1. Introduction
Hallux Abductus Valgus (HAV) is a pathological subluxation of the first metatarsophalangeal joint (IMPJ) with lateral deviation of the proximal phalanx of the hallux bone (PPH) toward abduction and valgus direction in both the transverse and frontal planes of motion, respectively. There is also deviation of the first metatarsocuneiform joint (IMCJ) through the first metatarsal bone (IMTT) toward adduction and valgus direction in both transverse and frontal planes of motion, respectively. There are occasionally bony enlargements of the first metatarsal head (also called a “bunion”) [
1,
2,
3]. The IMPJ bears 80% of the body load without help of any structure in heel-off phase, and this makes it a more sensitive joint to biomechanics deformities such HAV [
1].
The etiology of HAV can have multiple origins, and there are intrinsic and extrinsic factors in play [
4,
5,
6,
7,
8,
9]. Intrinsic factors include hyperpronation [
5,
10], soft tissue weakness [
1], and hyperlaxity with medial longitudinal arch collapse [
11,
12]; Windlass mechanism failure [
7], first ray hypermobility [
8], and female sex [
13,
14,
15] have been linked with HAV growth. As extrinsic factors, the use of high-heel shoes has also been detected as a possible cause of HAV development: The typical high-heeled shoe for women can lead to bad body repercussions and be detrimental to bone mineralization [
16], rear foot instability [
17], body mass center changes [
18], biomechanics gait changes [
19,
20], and general damage health [
21].
Some authors have reported increases in concentrate load under the forefoot with high heeled shoes [
22,
23,
24,
25], and this condition can predispose the subject to HAV development [
26]. A few studies have speculated that the current narrow box of high-heeled shoes are not the only cause of HAV because isolated high-heel shoes might cause weight to be placed on the forefoot, and this may overstretch the toes and lead to the development of splayfoot [
1,
27,
28]. However, this has not been reported in the literature.
The 2D [
29] and 3D kinematic movements of PPH and I MTT bone deviation during gait in subjects with and without HAV has shown the relationship between the rearfoot and midfoot eversion with respect to the first ray hypermobility and the presence on HAV [
10,
30]; other groups have studied the kinematic effects of improvements in taping in subjects with HAV during gait [
31] or the negative effects of HAV surgery to normal ambulation [
32]. Other work studied the kinematics effects on IMPJ using foot orthoses that incorporated forefoot and rearfoot posting—the results showed no negative effects on mobility [
33]. One prior study [
34] identified kinetic evidence of wearing 5 cm-heeled shoes during gait can lead to HAV development and an increase in hallux dorsiflexion in the final push-off phase; however, no report has described the transverse or frontal plane motion of the PPH or IMTT.
Therefore, the goal of this study is to determine how the heel height affects PPH and IMTT bone deviations either in the three planes of motion in static conditions and during the dorsiflexion of the IMPJ sequence (push-off phase of the dynamic condition) regardless of toe box of the shoe. The results can show if there is some movement related to HAV deviation that is characterized by PPH in abduction (away to medial body line) in transverse plane and valgus deviation in frontal plane toward the IMPJ [
2] and/or the adduction deviation of the IMTT (toward medial body line) regarding the second MTT in transverse plane and the presence of the valgus in the frontal plane toward the IMCJ [
2].
3. Results
None of the data were normally distributed (
p < 0.05). The means that the 96 measured variables were different when compared between each other (
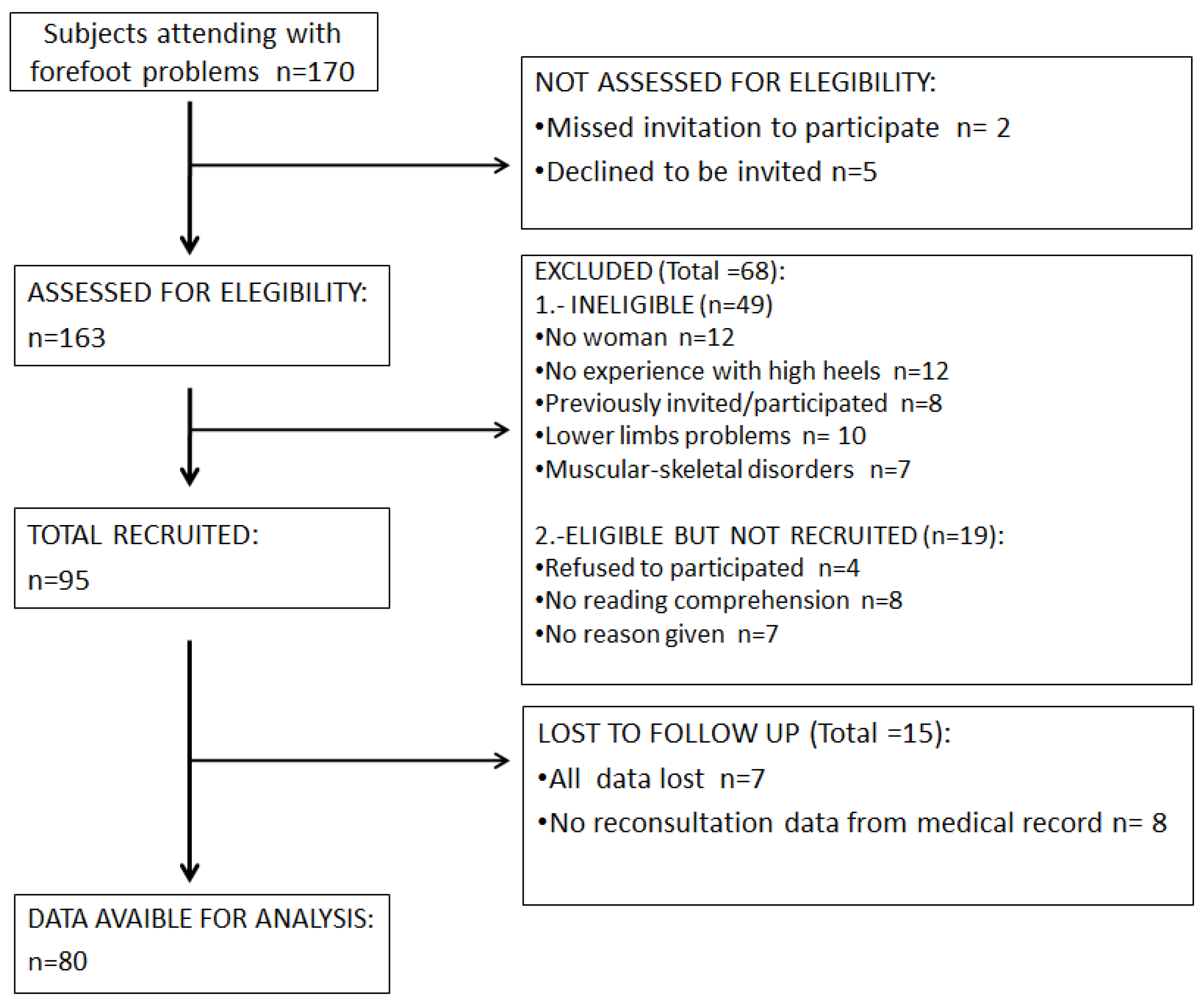
p < 0.001). Participants in this cross-sectional study were recruited from an orthopedic clinic in Madrid (Spain) over a 2-year period (May 2015 to May 2017). Of the 163 subjects who initially volunteered to participate in the study, 68 subjects did not meet the inclusion criteria. An additional 15 subjects did not present for testing. The remaining 80 subjects participated in the study (
Figure 8). The participants were only females; sociodemographic data are shown in
Table 1.
All Tables are shown with corresponding values of IMTT and PPH to the static test as well as independent of the dynamic values.
The reliability of the static variables in unshod and heels of 3 cm, 6 cm and 9 cm high are summarized in
Table 2. Each condition showed overall excellent reliability [
50] with ICCs ranging from 0.902 to 0.997 indicating high reliability. In addition, in general terms, CCC showed a strong statistically significant correlation (
p < 0.001) between unshod and either high heel in all movements of PPH and MTT except those related to a sagittal plane. The reliability of dynamic variables in unshod subjects for heel heights of 3 cm, 6 cm and 9 cm is summarized in
Table 3. Each condition showed an overall excellent reliability [
50] with ICCs ranging from 0.898 to 0.999 indicating high reliability. The CCC showed a strong correlation (
p < 0.001) in all movements of PPH and MTT in dynamic tests, as well. The inter-rater MDC 95% values to static (
Table 2) conditions ranged from 14.915° to 0.74° for sensor 1 (IMTT) and from 7.90° to 1.63° for sensor 2 (PPH); the inter-rater MDC 95% values to dynamic (
Table 3) conditions ranged from 26.78° to 1.12° for sensor 1 (MTT) and from 27.16° to 2.16° for sensor 2 (PPH).
The SEM values for 6 cm high heel in static abduction of PPH (
Table 2) was 0.591° and 0.782° for dynamic abduction condition (
Table 3); in addition, the SEM was 2.02° for valgus movement of PPH in dynamic condition with high heels of 6 cm and 2.33° in static condition.
Static mobility grades of IMTT (sensor 1) and PPH (sensor 2) bones in unshod and 3 cm, 6 cm and 9 cm heel height are summarized in
Table 4. The dynamic mobility grades of both sensor 1 and sensor 2 in unshod and 3 cm, 6 cm and 9 cm heel heights in
Table 5.
Under static conditions, the PPH abduction increases from 1.01 ± 0.36° to 1.31 ± 0.46° (p < 0.05) after wearing shoes with a 3 cm heel. There was a statistically significant valgus of the I MTT with increasing heel heights from 1.77 ± 0.20° without high heels to 2.15 ± 0.10° with 3 cm (p < 0.001) high heels. There was increased varus movement from 1.50 ± 0.23 to 3.87 ± 0.20 with 3 cm heels (p < 0.001).
In dynamic tests, wearing shoes with 6 cm high heels led to an increase in PPH valgus and abduction deviation from 3.15 ± 0.10° to 3.46 ± 0.05° (p < 0.05) and from 1.35 ± 0.28° to 1.69 ± 0.30° (p < 0.001), respectively. In addition, PPH had abduction that increased to 1.91 ± with 9 cm heels (p < 0.001). On the other hand, I MTT had a valgus decrease with 6 cm heels (from 3.94 ± 0.28 to 3.70 ± 0.13 (p < 0.001)) but without any concordance correlation.
Finally,
Table 6 and
Table 7 summarize the Spearman’s Rho correlation coefficients of static and dynamic conditions between the height of the heels and the movements of PPH and I MTT, respectively.
In static tests, adduction of IMTT had a statistically significant positive correlation while wearing 6 cm heels versus unshod condition (0.5, p < 0.001) as well as abduction (0.347, p < 0.001). Valgus values had a statistically significant positive correlation too under 3 cm high heel (0.51, p < 0.001). Regarding PPH abduction, there was a statistical positive correlation in 6 cm heels (0.261, p < 0.05) as well as a statistically significant negative correlation to adduction under 3 cm and 6 cm of high heels (p < 0.05).
During dynamic tests, PPH abduction had a statistically significant positive correlation with heels of 6 cm (0.527, p < 0.001) combined with a statistically significant inverse correlation in adduction (−0.278, p < 0.05) with 6 cm; there was a significant positive correlation with valgus values (0.242, p < 0.05).
4. Discussion
HAV is a forefoot pathology related to PPH in valgus and abduction deviations plus the IMTT bone in adduction deviation [
1,
2,
51]. Previous studies [
18,
52,
53,
54] have shown the relationship between HAV development and the narrow toe tip footwear typical of the high heel shoes; other groups [
1,
27] speculated that high heels have an etiology factor in HAV development with only one prior review [
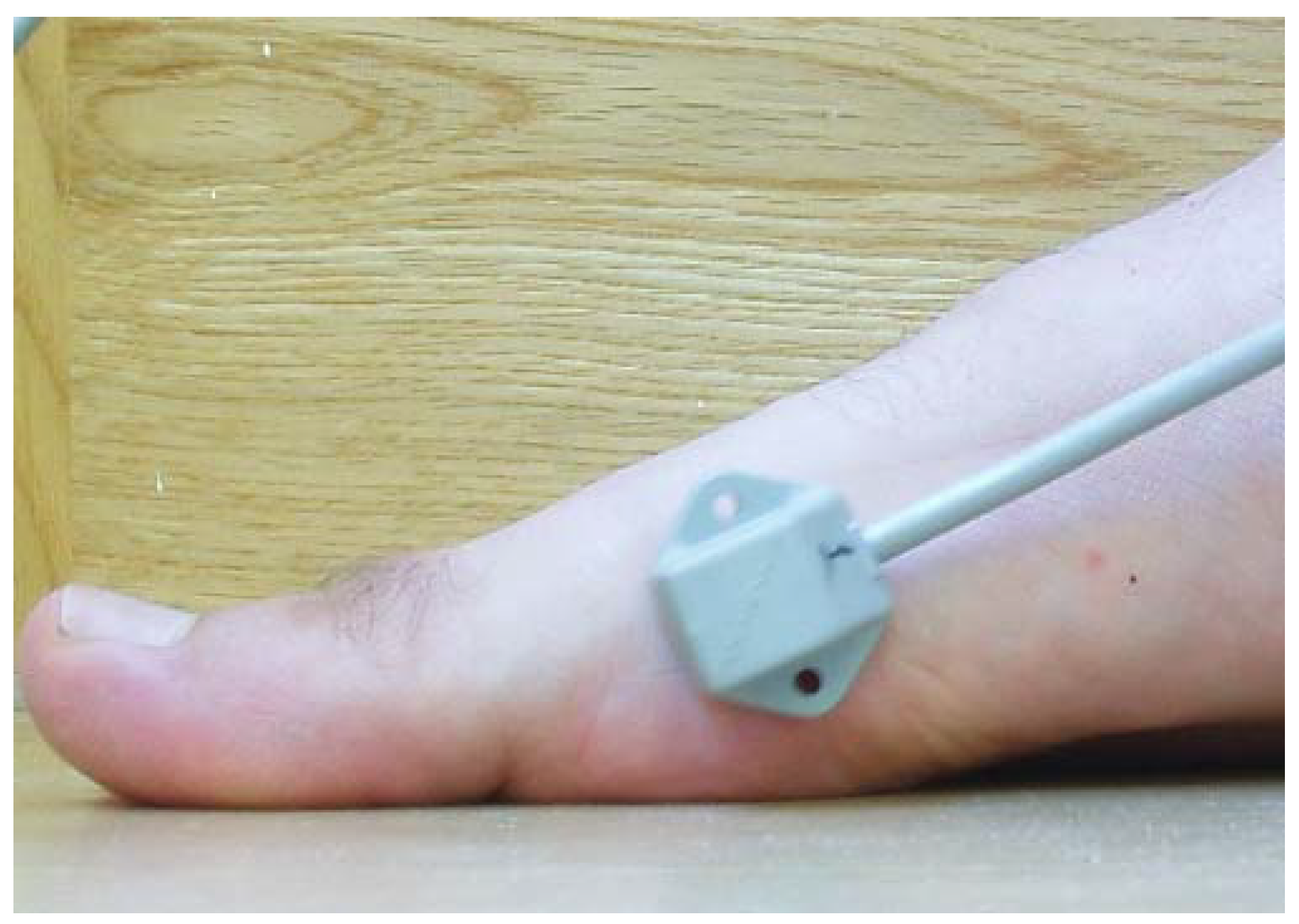
12] considering the isolated high heels’s effect on first MPJ deviation on its conclusions but without any further study. This research was the first study to use the Polhemus Fastrack
® to assess the effects of high heels on static and dynamic conditions on PPH and IMTT. Thus, many statistically significant variables have been obtained, but of the 96 variables studied here across 80 subjects, only a few had statistically significant correlations. Due to the independent evaluation of the bones, we could not establish a direct discussion with the findings of other authors who interpreted HAV as a global forefoot disease [
34]. In addition, this work has studied a healthy population without any limitation of mobility in their joints. Thus, a small difference in segment movements was expected.
Our results on the effect of high heels on PPH during dynamic testing showed that a high heel of 6 cm had a statistically significant increase in abduction in the transverse plane and valgus movement in the frontal plane through IMPJ. There was positive correlation of these values as well as a statistically significant reduction in the adduction; there was negative correlation to the barefoot condition. In addition, during static tests, there was a statistically significant abduction increase in PPH for high heels 6 cm or higher with a corresponding positive correlation; therefore, abduction is the only movement that appeared to have a positive correlation and statistical significance in both static and dynamic tests. Thus, we conclude that heels over 6 cm correlated with an abduction effect on PPH without the narrow shoe box interference. This agrees with arguments on the biomechanical development of HAV processes that claimed that the PPH was the first precursor bone segment to begin the HAV pathology [
51,
55,
56,
57] due to medial capsular tension ligaments that become hyper-elastic and let the PPH proceed to abduction deviation [
7]. The PPH then has a strong push forward to the IMTT in the push off phase that can lead to adduction deviation.
More recently, Wang et al. [
34] reported an increase in forefoot abduction while wearing 5 cm high-heeled shoes during walking vs. barefoot arguing that the squeezing effect of the high heels on the foot had a displacement toward the toe tip. This produced valgus and abduction of PPH. We agree with these conclusions, but we showed that the foot produces this “abductor effect” on PPH; it is not from the narrow box of the shoes. In addition, we obtained a large increase in the value of PPH abduction with a 3 cm heel. This result was not statistically significant.
The effects of high heels had contradictory effects on IMTT movements. There were no statistically significant results to justify its implication on HAV development in contrast with other groups that identified IMTT adduction and valgus [
1,
2] as well as inclination of the IMTT axis as risk factors of bunion [
58] or IMCJ hypermobility [
59]; both movements on transverse and frontal planes are under doubt because of a lack of objective data [
60]. Surprisingly, it seemed that wearing any high heel might decrease valgus deviation of IMTT although this condition only had statistical significance with 6 cm heels; there was no positive correlation. The absence of concrete IMTT values related with typical HAV development suggests that PPH may be the principal bone to start the pathological process. This agrees with a study that identified the presence of HAV with greater reduction in size of the adductor hallucis muscle [
61] as one of the most important muscles to balance the PPH.
In contrast to previous studies [
62] that found no association between footwear characteristics (heel height and narrow box) and HAV development, our cohort had (18–38 years) had movement deviation of PPH in heels over 6 cm. This agrees with other studies where older women reported HAV. They wore shoes with heels over 5 cm [
12]. This work showed data on IMTT and PPH from the two different static and dynamic conditions and 3 kinds of high heels. Thus, we selected and summarized heel heights and determined that high heels could develop HAV. 6 cm was the common height for both static and dynamic situations; these different variables converged to induce HAV development.
Most of the main limitations in other similar studies were equivocal results secondary to small sample size [
19], differences in anthropometric characteristics of the subjects groups [
63], or the inclusion of participants wearing their own high-heeled shoes [
64]. This leads to a heterogeneous sample [
19]. We studied a homogeneous sample that improved the measurement conditions of other groups that also failed to show ICC, CCC, SEM or MDC values [
10,
34]; our data had low to moderate correlation, and we considered these statistical parameters.
Coupling relationships between hindfoot inversion/eversion and forefoot abduction/adduction (
R2 = 0.5) and hallux dorsiflexion/plantarflexion (
R2 = 0.7) were the only prior references found on this topic [
65]. It had similar Spearman values in that work but did show any contrast between data because the authors did not assess individual movements of any segment bone as PPH or I MTT, like in the present work. These are the only specific correlations done relative to PPH and IMTT in the literature and confirm the low Spearman correlations of our values.

 ,
, 













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}