Optimized Electrode Locations for Wearable Single-Lead ECG Monitoring Devices: A Case Study Using WFEES Modules Based on the LANS Method



Abstract
:1. Introduction
2. Materials and Methods
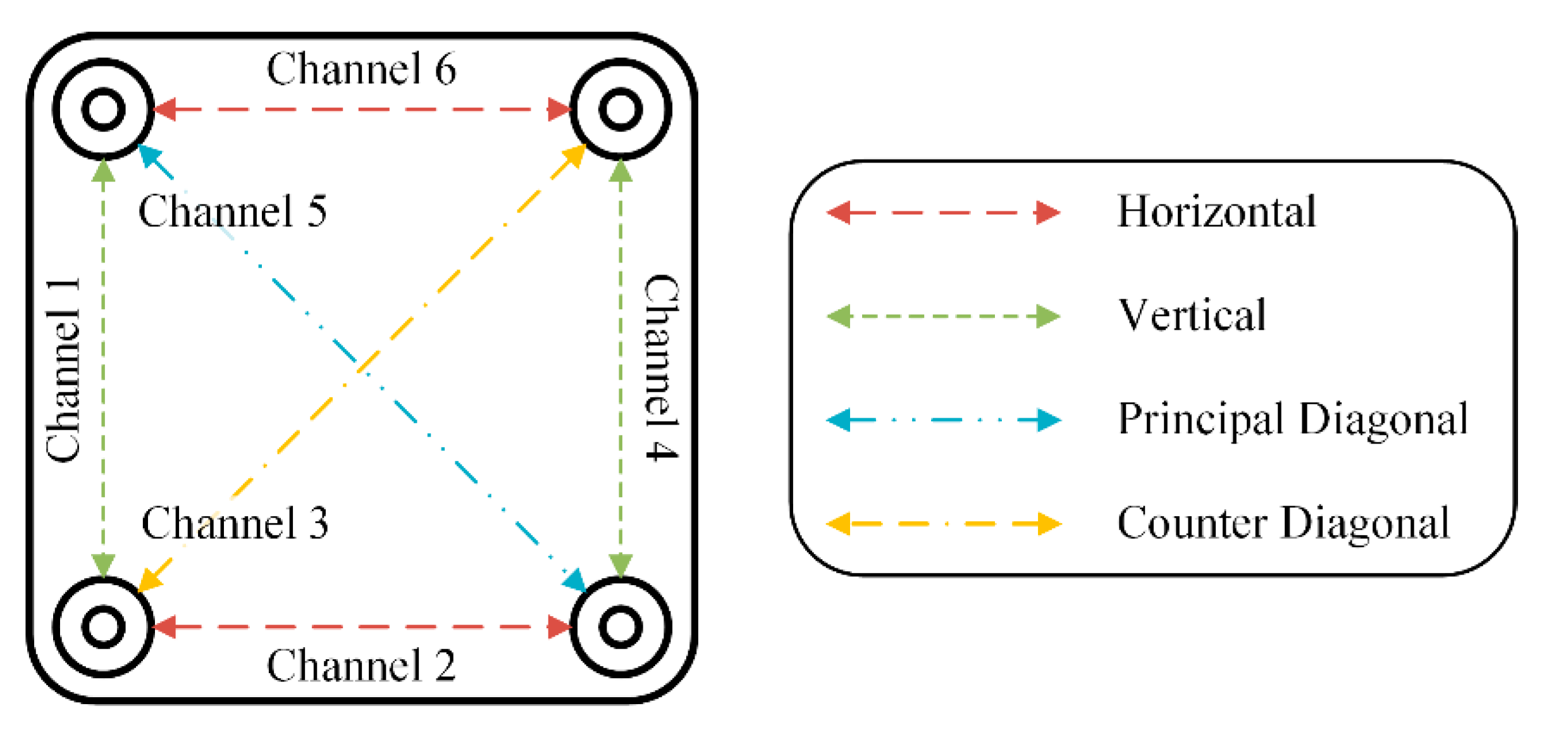
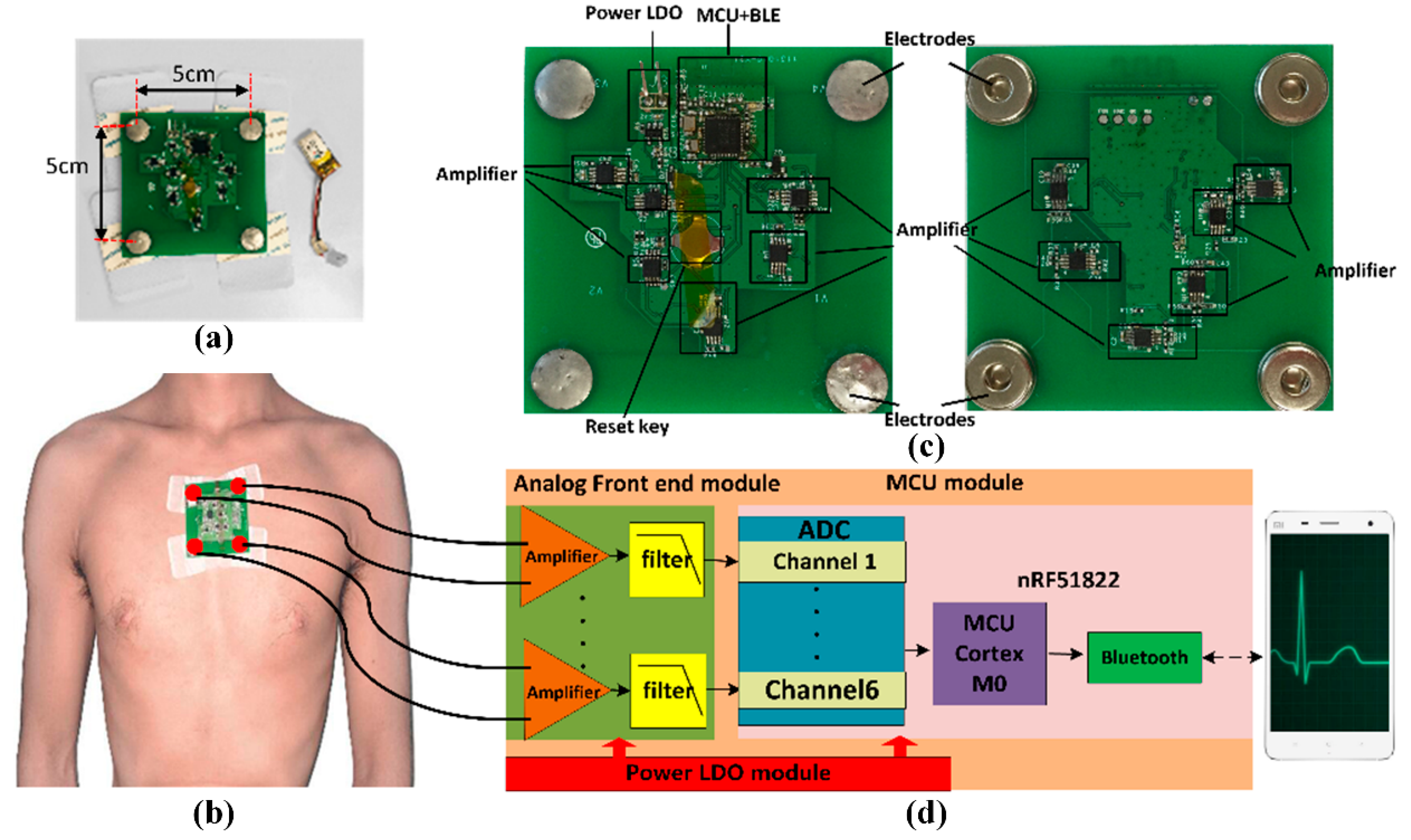
2.1. WFEES Module
2.2. LANS Method
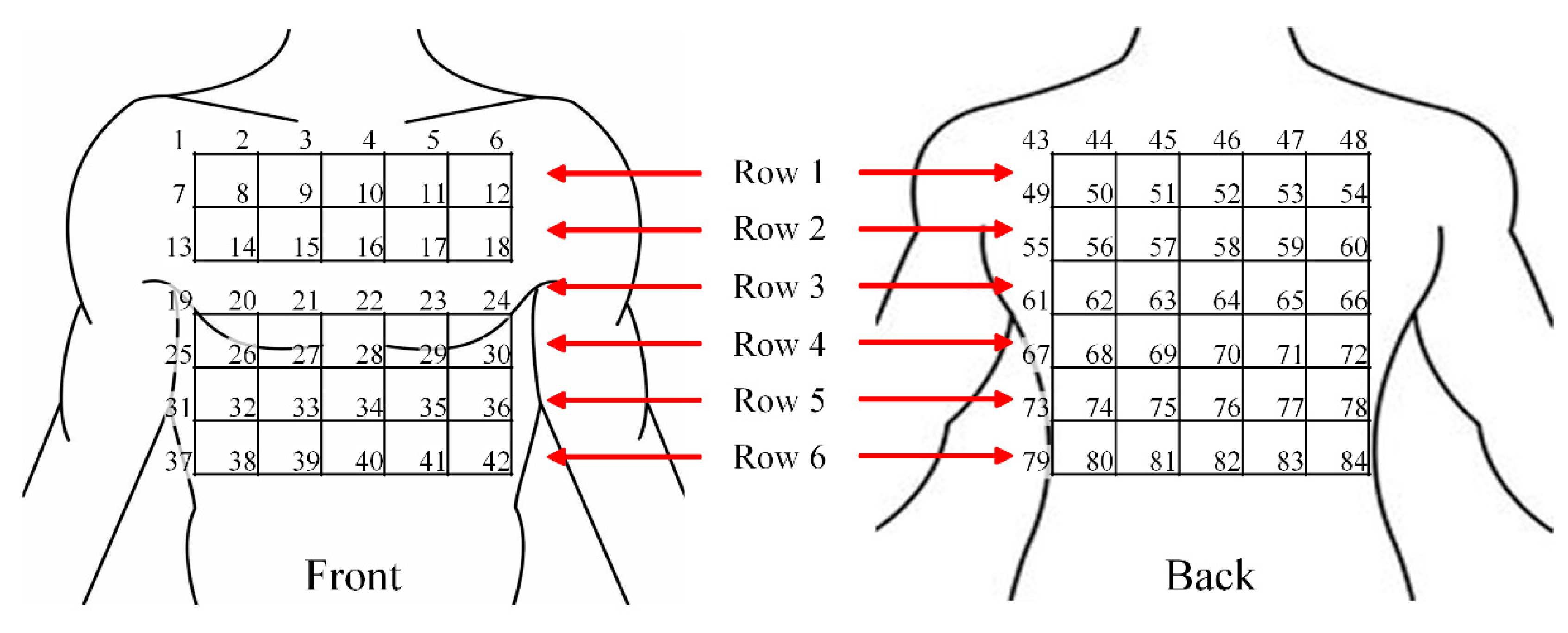
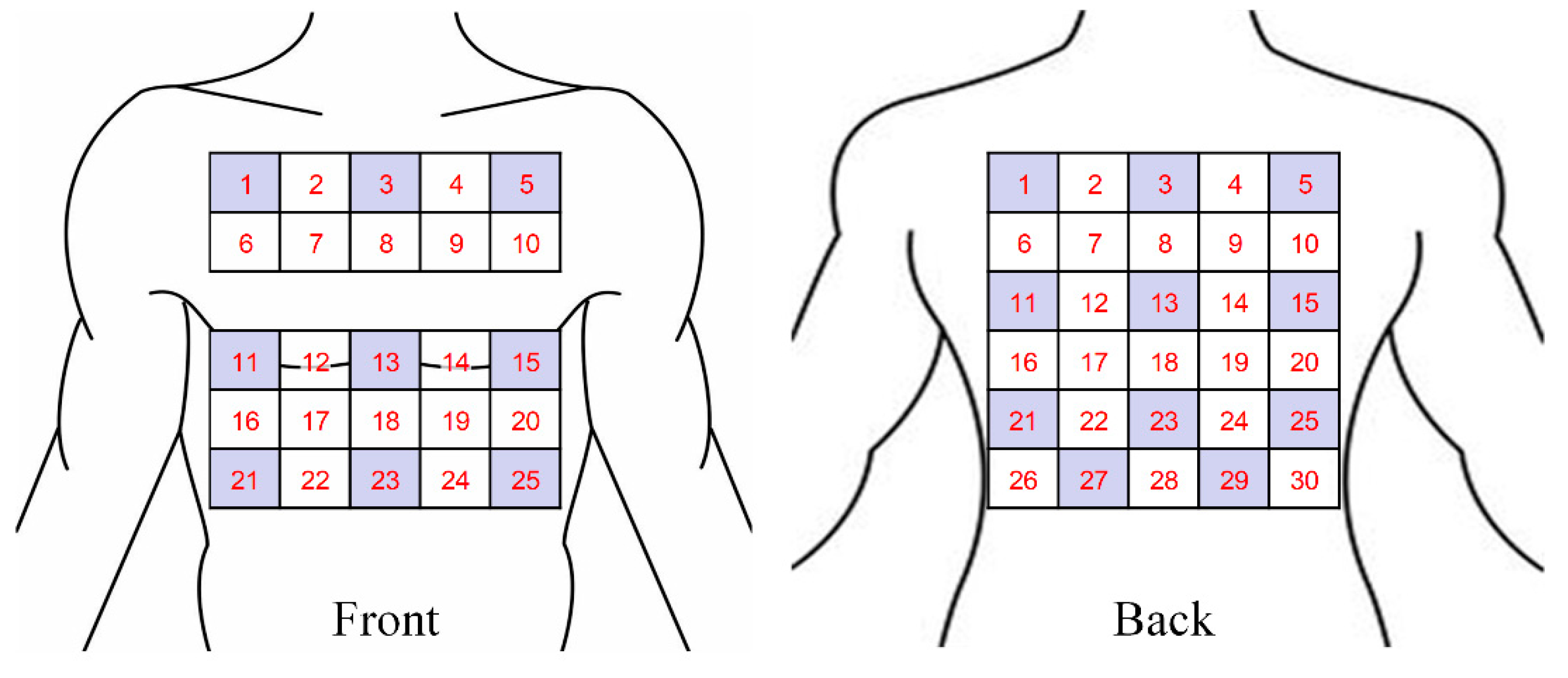
2.2.1. Torso Segmentation
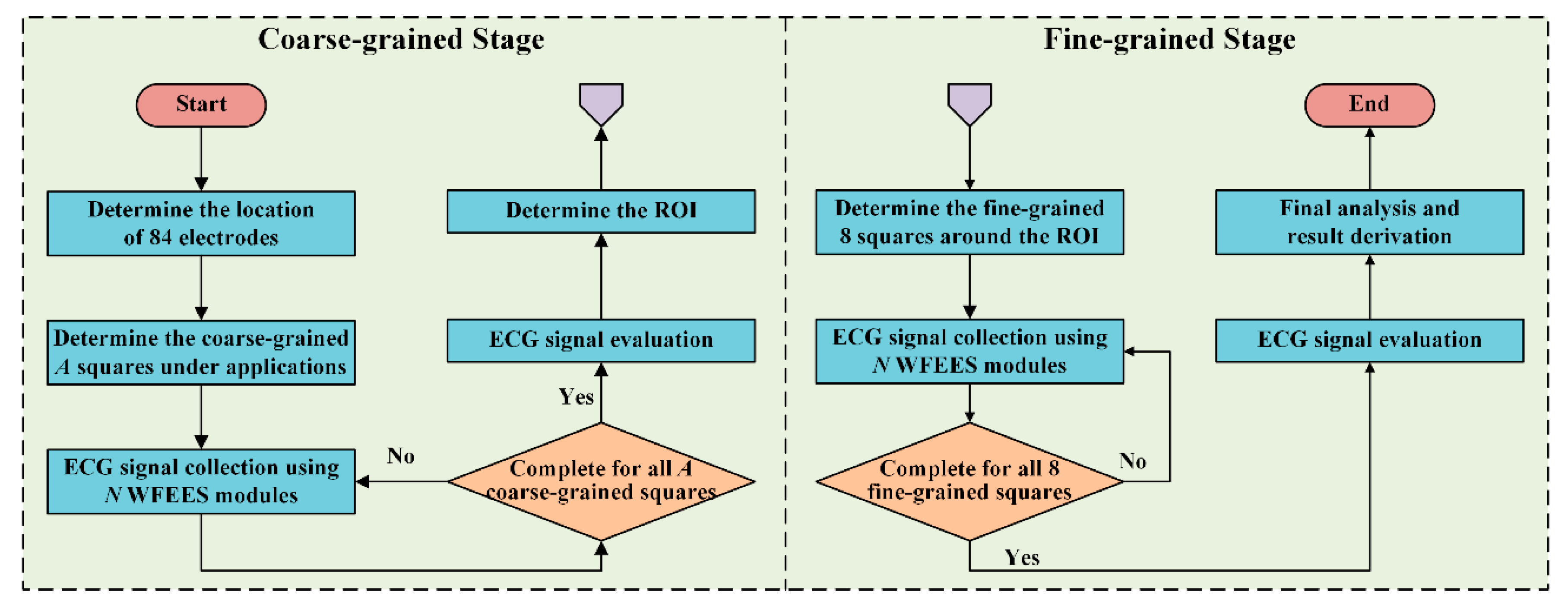
2.2.2. Layered (A, N) Square-based Method
2.3. Case Study: Optimized Electrode Locations Determination
2.3.1. Experimental Design
2.3.2. Study Population
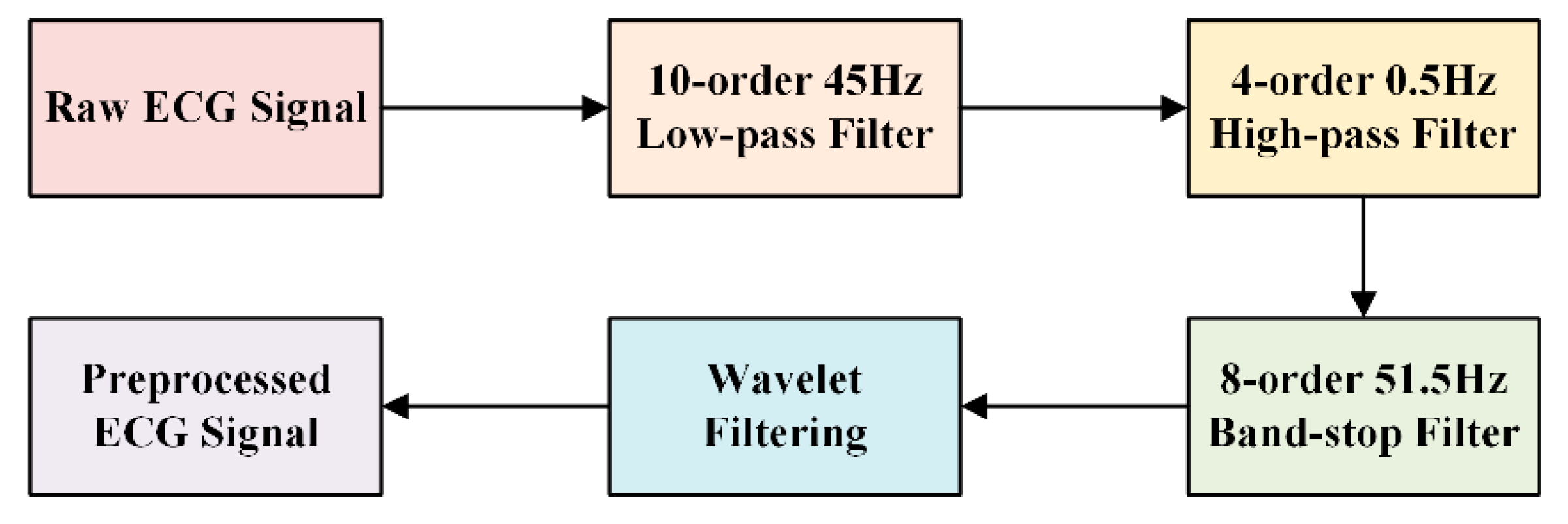
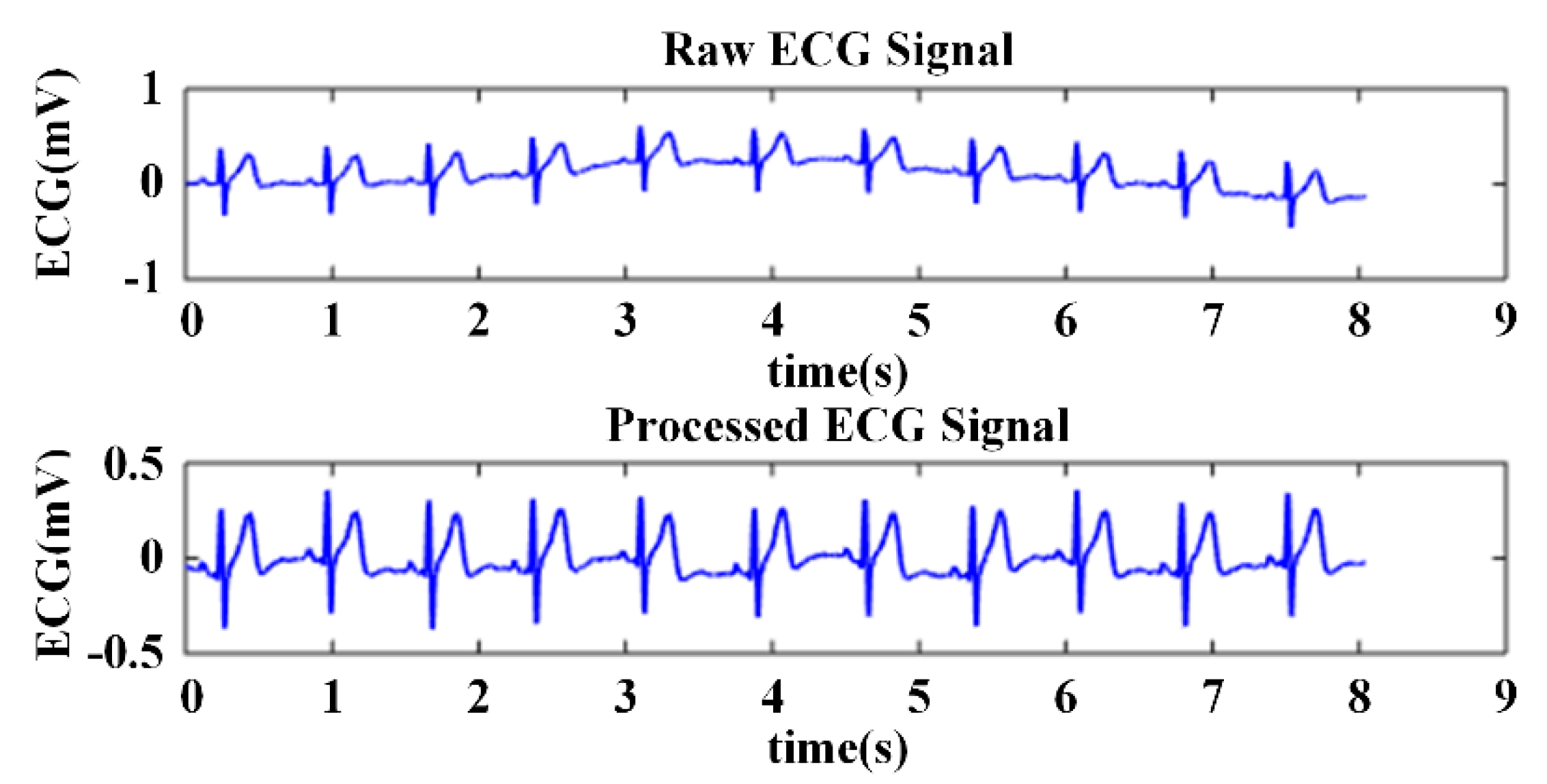
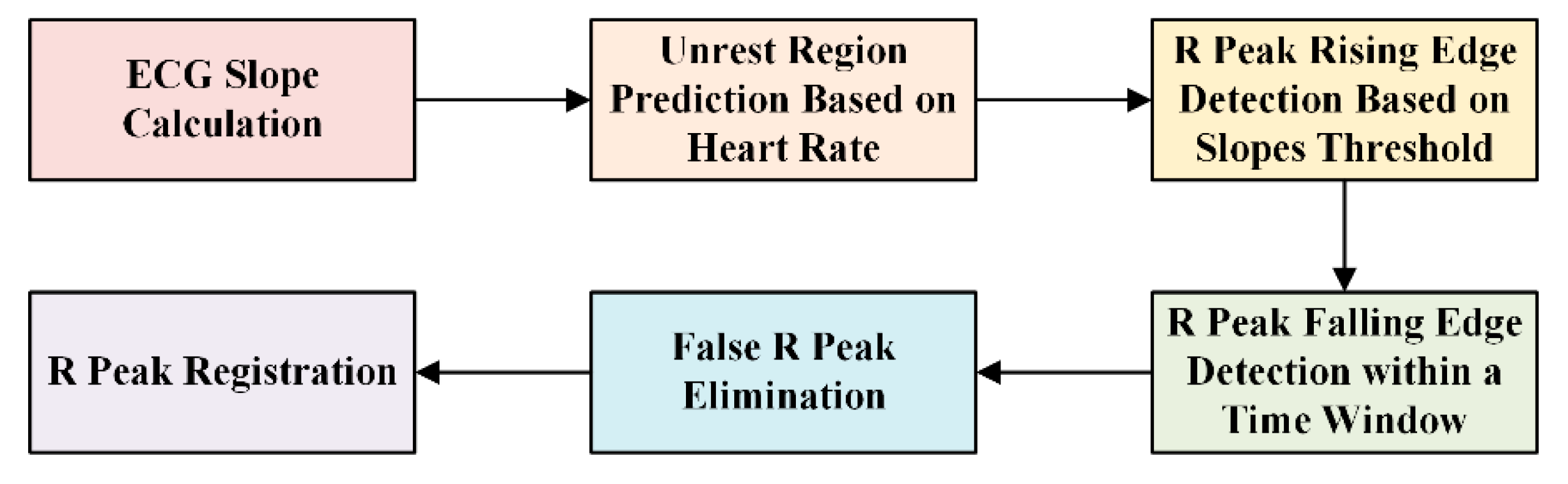
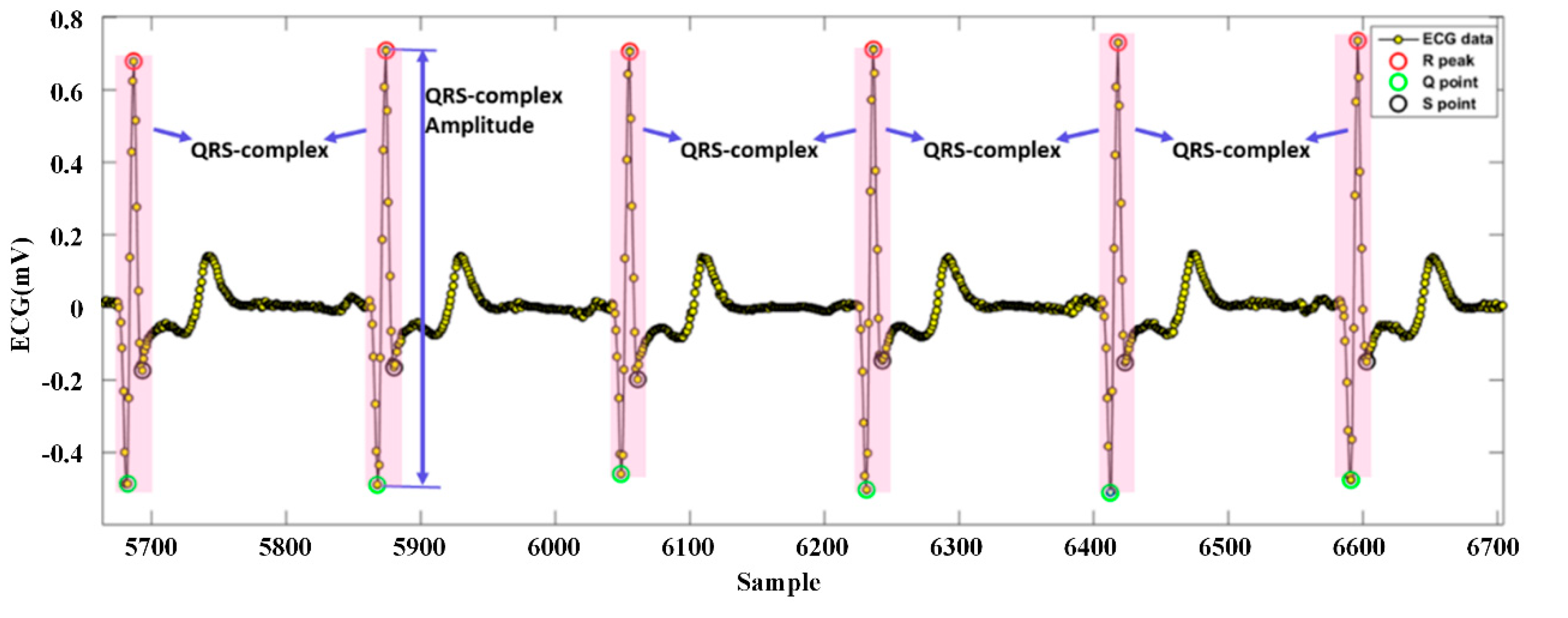
2.3.3. Signal Processing
2.3.4. Electrode Location Evaluation
3. Results
3.1. Improvement of WFEES Module and LANS Method
3.2. Optimized Electrode Location
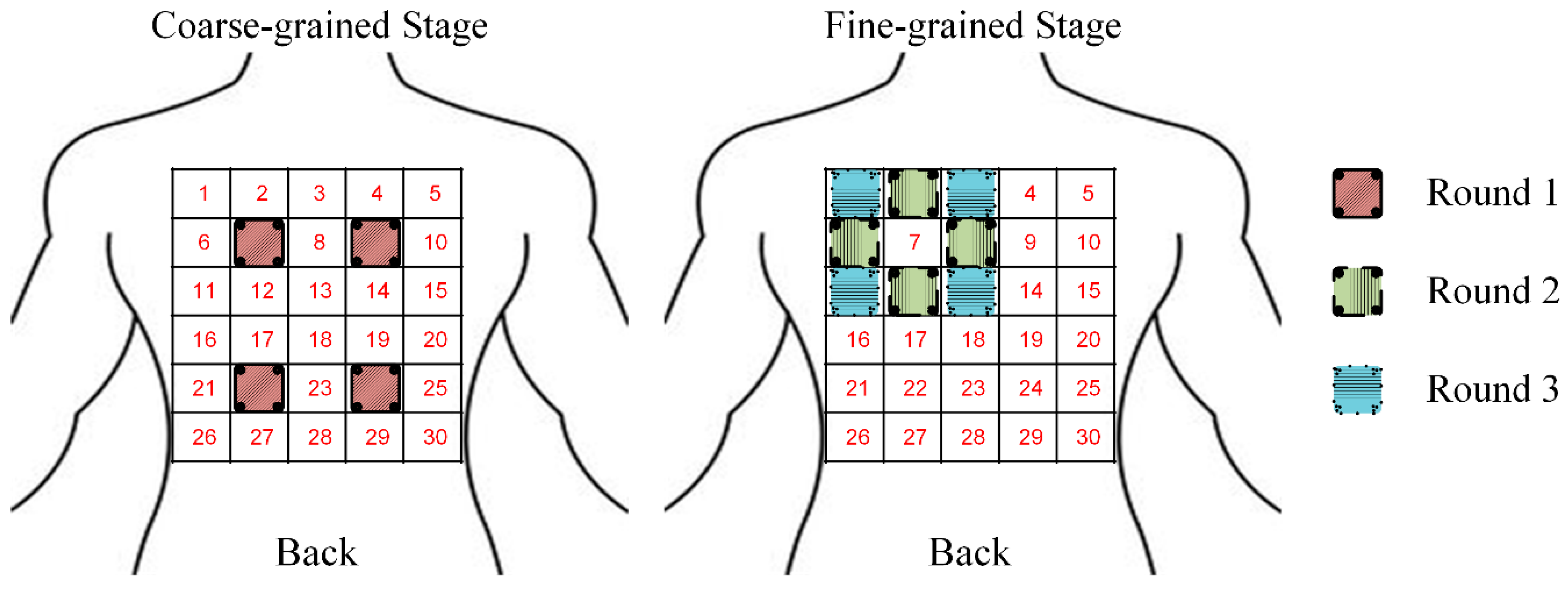
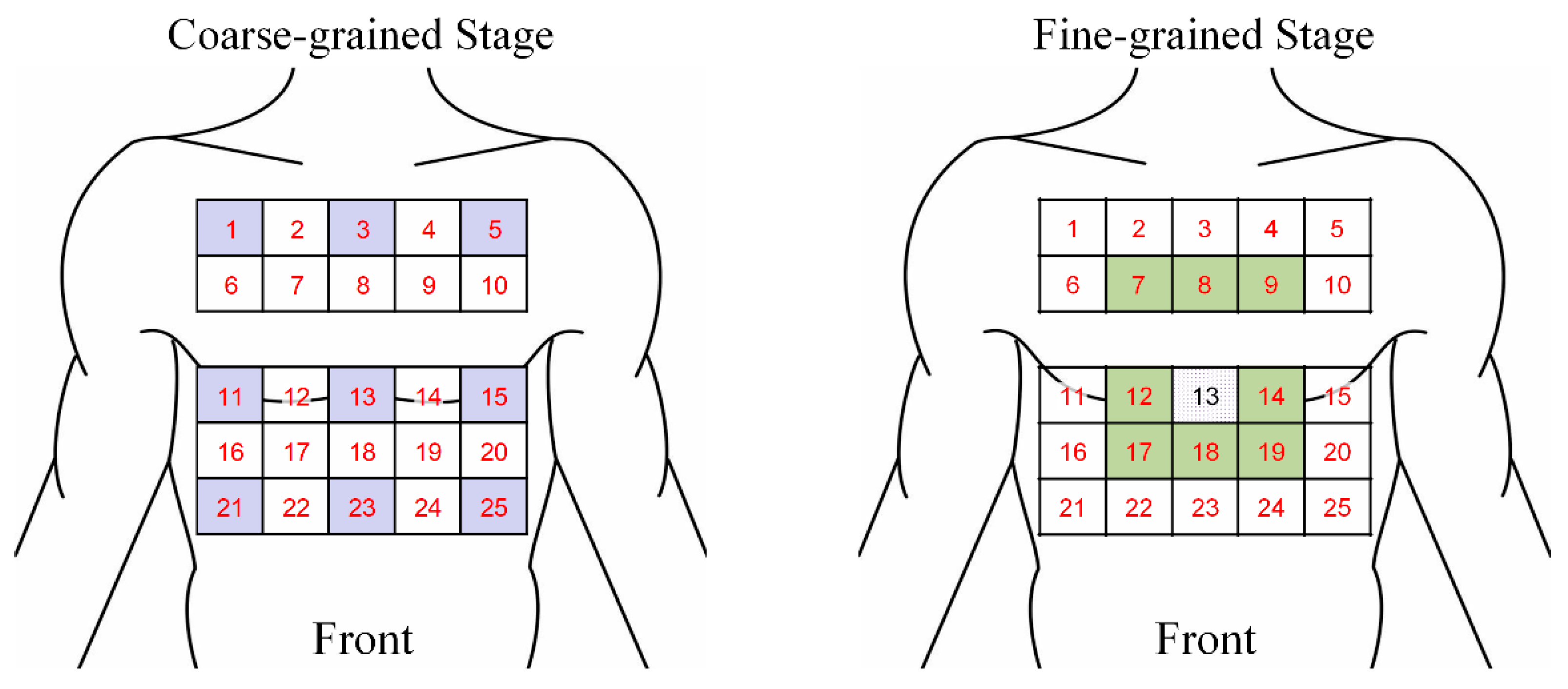
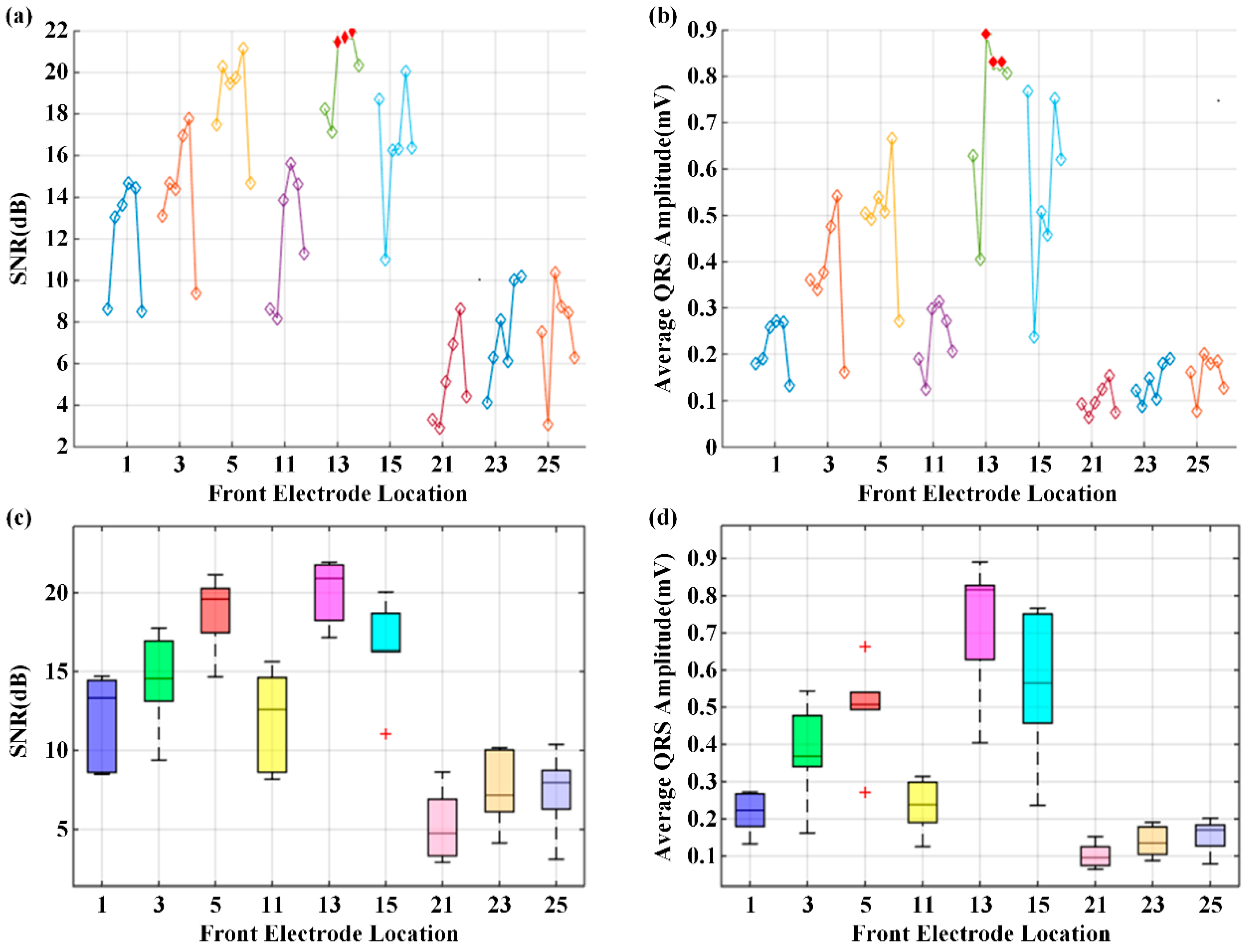
3.2.1. Coarse-Grained Stage for ROI Evaluation
3.2.2. Fine-Grained Stage to Determine the Optimal Electrode Location and Orientation
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Roth, G.A.; Johnson, C.; Abajobir, A.A.; Abd-Allah, F.; Abera, S.F.; Abyu, G.; Ahmed, M.; Aksut, B.; Alam, T.; Alam, K.; et al. Global, Regional, and National Burden of Cardiovascular Diseases for 10 Causes, 1990 to 2015. J. Am. Coll. Cardiol. 2017, 70, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Dilaveris, P.E.; Gialafos, E.J.; Sideris, S.K.; Theopistou, A.M.; Andrikopoulos, G.K.; Kyriakidis, M.; Gialafos, J.E.; Toutouzas, P.K. Simple electrocardiographic markers for the prediction of paroxysmal idiopathic atrial fibrillation. Am. Hear. J. 1998, 135, 733–738. [Google Scholar] [CrossRef]
- Reichlin, T.; Abächerli, R.; Twerenbold, R.; Kühne, M.; Schaer, B.; Müller, C.; Sticherling, C.; Osswald, S. Advanced ECG in 2016: Is there more than just a tracing? Swiss Med. Wkly. 2016, 146, w14303. [Google Scholar] [CrossRef] [PubMed]
- Guillem, M.S.; Millet, J.; Bodí, V.; Mora, C.; Chorro, F.J. Integration of a body surface potential mapping system. In Proceedings of the X Mediterranean Conference on Medical and Biological Engineering, Ischia, Italy, 31 July–5 August 2004. [Google Scholar]
- Kontos, M.C. Body Surface Potential Mapping and Left Circumflex Occlusion: Unmasking the Hidden Acute Myocardial Infarction. J. Am. Hear. Assoc. 2019, 8, 012417. [Google Scholar] [CrossRef]
- Giffard-Roisin, S.; Jackson, T.; Fovargue, L.; Lee, J.; Delingette, H. Noninvasive personalization of a cardiac electrophysiology model from body surface potential mapping. IEEE Trans. Biomed. Eng. 2016, 64, 2206–2218. [Google Scholar] [CrossRef] [PubMed]
- Ben Johnson, W.; Vatterott, P.J.; Peterson, M.A.; Bagwe, S.; Underwood, R.D.; Bank, A.J.; Gage, R.M.; Ramza, B.; Foreman, B.W.; Splett, V.; et al. Body surface mapping using an ECG belt to characterize electrical heterogeneity for different left ventricular pacing sites during cardiac resynchronization: Relationship with acute hemodynamic improvement. Hear. Rhythm. 2017, 14, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Potyagaylo, D.; Chmelevsky, M.; Zubarev, S.; Budanova, M.; Kalinin, V.; Kalinin, A.; and Lebedev, D. Evaluation of ECGI localization accuracy for single pacings in CRT patients. In Proceedings of the 2018 Computing in Cardiology Conference, Maastricht, The Netherlands, 23–26 September 2018. [Google Scholar]
- Kornreich, F. Clinical Utility of Body Surface Potential Mapping. Card. Electrophysiol. Rev. 1997, 1, 304–307. [Google Scholar] [CrossRef]
- Yang, Z.; Zhou, Q.; Lei, L.; Zheng, K.; Xiang, W. An IoT-cloud Based Wearable ECG Monitoring System for Smart Healthcare. J. Med. Syst. 2016, 40, 286. [Google Scholar] [CrossRef] [PubMed]
- Pani, D.; Dessì, A.; Saenz-Cogollo, J.F.; Barabino, G.; Fraboni, B.; Bonfiglio, A. Fully textile, PEDOT: PSS based electrodes for wearable ECG monitoring systems. IEEE Trans. Biomed. Eng. 2016, 63, 540–549. [Google Scholar] [CrossRef] [PubMed]
- Spano, E.; Di Pascoli, S.; Iannaccone, G. Low-Power Wearable ECG Monitoring System for Multiple-Patient Remote Monitoring. IEEE Sens. J. 2016, 16, 5452–5462. [Google Scholar] [CrossRef]
- Chen, C.L.; Chuang, C.T. A QRS detection and R point recognition method for wearable single-lead ECG devices. Sensors 2016, 17, 1969. [Google Scholar] [CrossRef] [PubMed]
- Keshishzadeh, S.; Rashidi, S. Single lead Electrocardiogram feature extraction for the human verification. In Proceedings of the 2015 5th International Conference on Computer and Knowledge Engineering (ICCKE), Changsha, China, 20–21 June 2015; pp. 118–122. [Google Scholar]
- Sadr, N.; Chazal, P.D. Automated detection of obstructive sleep apnoea by single-lead ECG through ELM classification. In Proceedings of the 2014 Computing in Cardiology Conference, Sydney, Australia, 1–3 October 2014. [Google Scholar]
- Bowers, E.; Murray, A.; Langley, P. Respiratory rate derived from principal component analysis of single lead electrocardiogram. In Proceedings of the 2008 Computers in Cardiology, Bologna, Italy, 14–17 September 2008; pp. 437–440. [Google Scholar]
- Hannun, A.Y.; Rajpurkar, P.; Haghpanahi, M.; Tison, G.H.; Bourn, C.; Turakhia, M.P.; Ng, A.Y. Cardiologist-level arrhythmia detection and classification in ambulatory electrocardiograms using a deep neural network. Nat. Med. 2019, 25, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Puurtinen, M.; Hyttinen, J.; Viik, J.; Kauppinen, P.; Malmivuo, J. Estimation of ECG signal of closely separated bipolar electrodes using thorax models. In Proceedings of the 26th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Francisco, CA, USA, 1–5 September 2004. [Google Scholar]
- Puurtinen, M.; Hyttinen, J.; Malmivuo, J. Optimizing bipolar electrode location for wireless ECG measurement–analysis of ECG signal strength and deviation between individuals. Int. J. Bioelectromagn. 2005, 7, 236–239. [Google Scholar]
- Donnelly, M.P.; Finlay, D.D.; Nugent, C.D.; Black, N.D. Lead selection: Old and new methods for locating the most electrocardiogram information. J. Electrocardiol. 2008, 41, 257–263. [Google Scholar] [CrossRef]
- Lux, R.L.; Greg, R. New leads for P wave detection and arrhythmia classification. J. Electrocardiol. 2004, 37, 80. [Google Scholar] [CrossRef]
- Puurtinen, M.; Viik, J.; Hyttinen, J. Best electrode locations for a small bipolar ECG device: Signal strength analysis of clinical data. Ann. Biomed. Eng. 2009, 37, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Väisänen, J.; Puurtinen, M.; Viik, J.; Hyttinen, J. New Bipolar ECG Electrode Locations in Differentiating Subjects with Left Ventricular Hypertrophy from Normal Subjects. In Proceedings of the 2009 World Congress on Medical Physics and Biomedical Engineering, Munich, Germany, 7–12 September 2009; pp. 848–850. [Google Scholar]
- Riistama, J.; Väisänen, J.; Heinisuo, S.; Harjunpää, H.; Arra, S. Wireless and inductively powered implant for measuring electrocardiogram. Med Biol. Eng. Comput. 2007, 45, 1163–1174. [Google Scholar] [CrossRef] [PubMed]
- Guillem, M.S.; Castells, F.; Climent, A.M.; Bodí, V.; Chorro, F.J.; Millet, J. Evaluation of lead selection methods for optimal reconstruction of body surface potentials. J. Electrocardiol. 2008, 41, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Chinese National Standard. GB10000-88: Human Dimension of Chinese Adults; Chinese National Standardization Institute: Beijing, China, 1988.
- Lin, H.-Y.; Liang, S.-Y.; Ho, Y.-L.; Lin, Y.-H.; Ma, H.-P. Discrete-wavelet-transform-based noise reduction and R wave detection for ECG signals. In Proceedings of the 2013 IEEE 15th International Conference on e-Health Networking, Applications and Services (Healthcom 2013), Lisbon, Portugal, 9–12 October 2013; pp. 355–360. [Google Scholar]
- Li, K.; Chen, F.; Pan, Y.; Huan, R.; Cheng, K.-T. Real-time lossless ECG compression for low-power wearable medical devices based on adaptive region prediction. Electron. Lett. 2014, 50, 1904–1906. [Google Scholar] [CrossRef]
- Groot, A.; Bots, M.L.; Rutten, F.H.; Ruijter, H.M.D.; Numans, M.E.; Vaartjes, I. Measurement of ECG abnormalities and cardiovascular risk classification: A cohort study of primary care patients in the Netherlands. Br. J. Gen. Pract. 2015, 65, e1–e8. [Google Scholar] [CrossRef] [PubMed]

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| Electrode Distance (cm) | 5 |
| Gain (V/V) | 1000 |
| Frequency Range (Hz) | 0–150 |
| Sampling Rate (Hz) | 200 |
| Resolution (bit) | 10 |
| Wireless Protocol | BLE |
| System | Electrode Number | Testing Lead Number | Lead Form | Data Transfer | System Size | System Cost |
|---|---|---|---|---|---|---|
| BSPM [21] | n/a | 192 | Wire required | Wired | Large | High |
| BSPM [22] | 120 | 120 | Wire required | Wired | Large | High |
| BSPM [23] | 120 | 113 | Wire required | Wired | Large | High |
| WFEES | N × 4 | N × 6 | Wireless | Wireless | Small | Low |
| Method | Testing Lead Number | Measurement Complexity 1 |
|---|---|---|
| Direct Testing | 330 | ⌈55/N⌉ |
| LANS | (A + 8) × 6 | ⌈(A + 8)/N⌉ |
| Front Electrode Location | Electrode Pair | Average SNR (dB) 1 | Average QRS Amplitude (mV) 1 | CV of QRS Amplitude (%) |
|---|---|---|---|---|
| Square 7 | 8/15 | 16.82 ± 4.75 | 0.42 ± 0.17 | 0.400 |
| Square 8 | 9/16 | 22.64 ± 3.67 | 1.10 ± 0.53 | 0.485 |
| Square 9 | 10/17 | 23.17 ± 2.25 | 1.05 ± 0.45 | 0.428 |
| Square 12 | 20/27 | 19.20 ± 5.28 | 0.56 ± 0.42 | 0.745 |
| Square 13 | 21/28 | 21.66 ± 3.09 | 0.82 ± 0.38 | 0.468 |
| Square 14 | 22/29 | 21.93 ± 5.47 | 1.08 ± 0.71 | 0.653 |
| Square 17 | 26/33 | 15.39 ± 4.11 | 0.29 ± 0.20 | 0.706 |
| Square 18 | 27/34 | 15.91 ± 3.28 | 0.37 ± 0.16 | 0.432 |
| Square 19 | 28/35 | 13.18 ± 6.01 | 0.27 ± 0.14 | 0.508 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhu, H.; Pan, Y.; Wu, F.; Huan, R. Optimized Electrode Locations for Wearable Single-Lead ECG Monitoring Devices: A Case Study Using WFEES Modules Based on the LANS Method. Sensors 2019, 19, 4458. https://doi.org/10.3390/s19204458
Zhu H, Pan Y, Wu F, Huan R. Optimized Electrode Locations for Wearable Single-Lead ECG Monitoring Devices: A Case Study Using WFEES Modules Based on the LANS Method. Sensors. 2019; 19(20):4458. https://doi.org/10.3390/s19204458
Chicago/Turabian StyleZhu, Huaiyu, Yun Pan, Fan Wu, and Ruohong Huan. 2019. "Optimized Electrode Locations for Wearable Single-Lead ECG Monitoring Devices: A Case Study Using WFEES Modules Based on the LANS Method" Sensors 19, no. 20: 4458. https://doi.org/10.3390/s19204458
APA StyleZhu, H., Pan, Y., Wu, F., & Huan, R. (2019). Optimized Electrode Locations for Wearable Single-Lead ECG Monitoring Devices: A Case Study Using WFEES Modules Based on the LANS Method. Sensors, 19(20), 4458. https://doi.org/10.3390/s19204458