Tracking and Characterization of Spinal Cord-Injured Patients by Means of RGB-D Sensors

 ,
,  ,
,  ,
, 

Abstract
:1. Introduction
2. State of the Art
3. Method
- Push: this occurs when the hands grab the wheelchair handrims and move the wheels forward.
- Recovery: this starts when the hands let the handrims go and finishes when the position of pushing is reached.
- Top center (TC): the hand reaches the top center position of the pushrim during the push.
- Initial contact (IC): the hand touches the pushrim to start the push.
- Hand off (HO): the hand leaves the pushrim and then the push finishes.
- End of follow through (End FT): the hand finishes going forward before starting the recovery movement.
- End of arm return (End AR): the recovery movement finishes before starting a new pushing cycle.
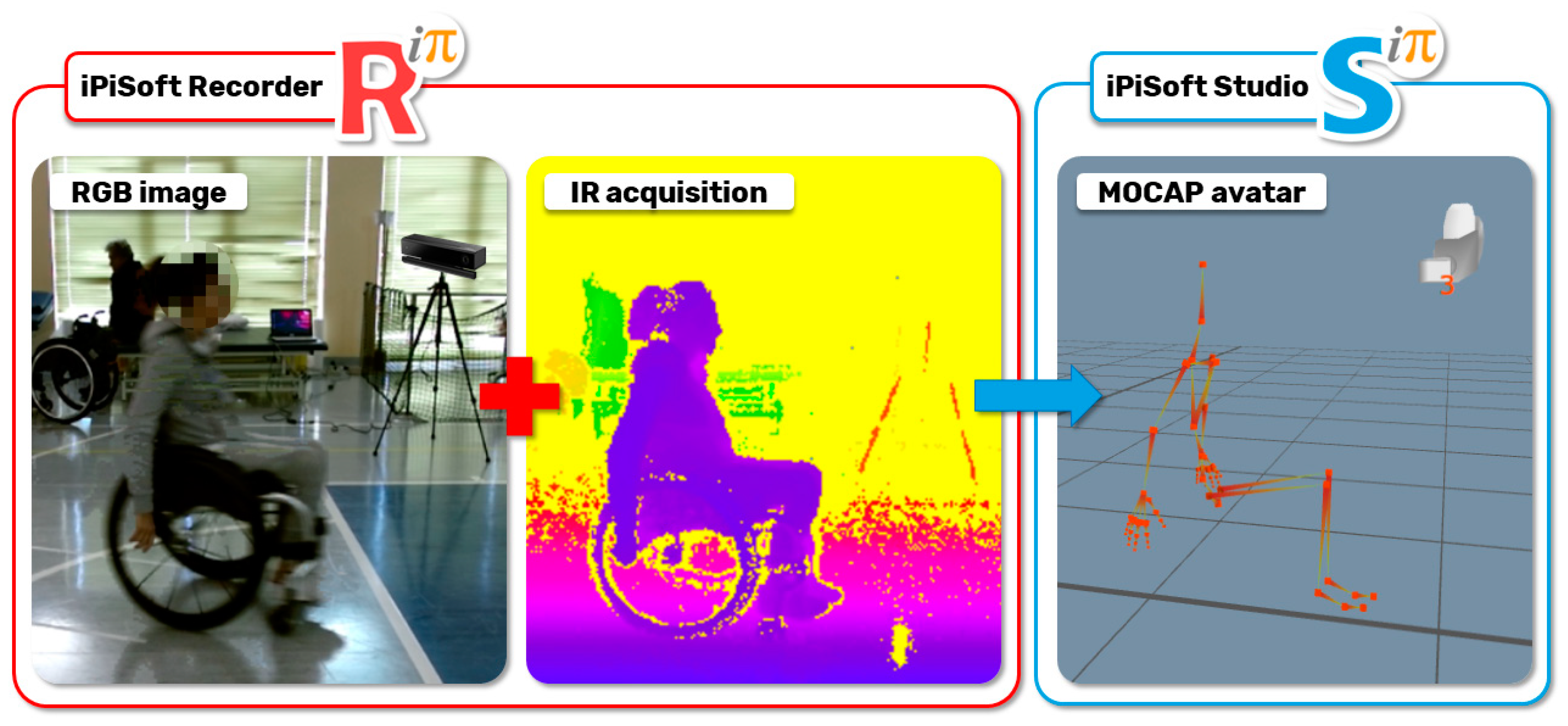
3.1. Phase 1: Mocap Acquisition
3.2. Phase 2: Data Extraction
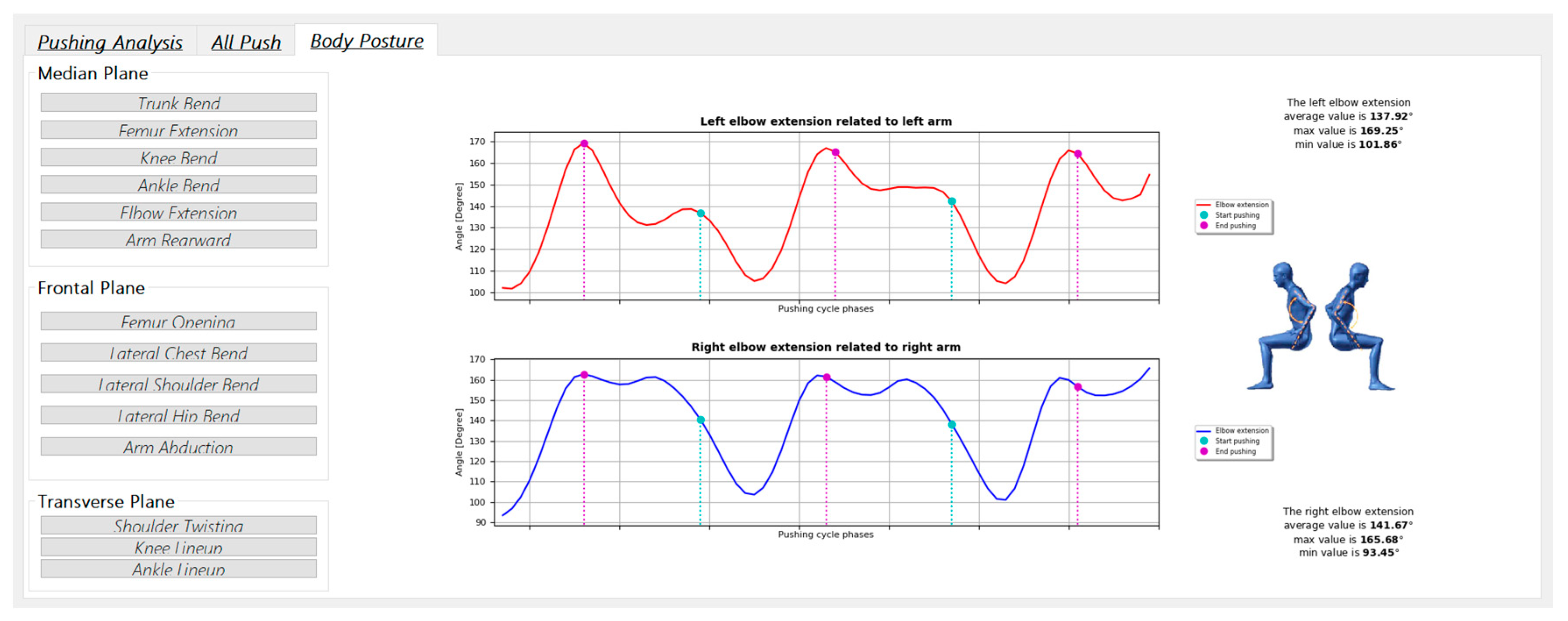
3.3. Phase 3: SCI-APP
- Computation of pushing analysis. This requires as input the kinematic data of the virtual skeleton to automatically detect all the instants relative to the beginning of both phases of the pushing cycle. It automatically checks if there are asymmetries between the left and the right pushing cycles.
- Data extrapolation of each pushing cycles. This makes available all the data of a specific pushing cycle. It is used to generate the graphs needed to compare the position of the hand with the position of the handrim and visually evaluates each type of pushing cycle.
- Measurements of specific patient movements. This computes the measurements of the human body articulations according to the medical reference system. The computed data are the linear and angular measurements described in Table 3.
- Generation of the medical reports. This permits us to automatically generate a report and save the computed data and measurements in a PDF or Excel file.
- Number of right and left pushing phases made by the patient during wheelchair propulsion.
- Length covered by the patient during the wheelchair propulsion.
- A warning when the application detects symmetry loss during one or more propulsion phases.
4. Campaign of Acquisition
5. Results and Discussion
5.1. Humeral Elevation
5.2. Horizontal Abduction of Humerus
5.3. Humeral Rotation
5.4. Elbow Flexion
5.5. Trunk Flexion/Extension
5.6. Final Considerations
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bickenbach, J.; Officer, A.; Shakespeare, T.; von Groote, P. International Perspectives on Spinal Cord Injury; World Health Organization: Geneva, Switzerland, 2013; ISBN 9789241564663. [Google Scholar]
- Kirshblum, S.C.; Burns, S.P.; Biering-Sorensen, F.; Donovan, W.; Graves, D.E.; Jha, A.; Johansen, M.; Jones, L.; Krassioukov, A.; Mulcahey, M.J.; et al. International standards for neurological classification of spinal cord injury (Revised 2011). J. Spinal Cord Med. 2011, 34, 535–546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kenny, S.; Gowran, R.J. Outcome measures for wheelchair and seating provision: A critical appraisal. Br. J. Occup. Ther. 2014, 77, 67–77. [Google Scholar] [CrossRef]
- Smith, E.M.; Low, K.; Miller, W.C. Interrater and intrarater reliability of the wheelchair skills test version 4.2 for power wheelchair users. Disabil. Rehabil. 2018, 40, 678–683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindquist, N.J.; Loudon, P.E.; Magis, T.F.; Rispin, J.E.; Kirby, R.L.; Manns, P.J. Reliability of the performance and safety scores of the wheelchair skills test version 4.1 for manual wheelchair users. Arch. Phys. Med. Rehabil. 2010, 91, 1752–1757. [Google Scholar] [CrossRef] [PubMed]
- Askari, S.; Kirby, R.L.; Parker, K.; Thompson, K.; O’Neill, J. Wheelchair propulsion test: Development and measurement properties of a new test for manual wheelchair users. Arch. Phys. Med. Rehabil. 2013, 94, 1690–1698. [Google Scholar] [CrossRef] [PubMed]
- Chow, J.W.; Millikan, T.A.; Carlton, L.G.; Chae, W.-S.; Lim, Y.-T.; Morse, M.I. Kinematic and Electromyographic Analysis of Wheelchair Propulsion on Ramps of Different Slopes for Young Men With Paraplegia. Arch. Phys. Med. Rehabil. 2009, 90, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Out-Front: The SmartWheel Clinical Tool. Available online: http://www.out-front.com/smartwheel_overview.php (accessed on 24 June 2020).
- Dellabiancia, F.; Porcellini, G.; Merolla, G. Instruments and techniques for the analysis of wheelchair propulsion and upper extremity involvement in patients with spinal cord injuries: Current concept review. Muscles Ligaments Tendons J. 2013, 3, 150–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vegter, R.J.K.; Hartog, J.; De Groot, S.; Lamoth, C.J.; Bekker, M.J.; Van Der Scheer, J.W.; Van Der Woude, L.H.V.; Veeger, D.H.E.J. Early motor learning changes in upper-limb dynamics and shoulder complex loading during handrim wheelchair propulsion. J. Neuroeng. Rehabil. 2015, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leving, M.T.; Horemans, H.L.D.; Vegter, R.J.K.; De Groot, S.; Bussmann, J.B.J.; van der Woude, L.H.V. Validity of consumer-grade activity monitor to identify manual wheelchair propulsion in standardized activities of daily living. PLoS ONE 2018, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Slikke, R.M.A.; Berger, M.A.M.; Bregman, D.J.J.; Lagerberg, A.H.; Veeger, H.E.J. Opportunities for measuring wheelchair kinematics in match settings; reliability of a three inertial sensor configuration. J. Biomech. 2015, 48, 3398–3405. [Google Scholar] [CrossRef] [PubMed]
- van der Slikke, R.M.A.; Berger, M.A.M.; Bregman, D.J.J.; Veeger, H.E.J. From big data to rich data: The key features of athlete wheelchair mobility performance. J. Biomech. 2016, 49, 3340–3346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boninger, M.L.; Souza, A.L.; Cooper, R.A.; Fitzgerald, S.G.; Koontz, A.M.; Fay, B.T. Propulsion patterns and pushrim biomechanics in manual wheelchair propulsion. Arch. Phys. Med. Rehabil. 2002, 83, 718–723. [Google Scholar] [CrossRef] [PubMed]
- OptiTrack—Motion Capture Systems. Available online: https://optitrack.com/ (accessed on 24 June 2020).
- Newsam, C.J.; Rao, S.S.; Mulroy, S.J.; Gronley, J.K.; Bontrager, E.L.; Perry, J. Three dimensional upper extremity motion during manual wheelchair propulsion in men with different levels of spinal cord injury. Gait Posture 1999, 10, 223–232. [Google Scholar] [CrossRef]
- Rammer, J.; Slavens, B.; Krzak, J.; Winters, J.; Riedel, S.; Harris, G. Assessment of a markerless motion analysis system for manual wheelchair application. J. Neuroeng. Rehabil. 2018, 15. [Google Scholar] [CrossRef] [PubMed]
- Vitali, A.; Regazzoni, D.; Rizzi, C. Digital motion acquisition to assess spinal cord injured (SCI) patients. Comput. Aided. Des. Appl. 2019, 16, 962–971. [Google Scholar] [CrossRef]
- Regazzoni, D.; Vitali, A.; Rizzi, C.; Colombo, G. A Method to Analyse Generic Human Motion With Low-Cost Mocap Technologies. In Proceedings of the International Design Engineering Technical Conferences and Computers and Information in Engineering Conference, Quebec City, QC, Canada, 26–29 August 2018. [Google Scholar]
- Regazzoni, D.; Vitali, A.; Rizzi, C.; Colombo Zefinetti, F. Motion Capture and Data Elaboration to Analyse Wheelchair Set-Up and Users’ Performance. In Proceedings of the International Mechanical Engineering Congress and Exposition, Pittsburgh, PA, USA, 9–15 November 2018. [Google Scholar]
- Galna, B.; Barry, G.; Jackson, D.; Mhiripiri, D.; Olivier, P.; Rochester, L. Accuracy of the Microsoft Kinect sensor for measuring movement in people with Parkinson’s disease. Gait Posture 2014, 39, 1062–1068. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vicon|Award Winning Motion Capture Systems. Available online: https://www.vicon.com/ (accessed on 24 June 2020).
- Milgrom, R.; Foreman, M.; Standeven, J.; Engsberg, J.R.; Morgan, K.A. Reliability and validity of the Microsoft Kinect for assessment of manual wheelchair propulsion. J. Rehabil. Res. Dev. 2016, 53, 901–918. [Google Scholar] [CrossRef] [PubMed]
- Motion Capture Camera & Software Leader|Motion Analysis Corporation. Available online: https://www.motionanalysis.com/ (accessed on 24 June 2020).
- iPi Soft- Markerless Motion Capture. Available online: http://ipisoft.com/ (accessed on 22 September 2020).
- Qt|Cross-Platform Software Development for Embedded & Desktop. Available online: https://www.qt.io/ (accessed on 22 September 2020).
- Otte, K.; Kayser, B.; Mansow-Model, S.; Verrel, J.; Paul, F.; Brandt, A.U.; Schmitz-Hübsch, T. Accuracy and reliability of the kinect version 2 for clinical measurement of motor function. PLoS ONE 2016, 11. [Google Scholar] [CrossRef] [PubMed]
- Stephens, C.L.; Engsberg, J.R. Comparison of overground and treadmill propulsion patterns of manual wheelchair users with tetraplegia. Disabil. Rehabil. Assist. Technol. 2010, 5, 420–427. [Google Scholar] [CrossRef] [PubMed]
- Kwarciak, A.M.; Turner, J.T.; Guo, L.; Richter, W.M. Comparing handrim biomechanics for treadmill and overground wheelchair propulsion. Spinal Cord 2010, 49, 457–462. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Plane Considered | Human Articulation Requested | Position/Movement | Biomechanics Joint Analyzed |
|---|---|---|---|
| Median Plane | Trunk Flection |  | It contributes to determining the patient stability during wheelchair propulsion. As the angle decreases, the stability increases, but over a threshold angle the wheelchair can overturn during the pushing phase. |
| Median Plane | Humeral Elevation |  | The humeral elevation describes the rotation of the shoulder along the median plane during the propulsion of the wheelchair. |
| Median Plane | Humeral Rotation |  | The humeral rotation is the rotation around the axes of the humerus. |
| Transverse Plane | Humeral Horizontal Abduction |  | The horizontal abduction of the humerus describes the rotation of the shoulder around the transverse plane during the propulsion of the wheelchair. |
| Median Plane | Elbow Flexion/Extension |  | The maximum and minimum values of this angle have to stay in an optimum range in order to prevent a problem with the elbow articulation. This angle depends on the seat translation compared to the wheel rotation axle. Right and left angles are compared to assess the symmetric propulsion. |
| To Do List for SCI Patients’ Acquisitions | ||||
|---|---|---|---|---|
 | ||||
| LAYOUT | To repeat once a day | 1.1 | Lay out the three-vertex carpet | |
| 1.2 | Check Kinect 1.20 m in height | |||
| 1.3 | Check Kinect horizontal inclination of −13° | |||
| 1.4 | Check vertical orientation of Kinect RGB camera field of view | |||
| 1.5 | Check ambient light source to darken (windows, lamps) | |||
| 1.6 | Check Kinect - PC USB cable link | |||
| 1.7 | Check ethernet cable link | |||
| 1.8 | Setup iPi Soft Recorder Master and Slaves computers | |||
| 1.9 | Setup new folder of the acquisition day “YYYY-MM-DD” | |||
| CALIBRATION 120 [sec] | To repeat for each calibration approx. every 30 min | 2.1 | Background iPi Soft Recorder 10 sec (with carpet on the floor), the Kinect field of view must be without anyone | |
| 2.2 | Setup Kinect with glass filter | |||
| 2.3 | Spiral movements with light marker + Recording using iPi Soft Recorder | |||
| 2.4 | Delete PC slave videos -> Button “Merge video” in iPi Soft Recorder | |||
| 2.5 | Calibration using iPi Soft Studio | |||
| 2.6 | Take off glass filter from Kinect | |||
| 2.7 | Take off carpet from the floor | |||
| 2.8 | Background iPi Soft Recorder 10 [sec] (without carpet on the floor), the Kinect field of view must be without anyone | |||
| VIDEO RECORDING | To repeat for each patient | 3.1 | Setup new patient’s folder “No. - Patient Surname” | |
| 3.2 | Change folder directory in iPi Soft Recorder | |||
| To repeat for each acquisition | 3.3 | Registration using iPi Soft Recorder | ||
| 3.4 | Delete PC slave videos -> Button “Merge video” in iPi Soft Recorder | |||
| Human Articulation | Data and Information | Virtual Joints and Segments | |
|---|---|---|---|
| Elbow Flection | Joints | Lower spine, neck. |  |
| Angle [°] | X-axis rotations. | ||
| Description | The bending of the trunk is measured as the angle between the vertical line and the segment passing between the lower spine and neck. | ||
| Humeral Elevation | Joints | R/L shoulder, R/L forearm. |  |
| Angle [°] | X-axis rotations. | ||
| Description | The humeral elevation is measured as the rotation of the shoulder joint around the X-axis. | ||
| Humeral Rotation | Joints | R/L shoulder. |  |
| Angle [°] | X-axis rotations. | ||
| Description | The humeral rotation is measured as the rotation of the shoulder joint around the axis defined as the vector between the shoulder position and the forearm position. | ||
| Humeral Horizontal Abduction | Joints | R/L shoulder, R/L forearm. |  |
| Angle [°] | Y-axis rotations. | ||
| Description | The humeral horizontal abduction is measured as the rotation of the shoulder joint around the X-axis. | ||
| Elbow Flexion/Extension | Joints | L/R forearm. |  |
| Angle [°] | X-axis rotations. | ||
| Description | During the propulsion phase, the angles considered have periodic movements. Max and min extensions are significant data by which to assess the upper limbs’ performance. | ||
| Humeral Elevation | IC | TC | HO | End FT | End AR | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Avg. | St.D. | Avg. | St.D. | Avg. | St.D. | Avg. | St.D. | Avg. | St.D. | |
| Low paraplegic (Ref. Val.) | 55.1 | 4.4 | 48.8 | 4.3 | 24.2 | 4.6 | 22.1 | 3.9 | 56.9 | 4.7 |
| Low paraplegic (Sci App) | 52.0 | 7.3 | 46.7 | 8.2 | 16.7 | 15.1 | 11.8 | 6.5 | 54.3 | 9.1 |
| Δ | −3.1 | −2.1 | −7.5 | −10.3 | −2.6 | |||||
| High paraplegic (Ref. Val.) | 53.8 | 7.8 | 47.1 | 7.9 | 23.7 | 4.3 | 22.1 | 4.0 | 55.7 | 7.2 |
| High paraplegic (Sci App) | 51.3 | 8.7 | 45.7 | 10.4 | 17.2 | 14.7 | 10.0 | 8.7 | 50.5 | 10.2 |
| Δ | −2.5 | −1.4 | −6.5 | −12.1 | −5.2 | |||||
| C7-tetraplegic (Ref. Val.) | 49.0 | 8.9 | 42.6 | 9.7 | 22.1 | 4.4 | 21.5 | 4.2 | 52.5 | 7.9 |
| C7-tetraplegic (Sci App) | 44.8 | 6.9 | 37.7 | 6.8 | 7.8 | 6.6 | 10.9 | 8.5 | 43.4 | 8.9 |
| Δ | −4.2 | −4.9 | −14.3 | −10.6 | −9.1 | |||||
| C6-tetraplegic (Ref. Val.) | 45.4 | 8.3 | 41.1 | 9.2 | 23.8 | 6.9 | 21.6 | 5.5 | 49.5 | 8.0 |
| C6-tetraplegic (Sci App) | 41.3 | 6.8 | 38.6 | 5.3 | 15.0 | 9.4 | 13.8 | 5.7 | 40.8 | 5.5 |
| Δ | −4.1 | −2.5 | −8.8 | −7.8 | −8.7 | |||||
| Horizontal Abduction | IC | TC | HO | End FT | End AR | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Avg. | St.D. | Avg. | St.D. | Avg. | St.D. | Avg. | St.D. | Avg. | St.D. | |
| Low paraplegic (Ref. Val.) | −53.6 | 8.1 | −41.8 | 8.5 | 6.8 | 12.5 | 21.8 | 14.8 | −55.3 | 8.3 |
| Low paraplegic (Sci Lab) | −51.7 | 10.1 | −46.7 | 10.8 | −13.9 | 21.1 | 22.8 | 18.8 | −51.2 | 10.2 |
| Δ | 1.9 | −4.9 | −20.7 | 1.0 | 4.1 | |||||
| High paraplegic (Ref. Val.) | −55.5 | 8.9 | −44.8 | 6.8 | 0.8 | 20.7 | 15.6 | 24.0 | −56.5 | 8.8 |
| High paraplegic (Sci Lab) | −54.2 | 9.1 | −46.4 | 9.2 | −18.2 | 18.1 | 15.1 | 18.4 | −52.1 | 8.8 |
| Δ | 1.3 | −1.6 | −19.0 | −0.5 | 4.4 | |||||
| C7-tetraplegic (Ref. Val.) | −58.3 | 7.7 | −48.8 | 6.8 | 8.6 | 17.9 | 19.6 | 21.1 | −59.3 | 6.7 |
| C7-tetraplegic (Sci Lab) | −59.2 | 8.3 | −52.8 | 10.2 | −5.4 | 20.3 | 23.4 | 18.7 | −57.0 | 6.1 |
| Δ | −0.9 | −4.0 | −14.0 | 3.8 | 2.3 | |||||
| C6-tetraplegic (Ref. Val.) | −54.6 | 8.4 | −43.5 | 13.3 | 8.2 | 14.2 | 9.9 | 15.4 | −55.1 | 8.4 |
| C6-tetraplegic (Sci Lab) | −56.2 | 8.3 | −51.1 | 7.8 | −9.9 | 29.3 | 17.9 | 11.0 | −52.1 | 7.1 |
| Δ | −1.6 | −7.6 | −18.1 | 8.0 | 3.0 | |||||
| Humeral Rotation | IC | TC | HO | End FT | End AR | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Avg. | St.D. | Avg. | St.D. | Avg. | St.D. | Avg. | St.D. | Avg. | St.D. | |
| Low paraplegic (Ref. Val.) | 78.0 | 14.8 | 69.9 | 14.6 | 37.0 | 18.7 | 24.4 | 22.2 | 77.7 | 14.5 |
| Low paraplegic (Sci Lab) | 74.0 | 3.6 | 70.6 | 4.1 | 53.1 | 10.4 | 36.6 | 10.3 | 75.0 | 5.0 |
| Δ | −4.0 | 0.7 | 16.1 | 12.2 | −2.7 | |||||
| High paraplegic (Ref. Val.) | 75.6 | 14.5 | 67.8 | 14.4 | 35.5 | 26.4 | 22.4 | 31.6 | 76.0 | 14.2 |
| High paraplegic (Sci Lab) | 75.7 | 4.6 | 71.8 | 4.3 | 57.1 | 8.5 | 43.2 | 7.0 | 75.5 | 5.0 |
| Δ | 0.1 | 4.0 | 21.6 | 20.8 | −0.5 | |||||
| C7-tetraplegic (Ref. Val.) | 73.6 | 12.9 | 70.7 | 12.6 | 27.2 | 22.4 | 17.3 | 27.5 | 72.0 | 12.9 |
| C7-tetraplegic (Sci Lab) | 68.7 | 6.0 | 63.5 | 5.2 | 43.0 | 9.3 | 34.6 | 7.1 | 67.6 | 5.8 |
| Δ | −4.9 | −7.2 | 15.8 | 17.3 | −4.4 | |||||
| C6-tetraplegic (Ref. Val.) | 74.6 | 10.4 | 69.3 | 15.2 | 27.6 | 18.9 | 19.1 | 23.1 | 72.6 | 10.2 |
| C6-tetraplegic (Sci Lab) | 70.6 | 5.0 | 68.1 | 5.2 | 52.1 | 10.6 | 37.5 | 8.4 | 70.3 | 3.4 |
| Δ | −4.0 | −1.2 | 24.5 | 18.4 | −2.3 | |||||
| Elbow Flexion | IC | TC | HO | End FT | End AR | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Avg. | St.D. | Avg. | St.D. | Avg. | St.D. | Avg. | St.D. | Avg. | St.D | |
| Low paraplegic (Ref. Val.) | 59.4 | 10.9 | 76.4 | 8.9 | 43.1 | 9.8 | 34.8 | 9.0 | 54.3 | 9.8 |
| Low paraplegic (Sci Lab) | 68.2 | 12.0 | 72.7 | 10.1 | 58.1 | 19.0 | 33.6 | 13.2 | 64.4 | 15.1 |
| Δ | 8.8 | −3.7 | 15.0 | −1.2 | 10.1 | |||||
| High paraplegic (Ref. Val.) | 59.8 | 11.6 | 77.1 | 11.1 | 46.1 | 11.7 | 37.4 | 12.7 | 55.0 | 11.1 |
| High paraplegic (Sci Lab) | 64.2 | 12.7 | 74.0 | 9.5 | 63.8 | 14.8 | 41.8 | 12.3 | 57.5 | 15.1 |
| Δ | 4.4 | −3.1 | 17.7 | 4.4 | 2.5 | |||||
| C7-tetraplegic (Ref. Val.) | 65.5 | 8.1 | 77.1 | 8.1 | 42.4 | 10.1 | 35.4 | 10.1 | 62.9 | 9.2 |
| C7-tetraplegic (Sci Lab) | 62.9 | 12.4 | 72.7 | 6.3 | 51.7 | 14.7 | 35.6 | 11.8 | 55.9 | 17.5 |
| Δ | −2.6 | −4.4 | 9.3 | 0.2 | −7.0 | |||||
| C6-tetraplegic (Ref. Val.) | 62.8 | 10.0 | 69.8 | 10.7 | 42.8 | 9.3 | 41.8 | 9.3 | 61.3 | 10.6 |
| C6-tetraplegic (Sci Lab) | 60.9 | 15.0 | 71.3 | 10.0 | 54.0 | 15.5 | 33.4 | 10.8 | 58.2 | 14.4 |
| Δ | −1.9 | 1.5 | 11.2 | −8.4 | −3.1 | |||||
| Trunk Extension | IC | TC | HO | End FT | End AR | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Avg. | St.D. | Avg. | St.D. | Avg. | St.D. | Avg. | St.D. | Avg. | St.D | |
| Low paraplegic | −3.4 | 4.9 | −3.8 | 5.0 | −3.9 | 5.3 | −2.6 | 5.2 | −2.6 | 5.1 |
| High paraplegic | 0.0 | 7.7 | 0.0 | 7.8 | 0.1 | 6.8 | 0.9 | 6.3 | 0.3 | 7.1 |
| C7-tetraplegic | 0.7 | 9.4 | 0.0 | 9.1 | −0.9 | 8.7 | −0.9 | 8.8 | 0.9 | 8.9 |
| C6-tetraplegic | 12.4 | 5.1 | 11.0 | 5.0 | 9.1 | 5.1 | 9.6 | 5.5 | 12.4 | 5.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colombo Zefinetti, F.; Vitali, A.; Regazzoni, D.; Rizzi, C.; Molinero, G. Tracking and Characterization of Spinal Cord-Injured Patients by Means of RGB-D Sensors. Sensors 2020, 20, 6273. https://doi.org/10.3390/s20216273
Colombo Zefinetti F, Vitali A, Regazzoni D, Rizzi C, Molinero G. Tracking and Characterization of Spinal Cord-Injured Patients by Means of RGB-D Sensors. Sensors. 2020; 20(21):6273. https://doi.org/10.3390/s20216273
Chicago/Turabian StyleColombo Zefinetti, Filippo, Andrea Vitali, Daniele Regazzoni, Caterina Rizzi, and Guido Molinero. 2020. "Tracking and Characterization of Spinal Cord-Injured Patients by Means of RGB-D Sensors" Sensors 20, no. 21: 6273. https://doi.org/10.3390/s20216273
APA StyleColombo Zefinetti, F., Vitali, A., Regazzoni, D., Rizzi, C., & Molinero, G. (2020). Tracking and Characterization of Spinal Cord-Injured Patients by Means of RGB-D Sensors. Sensors, 20(21), 6273. https://doi.org/10.3390/s20216273