Real-Time Dual-Wavelength Time-Resolved Diffuse Optical Tomography System for Functional Brain Imaging Based on Probe-Hosted Silicon Photomultipliers

 , , , , ,
, , , , ,  , and
, and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
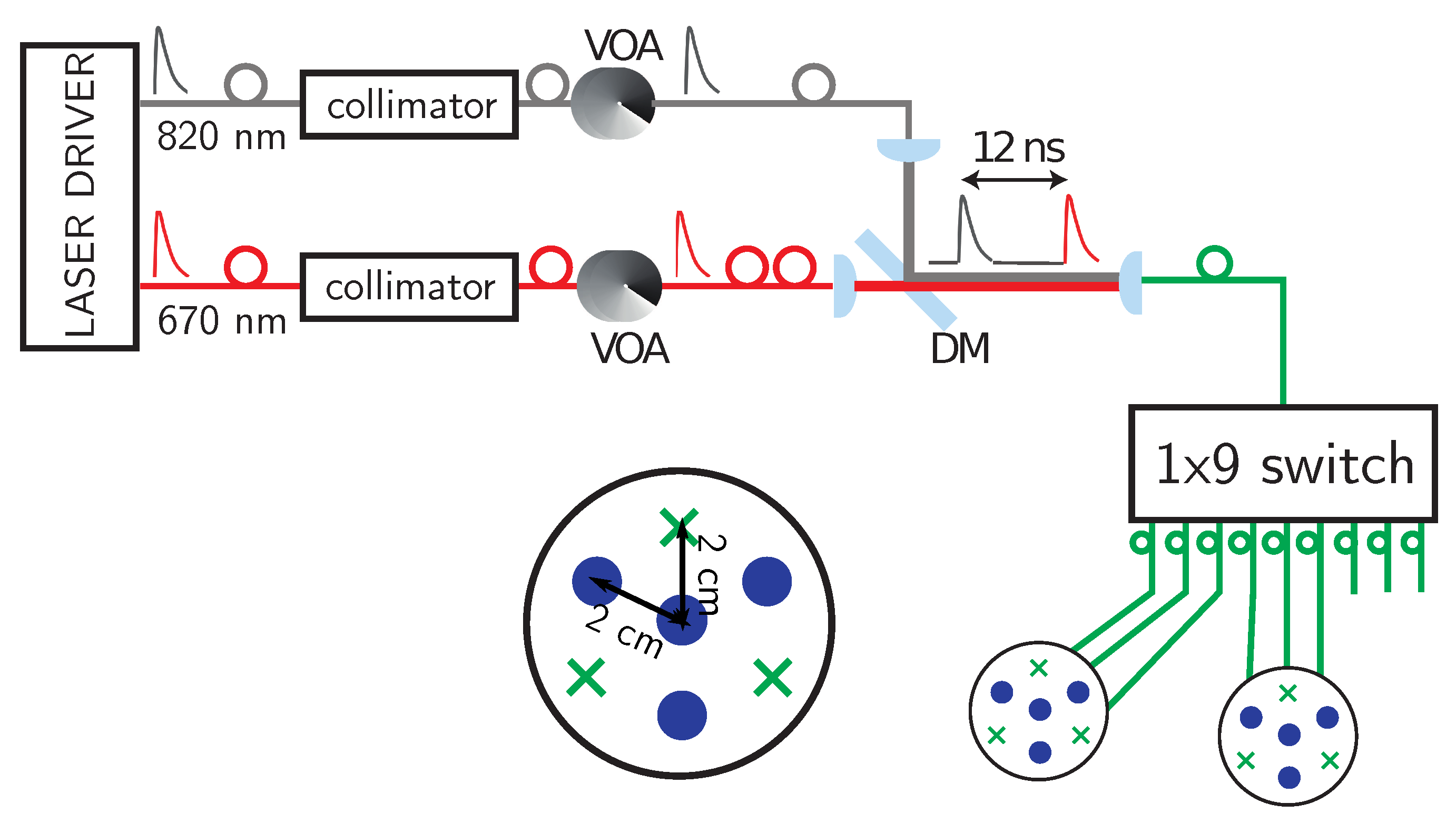
2. System Design
3. Experimental Protocols
3.1. Mechanically Switchable Solid Phantom
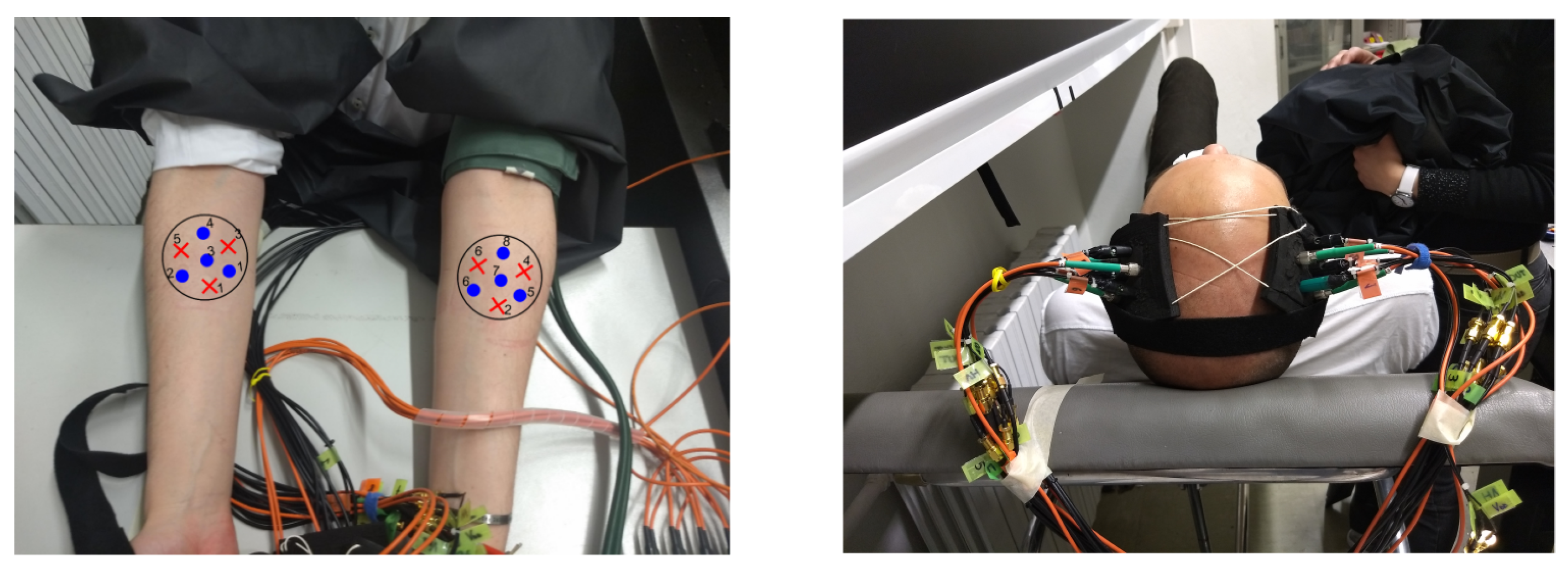
3.2. In-Vivo Experiments
3.2.1. Arm Cuff Occlusion Protocols
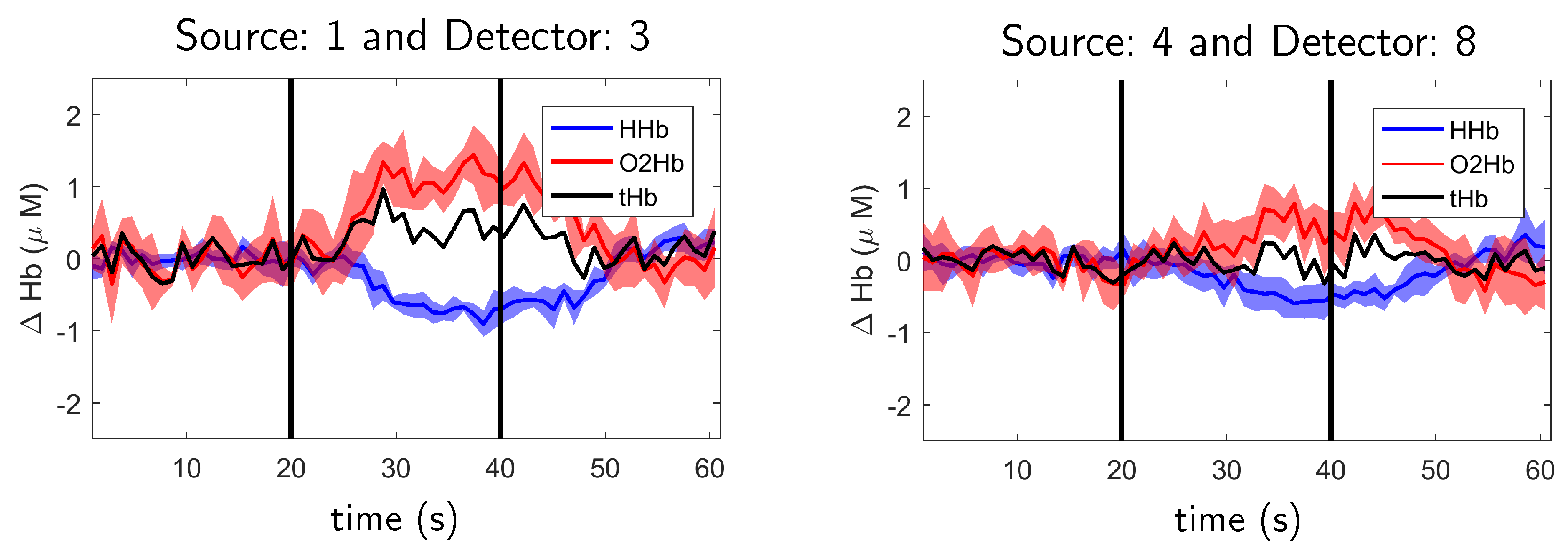
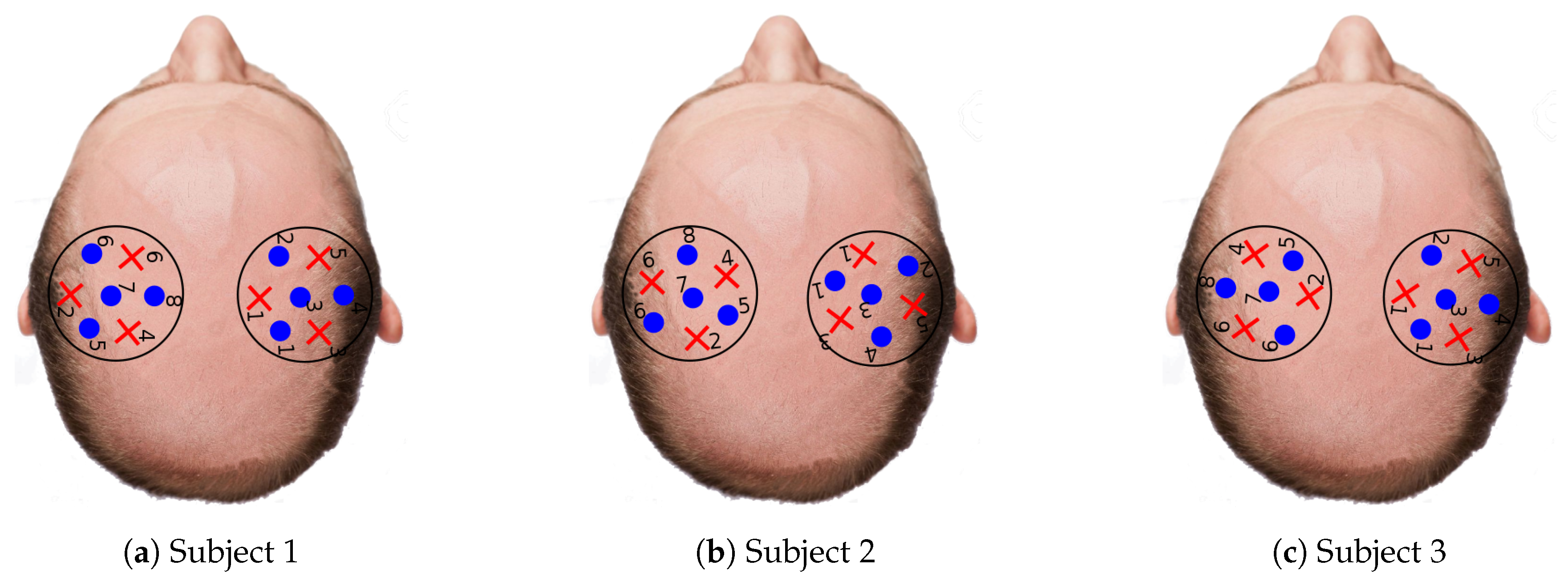
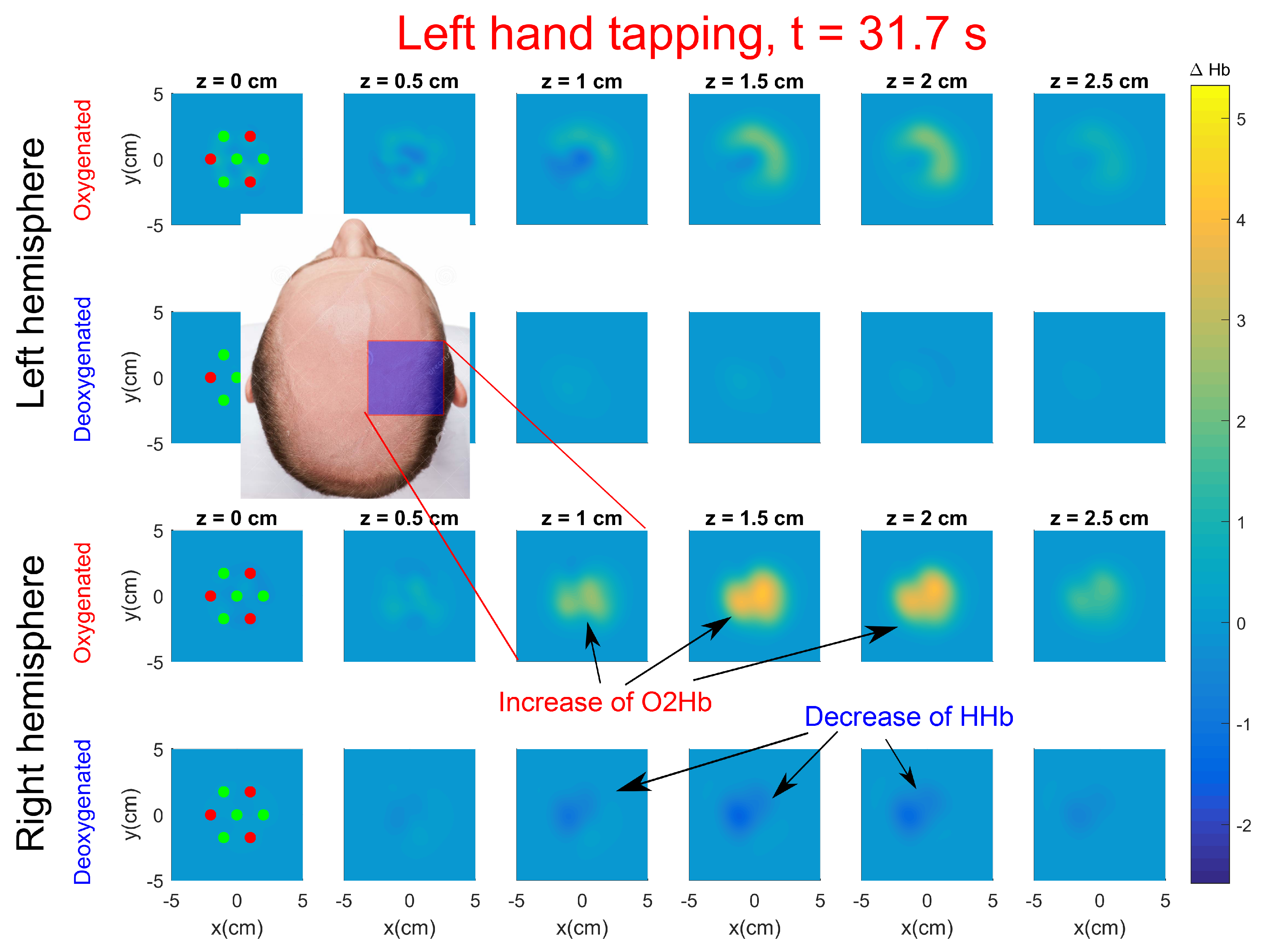
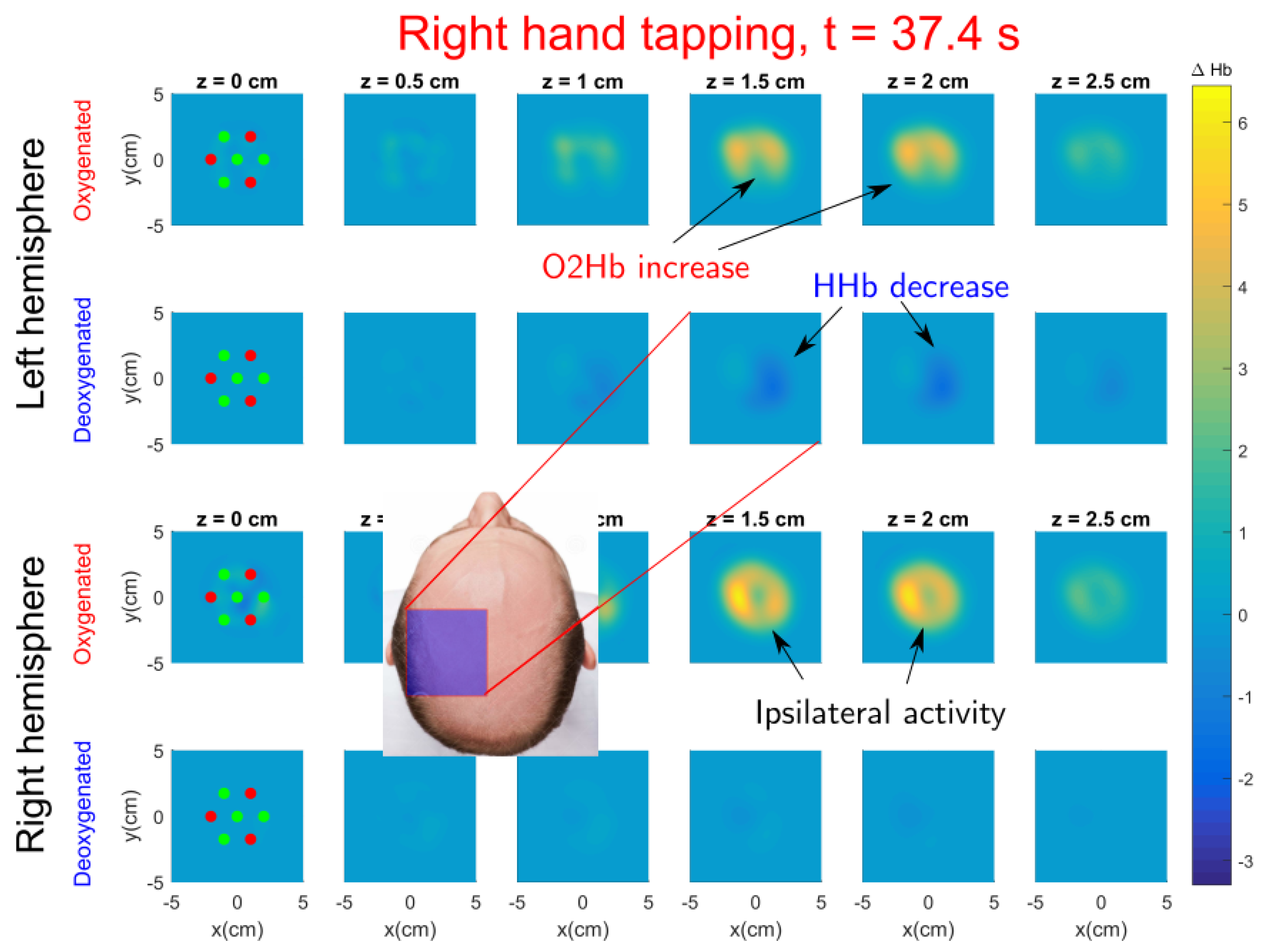
3.2.2. Finger Tapping Protocol
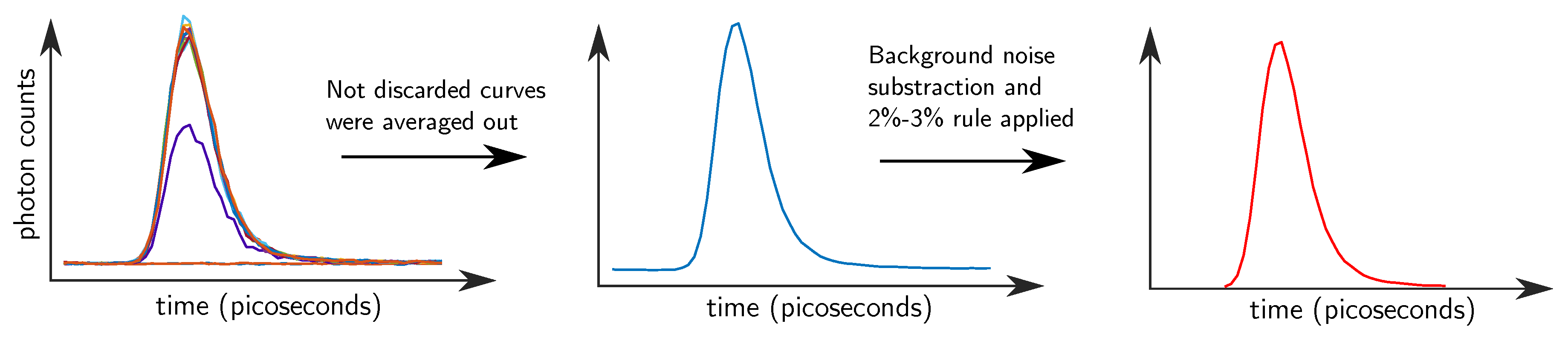
3.3. Data Processing
3.3.1. Pre-Processing
3.3.2. Intensity and Time-of-Flight Data Analysis
3.3.3. Mellin–Laplace Based Tomographic Algorithm
4. Results and Discussion
4.1. Solid Phantom
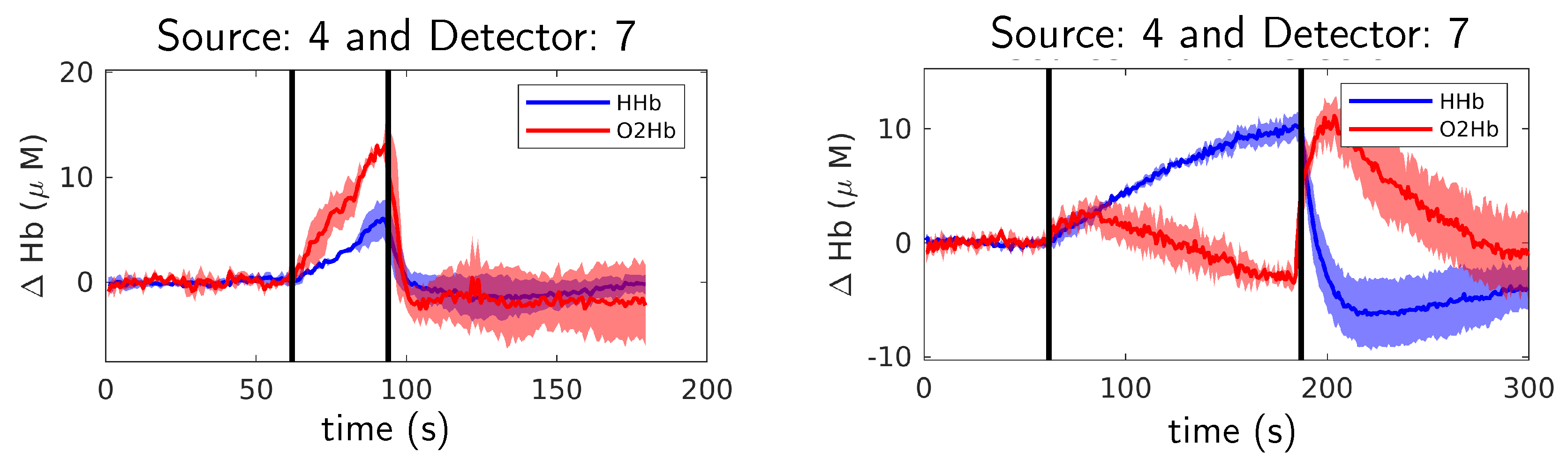
4.2. Arm Cuff Occlusion Experiments
4.3. Finger Tapping Experiments
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| DOT | Diffuse Optical Tomography |
| fMRI | functional Magnetic Resonance Imaging |
| PET | Positron Emission Tomography |
| CW | Continuous–Wave |
| TD | Time–Domain |
| TCSPC | Time–Correlated Single-Photon Counting |
| PMT | Photomultiplier Tube |
| SPAD | Single-Photon Avalanche Diode |
| SiPM | Silicon Photomultiplier |
| VOA | Variable Optical Attenuator |
| DM | Dichroic Mirror |
| TDC | Time-to-Digital Converter |
| LV-TTL | Low-Voltage Transistor-Transistor Logic |
| EEG | Electroencephalography |
| DTOF | Distribution of photons time-of-flight |
| SNR | Signal-to-Noise Ratio |
References
- Koch, S.P.; Habermehl, C.; Mehnert, J.; Schmitz, C.H.; Holtze, S.; Villringer, A.; Steinbrink, J.; Obrig, H. High-resolution optical functional mapping of the human somatosensory cortex. Front. Neuroenerg. 2010, 2, 12. [Google Scholar] [CrossRef] [Green Version]
- Singh, H.; Cooper, R.J.; Lee, C.W.; Dempsey, L.; Edwards, A.; Brigadoi, S.; Airantzis, D.; Everdell, N.; Michell, A.; Holder, D.; et al. Mapping cortical haemodynamics during neonatal seizures using diffuse optical tomography: A case study. NeuroImage Clin. 2014, 5, 256–265. [Google Scholar] [CrossRef]
- Pogue, B.W.; Testorf, M.; McBride, T.; Osterberg, U.; Paulsen, K. Instrumentation and design of a frequency-domain diffuse optical tomography imager for breast cancer detection. Opt. Express 1997, 1, 391–403. [Google Scholar] [CrossRef]
- Choe, R.; Konecky, S.D.; Corlu, A.; Lee, K.; Durduran, T.; Busch, D.R.; Pathak, S.; Czerniecki, B.J.; Tchou, J.C.; Fraker, D.L.; et al. Differentiation of benign and malignant breast tumors by in-vivo three-dimensional parallel-plate diffuse optical tomography. J. Biomed. Opt. 2009, 14, 024020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koenig, A.; Hervé, L.; Da Silva, A.; Dinten, J.M.; Boutet, J.; Berger, M.; Texier, I.; Peltié, P.; Rizo, P.; Josserand, V.; et al. Whole body small animal examination with a diffuse optical tomography instrument. Nucl. Instrum. Methods Phys. Res. Sect. A Accel. Spectrom. Detect. Assoc. Equip. 2007, 571, 56–59. [Google Scholar] [CrossRef]
- Dot, A.; Planat-Chrétien, A.; Perriollat, M.; Berger, M.; Lartizien, R.; Henry, M.; Bettega, G.; Coll, J.L. Blood oxygenation in buried flaps, a bi-layer reconstruction. In Proceedings of the European Conference on Biomedical Optics, Munich, Germany, 23–27 June 2019; Optical Society of America: Washington, DC, USA, 2019. [Google Scholar]
- Planat-Chrétien, A.; Berger, M.; Lartizien, R.; Henry, M.; Houang, B.; Bettega, G.; Coll, J.L. Time-Resolved Optical Monitoring to detect and identify deep flaps (Conference Presentation). In Molecular-Guided Surgery: Molecules, Devices, and Applications V; International Society for Optics and Photonics: Bellingham, WA, USA, 2019; Volume 10862, p. 1086207. [Google Scholar]
- Di Sieno, L.; Bettega, G.; Berger, M.; Hamou, C.; Aribert, M.; Dalla Mora, A.; Puszka, A.; Grateau, H.; Contini, D.; Hervé, L.; et al. Toward noninvasive assessment of flap viability with time-resolved diffuse optical tomography: A preclinical test on rats. J. Biomed. Opt. 2016, 21, 025004. [Google Scholar] [CrossRef] [Green Version]
- Durduran, T.; Choe, R.; Baker, W.B.; Yodh, A.G. Diffuse optics for tissue monitoring and tomography. Rep. Prog. Phys. 2010, 73, 076701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eggebrecht, A.T.; Ferradal, S.L.; Robichaux-Viehoever, A.; Hassanpour, M.S.; Dehghani, H.; Snyder, A.Z.; Hershey, T.; Culver, J.P. Mapping distributed brain function and networks with diffuse optical tomography. Nat. Photonics 2014, 8, 448. [Google Scholar] [CrossRef] [Green Version]
- Arridge, S.R.; Lionheart, W.R. Nonuniqueness in diffusion-based optical tomography. Opt. Lett. 1998, 23, 882–884. [Google Scholar] [CrossRef] [Green Version]
- Pifferi, A.; Contini, D.; Dalla Mora, A.; Farina, A.; Spinelli, L.; Torricelli, A. New frontiers in time-domain diffuse optics, a review. J. Biomed. Opt. 2016, 21, 091310. [Google Scholar] [CrossRef] [Green Version]
- Steinbrink, J.; Wabnitz, H.; Obrig, H.; Villringer, A.; Rinneberg, H. Determining changes in NIR absorption using a layered model of the human head. Phys. Med. Biol. 2001, 46, 879. [Google Scholar] [CrossRef] [PubMed]
- Torricelli, A.; Pifferi, A.; Spinelli, L.; Cubeddu, R.; Martelli, F.; Del Bianco, S.; Zaccanti, G. Time-resolved reflectance at null source-detector separation: Improving contrast and resolution in diffuse optical imaging. Phys. Rev. Lett. 2005, 95, 078101. [Google Scholar] [CrossRef] [PubMed]
- Cooper, R.J.; Magee, E.; Everdell, N.; Magazov, S.; Varela, M.; Airantzis, D.; Gibson, A.P.; Hebden, J.C. MONSTIR II: A 32-channel, multispectral, time-resolved optical tomography system for neonatal brain imaging. Rev. Sci. Instrum. 2014, 85, 053105. [Google Scholar] [CrossRef]
- Eda, H.; Oda, I.; Ito, Y.; Wada, Y.; Oikawa, Y.; Tsunazawa, Y.; Takada, M.; Tsuchiya, Y.; Yamashita, Y.; Oda, M.; et al. Multichannel time-resolved optical tomographic imaging system. Rev. Sci. Instrum. 1999, 70, 3595–3602. [Google Scholar] [CrossRef]
- Ueda, Y.; Yoshimoto, K.; Ohmae, E.; Suzuki, T.; Yamanaka, T.; Yamashita, D.; Ogura, H.; Teruya, C.; Nasu, H.; Imi, E.; et al. Time-resolved optical mammography and its preliminary clinical results. Technol. Cancer Res. Treat. 2011, 10, 393–401. [Google Scholar] [CrossRef] [Green Version]
- Ueda, Y.; Yamanaka, T.; Yamashita, D.; Suzuki, T.; Ohmae, E.; Oda, M.; Yamashita, Y. Reflectance diffuse optical tomography: Its application to human brain mapping. Jpn. J. Appl. Phys. 2005, 44, L1203. [Google Scholar] [CrossRef]
- Puszka, A.; Di Sieno, L.; Dalla Mora, A.; Pifferi, A.; Contini, D.; Boso, G.; Tosi, A.; Hervé, L.; Planat-Chrétien, A.; Koenig, A.; et al. Time-resolved diffuse optical tomography using fast-gated single-photon avalanche diodes. Biomed. Opt. Express 2013, 4, 1351–1365. [Google Scholar] [CrossRef] [Green Version]
- Mu, Y.; Niedre, M. Fast single photon avalanche photodiode-based time-resolved diffuse optical tomography scanner. Biomed. Opt. Express 2015, 6, 3596–3609. [Google Scholar] [CrossRef] [Green Version]
- Cova, S.; Ghioni, M.; Lacaita, A.; Samori, C.; Zappa, F. Avalanche photodiodes and quenching circuits for single-photon detection. Appl. Opt. 1996, 35, 1956–1976. [Google Scholar] [CrossRef]
- Dalla Mora, A.; Martinenghi, E.; Contini, D.; Tosi, A.; Boso, G.; Durduran, T.; Arridge, S.; Martelli, F.; Farina, A.; Torricelli, A.; et al. Fast silicon photomultiplier improves signal harvesting and reduces complexity in time-domain diffuse optics. Opt. Express 2015, 23, 13937–13946. [Google Scholar] [CrossRef] [Green Version]
- Zimmermann, R.; Braun, F.; Achtnich, T.; Lambercy, O.; Gassert, R.; Wolf, M. Silicon photomultipliers for improved detection of low light levels in miniature near-infrared spectroscopy instruments. Biomed. Opt. Express 2013, 4, 659–666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maira, G.; Chiarelli, A.M.; Brafa, S.; Libertino, S.; Fallica, G.; Merla, A.; Lombardo, S. Imaging System Based on Silicon Photomultipliers and Light Emitting Diodes for Functional Near-Infrared Spectroscopy. Appl. Sci. 2020, 10, 1068. [Google Scholar] [CrossRef] [Green Version]
- Kitsmiller, V.J.; O’Sullivan, T.D. Next-generation frequency domain diffuse optical imaging systems using silicon photomultipliers. Opt. Lett. 2019, 44, 562–565. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Bai, Y.; Wu, H.; Xu, M.; Cao, X.; Chen, X.; Zhu, S. Feasibility study of silicon photomultiplier based frequency domain diffuse optical tomography. In Medical Imaging 2019: Physics of Medical Imaging; International Society for Optics and Photonics: Bellingham, WA, USA, 2019; Volume 10948, p. 109483V. [Google Scholar]
- Di Sieno, L.; Pifferi, A.; Zouaoui, J.; Hervé, L.; Martinenghi, E.; Farina, A.; Derouard, J.; Dinten, J.M.; Dalla Mora, A. Time-domain diffuse optical tomography using silicon photomultipliers: Feasibility study. J. Biomed. Opt. 2016, 21, 116002. [Google Scholar] [CrossRef] [Green Version]
- Farina, A.; Tagliabue, S.; Di Sieno, L.; Martinenghi, E.; Durduran, T.; Arridge, S.; Martelli, F.; Torricelli, A.; Pifferi, A.; Dalla Mora, A. Time-domain functional diffuse optical tomography system based on fiber-free silicon photomultipliers. Appl. Sci. 2017, 7, 1235. [Google Scholar] [CrossRef] [Green Version]
- Re, R.; Martinenghi, E.; Dalla Mora, A.; Contini, D.; Pifferi, A.; Torricelli, A. Probe-hosted silicon photomultipliers for time-domain functional near-infrared spectroscopy: Phantom and in vivo tests. Neurophotonics 2016, 3, 045004. [Google Scholar] [CrossRef] [Green Version]
- Torricelli, A.; Contini, D.; Pifferi, A.; Caffini, M.; Re, R.; Zucchelli, L.; Spinelli, L. Time domain functional NIRS imaging for human brain mapping. Neuroimage 2014, 85, 28–50. [Google Scholar] [CrossRef] [Green Version]
- Hervé, L.; Puszka, A.; Planat-Chrétien, A.; Dinten, J.M. Time-domain diffuse optical tomography processing by using the Mellin–Laplace transform. Appl. Opt. 2012, 51, 5978–5988. [Google Scholar] [CrossRef]
- Ferocino, E.; Martinenghi, E.; Dalla Mora, A.; Pifferi, A.; Cubeddu, R.; Taroni, P. High throughput detection chain for time domain optical mammography. Biomed. Opt. Express 2018, 9, 755–770. [Google Scholar] [CrossRef] [Green Version]
- Maira, G.; Mazzillo, M.; Libertino, S.; Fallica, G.; Lombardo, S. Crucial aspects for the use of silicon photomultiplier devices in continuous wave functional near-infrared spectroscopy. Biomed. Opt. Express 2018, 9, 4679–4688. [Google Scholar] [CrossRef]
- Pifferi, A.; Torricelli, A.; Cubeddu, R.; Quarto, G.; Re, R.; Sekar, S.K.; Spinelli, L.; Farina, A.; Martelli, F.; Wabnitz, H. Mechanically switchable solid inhomogeneous phantom for performance tests in diffuse imaging and spectroscopy. J. Biomed. Opt. 2015, 20, 121304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wabnitz, H.; Jelzow, A.; Mazurenka, M.; Steinkellner, O.; Macdonald, R.; Milej, D.; Żołek, N.; Kacprzak, M.; Sawosz, P.; Maniewski, R.; et al. Performance assessment of time-domain optical brain imagers, part 2: nEUROPt protocol. J. Biomed. Opt. 2014, 19, 086012. [Google Scholar] [CrossRef] [PubMed]
- Lorenzo, J.R. Principles of Diffuse Light Propagation: Light Propagation in Tissues with Applications in Biology and Medicine; World Scientific: Singapore, 2012. [Google Scholar]
- Liebert, A.; Wabnitz, H.; Steinbrink, J.; Obrig, H.; Möller, M.; Macdonald, R.; Villringer, A.; Rinneberg, H. Time-resolved multidistance near-infrared spectroscopy of the adult head: Intracerebral and extracerebral absorption changes from moments of distribution of times of flight of photons. Appl. Opt. 2004, 43, 3037–3047. [Google Scholar] [CrossRef] [PubMed]
- Orive-Miguel, D.; Hervé, L.; Condat, L.; Mars, J. Improving Localization of Deep Inclusions in Time-Resolved Diffuse Optical Tomography. Appl. Sci. 2019, 9, 5468. [Google Scholar] [CrossRef] [Green Version]
- Chiarelli, A.M.; Maclin, E.L.; Low, K.A.; Mathewson, K.E.; Fabiani, M.; Gratton, G. Combining energy and Laplacian regularization to accurately retrieve the depth of brain activity of diffuse optical tomographic data. J. Biomed. Opt. 2016, 21, 036008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, Q.; Ji, L.; Jiang, T. Improving depth resolution of diffuse optical tomography with a layer-based sigmoid adjustment method. Opt. Express 2007, 15, 4018–4029. [Google Scholar] [CrossRef]
- Pogue, B.W.; McBride, T.O.; Prewitt, J.; Österberg, U.L.; Paulsen, K.D. Spatially variant regularization improves diffuse optical tomography. Appl. Opt. 1999, 38, 2950–2961. [Google Scholar] [CrossRef]
- Culver, J.P.; Durduran, T.; Furuya, D.; Cheung, C.; Greenberg, J.H.; Yodh, A. Diffuse optical tomography of cerebral blood flow, oxygenation, and metabolism in rat during focal ischemia. J. Cereb. Blood Flow Metab. 2003, 23, 911–924. [Google Scholar] [CrossRef] [Green Version]
- Niu, H.; Tian, F.; Lin, Z.J.; Liu, H. Development of a compensation algorithm for accurate depth localization in diffuse optical tomography. Opt. Lett. 2010, 35, 429–431. [Google Scholar] [CrossRef]
- Niu, H.; Lin, Z.; Tian, F.; Dhamne, S.; Liu, H. Comprehensive investigation of three-dimensional diffuse optical tomography with depth compensation algorithm. J. Biomed. Opt. 2010, 15, 046005. [Google Scholar] [CrossRef]
- Zouaoui, J.; Di Sieno, L.; Hervé, L.; Pifferi, A.; Farina, A.; Dalla Mora, A.; Derouard, J.; Dinten, J.M. Quantification in time-domain diffuse optical tomography using Mellin-Laplace transforms. Biomed. Opt. Express 2016, 7, 4346–4363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buxton, R.B. Introduction to Functional Magnetic Resonance Imaging: Principles and Techniques; Cambridge University Press: Cambridge, UK, 2009. [Google Scholar]
- Huppert, T.J.; Allen, M.S.; Diamond, S.G.; Boas, D.A. Estimating cerebral oxygen metabolism from fMRI with a dynamic multicompartment Windkessel model. Hum. Brain Mapp. 2009, 30, 1548–1567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frostig, R.D. In Vivo Optical Imaging of Brain Function; CRC Press: Boca Ratón, FL, USA, 2009. [Google Scholar]
- Huppert, T.; Barker, J.; Schmidt, B.; Walls, S.; Ghuman, A. Comparison of group-level, source localized activity for simultaneous functional near-infrared spectroscopy-magnetoencephalography and simultaneous fNIRS-fMRI during parametric median nerve stimulation. Neurophotonics 2017, 4, 015001. [Google Scholar] [CrossRef] [PubMed]
- Buxton, R.B.; Uludağ, K.; Dubowitz, D.J.; Liu, T.T. Modeling the hemodynamic response to brain activation. Neuroimage 2004, 23, S220–S233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehagnoul-Schipper, D.J.; van der Kallen, B.F.; Colier, W.N.; van der Sluijs, M.C.; van Erning, L.J.T.O.; Thijssen, H.O.; Oeseburg, B.; Hoefnagels, W.H.; Jansen, R.W. Simultaneous measurements of cerebral oxygenation changes during brain activation by near-infrared spectroscopy and functional magnetic resonance imaging in healthy young and elderly subjects. Hum. Brain Mapp. 2002, 16, 14–23. [Google Scholar] [CrossRef]
- Chitnis, D.; Cooper, R.J.; Dempsey, L.; Powell, S.; Quaggia, S.; Highton, D.; Elwell, C.; Hebden, J.C.; Everdell, N.L. Functional imaging of the human brain using a modular, fibre-less, high-density diffuse optical tomography system. Biomed. Opt. Express 2016, 7, 4275–4288. [Google Scholar] [CrossRef]
- Mattay, V.S.; Callicott, J.H.; Bertolino, A.; Santha, A.K.; Van Horn, J.D.; Tallent, K.A.; Frank, J.A.; Weinberger, D.R. Hemispheric control of motor function: A whole brain echo planar fMRI study. Psychiatry Res. Neuroimaging 1998, 83, 7–22. [Google Scholar] [CrossRef]
- Tinazzi, M.; Zanette, G. Modulation of ipsilateral motor cortex in man during unimanual finger movements of different complexities. Neurosci. Lett. 1998, 244, 121–124. [Google Scholar] [CrossRef]
- O’Connor, D. Time-Correlated Single Photon Counting; Academic Press: Cambridge, MA, USA, 2012. [Google Scholar]










© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orive-Miguel, D.; Di Sieno, L.; Behera, A.; Ferocino, E.; Contini, D.; Condat, L.; Hervé, L.; Mars, J.; Torricelli, A.; Pifferi, A.; et al. Real-Time Dual-Wavelength Time-Resolved Diffuse Optical Tomography System for Functional Brain Imaging Based on Probe-Hosted Silicon Photomultipliers. Sensors 2020, 20, 2815. https://doi.org/10.3390/s20102815
Orive-Miguel D, Di Sieno L, Behera A, Ferocino E, Contini D, Condat L, Hervé L, Mars J, Torricelli A, Pifferi A, et al. Real-Time Dual-Wavelength Time-Resolved Diffuse Optical Tomography System for Functional Brain Imaging Based on Probe-Hosted Silicon Photomultipliers. Sensors. 2020; 20(10):2815. https://doi.org/10.3390/s20102815
Chicago/Turabian StyleOrive-Miguel, David, Laura Di Sieno, Anurag Behera, Edoardo Ferocino, Davide Contini, Laurent Condat, Lionel Hervé, Jérôme Mars, Alessandro Torricelli, Antonio Pifferi, and et al. 2020. "Real-Time Dual-Wavelength Time-Resolved Diffuse Optical Tomography System for Functional Brain Imaging Based on Probe-Hosted Silicon Photomultipliers" Sensors 20, no. 10: 2815. https://doi.org/10.3390/s20102815
APA StyleOrive-Miguel, D., Di Sieno, L., Behera, A., Ferocino, E., Contini, D., Condat, L., Hervé, L., Mars, J., Torricelli, A., Pifferi, A., & Dalla Mora, A. (2020). Real-Time Dual-Wavelength Time-Resolved Diffuse Optical Tomography System for Functional Brain Imaging Based on Probe-Hosted Silicon Photomultipliers. Sensors, 20(10), 2815. https://doi.org/10.3390/s20102815