Smoothness of Gait in Healthy and Cognitively Impaired Individuals: A Study on Italian Elderly Using Wearable Inertial Sensor

 ,
, 
Abstract
:1. Introduction
Use of Accelerometers and IMU to Analyze Gait in Elderly with and without Cognitive Impairment
2. Materials and Methods
2.1. Participants
2.2. Neuropsychologic Assessment
- Healthy controls (HC): MMSE score ≥ 24 (n = 34)
- Early cognitive decline (ECD): 18 ≤ MMSE score < 24 (n = 37);
- Advanced cognitive decline (ACD): MMSE score < 18 (n = 19);
2.3. Instrumental Gait Analysis
- spatio-temporal parameters of gait (namely gait speed, stride length, cadence, duration of stance, swing and double support phase expressed as a percentage of the gait cycle). The identification of the gait cycle and the subsequent extraction of such parameters was carried out by means of a peak-detection algorithm, according to the procedure described by Zijlstra [44];
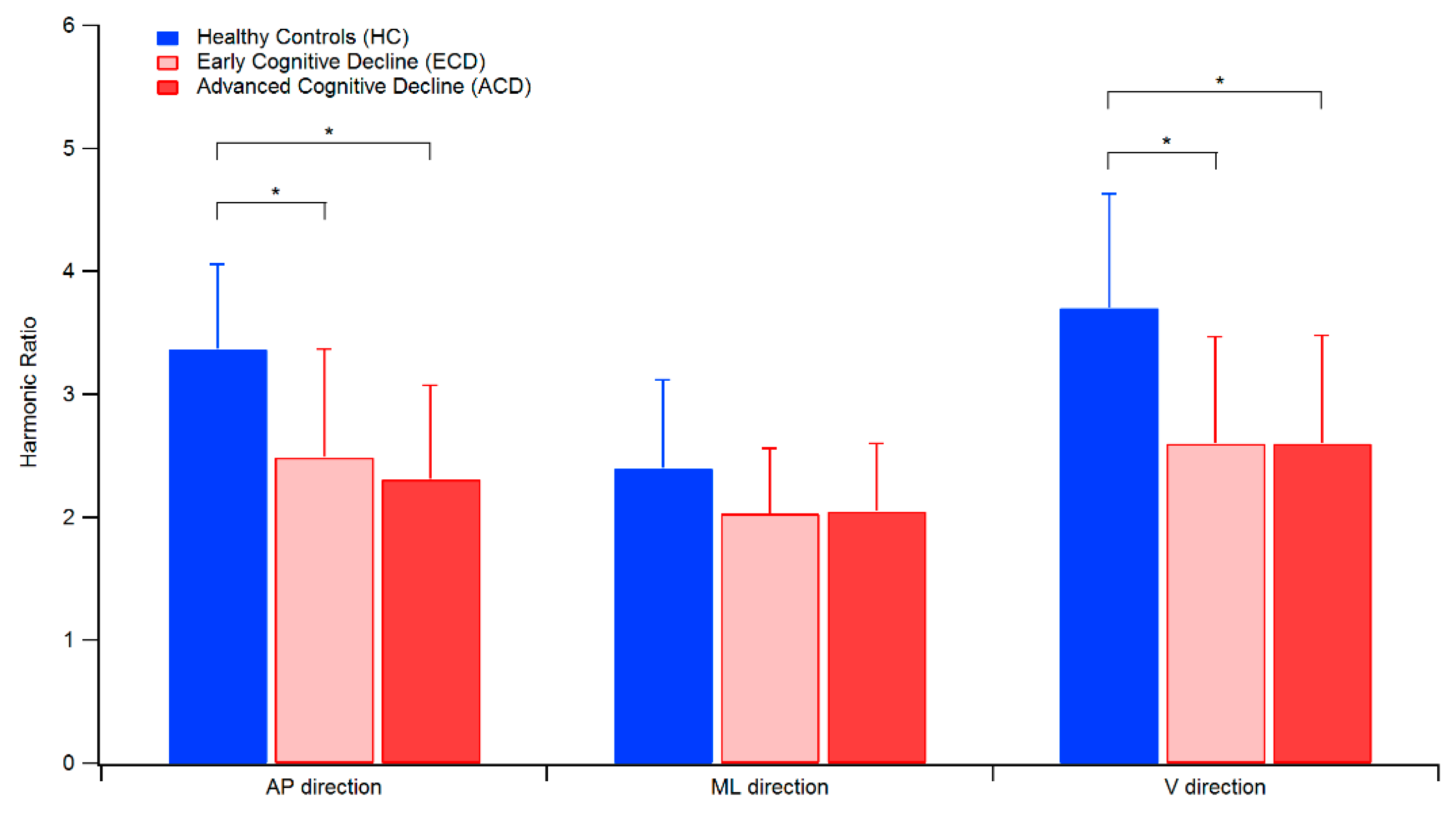
- HRs for AP, ML and V directions.
2.4. Statistical Analysis
3. Results
3.1. Spatio-Temporal Parameters of Gait and Harmonic Ratio
3.2. Correlation between Gait Parameters and Cognitive Impairment
4. Discussion
4.1. General Considerations
4.2. Smoothness of Gait
4.3. Correlation between Cognitive Status and Gait Parameters
4.4. Possible Issues Associated with the Use of IMU to Assess Gait Parameters and HR
4.5. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hardy, S.E.; Perera, S.; Roumani, Y.F.; Chandler, J.M.; Studenski, S.A. Improvement in Usual Gait Speed Predicts Better Survival in Older Adults. J. Am. Geriatr. Soc. 2007, 55, 1727–1734. [Google Scholar] [CrossRef]
- Studenski, S.; Perera, S.; Patel, K.; Rosano, C.; Faulkner, K.; Inzitari, M.; Brach, J.S.; Chandler, J.; Cawthon, P.; Connor, E.B.; et al. Gait Speed and Survival in Older Adults. JAMA 2011, 305, 50–58. [Google Scholar] [CrossRef] [Green Version]
- Sargent-Cox, K.; Anstey, K.J.; Luszcz, M.A. The relationship between change in self-perceptions of aging and physical functioning in older adults. Psychol. Aging 2012, 27, 750–760. [Google Scholar] [CrossRef] [PubMed]
- Rosso, A.; Taylor, J.A.; Tabb, L.P.; Michael, Y.L. Mobility, disability, and social engagement in older adults. J. Aging Heal. 2013, 25, 617–637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, J.C.; Bryan, S.; Best, J.R.; Li, L.C.; Hsu, C.L.; Gomez, C.; Vertes, K.A.; Liu-Ambrose, T. Mobility predicts change in older adults’ health-related quality of life: Evidence from a Vancouver falls prevention prospective cohort study. Heal. Qual. Life Outcomes 2015, 13, 101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rantakokko, M.; Mänty, M.; Rantanen, T. Mobility Decline in Old Age. Exerc. Sport Sci. Rev. 2013, 41, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Iosa, M.; Fusco, A.; Morone, G.; Paolucci, S. Development and Decline of Upright Gait Stability. Front. Aging Neurosci. 2014, 6, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ebeling, P.R.; Cicuttini, F.; Scott, D.; Jones, G. Promoting mobility and healthy aging in men: A narrative review. Osteoporos. Int. 2019, 30, 1911–1922. [Google Scholar] [CrossRef]
- Prince, F.; Corriveau, H.; Hébert, R.; Winter, D.A. Gait in the elderly. Gait Posture 1997, 5, 128–135. [Google Scholar] [CrossRef]
- Giladi, N.; Herman, T.; Reider-Groswasser, I.I.; Gurevich, T.; Hausdorff, J.M. Clinical characteristics of elderly patients with a cautious gait of unknown origin. J. Neurol. 2005, 252, 300–306. [Google Scholar] [CrossRef]
- Cohen, J.A.; Verghese, J.; Zwerling, J.L. Cognition and gait in older people. Maturitas 2016, 93, 73–77. [Google Scholar] [CrossRef] [PubMed]
- Beauchet, O.; Annweiler, C.; Montero-Odasso, M.; Fantino, B.; Herrmann, F.; Allali, G. Gait control: A specific subdomain of executive function? J. Neuroeng. Rehabil. 2012, 9, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montero-Odasso, M.; Verghese, J.; Beauchet, O.; Hausdorff, J.M. Gait and cognition: A complementary approach to understanding brain function and the risk of falling. J. Am. Geriatr. Soc. 2012, 60, 2127–2136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amboni, M.; Barone, P.; Hausdorff, J.M. Cognitive contributions to gait and falls: Evidence and implications. Mov. Disord. 2013, 28, 1520–1533. [Google Scholar] [CrossRef]
- Iosa, M.; Picerno, P.; Paolucci, S.; Morone, G. Wearable Inertial Sensors for Human Movement Analysis. Expert Rev. Med. Devices 2016, 13, 641–659. [Google Scholar] [CrossRef]
- Culhane, K.M.; O’Connor, M.; Lyons, D.; Lyons, G.M. Accelerometers in rehabilitation medicine for older adults. Age Ageing 2005, 34, 556–560. [Google Scholar] [CrossRef] [Green Version]
- Maquet, D.; Lekeu, F.; Warzee, E.; Gillain, S.; Wojtasik, V.; Salmon, E.; Petermans, J.; Croisier, J.L. Gait analysis in elderly adult patients with mild cognitive impairment and patients with mild Alzheimer’s disease: Simple versus dual task: A preliminary report. Clin. Physiol. Funct. Imaging 2010, 30, 51–56. [Google Scholar] [CrossRef]
- Choi, J.-S.; Oh, H.-S.; Kang, D.-W.; Mun, K.-R.; Choi, M.-H.; Lee, S.-J.; Yang, J.-W.; Chung, S.-C.; Mun, S.-W.; Tack, G.-R. Comparison of gait and cognitive function among the elderly with Alzheimer’s disease, Mild Cognitive Impairment and Healthy. Int. J. Precis. Eng. Manuf. 2011, 12, 169–173. [Google Scholar] [CrossRef]
- Mirelman, A.; Weiss, A.; Buchman, A.S.; Bennett, D.A.; Giladi, N.; Hausdorff, J.M. Association between performance on Timed Up and Go subtasks and mild cognitive impairment: Further insights into the links between cognitive and motor function. J. Am. Geriatr. Soc. 2014, 62, 673–678. [Google Scholar] [CrossRef]
- Grimm, B.; Bolink, S. Evaluating physical function and activity in the elderly patient using wearable motion sensors. EFORT Open Rev. 2016, 1, 112–120. [Google Scholar] [CrossRef]
- Mc Ardle, R.; Del Din, S.; Galna, B.; Thomas, A.; Rochester, L. Differentiating dementia disease subtypes with gait analysis: Feasibility of wearable sensors? Gait Posture 2020, 76, 372–376. [Google Scholar] [CrossRef] [PubMed]
- Brognara, L.; Palumbo, P.; Grimm, B.; Palmerini, L. Assessing Gait in Parkinson’s Disease Using Wearable Motion Sensors: A Systematic Review. Diseases 2019, 7, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jarchi, D.; Pope, J.; Lee, T.K.M.; Tamjidi, L.; Mirzaei, A.; Sanei, S. A Review on Accelerometry-Based Gait Analysis and Emerging Clinical Applications. IEEE Rev. Biomed. Eng. 2018, 11, 177–194. [Google Scholar] [CrossRef] [PubMed]
- Smidt, G.; Deusinger, R.; Arora, J.; Albright, J. An automated accelerometry system for gait analysis. J. Biomech. 1977, 10, 367–375. [Google Scholar] [CrossRef]
- Bellanca, J.; Lowry, K.A.; VanSwearingen, J.; Brach, J.S.; Redfern, M. Harmonic ratios: A quantification of step to step symmetry. J. Biomech. 2013, 46, 828–831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lowry, K.A.; Carrel, A.J.; Kerr, J.P.; Smiley-Oyen, A.L. Walking stability using harmonic ratios in Parkinson’s disease. Mov. Disord. 2009, 24, 261–267. [Google Scholar] [CrossRef]
- Brach, J.S.; McGurl, D.; Wert, D.; VanSwearingen, J.M.; Perera, S.; Cham, R.; Studenski, S. Validation of a Measure of Smoothness of Walking. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2010, 66, 136–141. [Google Scholar] [CrossRef]
- Iosa, M.; Bini, F.; Marinozzi, F.; Fusco, A.; Morone, G.; Koch, G.; Cinnera, A.M.; Bonnì, S.; Paolucci, S. Stability and Harmony of Gait in Patients with Subacute Stroke. J. Med. Boil. Eng. 2016, 36, 635–643. [Google Scholar] [CrossRef]
- Pau, M.; Mandaresu, S.; Pilloni, G.; Porta, M.; Coghe, G.; Marrosu, M.G.; Cocco, E. Smoothness of gait detects early alterations of walking in persons with multiple sclerosis without disability. Gait Posture 2017, 58, 307–309. [Google Scholar] [CrossRef]
- Yack, H.J.; Berger, R.C. Dynamic Stability in the Elderly: Identifying a Possible Measure. J. Gerontol. 1993, 48. [Google Scholar] [CrossRef]
- Menz, H.; Lord, S.R.; Fitzpatrick, R.C. Acceleration patterns of the head and pelvis when walking on level and irregular surfaces. Gait Posture 2003, 18, 35–46. [Google Scholar] [CrossRef]
- Byun, S.; Han, J.W.; Kim, T.H.; Kim, K.; Kim, T.H.; Park, J.Y.; Suh, S.W.; Seo, J.Y.; So, Y.; Lee, K.H.; et al. Gait Variability Can Predict the Risk of Cognitive Decline in Cognitively Normal Older People. Dement. Geriatr. Cogn. Disord. 2018, 45, 251–261. [Google Scholar] [CrossRef] [PubMed]
- Lamoth, C.J.C.; Van Deudekom, F.J.; Van Campen, J.P.; Appels, B.A.; De Vries, O.J.; Pijnappels, M. Gait stability and variability measures show effects of impaired cognition and dual tasking in frail people. J. Neuroeng. Rehabil. 2011, 8, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doi, T.; Shimada, H.; Makizako, H.; Tsutsumimoto, K.; Hotta, R.; Nakakubo, S.; Suzuki, T. Effects of white matter lesions on trunk stability during dual-task walking among older adults with mild cognitive impairment. AGE 2015, 37, 120. [Google Scholar] [CrossRef] [Green Version]
- Ijmker, T.; Lamoth, C.J.C. Gait and cognition: The relationship between gait stability and variability with executive function in persons with and without dementia. Gait Posture 2012, 35, 126–130. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. Mini-mental state. J. Psychiatry Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Magni, E.; Binetti, G.; Bianchetti, A.; Rozzini, R.; Trabucchi, M. Mini-Mental State Examination: A normative study in Italian elderly population. Eur. J. Neurol. 1996, 3, 198–202. [Google Scholar] [CrossRef]
- Mioshi, E.; Dawson, K.; Mitchell, J.; Arnold, R.; Hodges, J.R. The Addenbrooke’s Cognitive Examination Revised (ACE-R): A brief cognitive test battery for dementia screening. Int. J. Geriatr. Psychiatry 2006, 21, 1078–1085. [Google Scholar] [CrossRef]
- Pigliautile, M.; Ricci, M.; Mioshi, E.; Ercolani, S.; Mangialasche, F.; Monastero, R.; Croce, M.; Federici, S.; Mecocci, P. Validation Study of the Italian Addenbrooke’s Cognitive Examination Revised in a Young-Old and Old-Old Population. Dement. Geriatr. Cogn. Disord. 2011, 32, 301–307. [Google Scholar] [CrossRef]
- Isella, V.; Villa, M.; Frattola, L.; Appollonio, I. Screening cognitive decline in dementia: Preliminary data on the Italian version of the IQCODE. Neurol. Sci. 2002, 23, s79–s80. [Google Scholar] [CrossRef]
- Viscione, I.; D’Elia, F.; Vastola, R.; Sibilio, M. The Correlation between Technologies and Rating Scales in Gait Analysis. J. Sports Sci. 2016, 4, 119–123. [Google Scholar] [CrossRef]
- Pau, M.; Porta, M.; Pilloni, G.; Corona, F.; Fastame, M.C.; Hitchcott, P.K.; Penna, M.L.F. Texting While Walking Induces Gait Pattern Alterations in Healthy Older Adults. Proc. Hum. Factors Ergon. Soc. Annu. Meet. 2018, 62, 1908–1912. [Google Scholar] [CrossRef] [Green Version]
- Pasciuto, I.; Bergamini, E.; Iosa, M.; Vannozzi, G.; Cappozzo, A. Overcoming the limitations of the Harmonic Ratio for the reliable assessment of gait symmetry. J. Biomech. 2017, 53, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Zijlstra, W. Assessment of spatio-temporal parameters during unconstrained walking. Graefe’s Arch. Clin. Exp. Ophthalmol. 2004, 92, 39–44. [Google Scholar] [CrossRef]
- Menz, H.; Lord, S.R.; Fitzpatrick, R.C. Acceleration patterns of the head and pelvis when walking are associated with risk of falling in community-dwelling older people. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2003, 58, M446–M452. [Google Scholar] [CrossRef]
- Lowry, K.A.; Lokenvitz, N.; Smiley-Oyen, A. Age- and speed-related differences in harmonic ratios during walking. Gait Posture 2012, 35, 272–276. [Google Scholar] [CrossRef]
- Lazzarini, B.S.R.; Kataras, T.J. Treadmill walking is not equivalent to overground walking for the study of walking smoothness and rhythmicity in older adults. Gait Posture 2016, 46, 42–46. [Google Scholar] [CrossRef]
- Asai, T.; Misu, S.; Sawa, R.; Doi, T.; Yamada, M. The association between fear of falling and smoothness of lower trunk oscillation in gait varies according to gait speed in community-dwelling older adults. J. Neuroeng. Rehabil. 2017, 14, 5. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis. Curr. Dir. Psychol. Sci. 1992, 1, 98–101. [Google Scholar] [CrossRef]
- Peel, N.M.; Alapatt, L.J.; Jones, L.V.; Hubbard, R.E. The Association between Gait Speed and Cognitive Status in Community-Dwelling Older People: A Systematic Review and Meta-analysis. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2018, 74, 943–948. [Google Scholar] [CrossRef]
- Salzman, B.E. Gait and balance disorders in older adults. Am. Fam. Physician 2010, 82, 61–68. [Google Scholar] [PubMed]
- Allan, L.M.; Ballard, C.; Burn, D.; Kenny, R.A. Prevalence and Severity of Gait Disorders in Alzheimer’s and Non-Alzheimer’s Dementias. J. Am. Geriatr. Soc. 2005, 53, 1681–1687. [Google Scholar] [CrossRef] [PubMed]
- Beauchet, O.; Allali, G.; Berrut, G.; Hommet, C.; Dubost, V.; Assal, F. Gait analysis in demented subjects: Interests and perspectives. Neuropsychiatr. Dis. Treat. 2008, 4, 155–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eggermont, L.H.; Gavett, B.E.; Volkers, K.M.; Blankevoort, C.G.; Scherder, E.J.; Jefferson, A.L.; Steinberg, E.; Nair, A.; Green, R.C.; Stern, R. Lower-Extremity Function in Cognitively Healthy Aging, Mild Cognitive Impairment, and Alzheimer’s Disease. Arch. Phys. Med. Rehabil. 2010, 91, 584–588. [Google Scholar] [CrossRef] [Green Version]
- Shaw, F.E.; Bond, J.; Richardson, D.A.; Dawson, P.; Steen, I.N.; McKeith, I.G.; Kenny, R.A. Multifactorial intervention after a fall in older people with cognitive impairment and dementia presenting to the accident and emergency department: Randomised controlled trial. BMJ 2003, 326, 73. [Google Scholar] [CrossRef] [Green Version]
- Zhang, W.; Low, L.-F.; Schwenk, M.; Mills, N.; Gwynn, J.D.; Clemson, L. Review of Gait, Cognition, and Fall Risks with Implications for Fall Prevention in Older Adults with Dementia. Dement. Geriatr. Cogn. Disord. 2019, 48, 17–29. [Google Scholar] [CrossRef]
- Kikkert, L.H.J.; Vuillerme, N.; Van Campen, J.P.; Hortobágyi, T.; Lamoth, C.J.C. Walking ability to predict future cognitive decline in old adults: A scoping review. Ageing Res. Rev. 2016, 27, 1–14. [Google Scholar] [CrossRef]
- Morris, R.; Lord, S.; Bunce, J.; Burn, D.; Rochester, L. Gait and cognition: Mapping the global and discrete relationships in ageing and neurodegenerative disease. Neurosci. Biobehav. Rev. 2016, 64, 326–345. [Google Scholar] [CrossRef]
- Demnitz, N.; Esser, P.; Dawes, H.; Valkanova, V.; Johansen-Berg, H.; Ebmeier, K.P.; Sexton, C. A systematic review and meta-analysis of cross-sectional studies examining the relationship between mobility and cognition in healthy older adults. Gait Posture 2016, 50, 164–174. [Google Scholar] [CrossRef] [Green Version]
- Grande, G.; Triolo, F.; Nuara, A.; Welmer, A.-K.; Fratiglioni, L.; Vetrano, D.L. Measuring gait speed to better identify prodromal dementia. Exp. Gerontol. 2019, 124, 110625. [Google Scholar] [CrossRef] [PubMed]
- Zaninotto, P.; Sacker, A.; Head, J. Relationship between Wealth and Age Trajectories of Walking Speed among Older Adults: Evidence from the English Longitudinal Study of Ageing. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2013, 68, 1525–1531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Busch, T.; Duarte, Y.A.D.O.; Nunes, D.P.; Lebrão, M.L.; Naslavsky, M.S.; Rodrigues, A.D.S.; Amaro, E. Factors associated with lower gait speed among the elderly living in a developing country: A cross-sectional population-based study. BMC Geriatr. 2015, 15, 35. [Google Scholar] [CrossRef] [PubMed]
- Weber, D. Differences in physical aging measured by walking speed: Evidence from the English Longitudinal Study of Ageing. BMC Geriatr. 2016, 16, 2326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cimolin, V.; Cau, N.; Sartorio, A.; Capodaglio, P.; Galli, M.; Tringali, G.; Leban, B.; Porta, M.; Pau, M. Symmetry of Gait in Underweight, Normal and Overweight Children and Adolescents. Sensors 2019, 19, 2054. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Healthy Controls (HC) | Early Cognitive Decline (ECD) | Advanced Cognitive Decline (ACD) | |
|---|---|---|---|
| Participants # (F, M) | 34 (22 F, 12 M) | 37 (22 F, 15 M) | 19 (12 F, 7 M) |
| Female/Male Ratio | F 65%, M 35% | F 60%, M 40% | F 63%, M 37% |
| Age (years) | 79.1 ± 3.9 | 78.8 ± 5.8 | 78.9 ± 4.6 |
| Body Mass (kg) | 64.1 ± 13.5 | 62.5 ± 12.9 | 62.6 ± 17.1 |
| Height (cm) | 159.9 ± 8.6 | 159.3 ± 8.8 | 158.1 ± 9.7 |
| Mini Mental State Examination (MMSE) | 27.6 ± 1.7 | 22.0 ± 1.5 | 11.8 ± 5.1 |
| Addenbrooke’s Cognitive Examination Revised (ACE-R) | 77.8 ± 11.1 | 55.5 ± 9.7 | 25.0 ± 15.4 |
| Gait Parameter | Healthy Controls (HC) | Early Cognitive Decline (ECD) | Advanced Cognitive Decline (ACD) |
|---|---|---|---|
| Gait speed (m s−1) | 0.92 ± 0.23 | 0.68 ± 0.30 a | 0.63 ± 0.25 a |
| Stride length (m) | 1.03 ± 0.23 | 0.81 ± 0.32 a | 0.73 ± 0.23 a |
| Cadence (steps min−1) | 107.3 ± 8.5 | 100.6 ± 12.6 | 101.7 ± 11.8 |
| Stance phase (% GC) | 61.3 ± 2.0 | 61.9 ± 2.3 | 62.0 ± 1.6 |
| Swing phase (% GC) | 38.8 ± 1.9 | 38.1 ± 2.3 | 37.4 ± 2.8 |
| Double support phase (% GC) | 22.3 ± 2.0 | 23.8 ± 2.3 | 24.0 ± 1.7 |
| Harmonic ratio (HR) anteroposterior (AP) direction * | 3.37 ± 0.69 | 2.49 ± 0.88 a | 2.31 ± 0.76 a |
| HR mediolateral (ML) direction * | 2.40 ± 0.72 | 2.03 ± 0.53 | 2.05 ± 0.55 |
| HR vertical (V) direction * | 3.70 ± 0.93 | 2.60 ± 0.87 a | 2.60 ± 0.88 a |
| Gait Variables | MMSE | ACE-R | |
|---|---|---|---|
| Spatial-temporal parameters | Gait speed | 0.449 †† | 0.430 †† |
| Stride length | 0.446 †† | 0.422 †† | |
| Cadence | 0.199 | 0.191 | |
| Stance phase | −0.156 | −0.143 | |
| Swing phase | 0.192 | 0.182 | |
| Double support phase | −0.153 | −0.149 | |
| Harmonic Ratio | HR AP direction * | 0.323 †† | 0.303 †† |
| HR ML direction * | 0.213 † | 0.251† | |
| HR V direction * | 0.259 † | 0.207 † | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pau, M.; Mulas, I.; Putzu, V.; Asoni, G.; Viale, D.; Mameli, I.; Leban, B.; Allali, G. Smoothness of Gait in Healthy and Cognitively Impaired Individuals: A Study on Italian Elderly Using Wearable Inertial Sensor. Sensors 2020, 20, 3577. https://doi.org/10.3390/s20123577
Pau M, Mulas I, Putzu V, Asoni G, Viale D, Mameli I, Leban B, Allali G. Smoothness of Gait in Healthy and Cognitively Impaired Individuals: A Study on Italian Elderly Using Wearable Inertial Sensor. Sensors. 2020; 20(12):3577. https://doi.org/10.3390/s20123577
Chicago/Turabian StylePau, Massimiliano, Ilaria Mulas, Valeria Putzu, Gesuina Asoni, Daniela Viale, Irene Mameli, Bruno Leban, and Gilles Allali. 2020. "Smoothness of Gait in Healthy and Cognitively Impaired Individuals: A Study on Italian Elderly Using Wearable Inertial Sensor" Sensors 20, no. 12: 3577. https://doi.org/10.3390/s20123577
APA StylePau, M., Mulas, I., Putzu, V., Asoni, G., Viale, D., Mameli, I., Leban, B., & Allali, G. (2020). Smoothness of Gait in Healthy and Cognitively Impaired Individuals: A Study on Italian Elderly Using Wearable Inertial Sensor. Sensors, 20(12), 3577. https://doi.org/10.3390/s20123577