obozinski, G. SPAMS: A SPArse Modeling Software, v2. 3. 2014. Available online: http://spams-devel.gforge.inria.fr/downloads.html (accessed on 1 November 2018).
- Riillo, F.; Quitadamo, L.R.; Cavrini, F.; Gruppioni, E.; Pinto, C.A.; Pastò, N.C.; Sbernini, L.; Albero, L.; Saggio, G. Optimization of EMG-based hand gesture recognition: Supervised vs. unsupervised data preprocessing on healthy subjects and transradial amputees. Biomed. Signal Process. Control 2014, 14, 117–125. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Ma, Y. Application of supervised machine learning algorithms in the classification of sagittal gait patterns of cerebral palsy children with spastic diplegia. Comput. Biol. Med. 2019, 106, 33–39. [Google Scholar] [CrossRef]
- Standring, S.; Borley, N.R.; Gray, H. Gray’s Anatomy: The Anatomical Basis of Clinical Practice, 40th ed.; Churchill Livingstone/Elsevier: London, UK, 2008. [Google Scholar]
- Young, A.J.; Hargrove, L.J.; Kuiken, T.A. Improving myoelectric pattern recognition robustness to electrode shift by changing interelectrode distance and electrode configuration. IEEE Trans. Biomed. Eng. 2012, 59, 645–652. [Google Scholar] [CrossRef]
- Li, H.; Xu, S.; Yang, P.; Chen, L. A research and design on surface emg amplifier. In Proceedings of the International Conference on Measuring Technology and Mechatronics Automation (ICMTMA), Changsha, China, 13–14 March 2010; pp. 306–309. [Google Scholar]
- Gerdle, B.; Karlsson, S.; Day, S.; Djupsjöbacka, M. Acquisition, processing and analysis of the surface electromyogram. In Modern Techniques in Neuroscience Research; Springer: Berlin, Germany, 1999; pp. 705–755. [Google Scholar]
- Phinyomark, A.; Phukpattaranont, P.; Limsakul, C. A review of control methods for electric power wheelchairs based on electromyography signals with special emphasis on pattern recognition. IETE Tech. Rev. 2011, 28, 316–326. [Google Scholar] [CrossRef]
- Jang, G.; Kim, J.; Lee, S.; Choi, Y. EMG-based continuous control scheme with simple classifier for electric-powered wheelchair. IEEE Trans. Ind. Electron. 2016, 63, 3695–3705. [Google Scholar] [CrossRef]
- Hamedi, M.; Salleh, S.-H.; Astaraki, M.; Noor, A.M. EMG-based facial gesture recognition through versatile elliptic basis function neural network. Biomed. Eng. Online 2013, 12, 73. [Google Scholar] [CrossRef]
- Gu, S.; Zhang, L.; Zuo, W.; Feng, X. Projective dictionary pair learning for pattern classification. In Proceedings of the Advances in Neural Information Processing Systems, Montreal, Canada, 8–13 December 2014; pp. 793–801. [Google Scholar]
- Xia, P.; Hu, J.; Peng, Y. EMG—Based estimation of limb movement using deep learning with recurrent convolutional neural networks. Artif. Organs 2018, 42, e67–e77. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SVM_rbf | SVM_lin | LDA | KNN | NB | RF | DFDL | |
|---|---|---|---|---|---|---|---|
| Targeted Method | |||||||
| Acc (%) | 91.6 | 90.6 | 69.9 | 90.4 | 73.2 | 62.1 | 94.1 |
| p-val | 0.343 | 0.018 | 0.000 | 0.001 | 0.000 | 0.000 | |
| Untargeted Methods | |||||||
| Acc (%) | 87.6 | 86.5 | 65.7 | 86.0 | 66.0 | 60.4 | 90.2 |
| p-val | 0.414 | 0.047 | 0.000 | 0.020 | 0.000 | 0.000 | |
| SVM_rbf | SVM_lin | LDA | KNN | NB | RF | DFDL | |
|---|---|---|---|---|---|---|---|
| Acc (%) | 62.3 | 60.7 | 35.8 | 55.5 | 35.6 | 24.6 | 65.1 |
| p-val | 0.736 | 0.292 | 0.000 | 0.002 | 0.000 | 0.000 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoo, H.-J.; Park, H.-j.; Lee, B. Myoelectric Signal Classification of Targeted Muscles Using Dictionary Learning. Sensors 2019, 19, 2370. https://doi.org/10.3390/s19102370
Yoo H-J, Park H-j, Lee B. Myoelectric Signal Classification of Targeted Muscles Using Dictionary Learning. Sensors. 2019; 19(10):2370. https://doi.org/10.3390/s19102370
Chicago/Turabian StyleYoo, Hyun-Joon, Hyeong-jun Park, and Boreom Lee. 2019. "Myoelectric Signal Classification of Targeted Muscles Using Dictionary Learning" Sensors 19, no. 10: 2370. https://doi.org/10.3390/s19102370
APA StyleYoo, H. -J., Park, H. -j., & Lee, B. (2019). Myoelectric Signal Classification of Targeted Muscles Using Dictionary Learning. Sensors, 19(10), 2370. https://doi.org/10.3390/s19102370