Fusion iENA Scholar Study: Sensor-Navigated I-124-PET/US Fusion Imaging versus Conventional Diagnostics for Retrospective Functional Assessment of Thyroid Nodules by Medical Students

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients, Ethics, and Registrations
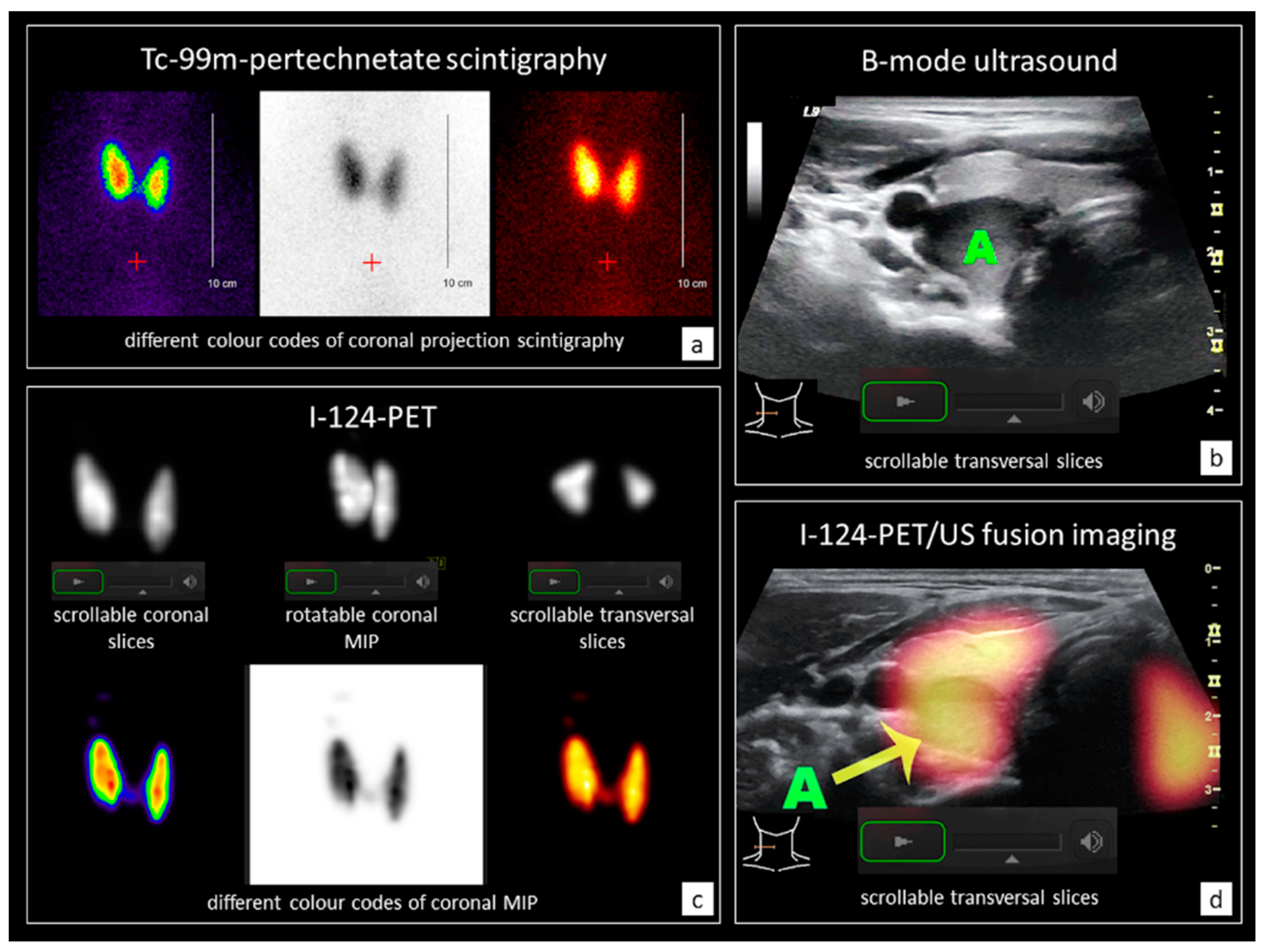
2.2. Conventional Diagnostics (CD) and I-124-PET/US Fusion Imaging (PET/US)
2.3. Patient Case Files (PCF) and Observers
2.4. Data Analyses/Statistics
3. Results
3.1. Patient and Observer Data
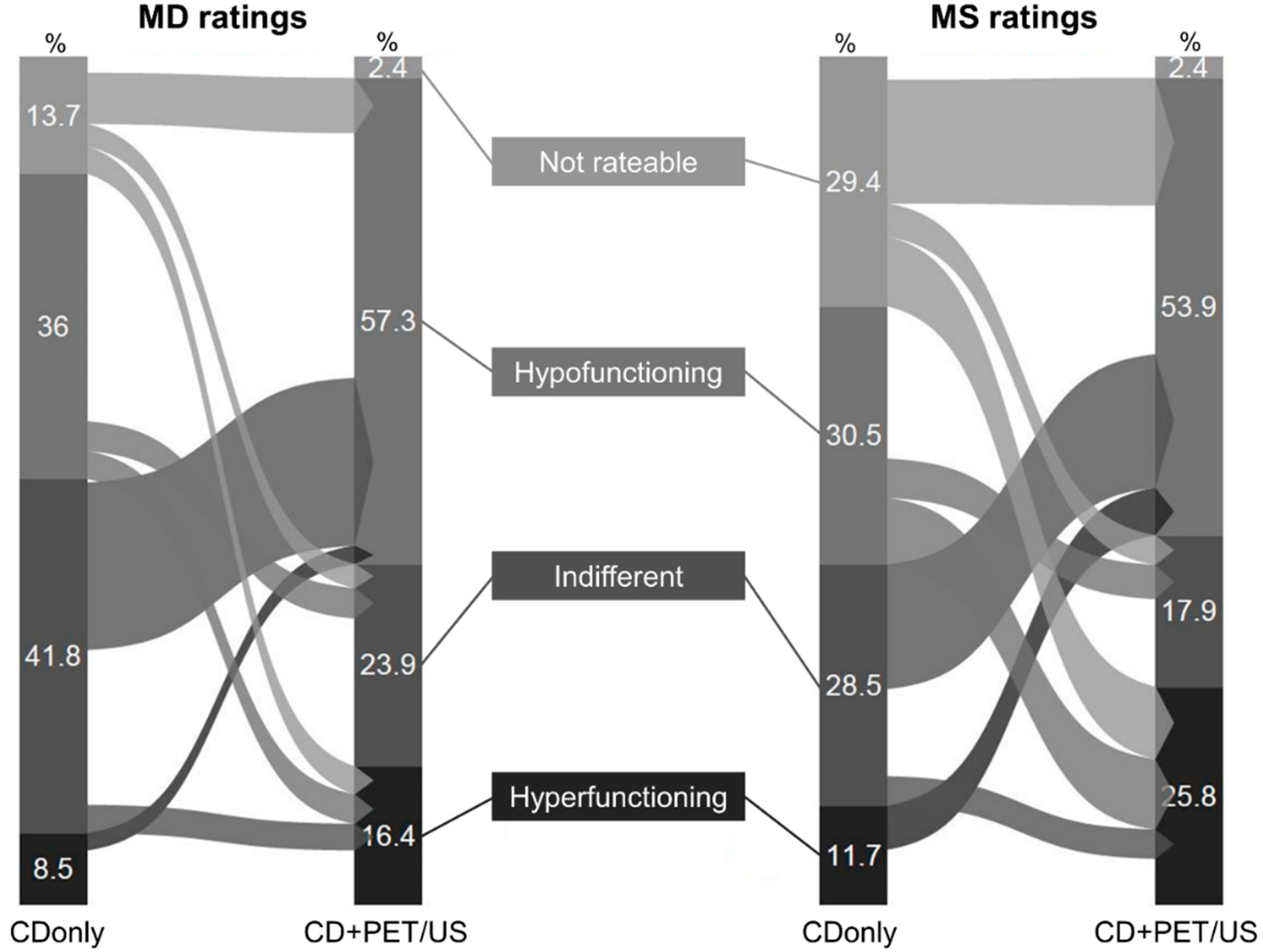
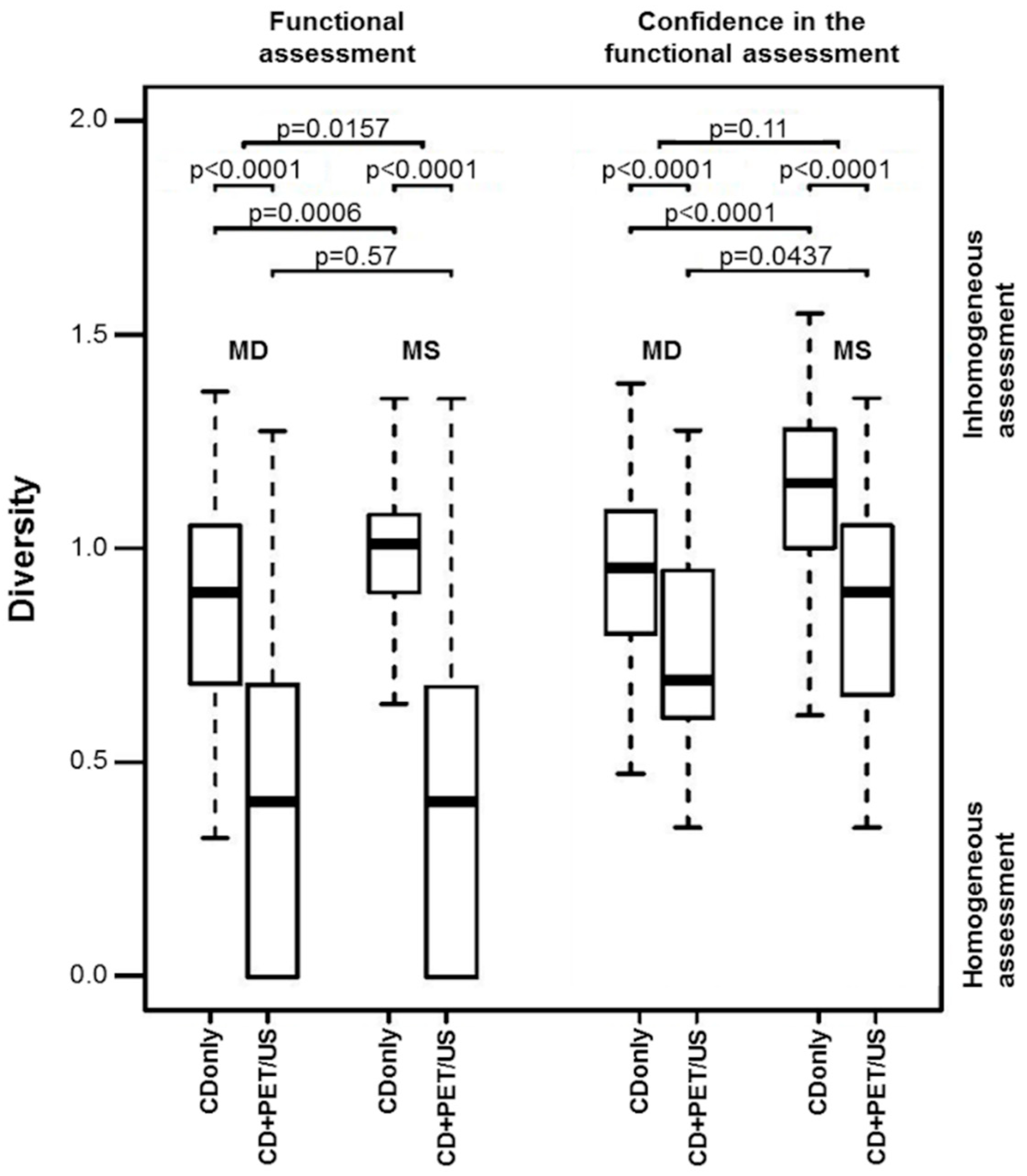
3.2. Functional Assessment
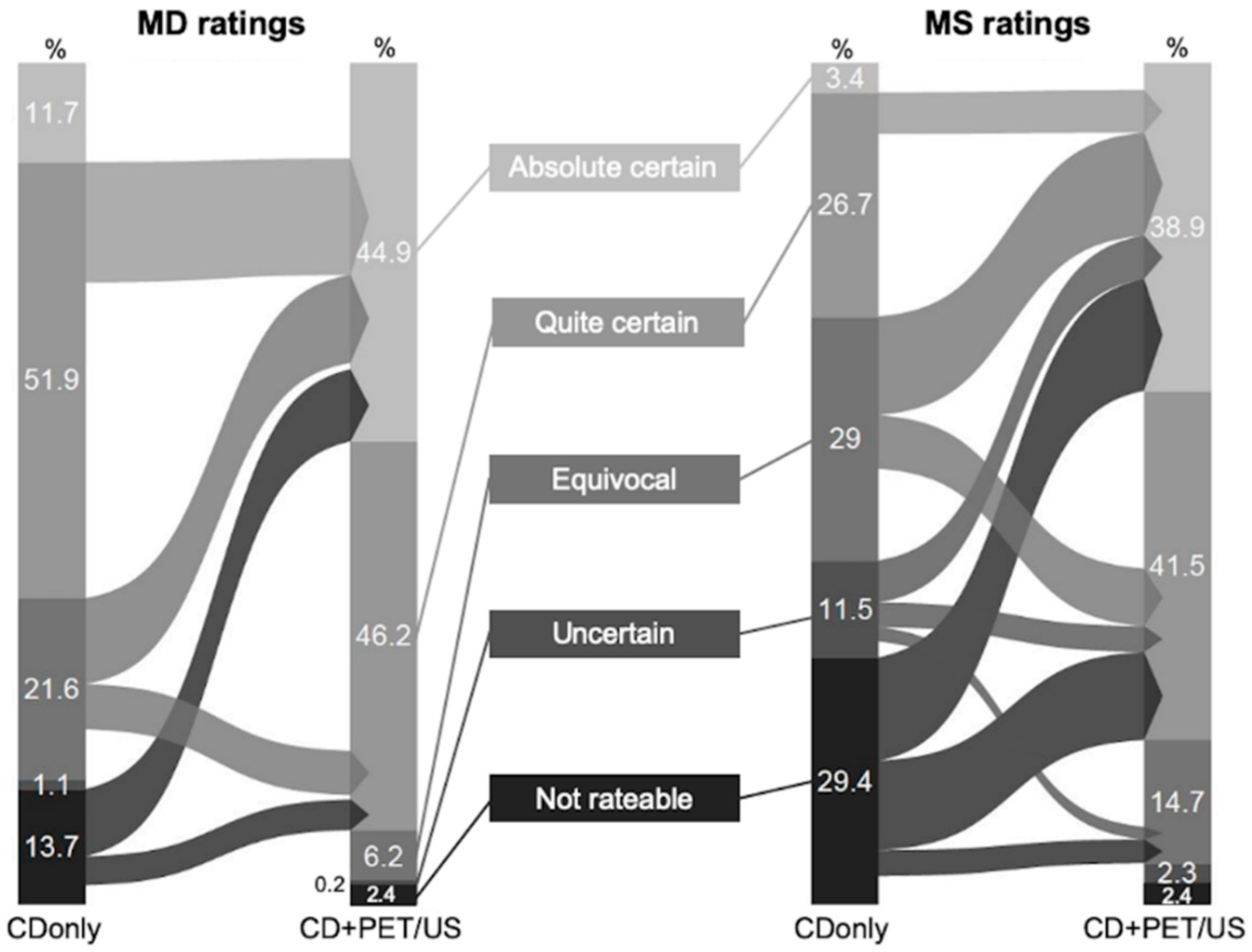
3.3. Confidence in Functional Assessment
4. Discussion
4.1. Statement of Principal Findings
4.2. Strengths and Weaknesses of the Study
4.3. Implications for Clinicians
4.4. Unanswered Questions and Future Research
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Key Points
References
- Moon, J.H.; Hyun, M.K.; Lee, J.Y.; Im Shim, J.; Kim, T.H.; Choi, H.S.; Ahn, H.Y.; Kim, K.W.; Park, D.J.; Park, Y.J.; et al. Prevalence of thyroid nodules and their associated clinical parameters: A large-scale, multicenter-based health checkup study. Korean J. Intern. Med. 2018, 33, 753–762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reiners, C.; Schumm-Draeger, P.M.; Geling, M.; Mastbaum, C.; Schönberger, J.; Laue-Savic, A.; Hackethal, K.; Hampel, R.; Heinken, U.; Kullak, W.; et al. Thyroid gland ultrasound screening (Papillon Initiative). Report of 15 incidentally detected thyroid cancers. Internist (Berlin) 2003, 44, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Verburg, F.A.; Grelle, I.; Tatschner, K.; Reiners, C.; Luster, M. Prevalence of thyroid disorders in elderly people in Germany. A screening study in a country with endemic goitre. Nuklearmedizin 2017, 56, 9–13. [Google Scholar] [CrossRef]
- Durante, C.; Costante, G.; Lucisano, G.; Bruno, R.; Meringolo, D.; Paciaroni, A.; Puxeddu, E.; Torlontano, M.; Tumino, S.; Attard, M.; et al. The natural history of benign thyroid nodules. JAMA 2015, 313, 926–935. [Google Scholar] [CrossRef]
- Oh, C.M.; Jung, K.W.; Won, Y.J.; Shin, A.; Kong, H.J.; Lee, J.S. Age-Period-Cohort Analysis of Thyroid Cancer Incidence in Korea. Cancer Res. Treat. 2015, 47, 362–369. [Google Scholar] [CrossRef] [Green Version]
- Kitahara, C.M.; Sosa, J.A. The changing incidence of thyroid cancer. Nat. Rev. Endocrinol. 2016, 12, 646–653. [Google Scholar] [CrossRef]
- Galuppini, F.; Pennelli, G.; Rugge, M. The rising incidence of papillary thyroid cancer: More cancers or more assessments? Indian J. Cancer 2019, 56, 183–184. [Google Scholar]
- Pereira, M.M.; Williams, V.L.; Hallanger-Johnson, J.E.; Valderrabano, P. Thyroid cancer incidence trends in the United States: Association with changes in professional guidelines’ recommendations. Thyroid 2020. [Google Scholar] [CrossRef]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaccarella, S.; Franceschi, S.; Bray, F.; Wild, C.P.; Plummer, M.; Dal Maso, L. Worldwide Thyroid-Cancer Epidemic? The Increasing Impact of Overdiagnosis. N. Engl. J. Med. 2016, 375, 614–617. [Google Scholar] [CrossRef] [PubMed]
- Seifert, P.; Freesmeyer, M. Preoperative diagnostics in differentiated thyroid carcinoma. Nuklearmedizin 2017, 56, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Evranos, B.; Polat, S.B.; Cuhaci, F.N.; Baser, H.; Topaloglu, O.; Kilicarslan, A.; Kilic, M.; Ersoy, R.; Cakir, B. A cancer of undetermined significance: Incidental thyroid carcinoma. Diagn. Cytopathol. 2019, 47, 412–416. [Google Scholar] [CrossRef] [PubMed]
- Wienhold, R.; Scholz, M.; Adler, J.B.; Günster, C.; Paschke, R. The management of thyroid nodules: A retrospective analysis of health insurance data. Dtsch. Arztebl. Int. 2013, 110, 827–834. [Google Scholar] [PubMed] [Green Version]
- Horvath, E.; Majlis, S.; Rossi, R.; Franco, C.; Niedmann, J.P.; Castro, A.; Dominguez, M. An ultrasonogram reporting system for thyroid nodules stratifying cancer risk for clinical management. J. Clin. Endocrinol. Metab. 2009, 94, 1748–1751. [Google Scholar] [CrossRef] [PubMed]
- Tessler, F.N.; Middleton, W.D.; Grant, E.G.; Hoang, J.K.; Berland, L.L.; Teefey, S.A.; Cronan, J.J.; Beland, M.D.; Desser, T.S.; Frates, M.C.; et al. ACR Thyroid Imaging, Reporting and Data System (TI-RADS): White Paper of the ACR TI-RADS Committee. J. Am. Coll. Radiol. 2017, 14, 587–595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azizi, G.; Keller, J.; Lewis, M.; Puett, D.; Rivenbark, K.; Malchoff, C. Performance of elastography for the evaluation of thyroid nodules: A prospective study. Thyroid 2013, 23, 734–740. [Google Scholar] [CrossRef]
- Cantisani, V.; Bertolotto, M.; Weskott, H.P.; Romanini, L.; Grazhdani, H.; Passamonti, M.; Drudi, F.M.; Malpassini, F.; Isidori, A.; Meloni, F.M.; et al. Growing indications for CEUS: The kidney, testis, lymph nodes, thyroid, prostate, and small bowel. Eur. J. Radiol. 2015, 84, 1675–1684. [Google Scholar] [CrossRef]
- Roll, W.; Markwardt, N.A.; Masthoff, M.; Helfen, A.; Claussen, J.; Eisenblätter, M.; Hasenbach, A.; Hermann, S.; Karlas, A.; Wildgruber, M.; et al. Multispectral Optoacoustic Tomography of Benign and Malignant Thyroid Disorders: A Pilot Study. J. Nucl. Med. 2019, 60, 1461–1466. [Google Scholar] [CrossRef]
- Perros, P.; Boelaert, K.; Colley, S.; Evans, C.; Evans, R.M.; Gerrard, B.A.G.; Gilbert, J.; Harrison, B.; Johnson, S.J.; Giles, T.E.; et al. Guidelines for the management of thyroid cancer. Clin. Endocrinol. (Oxford) 2014, 81 (Suppl. 1), 1–122. [Google Scholar] [CrossRef]
- Liu, J.; Wang, Y.; Da, D.; Zheng, M. Hyperfunctioning thyroid carcinoma: A systematic review. Mol. Clin. Oncol. 2019, 11, 535–550. [Google Scholar] [CrossRef] [Green Version]
- Rosario, P.W.; Rocha, T.G.; Mourao, G.F.; Calsolari, M.R. Is radioiodine scintigraphy still of value in thyroid nodules with indeterminate cytology?: A prospective study in an iodine-sufficient area. Nucl. Med. Commun. 2018, 39, 1059–1060. [Google Scholar] [CrossRef] [PubMed]
- Schenke, S.; Seifert, P.; Zimny, M.; Winkens, T.; Binse, I.; Goerges, R. Risk stratification of thyroid nodules using thyroid imaging reporting and data system (TIRADS): The omission of thyroid scintigraphy increases the rate of falsely suspected lesions. J. Nucl. Med. 2019, 60, 342–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noto, B.; Eveslage, M.; Pixberg, M.; Carvalho, J.M.; Schäfers, M.; Riemann, B.; Kies, P. Prevalence of hyperfunctioning thyroid nodules among those in need of fine needle aspiration cytology according to ATA 2015, EU-TIRADS, and ACR-TIRADS. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 1518–1526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freesmeyer, M.; Winkens, T.; Kuehnel, C.; Opfermann, T.; Seifert, P. 99mTc-Pertechnetate-SPECT/US Hybrid Imaging Enhances Diagnostic Certainty Compared With Conventional Thyroid Imaging With Scintigraphy and Ultrasound. Clin. Nucl. Med. 2018, 43, 747–748. [Google Scholar] [CrossRef] [PubMed]
- Freesmeyer, M.; Winkens, T.; Kuhnel, C.; Opfermann, T.; Seifert, P. Technetium-99m SPECT/US Hybrid Imaging Compared with Conventional Diagnostic Thyroid Imaging with Scintigraphy and Ultrasound. Ultrasound Med. Biol. 2019, 45, 1243–1252. [Google Scholar] [CrossRef]
- Seifert, P.; Guhne, F.; Freesmeyer, M. Hyperfunctioning Papillary Microcarcinoma Diagnosed by 124I PET/Ultrasound Fusion Imaging. Clin. Nucl. Med. 2019, 44, 404–405. [Google Scholar] [CrossRef]
- Seifert, P.; Winkens, T.; Kuhnel, C.; Guhne, F.; Freesmeyer, M. I-124-PET/US Fusion Imaging in Comparison to Conventional Diagnostics and Tc-99m Pertechnetate SPECT/US Fusion Imaging for the Function Assessment of Thyroid Nodules. Ultrasound Med. Biol. 2019, 45, 2298–2308. [Google Scholar] [CrossRef]
- Winkens, T.; Seifert, P.; Hollenbach, C.; Kuhnel, C.; Guhne, F.; Freesmeyer, M. The FUSION iENA Study: Comparison of I-124-PET/US Fusion Imaging with Conventional Diagnostics for the Functional Assessment of Thyroid Nodules by Multiple Observers. Nuklearmedizin 2019, 58, 434–442. [Google Scholar] [CrossRef]
- Freesmeyer, M.; Schleussner, E.; Winkens, T. Diagnosis of struma ovarii in a patient with papillary thyroid carcinoma--verification via 124I-PET/US fusion. Ultraschall Med. 2014, 35, 368–370. [Google Scholar] [CrossRef]
- Freesmeyer, M.; Winkens, T.; Darr, A. Diagnosis of small papillary thyroid cancer via sensor-navigated (124)iodine PET/ultrasound ((124)I-PET/US) fusion. J. Clin. Endocrinol. Metab. 2015, 100, 13–14. [Google Scholar] [CrossRef] [Green Version]
- Freesmeyer, M.; Opfermann, T. Diagnosis of de quervain’s subacute thyroiditis via sensor-navigated 124Iodine PET/ultrasound (124I-PET/US) fusion. Endocrine 2015, 49, 293–295. [Google Scholar] [CrossRef] [PubMed]
- Kwak, J.Y.; Han, K.H.; Yoon, J.H.; Moon, H.J.; Son, E.J.; Park, S.H.; Jung, H.K.; Choi, J.S.; Kim, B.M.; Kim, E.-K. Thyroid imaging reporting and data system for US features of nodules: A step in establishing better stratification of cancer risk. Radiology 2011, 260, 892–899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russ, G.; Bonnema, S.J.; Erdogan, M.F.; Durante, C.; Ngu, R.; Leenhardt, L. European Thyroid Association Guidelines for Ultrasound Malignancy Risk Stratification of Thyroid Nodules in Adults: The EU-TIRADS. Eur. Thyroid J. 2017, 6, 225–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grani, G.; Lamartina, L.; Cantisani, V.; Maranghi, M.; Lucia, P.; Durante, C. Interobserver agreement of various thyroid imaging reporting and data systems. Endocr. Connect. 2018, 7, 1–7. [Google Scholar] [CrossRef]
- Seifert, P.; Gorges, R.; Zimny, M.; Kreissl, M.C.; Schenke, S. Interobserver agreement and efficacy of consensus reading in Kwak-, EU-, and ACR-thyroid imaging recording and data systems and ATA guidelines for the ultrasound risk stratification of thyroid nodules. Endocrine 2020, 67, 143–154. [Google Scholar] [CrossRef]
- Baek, H.J.; Kim, D.W.; Ryu, K.H.; Shin, G.W.; Park, J.Y.; Lee, Y.J.; Choo, H.J.; Park, H.K.; Ha, T.K.; Kim, D.H.; et al. Thyroid Imaging Reporting and Data System for Detecting Diffuse Thyroid Disease on Ultrasonography: A Single-Center Study. Front. Endocrinol. (Lausanne) 2019, 10, 776. [Google Scholar] [CrossRef]
- Schroder, S.; Marthaler, B. Autonomy and malignancy of thyroid glad tumors. A critical analysis of the literature on the existence of hyperfunctioning follicular and papillary thyroid gland carcinomas. Pathologe 1996, 17, 349–357. [Google Scholar]
- Görges, R.; Kandror, T.; Kuschnerus, S.; Zimny, M.; Pink, R.; Palmedo, H.; Hach, A.; Rau, H.; Tanner, C.; Zaplatnikov, K.; et al. Scintigraphically “hot” thyroid nodules mainly go hand in hand with a normal TSH. Nuklearmedizin 2011, 50, 179–188. [Google Scholar]
- Treglia, G.; Trimboli, P.; Verburg, F.A.; Luster, M.; Giovanella, L. Prevalence of normal TSH value among patients with autonomously functioning thyroid nodule. Eur. J. Clin. Investig. 2015, 45, 739–744. [Google Scholar] [CrossRef]
- Reschini, E.; Ferrari, C.; Castellani, M.; Matheoud, R.; Paracchi, A.; Marotta, G.; Gerundini, P. The trapping-only nodules of the thyroid gland: Prevalence study. Thyroid 2006, 16, 757–762. [Google Scholar] [CrossRef]
- Wong, K.K.; Gandhi, A.; Viglianti, B.L.; Fig, L.M.; Rubello, D.; Gross, M.D. Endocrine radionuclide scintigraphy with fusion single photon emission computed tomography/computed tomography. World J. Radiol. 2016, 8, 635–655. [Google Scholar] [CrossRef] [PubMed]
- Giovanella, L.; Ceriani, L.; Treglia, G. Role of isotope scan, including positron emission tomography/computed tomography, in nodular goitre. Best Pract. Res. Clin. Endocrinol. Metab. 2014, 28, 507–518. [Google Scholar] [CrossRef] [PubMed]
- Rahmim, A.; Zaidi, H. PET versus SPECT: Strengths, limitations and challenges. Nucl. Med. Commun. 2008, 29, 193–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westphal, J.G.; Winkens, T.; Kuhnel, C.; Freesmeyer, M. Low-activity (124)I-PET/low-dose CT versus (131)I probe measurements in pretherapy assessment of radioiodine uptake in benign thyroid diseases. J. Clin. Endocrinol. Metab. 2014, 99, 2138–2145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berman, M.; Braverman, L.E.; Burke, J.; De Groot, L.; McCormack, K.R.; Oddie, T.H.; Rohrer, R.H.; Wellman, H.N.; Smith, E.M. Summary of current radiation dose estimates to humans from 123I, 124I, 125I, 126I, 130I, 131I, and 132I as sodium iodide. J. Nucl. Med. 1975, 16, 857–860. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Functional Assessment | CDonly (n = 555) | CD+PET/US (n = 532) | p Values |
|---|---|---|---|
| Hyperfunctioning, n (%) | |||
| MD | 47 (8.5) | 87 (16.4) | <0.0001 |
| MS | 65 (11.7) | 137 (25.8) | <0.0001 |
| p values | 0.0902 | 0.0002 | |
| Indifferent, n (%) | |||
| MD | 232 (41.8) | 127 (23.9) | <0.0001 |
| MS | 158 (28.5) | 95 (17.9) | <0.0001 |
| p values | <0.0001 | 0.0193 | |
| Hypofunctioning, n (%) | |||
| MD | 200 (36.0) | 305 (57.3) | <0.0001 |
| MS | 169 (30.5) | 287 (53.9) | <0.0001 |
| p values | 0.0559 | 0.31 | |
| Not Rateable, n (%) | |||
| MD | 76 (13.7) | 13 (2.4) | <0.0001 |
| MS | 163 (29.4) | 13 (2.4) | <0.0001 |
| p values | <0.0001 | 0.99 | |
| Rating Confidence | CDonly (n = 555) | CD+PET/US (n = 532) | p Values |
|---|---|---|---|
| Absolute Certain, n (%) | |||
| MD | 65 (11.7) | 239 (44.9) | <0.0001 |
| MS | 19 (3.4) | 207 (38.9) | <0.0001 |
| p values | <0.0001 | 0.0541 | |
| Quite Certain, n (%) | |||
| MD | 288 (51.9) | 246 (46.2) | 0.0715 |
| MS | 148 (26.7) | 221 (41.5) | <0.0001 |
| p values | <0.0001 | 0.15 | |
| Equivocal, n (%) | |||
| MD | 120 (21.6) | 33 (6.2) | <0.0001 |
| MS | 161 (29.0) | 79 (14.8) | <0.0001 |
| p values | 0.0051 | <0.0001 | |
| Uncertain, n (%) | |||
| MD | 6 (1.1) | 1 (0.2) | 0.1244 |
| MS | 64 (11.5) | 12 (2.3) | <0.0001 |
| p values | <0.0001 | 0.0032 | |
| Not Rateable, n (%) | |||
| MD | 76 (13.7) | 13 (2.4) | <0.0001 |
| MS | 163 (29.4) | 13 (2.4) | <0.0001 |
| p values | <0.0001 | 0.99 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Freesmeyer, M.; Winkens, T.; Weissenrieder, L.; Kühnel, C.; Gühne, F.; Schenke, S.; Drescher, R.; Seifert, P. Fusion iENA Scholar Study: Sensor-Navigated I-124-PET/US Fusion Imaging versus Conventional Diagnostics for Retrospective Functional Assessment of Thyroid Nodules by Medical Students. Sensors 2020, 20, 3409. https://doi.org/10.3390/s20123409
Freesmeyer M, Winkens T, Weissenrieder L, Kühnel C, Gühne F, Schenke S, Drescher R, Seifert P. Fusion iENA Scholar Study: Sensor-Navigated I-124-PET/US Fusion Imaging versus Conventional Diagnostics for Retrospective Functional Assessment of Thyroid Nodules by Medical Students. Sensors. 2020; 20(12):3409. https://doi.org/10.3390/s20123409
Chicago/Turabian StyleFreesmeyer, Martin, Thomas Winkens, Luis Weissenrieder, Christian Kühnel, Falk Gühne, Simone Schenke, Robert Drescher, and Philipp Seifert. 2020. "Fusion iENA Scholar Study: Sensor-Navigated I-124-PET/US Fusion Imaging versus Conventional Diagnostics for Retrospective Functional Assessment of Thyroid Nodules by Medical Students" Sensors 20, no. 12: 3409. https://doi.org/10.3390/s20123409
APA StyleFreesmeyer, M., Winkens, T., Weissenrieder, L., Kühnel, C., Gühne, F., Schenke, S., Drescher, R., & Seifert, P. (2020). Fusion iENA Scholar Study: Sensor-Navigated I-124-PET/US Fusion Imaging versus Conventional Diagnostics for Retrospective Functional Assessment of Thyroid Nodules by Medical Students. Sensors, 20(12), 3409. https://doi.org/10.3390/s20123409