Paraspinal Muscle Segmentation Based on Deep Neural Network

Abstract
:1. Introduction
2. Methods
2.1. Preprocessing
2.2. Residual Module
2.3. Feature Pyramid Attention Module
2.4. Network Architecture
3. Experiment and Results
3.1. Dataset
3.2. Implementation Details
3.3. Evaluation Criteria
- Dice similarity coefficient (DSC):
- True negative rate/specificity (TNR):
- True positive rate/sensitivity (TPR):
- Hausdorff distance (HD):where and denote the pixel sets of the manually labeled ground truth and automatically segmented muscle, respectively. DSC measures the overlap of the segmentation with the ground truth, while specificity reflects the miss rate, sensitivity reflects the mistake rate and HD is the maximum distance from all the minimum distances between the boundaries of the ground truth and segmentation. For DSC, TNR, and TPR, the larger the value, the better the performance, while for HD, the smaller the value, the better the performance.
3.4. Modules Analysis by Intra-Comparison
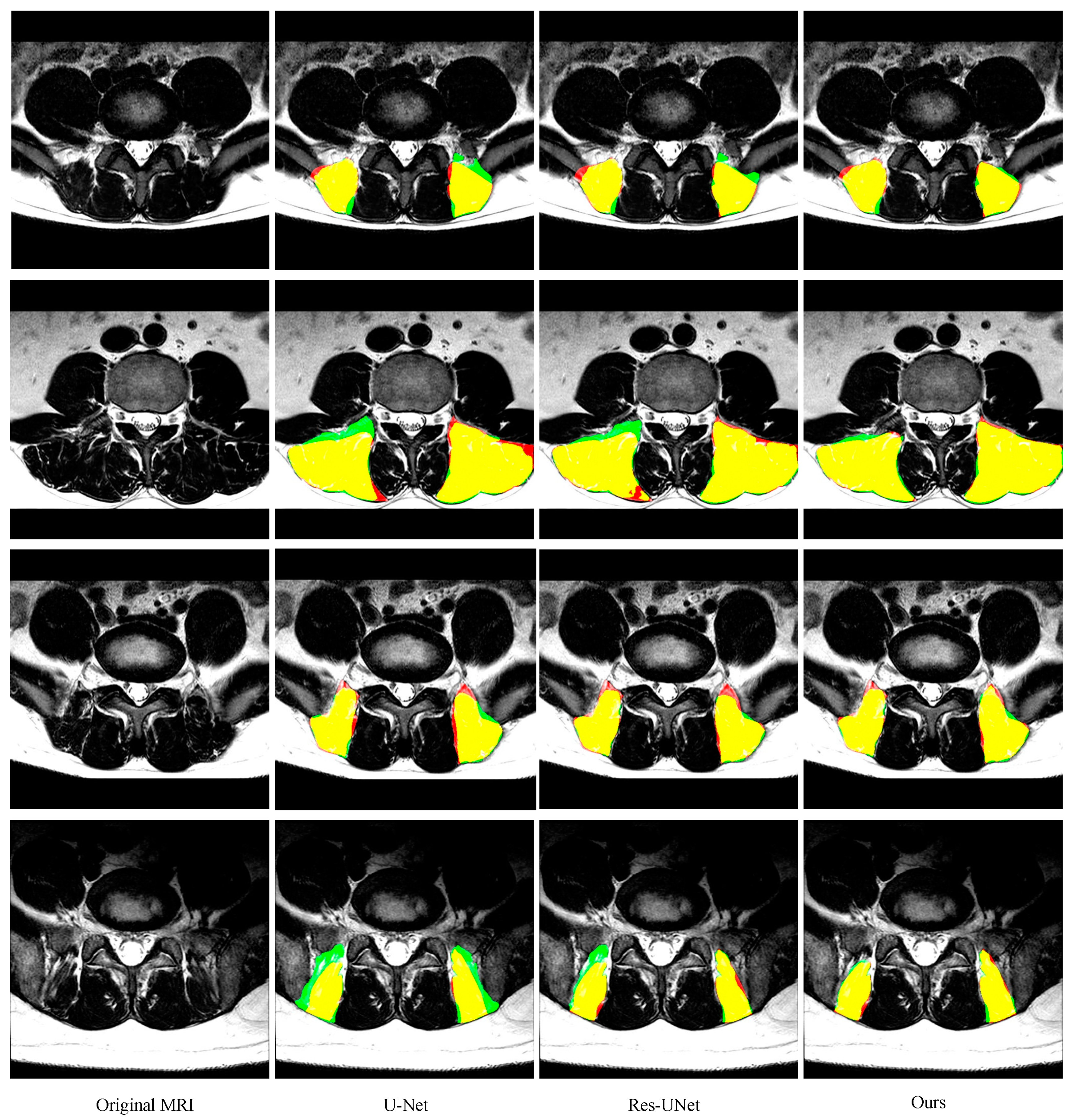
3.5. Comparison with other State-of-the-Art Methods
3.6. Muscle CSA Measurements
4. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Ward, S.R.; Kim, C.W.; Eng, C.M.; Gottschalk, L.J.; Tomiya, A.; Garfin, S.R. Architectural analysis and intraoperative measurements demonstrate the unique design of the multifidus muscle for lumbar spine stability. J. Bone Joint Surg. Am. 2009, 91, 176–185. [Google Scholar] [CrossRef] [PubMed]
- Fortin, M.; Lazáry, A.; Varga, P.P.; Battié, M.C. Association between paraspinal muscle morphology clinical symptoms and functional status in patients with lumbar spinal stenosis. Eur. Spine J. 2017, 26, 2543–2551. [Google Scholar] [CrossRef] [PubMed]
- Teichtahl, A.J.; Urquhart, D.M.; Wang, Y.; Wluka, A.E.; Wijethilake, P.; O’Sullivan, R.; Cicuttini, F.M. Fat infltration of paraspinal muscles is associated with low back pain, disability, and structural abnormalities in community-based adults. Spine J. 2015, 15, 1593–1601. [Google Scholar] [CrossRef] [PubMed]
- Takayama, K.; Kita, T.; Nakamura, H.; Kanematsu, F.; Yasunami, T.; Sakanaka, H. New predictive index for lumbar paraspinal muscle degeneration associated with aging. Spine 2016, 41, E84–E90. [Google Scholar] [CrossRef] [PubMed]
- Shahidi, B.; Parra, C.L.; Berry, D.B.; Hubbard, J.C.; Gombatto, S.; Zlomislic, V. Contribution of lumbar spine pathology and age to paraspinal muscle size and fatty infiltration. Spine 2017, 42, 616–623. [Google Scholar] [CrossRef] [PubMed]
- Jun, H.S.; Kim, J.H.; Ahn, J.H.; Chang, I.B.; Song, J.H.; Kim, T.H. The effect of lumbar spinal muscle on spinal sagittal alignment. Neurosurgery 2016, 79, 847–855. [Google Scholar] [CrossRef] [PubMed]
- Ranson, C.A.; Burnett, A.F.; Kerslake, R. An investigation into the use of MR imaging to determine the functional cross sectional area of lumbar paraspinal muscles. Eur. Spine J. 2006, 15, 764–773. [Google Scholar] [CrossRef] [PubMed]
- Engstrom, C.M.; Fripp, J.; Jurcak, V. Segmentation of the quadratus lumborum muscle using statistical shape modeling. J. Magn. Reson. Imaging 2011, 33, 1422–1429. [Google Scholar] [CrossRef]
- Hu, Z.J.; He, J.; Zhao, F.D. An assessment of the intra- and inter-reliability of the lumbar paraspinal muscle parameters using CT scan and magnetic resonance imaging. Spine 2011, 36, E868–E874. [Google Scholar] [CrossRef]
- Fortin, M.; Omidyeganeh, M.; Battié, M.C.; Ahmad, O.; Rivaz, H. Evaluation of an automated thresholding algorithm for the quantification of paraspinal muscle composition from MRI images. BioMed. Eng. OnLine 2017, 16. [Google Scholar] [CrossRef]
- Crawford, R.J.; Cornwall, J.; Abbott, R. Manually defining regions of interest when quantifying paravertebral muscles fatty infiltration from axial magnetic resonance imaging: A proposed method for the lumbar spine with anatomical cross-reference. BMC Musculoskelet. Disord. 2017, 18, 25. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, R.J.; Harding, P.J.; Loram, I.D. Real-time ultrasound segmentation, analysis and visualisation of deep cervical muscle structure. IEEE Trans. Med. Imaging 2017, 36, 653–665. [Google Scholar] [CrossRef] [PubMed]
- Berry, D.B.; Padwal, J.; Johnson, S. Methodological considerations in region of interest definitions for paraspinal muscles in axial MRIs of the lumbar spine. BMC Musculoskelet. Disord. 2018, 19, 135. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Y.; Fortin, M.; Battié, M.C. Population-averaged MRI atlases for automated image processing and assessments of lumbar paraspinal muscles. Eur. Spine J. 2018, 27, 2442–2448. [Google Scholar] [CrossRef] [PubMed]
- Long, J.; Shelhamer, E.; Darrell, T. Fully convolutional networks for semantic segmentation. IEEE Trans. Pattern Anal. Mach. Intell. 2014, 39, 640–651. [Google Scholar]
- Ronneberger, O.; Fischer, P.; Brox, T. U-net: Convolutional networks for biomedical image segmentation. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Granada, Spain, 16–20 September 2015. [Google Scholar]
- Dong, S.; Luo, G.; Wang, K.; Cao, S.; Li, Q.; Zhang, H. A Combined Fully Convolutional Networks and Deformable Model for Automatic Left Ventricle Segmentation Based on 3D Echocardiography. BioMed. Res. Int. 2018, 2018, 5682365. [Google Scholar] [CrossRef]
- Tran, P.V. A fully convolutional neural network for cardiac segmentation in short-axis MRI. arXiv 2016, arXiv:1604.00494. [Google Scholar]
- Wenjia, B.; Matthew, S.; Giacomo, T.; Ozan, O.; Martin, R.; Ghislain, V.; Aaron, M.L.; Nay, A.; Elena, L.; Mihir, M.S.; et al. Automated cardiovascular magnetic resonance image analysis with fully convolutional networks. J. Cardiovasc. Magn. Reson. 2018, 20, 65. [Google Scholar]
- Nie, D.; Wang, L.; Gao, Y.; Shen, D. Fully convolutional networks for multi-modality isointense infant brain image segmentation. In Proceedings of the 13th International Symposium on Biomedical Imaging (ISBI), Prague, Czech Republic, 13–16 April 2016. [Google Scholar]
- Shakeri, M.; Tsogkas, S.; Ferrante, E.; Lippe, S.; Kadoury, S.; Paragios, N.; Kokkinos, I. Sub-cortical brain structure segmentation using F-CNN’s. In Proceedings of the 13th International Symposium on Biomedical Imaging (ISBI), Prague, Czech Republic, 13–16 April 2016. [Google Scholar]
- Ghafoorian, M.; Karssemeijer, N.; Heskes, T.; Bergkamp, M.; Wissink, J.; Obels, J.; Keizer, K.; de Leeuw, F.-E.; van Ginneken, B.; Marchiori, E.; et al. Deep multi-scale location-aware 3D convolutional neural networks for automated detection of lacunes of presumed vascular origin. NeuroImage Clin. 2017, 14, 391–399. [Google Scholar] [CrossRef] [PubMed]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Identity mappings in deep residual networks. In Proceedings of the European Conference on Computer Vision, Munich, Germany, 8–14 September 2016. [Google Scholar]
- Li, H.; Xiong, P.; An, J.; Wang, L. Pyramid attention network for semantic segmentation. arXiv 2018, arXiv:1805.10180. [Google Scholar]
- Zhao, H.; Shi, J.; Qi, X.; Wang, X.; Jia, J. Pyramid scene parsing network. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 22–26 July 2016. [Google Scholar]
- Milletari, F.; Navab, N.; Ahmadi, S.A. V-net: Fully convolutional neural networks for volumetric medical image segmentation. In Proceedings of the Fourth International Conference on 3D Vision (3DV), Stanford, CA, USA, 25–28 October 2016. [Google Scholar]
- Badrinarayanan, V.; Kendall, A.; Cipolla, R. Segnet: A deep convolutional encoder-decoder architecture for scene segmentation. IEEE Trans. Pattern Anal. Mach. Intell. 2017, 39, 2481–2495. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.C.; Zhu, Y.; Papandreou, G.; Schroff, F.; Adam, H. Encoder-decoder with atrous separable convolution for semantic image segmentation. In Proceedings of the European Conference on Computer Vision (ECCV), Munich, Germany, 8–14 September 2018. [Google Scholar]
- Bland, J.M.; Altman, D.G. Measuring agreement in method comparison studies. Stat. Methods Med. Res. 1999, 8, 135–169. [Google Scholar] [CrossRef] [PubMed]
- Bland, J.M.; Altman, D. Statistical method for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Method | DSC | Sensitivity | Specificity | HD (mm) |
|---|---|---|---|---|
| FCN | 0.908 ± 0.057 | 0.925 ± 0.069 | 0.878 ± 0.057 | 10.76 ± 10.0 |
| SegNet | 0.938 ± 0.038 | 0.949 ± 0.472 | 0.930 ± 0.052 | 7.51 ± 8.29 |
| PSPNet | 0.936 ± 0.036 | 0.931 ± 0.043 | 0.944 ± 0.053 | 5.19 ± 3.84 |
| DeepLabv3+ | 0.943 ± 0.035 | 0.940 ± 0.042 | 0.947 ± 0.044 | 5.02 ± 3.89 |
| U-Net | 0.921 ± 0.039 | 0.925 ± 0.049 | 0.920 ± 0.056 | 6.16 ± 5.14 |
| ResU-Net | 0.944 ± 0.043 | 0.946 ± 0.063 | 0.945 ± 0.045 | 4.68 ± 3.25 |
| Ours | 0.949 ± 0.034 | 0.951 ± 0.046 | 0.950 ± 0.035 | 4.62 ± 2.81 |
| Method | DSC | Sensitivity | Specificity | HD (mm) |
|---|---|---|---|---|
| FCN | 0.873 ± 0.079 | 0.865 ± 0.075 | 0.892 ± 0.111 | 15.24 ± 14.85 |
| SegNet | 0.904 ± 0.082 | 0.918 ± 0.096 | 0.901 ± 0.092 | 9.9 ± 9.85 |
| PSPNet | 0.901 ± 0.081 | 0.90.1 ±0.089 | 0.915 ± 0.098 | 8.46 ± 6.55 |
| DeepLabv3+ | 0.908 ± 0.077 | 0.919 ± 0.075 | 0.908 ± 0.10 | 8.19 ± 5.92 |
| U-Net | 0.895 ± 0.080 | 0.917 ± 0.086 | 0.887 ± 0.105 | 9.75 ± 8.72 |
| ResU-Net | 0.905 ± 0.092 | 0.915 ± 0.102 | 0.902 ± 0.109 | 8.86 ± 8.42 |
| Ours | 0.913 ± 0.082 | 0.920 ± 0.100 | 0.919 ± 0.073 | 7.89 ± 5.61 |
| Method | FCN | SegNet | PSPNet | DeepLabv3+ | U-Net | ResU-Net | Ours |
|---|---|---|---|---|---|---|---|
| Parameter | 10.9M | 29.4M | 11.2M | 41M | 28.8M | 5.1M | 5.0M |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, H.; Luo, H.; Liu, Y. Paraspinal Muscle Segmentation Based on Deep Neural Network. Sensors 2019, 19, 2650. https://doi.org/10.3390/s19122650
Li H, Luo H, Liu Y. Paraspinal Muscle Segmentation Based on Deep Neural Network. Sensors. 2019; 19(12):2650. https://doi.org/10.3390/s19122650
Chicago/Turabian StyleLi, Haixing, Haibo Luo, and Yunpeng Liu. 2019. "Paraspinal Muscle Segmentation Based on Deep Neural Network" Sensors 19, no. 12: 2650. https://doi.org/10.3390/s19122650
APA StyleLi, H., Luo, H., & Liu, Y. (2019). Paraspinal Muscle Segmentation Based on Deep Neural Network. Sensors, 19(12), 2650. https://doi.org/10.3390/s19122650