Recognizing Physical Activity of Older People from Wearable Sensors and Inconsistent Data

 ,
,  ,
, 
Abstract
:1. Introduction
1.1. Related Work
1.2. Challenges in Activity Recognition Using Wearable Sensors
1.3. Aim of Current Study
- A SVM-based classification method is developed and assessed exclusively on older people’s recordings from a wearable sensor in everyday life conditions.
- Variations of the basic model are proposed to address device-relative issues that are due to data acquisition based on two different wearable devices, as well as their possible misplacement, during monitoring of physiological activity.
- The subject-specific prediction models of our previous work [12] are replaced with subject-independent models to avoid the laborious pre-training phase for every new-coming subject.
- Temporal consistency criteria are enforced to improve the predictions’ robustness.
- Three different convolutional neural network architectures are developed and applied to the same ADL recognition problem improving classification accuracy over our standard approach [8].
- Advanced Bayesian optimization is exploited for efficient hyper-parameter tuning.
2. Materials and Methods
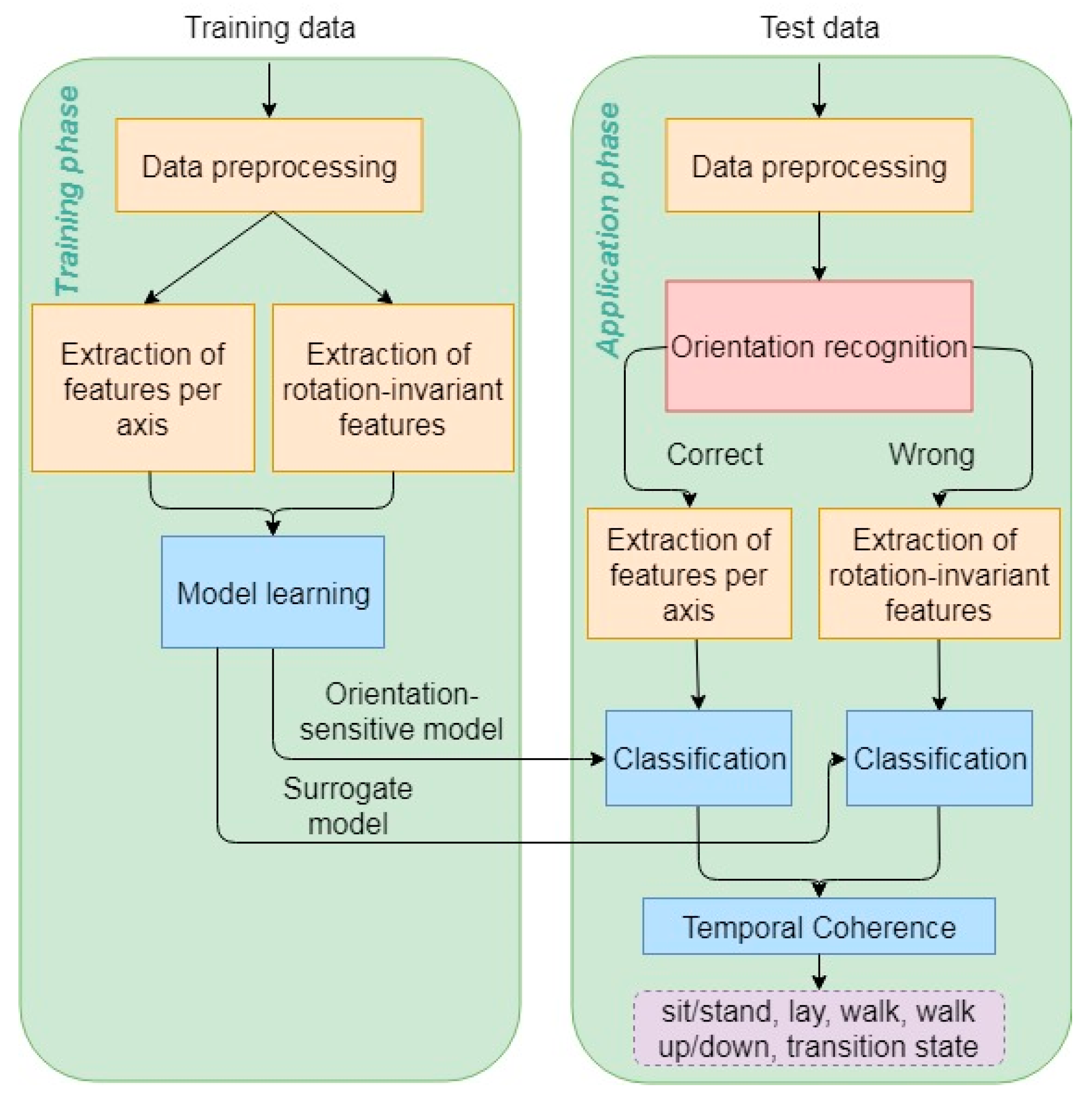
2.1. The Augmented Standard Approach
2.1.1. Preprocessing and Feature Extraction
2.1.2. Reducing Differences across Devices
2.1.3. Resolving the Rotation of Axes Issue
2.1.4. Classification and Feature Selection
2.1.5. Enforcing Temporal Coherency of Activities
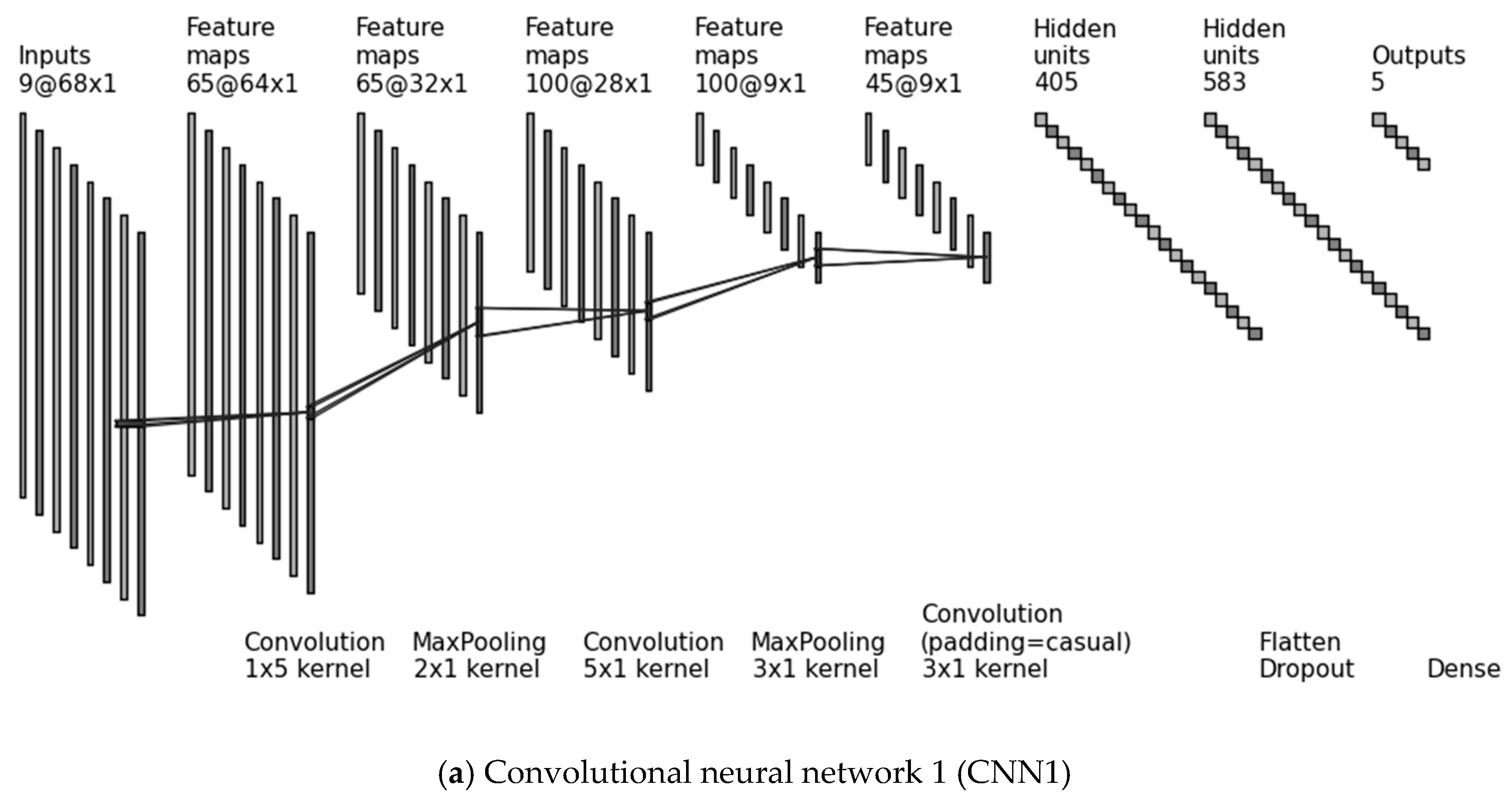
2.2. Deep Learning Approach
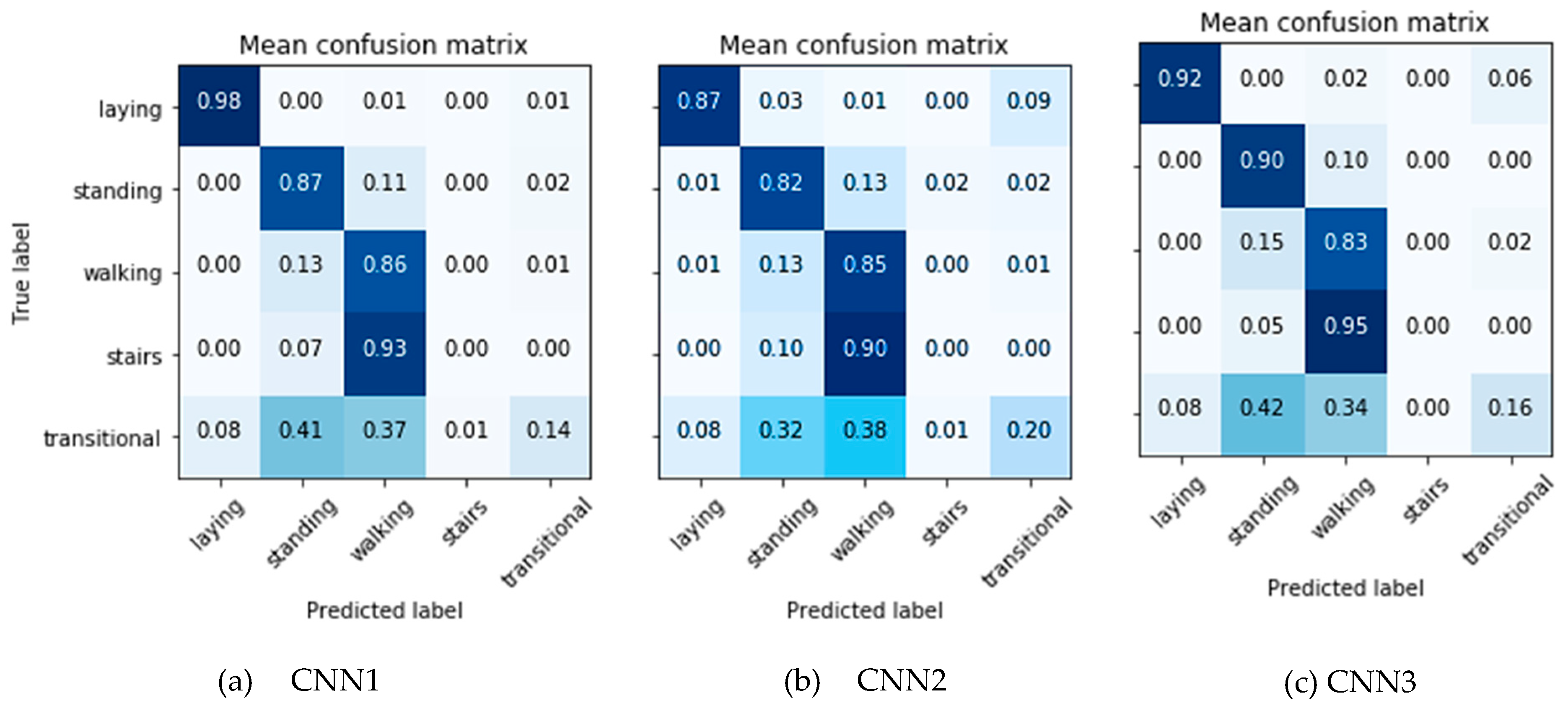
- CNN1: 1D convolution is performed on the input data along the temporal dimension only, with a convolutional kernel of size . The data consist of 9 channels, which are the recordings of the 3 tri-axial sensors, arranged in the depth dimension ().
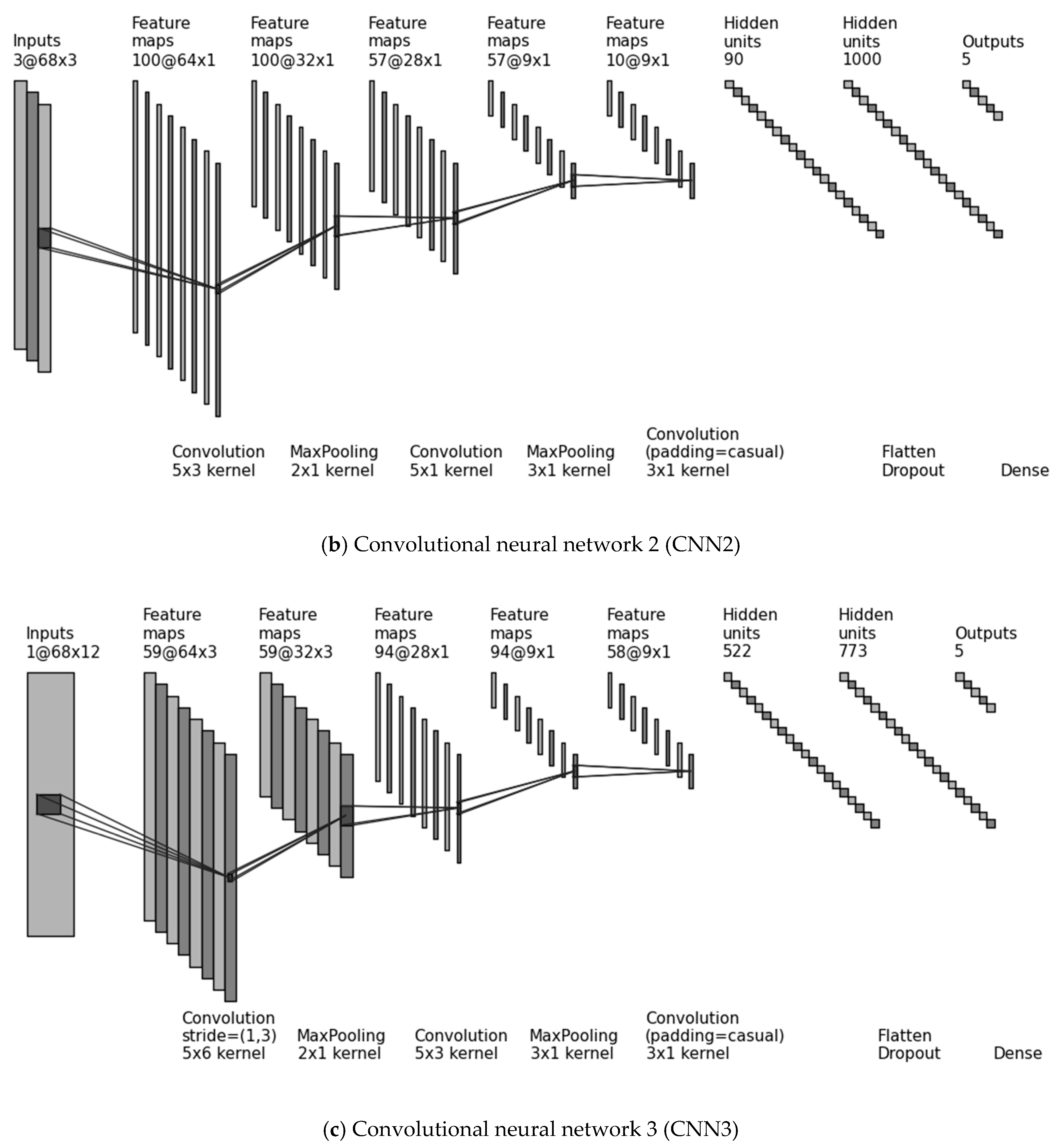
- CNN2: 2D convolution is performed with a convolutional kernel along the temporal dimension and the sensing modality by stacking the different sensors (accelerometer, gyroscope, magnetometer) row-by-row and arranging the , and axes in the depth dimension (). Since the height of the input data equals the height of the convolutional kernel (), the 2D kernel slides only along the temporal dimension.
- CNN3: Following the idea of Jiang and Yin [20], we created a “2D signal image” by stacking the input channels row-by-row with repetition, such that every sensor becomes adjacent to every other sensor. Specifically, we arranged the recordings of the accelerometer in , , , the gyroscope in , , and the magnetometer in , , , and introduced again the accelerometer in , , , thereby creating a 2D signal image of height . By using a convolutional kernel , all different sensor combinations were possible (accelerometer with gyroscope, gyroscope with magnetometer and magnetometer with accelerometer). The convolutional kernel this time slides along both axes (over time and over sensors). By using a stride of the bundles of , , and channels were kept together. The depth dimension is vanished in this architecture ().
Implementation Details
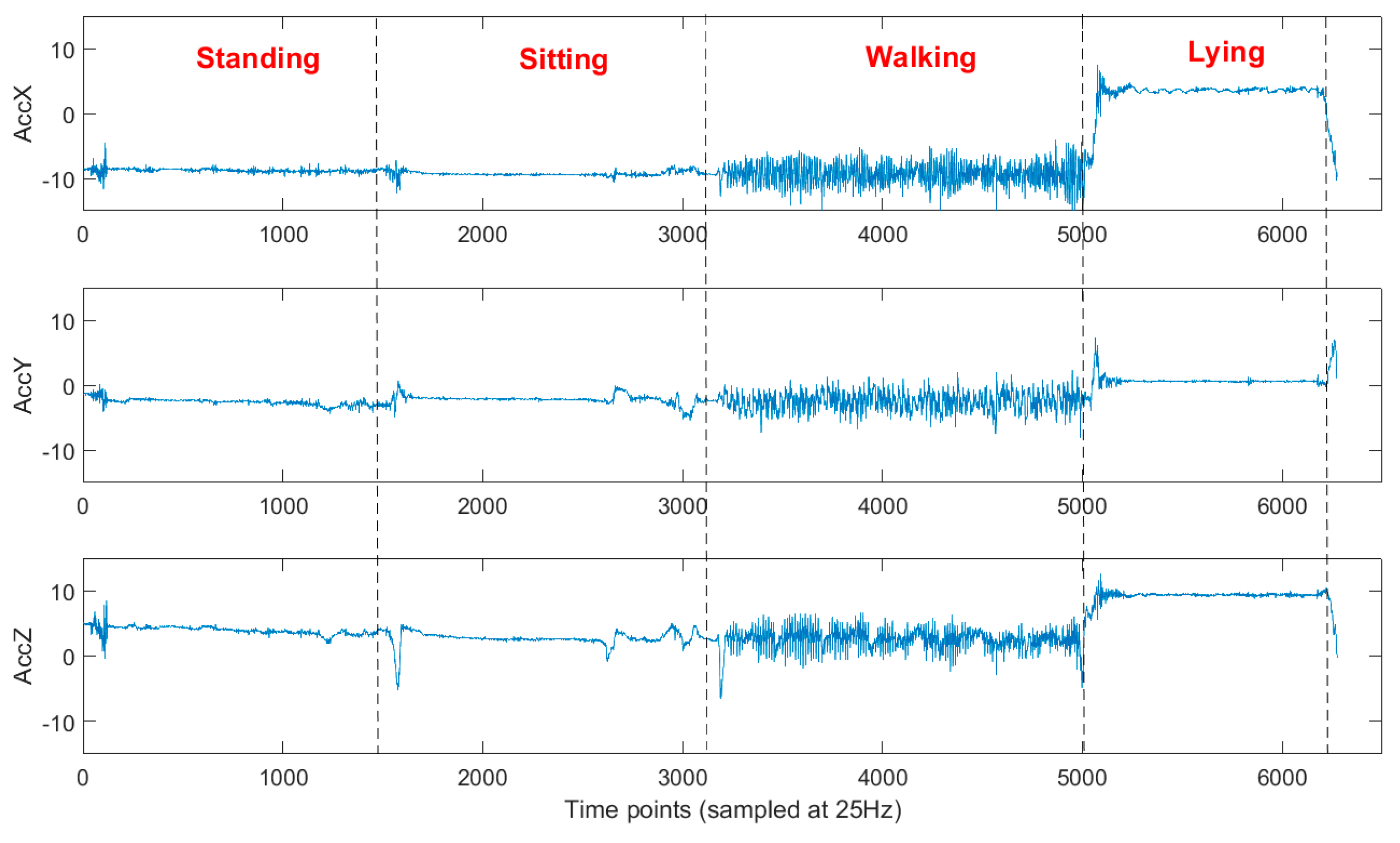
2.3. Experimental Procedure
- Standing for 1 min;
- Sitting for 1 min;
- Walking for 1 min;
- Walking upstairs for 30 s;
- Walking downstairs for 30 s;
- Laying for 30 s.
3. Results
3.1. Augmented Standard Approach
3.2. Deep-Learning Approach
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Chiauzzi, E.; Rodarte, C.; DasMahapatra, P. Patient-centered activity monitoring in the self-management of chronic health conditions. BMC Med. 2015, 13, 77. [Google Scholar] [CrossRef] [PubMed]
- Bauman, A.; Merom, D.; Bull, F.C.; Buchner, D.M.; Singh, F.A.M.A. Updating the evidence for physical activity: Summative reviews of the epidemiological evidence, prevalence, and interventions to promote “active aging”. Gerontologist 2016, 56, S268–S280. [Google Scholar] [CrossRef]
- Mugueta-Aguinaga, I.; Garcia-Zapirain, B. Is technology present in frailty? Technology a back-up tool for dealing with frailty in the elderly: A systematic review. Aging Dis. 2017, 8, 176. [Google Scholar] [CrossRef] [PubMed]
- Van Velsen, L.; Illario, M.; Jansen-Kosterink, S.; Crola, C.; di Somma, C.; Colao, A.; Vollenbroek-Hutten, M. A community-based, technology-supported health service for detecting and preventing frailty among older adults: A participatory design development process. J. Aging Res. 2015, 2015. [Google Scholar] [CrossRef] [PubMed]
- Kalogiannis, S.; Zacharaki, E.I.; Deltouzos, K.; Kotsani, M.; Ellul, J.; Benetos, A.; Megalooikonomou, V. Geriatric group analysis by clustering non-linearly embedded multi-sensor data. In Proceedings of the 2018 Innovations in Intelligent Systems and Applications (INISTA), Thessaloniki, Greece, 3–5 July 2018; pp. 1–7. [Google Scholar]
- Fang, Y.; Chau, A.K.C.; Wong, A.; Fung, H.H.; Woo, J. Information and communicative technology use enhances psychological well-being of older adults: The roles of age, social connectedness, and frailty status. Aging Ment. Health 2017, 22, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Papastergiou, T.; Zacharaki, E.I.; Megalooikonomou, V. Tensor decomposition for multiple instance classification of high-order medical data. Complexity 2018, 2018, 8651930. [Google Scholar] [CrossRef]
- Papagiannaki, A.; Zacharaki, E.I.; Deltouzos, K.; Orselli, R.; Freminet, A.; Cela, S.; Aristodemou, E.; Polycarpou, M.; Kotsani, M.; Benetos, A.; et al. Meeting challenges of activity recognition for ageing population in real life settings. In Proceedings of the 2018 IEEE 20th International Conference on e-Health Networking, Applications and Services (Healthcom), Ostrava, Czech Republic, 17–20 September 2018. [Google Scholar]
- FrailSafe Project. Available online: https://frailsafe-project.eu/ (accessed on 19 February 2019).
- Bao, L.; Intille, S.S. Activity recognition from user-annotated acceleration data. In Proceedings of the International Conference on Pervasive Computing, Linz/Vienna, Austria, 18–23 April 2004. [Google Scholar]
- Andò, B.; Baglio, S.; Lombardo, C.O.; Marletta, V.; Pergolizzi, E.A.; Pistorio, A.; Valastro, A. ADL Detection for the Active Ageing of Elderly People. In Ambient Assisted Living; Springer: Cham, Switzerland, 2015; pp. 287–294. [Google Scholar]
- Pippa, E.; Mporas, I.; Megalooikonomou, V. Feature Selection Evaluation for Light Human Motion Identification in Frailty Monitoring System. In Proceedings of the International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AWE 2016), Rome, Italy, 21–22 April 2016; pp. 88–95. [Google Scholar]
- Sebestyen, G.; Stoica, I.; Hangan, A. Human activity recognition and monitoring for elderly people. In Proceedings of the 2016 IEEE 12th International Conference on in Intelligent Computer Communication and Processing (ICCP), Cluj-Napoca, Romania, 8–10 September 2016. [Google Scholar]
- Ranasinghe, D.C.; Torres, R.L.S.; Wickramasinghe, A. Automated activity recognition and monitoring of elderly using wireless sensors: Research challenges. In Proceedings of the 2013 5th IEEE International Workshop on Advances in Sensors and Interfaces (IWASI), Bari, Italy, 13–14 June 2013. [Google Scholar]
- Chernbumroong, S.; Cang, S.; Atkins, A.; Yu, H. Elderly activities recognition and classification for applications in assisted living. Expert Sys. Appl. 2013, 40, 1662–1674. [Google Scholar] [CrossRef]
- Liu, J.; Sohn, J.; Kim, S. Classification of Daily Activities for the Elderly Using Wearable Sensors. J. Healthc. Eng. 2017, 2017. [Google Scholar] [CrossRef]
- El Achkar, C.M.; Lenoble-Hoskovec, C.; Paraschiv-Ionescu, A.; Major, K.; Büla, C.; Aminian, K. Instrumented shoes for activity classification in the elderly. Gait Posture 2016, 44, 12–17. [Google Scholar] [CrossRef]
- Gokalp, H.; Clarke, M. Monitoring activities of daily living of the elderly and the potential for its use in telecare and telehealth: A review. Telemed. e-Health 2013, 19, 910–923. [Google Scholar] [CrossRef]
- Yang, J.; Nguyen, M.N.; San, P.P.; Li, X.; Krishnaswamy, S. Deep Convolutional Neural Networks on Multichannel Time Series for Human Activity Recognition. IJCAI 2015, 15, 3995–4001. [Google Scholar]
- Zeng, M.; Nguyen, L.T.; Yu, B.; Mengshoel, O.J.; Zhu, J.; Wu, P.; Zhang, J. Convolutional neural networks for human activity recognition using mobile sensors. In Proceedings of the 2014 6th International Conference on Mobile Computing, Applications and Services (MobiCASE), Austin, TX, USA, 6–7 November 2014. [Google Scholar]
- Ordóñez, F.; Roggen, D. Deep convolutional and lstm recurrent neural networks for multimodal wearable activity recognition. Sensors 2016, 16, 115. [Google Scholar] [CrossRef]
- Jiang, W.; Yin, Z. Human activity recognition using wearable sensors by deep convolutional neural networks. In Proceedings of the 23rd ACM International Conference on Multimedia, Brisbane, Australia, 26–30 October 2015. [Google Scholar]
- Bulling, A.; Blanke, U.; Schiele, B. A tutorial on human activity recognition using body-worn inertial sensors. ACM Comput. Surv. 2014, 46, 33. [Google Scholar] [CrossRef]
- Roggen, D.; Calatroni, A.; Rossi, M.; Holleczek, T.; Förster, K.; Tröster, G.; Lukowicz, P.; Bannach, D.; Pirkl, G.; Ferscha, A.; et al. Collecting complex activity datasets in highly rich networked sensor environments. In Proceedings of the 2010 Seventh International Conference on Networked Sensing Systems (INSS), Kassel, Germany, 15–18 June 2010. [Google Scholar]
- Sagha, H.; Digumarti, S.T.; Millán, J.D.R.; Chavarriaga, R.; Calatroni, A.; Roggen, D.; Tröster, G. Benchmarking classification techniques using the Opportunity human activity dataset. In Proceedings of the 2011 IEEE International Conference on Systems, Man, and Cybernetics (SMC), Anchorage, AK, USA, 9–12 October 2011. [Google Scholar]
- Fekri, M.; Shafiq, M.O. Deep Convolutional Neural Network Learning for Activity Recognition using real-life sensor’s data in smart devices. In Proceedings of the IEEE 20th International Conference on e-Health Networking, Applications and Services (Healthcom), Ostrava, Czech Republic, 17–20 September 2018. [Google Scholar]
- Lockhart, J.W.; Weiss, G.M.; Xue, J.C.; Gallagher, S.T.; Grosner, A.B.; Pulickal, T.T. Design considerations for the WISDM smart phone-based sensor mining architecture. In Proceedings of the Fifth International Workshop on Knowledge Discovery from Sensor Data, San Diego, CA, USA, 21 August 2011. [Google Scholar]
- Hinton, G.E.; Osindero, S.; Teh, Y.-W. A fast learning algorithm for deep belief nets. Neural Comput. 2006, 18, 1527–1554. [Google Scholar] [CrossRef] [PubMed]
- Plötz, T.; Hammerla, N.Y.; Olivier, P. Feature learning for activity recognition in ubiquitous computing. In Proceedings of the International Joint Conference on Artificial Intelligence, Barcelona, Spain, 16–22 July 2011. [Google Scholar]
- Rokni, S.A.; Ghasemzadeh, H. Autonomous Training of Activity Recognition Algorithms in Mobile Sensors: A Transfer Learning Approach in Context-Invariant Views. IEEE Trans. Mob. Comput. 2018, 17, 1764–1777. [Google Scholar] [CrossRef]
- Saeedi, R.; Norgaard, S.; Gebremedhin, A.H. A closed-loop deep learning architecture for robust activity recognition using wearable sensors. In Proceedings of the IEEE International Conference on Big Data, Boston, MA, USA, 11–14 December 2017. [Google Scholar]
- Hammerla, N.; Halloran, S.; Ploetz, T. Deep, convolutional, and recurrent models for human activity recognition using wearables. arXiv, 2016; arXiv:1604.08880. [Google Scholar]
- Baños, O.; Damas, M.; Pomares, H.; Rojas, I.; Tóth, M.A.; Amft, O. A benchmark dataset to evaluate sensor displacement in activity recognition. In Proceedings of the 2012 ACM Conference on Ubiquitous Computing, Pittsburgh, PA, USA, 5–8 September 2012. [Google Scholar]
- Rey, V.F.; Lukowicz, P. Label Propagation: An Unsupervised Similarity Based Method for Integrating New Sensors in Activity Recognition Systems. Proc. ACM Interact. Mob. Wearable Ubiquitous Technol. 2017, 1, 94. [Google Scholar] [CrossRef]
- Smartex. Available online: http://www.smartex.it/en/ (accessed on 19 February 2019).
- Kalogiannis, S.; Deltouzos, K.; Zacharaki, E.I.; Vasilakis, A.; Moustakas, K.; Ellul, J.; Megalooikonomou, V. Integrating an openEHR-based personalized virtual model for the ageing population within HBase. BMC Med. Inf. Dec. Mak. 2019, 19, 1. [Google Scholar] [CrossRef] [PubMed]
- Anguita, D.; Ghio, A.; Oneto, L.; Parra, X.; Reyes-Ortiz, J.L. Human activity recognition on smartphones using a multiclass hardware-friendly support vector machine. In Proceedings of the International conference on ambient assisted living and Home Care, Vitoria-Gasteiz, Spain, 3–5 December 2012; pp. 216–223. [Google Scholar]
- Chakravarty, I.M.; Roy, J.D.; Laha, R.G. Handbook of Methods of Applied Statistics; John Wiley and Sons: Hoboken, NJ, USA, 1967. [Google Scholar]
- Chang, C.-C.; Lin, C.-J. LIBSVM: A library for support vector machines. ACM Trans. Intell. Syst. Technol. (TIST) 2011, 2, 27. [Google Scholar] [CrossRef]
- Zacharaki, E.I.; Mporas, I.; Garganis, K.; Megalooikonomou, V. Spike pattern recognition by supervised classification in low dimensional embedding space. Brain Inform. 2016, 3, 73–83. [Google Scholar] [CrossRef] [Green Version]
- Mporas, I.; Tsirka, V.; Zacharaki, E.; Koutroumanidis, M.; Megalooikonomou, V. Evaluation of time and frequency domain features for seizure detection from combined EEG and ECG signals. In Proceedings of the 7th International Conference on Pervasive Technologies Related to Assistive Environments, Rhodes, Greece, 27–30 May 2014. [Google Scholar]
- Pippa, E.; Zacharaki, E.I.; Özdemir, A.T.; Barshan, B.; Megalooikonomou, V. Global vs local classification models for multi-sensor data fusion. In Proceedings of the 10th Hellenic Conference on Artificial Intelligence, Patras, Greece, 9–12 July 2018. [Google Scholar]
- Kononenko, I. Estimating attributes: Analysis and extensions of RELIEF. In Proceedings of the European Conference on Machine Learning, Catania, Italy, 6–8 April 1994. [Google Scholar]
- Pippa, E.; Zacharaki, E.I.; Mporas, I.; Tsirka, V.; Richardson, M.P.; Koutroumanidis, M.; Megalooikonomou, V. Improving classification of epileptic and non-epileptic EEG events by feature selection. Neurocomputing 2016, 171, 576–585. [Google Scholar] [CrossRef] [Green Version]
- Cao, H.; Nguyen, M.N.; Phua, C.; Krishnaswamy, S.; Li, X.L. An integrated framework for human activity classification. In Proceedings of the ACM International Conference on Ubiquitous Computing, Pittsburgh, PA, USA, 5–8 September 2012. [Google Scholar]
- Dewancker, I.; McCourt, M.; Clark, S.; Hayes, P.; Johnson, A.; Ke, G. A Stratified Analysis of Bayesian Optimization Methods. arXiv, 2016; arXiv:1603.09441. [Google Scholar]
- Snoek, J.; Larochelle, H.; Adams, R.P. Practical bayesian optimization of machine learning algorithms. In Proceedings of the 25th International Conference on Neural Information Processing Systems, Harrahs and Harveys, Lake Tahoe, CA, USA, 3–8 December 2012. [Google Scholar]
- Abadi, M.; Barham, P.; Chen, J.; Chen, Z.; Davis, A.; Dean, J.; Devin, M.; Ghemawat, S.; Irving, G.; Isard, M.; et al. Tensorflow: A system for large-scale machine learning. OSDI 2016, 16, 265–283. [Google Scholar]
- Keras. 2015. Available online: https://github.com/fchollet/keras (accessed on 19 February 2019).
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M157. [Google Scholar] [CrossRef]
- Zheng, W.-L.; Lu, B.-L. Personalizing EEG-based affective models with transfer learning. In Proceedings of the Twenty-Fifth International Joint Conference on Artificial Intelligence, New York, NY, USA, 9–15 July 2016. [Google Scholar]
- Ali, H.; Messina, E.; Bisiani, R. Subject-dependent physical activity recognition model framework with a semi-supervised clustering approach. In Proceedings of the IEEE European Modelling Symposium (EMS), Manchester, UK, 20–22 November 2013. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID | WWBS | Probably Correct Orientation | Used for Training | Older Adults |
|---|---|---|---|---|
| 3087 | yes | yes | yes | yes |
| 3098 | yes | yes | yes | yes |
| 3104 | yes | yes | yes | yes |
| 3116 | yes | yes | yes | yes |
| 3117 | yes | yes | yes | yes |
| 3593 | yes | yes | yes | yes |
| 3600 | yes | yes | yes | yes |
| 3601 | yes | yes | yes | yes |
| 1117 | yes | yes | no | yes |
| 2101 | yes | yes | no | yes |
| 2113 | yes | yes | no | yes |
| 2615 | yes | yes | no | yes |
| 3084 | yes | yes | no | yes |
| 3091 | yes | yes | no | yes |
| 3112 | yes | yes | no | yes |
| 3118 | yes | yes | no | yes |
| 1507 | yes | no | no | yes |
| 1538 | yes | no | no | yes |
| 2094 | no | — | no | yes |
| 2102 | no | — | no | yes |
| 9000 | no | — | no | no |
| 9001 | no | — | no | no |
| Actual | Predicted | |||||
| Classes | Sit/Stand | Laying | Walking | Walking up/down | Transition | |
| Sit/Stand | 96.08 | 0 | 0.76 | 0 | 3.16 | |
| Laying | 0 | 86.75 | 1.65 | 0 | 11.60 | |
| Walking | 8.26 | 0 | 74.33 | 1.56 | 15.85 | |
| Walking up/down | 0 | 0 | 100 | 0 | 0 | |
| Transition | 36.07 | 2.73 | 18.03 | 0 | 43.17 | |
| Subject | Classification Accuracy % | Increased by % | |
|---|---|---|---|
| Orientation Sensitive Model | Surrogate Model | ||
| 1 | 19.4 | 60.2 | 40.8 |
| 2 | 19.6 | 60.4 | 40.8 |
| 3 | 23.1 | 72.6 | 49.5 |
| 4 | 29.8 | 78.0 | 48.2 |
| 5 | 25.3 | 64.5 | 39.3 |
| 6 | 7.0 | 69.2 | 62.1 |
| 7 | 7.2 | 87.1 | 79.9 |
| 8 | 25.4 | 78.5 | 53.2 |
| Hyper-Parameters | Values | Contribution in the Model | |||||
|---|---|---|---|---|---|---|---|
| CNN1 | CNN2 | CNN3 | CNN1 | CNN2 | CNN3 | ||
| FrailSafe dataset | Batch | 100 | 100 | 59 | 2.14% | 1.50% | 1.62% |
| Dense Layer Size | 583 | 1000 | 773 | 1.17% | 1.82% | 1.92% | |
| Dropout prob. | 0.6 | 0.39 | 0.6 | 2.68% | 2.20% | 1.29% | |
| Epochs | 100 | 100 | 100 | 3.90% | 2.65% | 3.76% | |
| Filter 1 | 65 | 100 | 59 | 2.38% | 1.95% | 2.06% | |
| Filter 2 | 100 | 57 | 94 | 2.12% | 2.41% | 1.88% | |
| Filter 3 | 45 | 10 | 58 | 1.78% | 1.17% | 1.29% | |
| Learning rate | 0.0330 | 0.0480 | 0.1000 | 17.49% | 9.46% | 26.61% | |
| Regulariz. rate | 0.0030 | 0.0001 | 0.0001 | 16.83% | 9.32% | 32.63% | |
| Optimizer | SGD | SGD | SGD | 48.72% | 67.52% | 26.89% | |
| CNN1 | CNN2 | CNN3 | |
|---|---|---|---|
| Test Accuracy | 81.91(±2.45) | 78.49(±3.66) | 82.47(±4.24) |
| Train Accuracy | 90.64(±1.34) | 90.86(±0.83) | 91.84(±1.17) |
| Study | Sensor/Location | Measurement | Method | Cross-Val. | Inter-Subj. | Accuracy |
|---|---|---|---|---|---|---|
| Current study | IMU at sternum | acceler. | SVM | yes | yes | 81.7% |
| acceler., gyroscope, magnetometer | CNN3 | 82.47% | ||||
| [15] | Smart watch | acceler., temperature, altitude | NNs, SVM | yes | no | 90.23% |
| [16] | IMUs at sternum and thigh | orientation, acceler., angular velocity | Rule-based | no | no | 97.2% |
| [17] | Instrumented shoes | foot loading, orientation, elevation | Decision Tree | no | no | 97.41% |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papagiannaki, A.; Zacharaki, E.I.; Kalouris, G.; Kalogiannis, S.; Deltouzos, K.; Ellul, J.; Megalooikonomou, V. Recognizing Physical Activity of Older People from Wearable Sensors and Inconsistent Data. Sensors 2019, 19, 880. https://doi.org/10.3390/s19040880
Papagiannaki A, Zacharaki EI, Kalouris G, Kalogiannis S, Deltouzos K, Ellul J, Megalooikonomou V. Recognizing Physical Activity of Older People from Wearable Sensors and Inconsistent Data. Sensors. 2019; 19(4):880. https://doi.org/10.3390/s19040880
Chicago/Turabian StylePapagiannaki, Aimilia, Evangelia I. Zacharaki, Gerasimos Kalouris, Spyridon Kalogiannis, Konstantinos Deltouzos, John Ellul, and Vasileios Megalooikonomou. 2019. "Recognizing Physical Activity of Older People from Wearable Sensors and Inconsistent Data" Sensors 19, no. 4: 880. https://doi.org/10.3390/s19040880
APA StylePapagiannaki, A., Zacharaki, E. I., Kalouris, G., Kalogiannis, S., Deltouzos, K., Ellul, J., & Megalooikonomou, V. (2019). Recognizing Physical Activity of Older People from Wearable Sensors and Inconsistent Data. Sensors, 19(4), 880. https://doi.org/10.3390/s19040880