Wearable Potentiometric Sensors for Medical Applications




Abstract
:1. Introduction
- There is a noticeable trend toward measuring ions in sweat (ca. 80% of the reported papers in the last eight years comprise sweat analyses) that is clearly owing to the high ion content in this matrix (on the mM range), the simplicity of the sample (with affordable selectivity requirements for ISEs) and the easy adaptation of daily objects/materials (such as sweatbands, epidermal patches and textiles), which are in contact with the skin for potentiometric measurements with ISEs.
- Despite sweat collection not involving any invasive and/or painful procedure in the individual, the secretion of a sufficient amount of sweat is needed. While this statement is compatible once the wearable sensor is applied to a sport activity, in the case of medical applications, it is necessary to expose the patient to high temperatures to increase the sweating rate, which will vary for different patients, or using alternatives techniques, such as iontophoresis-based instrumentation. The first option may sometimes disturb patient well-being, especially in elderly people, because of side problems related to exposure to high temperatures, such as low blood pressure or dizziness, whereas the iontophoresis-induction process may cause skin burning and skin allergies. Consequently, wearable potentiometric sensors have been mainly applied to sweat analysis during physical exertion, although the authors usually claimed that the devices could be used also for medical purposes [14,26,27].
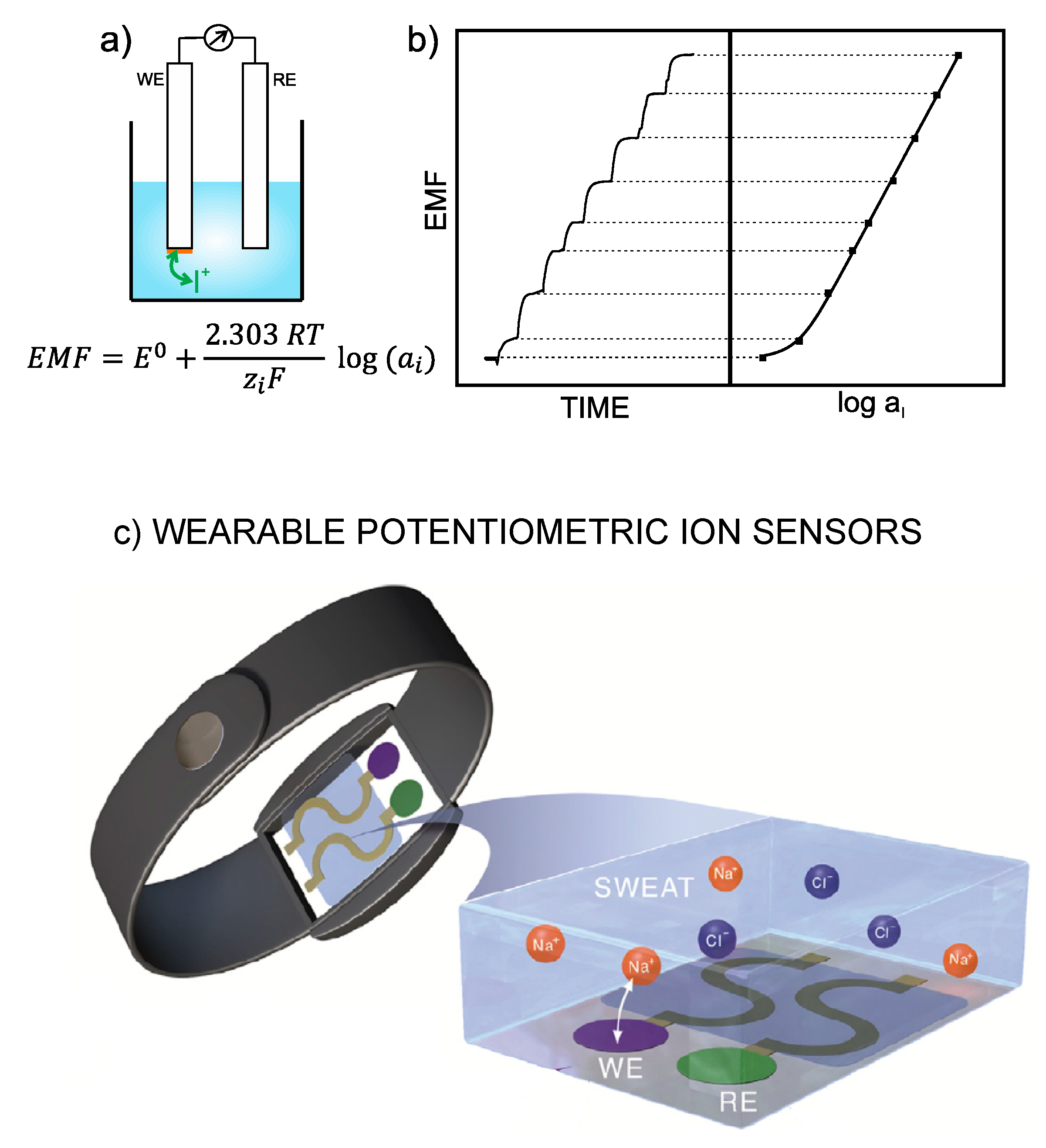
- The all-solid-contact configuration is incorporated in all assessed wearable sensors contributions. In general, the devices are based on ISEs that were already characterized in a traditional configuration before its implementation into the wearable platform. The general strategy consists on the modification of a flexible substrate with a conductive path, then with the ion-to-electron transducer and finally with the sensing element (Figure 1c). Thus, ISEs comprising polymeric ISMs are used for the detection of , , and , the conventional Ag/AgCl electrode for sensing, while pH detection is conducted by solid electrodes based on polyaniline (PANI) or iridium oxide.
- As the selected papers were focused on wearables fitting sport activity monitoring, many authors investigated the resiliency of the sensor response facing different physical tests (such as stretching, bending, torsion, poking, crumpling and indention) as well as putting forward the use of novel electrode designs and advanced materials to circumvent any possible influence on electrode response [28].
2. Discussion on Potential Biological Fluids to Be Analyzed by Wearable Potentiometric Ion Sensors
3. Description and Critical Evaluation of Recent Wearable Potentiometric Ion Sensors with Potential Medical Applications
4. Description and Critical Evaluation of Wearable Potentiometric Ion Sensors Reported in the Last Five Years for Biomedical Applications
5. Tentative Guidance for the Successful Characterization of a Wearable Potentiometric Ion Sensor
5.1. Calibration of the Sensors
5.2. Other Analytical Parameters
- Reversibility. The so-called ‘carry-over test’ evaluates the possibility of measuring increasing and decreasing steps in the ion analyte concentration [27]. It is crucial to carry out this test once the electrodes are implemented with the sampling strategy.
- Response time inherent to the electrode and response time associated to the device involving the sample collection. When a sampling cell is used for this purpose, this latter comprises the time needed to fill the sensor compartment and depends on the sweat rate of the subject. It is here also critical to adopt a correction of the measurements depending on the sweat rate at each moment, just as in the case of the Javey group [39]. Notably, it would be convenient to more deeply analyze the behavior of the electrodes in this type of flow cell. We are referring to investigating the effect of convection, diffusion and the magnitude of the flow rate during the potentiometric response. In this regard, it is crucial to consider that the use of the initial calibration will be conditioned by the fact that these factors may slightly affect the electrode response, therefore introducing a source of error.On the other hand, it is hard to assure on-body monitoring in real time because a certain amount of sample is always needed to fill the reservoir in which the sensors are embedded. Thereafter, the reservoir continuously renews the sweat, but this does not occur exactly at the same time the individual is sweating. Time is needed for the generated sweat to reach the sensors’ chamber and then each sensor (in the case of multiplexed analysis), which involves a delay between the sweating process and data observation.In the case of an absorbent material coupled to iontophoresis-based sweat collection, the response time depends on the filling of the pad together with several minutes of potential recording [57].
- Between-electrode reproducibility and response repeatability (same electrode). These two features are vital for the final use of the wearable potentiometric sensors reaching mass production and commercialization. In the ideal case, a universal calibration graph valid for each ion analyte is implemented in software that permits the end-user to read the corresponding concentration in sweat. However, this is only valid when exactly the same calibration is observed for different electrodes fabricated in the same manner and for the same electrode over time. Yet, this does not happen in reality. Conversely, current efforts in the development of new ISEs focus on the direction of achieving this purpose, or what are called calibration-free sensors. Several strategies have been published over the last five years, such as the use of redox pairs as ion-to-electron transducers [76], the adjustment of the E0 of the calibration graph by applying a controlled potential or current as well as short-circuiting [77,78] and charge counting either by interrogating ISMs using dynamic electrochemical techniques rather than potentiometry or by the confinement of the sample to a thin-layer gap [79]. Regrettably, none of them has yet been implemented into a wearable configuration, as far as we know, and maybe, the next generation of calibration-free wearable ion sensors relies on this advancement.
- A characterization of the reference electrode is missing in most of the wearable potentiometric sensors. Indeed, a misbehavior of the reference electrode is a strong source of error in the calculation of the ion analyte concentration if, for any reason, the electrode does not provide constant potential. In this regard, it is important to characterize the reference electrode independently and then together with the potentiometric electrodes once implemented in the wearable. In a first step, the potential of the reference electrode must be tested for changes in electrolyte concentrations, redox species, pH, temperature, physical deformation as well as light/darkness conditions. Then, medium-term stability in (artificial) sweat (or other fluids) should be also assessed.
5.3. On-Body Measurements and Validation
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bobacka, J.; Ivaska, A.; Lewenstam, A. Potentiometric ion sensors. Chem. Rev. 2008, 108, 329–351. [Google Scholar] [CrossRef] [PubMed]
- Bakker, E.; Pretsch, E. Modern Potentiometry. Angew. Chem. Int. Ed. 2007, 46, 5660–5668. [Google Scholar] [CrossRef]
- Cuartero, M.; Crespo, G.A. Using Potentiometric Electrodes Based on Nonselective Polymeric Membranes as Potential Universal Detectors for Ion Chromatography: Investigating an Original Research Problem from an Inquiry-Based-Learning Perspective. J. Chem. Educ. 2018, 95, 2172–2181. [Google Scholar] [CrossRef]
- Parrilla, M.; Cuartero, M.; Crespo, G.A. Wearable potentiometric ion sensors. TrAC-Trends Anal. Chem. 2019, 110, 303–320. [Google Scholar] [CrossRef]
- Bobacka, J. Potential stability of all-solid-state ion-selective electrodes using conducting polymers as ion-to-electron transducers. Anal. Chem. 1999, 71, 4932–4937. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.B.; Stein, A.; Buhlmann, P. Rational design of all-solid-state ion-selective electrodes and reference electrodes. TrAC-Trends Anal. Chem. 2016, 76, 102–114. [Google Scholar] [CrossRef]
- Cuartero, M.; Crespo, G.A.; Bakker, E. Tandem Electrochemical Desalination-Potentiometric Nitrate Sensing for Seawater Analysis. Anal. Chem. 2015, 87, 8084–8089. [Google Scholar] [CrossRef]
- Pankratova, N.; Cuartero, M.; Cherubini, T.; Crespo, G.A.; Bakker, E. In-Line Acidification for Potentiometric Sensing of Nitrite in Natural Waters. Anal. Chem. 2017, 89, 571–575. [Google Scholar] [CrossRef] [PubMed]
- Cuartero, M.; del Rio, J.S.; Blondeau, P.; Ortuno, J.A.; Rius, F.X.; Andrade, F.J. Rubber-based substrates modified with carbon nanotubes inks to build flexible electrochemical sensors. Anal. Chim. Acta 2014, 827, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Novell, M.; Parrilla, M.; Crespo, G.A.; Rius, F.X.; Andrade, F.J. Paper-Based Ion-Selective Potentiometric Sensors. Anal. Chem. 2012, 84, 4695–4702. [Google Scholar] [CrossRef]
- Guinovart, T.; Parrilla, M.; Crespo, G.A.; Rius, F.X.; Andrade, F.J. Potentiometric sensors using cotton yarns, carbon nanotubes and polymeric membranes. Analyst 2013, 138, 5208–5215. [Google Scholar] [CrossRef] [PubMed]
- Crespo, G.A. Recent Advances in Ion-selective membrane electrodes for in situ environmental water analysis. Electrochim. Acta 2017, 245, 1023–1034. [Google Scholar] [CrossRef]
- Cuartero, M.; Crespo, G.A. All-Solid-State Potentiometric Sensors: A New Wave for In Situ Aquatic Research. Cur. Opin. Electrochem. 2018, 10, 98–106. [Google Scholar] [CrossRef]
- McCaul, M.; Glennin, T.; Diamond, D. Challenges and opportunities in wearable technology for biomedical analysis in sweat. Curr. Opin. Electrochem. 2017, 3, 46–50. [Google Scholar] [CrossRef]
- Hayward, J.; Pugh, D.; Chansin, G. Wearable Sensors 2018–2028: Technologies, Markets & Players; IDTechEx: Cambridge, UK, 2018. [Google Scholar]
- Berrocal, M.J.; Badr, I.H.A.; Gao, D.O.; Bachas, L.G. Reducing the thrombogenicity of ion-selective electrode membranes through the use of a silicone-modified segmented polyurethane. Anal. Chem. 2001, 73, 5328–5333. [Google Scholar] [CrossRef] [PubMed]
- Gao, W.; Brooks, G.A.; Klonoff, D.C. Wearable physiological systems and technologies for metabolic monitoring. J. Appl. Physiol. 2018, 124, 548–556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McLister, A.; McHugh, J.; Cundell, J.; Davis, J. New Developments in Smart Bandage Technologies for Wound Diagnostics. Adv. Mater. 2016, 28, 5732–5737. [Google Scholar] [CrossRef]
- Scurati-Manzoni, E.; Fossali, E.F.; Agostoni, C.; Riva, E.; Simonetti, G.D.; Zanolari-Calderari, M.; Bianchetti, M.G.; Lava, S.A.G. Electrolyte abnormalities in cystic fibrosis: Systematic review of the literature. Pediatr. Nephrol. 2014, 29, 1015–1023. [Google Scholar] [CrossRef]
- Guinovart, T.; Hernandez-Alonso, D.; Adriaenssens, L.; Blondeau, P.; Rius, F.X.; Ballester, P.; Andrade, F.J. Characterization of a new ionophore-based ion-selective electrode for the potentiometric determination of creatinine in urine. Biosens. Bioelectron. 2017, 87, 587–592. [Google Scholar] [CrossRef]
- Albero, M.I.; Ortuno, J.A.; Garcia, M.S.; Cuartero, M.; Alcaraz, M.C. Novel flow-through bulk optode for spectrophotometric determination of lithium in pharmaceuticals and saliva. Sens. Actuators B Chem. 2010, 145, 133–138. [Google Scholar] [CrossRef]
- Ortuno, J.A.; Garcia, M.S.; Albero, M.I.; Cuartero, M. A Micro-Coated Wire Ion-Selective Electrode for Flow-Injection Analysis of Trazodone in Pharmaceuticals, Human Urine and Serum. Sens. Lett. 2009, 7, 615–620. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, Z.; Jain, V.; Yi, J.; Mueller, S.; Sokolov, J.; Liu, Z.; Levon, K.; Rigas, B.; Rafailovich, M.H. Potentiometric sensors based on surface molecular imprinting: Detection of cancer biomarkers and viruses. Sens. Actuators B Chem. 2010, 146, 381–387. [Google Scholar] [CrossRef]
- Sharma, P.S.; Wojnarowicz, A.; Sosnowska, M.; Benincori, T.; Noworyta, K.; D’Souza, F.; Kutner, W. Potentiometric chemosensor for neopterin, a cancer biomarker, using an electrochemically synthesized molecularly imprinted polymer as the recognition unit. Biosens. Bioelectron. 2016, 77, 565–572. [Google Scholar] [CrossRef]
- Schazmann, B.; Morris, D.; Slater, C.; Beirne, S.; Fay, C.; Reuveny, R.; Moyna, N.; Diamond, D. A wearable electrochemical sensor for the real-time measurement of sweat sodium concentration. Anal. Methods 2010, 2, 342–348. [Google Scholar] [CrossRef] [Green Version]
- Gao, W.; Emaminejad, S.; Nyein, H.Y.Y.; Challa, S.; Chen, K.V.; Peck, A.; Fahad, H.M.; Ota, H.; Shiraki, H.; Kiriya, D.; et al. Fully integrated wearable sensor arrays for multiplexed in situ perspiration analysis. Nature 2016, 529, 509–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sempionatto, J.R.; Martin, A.; Garcia-Carmona, L.; Barfidokht, A.; Kurniawan, J.F.; Moreto, J.R.; Tang, G.; Shin, A.; Liu, X.; Escarpa, A.; et al. Skin-worn soft microfluidic potentiometric detection system. Electroanalysis 2018, in press. [Google Scholar] [CrossRef]
- Heikenfeld, J.; Jajack, A.; Rogers, J.; Gutruf, P.; Tian, L.; Pan, T.; Li, R.; Khine, M.; Kim, J.; Wang, J. Wearable sensors: Modalities, challenges, and prospects. Lab Chip 2018, 18, 217–248. [Google Scholar] [CrossRef]
- Liu, Y.; Pharr, M.; Salvatore, G.A. Lab-on-Skin: A Review of Flexible and Stretchable Electronics for Wearable Health Monitoring. ACS Nano 2017, 11, 9614–9635. [Google Scholar] [CrossRef]
- Bandodkar, A.J.; Jeerapan, I.; Wang, J. Wearable Chemical Sensors: Present Challenges and Future Prospects. ACS Sens. 2016, 1, 464–482. [Google Scholar] [CrossRef]
- Mannoor, M.S.; Tao, H.; Clayton, J.D.; Sengupta, A.; Kaplan, D.L.; Naik, R.R.; Verma, N.; Omenetto, F.G.; McAlpine, M.C. Graphene-based wireless bacteria detection on tooth enamel. Nat. Commun. 2012, 3, 763. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Valdes-Ramirez, G.; Bandodkar, A.J.; Jia, W.Z.; Martinez, A.G.; Ramirez, J.; Mercier, P.; Wang, J. Non-invasive mouthguard biosensor for continuous salivary monitoring of metabolites. Analyst 2014, 139, 1632–1636. [Google Scholar] [CrossRef]
- Kim, J.; Imani, S.; de Araujo, W.R.; Warchall, J.; Valdes-Ramirez, G.; Paixao, T.; Mercier, P.P.; Wang, J. Wearable salivary uric acid mouthguard biosensor with integrated wireless electronics. Biosens. Bioelectron. 2015, 74, 1061–1068. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yao, H.F.; Shum, A.J.; Cowan, M.; Lahdesmaki, I.; Parviz, B.A. A contact lens with embedded sensor for monitoring tear glucose level. Biosens. Bioelectron. 2011, 26, 3290–3296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- diaTribe. Google Secures Patent for Glucose-Sensing Contact Lens. Available online: https://diatribe.org/google-secures-patent-glucose-sensing-sontact-lens (accessed on 1 October 2018).
- FierceBiotech. Available online: https://www.fiercebiotech.com/r-d/novartis-chairman-google-smart-lens-a-high-risk-project (accessed on 1 October 2018).
- Rodbard, D. Continuous Glucose Monitoring: A Review of Successes, Challenges, and Opportunities. Diabetes Technol. Ther. 2016, 18, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, A.; Utsunomiya, F.; Douseki, T. Wearable Self-Powered Diaper-Shaped Urinary-Incontinence Sensor Suppressing Response-Time Variation with 0.3 V Start-Up Converter. IEEE Sens. J. 2016, 16, 3472–3479. [Google Scholar] [CrossRef]
- Nyein, H.Y.Y.; Tai, L.C.; Ngo, Q.P.; Chao, M.H.; Zhang, G.B.; Gao, W.; Bariya, M.; Bullock, J.; Kim, H.; Fahad, H.M.; et al. A Wearable Microfluidic Sensing Patch for Dynamic Sweat Secretion Analysis. ACS Sens. 2018, 3, 944–952. [Google Scholar] [CrossRef] [PubMed]
- Nyein, H.Y.Y.; Gao, W.; Shahpar, Z.; Emaminejad, S.; Challa, S.; Chen, K.; Fahad, H.M.; Tai, L.C.; Ota, H.; Davis, R.W.; et al. A Wearable Electrochemical Platform for Noninvasive Simultaneous Monitoring of Ca2+ and pH. ACS Nano 2016, 10, 7216–7224. [Google Scholar] [CrossRef]
- Matzeu, G.; O’Quigley, C.; McNamara, E.; Zuliani, C.; Fay, C.; Glennon, T.; Diamond, D. An integrated sensing and wireless communications platform for sensing sodium in sweat. Anal. Methods 2016, 8, 64–71. [Google Scholar] [CrossRef]
- Alizadeh, A.; Burns, A.; Lenigk, R.; Gettings, R.; Ashe, J.; Porter, A.; McCaul, M.; Barrett, R.; Diamond, D.; White, P.; et al. A wearable patch for continuous monitoring of sweat electrolytes during exertion. Lab Chip 2018, 18, 2632–2641. [Google Scholar] [CrossRef]
- Lewenstam, A.; Majzurawska, M.; Hulanicki, A. Application of Ion-Selective Electrodes in Clinical Analysis. Electroanalysis 1991, 3, 727–734. [Google Scholar] [CrossRef]
- Tudos, A.J.; Besselink, G.A.J.; Schasfoort, R.B.M. Trends in miniaturized total analysis systems for point-of-care testing in clinical chemistry. Lab Chip 2001, 1, 83–95. [Google Scholar] [CrossRef] [PubMed]
- Hoekstra, R.; Blondeau, P.; Andrade, F.J. IonSens: A Wearable Potentiometric Sensor Patch for Monitoring Total Ion Content in Sweat. Electroanalysis 2018, 30, 1536–1544. [Google Scholar] [CrossRef]
- Glennon, T.; O’Quigley, C.; McCaul, M.; Matzeu, G.; Beirne, S.; Wallace, G.G.; Stroiescu, F.; O’Mahoney, N.; White, P.; Diamond, D. ‘SWEATCH’: A Wearable Platform for Harvesting and Analysing Sweat Sodium Content. Electroanalysis 2016, 28, 1283–1289. [Google Scholar] [CrossRef]
- Choi, D.-H.; Kim, J.S.; Cutting, G.R.; Searson, P.C. Wearable Potentiometric Chloride Sweat Sensor: The Critical Role of the Salt Bridge. Anal. Chem. 2016, 88, 12241–12247. [Google Scholar] [CrossRef]
- Guinovart, T.; Bandodk, A.J.; Windmiller, J.R.; Andrade, F.J.; Wang, J. A potentiometric tattoo sensor for monitoring ammonium in sweat. Analyst 2013, 138, 7031–7038. [Google Scholar] [CrossRef] [PubMed]
- Bandodkar, A.J.; Jia, W.Z.; Wang, J. Tattoo-Based Wearable Electrochemical Devices: A Review. Electroanalysis 2015, 27, 562–572. [Google Scholar] [CrossRef]
- Parrilla, M.; Canovas, R.; Jeerapan, I.; Andrade, F.J.; Wang, J. A Textile-Based Stretchable Multi-Ion Potentiometric Sensor. Adv. Health Mater. 2016, 5, 996–1001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guinovart, T.; Valdes-Ramirez, G.; Windmiller, J.R.; Andrade, F.J.; Wang, J. Bandage-Based Wearable Potentiometric Sensor for Monitoring Wound pH. Electroanalysis 2014, 26, 1345–1353. [Google Scholar] [CrossRef]
- Rahimi, R.; Ochoa, M.; Parupudi, T.; Zhao, X.; Yazdi, I.K.; Dokmeci, M.R.; Tamayol, A.; Khademhosseini, A.; Ziaie, B. A low-cost flexible pH sensor array for wound assessment. Sens. Actuators B Chem. 2016, 229, 609–617. [Google Scholar] [CrossRef] [Green Version]
- Garcia, M.S.; Ortuno, J.; Albero, M.I.; Cuartero, M. Application of a trazodone-selective electrode to pharmaceutical quality control and urine analyses. Anal. Bioanal. Chem. 2009, 394, 1563–1567. [Google Scholar] [CrossRef]
- Chung, H.J.; Sulkin, M.S.; Kim, J.S.; Goudeseune, C.; Chao, H.Y.; Song, J.W.; Yang, S.Y.; Hsu, Y.Y.; Ghaffari, R.; Efimov, I.R.; et al. Stretchable, Multiplexed pH Sensors With Demonstrations on Rabbit and Human Hearts Undergoing Ischemia. Adv. Health Mater. 2014, 3, 59–68. [Google Scholar] [CrossRef]
- Tahirbegi, I.B.; Mir, M.; Schostek, S.; Schurr, M.; Samitier, J. In vivo ischemia monitoring array for endoscopic surgery. Biosens. Bioelectron. 2014, 61, 124–130. [Google Scholar] [CrossRef]
- Mostafalu, P.; Akbari, M.; Alberti, K.A.; Xu, Q.B.; Khademhosseini, A.; Sonkusale, S.R. A toolkit of thread-based microfluidics, sensors, and electronics for 3D tissue embedding for medical diagnostics. Microsyst. Nanoeng. 2016, 2, 16039. [Google Scholar] [CrossRef] [Green Version]
- Emaminejad, S.; Gao, W.; Wu, E.; Davies, Z.A.; Nyein, H.Y.Y.; Challa, S.; Ryan, S.P.; Fahad, H.M.; Chen, K.; Shahpar, Z.; et al. Autonomous sweat extraction and analysis applied to cystic fibrosis and glucose monitoring using a fully integrated wearable platform. Proc. Natl. Acad. Sci. USA 2017, 114, 4625–4630. [Google Scholar] [CrossRef] [Green Version]
- Gonzalo-Ruiz, J.; Mas, R.; de Haro, C.; Cabruja, E.; Camero, R.; Alonso-Lomillo, M.A.; Munoz, F.J. Early determination of cystic fibrosis by electrochemical chloride quantification in sweat. Biosens. Bioelectron. 2009, 24, 1788–1791. [Google Scholar] [CrossRef]
- Choi, D.H.; Thaxton, A.; Jeong, I.C.; Kim, K.; Sosnay, P.R.; Cutting, G.R.; Searson, P.C. Sweat test for cystic fibrosis: Wearable sweat sensor vs. standard laboratory test. J. Cyst. Fibros. 2018, 17, e35–e38. [Google Scholar] [CrossRef]
- Choi, D.H.; Li, Y.; Cutting, G.R.; Searson, P.C. A wearable potentiometric sensor with integrated salt bridge for sweat chloride measurement. Sens. Actuators B Chem. 2017, 250, 673–678. [Google Scholar]
- Parrilla, M.; Cuartero, M.; Padrell, S.; Rajabi, M.; Roxhed, N.; Niklaus, F.; Crespo, G.A. Wearable All-Solid-State Potentiometric Microneedle Patch for Intradermal Potassium Detection. Anal. Chem. 2019, in press. [Google Scholar] [CrossRef]
- Lee, Y.; How, C.; Mishra, S.; Lee, D.S.; Mahmood, M.; Piper, M.; Kim, Y.; Tieu, K.; Byun, H.S.; Coffey, J.P.; et al. Wireless, intraoral hybrid electronics for real-time quantification of sodium intake toward hypertension management. Proc. Natl. Acad. Sci. USA 2018, 115, 5377–5382. [Google Scholar] [CrossRef]
- Shukla, V.K.; Shukla, D.; Tiwary, S.K.; Agrawal, S.; Rastogi, A. Evaluation of pH measurement as a method of wound assessment. J. Wound Care 2007, 16, 291–294. [Google Scholar] [CrossRef]
- Ono, S.; Imai, R.; Ida, Y.; Shibata, D.; Komiya, T.; Matsumura, H. Increased wound pH as an indicator of local wound infection in second degree burns. Burns 2015, 41, 820–824. [Google Scholar] [CrossRef]
- Farrell, P.M.; White, T.B.; Ren, C.L.; Hempstead, S.E.; Accurso, F.; Derichs, N.; Howenstine, M.; McColley, S.A.; Rock, M.; Rosenfeld, M.; et al. Diagnosis of Cystic Fibrosis: Consensus Guidelines from the Cystic Fibrosis Foundation. J. Pediatr. 2017, 181, S4–S15. [Google Scholar] [CrossRef]
- Simmer, P.; Li, S.K.; Kasting, G.; Heikenfeld, J. Prolonged and localized sweat stimulation by iontophoretic delivery of the slowly-metabolized cholinergic agent carbachol. J. Dermatol. Sci. 2018, 89, 40–51. [Google Scholar] [CrossRef]
- Augarten, A.; Hacham, S.; Kerem, E.; Kerem, B.S.; Szeinberg, A.; Laufer, J.; Doolman, R.; Altshuler, R.; Blau, H.; Bentur, L.; et al. The significance of sweat Cl/Na ratio in patients with borderline sweat test. Pediatr. Pulmonol. 1995, 20, 369–371. [Google Scholar] [CrossRef]
- Miller, P.R.; Xiao, X.Y.; Brener, I.; Burckel, D.B.; Narayan, R.; Polsky, R. Microneedle-Based Transdermal Sensor for On-Chip Potentiometric Determination of K+. Adv. Health Mater. 2014, 3, 876–881. [Google Scholar] [CrossRef]
- Cuartero, M.; Ortuno, J.A.; Garcia, M.S.; Sanchez, G.; Mas-Montoya, M.; Curiel, D. Benzodipyrrole derivates as new ionophores for anion-selective electrodes: Improving potentiometric selectivity towards divalent anions. Talanta 2011, 85, 1876–1881. [Google Scholar] [CrossRef]
- Hauke, A.; Simmers, P.; Osha, Y.R.; Cameron, B.D.; Ballweg, R.; Zhang, T.; Twine, N.; Brothers, M.; Gomez, E.; Heikenfeld, J. Complete validation of a continuous and blood-correlated sweat biosensing device with integrated sweat stimulation. Lab Chip 2018, 18, 3750–3759. [Google Scholar] [CrossRef]
- Simmers, P.; Yuan, Y.; Sonner, Z.; Heikenfeld, J. Membrane isolation of repeated-use sweat stimulants for mitigating both direct dermal contact and sweat dilution. Biomicrofluidics 2018, 12, 034101. [Google Scholar] [CrossRef]
- Sonner, Z.; Wilder, E.; Gaillard, T.; Kasting, G.; Heikenfeld, J. Integrated sudomotor axon reflex sweat stimulation for continuous sweat analyte analysis with individuals at rest. Lab Chip 2017, 17, 2550–2560. [Google Scholar] [CrossRef]
- Cuartero, M.; Crespo, G.; Cherubini, T.; Pakratova, N.; Massa, F.; Confalonieri, F.; Tercier-Waeber, M.; Abdou, M.; Schafer, J.; Bakker, E. In situ detection of macronutrients and chloride in seawater by submersible electrochemical sensors. Anal. Chem. 2018, 9, 4702–4710. [Google Scholar] [CrossRef]
- Cuartero, M.; Pankratova, N.; Cherubini, T.; Crespo, G.A.; Massa, F.; Confalonieri, F.; Bakker, E. In Situ Detection of Species Relevant to the Carbon Cycle in Seawater with Submersible Potentiometric Probes. Environ. Sci. Technol. Lett. 2017, 4, 410–415. [Google Scholar] [CrossRef]
- Meier, P.C. Two-parameter Debye-Huckel approximation for the evaluation of mean activity coefficients of 109 electrolytes. Anal. Chim. Acta 1982, 136, 363–368. [Google Scholar] [CrossRef]
- Zou, X.U.; Zhen, X.V.; Cheong, J.H.; Buhlmann, P. Calibration-Free Ionophore-Based Ion-Selective Electrodes With a Co(II)/Co(III) Redox Couple-Based Solid Contact. Anal. Chem. 2014, 86, 8687–8692. [Google Scholar] [CrossRef]
- Vanamo, U.; Bobacka, J. Electrochemical control of the standard potential of solid-contact ion-selective electrodes having a conducting polymer as ion-to-electron transducer. Electrochim. Acta 2014, 122, 316–321. [Google Scholar] [CrossRef]
- Vanamo, U.; Bobacka, J. Instrument-Free Control of the Standard Potential of Potentiometric Solid-Contact Ion-Selective Electrodes by Short-Circuiting with a Conventional Reference Electrode. Anal. Chem. 2014, 86, 10540–10545. [Google Scholar] [CrossRef]
- Cuartero, M.; Crespo, G.A.; Bakker, E. Thin Layer Samples Controlled by Dynamic Electrochemistry. Chimia 2015, 69, 203–206. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Analyte | Platform | Sensor | Working Range | Application | Medical Information | Sample Collection | Real Tests | Ref. |
|---|---|---|---|---|---|---|---|---|
| pH | Adhesive band aid | PANI | 5–8 | Wound | Wound healing a | No | No b | [51] |
| pH | Polymer-coated paper | PANI | 4–10 | Wound | Wound assessment a | No | No | [52] |
| pH | Elastomer | IrOx | 4–10 | Heart | Ischemia-reperfusion | Explanted heart | Rabbit and human heart c | [54] |
| pH | Beryllium copper alloy pins d | pH-SM KSM | 0.7–1.5 0.1–10 mM | Gastric mucosa | Ischemia-reperfusion | No | Pig stomach | [55] |
| pH | Conductive threads | PANI | 3.5–8 | Subcutaneous and gastric | Sutures and implants a | Wicking | Rats | [56] |
Cl− | PET | NaSM Ag/AgCl | 10–160 mM | Sweat | CF | Iontophoresis + pad | Healthy and CF patients | [57] |
| Cl− | Polyester | Ag/AgCl | 10–100 mM | Sweat | CF | Iontophoresis | CF patients | [58] |
| Cl− | PET | Ag/AgCl + bridge | 10–100 mM | Sweat | CF | Iontophoresis | Healthy and CF patients | [59,60] |
| MN (Steel) | KSM | 6·10−5–8·10−2 M | Interstitial fluid | K imbalance a | No e | Chicken skin c | [61] | |
| Dental retainer | NaSM | 1·10−3–1 M | Saliva | Hypertension management a | No | Drinking saline water | [62] |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cuartero, M.; Parrilla, M.; Crespo, G.A. Wearable Potentiometric Sensors for Medical Applications. Sensors 2019, 19, 363. https://doi.org/10.3390/s19020363
Cuartero M, Parrilla M, Crespo GA. Wearable Potentiometric Sensors for Medical Applications. Sensors. 2019; 19(2):363. https://doi.org/10.3390/s19020363
Chicago/Turabian StyleCuartero, María, Marc Parrilla, and Gaston A. Crespo. 2019. "Wearable Potentiometric Sensors for Medical Applications" Sensors 19, no. 2: 363. https://doi.org/10.3390/s19020363
APA StyleCuartero, M., Parrilla, M., & Crespo, G. A. (2019). Wearable Potentiometric Sensors for Medical Applications. Sensors, 19(2), 363. https://doi.org/10.3390/s19020363