Adaptive Separation of Respiratory and Heartbeat Signals among Multiple People Based on Empirical Wavelet Transform Using UWB Radar


Abstract
:1. Introduction
2. Signal Model and Proposed Algorithm
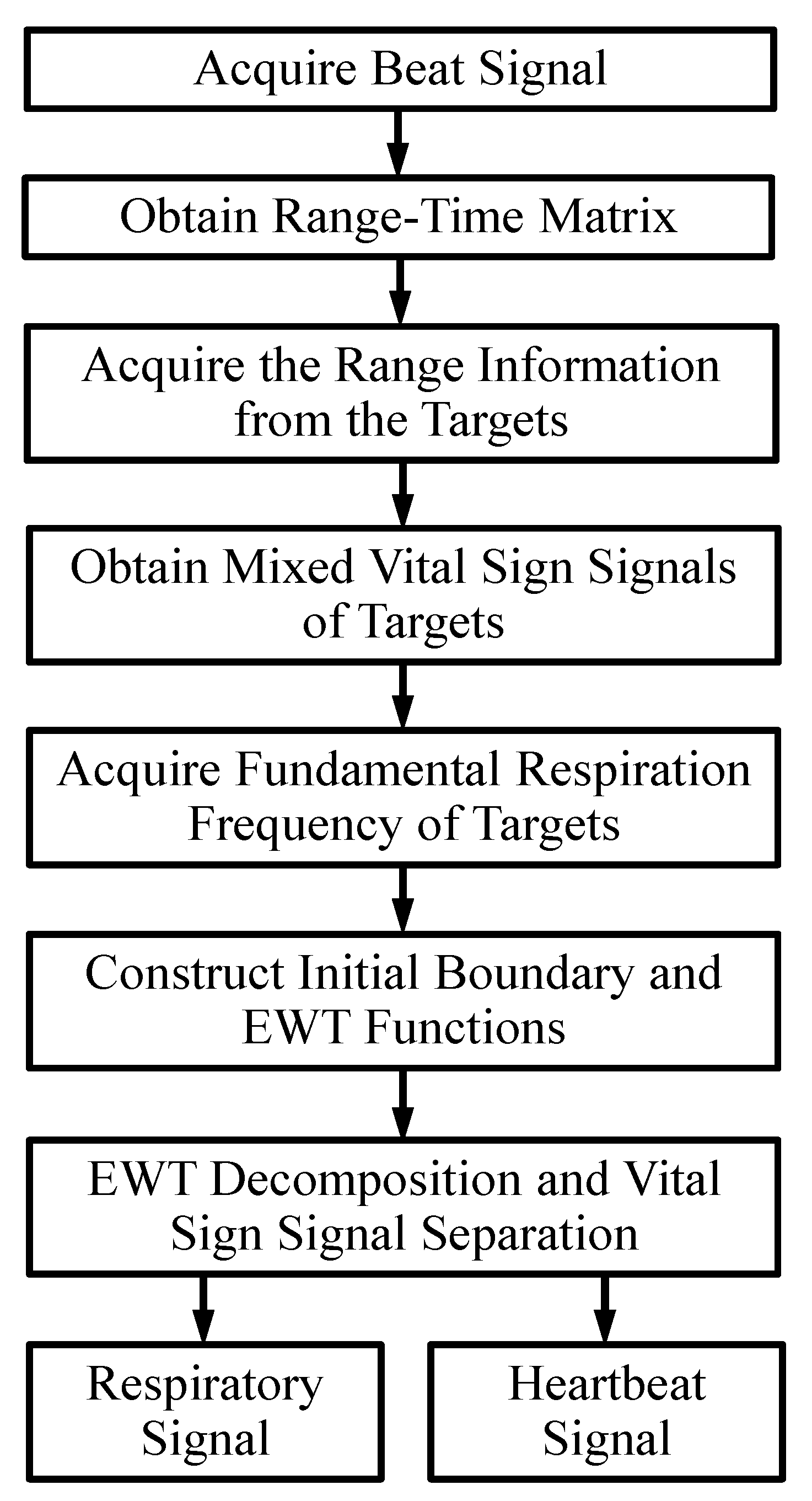
2.1. Block Diagram of Signal Processing
2.1.1. Acquire the Beat Signal
2.1.2. Obtain the Range-Time Matrix
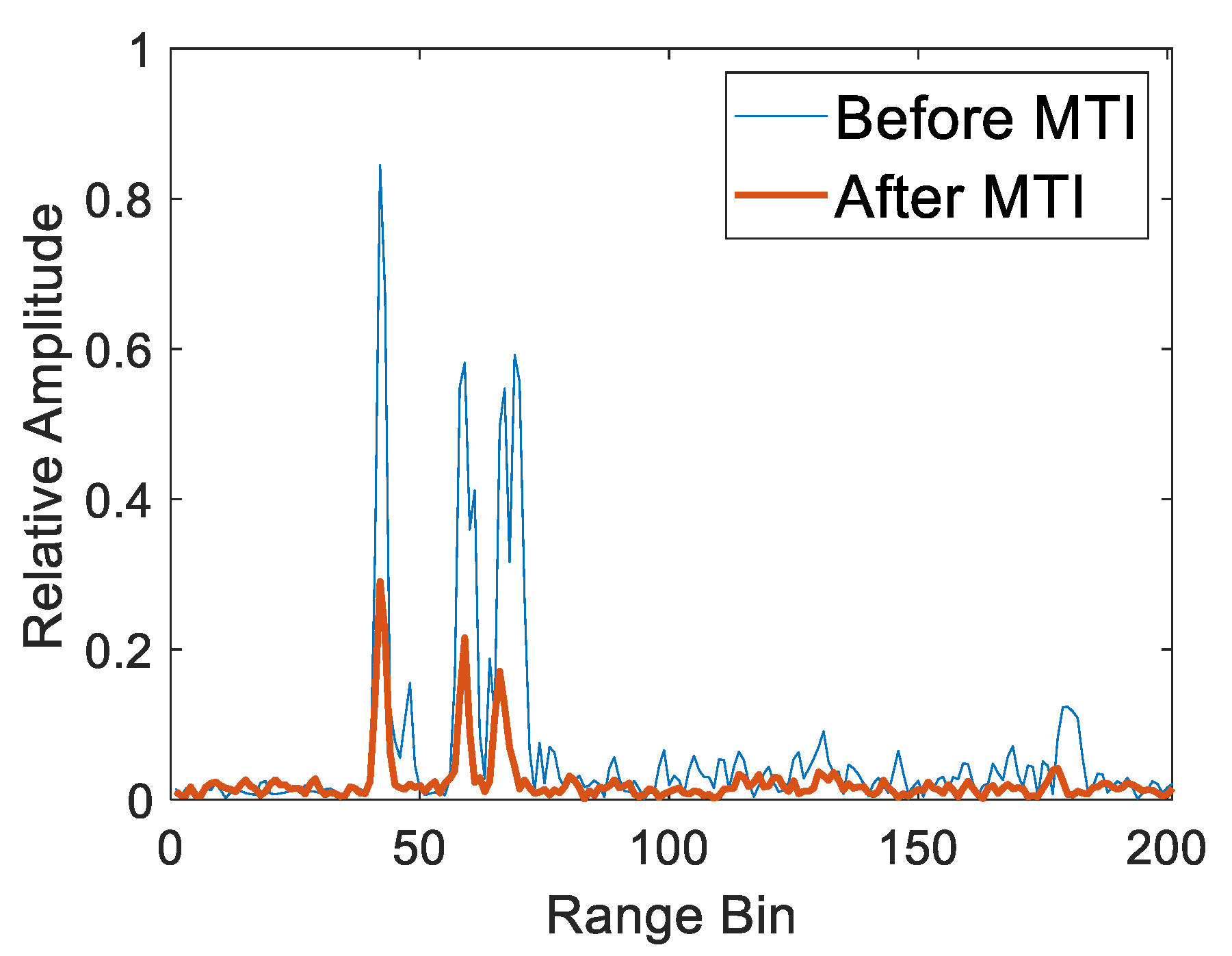
2.1.3. Acquire the Range Information from the Targets
2.1.4. Obtain Mixed Vital Sign Signals of Targets
2.1.5. Acquire the Fundamental Respiration Frequency of Targets
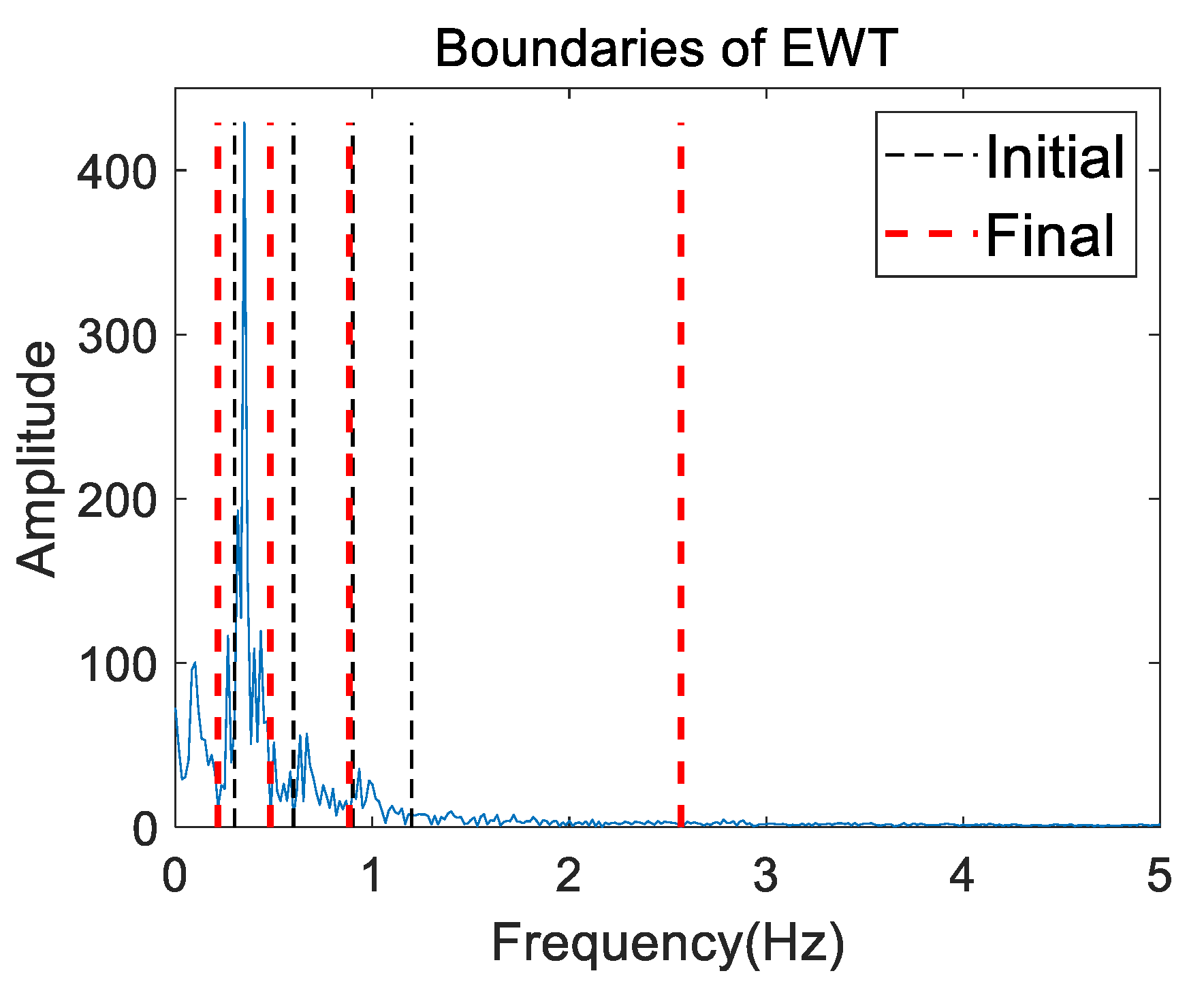
2.1.6. Construct Initial Boundary and Empirical Wavelet Functions
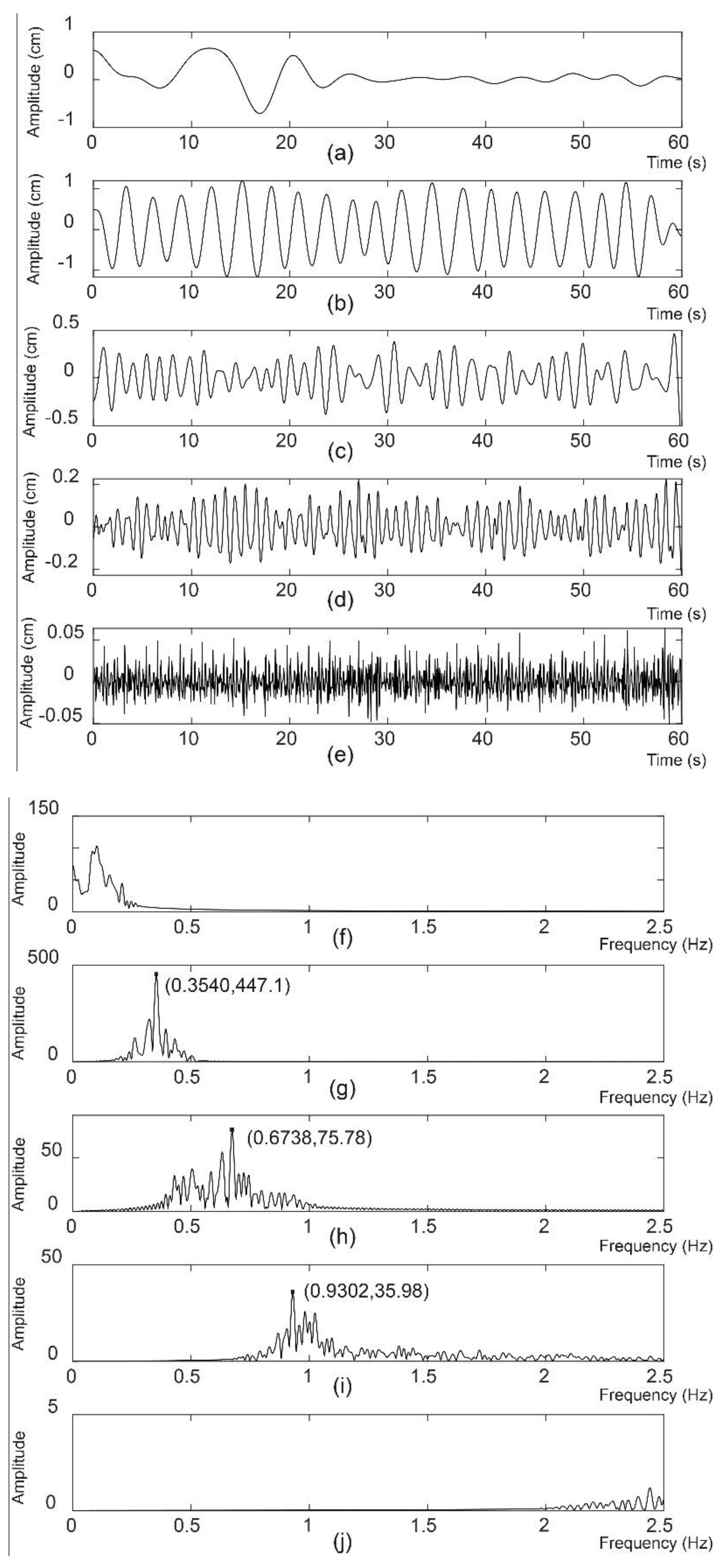
2.1.7. EWT Decomposition and Vital Sign Signal Separation
2.2. Signal Model of the SFCW-UWB Radar
2.3. Theory of the Proposed Algorithm Based on EWT
3. Experiment
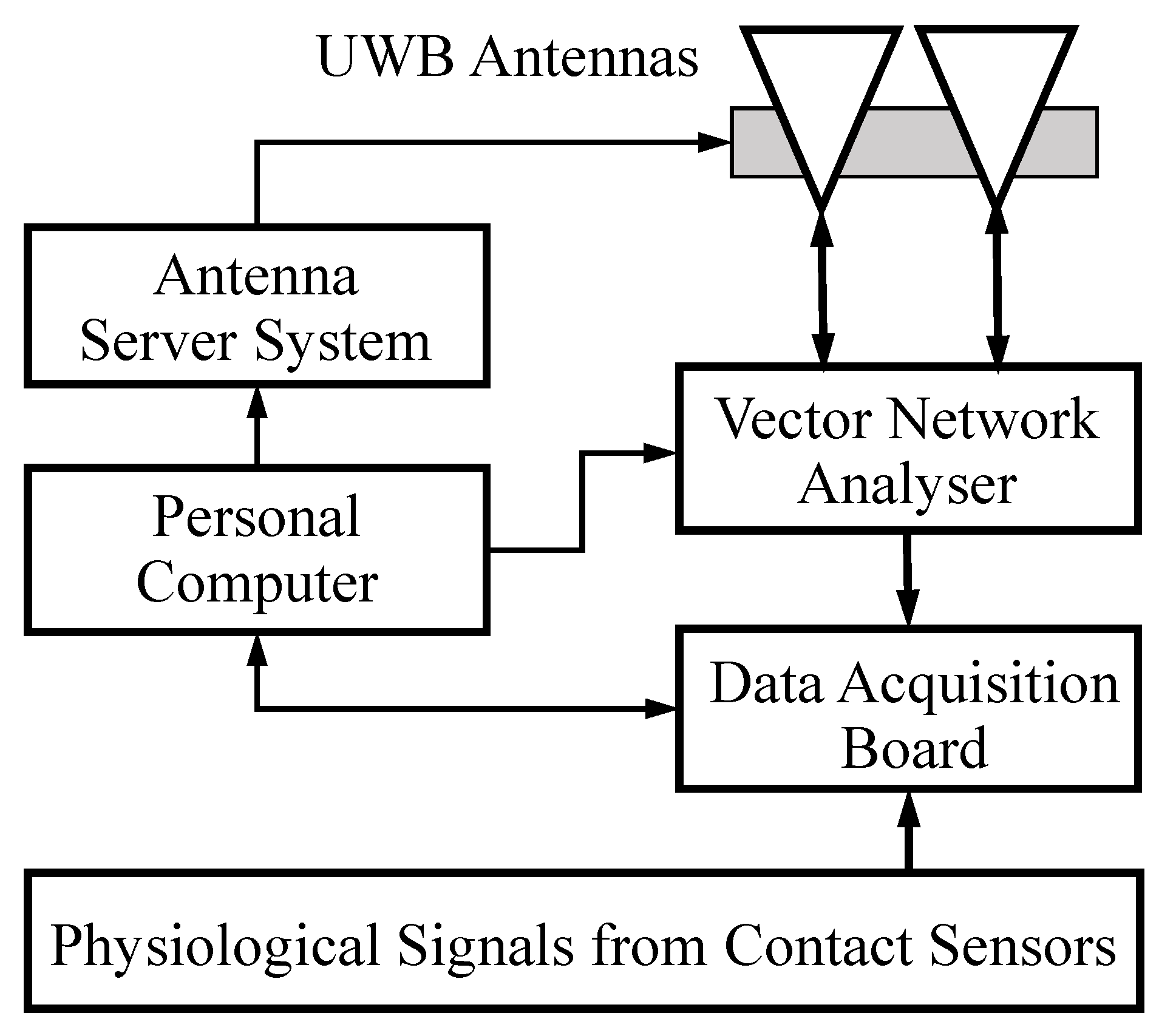
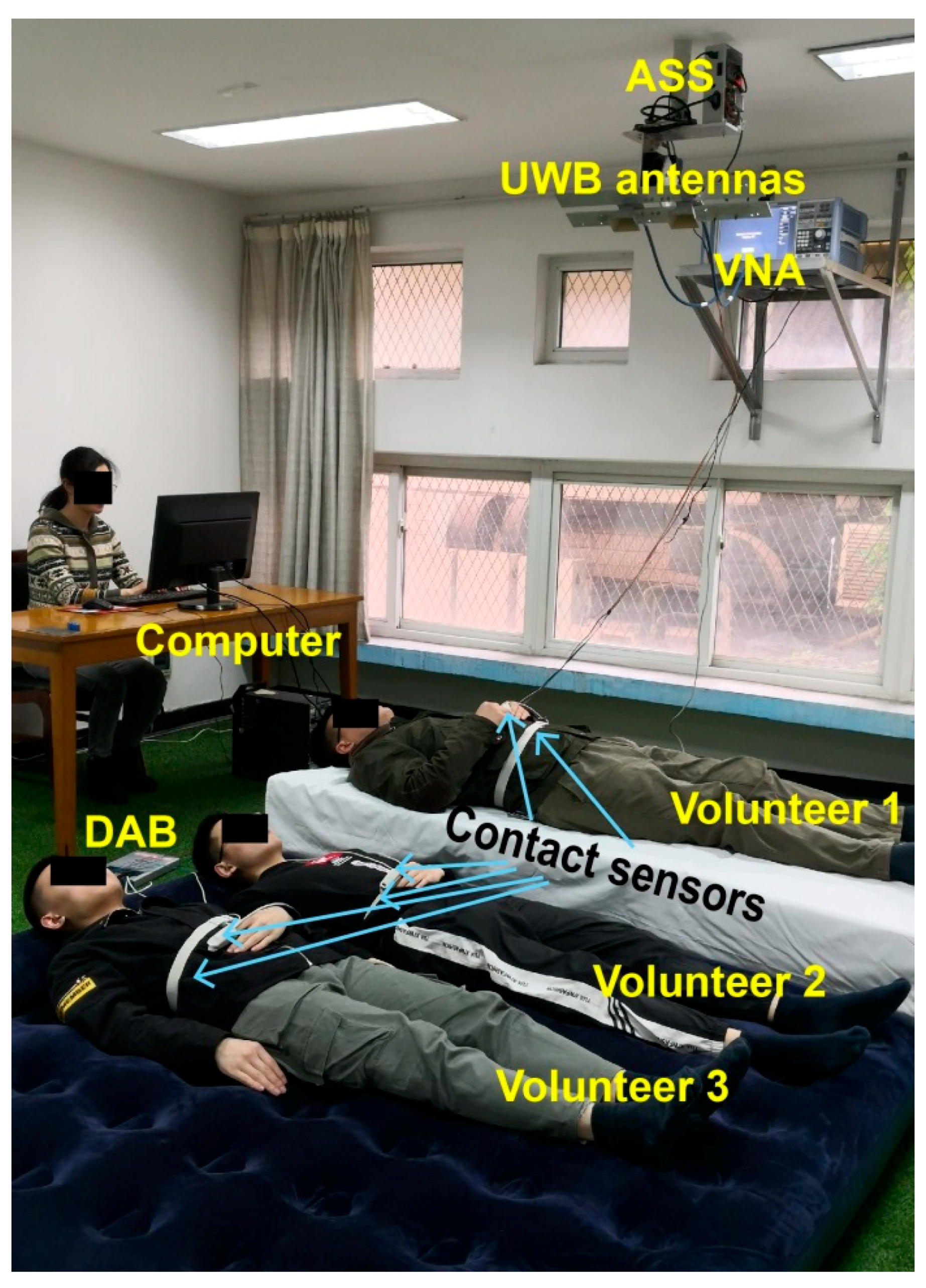
3.1. UWB Radar Platform
3.2. Participants
3.3. Data Acquisition and Analysis
4. Results and Discussion
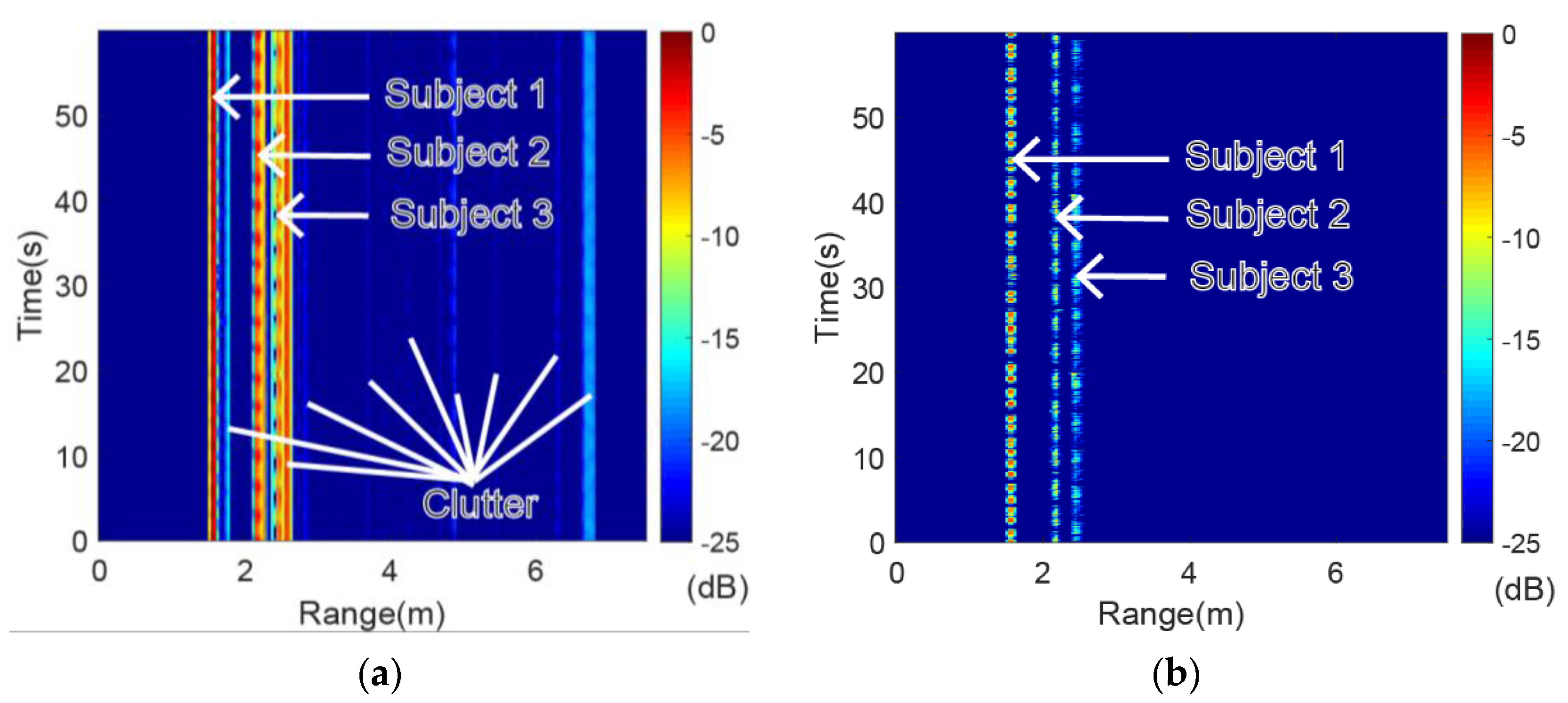
4.1. Range-Time Spectrogram of Volunteers
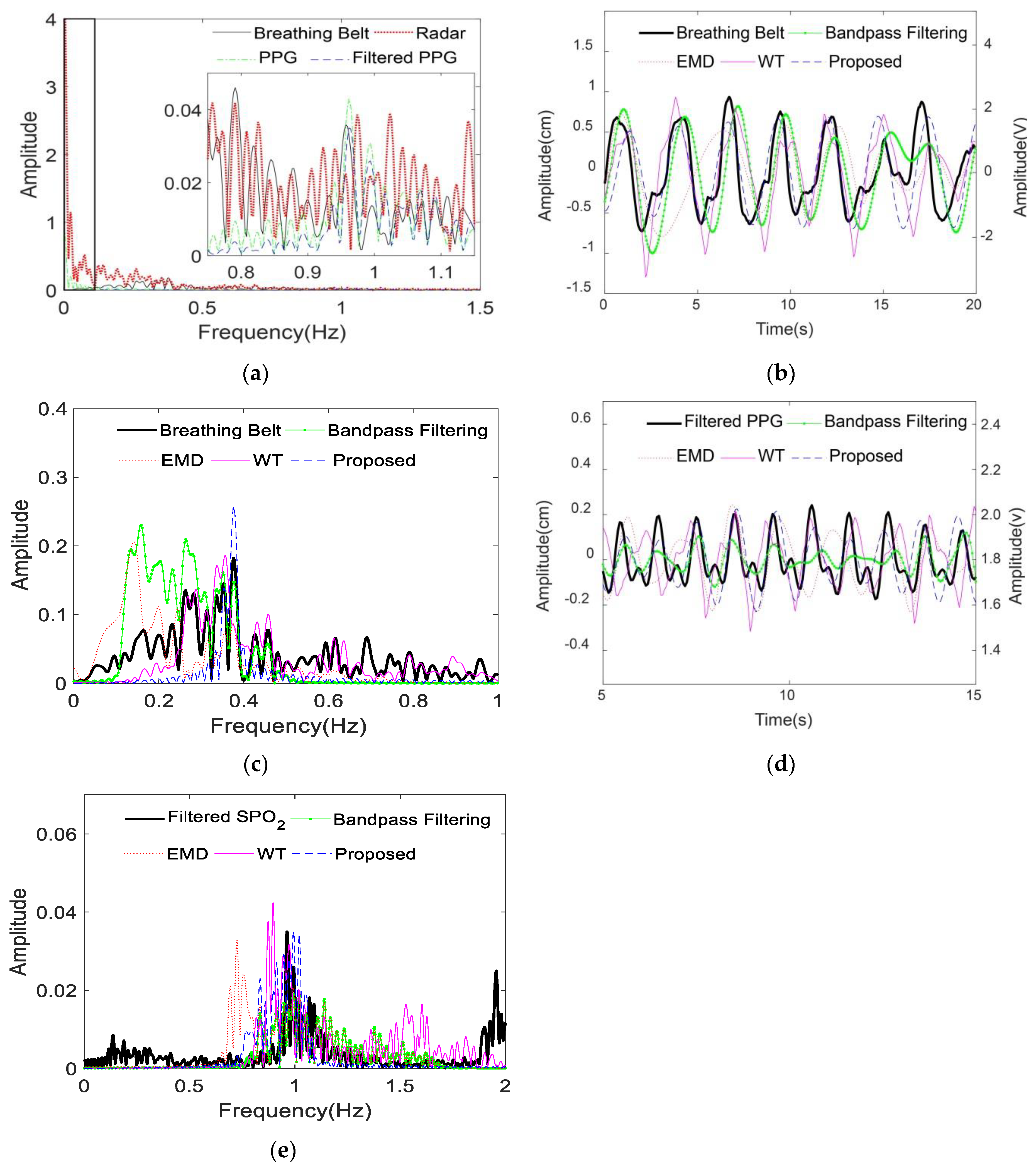
4.2. EWT Composition
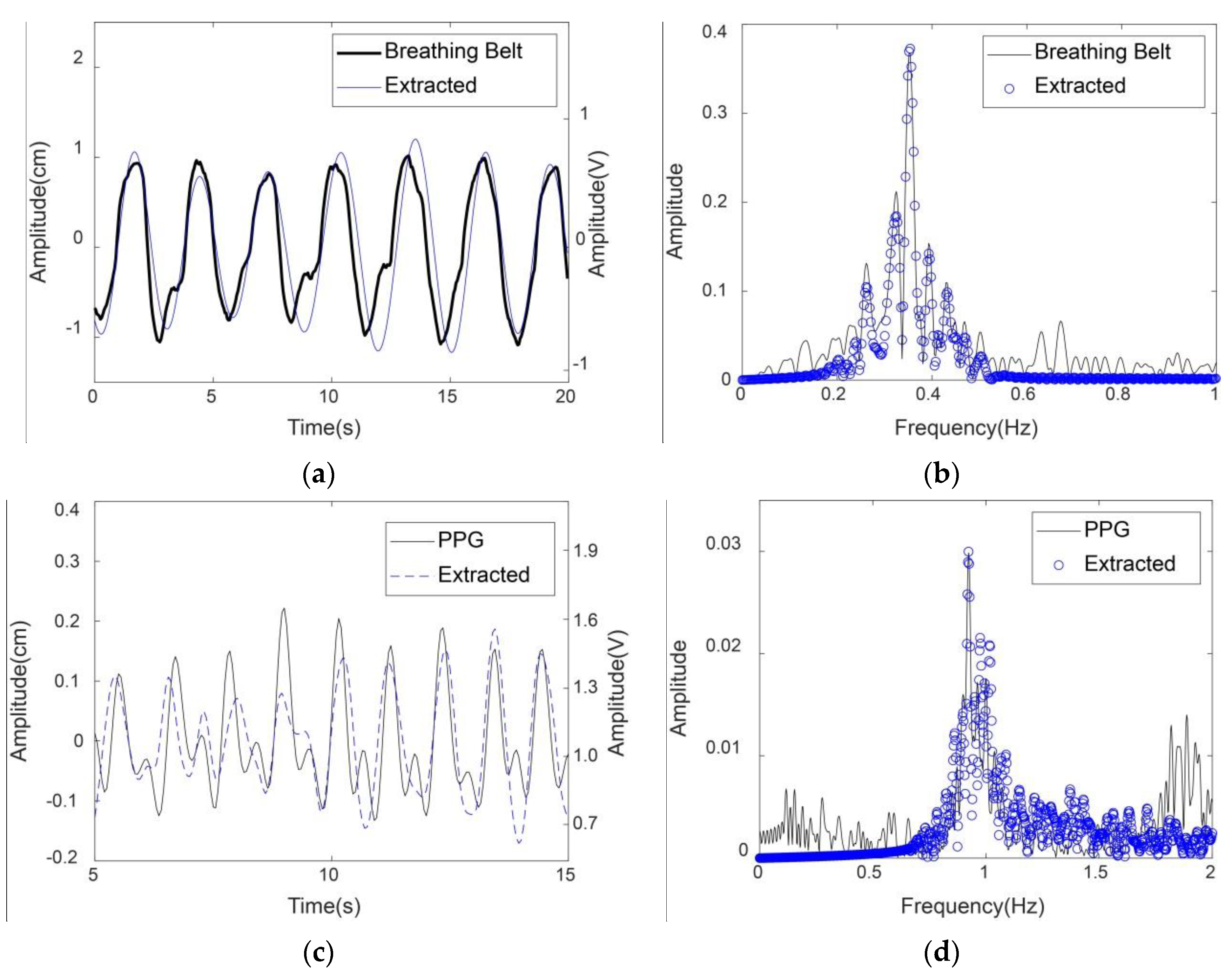
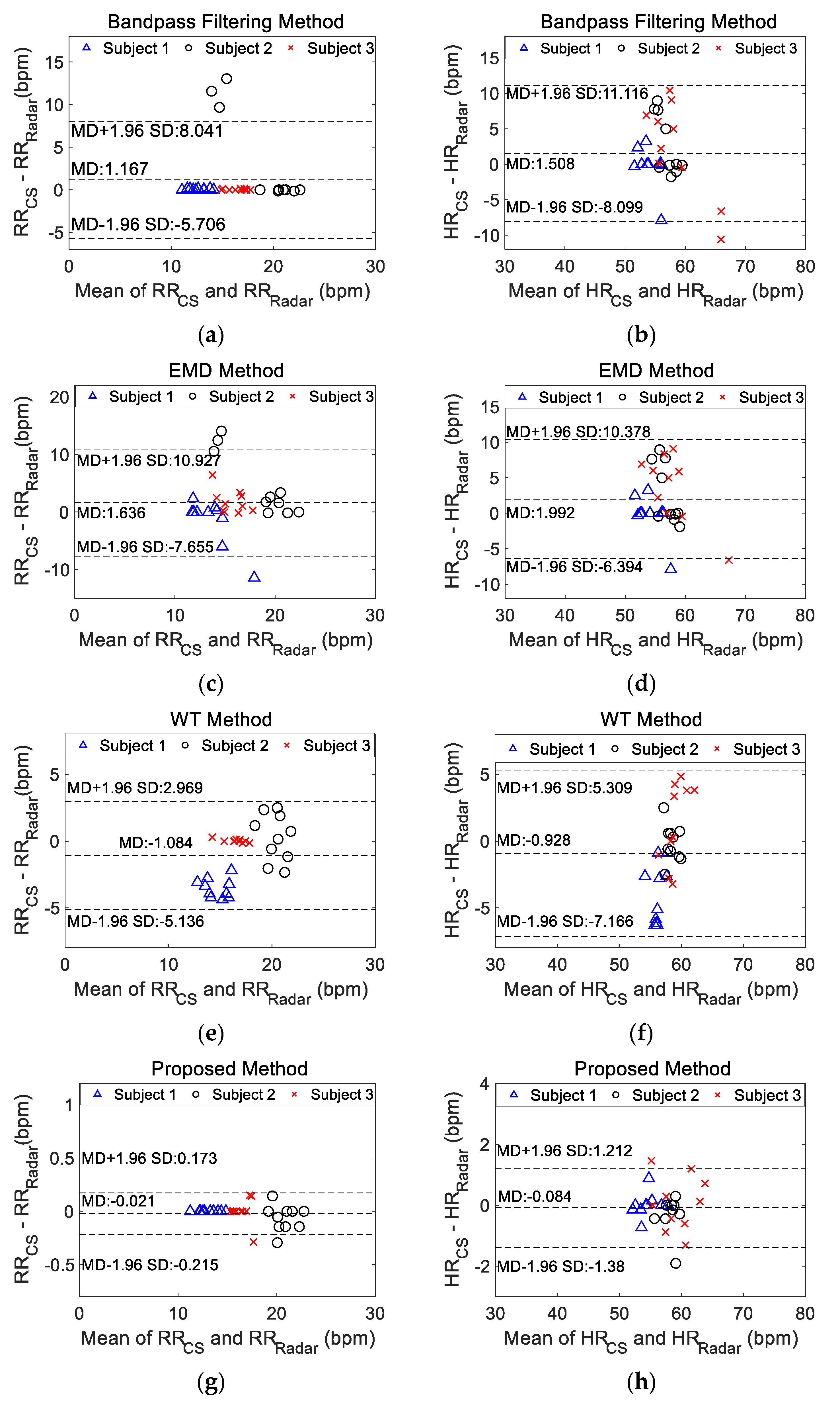
4.3. Comparison of Different Methods
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Min, S.D.; Kim, J.K.; Shin, H.S.; Yun, Y.H.; Lee, C.K.; Lee, M. Noncontact respiration rate measurement system using an ultrasonic proximity sensor. IEEE Sens. J. 2010, 10, 1732–1739. [Google Scholar] [CrossRef]
- Ren, L.; Kong, L.; Foroughian, F.; Wang, H.; Theilmann, P.; Fathy, A.E. Comparison study of noncontact vital signs detection using a doppler stepped-frequency continuous-wave radar and camera-based imaging photoplethysmography. IEEE Trans. Microw. Theory Tech. 2017, 65, 3519–3529. [Google Scholar] [CrossRef]
- Mercuri, M.; Liu, Y.H.; Lorato, I.; Torfs, T.; Wieringa, F.; Bourdoux, A.; Van Hoof, C. A direct phase-tracking doppler radar using wavelet independent component analysis for non-contact respiratory and heart rate monitoring. IEEE Trans. Biomed. Circuits Syst. 2018, 12, 632–643. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Hong, H.; Miao, D.; Li, Y.; Zhang, H.; Zhang, Y.; Li, C.; Zhu, X. A noncontact breathing disorder recognition system using 2.4-GHz digital-IF doppler radar. IEEE J. Biomed. Health Inform. 2019, 23, 208–217. [Google Scholar] [CrossRef] [PubMed]
- van Loon, K.; Breteler, M.J.M.; van Wolfwinkel, L.; Rheineck Leyssius, A.T.; Kossen, S.; Kalkman, C.J.; van Zaane, B.; Peelen, L.M. Wireless non-invasive continuous respiratory monitoring with FMCW radar: A clinical validation study. J. Clin. Monit. Comput. 2016, 30, 797–805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sachs, J. Handbook of Ultra-Wideband Short-Range Sensing: Theory, Sensors, Applications; Wiley-VCH Verlag: Singapore, 2012. [Google Scholar]
- Schires, E.; Georgiou, P.; Lande, T.S. Vital sign monitoring through the back using an UWB impulse radar with body coupled antennas. IEEE Trans. Biomed. Circuits Syst. 2018, 12, 292–302. [Google Scholar] [CrossRef] [PubMed]
- Tayaranian Hosseini, S.M.A.; Amindavar, H.; Amirmazlaghani, M. A new robust vital sign detection in complex environments using ultrawideband radar. IEEE Trans. Geosci. Remote Sens. 2016, 54, 6771–6782. [Google Scholar] [CrossRef]
- van Loon, K.; Peelen, L.M.; van de Vlasakker, E.C.; Kalkman, C.J.; van Wolfswinkel, L.; van Zaane, B. Accuracy of remote continuous respiratory rate monitoring technologies intended for low care clinical settings: A prospective observational study. Can. J. Anaesth. 2018, 65, 1324–1332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, M.; Nian, Y.; Liu, B. Noncontact heart beat signal extraction based on wavelet transform. In Proceedings of the 2015 8th International Conference on Biomedical Engineering and Informatics (BMEI), Shenyang, China, 14–16 October 2015; IEEE: Shenyang, China, 2015; pp. 209–213. [Google Scholar]
- Shyu, K.K.; Chiu, L.J.; Lee, P.L.; Tung, T.H.; Yang, S.H. Detection of breathing and heart rates in uwb radar sensor data using FVPIEF-based two-layer EEMD. IEEE Sens. J. 2019, 19, 774–784. [Google Scholar] [CrossRef]
- Li, J.; Liu, C.; Zeng, Z.; Chen, L. GPR signal denoising and target extraction with the CEEMD method. IEEE Geosci. Remote Sens. Lett. 2015, 12, 1615–1619. [Google Scholar] [CrossRef]
- Ye, C.; Toyoda, K.; Ohtsuki, T. Blind source separation on non-contact heartbeat detection by non-negative matrix factorization algorithms. IEEE Trans. Biomed. Circuits Syst. 2020, 67, 482–494. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Chen, W. Recent advancements in empirical wavelet transform and its applications. IEEE Access 2019, 7, 103770–103780. [Google Scholar] [CrossRef]
- He, M.; Nian, Y.; Wang, X.; Xiao, S.; Li, Y. Improved clutter suppression algorithm for atmospheric target detection using polarimetric doppler radar. IEEE J. Sel. Top. Appl. Earth Obs. Remote Sens. 2011, 4, 911–922. [Google Scholar] [CrossRef]
- Ceba, F.; Makhoul, E.; Broquetas, A.; Zhan, Y.; Beaton, A.J. Modeling fast boat motion impact on satellite SAR MTI systems. IEEE Geosci. Remote Sens. Lett. 2015, 12, 2145–2149. [Google Scholar] [CrossRef]
- Ward, K.D.; Tough, R.; Watts, S. Sea Clutter: Scattering, the K Distribution and Radar Performance; IET: London, UK, 2013. [Google Scholar]
- Sherwood, L. Fundamentals of Physiology: A Human Perspective; Brooks Cole: Florence, KY, USA, 2005. [Google Scholar]
- Gilles, J. Empirical wavelet transform. IEEE Trans. Signal Process. 2013, 61, 3999–4010. [Google Scholar] [CrossRef]
- Wang, G.; Munoz-Ferreras, J.M.; Gu, C.; Li, C.; Gomez-Garcia, R. Application of linear-frequency-modulated continuous-wave (LFMCW) radars for tracking of vital signs. IEEE Trans. Microw. Theory Tech. 2014, 62, 1387–1399. [Google Scholar] [CrossRef]
- Altman, D.G.; Bland, J.M. Measurement in medicine: The analysis of method comparison studies. Statistician 1983, 32, 307–317. [Google Scholar] [CrossRef]
- Giavarina, D. Understanding bland altman analysis. Biochem. Med. 2015, 25, 141–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanz, P.; Krieger, S.; Drillich, M.; Iwersen, M. Technical note: Evaluation of a wireless pulse oximeter for measuring arterial oxygen saturation and pulse rate in newborn Holstein Friesian calves. J. Dairy Sci. 2018, 101, 6437–6442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Association for the Advancement of Medical Instrumentation. Cardiac Monitors, Heart Rate Meters, and Alarms [American National Standard (ANSI/AAMI EC13:2002)]; Association for the Advancement of Medical Instrumentation: Arlington, VA, USA, 2002. [Google Scholar]
- Sundararajan, D. Discrete Wavelet Transform: A Signal Processing Approach; John Wiley & Sons: Singapore, 2015. [Google Scholar]
- Ren, L.; Koo, Y.S.; Wang, H.; Wang, Y.; Liu, Q.; Fathy, A.E. Noncontact multiple heartbeats detection and subject localization using UWB impulse doppler radar. IEEE Microw. Wirel. Compon. Lett. 2015, 25, 690–692. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Vital Signs | Statistical Parameters | Method | |||
|---|---|---|---|---|---|
| BPF | EMD | WT | Proposed | ||
| RR | MD | −1.167 | −1.636 | 1.084 | 0.021 |
| SD | 3.507 | 4.740 | 2.068 | 0.099 | |
| MD + 1.96SD | 5.706 | 7.655 | 5.136 | 0.215 | |
| MD − 1.96SD | −8.041 | −10.927 | −2.969 | −0.173 | |
| HR | MD | −1.508 | −1.992 | 0.928 | 0.084 |
| SD | 3.182 | 4.279 | 3.182 | 0.661 | |
| MD + 1.96SD | 4.729 | 6.394 | 7.166 | 1.380 | |
| MD − 1.96SD | −7.746 | −10.378 | −5.309 | −1.212 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
He, M.; Nian, Y.; Xu, L.; Qiao, L.; Wang, W. Adaptive Separation of Respiratory and Heartbeat Signals among Multiple People Based on Empirical Wavelet Transform Using UWB Radar. Sensors 2020, 20, 4913. https://doi.org/10.3390/s20174913
He M, Nian Y, Xu L, Qiao L, Wang W. Adaptive Separation of Respiratory and Heartbeat Signals among Multiple People Based on Empirical Wavelet Transform Using UWB Radar. Sensors. 2020; 20(17):4913. https://doi.org/10.3390/s20174913
Chicago/Turabian StyleHe, Mi, Yongjian Nian, Luping Xu, Lihong Qiao, and Wenwu Wang. 2020. "Adaptive Separation of Respiratory and Heartbeat Signals among Multiple People Based on Empirical Wavelet Transform Using UWB Radar" Sensors 20, no. 17: 4913. https://doi.org/10.3390/s20174913
APA StyleHe, M., Nian, Y., Xu, L., Qiao, L., & Wang, W. (2020). Adaptive Separation of Respiratory and Heartbeat Signals among Multiple People Based on Empirical Wavelet Transform Using UWB Radar. Sensors, 20(17), 4913. https://doi.org/10.3390/s20174913