Sensor-Based Daily Physical Activity: Towards Prediction of the Level of Concern about Falling in Peripheral Neuropathy



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Clinical Measures
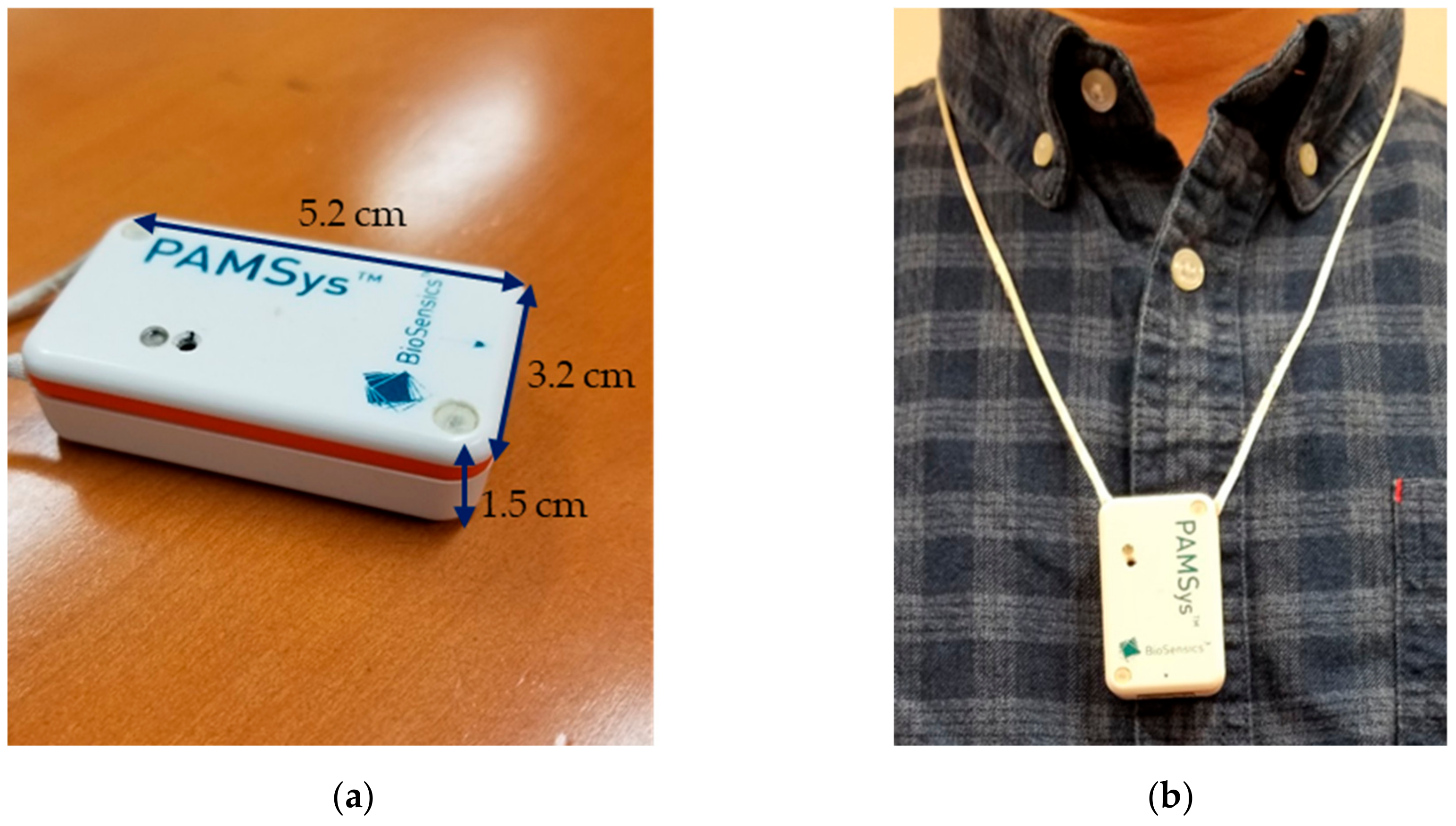
2.3. Sensor-Based Measures of Physical Activity
2.4. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics
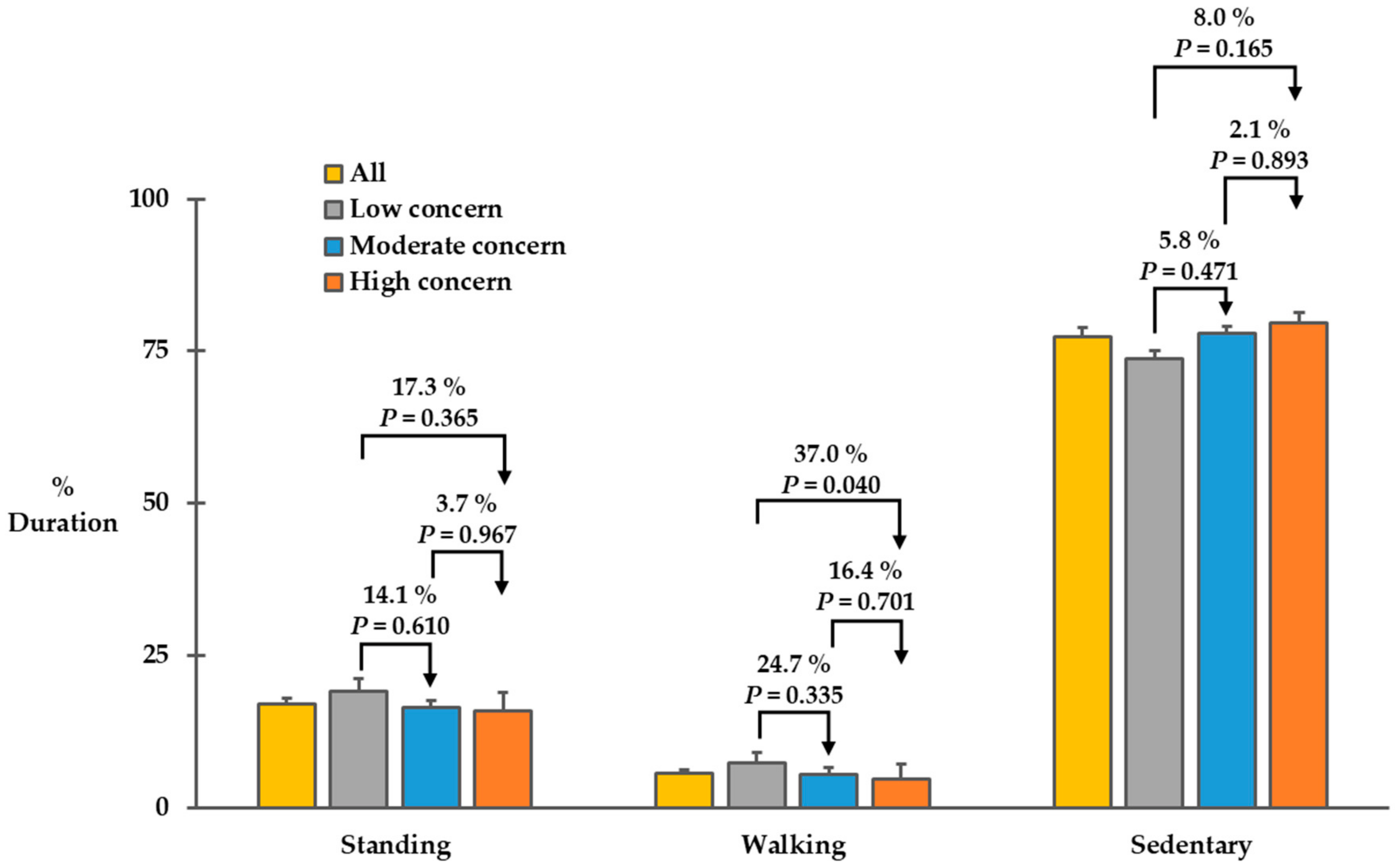
3.2. Physical Activity Characteristics
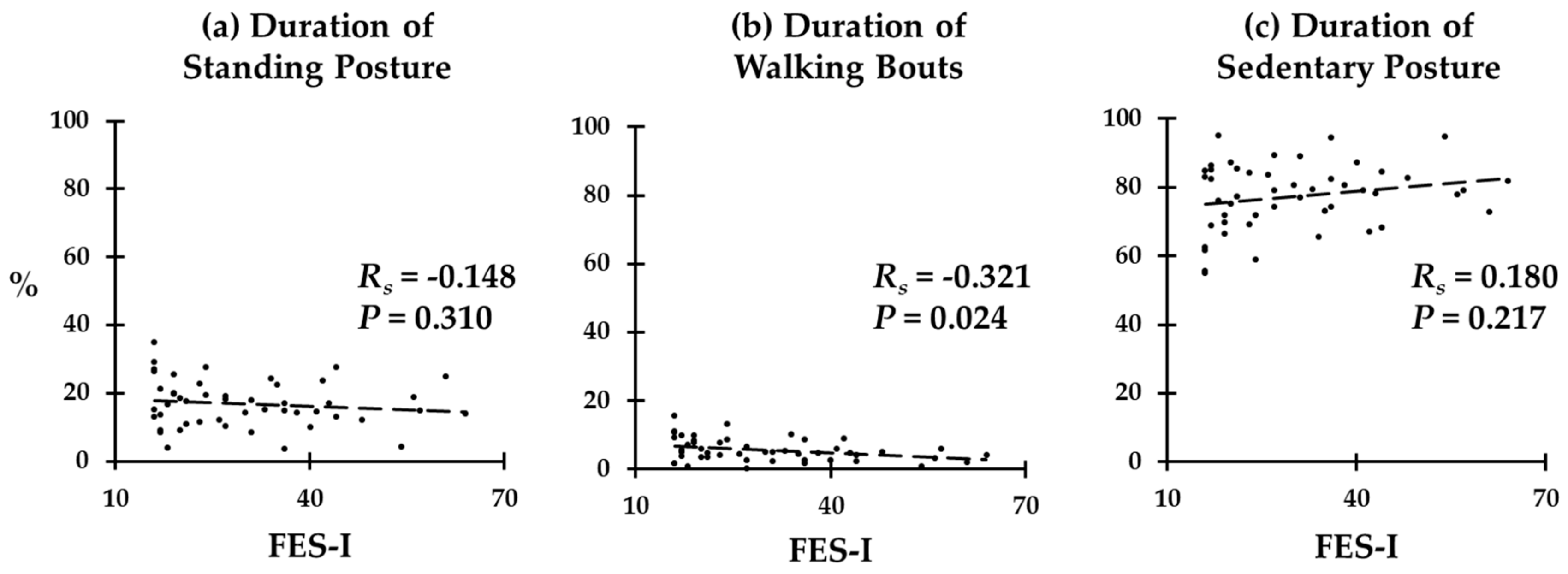
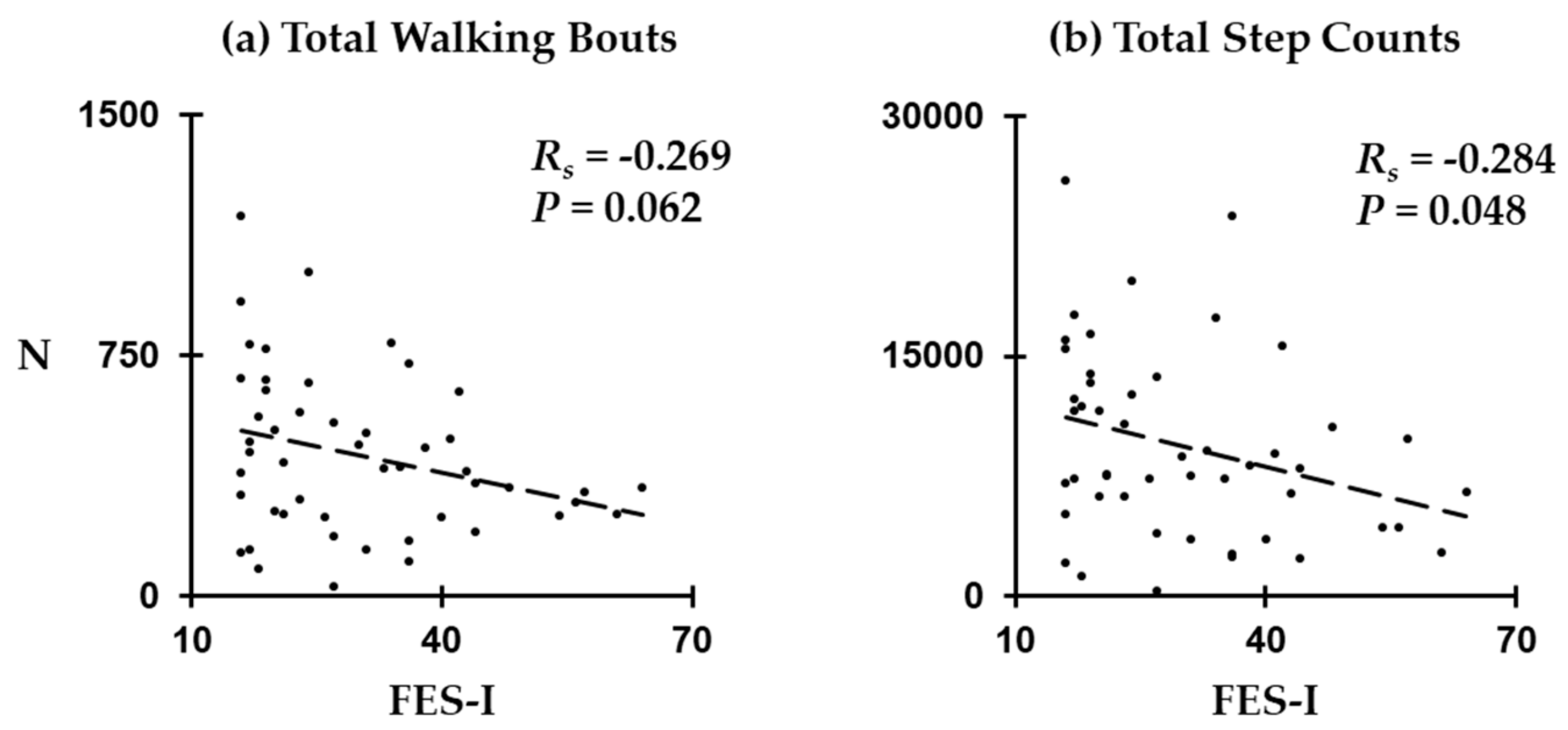
3.3. Correlations between FES-I Scores and Physical Activity Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- The Foundation for Peripheral Neuropathy. 2019. Available online: https://www.foundationforpn.org/what-is-peripheral-neuropathy/types-risk-factors/ (accessed on 30 November 2019).
- Richardson, J.K.; Hurvitz, E.A. Peripheral neuropathy: A true risk factor for falls. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 1995, 50, M211–M215. [Google Scholar] [CrossRef]
- Cavanagh, P.; Derr, J.; Ulbrecht, J.; Maser, R.; Orchard, T. Problems with gait and posture in neuropathic patients with insulin-dependent diabetes mellitus. Diabet. Med. 1992, 9, 469–474. [Google Scholar] [CrossRef]
- Kolb, N.A.; Smith, A.G.; Singleton, J.R.; Beck, S.L.; Stoddard, G.J.; Brown, S.; Mooney, K. The association of chemotherapy-induced peripheral neuropathy symptoms and the risk of falling. JAMA Neurol. 2016, 73, 860–866. [Google Scholar] [CrossRef] [Green Version]
- Vellas, B.J.; Wayne, S.J.; Romero, L.J.; Baumgartner, R.N.; Garry, P.J. Fear of falling and restriction of mobility in elderly fallers. Age Ageing 1997, 26, 189–193. [Google Scholar] [CrossRef] [Green Version]
- Yardley, L.; Smith, H. A prospective study of the relationship between feared consequences of falling and avoidance of activity in community-living older people. Gerontologist 2002, 42, 17–23. [Google Scholar] [CrossRef] [Green Version]
- Delbaere, K.; Crombez, G.; Vanderstraeten, G.; Willems, T.; Cambier, D. Fear-related avoidance of activities, falls and physical frailty. A prospective community-based cohort study. Age Ageing 2004, 33, 368–373. [Google Scholar] [CrossRef] [Green Version]
- Murphy, S.L.; Williams, C.S.; Gill, T.M. Characteristics associated with fear of falling and activity restriction in community-living older persons. J. Am. Geriatr. Soc. 2002, 50, 516–520. [Google Scholar] [CrossRef]
- Yardley, L.; Beyer, N.; Hauer, K.; Kempen, G.; Piot-Ziegler, C.; Todd, C. Development and initial validation of the Falls Efficacy Scale-International (FES-I). Age Ageing 2005, 34, 614–619. [Google Scholar] [CrossRef] [Green Version]
- Delbaere, K.; Close, J.C.; Mikolaizak, A.S.; Sachdev, P.S.; Brodaty, H.; Lord, S.R. The falls efficacy scale international (FES-I). A comprehensive longitudinal validation study. Age Ageing 2010, 39, 210–216. [Google Scholar] [CrossRef] [Green Version]
- Cumming, R.G.; Kelsey, J.L.; Nevitt, M.C. Methodologic issues in the study of frequent and recurrent health problems falls in the elderly. Ann. Epidemiol. 1990, 1, 49–56. [Google Scholar] [CrossRef]
- Ganz, D.A.; Higashi, T.; Rubenstein, L.Z. Monitoring falls in cohort studies of community-dwelling older people: Effect of the recall interval. J. Am. Geriatr. Soc. 2005, 53, 2190–2194. [Google Scholar] [CrossRef]
- Falck, R.S.; McDonald, S.M.; Beets, M.W.; Brazendale, K.; Liu-Ambrose, T. Measurement of physical activity in older adult interventions: A systematic review. Br. J. Sports Med. 2016, 50, 464–470. [Google Scholar] [CrossRef]
- Bruce, D.G.; Devine, A.; Prince, R.L. Recreational physical activity levels in healthy older women: The importance of fear of falling. J. Am. Geriatr. Soc. 2002, 50, 84–89. [Google Scholar] [CrossRef]
- Loprinzi, P.D.; Hager, K.K.; Ramulu, P.Y. Physical activity, glycemic control, and diabetic peripheral neuropathy: A national sample. J. Diabetes Complicat. 2014, 28, 17–21. [Google Scholar] [CrossRef]
- Tuttle, L.J.; Sinacore, D.R.; Cade, W.T.; Mueller, M.J. Lower physical activity is associated with higher intermuscular adipose tissue in people with type 2 diabetes and peripheral neuropathy. Phys. Ther. 2011, 91, 923–930. [Google Scholar] [CrossRef]
- Najafi, B.; Crews, R.T.; Wrobel, J.S. Importance of time spent standing for those at risk of diabetic foot ulceration. Diabetes Care 2010, 33, 2448–2450. [Google Scholar] [CrossRef] [Green Version]
- Muchna, A.; Najafi, B.; Wendel, C.S.; Schwenk, M.; Armstrong, D.G.; Mohler, J. Foot problems in older adults: Associations with incident falls, frailty syndrome, and sensor-derived gait, balance, and physical activity measures. J. Am. Podiatr. Med. Assoc. 2018, 108, 126–139. [Google Scholar] [CrossRef] [Green Version]
- Najafi, B.; Grewal, G.S.; Bharara, M.; Menzies, R.; Talal, T.K.; Armstrong, D.G. Can’t stand the pressure: The association between unprotected standing, walking, and wound healing in people with diabetes. J. Diabetes Sci. Technol. 2017, 11, 657–667. [Google Scholar] [CrossRef]
- Moyle, W.; Jones, C.; Murfield, J.; Draper, B.; Beattie, E.; Shum, D.; Thalib, L.; O’Dwyer, S.; Mervin, C.M. Levels of physical activity and sleep patterns among older people with dementia living in long-term care facilities: A 24-h snapshot. Maturitas 2017, 102, 62–68. [Google Scholar] [CrossRef] [Green Version]
- Marmeleira, J.; Ferreira, S.; Raimundo, A. Physical activity and physical fitness of nursing home residents with cognitive impairment: A pilot study. Exp. Gerontol. 2017, 100, 63–69. [Google Scholar] [CrossRef]
- Mc Ardle, R.; Del Din, S.; Donaghy, P.; Galna, B.; Thomas, A.; Rochester, L. Factors that influence habitual activity in mild cognitive impairment and dementia. Gerontology 2019, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Najafi, B.; Crews, R.T.; Wrobel, J.S. A novel plantar stimulation technology for improving protective sensation and postural control in patients with diabetic peripheral neuropathy: A double-blinded, randomized study. Gerontology 2013, 59, 473–480. [Google Scholar] [CrossRef] [PubMed]
- Kang, G.E.; Zahiri, M.; Lepow, B.; Saleem, N.; Najafi, B. The Effect of Daily Use of Plantar Mechanical Stimulation Through Micro-Mobile Foot Compression Device Installed in Shoe Insoles on Vibration Perception, Gait, and Balance in People With Diabetic Peripheral Neuropathy. J. Diabetes Sci. Technol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Najafi, B.; Talal, T.K.; Grewal, G.S.; Menzies, R.; Armstrong, D.G.; Lavery, L.A. Using plantar electrical stimulation to improve postural balance and plantar sensation among patients with diabetic peripheral neuropathy: A randomized double blinded study. J. Diabetes Sci. Technol. 2017, 11, 693–701. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.; Goel, R.; Rahemi, H.; Zhang, Q.; Lepow, B.; Najafi, B. Effectiveness of daily use of bilateral custom-made ankle-foot orthoses on balance, fear of falling, and physical activity in older adults: A randomized controlled trial. Gerontology 2019, 65, 299–307. [Google Scholar] [CrossRef]
- Zahiri, M.; Chen, K.M.; Zhou, H.; Nguyen, H.; Workeneh, B.T.; Yellapragada, S.V.; Sada, Y.H.; Schwenk, M.; Najafi, B. Using wearables to screen motor performance deterioration because of cancer and chemotherapy-induced peripheral neuropathy (CIPN) in adults-Toward an early diagnosis of CIPN. J. Geriatr. Oncol. 2019, 10, 960–967. [Google Scholar] [CrossRef] [Green Version]
- Rioul, O.; Vetterli, M. Wavelets and signal processing. IEEE Signal Process. Mag. 1991, 8, 14–38. [Google Scholar] [CrossRef] [Green Version]
- Najafi, B.; Aminian, K.; Paraschiv-Ionescu, A.; Loew, F.; Bula, C.J.; Robert, P. Ambulatory system for human motion analysis using a kinematic sensor: Monitoring of daily physical activity in the elderly. IEEE Trans. Biomed. Eng. 2003, 50, 711–723. [Google Scholar] [CrossRef]
- Najafi, B.; Aminian, K.; Loew, F.; Blanc, Y.; Robert, P.A. Measurement of stand-sit and sit-stand transitions using a miniature gyroscope and its application in fall risk evaluation in the elderly. IEEE Trans. Biomed. Eng. 2002, 49, 843–851. [Google Scholar] [CrossRef]
- Najafi, B.; Armstrong, D.G.; Mohler, J. Novel Wearable Technology for Assessing Spontaneous Daily Physical Activity and Risk of Falling in Older Adults with Diabetes; SAGE Publications: Los Angeles, CA, USA, 2013. [Google Scholar]
- Parvaneh, S.; Mohler, J.; Toosizadeh, N.; Grewal, G.S.; Najafi, B. Postural transitions during activities of daily living could identify frailty status: Application of wearable technology to identify frailty during unsupervised condition. Gerontology 2017, 63, 479–487. [Google Scholar] [CrossRef] [Green Version]
- Mohler, M.J.; Wendel, C.S.; Taylor-Piliae, R.E.; Toosizadeh, N.; Najafi, B. Motor performance and physical activity as predictors of prospective falls in community-dwelling older adults by frailty level: Application of wearable technology. Gerontology 2016, 62, 654–664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Razjouyan, J.; Naik, A.; Horstman, M.; Kunik, M.; Amirmazaheri, M.; Zhou, H.; Sharafkhaneh, A.; Najafi, B. Wearable sensors and the assessment of frailty among vulnerable older adults: An observational cohort study. Sensors 2018, 18, 1336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Najafi, B.; Reeves, N.D.; Armstrong, D.G. Leveraging smart technologies to improve the management of diabetic foot ulcers and extend ulcer-free days in remission. Diabetes Metab. Res. Rev. 2020, e3239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, G.E.; Zhou, H.; Varghese, V.; Najafi, B. Characteristics of the gait initiation phase in older adults with diabetic peripheral neuropathy compared to control older adults. Clin. Biomech. 2020, 72, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Richardson, J.K.; Ashton-Miller, J.A. Peripheral neuropathy: An often-overlooked cause of falls in the elderly. Postgrad. Med. 1996, 99, 161–172. [Google Scholar] [CrossRef] [PubMed]
- Horak, F.B. Postural orientation and equilibrium: What do we need to know about neural control of balance to prevent falls? Age Ageing 2006, 35, ii7–ii11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwenk, M.; Mohler, J.; Wendel, C.; Fain, M.; Taylor-Piliae, R.; Najafi, B. Wearable sensor-based in-home assessment of gait, balance, and physical activity for discrimination of frailty status: Baseline results of the Arizona frailty cohort study. Gerontology 2015, 61, 258–267. [Google Scholar] [CrossRef] [Green Version]
- Toosizadeh, N.; Joseph, B.; Heusser, M.R.; Jokar, T.O.; Mohler, J.; Phelan, H.A.; Najafi, B. Assessing upper-extremity motion: An innovative, objective method to identify frailty in older bed-bound trauma patients. J. Am. Coll. Surg. 2016, 223, 240–248. [Google Scholar] [CrossRef] [Green Version]
- Hornyak, V.; Brach, J.S.; Wert, D.M.; Hile, E.; Studenski, S.; VanSwearingen, J.M. What is the relation between fear of falling and physical activity in older adults? Arch. Phys. Med. Rehabil. 2013, 94, 2529–2534. [Google Scholar] [CrossRef] [Green Version]
- Tinetti, M.E.; De Leon, C.F.M.; Doucette, J.T.; Baker, D.I. Fear of falling and fall-related efficacy in relationship to functioning among community-living elders. J. Gerontol. 1994, 49, M140–M147. [Google Scholar] [CrossRef]
- Martin, F.C.; Hart, D.; Spector, T.; Doyle, D.V.; Harari, D. Fear of falling limiting activity in young-old women is associated with reduced functional mobility rather than psychological factors. Age Ageing 2005, 34, 281–287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deshpande, N.; Metter, E.J.; Lauretani, F.; Bandinelli, S.; Guralnik, J.; Ferrucci, L. Activity restriction induced by fear of falling and objective and subjective measures of physical function: A prospective cohort study. J. Am. Geriatr. Soc. 2008, 56, 615–620. [Google Scholar] [CrossRef] [PubMed]
- Stubbs, B.; Patchay, S.; Soundy, A.; Schofield, P. The avoidance of activities due to fear of falling contributes to sedentary behavior among community-dwelling older adults with chronic musculoskeletal pain: A multisite observational study. Pain Med. 2014, 15, 1861–1871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Powell, M.W.; Carnegie, D.H.; Burke, T.J. Reversal of diabetic peripheral neuropathy with phototherapy (MIRE™) decreases falls and the fear of falling and improves activities of daily living in seniors. Age Ageing 2005, 35, 11–16. [Google Scholar] [CrossRef] [Green Version]
- Doheny, E.P.; Walsh, C.; Foran, T.; Greene, B.R.; Fan, C.W.; Cunningham, C.; Kenny, R.A. Falls classification using tri-axial accelerometers during the five-times-sit-to-stand test. Gait Posture 2013, 38, 1021–1025. [Google Scholar] [CrossRef]
- Schoene, D.; Smith, S.T.; Davies, T.A.; Delbaere, K.; Lord, S.R. A Stroop Stepping Test (SST) using low-cost computer game technology discriminates between older fallers and nonfallers. Age Ageing 2013, 43, 285–289. [Google Scholar] [CrossRef] [Green Version]
- Ejupi, A.; Lord, S.R.; Delbaere, K. New methods for fall risk prediction. Curr. Opin. Clin. Nutr. Metab. Care 2014, 17, 407–411. [Google Scholar] [CrossRef]
- Mancini, M.; Schlueter, H.; El-Gohary, M.; Mattek, N.; Duncan, C.; Kaye, J.; Horak, F.B. Continuous monitoring of turning mobility and its association to falls and cognitive function: A pilot study. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2016, 71, 1102–1108. [Google Scholar] [CrossRef] [Green Version]
- Stone, E.E.; Skubic, M. Evaluation of an inexpensive depth camera for passive in-home fall risk assessment. In Proceedings of the 2011 5th International Conference on Pervasive Computing Technologies for Healthcare (PervasiveHealth) and Workshops, Dublin, Ireland, 23–26 May 2011; pp. 71–77. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Measures | All | Low | Moderate | High | p-Value * |
|---|---|---|---|---|---|
| Sample, N | 49 | 15 | 12 | 22 | - |
| Age, years | 68.5 ± 7.1 | 68.4 ± 7.5 | 67.3 ± 7.7 | 69.3 ± 6.8 | 0.666 |
| Women, N (%) | 21 (42.9%) | 5 (33.3%) | 4 (25.0%) | 13 (59.1%) | 0.106 |
| BMI, kg/m2 | 30.01 ± 5.83 | 30.18 ± 3.94 | 26.54 ± 4.08 | 31.79 ± 6.95 | 0.039 |
| FES-I, no unit | 30.1 ± 13.4 | 17.1 ± 1.2 | 23.6 ± 2.7 | 42.5 ± 10.1 | <0.001 |
| Falls, N † | 0.7 ± 1.1 | 0.1 ± 0.3 | 0.6 ± 1.0 | 1.1 ± 1.4 | 0.009 |
| Fallers, N † | 17 (34.7%) | 1 (6.7%) | 4 (33.3%) | 12 (54.5%) | 0.011 |
| VPT, volts | 27.5 ± 11.9 | 26.2 ± 12.3 | 26.6 ± 11.4 | 28.8 ± 12.4 | 0.796 |
| Measures, N | All | Low | Moderate | High | p-Value * |
|---|---|---|---|---|---|
| Total walking bouts | 440 ± 36 | 548 ± 79 | 417 ± 76 | 378 ± 38 | 0.119 |
| Total step counts | 9377 ± 826 | 11836 ± 1668 | 8990 ± 1462 | 7912 ± 1137 | 0.123 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, G.E.; Najafi, B. Sensor-Based Daily Physical Activity: Towards Prediction of the Level of Concern about Falling in Peripheral Neuropathy. Sensors 2020, 20, 505. https://doi.org/10.3390/s20020505
Kang GE, Najafi B. Sensor-Based Daily Physical Activity: Towards Prediction of the Level of Concern about Falling in Peripheral Neuropathy. Sensors. 2020; 20(2):505. https://doi.org/10.3390/s20020505
Chicago/Turabian StyleKang, Gu Eon, and Bijan Najafi. 2020. "Sensor-Based Daily Physical Activity: Towards Prediction of the Level of Concern about Falling in Peripheral Neuropathy" Sensors 20, no. 2: 505. https://doi.org/10.3390/s20020505
APA StyleKang, G. E., & Najafi, B. (2020). Sensor-Based Daily Physical Activity: Towards Prediction of the Level of Concern about Falling in Peripheral Neuropathy. Sensors, 20(2), 505. https://doi.org/10.3390/s20020505