A Review of Microelectronic Systems and Circuit Techniques for Electrical Neural Recording Aimed at Closed-Loop Epilepsy Control



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
1.1. Engineering Overview of Epilepsy, Seizures and Treatment
- At least two unprovoked (or reflex) seizures occurring >24 h apart.
- one unprovoked (or reflex) seizure and a probability of further seizures similar to the general recurrence risk (at least 60%) after two unprovoked seizures, occurring over the next 10 years.
- diagnosis of an epilepsy syndrome.
1.1.1. Phases of a Seizure
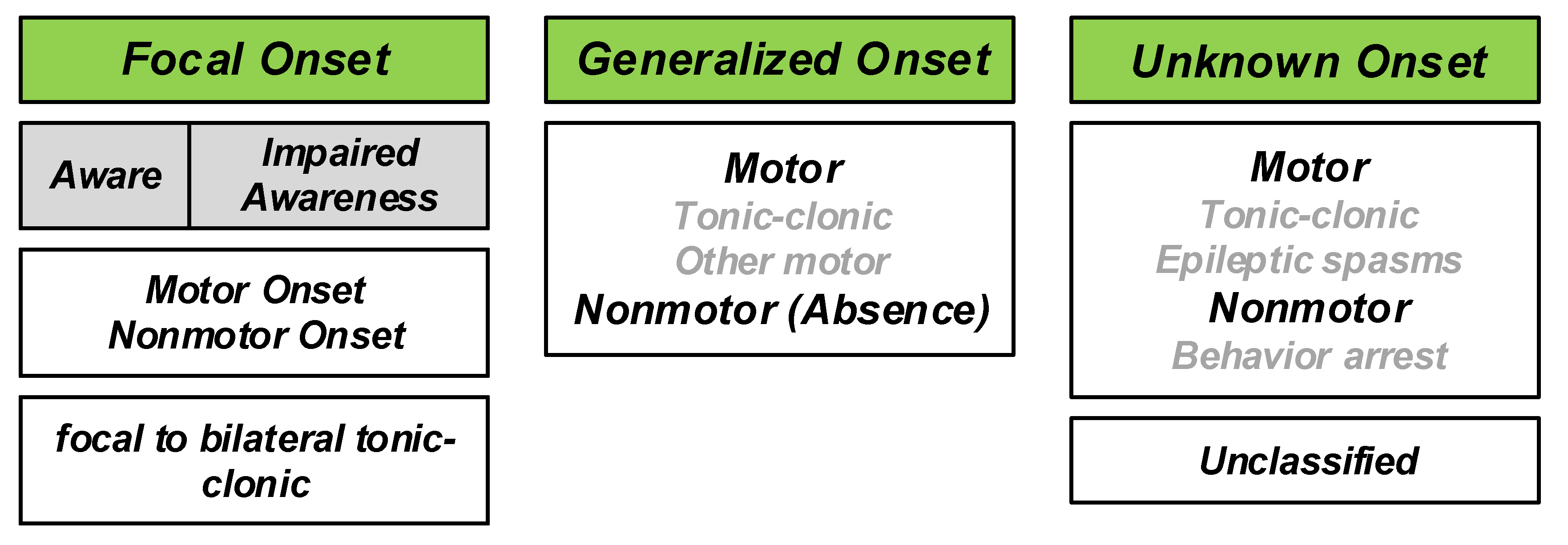
1.1.2. Seizure Classification
- The onset or beginning of a seizure;
- a person’s level of awareness during a seizure, and
- whether body movements occur during a seizure.
1.1.3. Statistics
1.1.4. Epilepsy Treatment
- Seizures diffuse over an excessively large area;
- seizures occur in sensitive areas of eloquent cortex that may not be surgically treated;
- seizures have multiple foci (multifocal seizures) which are thus difficult to individual localization and in practice impossible to surgically treat;
- surgery may not be tolerable due to specific medical conditions.
2. Introduction to Epilepsy Control Using Implantable Microelectronic Systems
2.1. Electrical Stimulation
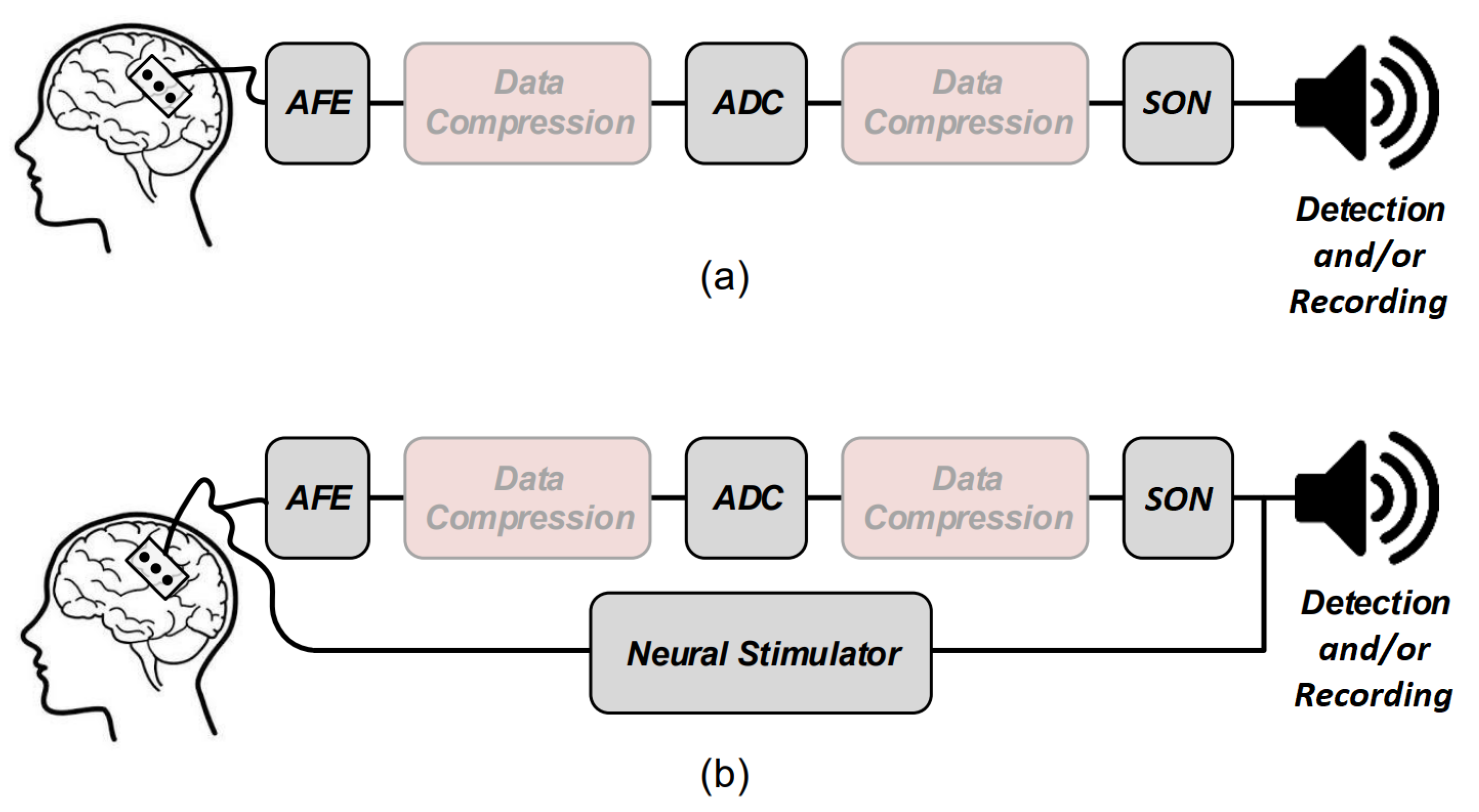
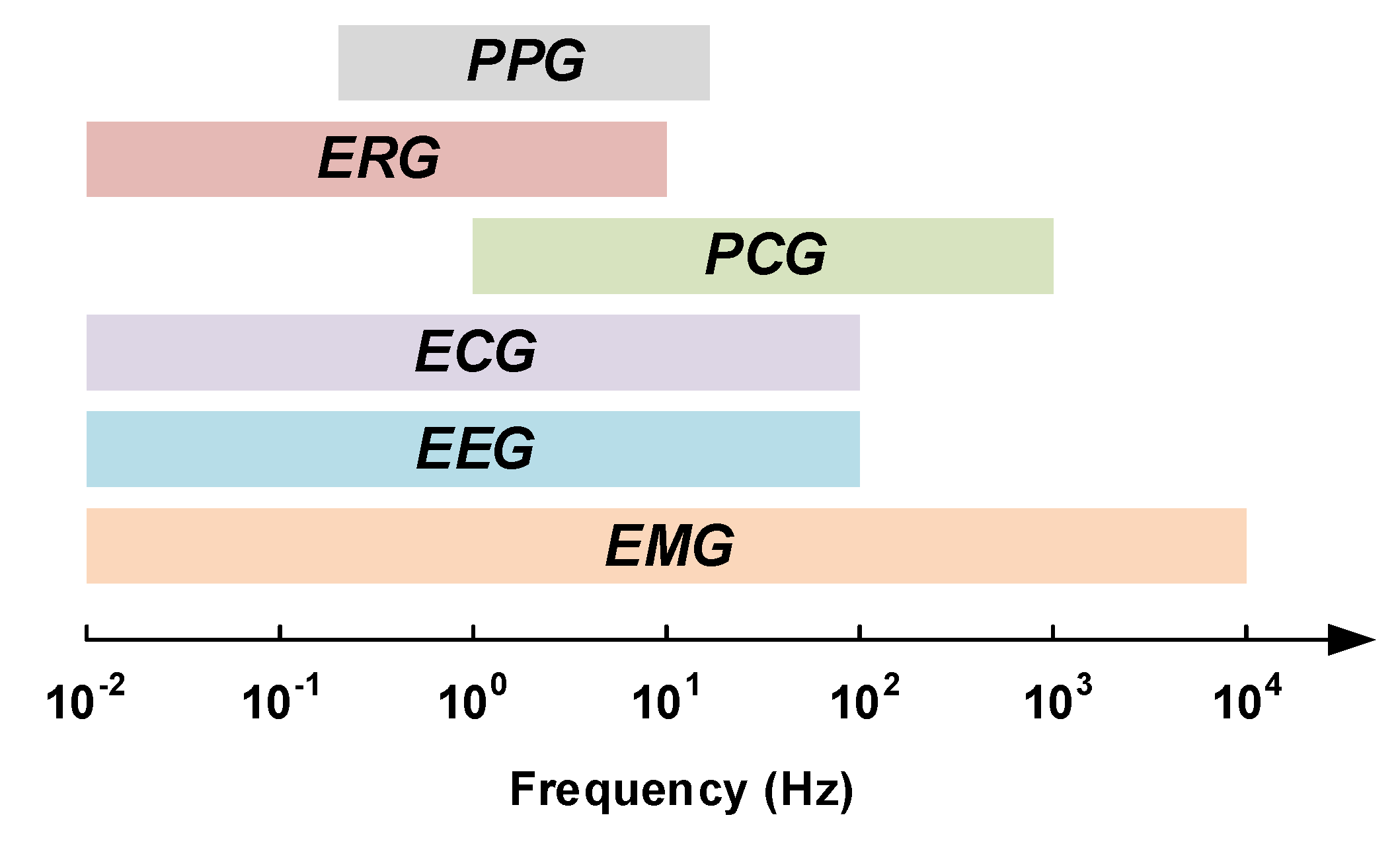
2.2. Physiological Signal Recording
Neural Signal Recording
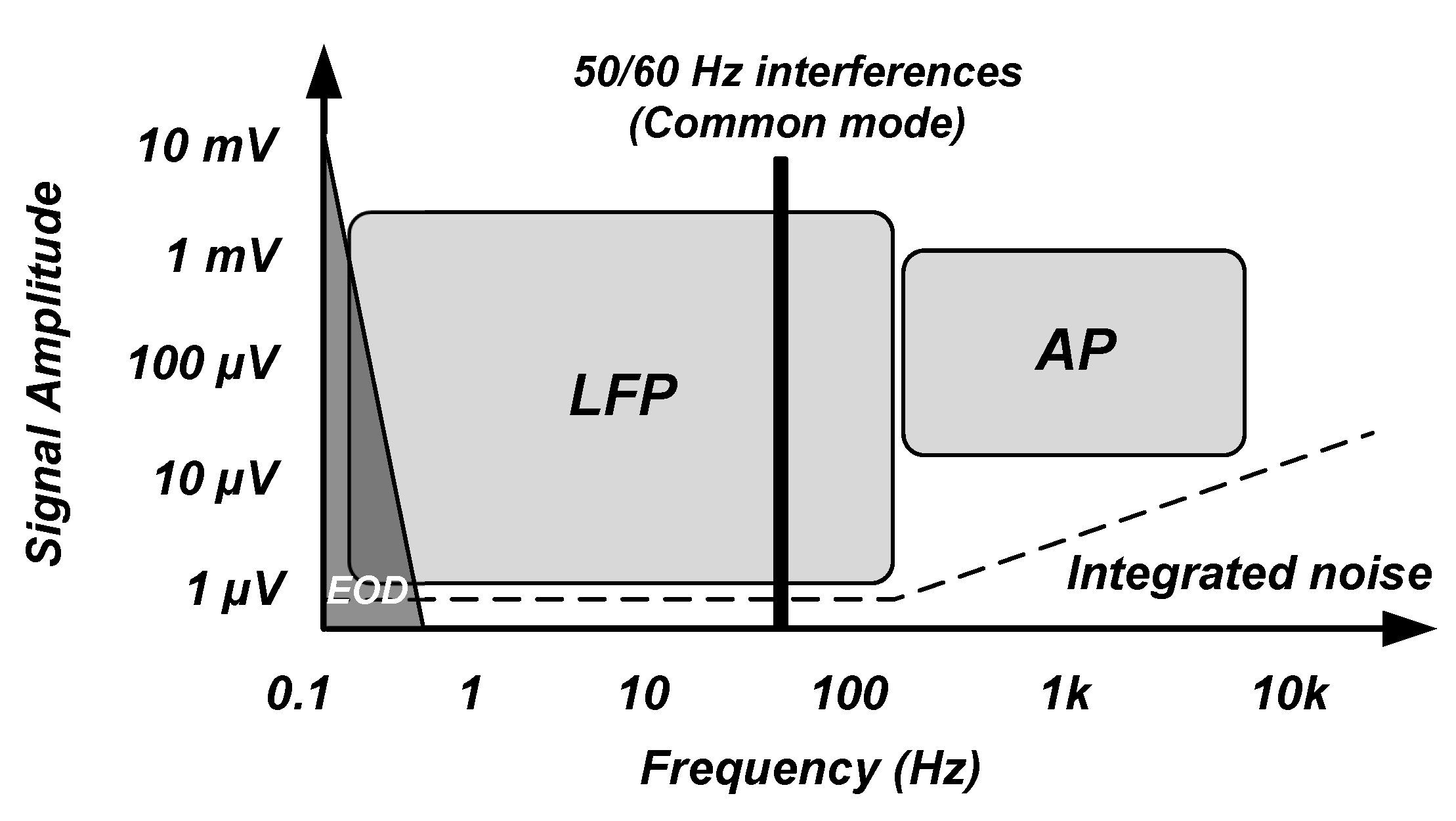
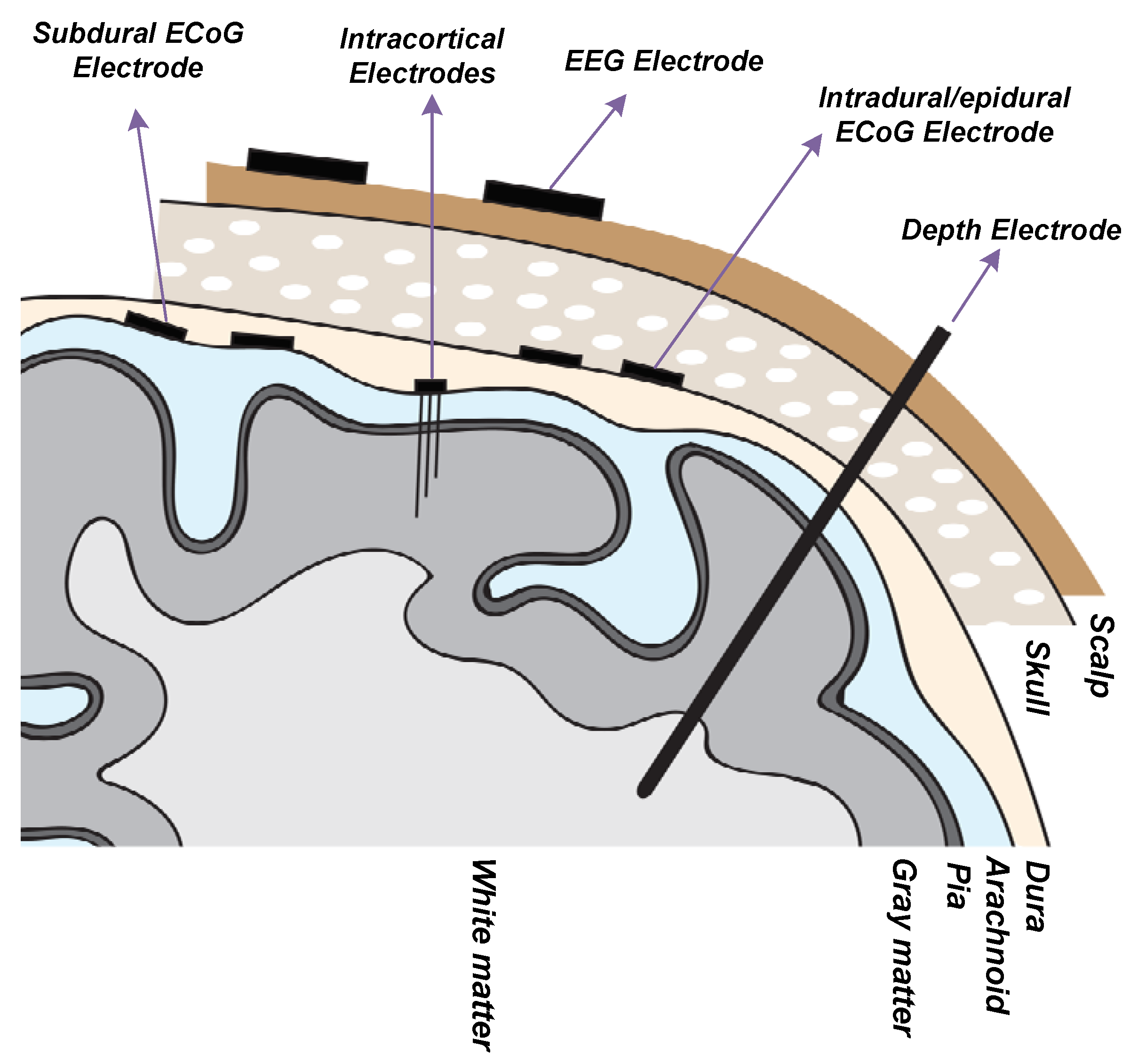
- Electroencephalography (EEG) Electrode ([32,33,34]): EEG electrodes are placed on the surface of the scalp. The international 10–20 system is a well-known and internationally recognized distribution of each of the EEG electrodes on the scalp. EEG recording offers several applications including brain-machine interfaces (BMI), polysomnography (PSG) for a sleep study, seizure detection, as well as other medical applications aiming at brain research. EEG recording is not an invasive method. The amplitude and bandwidth of the neural signals recorded by EEG electrodes are significantly smaller than the signals recorded by implantable electrodes due to the filtering behavior of cerebrospinal fluid (CSF), dura, skull and scalp. Furthermore, the fragile EEG signals are more exposed to different sources of artifacts including patient-related artifacts (e.g., movement, sweating, ECG, eye movements) and technical artifacts (50/60 Hz artifact, cable movements, electrode paste-related). The bandwidth of the EEG signals lies in the bandwidth of the LFP signals.
- Intracranial Electroencephalography (iEEG) [35]: Recording the neural signals inside the skull provides better signal quality in terms of signal-to-noise ratio and bandwidth. Intracranial EEG recording can be done using different types of electrodes including epidural electro-corticography (ECoG) electrodes, subdural ECoG electrodes, intracortical electrodes and depth electrodes.
2.3. Additional Blocks of Closed-Loop Epilepsy Control System
3. Commercial Systems and Products for Epilepsy Control
3.1. FDA Approved Implantable Electronic Medical Devices
3.1.1. Vagus Nerve Stimulation Therapy
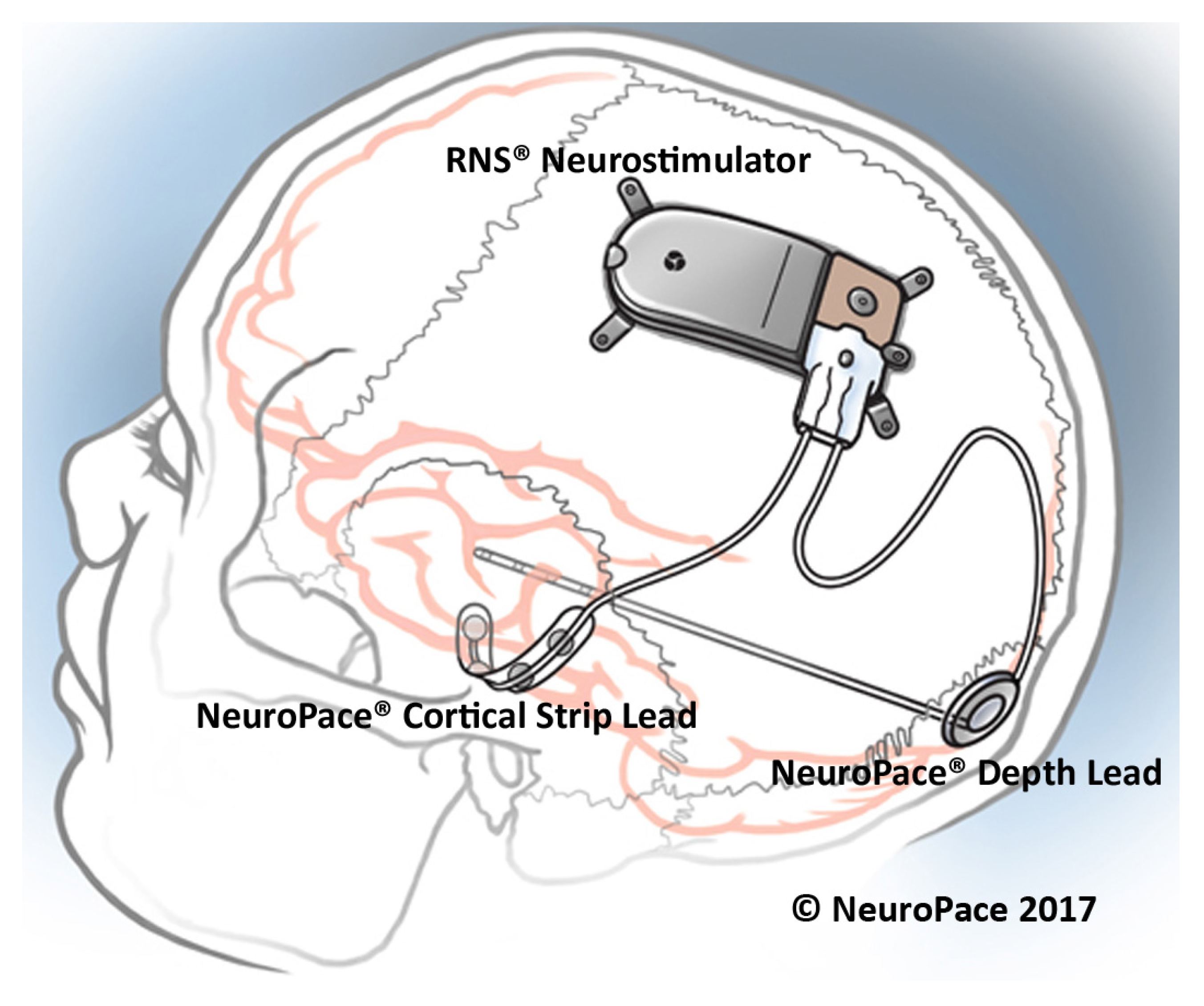
3.1.2. Responsive Neurostimulation
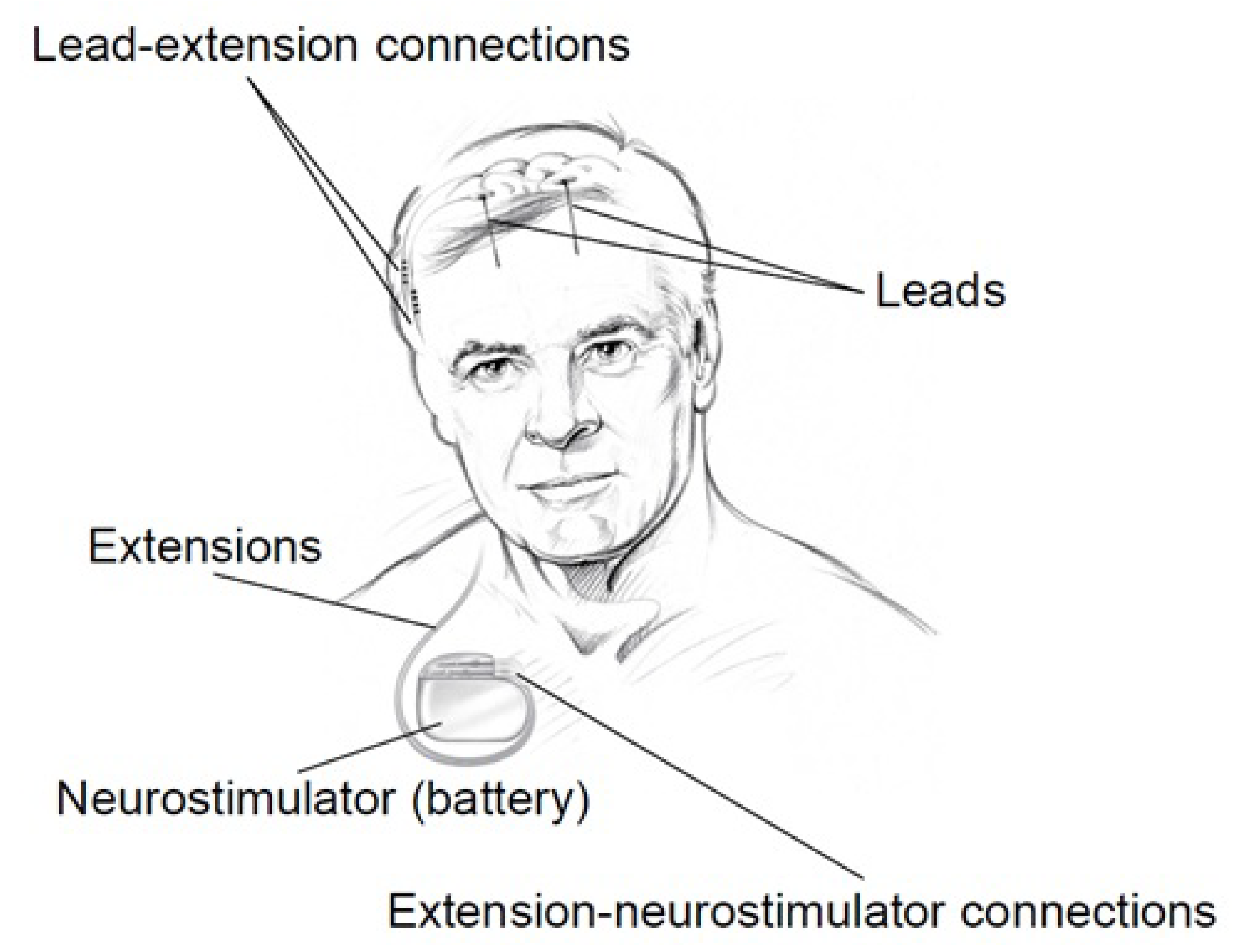
3.1.3. DBS
3.2. Commercialized Non-invasive Medical Devices
- external stimulators, and
- seizure alerting devices.
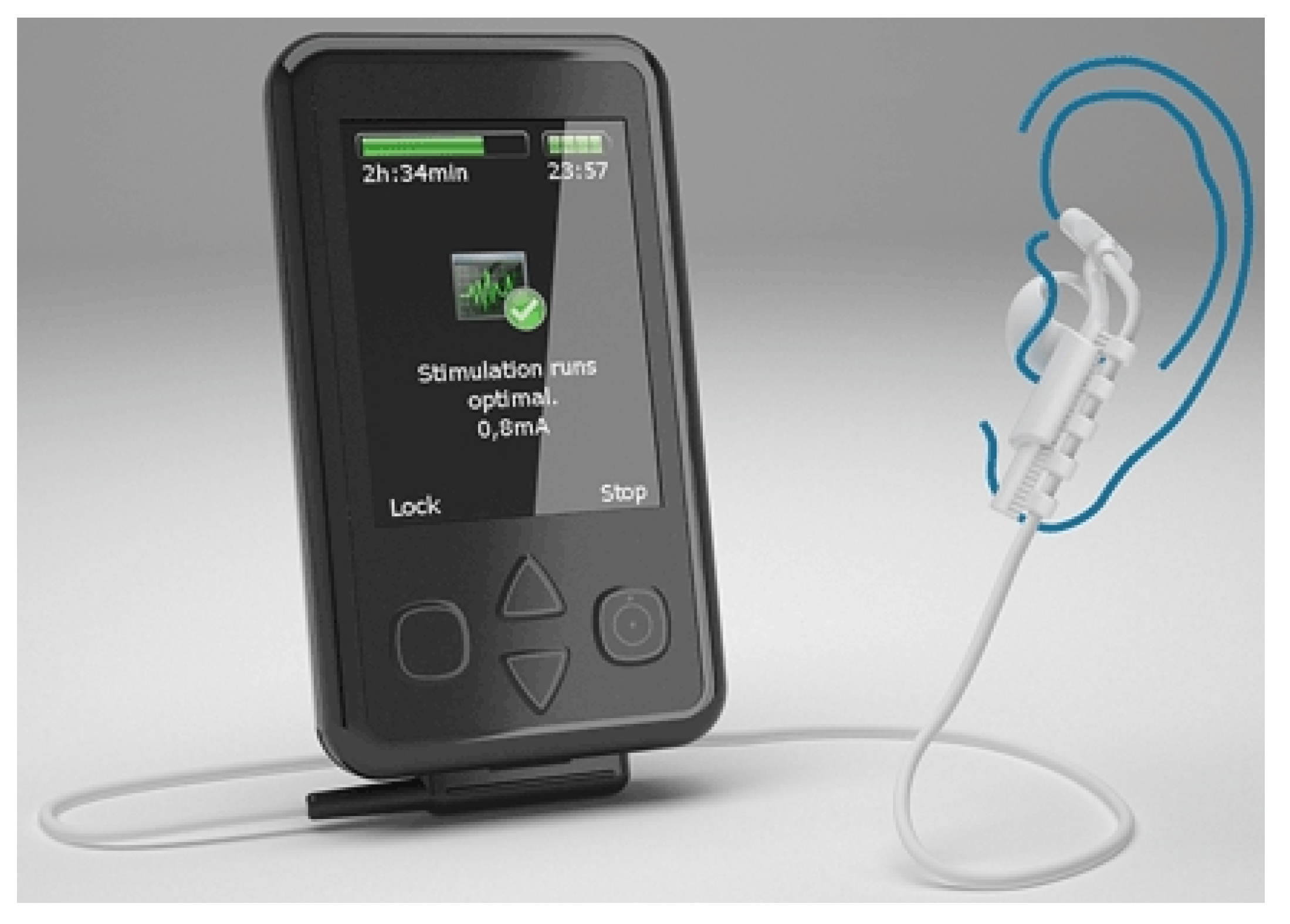
3.2.1. External Stimulators
3.2.2. Seizure Alerting Devices
- Watch devices
- Motion devices
- Mattress devices
- Camera devices
4. Neural Recording Circuit Techniques
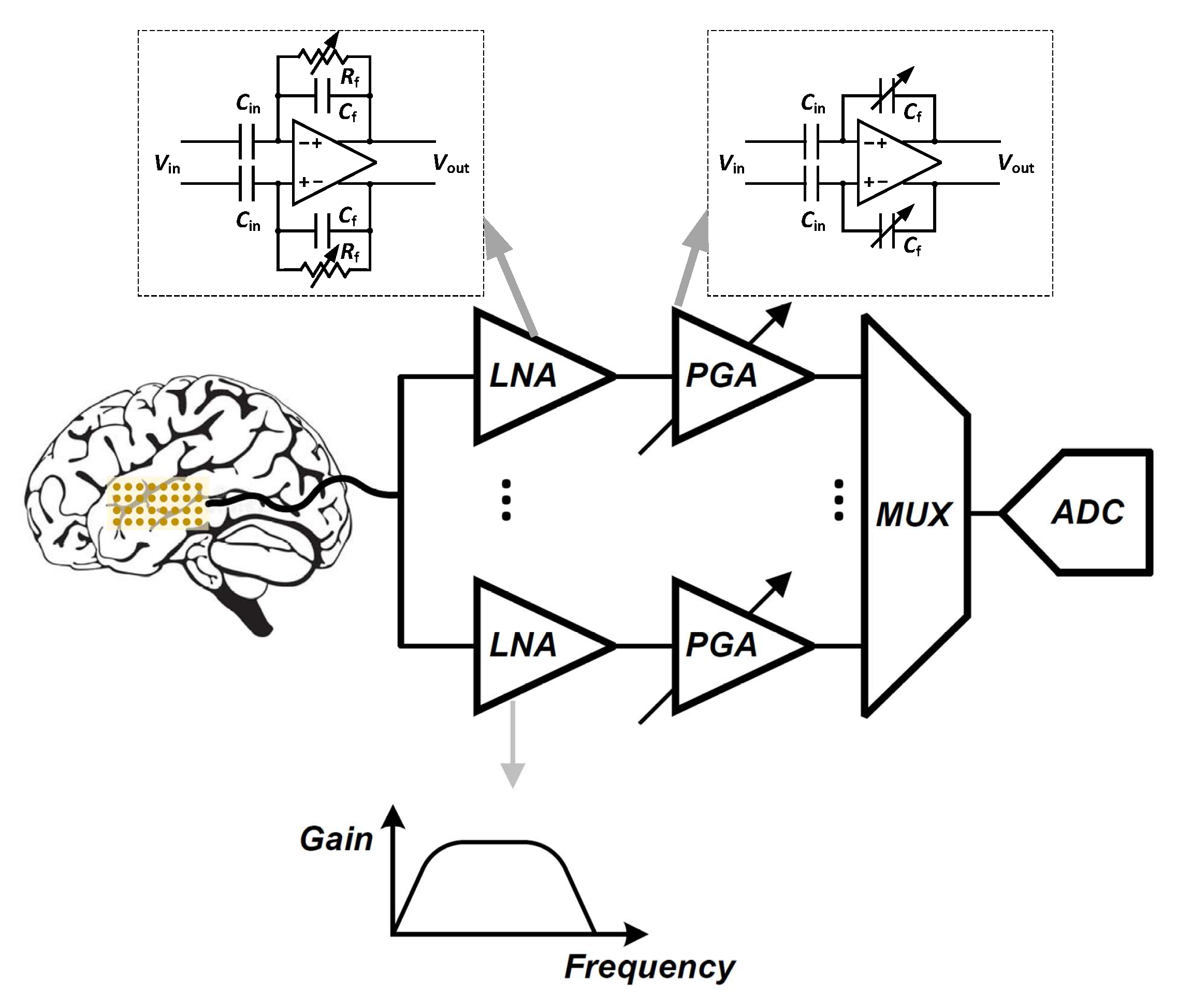
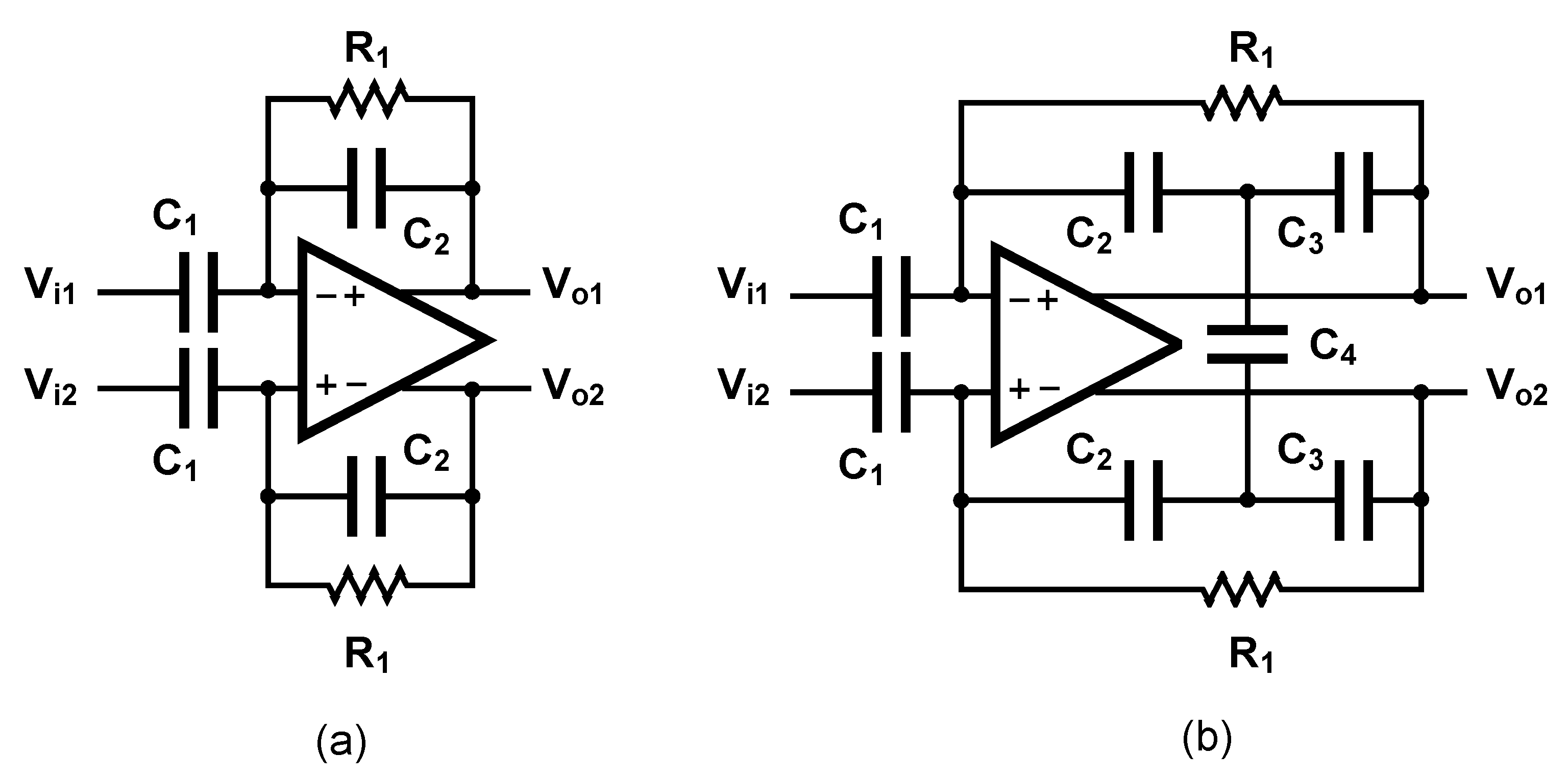
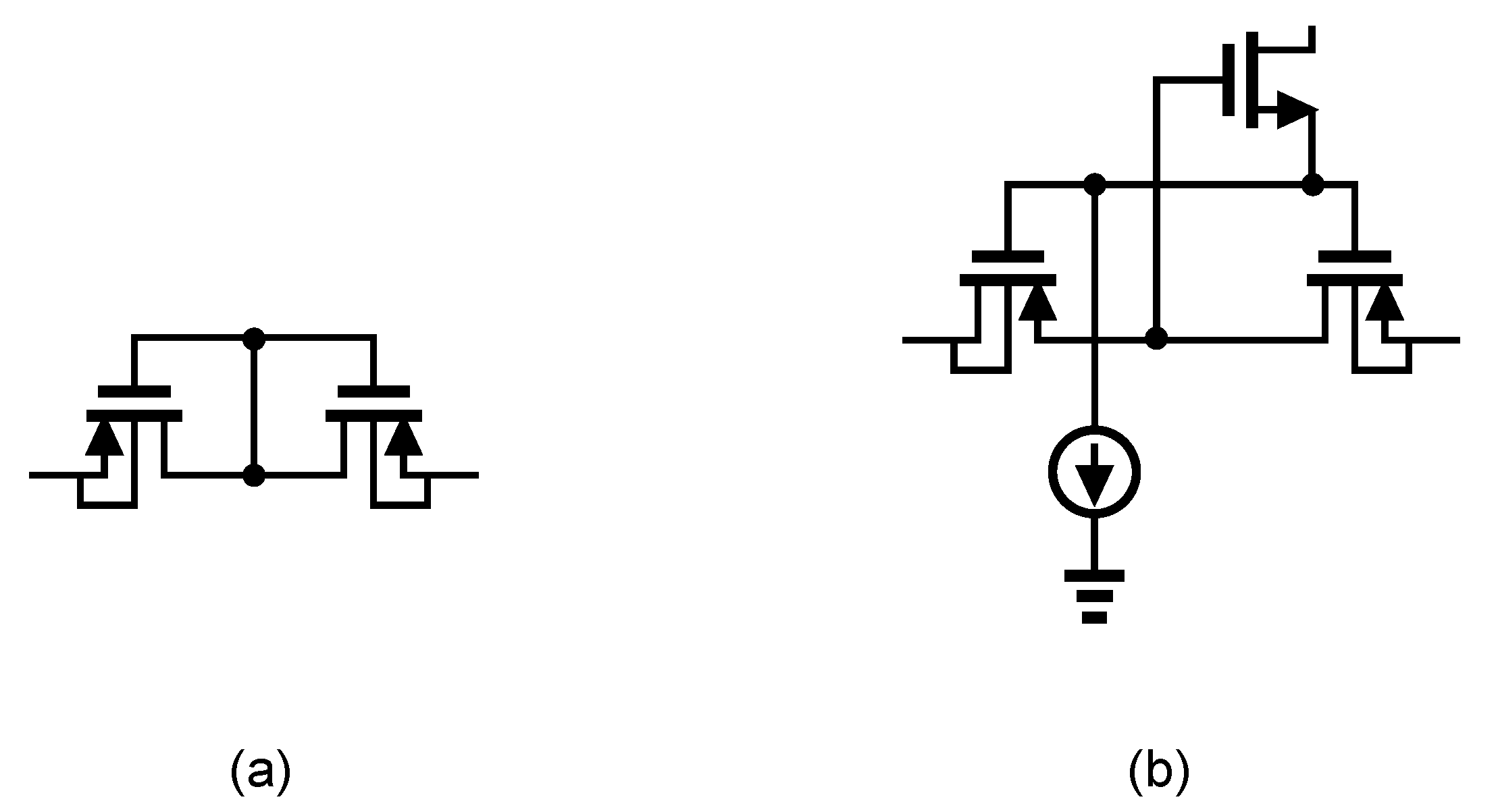
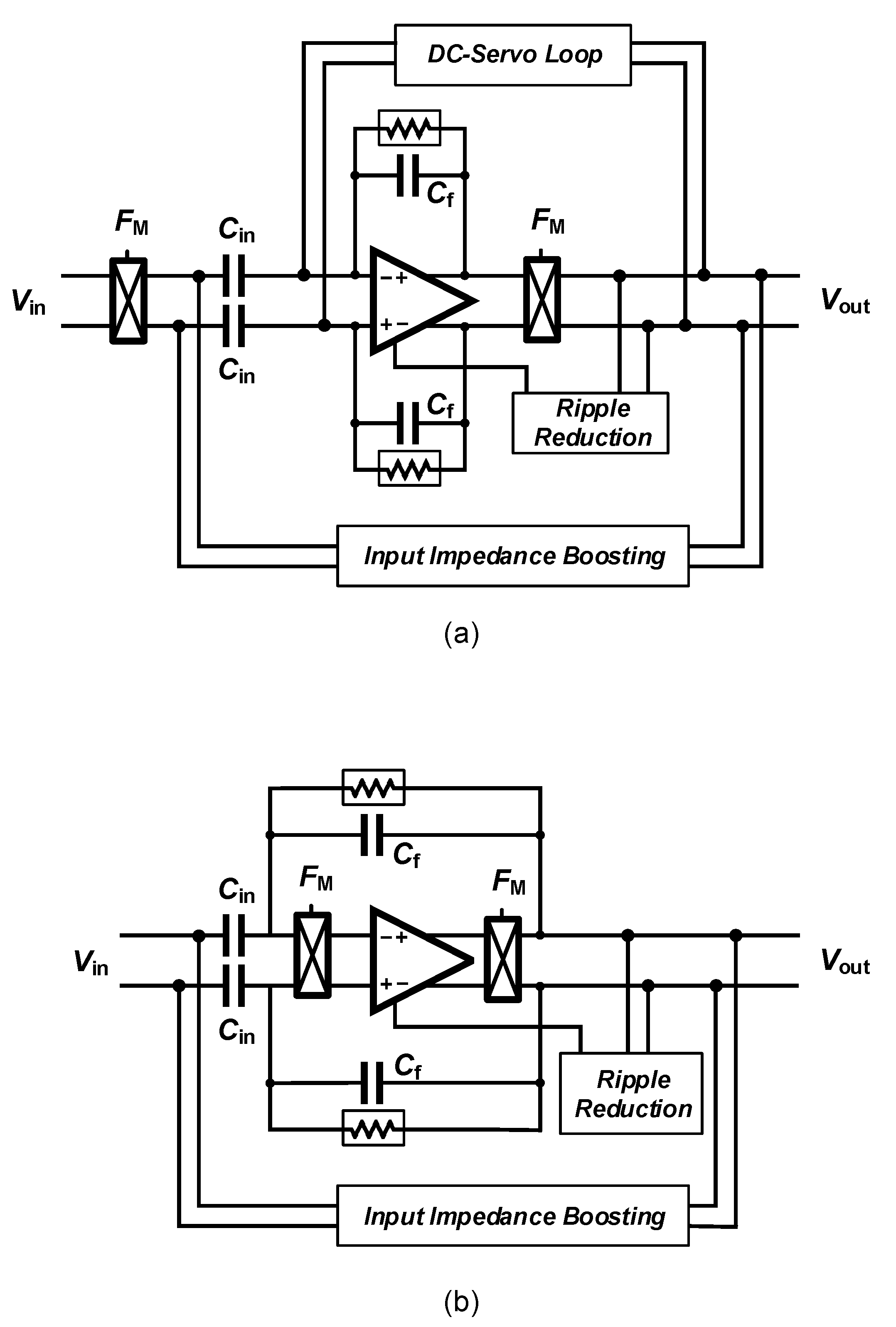
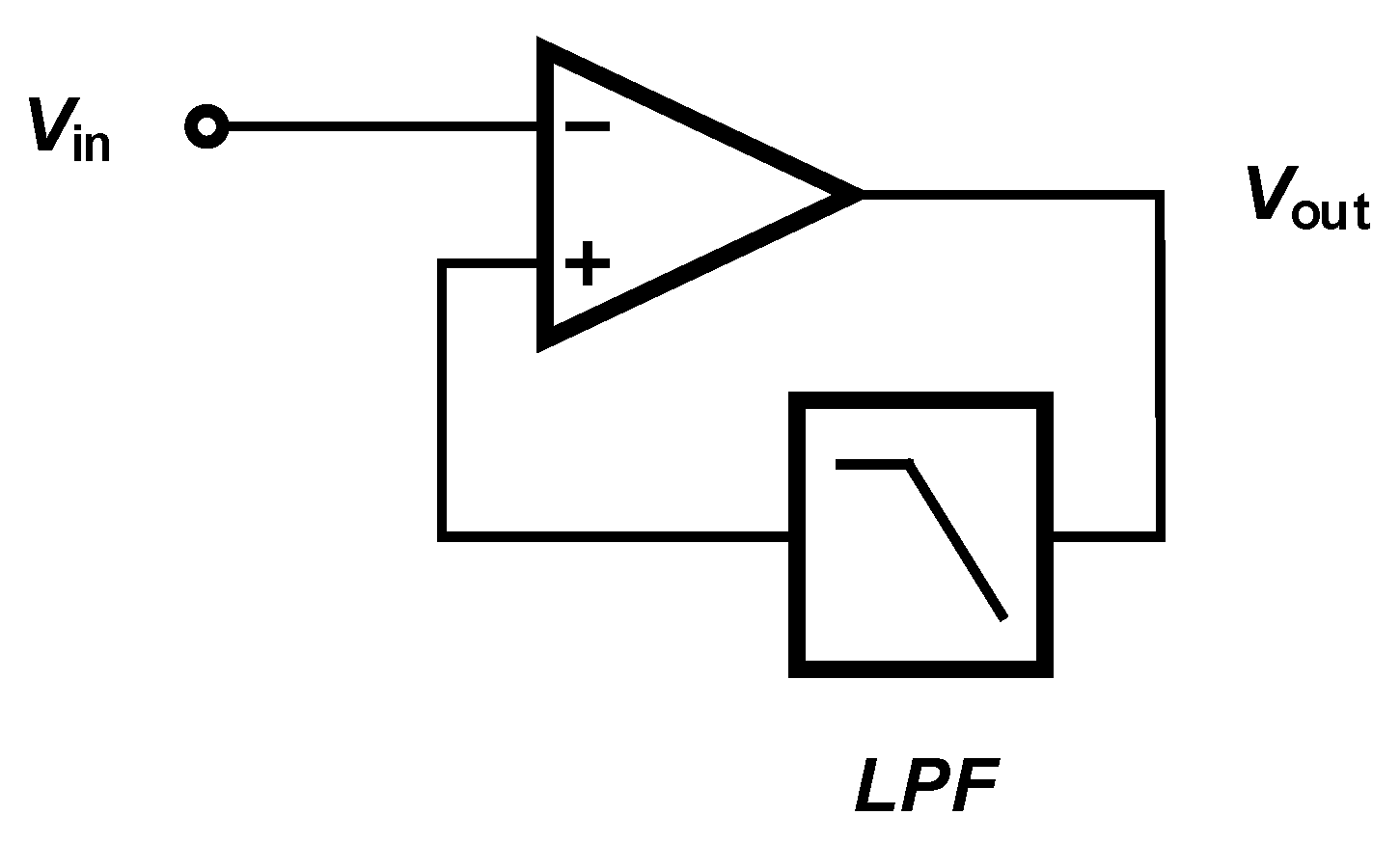
4.1. Low-Noise Front-End Amplifier
- high-pass filtering for electrode offset rejection
- appropriate gain for conditioning the signals prior to digitization
- low input-referred noise for sensing weak neural signals
- low-power consumption (for neural amplifiers used in implantable devices)
- compact size (for neural amplifiers used in implantable devices)
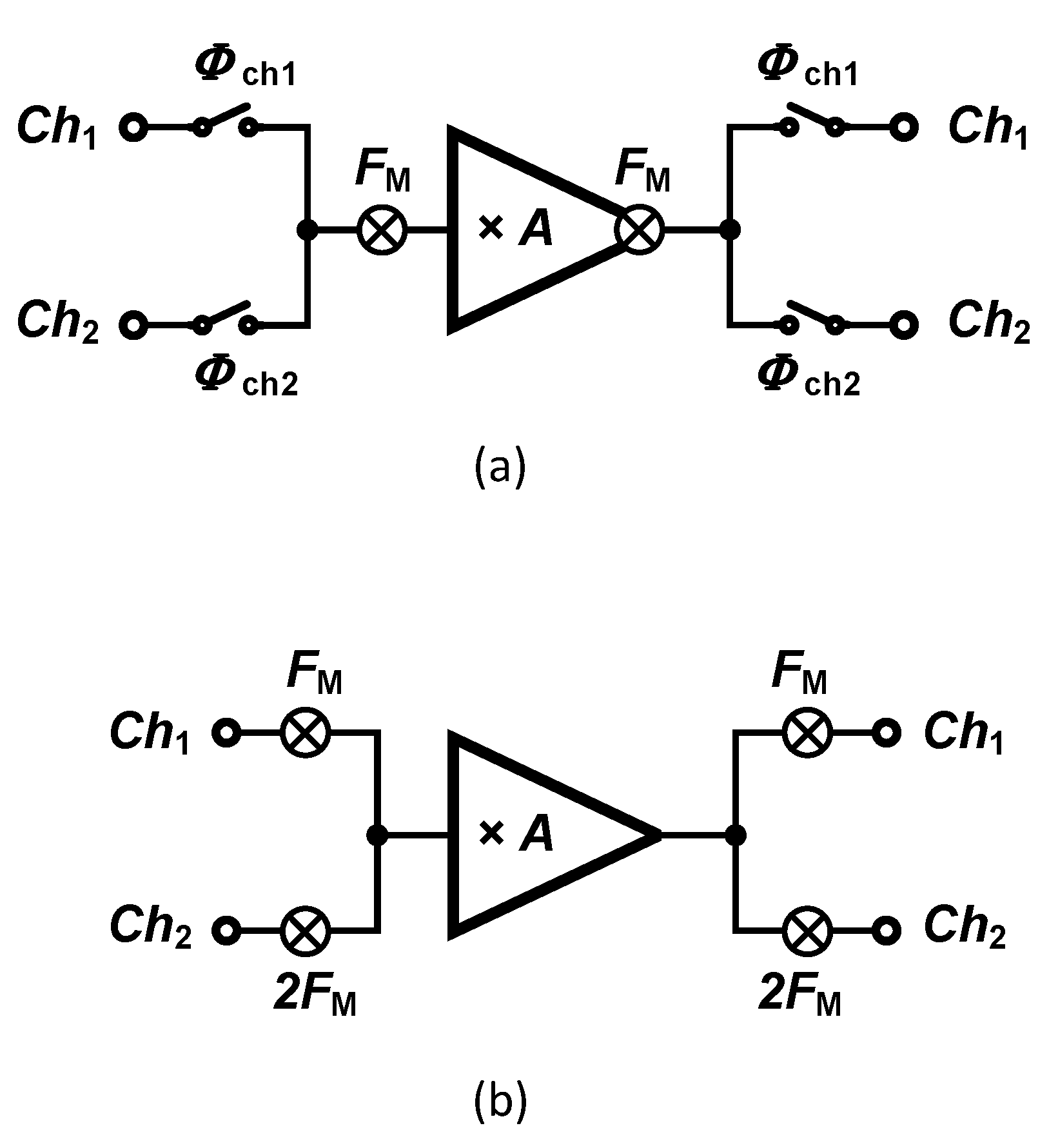
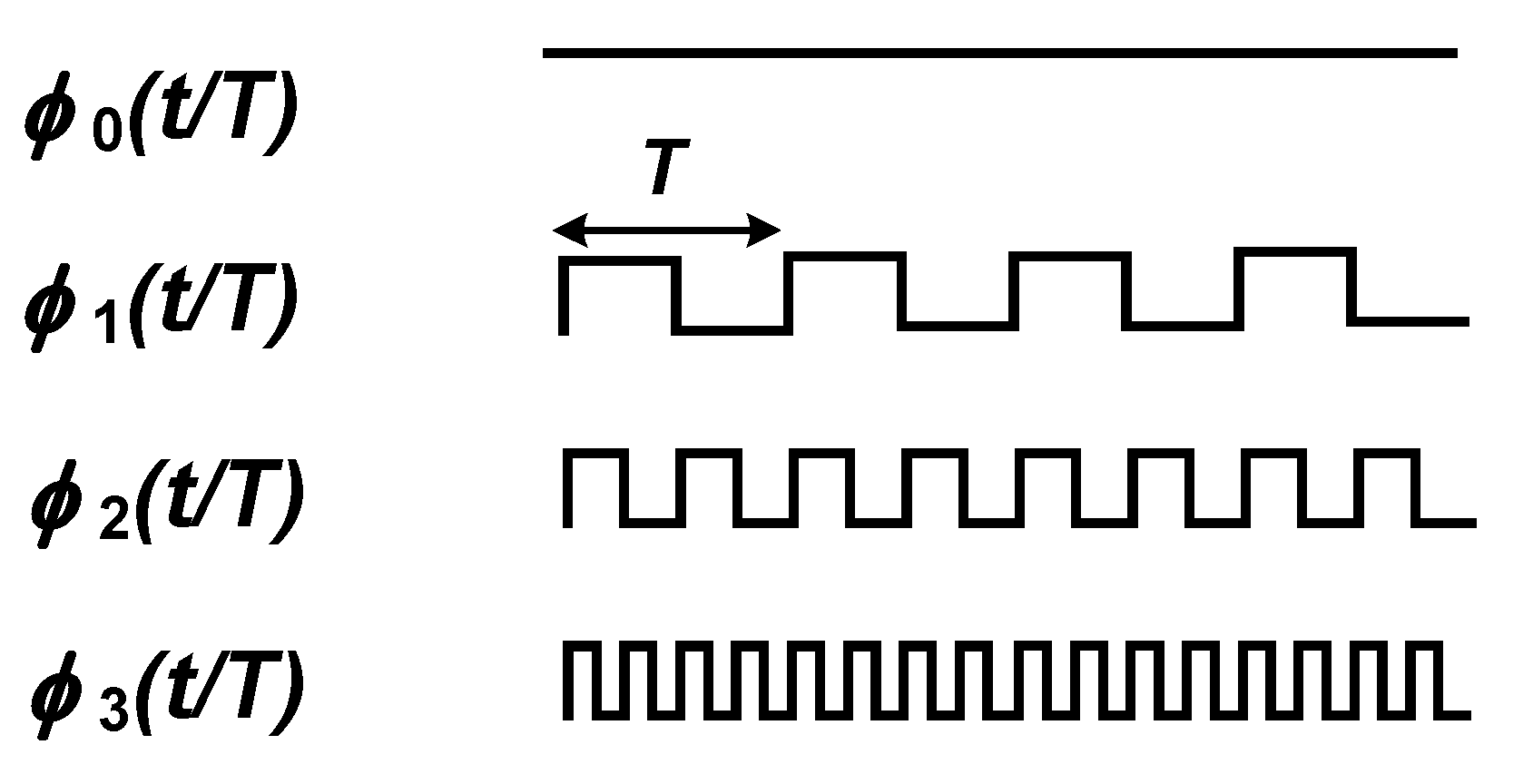
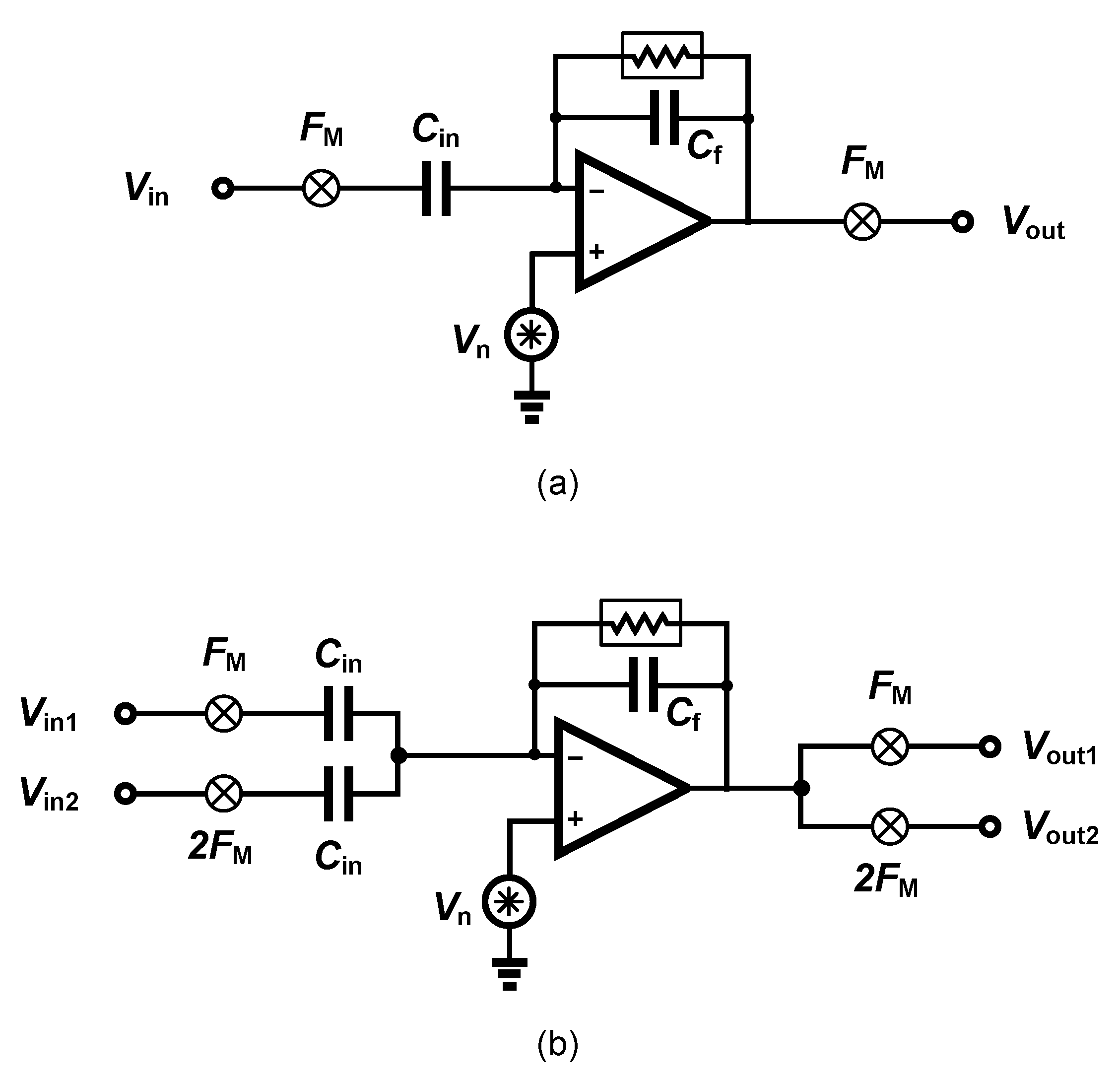
Amplifier Sharing Methods
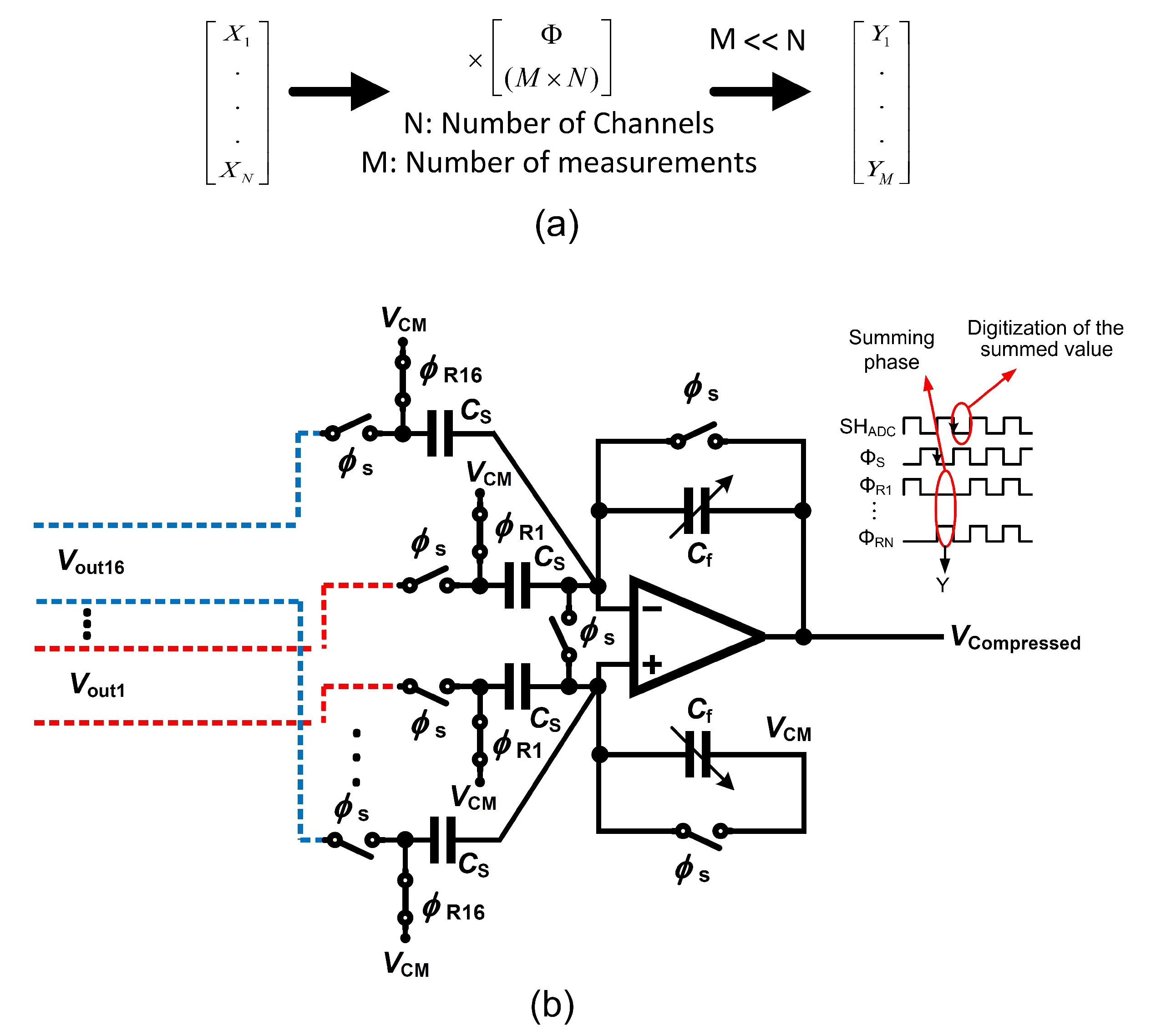
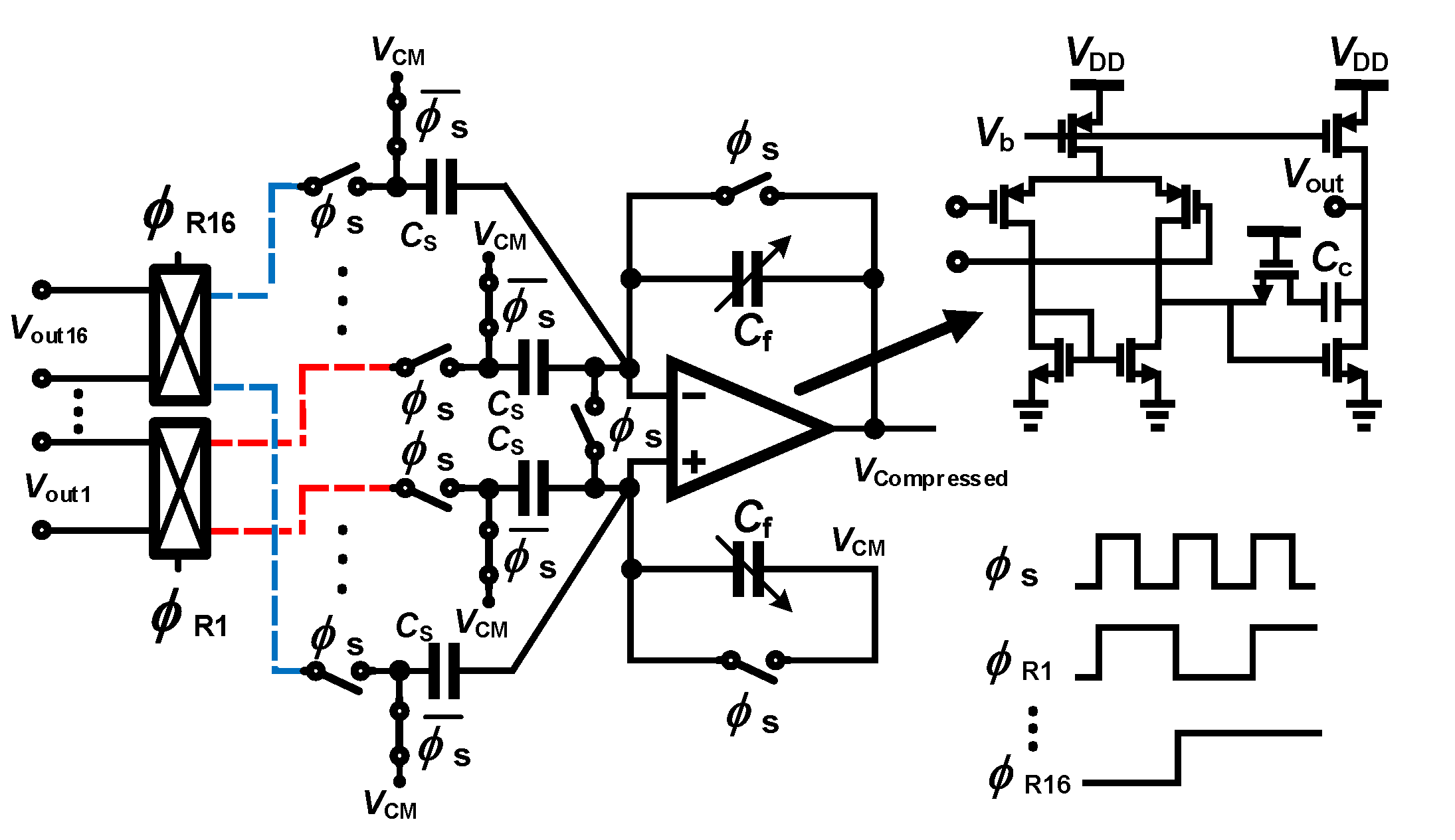
4.2. Data Compression
4.3. Feature Extraction
- Time-domain feature extraction. The raw signal originating from the signal conditioning chain to the ADC is in turn processed. Usually, the algorithms process the data delivered as successive windows comprising a fixed number of samples. The processed feature score is compared to a threshold yielding a decision.
- Frequency-domain features. Spectral-based feature extractors operate in the digital domain. A fast-Fourier transform is typically applied to the input signal originating from an ADC, and prior to extracting features in the frequency domain. Bandwidths of interests are determined, and the energy is computed within a selected frequency range, e.g., [91]. The process is repeated in time (or time-window) yielding a decision.
- Energy: the energy feature is a popular feature. The average energy of d samples is calculated as expressed in Equation (7).A multiple and accumulate block is used to process the data that streams-into. The inputs of the multiplier are identical, yielding the operation.
- Accumulated energy: the accumulated energy extractor applies the energy criteria over several time-windows.
- Variance and Hjorth variance The variance criteria has extensively been applied in EEG studies. The variance is processed over a window of d samples, and then averaged. The intuitive formulation that directs the hardware implementation is expressed in Equation (8).The hardware is more complex than the hardware required in the energy extractor, and consists of multipliers and accumulators, subtractors and temporary storage registers.
- Line-length or Coastline: the line-length is a measure of the absolute value of the length between two consecutive data points. Line-length is a feature that increases with low-amplitude while high-frequency signals are presented, as well high-amplitude while low-frequency signals are presented. The line-length feature for d samples is calculated as expressed in Equation (9).The hardware is relatively straightforward and consists of multipliers and accumulators, temporary storage registers as well as multiplexers.
- Area: area is a popular feature for seizure detection. The simplicity of the algorithm enables a low-cost and accurate seizure detection. Area is one of the features used in RNS (Section 3.1.2. The area feature for d samples of the signal is calculated as expressed in Equation (10).
- Non-linear autocorrelation: non-linear autocorrelation feature extraction is based on detecting and accumulating the minimum of the maximum of the samples in three consecutive windows, also detecting and accumulating the maximum of the minima of the samples in three consecutive windows, and finally subtracting the latter from the former result, as expressed in Equation (11).The hardware requires many resources including a multiplier-accumulators, subtractors, storage resisters as well as several comparators.
5. Discussion
- Size: the most important challenge of an implantable system is the size. Any implantable medical device (IEMD) is composed of several electrical modules. Some of these modules consist of off-chip components such as wireless powering modules or the wireless data transmitter. The specification of these modules should be defined in a way that the IEMD system presents an acceptable size. The IEMD weight is a related parameter. Increasing the size and the weight of IEMDs also increases the complexity of the surgery. Hence, for the convenience of the patients, IEMDs should have a minimum number of off-chip components in order to present a minimum size and weight.A solution for decreasing the size of an implant is to integrate the active circuits as close as possible to the electrode. One method to realize this solution consists of fabricating a silicon-based electrode which allows the active circuits to be implemented on the same silicon or by attaching the active circuitry to the silicon-based electrode using post-CMOS processes.
- Power consumption and temperature elevation: a limitation for temperature raise is imposed by medical regulations for IEMDs. IEMDs temperature should not exceed predefined limits. Generally, the temperature of the outer surface of an implanted device must be limited to 2 °C above body temperature [97]. However, this limit is reported to be 1 °C above body temperature in IEEE standards [98], specially in cortical implants [99]. A device that exceeds this limit should be turned off immediately. Hence, temperature sensors should be considered in the design of IEMDs and stimulators to enable temperature management capabilities of the systems [100].
- Battery powering and rechargeability: IEMDs should offer freedom to patients to proceed in their life with regular activities. This autonomy cannot be provided without using an implanted battery. Moreover, to increase the lifetime of IEMDs, the battery should be rechargeable. Therefore, patients undergo less surgery for the placement and/or removal of the IEMDs. However, the main challenge in the design of rechargeable IEMDs consists of wirelessly and efficiently recharging the implanted battery. Efficiency in the wireless battery charging is very important since this procedure may generate heat and cause skin burning or unpleasant feeling during the battery charging process.
- Biocompatibility: the package and enclosure of IEMDs must be bio-compatible. A biocompatible package serves as a barrier between the electronics and other chemical materials to which a biological system may adversely react. The host response to an implanted IEMD (resulting from tissue trauma during the implantation of an IEMD and the presence of the device in the body [101]) depends on the type of material that is used for the packaging and the enclosure of the IEMD. The importance of the biocompatibility lies in the fact that the systemic toxicity impairs the entire biological system such as the nervous or the immune system [101]. In addition, the reason for a systemic reaction due to the biocompatibility cannot be traced back to its origin since it generally takes place at a location far from the point of contact of an IEMD. Due to all aforementioned issues, biocompatibility has become the most important part of the U.S. FDA approval procedure, even for Class I devices (lowest risk). Furthermore, biocompatibility is the major part of acquiring an ISO (International Organization for Standardization) standard such as ISO 10993.
- Data storage: in order to increase the accuracy of the seizure detection as well as to provide freedom and autonomy to the patient during the recording period, the implant should store data over a few hours. This feature is important since patients should not have to wear any bulky holder of an external unit (helmet, belt) during some specific activities or during sleeping. Hence, the system should save the recorded data on an implanted memory. If the IEMD is powered by a rechargeable battery, the IEMD should save the recorded data on a non-volatile memory since the IEMD may be turned off by the under-voltage lockout detection circuit.
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ACS | Analog Compressive Sensing |
| ADC | Analog-to-Digital Converter |
| AED | Anti-Epileptic Drug |
| AFE | Analog Front-End |
| BMI | Brain-Machine Interface |
| CC-LNA | Capacitive-Coupled Low-Noise Amplifier |
| CMRR | Common-Mode Rejection Ratio |
| CS | Compressive Sensing |
| CSF | Cerebrospinal Fluid |
| DBS | Deep-Brain Stimulation |
| DCS | Digital Compressive Sensing |
| DSL | dc Servo Loop |
| ECG | Electrocardiogram |
| ECoG | Electrocotricogram |
| EDA | Electrodermal Activity |
| EDO | Electrode dc Offset |
| EEG | Electroencephalogram |
| EMG | Electromyogram |
| ENOB | Effective Number of Bits |
| ERG | Electroretinogram |
| eTNS | External Trigeminal Nerve Stimulation |
| FDA | Food and Drug Administration |
| FDM | Frequency-Division Multiplexing |
| FE | Feature Extractor |
| FES | Functional Electrical Stimulation |
| ICP | Intracranial Pressure |
| iEEG | Intracranial Electroencephalography |
| IEMD | Implantable Electronic Medical Device |
| ILAE | International League Against Epilepsy |
| IMD | Implantable Medical Device |
| IPG | Integrated Pulse Generator |
| LFP | Local Field Potentials |
| LL | Line-length |
| LNA | Low-Noise Amplifier |
| MCS | Multi-channel Compressive Sensing |
| MEG | Magnetoencephalography |
| MISOCS | Multi-Input Single-Output Compressive Sensing |
| mMISOCS | modified Multi-Input Single-Output Compressive Sensing |
| MRI | Magnetic Resonance Imaging |
| NEF | Noise Efficiency Factor |
| OTA | Operational Transconductance Amplifier |
| PCG | Phonocardiogram |
| PET | Positron Emission Tomography |
| PGA | Programmable-Gain Amplifier |
| PMA | Premarket Approval |
| PPG | Photoplethysmogram |
| PSG | Polysomnography |
| RNS | Responsive Neurostimulation |
| PVT | Process, Voltage and Temperature |
| SEEG | Stereo-EEG |
| sEMG | Surface Electromyography |
| SNR | Signal-to-Noise Ratio |
| SPECT | Single-Photon Emission Computed Tomography |
| SUDEP | Sudden Unexpected Death in EPilepsy |
| tACS | transcranial Alternating Current Stimulation |
| tDCS | transcranial Direct Current Stimulation |
| TDM | Time-Division Multiplexing |
| tENS | transcutaneous Electric Nerve Stimulation |
| tTNS | Transcranial Trigeminal Nerve Stimulation |
| tVNS | transcutaneous Vagus Nerve Stimulation |
| VLSI | Very Large-Scale Integration |
| VNS | Vagus Nerve Stimulation |
| WHO | World Health Organization |
References
- Abbott, Inc., Cardiovascular. CardioMEMS HF. Available online: https://www.cardiovascular.abbott/ (accessed on 11 June 2020).
- Boston Scientific Corp. Available online: http://www.bostonscientific.com/ (accessed on 11 June 2020).
- Fisher, R.S.; Acevedo, C.; Arzimanoglou, A.; Bogacz, A.; Cross, J.H.; Elger, C.E.; Engel, J., Jr.; Forsgren, L.; French, J.A.; Glynn, M.; et al. ILAE official report: A practical clinical definition of epilepsy. Epilepsia 2014, 55, 475–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Epilepsy Foundation. Available online: https://www.epilepsy.com/ (accessed on 11 June 2020).
- Caveness, W.F.; AM LORENTZ, H.J.M.; RADERMECKER, J. A Proposed International Classification of Epileptic Seizures. Epilepsia 1964, 5, 297–306. [Google Scholar] [CrossRef]
- Bancaud, J.; Henriksen, O.; Rubio-Donnadieu, F.; Seino, M.; Dreifuss, F.; Penry, J. Commission on classification and terminology of the international league against epilepsy. Proposal for revised clinical and electroencephalographic classification of epileptic seizures. Epilepsia 1981, 22, 489–501. [Google Scholar]
- Fisher, R.S.; Cross, J.H.; French, J.A.; Higurashi, N.; Hirsch, E.; Jansen, F.E.; Lagae, L.; Moshé, S.L.; Peltola, J.; Roulet Perez, E.; et al. Operational classification of seizure types by the International League Against Epilepsy: Position Paper of the ILAE Commission for Classification and Terminology. Epilepsia 2017, 58, 522–530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korff, C.M.; Scheffer, I.E. Epilepsy classification: A cycle of evolution and revolution. Curr. Opin. Neurol. 2013, 26, 163–167. [Google Scholar] [CrossRef]
- Berg, A.T.; Scheffer, I.E. New concepts in classification of the epilepsies: Entering the 21st century. Epilepsia 2011, 52, 1058–1062. [Google Scholar] [CrossRef]
- Gao, H.; Sander, J.W.; Xiao, Y.; Zhang, Y.; Zhou, D. A comparison between the 1981 and 2017 International League Against Epilepsy classification of seizure types based on an outpatient setting. Epileptic Disorders 2018, 20, 257–264. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Available online: https://www.who.int/ (accessed on 11 June 2020).
- Traub, R.D.; Wong, R. Cellular mechanism of neuronal synchronization in epilepsy. Science 1982, 216, 745–747. [Google Scholar] [CrossRef]
- Gómez-Gonzalo, M.; Losi, G.; Chiavegato, A.; Zonta, M.; Cammarota, M.; Brondi, M.; Vetri, F.; Uva, L.; Pozzan, T.; de Curtis, M.; et al. An excitatory loop with astrocytes contributes to drive neurons to seizure threshold. PLoS Biol. 2010, 8, e1000352. [Google Scholar] [CrossRef] [Green Version]
- Toole, C.; Martinez-Juárez, I.E.; Gaitanis, J.N.; Blum, A.; Sunderam, S.; Ding, L.; DiCecco, J.; Besio, W.G. Source localization of high-frequency activity in tripolar electroencephalography of patients with epilepsy. Epilepsy Behav. 2019, 101, 106519. [Google Scholar] [CrossRef]
- Uchida, D.; Fujimoto, A.; Yamazoe, T.; Yamamoto, T.; Enoki, H. Seizure frequency can be reduced by changing intracranial pressure: A case report in drug-resistant epilepsy. Epilepsy Behav. Case Rep. 2018, 10, 14–17. [Google Scholar] [CrossRef] [PubMed]
- Verkhratsky, A.; Krishtal, O.; Petersen, O. From Galvani to patch clamp: The development of electrophysiology. Eur. J. Physiol. 2006, 453, 233–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonato, P. Wearable sensors/systems and their impact on biomedical engineering. IEEE Eng. Med. Biol. Mag. 2003, 22, 18–20. [Google Scholar] [CrossRef] [PubMed]
- Ryoo, D.W.; Kim, Y.S.; Lee, J.W. Wearable systems for service based on physiological signals. In Proceedings of the 2005 IEEE Engineering in Medicine and Biology 27th Annual Conference, Shanghai, China, 17–18 January 2006. [Google Scholar]
- Grasso, A.D.; Marano, D.; Palumbo, G.; Pennisi, S. Design methodology of subthreshold three-stage CMOS OTAs suitable for ultra-low-power low-area and high driving capability. IEEE Trans. Circuits Syst. Regul. Pap. 2015, 62, 1453–1462. [Google Scholar] [CrossRef]
- Li, Y.; Poon, C.C.; Zhang, Y.T. Analog integrated circuits design for processing physiological signals. IEEE Rev. Biomed. Eng. 2010, 3, 93–105. [Google Scholar] [CrossRef]
- Gibbs, F.A.; Davis, H. Changes in the human electroencephalogram associated with loss of consciousness. Am. J. Physiol. 1935, 113, 49–50. [Google Scholar]
- American Clinical Neurophysiology Society. Available online: https://www.acns.org/ (accessed on 11 June 2020).
- Engel, A.K.; Moll, C.K.; Fried, I.; Ojemann, G.A. Invasive recordings from the human brain: Clinical insights and beyond. Nat. Rev. Neurosci. 2005, 6, 35–47. [Google Scholar] [CrossRef]
- Lebedev, M.A.; Nicolelis, M.A. Brain–machine interfaces: Past, present and future. Trends Neurosci. 2006, 29, 536–546. [Google Scholar] [CrossRef]
- Schwartz, A.B.; Cui, X.T.; Weber, D.J.; Moran, D.W. Brain-controlled interfaces: Movement restoration with neural prosthetics. Neuron 2006, 52, 205–220. [Google Scholar] [CrossRef] [Green Version]
- Hochberg, L.R.; Serruya, M.D.; Friehs, G.M.; Mukand, J.A.; Saleh, M.; Caplan, A.H.; Branner, A.; Chen, D.; Penn, R.D.; Donoghue, J.P. Neuronal ensemble control of prosthetic devices by a human with tetraplegia. Nature 2006, 442, 164–171. [Google Scholar] [CrossRef]
- Viswam, V.; Chen, Y.; Shadmani, A.; Dragas, J.; Bounik, R.; Milos, R.; Müller, J.; Hierlemann, A. 2048 action potential recording channels with 2.4 μVrms noise and stimulation artifact suppression. In Proceedings of the 2016 IEEE Biomedical Circuits and Systems Conference (BioCAS), Shanghai, China, 17–19 October 2016. [Google Scholar]
- Chandrakumar, H.; Marković, D. A High Dynamic-Range Neural Recording Chopper Amplifier for Simultaneous Neural Recording and Stimulation. IEEE J. Solid-State Circuits 2017, 52, 645–656. [Google Scholar] [CrossRef]
- Burkhard, P.R.; Vingerhoets, F.; Berney, A.; Bogousslavsky, J.; Villemure, J.G.; Ghika, J. Suicide after successful deep brain stimulation for movement disorders. Neurology 2004, 63, 2170–2172. [Google Scholar] [CrossRef] [PubMed]
- Heldman, D.A.; Wang, W.; Chan, S.S.; Moran, D.W. Local field potential spectral tuning in motor cortex during reaching. IEEE Trans. Neural Syst. Rehabil. Eng. 2006, 14, 180–183. [Google Scholar] [CrossRef] [PubMed]
- Ward, M.P.; Rajdev, P.; Ellison, C.; Irazoqui, P.P. Toward a comparison of microelectrodes for acute and chronic recordings. Brain Res. 2009, 1282, 183–200. [Google Scholar] [CrossRef] [PubMed]
- Millett, D.; Coutin-Churchman, P.; Stern, J. Basic Principles of Electroencephalography. Neurosci. Biobehav. Psychol. 2015, 1, 75–80. [Google Scholar] [CrossRef]
- Srinivasan, R.; Nunez, P. Electroencephalography. Encyclopedia of Human Behavior, 2nd ed.; Elsevier: Amsterdam, The Netherslands, 2012; pp. 15–23. [Google Scholar] [CrossRef] [Green Version]
- Im, C.; Seo, J. A review of electrodes for the electrical brain signal recording. Biomed. Eng. Lett. 2016, 6, 104–112. [Google Scholar] [CrossRef]
- Parvizi, J.; Kastner, S. Promises and limitations of human intracranial electroencephalography. Nat. Neurosci. 2018, 21, 474–483. [Google Scholar] [CrossRef]
- Shokoueinejad, M.; Park, D.W.; Jung, Y.; Brodnick, S.; Novello, J.; Dingle, A.; Swanson, K.; Baek, D.H.; Suminski, A.; Lake, W.; et al. Progress in the Field of Micro-Electrocorticography. Micromachines 2019, 10, 62. [Google Scholar] [CrossRef] [Green Version]
- Volkova, K.; Lebedev, M.A.; Kaplan, A.; Ossadtchi, A. Decoding Movement From Electrocorticographic Activity: A Review. Front. Neuroinform. 2019, 13, 74. [Google Scholar] [CrossRef] [Green Version]
- Badi, A.; Kertesz, T.; Gurgel, R.; Shelton, C.; Normann, R. Development of a novel eighth-nerve intraneural auditory neuroprosthesis. Laryngoscope 2003, 5. [Google Scholar] [CrossRef]
- Bundy, D.T.; Zellmer, E.; Gaona, C.M.; Sharma, M.; Szrama, N.; Hacker, C.; Freudenburg, Z.V.; Daitch, A.; Moran, D.W.; Leuthardt, E.C. Characterization of the effects of the human dura on macro- and micro-electrocorticographic recordings. J. Neural Eng. 2014, 11, 016006. [Google Scholar] [CrossRef] [Green Version]
- Wang, M.; Guo, L. Intracortical Electrodes. In Neural Interface Engineering: Linking the Physical World and the Nervous System; Springer: New York, NY, USA, 2020; pp. 67–94. [Google Scholar]
- NeuroNexus. Available online: https://neuronexus.com/ (accessed on 2 September 2020).
- Cagnan, H.; Denison, T.; McIntyre, C. Emerging technologies for improved deep brain stimulation. Nat. Biotechnol. 2019, 37, 1024–1033. [Google Scholar] [CrossRef] [PubMed]
- DIXI Medical. Available online: http://www.diximedical.com/ (accessed on 11 June 2020).
- Salam, M.T.; Velazquez, J.L.P.; Genov, R. Seizure suppression efficacy of closed-loop versus open-loop deep brain stimulation in a rodent model of epilepsy. IEEE Trans. Neural Syst. Rehabil. Eng. 2016, 24, 710–719. [Google Scholar] [CrossRef] [PubMed]
- EaglePicher Technologies. Available online: https://www.eaglepicher.com/ (accessed on 11 June 2020).
- Schachter, S.; Schmidt, D. Epilepsy: Problem Solving in Clinical Practice; CRC Press: Boca Raton, FL, USA, 2000; p. 448. [Google Scholar]
- Cyberonics Inc. Available online: https://www.cyberonics.com/ (accessed on 11 June 2020).
- Fogel, B.S.; Greenberg, D.B. Psychiatric Care of the Medical Patient; Oxford University Press: Oxford, UK, 2015; p. 505. [Google Scholar]
- Sackeim, H.A.; Rush, A.J.; George, M.S.; Marangell, L.B.; Husain, M.M.; Nahas, Z.; Johnson, C.R.; Seidman, S.; Giller, C.; Haines, S.; et al. Vagus nerve stimulation (VNST) for treatment-resistant depression: Efficacy, side effects, and predictors of outcome. Neuropsychopharmacology 2001, 25, 713–728. [Google Scholar] [CrossRef] [Green Version]
- Labiner, D.M.; Ahern, G.L. Vagus nerve stimulation therapy in depression and epilepsy: Therapeutic parameter settings. Acta Neurol. Scand. 2007, 115, 23–33. [Google Scholar] [CrossRef] [PubMed]
- Boon, P.; Vonck, K.; van Rijckevorsel, K.; El Tahry, R.; Elger, C.E.; Mullatti, N.; Schulze-Bonhage, A.; Wagner, L.; Diehl, B.; Hamer, H.; et al. A prospective, multicenter study of cardiac-based seizure detection to activate vagus nerve stimulation. Seizure 2015, 32, 52–61. [Google Scholar] [CrossRef]
- VNSTherapy, LivaNova. An Introduction to VNS Therapy. Available online: https://vnstherapy.co.uk/sites/vnstherapy.com/files/vns-therapy-patient-brochure_1.pdf (accessed on 7 October 2020).
- RNS System User Maual. Available online: https://www.neuropace.com/wp-content/uploads/2015/11/PDMSManual.pdf (accessed on 7 October 2020).
- Thomas, G.P.; Jobst, B.C. Critical review of the responsive neurostimulator system for epilepsy. Med. Devices 2015, 8, 405. [Google Scholar]
- Sun, F.T.; Morrell, M.J. Closed-loop neurostimulation: The clinical experience. Neurotherapeutics 2014, 11, 553–563. [Google Scholar] [CrossRef] [Green Version]
- Bergey, G.K.; Morrell, M.J.; Mizrahi, E.M.; Goldman, A.; King-Stephens, D.; Nair, D.; Srinivasan, S.; Jobst, B.; Gross, R.E.; Shields, D.C.; et al. Long-term treatment with responsive brain stimulation in adults with refractory partial seizures. Neurology 2015, 84, 1210–1212. [Google Scholar] [CrossRef]
- Medtronic Inc. Available online: https://www.medtronic.com/ (accessed on 11 June 2020).
- Medtronic Activa PC, Implant Manual; Medtronic. 2008. Available online: http://manuals.medtronic.com (accessed on 7 October 2020).
- Carlson, C. Epilepsy Treatment Stimulus Package? Deep Brain Stimulation in Treatment-Resistant Focal Epilepsy. Epilepsy Curr. 2010, 10, 148–150. [Google Scholar] [CrossRef] [Green Version]
- Yap, J.Y.Y.; Keatch, C.; Lambert, E.; Woods, W.; Stoddart, P.R.; Kameneva, T. Critical Review of Transcutaneous Vagus Nerve Stimulation: Challenges for Translation to Clinical Practice. Front. Neurosci. 2020, 14, 284. [Google Scholar] [CrossRef] [PubMed]
- Rong, P.J.; Fang, J.L.; Wang, L.P.; Meng, H.; Liu, J.; Ma, Y.g.; Ben, H.; Li, L.; Liu, R.P.; Huang, Z.X.; et al. Transcutaneous vagus nerve stimulation for the treatment of depression: A study protocol for a double blinded randomized clinical trial. BMC Complement. Altern. Med. 2012, 12, 255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stefan, H.; Kreiselmeyer, G.; Kerling, F.; Kurzbuch, K.; Rauch, C.; Heers, M.; Kasper, B.S.; Hammen, T.; Rzonsa, M.; Pauli, E.; et al. Transcutaneous vagus nerve stimulation (t-VNS) in pharmacoresistant epilepsies: A proof of concept trial. Epilepsia 2012, 53, e115–e118. [Google Scholar] [CrossRef] [PubMed]
- Cerbomed GmbH. Nemos, Vitos Devices. Available online: https://cerbomed.com/ (accessed on 11 June 2020).
- ElectroCore, Inc. Gammacore. Available online: https://www.gammacore.com/ (accessed on 11 June 2020).
- Soss, J.; Heck, C.; Murray, D.; Markovic, D.; Oviedo, S.; Corrale-Leyva, G.; Gordon, S.; Kealey, C.; DeGiorgio, C. A prospective long-term study of external trigeminal nerve stimulation for drug-resistant epilepsy. Epilepsy Behav. 2015, 42, 44–47. [Google Scholar] [CrossRef] [PubMed]
- NeuroSigma, Inc. Available online: http://www.neurosigma.com/ (accessed on 11 June 2020).
- SmartMonitor. Available online: https://smart-monitor.com/ (accessed on 11 June 2020).
- Benedek, M.; Kaernbach, C. A continuous measure of phasic electrodermal activity. J. Neurosci. Methods 2010, 190, 80–91. [Google Scholar] [CrossRef] [Green Version]
- Poh, M.Z.; Loddenkemper, T.; Reinsberger, C.; Swenson, N.C.; Goyal, S.; Madsen, J.R.; Picard, R.W. Autonomic changes with seizures correlate with postictal EEG suppression. Neurology 2012, 78, 1868–1876. [Google Scholar] [CrossRef] [Green Version]
- Onorati, F.; Regalia, G.; Caborni, C.; Picard, R. Improvement of a convulsive seizure detector relying on accelerometer and electrodermal activity collected continuously by a wristband. In Proceedings of the Epilepsy Pipeline Conference, San Francisco, CA, USA, 25–27 February 2016. [Google Scholar]
- Regalia, G.; Onorati, F.; Migliorini, M.; Picard, R. An Improved Wrist-worn Convulsive Seizure Detector based on Accelerometry and Electrodermal Activity Sensors, American Epilepsy Society Annual Meeting 2015. Available online: https://www.aesnet.org/meetings_events/annual_meeting_abstracts/view/2327131 (accessed on 11 June 2020).
- Empatica Inc. Available online: https://www.empatica.com/ (accessed on 11 June 2020).
- Sarkis, R.A.; Thome-Souza, S.; Poh, M.Z.; Llewellyn, N.; Klehm, J.; Madsen, J.R.; Picard, R.; Pennell, P.B.; Dworetzky, B.A.; Loddenkemper, T.; et al. Autonomic changes following generalized tonic clonic seizures: An analysis of adult and pediatric patients with epilepsy. Epilepsy Res. 2015, 115, 113–118. [Google Scholar] [CrossRef]
- Poppel, K.V.; Fulton, S.P.; McGregor, A.; Ellis, M.; Patters, A.; Wheless, J. Prospective study of the Emfit movement monitor. J. Child Neurol. 2013, 28, 1434–1436. [Google Scholar] [CrossRef]
- Harrison, R.R.; Charles, C. A low-power low-noise CMOS amplifier for neural recording applications. IEEE J. Solid-State Circuits 2003, 38, 958–965. [Google Scholar] [CrossRef]
- Tajalli, A.; Leblebici, Y. A widely-tunable and ultra-low-power MOSFET-C filter operating in subthreshold. In Proceedings of the 2009 IEEE Custom Integrated Circuits Conference, Rome, Italy, 13–16 September 2009. [Google Scholar]
- Ng, K.A.; Xu, Y.P. A compact, low input capacitance neural recording amplifier. IEEE Trans. Biomed. Circuits Syst. 2013, 7, 610–620. [Google Scholar] [CrossRef]
- Xu, J.; Yazicioglu, R.F.; Grundlehner, B.; Harpe, P.; Makinwa, K.A.; Van Hoof, C. A 160 muW 8-Channel Active Electrode System for EEG Monitoring. IEEE Trans. Biomed. Circuits Syst. 2011, 5, 555–567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verma, N.; Shoeb, A.; Bohorquez, J.; Dawson, J.; Guttag, J.; Chandrakasan, A.P. A micro-power EEG acquisition SoC with integrated feature extraction processor for a chronic seizure detection system. IEEE J. Solid-State Circuits 2010, 45, 804–816. [Google Scholar] [CrossRef]
- Gosselin, B.; Sawan, M.; Chapman, C.A. A low-power integrated bioamplifier with active low-frequency suppression. IEEE Trans. Biomed. Circuits Syst. 2007, 1, 184–192. [Google Scholar] [CrossRef] [PubMed]
- Yeager, D.; Biederman, W.; Narevsky, N.; Alon, E.; Rabaey, J. A fully-integrated 10.5 μw miniaturized (0.125 mm2) wireless neural sensor. In Proceedings of the 2012 Symposium on VLSI Circuits (VLSIC), Honolulu, HI, USA, 13–15 June 2012. [Google Scholar]
- Yazicioglu, R.F.; Merken, P.; Puers, R.; Van Hoof, C. A 200muW Eight-Channel EEG Acquisition ASIC for Ambulatory EEG Systems. IEEE J. Solid-State Circuits 2008, 43, 3025–3038. [Google Scholar] [CrossRef]
- Johnson, B.; Molnar, A. An orthogonal current-reuse amplifier for multi-channel sensing. IEEE J. Solid-State Circuits 2013, 48, 1487–1496. [Google Scholar] [CrossRef]
- Altaf, M.A.B.; Zhang, C.; Yoo, J. A 16-channel patient-specific seizure onset and termination detection soc with impedance-adaptive transcranial electrical stimulator. IEEE J. Solid-State Circuits 2015, 50, 2728–2740. [Google Scholar] [CrossRef]
- Tsai, Y.L.; Lee, F.W.; Chen, T.Y.; Lin, T.H. 5.3 A 2-channel- 83.2 dB crosstalk 0.061 mm2 CCIA with an orthogonal frequency chopping technique. In Proceedings of the 2015 IEEE International Solid-State Circuits Conference - (ISSCC) Digest of Technical Papers, San Francisco, CA, USA, 22–26 February 2015. [Google Scholar]
- Zhang, C.; Altaf, M.A.B.; Yoo, J. Design and implementation of an on-chip patient-specific closed-loop seizure onset and termination detection system. IEEE J. Biomed. Health Inf. 2016, 20, 996–1007. [Google Scholar] [CrossRef]
- Ranjandish, R.; Schmid, A. A Sub-μW/Channel, 16-Channel Seizure Detection and Signal Acquisition SoC Based on Multichannel Compressive Sensing. IEEE Trans. Circuits Syst. Express Briefs 2018, 65, 1400–1404. [Google Scholar] [CrossRef]
- Chen, F.; Chandrakasan, A.P.; Stojanovic, V.M. Design and analysis of a hardware-efficient compressed sensing architecture for data compression in wireless sensors. IEEE J. Solid-State Circuits 2012, 47, 744–756. [Google Scholar] [CrossRef] [Green Version]
- Ranjandish, R.; Ture, K.; Maloberti, F.; Dehollain, C.; Schmid, A. All Wireless, 16-Channel Epilepsy Control System with Sub-µW/Channel and Closed-Loop Stimulation Using a Switched-Capacitor-Based Active Charge Balancing Method. In Proceedings of the ESSCIRC 2018-IEEE 44th European Solid State Circuits Conference (ESSCIRC), Dresden, Germany, 3–6 September 2018. [Google Scholar]
- Sunderam, S. How to Detect and Quantify Epileptic Seizures. In EPILEPSY the Intersection of Neurosciences, Biology, Mathematics, Engineering, and Physics; CRC Press: Boca Raton, FL, USA, 2011; Chapter 10. [Google Scholar]
- Akter, M.S.; Islam, M.R.; Iimura, Y.; Sugano, H.; Fukumori, K.; Wang, D.; Tanaka, T.; Cichocki, A. Multiband entropy-based feature-extraction method for automatic identification of epileptic focus based on high-frequency components in interictal iEEG. Sci. Rep. 2020, 10. [Google Scholar] [CrossRef]
- Si, Y. FMachine learning applications for electroencephalograph signals in epilepsy: A quick review. Acta Epileptol. 2020, 2, 1–7. [Google Scholar] [CrossRef]
- Siddiqui, M.; Morales-Menendez, R.; Huang, X.; Hussain, N. Review of epileptic seizure detection using machine learning classifiers. Brain Inform. 2020, 7, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.; Nguyen, P.; Pham, N.; Bui, N.; Truong, H.; Ha, S.; Vu, T. Epileptic Seizure Detection and Experimental Treatment: A Review. Front. Neurol. 2020, 11, 701. [Google Scholar] [CrossRef] [PubMed]
- Rasheed, K.; Qayyum, A.; Qadir, J.; Sivathamboo, S.; Kwan, P.; Kuhlmann, L.; O’Brien, T.; Razi, A. Machine Learning for Predicting Epileptic Seizures Using EEG Signals: A Review. arXiv 2020, arXiv:2002.01925. [Google Scholar] [CrossRef]
- Raghunathan, S.; Gupta, S.K.; Markandeya, H.S.; Roy, K.; Irazoqui, P.P. A hardware-algorithm co-design approach to optimize seizure detection algorithms for implantable applications. J. Neurosci. Methods 2010, 193, 106–117. [Google Scholar] [CrossRef]
- Borton, D.A.; Yin, M.; Aceros, J.; Nurmikko, A. An implantable wireless neural interface for recording cortical circuit dynamics in moving primates. J. Neural Eng. 2013, 10, 026010. [Google Scholar] [CrossRef] [Green Version]
- IEEE Standard for Safety Levels with Respect to Human Exposure to Radio Frequency Electromagnetic Fields, 3 kHz to 300 GHz; IEEE Std C95.1-2005 (Revision of IEEE Std C95.1-1991); IEEE: Piscataway, NJ, USA, 2006; pp. 1–238. [CrossRef]
- Majidzadeh, V.; Schmid, A.; Leblebici, Y. Energy Efficient Low-Noise Neural Recording Amplifier With Enhanced Noise Efficiency Factor. IEEE Trans. Biomed. Circuits Syst. 2011, 5, 262–271. [Google Scholar] [CrossRef]
- Tran, N.; Bai, S.; Yang, J.; Chun, H.; Kavehei, O.; Yang, Y.; Muktamath, V.; Ng, D.; Meffin, H.; Halpern, M.; et al. A complete 256-electrode retinal prosthesis chip. IEEE J. Solid-State Circuits 2014, 49, 751–765. [Google Scholar] [CrossRef]
- Pittsburgh Plastics Manufacturing Inc. 8 Things to Know About Why Biocompatible Materials are Important in a Medical Device. Available online: http://www.pittsburghplastics.com/ (accessed on 11 June 2020).























© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ranjandish, R.; Schmid, A. A Review of Microelectronic Systems and Circuit Techniques for Electrical Neural Recording Aimed at Closed-Loop Epilepsy Control. Sensors 2020, 20, 5716. https://doi.org/10.3390/s20195716
Ranjandish R, Schmid A. A Review of Microelectronic Systems and Circuit Techniques for Electrical Neural Recording Aimed at Closed-Loop Epilepsy Control. Sensors. 2020; 20(19):5716. https://doi.org/10.3390/s20195716
Chicago/Turabian StyleRanjandish, Reza, and Alexandre Schmid. 2020. "A Review of Microelectronic Systems and Circuit Techniques for Electrical Neural Recording Aimed at Closed-Loop Epilepsy Control" Sensors 20, no. 19: 5716. https://doi.org/10.3390/s20195716
APA StyleRanjandish, R., & Schmid, A. (2020). A Review of Microelectronic Systems and Circuit Techniques for Electrical Neural Recording Aimed at Closed-Loop Epilepsy Control. Sensors, 20(19), 5716. https://doi.org/10.3390/s20195716