Gait Phase Detection for Lower-Limb Exoskeletons using Foot Motion Data from a Single Inertial Measurement Unit in Hemiparetic Individuals


Abstract
:1. Introduction
2. Related Works
3. Materials and Methods
3.1. Theoretical Approach
3.1.1. Classification Using a Threshold-Based Detection Algorithm
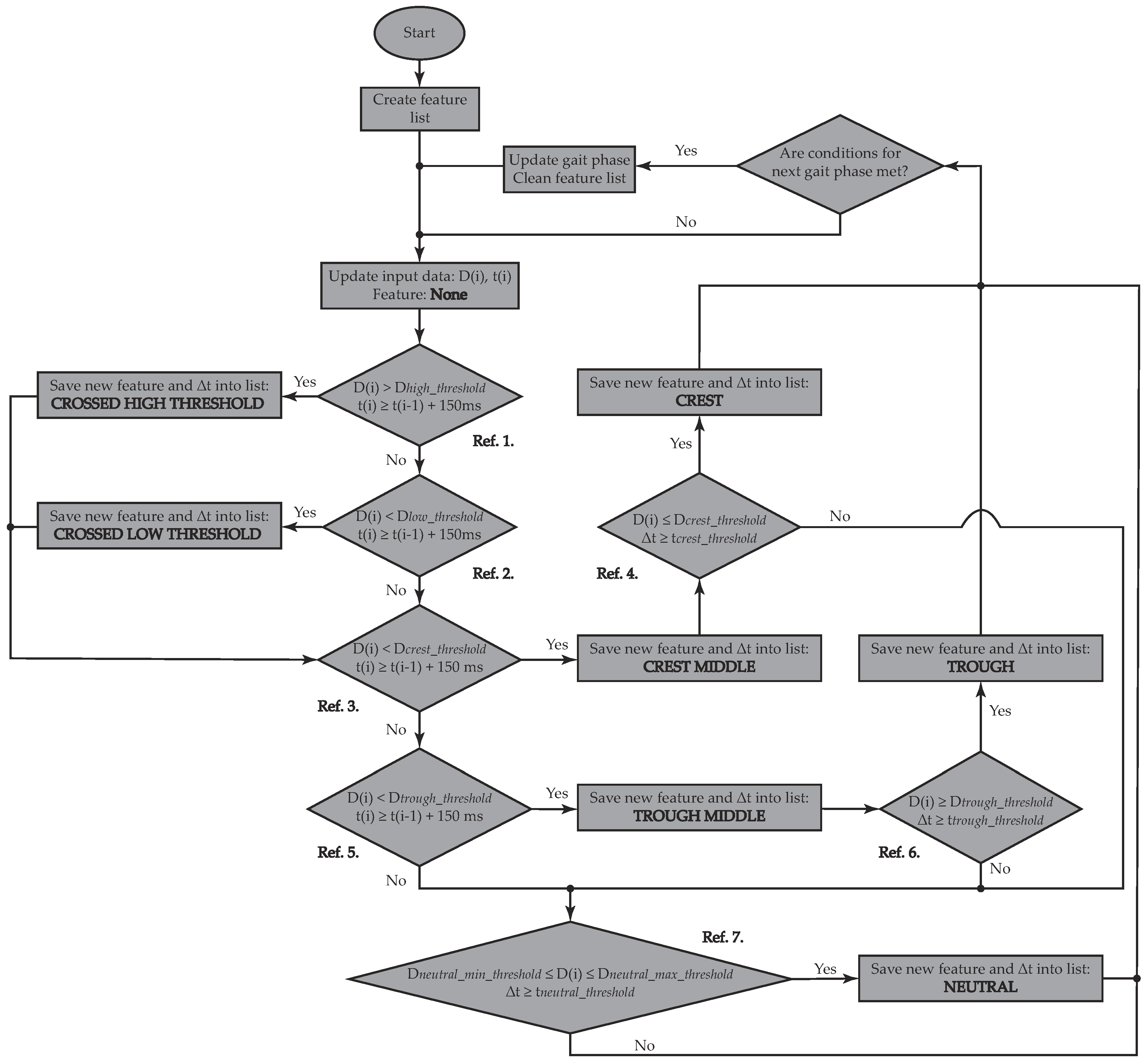
- Crossed High Threshold (Ref. 1 in Figure 1): Current data () should be higher than a pre-specified threshold () and at least 150 ms should have passed since the last saved feature. The time difference between features () is saved, along with the spotted feature into the feature list.
- Crossed Low Threshold (Ref. 2 in Figure 1): Current data () should be lower than a pre-specified threshold () and at least 150 ms should have passed since the last saved feature. is also saved into the feature list.
- Crest Middle (Ref. 3 in Figure 1): Current data () should be higher than a pre-specified threshold () and at least 150 ms should have passed since the last saved feature. is also saved into the feature list.
- Crest (Ref. 4 in Figure 1): This feature is only assessed if Crest Middle has been saved into the list. Therefore, current data () should have crossed the already exceeded pre-specified threshold () and a certain amount of time (), which differs between acquired signals (, ), should have passed since the last saved feature, so that a crest may be reported. is also saved into the feature list.
- Trough Middle (Ref. 5 in Figure 1): Current data () should be lower than a pre-specified threshold () and at least 150 ms should have passed since the last saved feature. is also saved into the feature list.
- Trough (Ref. 6 in Figure 1): This feature is only assessed if Trough Middle has been saved into the list. Therefore, current data () should again be above the already crossed pre-specified threshold () and a certain amount of time (), which differs between acquired signals (, ), should have passed since the last saved feature, so that a crest may be reported. is also saved into the feature list.
- Neutral (Ref. 7 in Figure 1): A neutral region is only reported as long as the current data () remains within the range between and , and if a certain amount of time (), which differs between acquired signals (, ), has passed since the last saved feature. is also saved into the feature list.
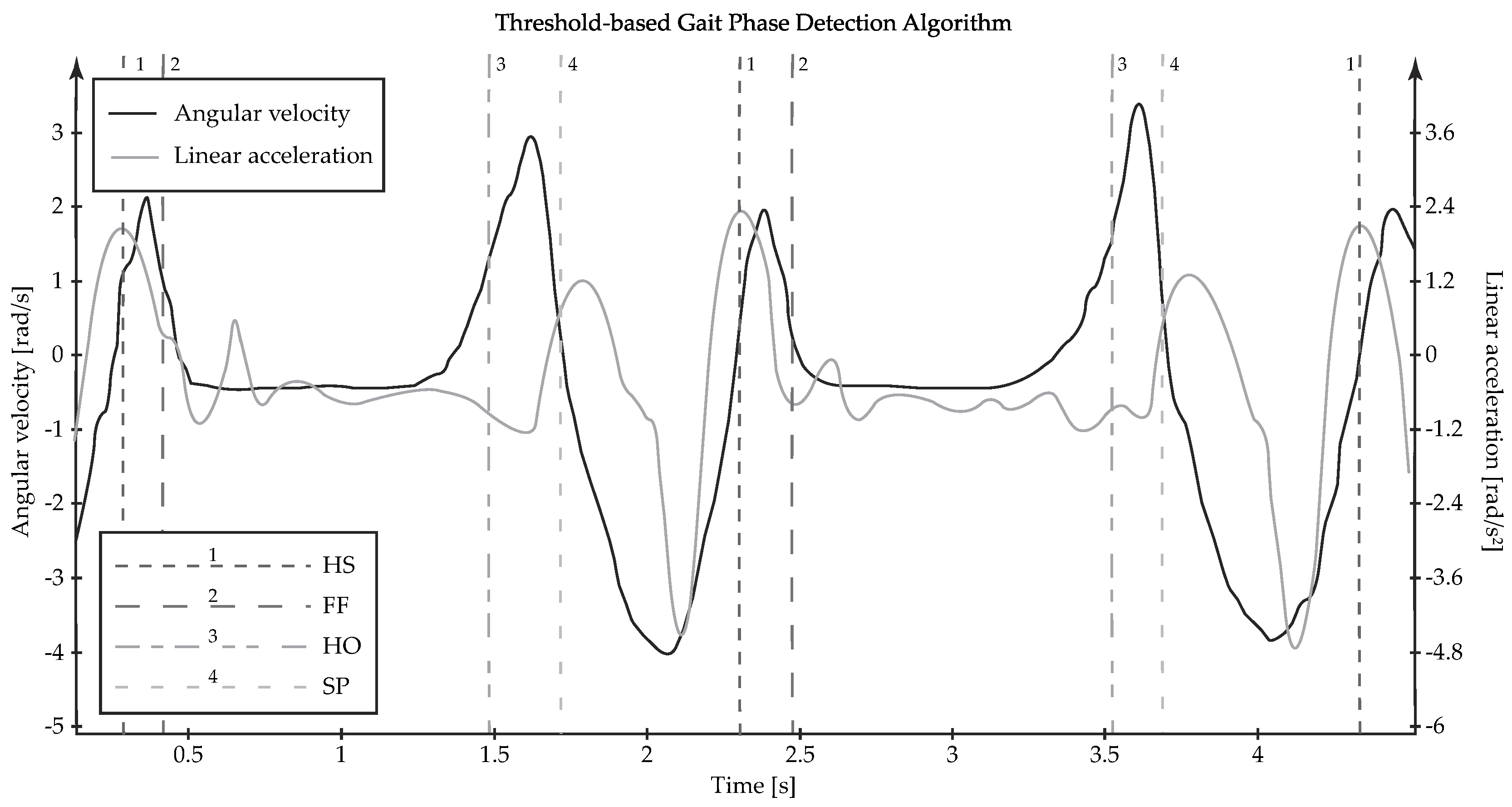
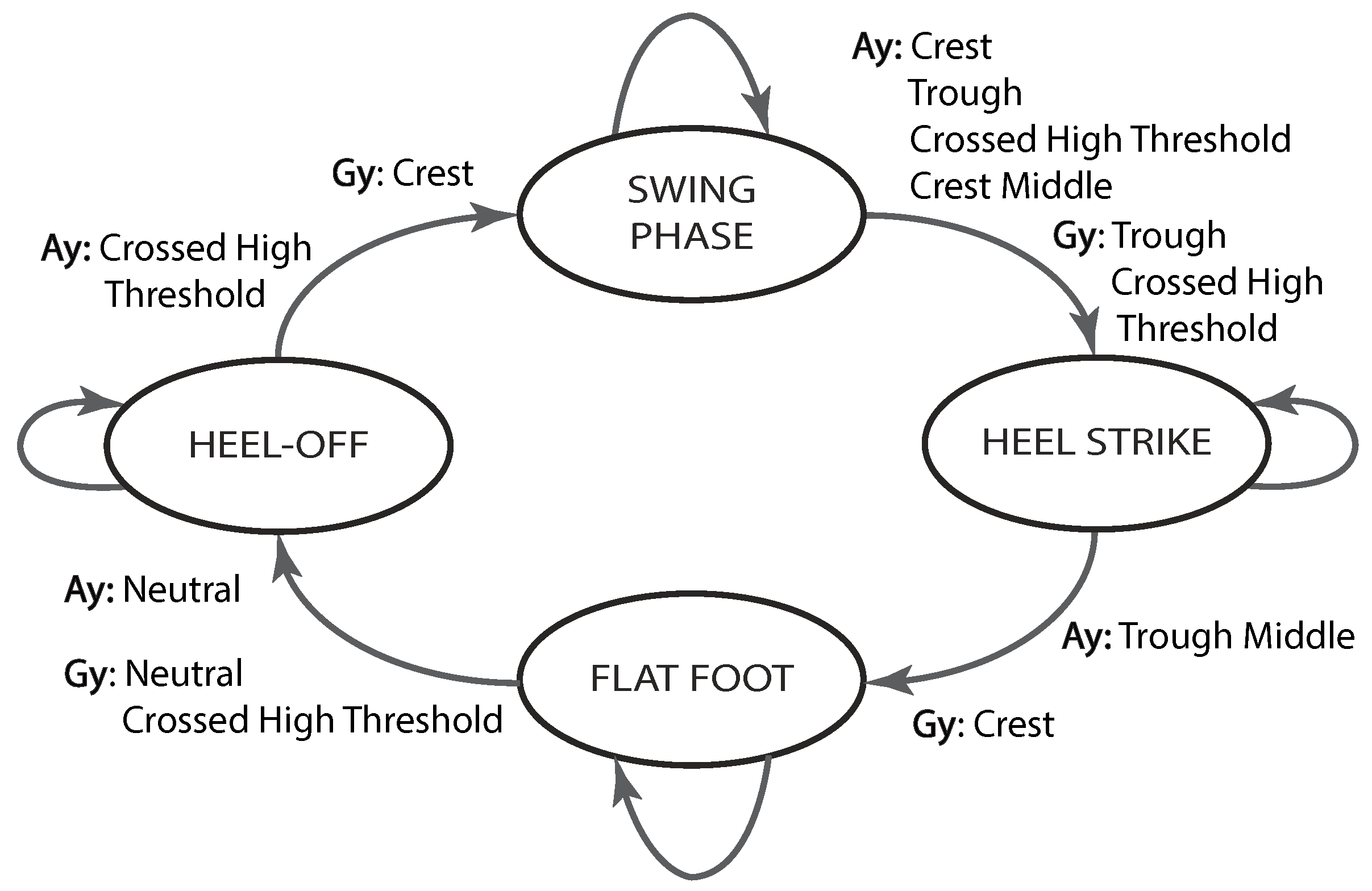
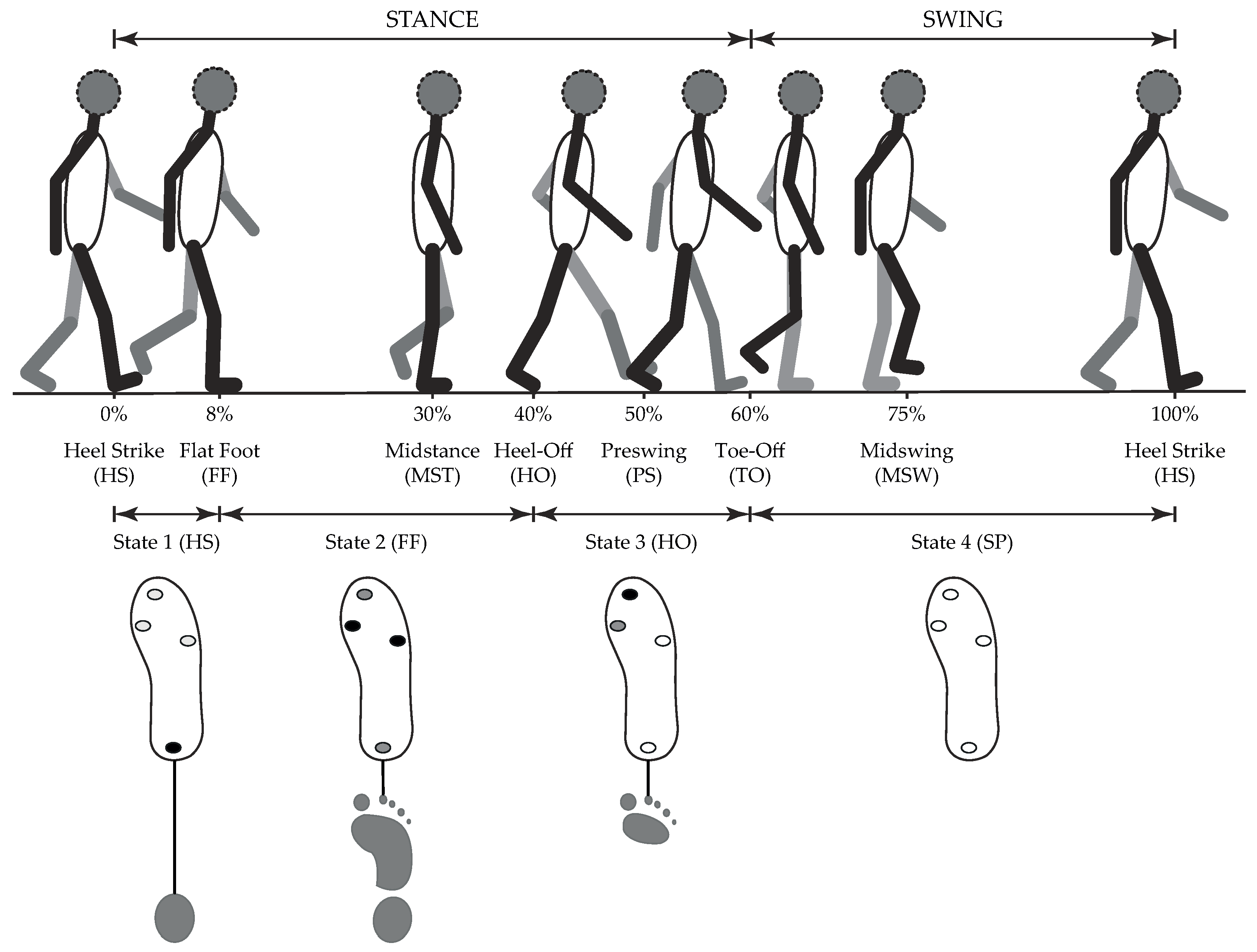
- SP → HS: With the aim of detecting the onset of HS, the current linear acceleration data should be right in the middle of a crest, after another crest, a trough and a crossed high threshold have been sequentially entered in the feature list, whereas the angular velocity signal should have exhibited a trough and a crossed high threshold, as shown in Figure 2.
- HS → FF: With the aim of detecting the onset of FF, the current linear acceleration data should be right in the middle of a trough, after entering the crest corresponding to HS in the feature list, whereas the angular velocity signal should have exhibited a crest (see Figure 2).
- FF → HO: With the aim of detecting the onset of HO, the current linear acceleration data should remain within a neutral region for a certain amount of time, as the angular velocity signal also exhibits a neutral region, followed by a crossed high threshold (see Figure 2).
- HO → SP: With the aim of detecting the onset of SP, the current linear acceleration data should have crossed a pre-defined threshold, whereas the angular velocity signal should have exhibited a crest, as shown in Figure 2.
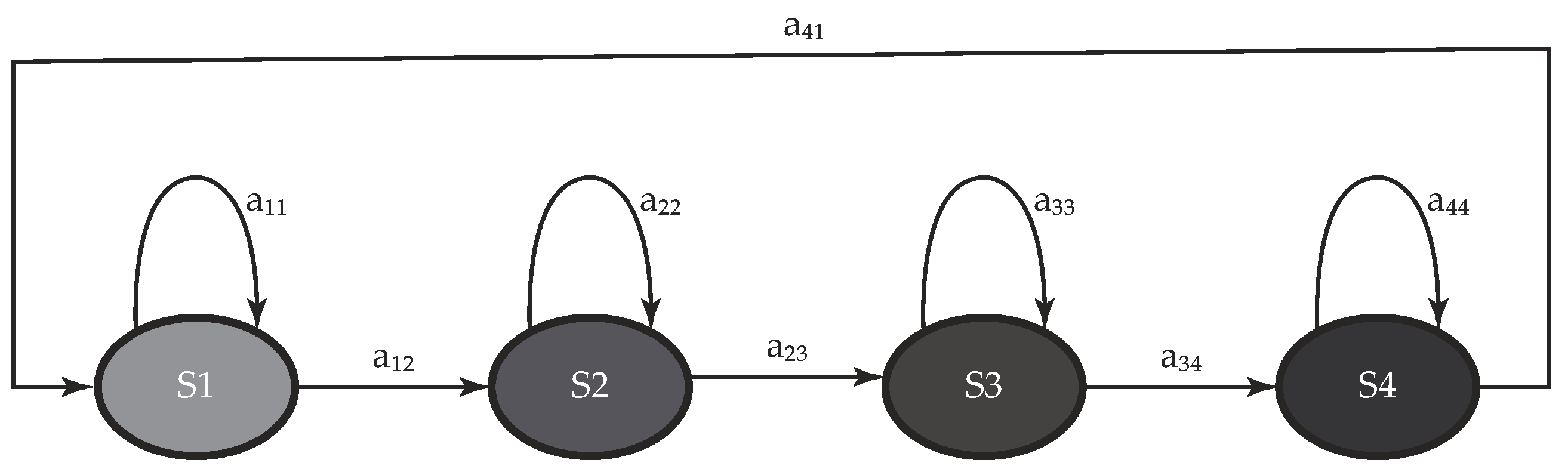
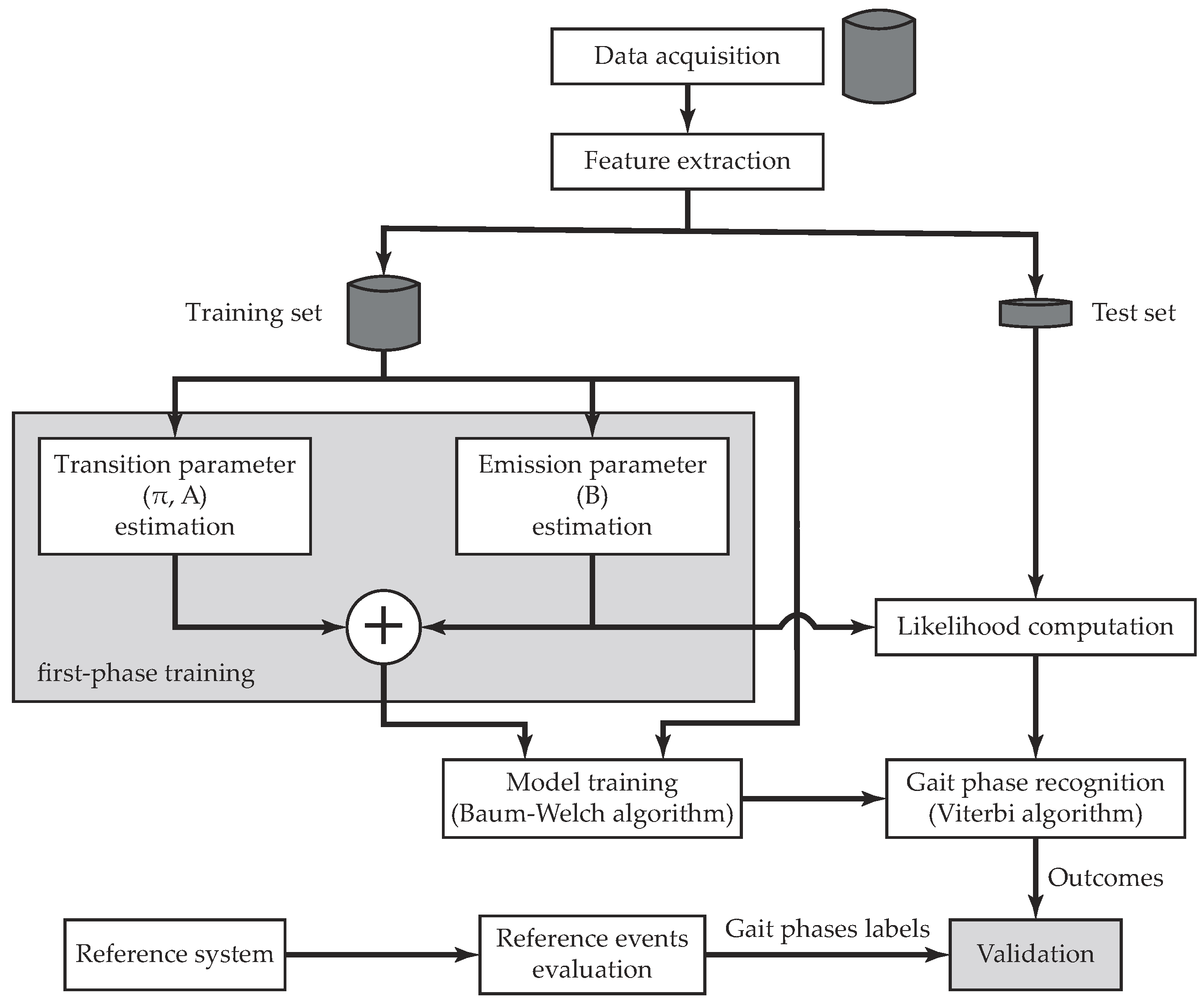
3.1.2. Classification Using a Hidden Markov Model
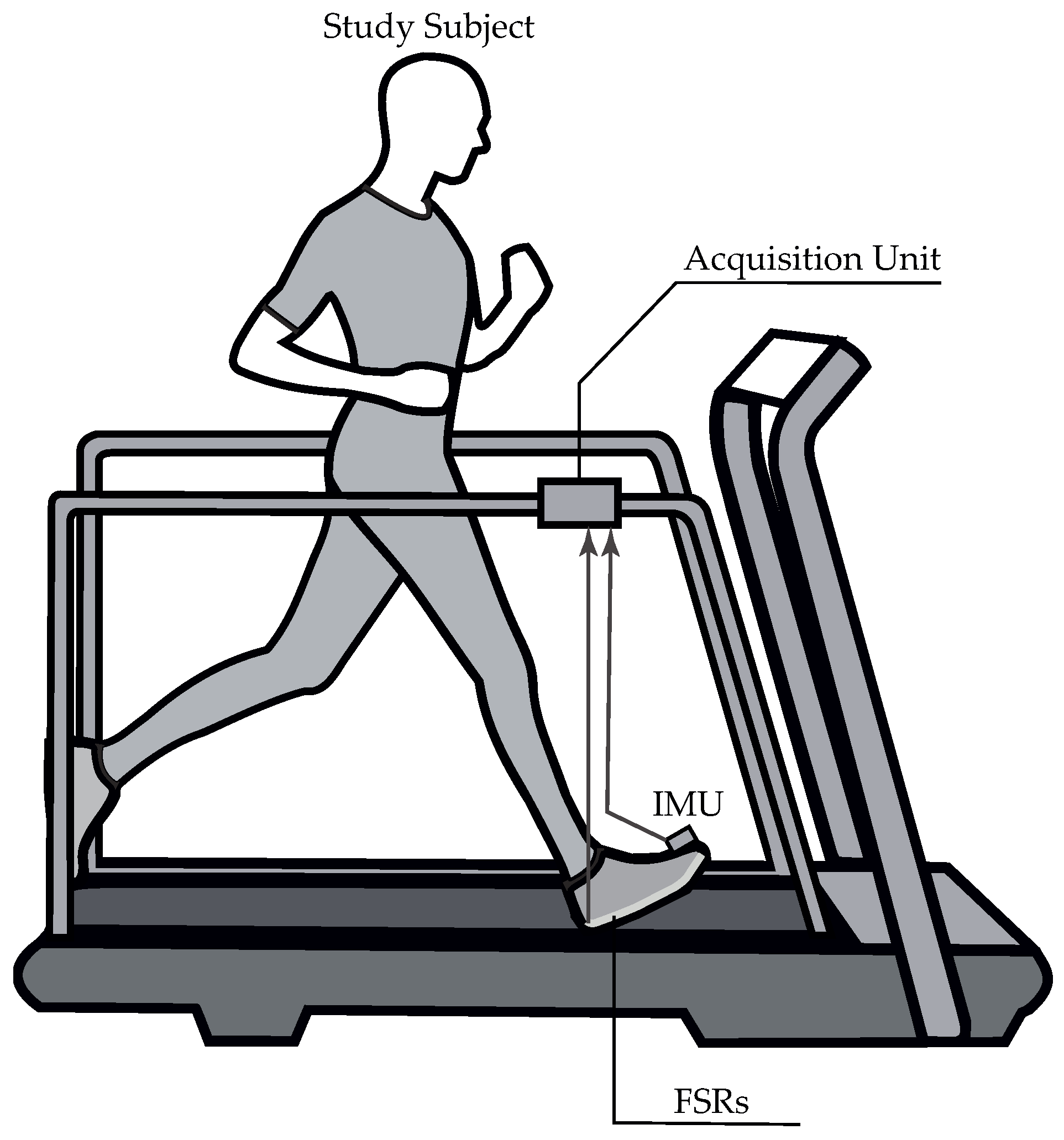
3.2. Experimental Procedure
3.3. Data Processing
3.4. Data Analysis
3.5. Statistical Analysis
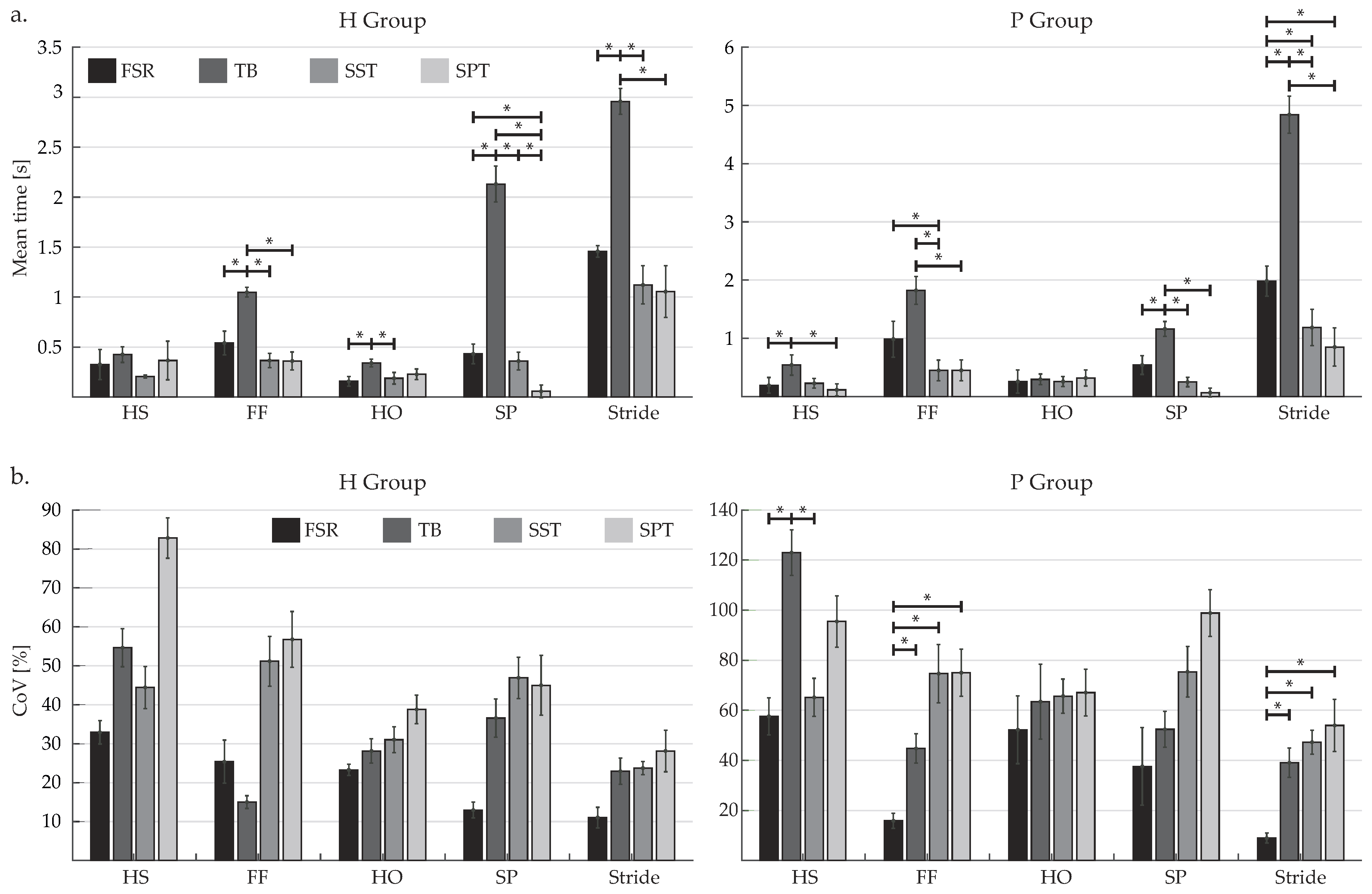
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| FES | Functional Electrical Stimulation |
| IC | Initial Contact |
| HS | Heel Strike |
| FF | Flat Foot |
| HO | Heel-Off |
| SP | Swing Phase |
| TO | Toe-Off |
| AFO | Ankle-Foot Orthosis |
| ENG | Electroneugram |
| EMG | Electromyography |
| FSR | Force-Sensitive Resistor |
| IMU | Inertial Measurement Unit |
| GPDS | Gait Phase Detection System |
| TB | Threshold-Based |
| HMM | Hidden Markov Model |
| SVM | Support Vector Machine |
| LDA | Linear Discriminant Analysis |
| GMM | Gaussian Mixture Model |
| ANN | Artificial Neural Network |
| MS | Mid-Swing |
| SPT | Standardized Parameters Training |
| ROS | Robot Operative System |
| FSM | Finite State Machine |
| Probability Density Function | |
| BMI | Body Mass Index |
| GRF | Ground Reaction Force |
| LR | Loading Response |
| MST | Midstance |
| PS | Preswing |
| SST | Subject Specific Training |
| SPT | Standardized Parameters Training |
| CI | Confidence Interval |
| G | Goodness Index |
| ROC | Receiver Operating Characteristic |
| TPR | True Positive Rate |
| TNR | True Negative Rate |
| MT | Mean Time |
| CoV | Coefficient of Variation |
| std | Standard Deviation |
| ICC | Intra-class Correlation Coefficient |
| SCI | Spinal Cord Injury |
References
- Wagenaar, R.C.; van Emmerik, R.E. Dynamics of pathological gait. Hum. Mov. Sci. 1994, 13, 441–471. [Google Scholar] [CrossRef]
- Veneman, J.; Kruidhof, R.; Hekman, E.; Ekkelenkamp, R.; Van Asseldonk, E.; van der Kooij, H. Design and Evaluation of the LOPES Exoskeleton Robot for Interactive Gait Rehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 2007, 15, 379–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rueterbories, J.; Spaich, E.G.; Andersen, O.K. Gait event detection for use in FES rehabilitation by radial and tangential foot accelerations. Med. Eng. Phys. 2014, 36, 502–508. [Google Scholar] [CrossRef] [PubMed]
- Chu, J.U.; Song, K.I.; Han, S.; Lee, S.H.; Kang, J.Y.; Hwang, D.; Suh, J.K.F.; Choi, K.; Youn, I. Gait phase detection from sciatic nerve recordings in functional electrical stimulation systems for foot drop correction. Physiol. Meas. 2013, 34, 541–565. [Google Scholar] [CrossRef] [PubMed]
- Mannini, A.; Trojaniello, D.; Cereatti, A.; Sabatini, A. A Machine Learning Framework for Gait Classification Using Inertial Sensors: Application to Elderly, Post-Stroke and Huntington’s Disease Patients. Sensors 2016, 16, 134. [Google Scholar] [CrossRef] [PubMed]
- Cheng, W.C.; Jhan, D.M. Triaxial Accelerometer-Based Fall Detection Method Using a Self-Constructing Cascade-AdaBoost-SVM Classifier. IEEE J. Biomed. Health Inform. 2013, 17, 411–419. [Google Scholar] [CrossRef]
- Beauchet, O.; Allali, G.; Berrut, G.; Hommet, C.; Dubost, V.; Assal, F. Gait analysis in demented subjects: Interests and perspectives. Neuropsychiatr. Dis. Treat. 2008, 4, 155–160. [Google Scholar] [CrossRef] [Green Version]
- Figueiredo, J.; Ferreira, C.; Santos, C.P.; Moreno, J.C.; Reis, L.P. Real-Time Gait Events Detection during Walking of Biped Model and Humanoid Robot through Adaptive Thresholds. In Proceedings of the 2016 International Conference on Autonomous Robot Systems and Competitions (ICARSC), Bragança, Portugal, 4–6 May 2016; pp. 66–71. [Google Scholar] [CrossRef]
- Vu, H.T.T.; Gomez, F.; Cherelle, P.; Lefeber, D.; Nowé, A.; Vanderborght, B. ED-FNN: A New Deep Learning Algorithm to Detect Percentage of the Gait Cycle for Powered Prostheses. Sensors 2018, 18, 2389. [Google Scholar] [CrossRef]
- Murray, S.; Goldfarb, M. Towards the use of a lower limb exoskeleton for locomotion assistance in individuals with neuromuscular locomotor deficits. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August–1 September 2012; Volume 2012, pp. 1912–1915. [Google Scholar] [CrossRef]
- Taborri, J.; Scalona, E.; Rossi, S.; Palermo, E.; Patane, F.; Cappa, P. Real-time gait detection based on Hidden Markov Model: Is it possible to avoid training procedure? In Proceedings of the 2015 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Torino, Italy, 7–9 May 2015; pp. 141–145. [Google Scholar]
- Taborri, J.; Palermo, E.; Rossi, S.; Cappa, P. Gait Partitioning Methods: A Systematic Review. Sensors 2016, 16, 66. [Google Scholar] [CrossRef]
- Kim, J.; Hwang, S.; Sohn, R.; Lee, Y.; Kim, Y. Development of an Active Ankle Foot Orthosis to Prevent Foot Drop and Toe Drag in Hemiplegic Patients: A Preliminary Study. Appl. Bionics Biomech. 2011, 8, 377–384. [Google Scholar] [CrossRef]
- Gu, G.M.; Kyeong, S.; Park, D.S.; Kim, J. SMAFO: Stiffness modulated Ankle Foot Orthosis for a patient with foot drop. In Proceedings of the 2015 IEEE International Conference on Rehabilitation Robotics (ICORR), Singapore, 11–14 August 2015; pp. 543–548. [Google Scholar] [CrossRef]
- Blaya, J.; Herr, H. Adaptive Control of a Variable-Impedance Ankle-Foot Orthosis to Assist Drop-Foot Gait. IEEE Trans. Neural Syst. Rehabil. Eng. 2004, 12, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Miller, A. Gait event detection using a multilayer neural network. Gait Posture 2009, 29, 542–545. [Google Scholar] [CrossRef] [PubMed]
- Attal, F.; Amirat, Y.; Chibani, A.; Mohammed, S. Automatic Recognition of Gait phases Using a Multiple Regression Hidden Markov Model. IEEE/ASME Trans. Mechatron. 2018, 23, 1597–1607. [Google Scholar] [CrossRef]
- Qi, Y.; Soh, C.B.; Gunawan, E.; Low, K.S.; Thomas, R. Assessment of Foot Trajectory for Human Gait Phase Detection Using Wireless Ultrasonic Sensor Network. IEEE Trans. Neural Syst. Rehabil. Eng. 2016, 24, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Lim, D.H.; Kim, W.S.; Kim, H.J.; Han, C.S. Development of real-time gait phase detection system for a lower extremity exoskeleton robot. Int. J. Precis. Eng. Manuf. 2017, 18, 681–687. [Google Scholar] [CrossRef]
- Yu, L.; Zheng, J.; Wang, Y.; Song, Z.; Zhan, E. Adaptive method for real-time gait phase detection based on ground contact forces. Gait Posture 2015, 41, 269–275. [Google Scholar] [CrossRef]
- González, I.; Fontecha, J.; Hervás, R.; Bravo, J. An Ambulatory System for Gait Monitoring Based on Wireless Sensorized Insoles. Sensors 2015, 15, 16589–16613. [Google Scholar] [CrossRef] [Green Version]
- Nazmi, N.; Abdul Rahman, M.A.; Yamamoto, S.I.; Ahmad, S.A. Walking gait event detection based on electromyography signals using artificial neural network. Biomed. Signal Process. Control 2019, 47, 334–343. [Google Scholar] [CrossRef]
- Chia Bejarano, N.; Ambrosini, E.; Pedrocchi, A.; Ferrigno, G.; Monticone, M.; Ferrante, S. A Novel Adaptive, Real-Time Algorithm to Detect Gait Events From Wearable Sensors. IEEE Trans. Neural Syst. Rehabil. Eng. 2015, 23, 413–422. [Google Scholar] [CrossRef]
- Aung, M.S.H.; Thies, S.B.; Kenney, L.P.J.; Howard, D.; Selles, R.W.; Findlow, A.H.; Goulermas, J.Y. Automated Detection of Instantaneous Gait Events Using Time Frequency Analysis and Manifold Embedding. IEEE Trans. Neural Syst. Rehabil. Eng. 2013, 21, 908–916. [Google Scholar] [CrossRef]
- Islam, M.; Hsiao-Wecksler, E.T. Detection of Gait Modes Using an Artificial Neural Network during Walking with a Powered Ankle-Foot Orthosis. J. Biophys. 2016, 2016, 7984157. [Google Scholar] [CrossRef] [PubMed]
- Yuwono, M.; Su, S.W.; Guo, Y.; Moulton, B.D.; Nguyen, H.T. Unsupervised nonparametric method for gait analysis using a waist-worn inertial sensor. Appl. Soft Comput. 2014, 14, 72–80. [Google Scholar] [CrossRef]
- Winiarski, S.; Rutkowska-Kucharska, A. Estimated ground reaction force in normal and pathological gait. Acta Bioeng. Biomech. 2009, 11, 53–60. [Google Scholar] [PubMed]
- Ding, S.; Ouyang, X.; Li, Z.; Yang, H. Proportion-based fuzzy gait phase detection using the smart insole. Sens. Actuators A Phys. 2018, 284, 96–102. [Google Scholar] [CrossRef]
- Goršič, M.; Kamnik, R.; Ambrožič, L.; Vitiello, N.; Lefeber, D.; Pasquini, G.; Munih, M. Online Phase Detection Using Wearable Sensors for Walking with a Robotic Prosthesis. Sensors 2014, 14, 2776–2794. [Google Scholar] [CrossRef]
- Jiang, X.; Chu, K.H.T.; Khoshnam, M.; Menon, C. A Wearable Gait Phase Detection System Based on Force Myography Techniques. Sensors 2018, 18, 1279. [Google Scholar] [CrossRef]
- Taborri, J.; Rossi, S.; Palermo, E.; Patanè, F.; Cappa, P. A Novel HMM Distributed Classifier for the Detection of Gait Phases by Means of a Wearable Inertial Sensor Network. Sensors 2014, 14, 16212–16234. [Google Scholar] [CrossRef]
- Abaid, N.; Cappa, P.; Palermo, E.; Petrarca, M.; Porfiri, M. Gait detection in children with and without hemiplegia using single-axis wearable gyroscopes. PLoS ONE 2013, 8, e73152. [Google Scholar] [CrossRef]
- Taborri, J.; Scalona, E.; Palermo, E.; Rossi, S.; Cappa, P. Validation of Inter-Subject Training for Hidden Markov Models Applied to Gait Phase Detection in Children with Cerebral Palsy. Sensors 2015, 15, 24514–24529. [Google Scholar] [CrossRef] [Green Version]
- Behboodi, A.; Wright, H.; Zahradka, N.; Lee, S.C.K. Seven phases of gait detected in real-time using shank attached gyroscopes. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milano, Italy, 25–29 August 2015; Volume 2015, pp. 5529–5532. [Google Scholar] [CrossRef]
- Kim, M.; Lee, D. Development of an IMU-based foot-ground contact detection (FGCD) algorithm. Ergonomics 2017, 60, 384–403. [Google Scholar] [CrossRef]
- Smith, B.; Coiro, D.; Finson, R.; Betz, R.; McCarthy, J. Evaluation of force-sensing resistors for gait event detection to trigger electrical stimulation to improve walking in the child with cerebral palsy. IEEE Trans. Neural Syst. Rehabil. Eng. 2002, 10, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Gouwanda, D.; Gopalai, A.A. A robust real-time gait event detection using wireless gyroscope and its application on normal and altered gaits. Med. Eng. Phys. 2015, 37, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Caldas, R.; Mundt, M.; Potthast, W.; Buarque de Lima Neto, F.; Markert, B. A systematic review of gait analysis methods based on inertial sensors and adaptive algorithms. Gait Posture 2017, 57, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Guenterberg, E.; Yang, A.; Ghasemzadeh, H.; Jafari, R.; Bajcsy, R.; Sastry, S. A Method for Extracting Temporal Parameters Based on Hidden Markov Models in Body Sensor Networks With Inertial Sensors. IEEE Trans. Inf. Technol. Biomed. 2009, 13, 1019–1030. [Google Scholar] [CrossRef] [PubMed]
- Catalfamo, P.; Ghoussayni, S.; Ewins, D. Gait event detection on level ground and incline walking using a rate gyroscope. Sensors 2010, 10, 5683–5702. [Google Scholar] [CrossRef] [PubMed]
- Kotiadis, D.; Hermens, H.; Veltink, P. Inertial Gait Phase Detection for control of a drop foot stimulator. Med. Eng. Phys. 2010, 32, 287–297. [Google Scholar] [CrossRef] [PubMed]
- Sabatini, A.; Martelloni, C.; Scapellato, S.; Cavallo, F. Assessment of Walking Features From Foot Inertial Sensing. IEEE Trans. Biomed. Eng. 2005, 52, 486–494. [Google Scholar] [CrossRef] [Green Version]
- González, R.C.; López, A.M.; Rodriguez-Uría, J.; Álvarez, D.; Alvarez, J.C. Real-time gait event detection for normal subjects from lower trunk accelerations. Gait Posture 2010, 31, 322–325. [Google Scholar] [CrossRef]
- Mannini, A.; Sabatini, A.M. Gait phase detection and discrimination between walking–jogging activities using hidden Markov models applied to foot motion data from a gyroscope. Gait Posture 2012, 36, 657–661. [Google Scholar] [CrossRef]
- Mannini, A.; Sabatini, A.M. A hidden Markov model-based technique for gait segmentation using a foot-mounted gyroscope. In Proceedings of the 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011; Volume 2011, pp. 4369–4373. [Google Scholar] [CrossRef]
- Mannini, A.; Genovese, V.; Sabatin, A.M. Online Decoding of Hidden Markov Models for Gait Event Detection Using Foot-Mounted Gyroscopes. IEEE J. Biomed. Health Inform. 2014, 18, 1122–1130. [Google Scholar] [CrossRef]
- Kong, W.; Saad, M.H.; Hannan, M.A.; Hussain, A. Human gait state classification using artificial neural network. In Proceedings of the 2014 IEEE Symposium on Computational Intelligence for Multimedia, Signal and Vision Processing (CIMSIVP), Orlando, FL, USA, 9–12 December 2014; pp. 1–5. [Google Scholar] [CrossRef]
- Jung, J.Y.; Heo, W.; Yang, H.; Park, H. A Neural Network-Based Gait Phase Classification Method Using Sensors Equipped on Lower Limb Exoskeleton Robots. Sensors 2015, 15, 27738–27759. [Google Scholar] [CrossRef] [PubMed]
- Evans, R.; Arvind, D. Detection of Gait Phases Using Orient Specks for Mobile Clinical Gait Analysis. In Proceedings of the 2014 11th International Conference on Wearable and Implantable Body Sensor Networks, Zurich, Switzerland, 16–19 June 2014; pp. 149–154. [Google Scholar] [CrossRef]
- Sanchez-Manchola, M.; Gomez-Vargas, D.; Casas-Bocanegra, D.; Munera, M.; Cifuentes, C. Development of a Robotic Lower-Limb Exoskeleton for Gait Rehabilitation: AGoRA Exoskeleton. In Proceedings of the 2018 IEEE ANDESCON, Cali, Colombia, 22–24 August 2018. [Google Scholar] [CrossRef]
- Martinez, A.; Fernndez, E. Learning ROS for Robotics Programming; Packt Publishing: Birmingham, UK, 2013. [Google Scholar]
- Rabiner, L. A tutorial on hidden Markov models and selected applications in speech recognition. Proc. IEEE 1989, 77, 257–286. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Lu, K.; Yan, S.; Sun, M.; Lester, D.K.; Zhang, K. Gait phase varies over velocities. Gait Posture 2014, 39, 756–760. [Google Scholar] [CrossRef] [PubMed]
- Brisswalter, J.; Mottet, D. Energy cost and stride duration variability at preferred transition gait speed between walking and running. Can. J. Appl. Physiol. 1996, 21, 471–480. [Google Scholar] [CrossRef] [PubMed]
- Lemke, M.R.; Wendorff, T.; Mieth, B.; Buhl, K.; Linnemann, M. Spatiotemporal gait patterns during over ground locomotion in major depression compared with healthy controls. J. Psychiatr. Res. 2000, 34, 277–283. [Google Scholar] [CrossRef]
- Lee, S.J.; Hidler, J. Biomechanics of overground vs. treadmill walking in healthy individuals. J. Appl. Physiol. 2008, 104, 747–755. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject | Age | BMI [kg/m] | Gender | Walking Speed [m/s] |
|---|---|---|---|---|
| H1 | 23 | 22.2 | Male | 0.944 |
| H2 | 22 | 20.9 | Female | 0.750 |
| H3 | 22 | 22.7 | Male | 0.750 |
| H4 | 23 | 24.1 | Female | 0.694 |
| H5 | 22 | 23.7 | Male | 0.694 |
| H6 | 20 | 26.0 | Female | 0.639 |
| H7 | 25 | 20.7 | Female | 0.556 |
| H8 | 25 | 23.7 | Male | 0.833 |
| H9 | 27 | 23.7 | Male | 0.833 |
| Subject | Age | BMI [kg/m] | Gender | Etiology | Paretic Side | Year of Ocurrence | Walking Speed | Walking Aids |
|---|---|---|---|---|---|---|---|---|
| P1 | 37 | 24.7 | Female | Ischemic Stroke | Left | 2016 | 0.417 | Cane |
| P2 | 75 | 20.1 | Female | Ischemic Stroke | Right | 2016 | 0.306 | Cane or Wheelchair |
| P3 | 49 | 26.9 | Female | Ischemic Stroke | Left | 2010 | 0.278 | AFO |
| P4 | 38 | 25.0 | Male | Hemorrhagic Stroke | Left | 2017 | 0.639 | None |
| P5 | 47 | 34.0 | Male | Ischemic Stroke | Left | 2016 | 0.444 | AFO |
| P6 | 33 | 22.0 | Female | Hemorrhagic Stroke | Right | 2012 | 0.417 | Cane |
| P7 | 46 | 31.2 | Male | Ischemic Stroke | Right | 2001 | 0.417 | Cane |
| P8 | 20 | 21.7 | Male | Cerebral Palsy | Left | 1998 (Birth) | 0.5 | None |
| P9 | 35 | 23.4 | Male | Hemorragic Stroke | Left | 2013 | 0.667 | None |
| H Group | P Group | |||||
|---|---|---|---|---|---|---|
| TB Method | SST Method | SPT Method | TB Method | SST Method | SPT Method | |
| HS | * | * | ||||
| FF | * | * | * | * | ||
| HO | * | * | ||||
| SP | * | * | ||||
| ICC | |||||||
|---|---|---|---|---|---|---|---|
| Group | Index | Reference/Classifier | HS | FF | HO | SP | Stride |
| H | MT | FSR | |||||
| TB | |||||||
| SST | |||||||
| SPT | |||||||
| CoV | FSR | ||||||
| TB | |||||||
| SST | |||||||
| SPT | |||||||
| P | MT | FSR | |||||
| TB | |||||||
| SST | |||||||
| SPT | |||||||
| CoV | FSR | ||||||
| TB | |||||||
| SST | |||||||
| SPT | |||||||
 Poor
Poor  Fair
Fair  Good
Good  Excellent.
Excellent.| Classification Output | ||||||
|---|---|---|---|---|---|---|
| HS | FF | HO | SP | |||
| 1. TB algorithm | ||||||
| Actual Label | H | HS | 57.11% | 16.59% | 5.58% | 20.72% |
| FF | 1.03% | 72.08% | 0.47% | 26.42% | ||
| HO | 1.50% | 18.77% | 52.98% | 26.75% | ||
| SP | 13.72% | 7.5% | 12.62% | 66.16% | ||
| Overall accuracy: 63.96%. 95% CI: 63.91–64.01% | ||||||
| P | HS | 57.82% | 18.24% | 4.17% | 19.77% | |
| FF | 2.91% | 70.24% | 0.77% | 26.08% | ||
| HO | 3.48% | 20.1% | 53.13% | 23.29% | ||
| SP | 10.71% | 13.77% | 8.19% | 67.33% | ||
| Overall accuracy: 65.43%. 95% CI: 65.38–65.48% | ||||||
| 2. HMM-based algorithm with SST approach | ||||||
| Actual Label | H | HS | 70.15% | 12.08% | 7.22% | 10.55% |
| FF | 5.02% | 85.81% | 6.42% | 2.75% | ||
| HO | 4.40% | 5.85% | 81.57% | 8.18% | ||
| SP | 5.33% | 2.05% | 2.61% | 90.01% | ||
| Overall accuracy: 81.44%. 95% CI: 81.40–81.48% | ||||||
| P | HS | 67.22% | 10.65% | 9.2% | 12.93% | |
| FF | 6.44% | 81.87% | 9.39% | 2.30% | ||
| HO | 5.86% | 9.36% | 77.28% | 7.50% | ||
| SP | 11.66% | 2.31% | 7.20% | 78.83% | ||
| Overall accuracy: 78.06%. 95% CI: 78.02–78.10% | ||||||
| 3. HMM-based algorithm with SPT approach | ||||||
| Actual Label | H | HS | 75.55% | 9.79% | 2.92% | 11.74% |
| FF | 7.29% | 85.85% | 5.98% | 0.88% | ||
| HO | 2.19% | 4.05% | 90.55% | 3.21% | ||
| SP | 24.76% | 0.58% | 13.19% | 61.47% | ||
| Overall accuracy: 76.91%. 95% CI: 76.84–76.99% | ||||||
| P | HS | 63.50% | 14.89% | 4.78% | 16.92% | |
| FF | 2.66% | 84.97% | 11.33% | 1.04% | ||
| HO | 1.49% | 12.37% | 81.69% | 4.45% | ||
| SP | 16.33% | 2.96% | 17.45% | 63.26% | ||
| Overall accuracy: 76.36%. 95% CI: 76.29–76.43% | ||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez Manchola, M.D.; Bernal, M.J.P.; Munera, M.; Cifuentes, C.A. Gait Phase Detection for Lower-Limb Exoskeletons using Foot Motion Data from a Single Inertial Measurement Unit in Hemiparetic Individuals. Sensors 2019, 19, 2988. https://doi.org/10.3390/s19132988
Sánchez Manchola MD, Bernal MJP, Munera M, Cifuentes CA. Gait Phase Detection for Lower-Limb Exoskeletons using Foot Motion Data from a Single Inertial Measurement Unit in Hemiparetic Individuals. Sensors. 2019; 19(13):2988. https://doi.org/10.3390/s19132988
Chicago/Turabian StyleSánchez Manchola, Miguel D., María J. Pinto Bernal, Marcela Munera, and Carlos A. Cifuentes. 2019. "Gait Phase Detection for Lower-Limb Exoskeletons using Foot Motion Data from a Single Inertial Measurement Unit in Hemiparetic Individuals" Sensors 19, no. 13: 2988. https://doi.org/10.3390/s19132988
APA StyleSánchez Manchola, M. D., Bernal, M. J. P., Munera, M., & Cifuentes, C. A. (2019). Gait Phase Detection for Lower-Limb Exoskeletons using Foot Motion Data from a Single Inertial Measurement Unit in Hemiparetic Individuals. Sensors, 19(13), 2988. https://doi.org/10.3390/s19132988