A Privacy-Preserving Healthcare Framework Using Hyperledger Fabric

 ,
,  ,
,  ,
,  and
and 
Abstract
:1. Introduction
Contributions
- The development of PREHEALTH, a privacy-preserving healthcare data solution. This uses distributed ledger technology and the Identity Mixer (Idemix) suite. Idemix is a zero-knowledge proof (ZKP) cryptographic protocol that provides privacy-preserving features, such as anonymity and unlinkability.
- An evaluation of the robustness and security of PREHEALTH against popular attack vectors.
- Empirical comparison of the performance of PREHEALTH against relevant blockchain solutions in the literature, and against a traditional database that offers related in-context column-level encryption.
2. Background
- Execution Phase. A client application sends a transaction proposal to endorsing peers as specified by the relative endorsement policy, in order to invoke a chaincode function with regard to interacting with the blockchain ledger. As soon as the endorsers have successfully executed the chaincode, the endorsement is sent back to the client. A transaction is then assembled and signed with credentials obtained from a Membership Service Provider (MSP), which is a party that handles all the identities of peers and validators within each organization.
- Ordering Phase. A client then sends constructed transactions to the ordering service. This is a collection of nodes known as orderers, which effectively combine multiple transactions into a single block and then broadcast the ordered transactions to all peers in the network.
- Validation Phase. Lastly, each peer verifies received transactions with regard to the endorsement policy and then updates the local ledger state.
3. Related Work
PREHEALTH’s Features
4. Experimentation Environment
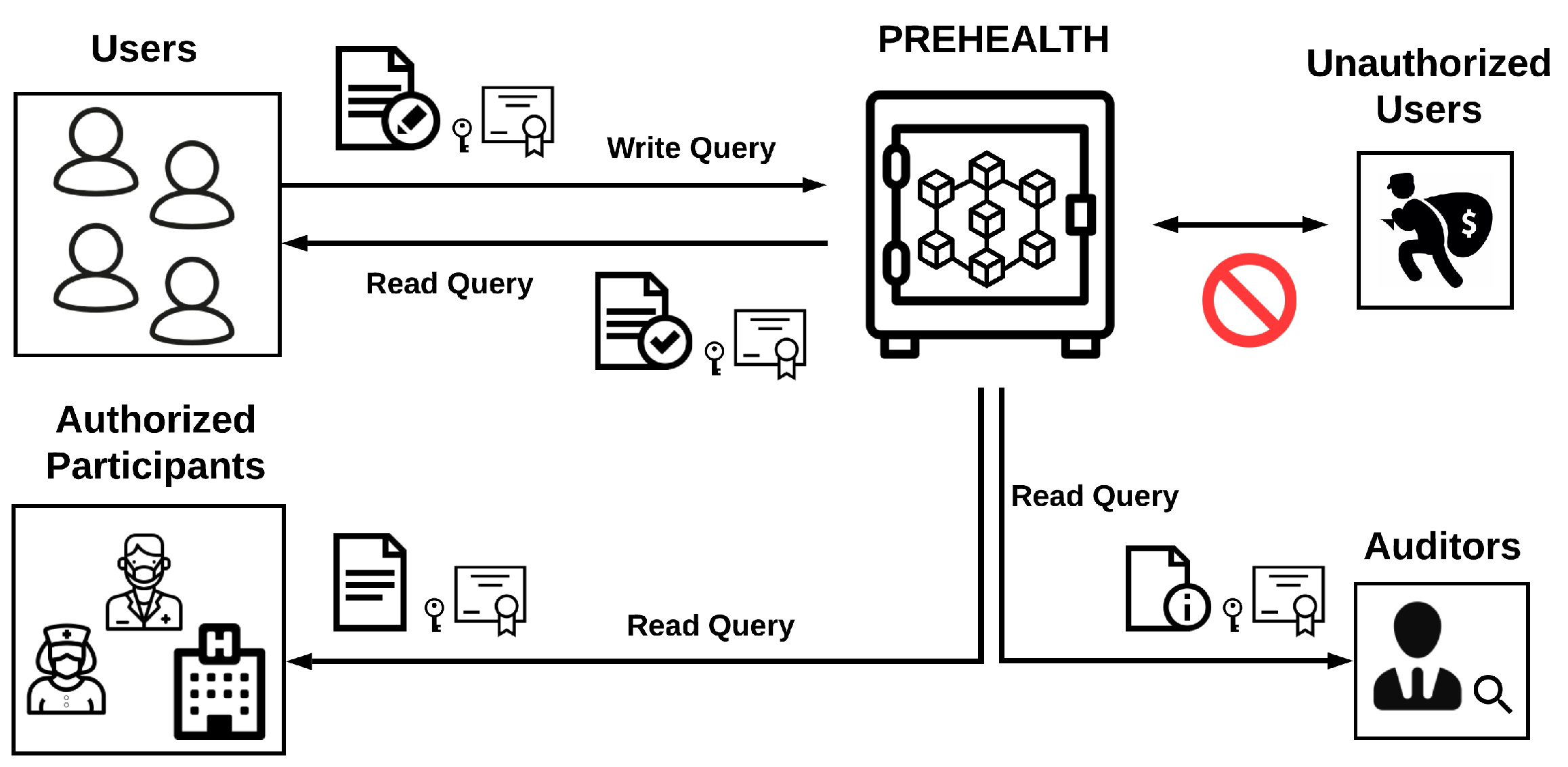
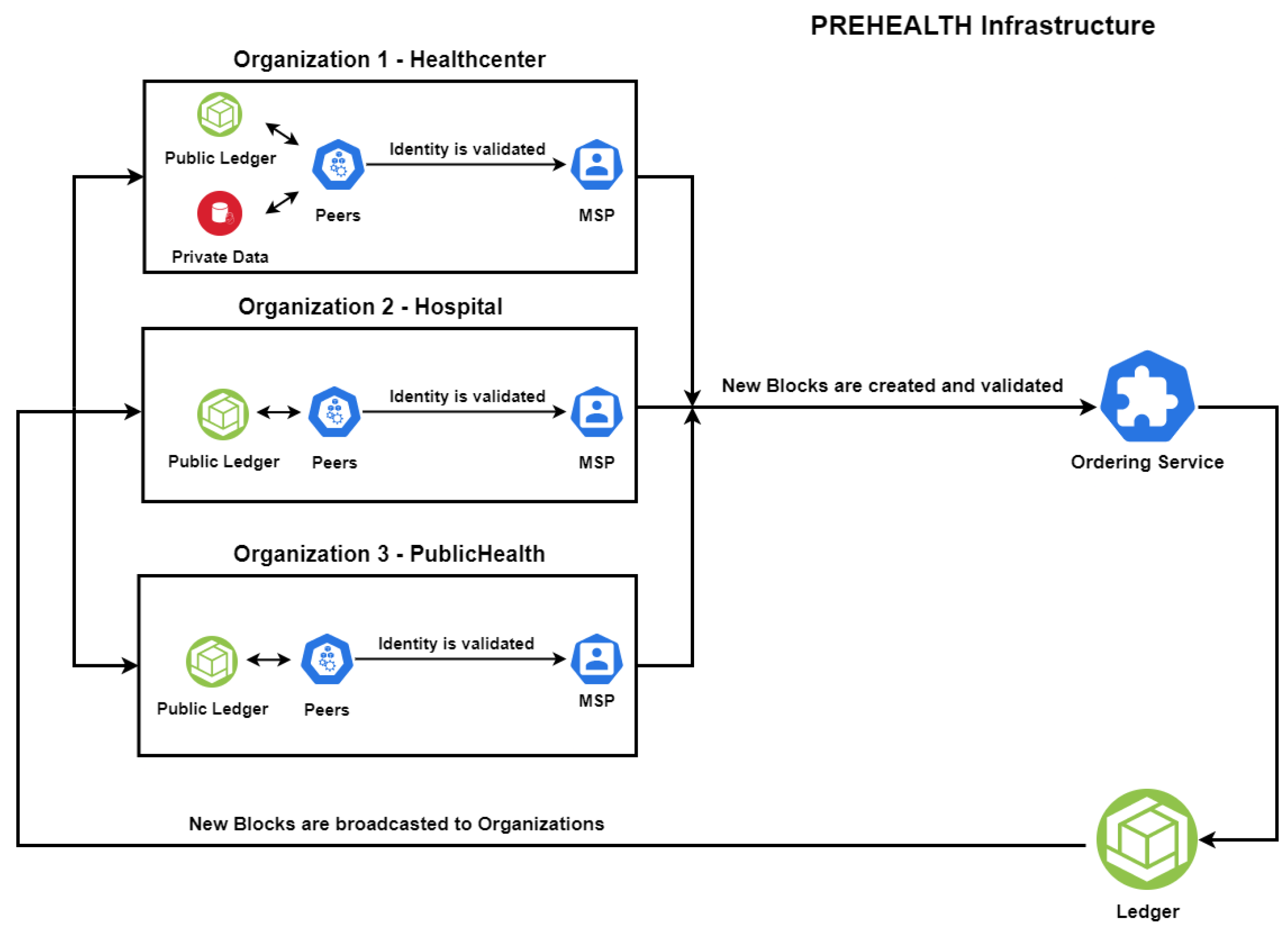
- Once a peer is validated by the MSP, it sends the proposed transaction to the ordering service.
- The ordering service validates the transaction according to the associated chaincode and updates the public ledger.
- Public ledger changes are broadcast to all the peers in order to verify, accept and update their local copy of the ledger.
5. Evaluation
5.1. Security Evaluation
5.2. Anonymity Evaluation
- Number of organizations, peers and orderers—Considering complexity and technical limitations, three organizations were established, consisting of three peers each acting as validators and an ordering service of three orderers.
- Endorsement policy—Each transaction proposal requires at least one peer of any corresponding organization to sign the transaction request, thus eliminating unnecessary communication between endorsing parties.
- Membership service provider—Idemix technology requires a distinct authentication provider in contrast to the prevailing X.509 public key certificate mechanism [41].
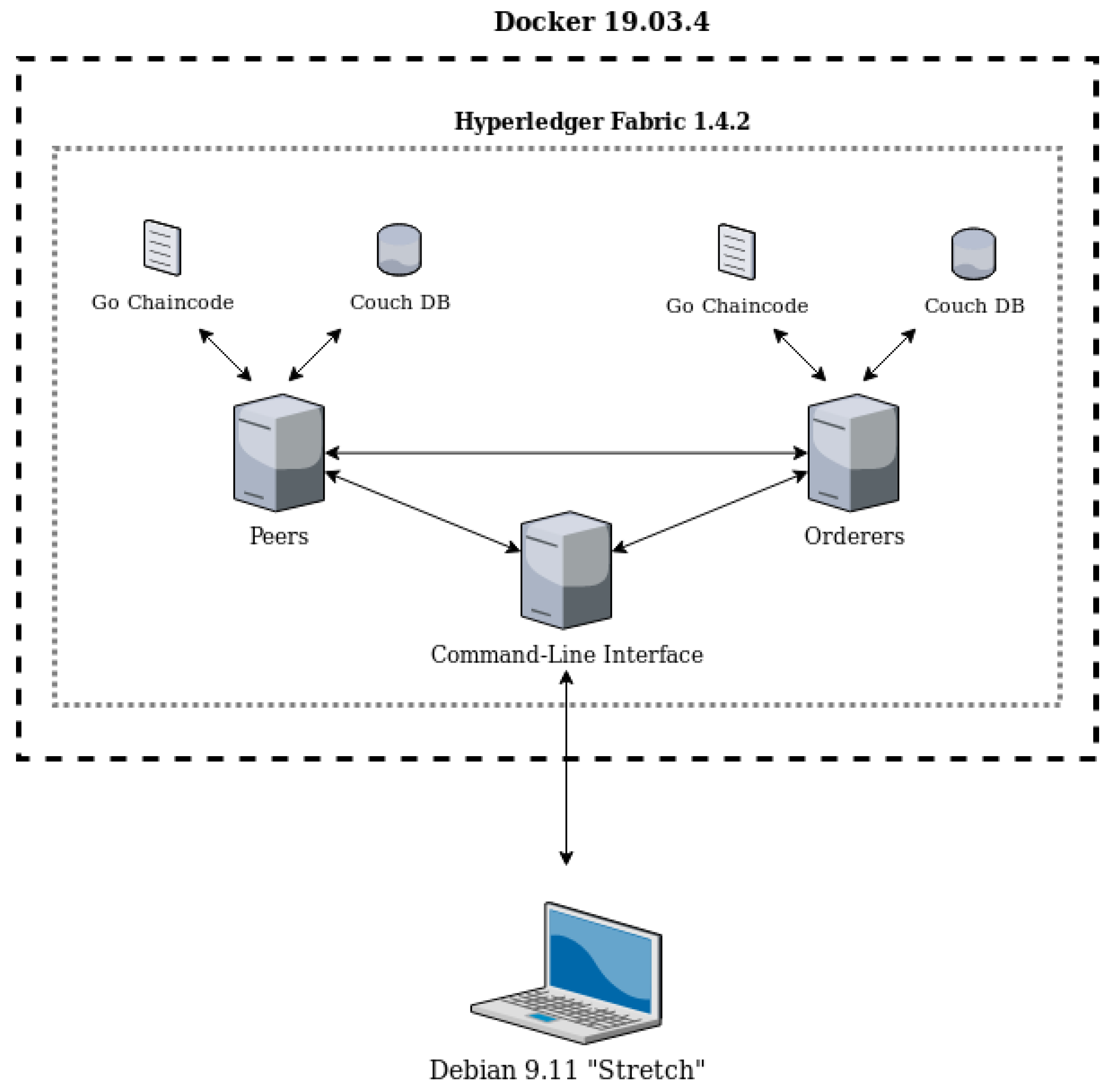
- Registration scheme for users—Unique CLI commands are required in the context of Idemix user registration. Specifically, a suitable CLI docker container was developed, as presented in Figure 2, in which relevant Idemix parameters were handled as command-line arguments in order for a user to register and interact with the blockchain network.
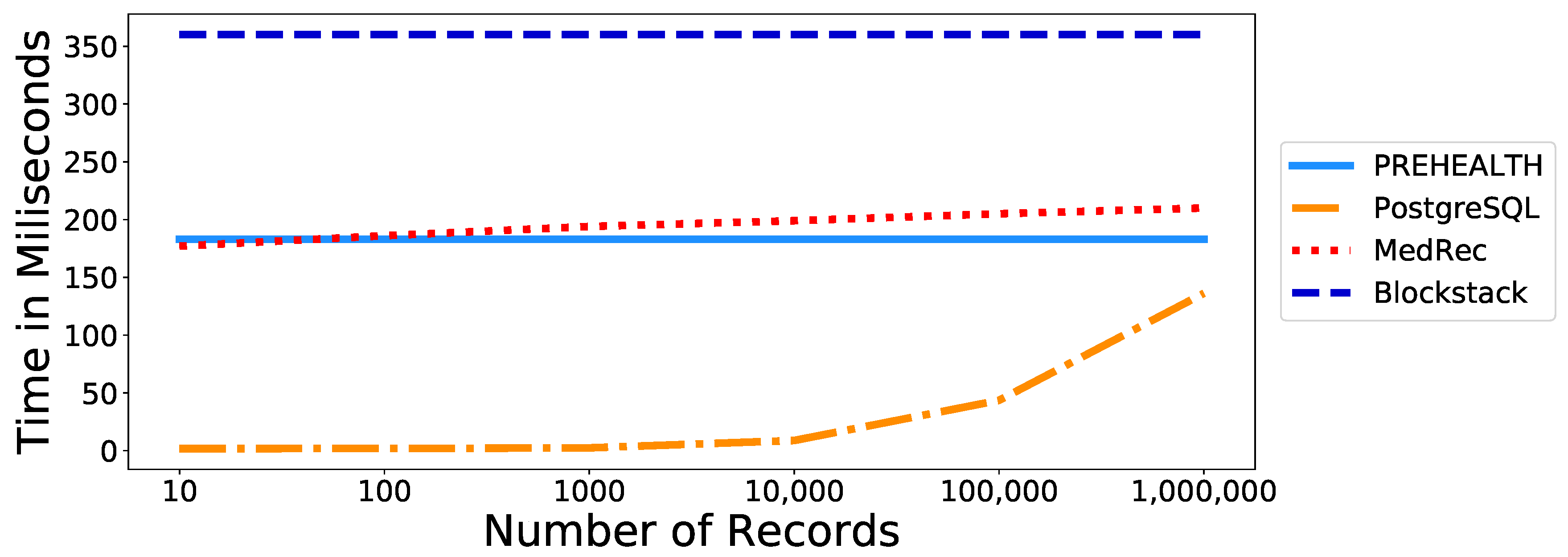
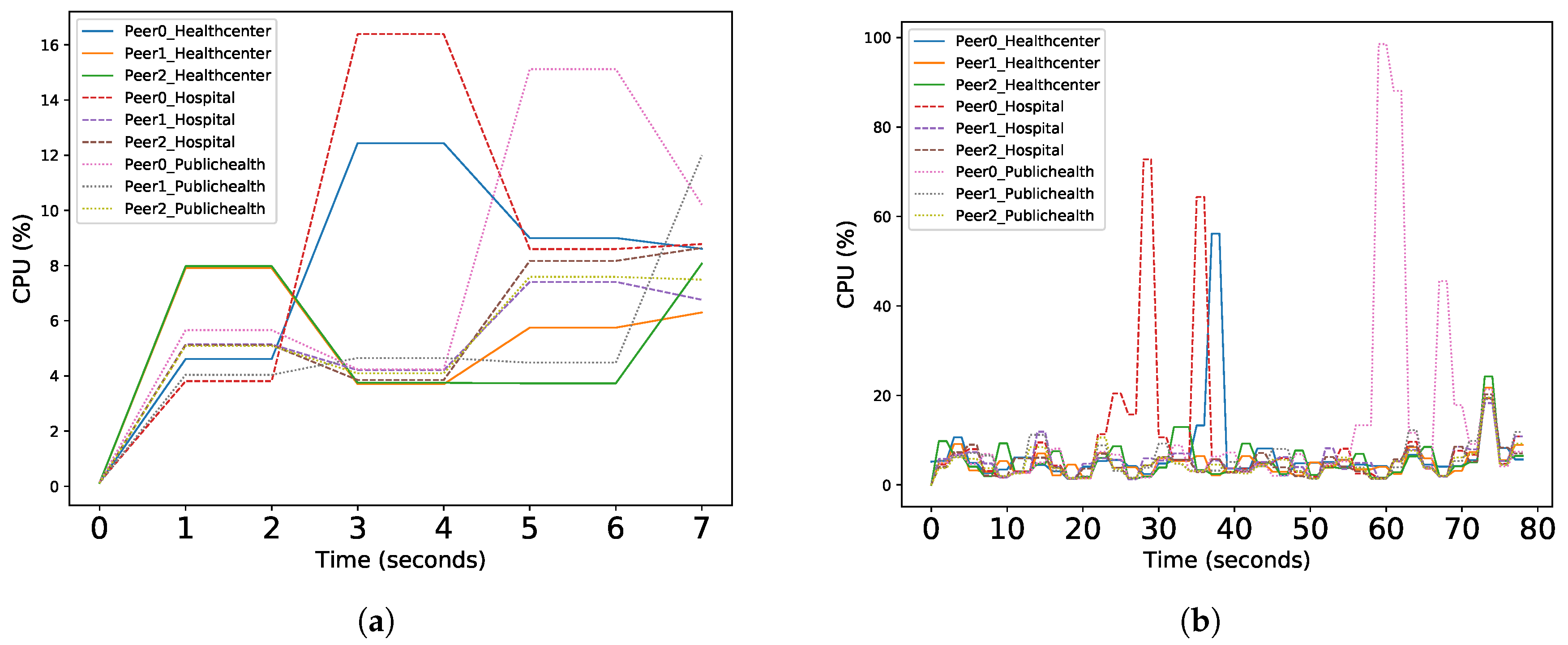
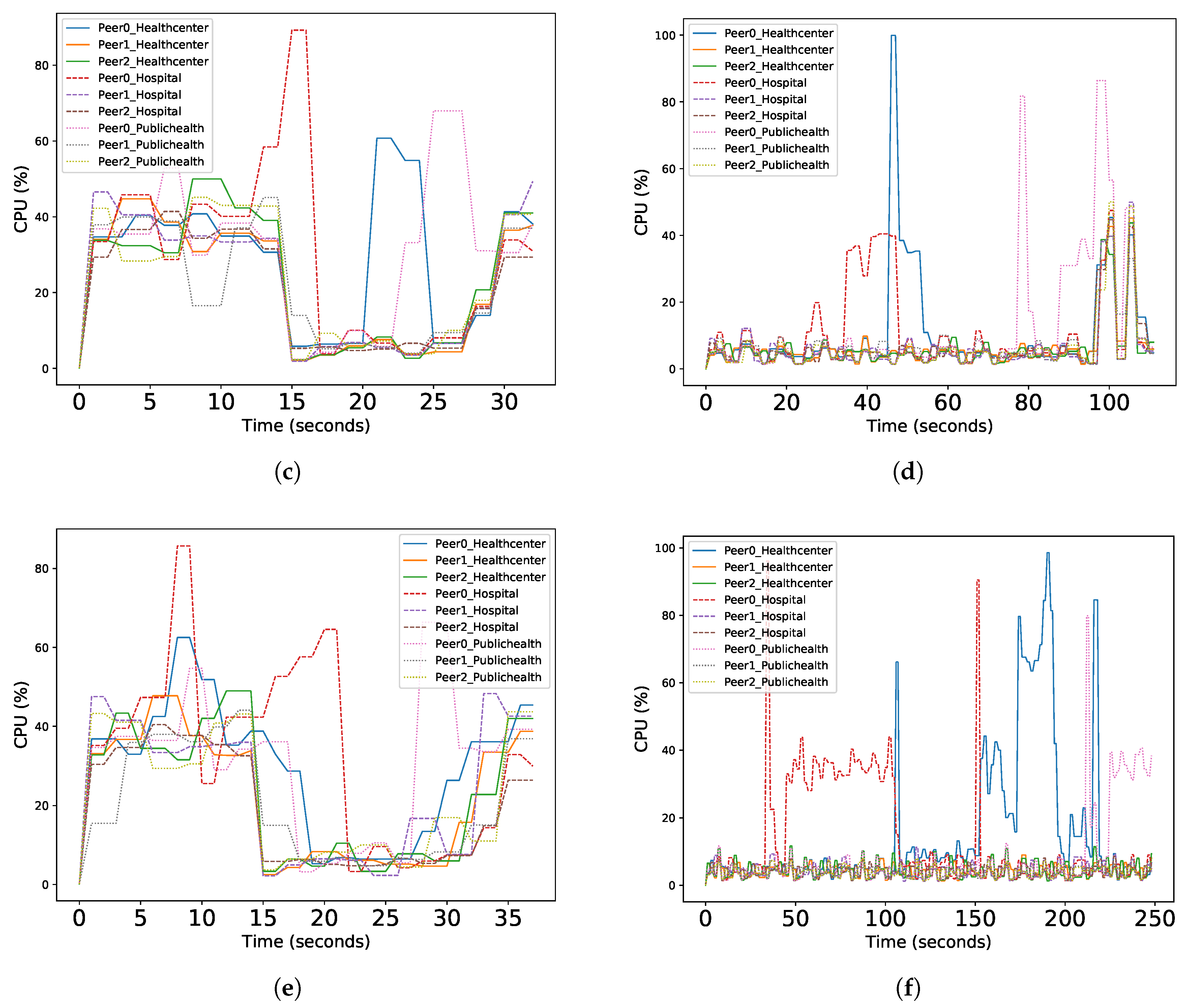
5.3. Performance Evaluation
6. Discussion
7. Conclusions and Future Work
Author Contributions
Funding
Conflicts of Interest
References
- Abbas, A.; Khan, S.U. A review on the state-of-the-art privacy-preserving approaches in the e-health clouds. IEEE J. Biomed. Health Inform. 2014, 18, 1431–1441. [Google Scholar] [CrossRef] [PubMed]
- Dubovitskaya, A.; Xu, Z.; Ryu, S.; Schumacher, M.; Wang, F. Secure and trustable electronic medical records sharing using blockchain. AMIA Annu. Symp. Proc. 2017, 2017, 650–659. [Google Scholar] [PubMed]
- Coventry, L.; Branley, D. Cybersecurity in healthcare: A narrative review of trends, threats and ways forward. Maturitas 2018, 113, 48–52. [Google Scholar] [CrossRef] [PubMed]
- Smart, W. Lessons Learned Review of the WannaCry Ransomware Cyber Attack; Department of Health and Social Care: London, UK, 2018; Volume 1, pp. 10–1038.
- Alvarez, M. Security Trends in the Healthcare Industry; Somers IBM: Somers, NY, USA, 2017; pp. 2–18. Available online: https://www.ibm.com/downloads/cas/PLWZ76MM (accessed on 17 November 2020).
- Yüksel, B.; Küpçü, A.; Özkasap, Ö. Research issues for privacy and security of electronic health services. Future Gener. Comput. Syst. 2017, 68, 1–13. [Google Scholar] [CrossRef]
- Renuka, K.; Kumar, S.; Kumari, S.; Chen, C.M. Cryptanalysis and improvement of a privacy-preserving three-factor authentication protocol for wireless sensor networks. Sensors 2019, 19, 4625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dubovitskaya, A.; Urovi, V.; Vasirani, M.; Aberer, K.; Schumacher, M.I. A cloud-based ehealth architecture for privacy preserving data integration. In Proceedings of the IFIP International Information Security and Privacy Conference, Hamburg, Germany, 26–28 May 2015; pp. 585–598. [Google Scholar]
- Angelis, S.D.; Aniello, L.; Baldoni, R.; Lombardi, F.; Margheri, A.; Sassone, V. PBFT vs proof-of-authority: Applying the CAP theorem to permissioned blockchain. In Proceedings of the Italian Conference on Cyber Security, Milan, Italy, 6 February 2018. [Google Scholar]
- Kuo, T.T.; Kim, H.E.; Ohno-Machado, L. Blockchain distributed ledger technologies for biomedical and health care applications. J. Am. Med. Inform. Assoc. 2017, 24, 1211–1220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Podda, A.S.; Pompianu, L. An overview of blockchain-based systems and smart contracts for digital coupons. In Proceedings of the IEEE/ACM 42nd International Conference on Software Engineering Workshops, Seoul, Korea, 24 June–16 July 2020; pp. 770–778. [Google Scholar]
- Longo, R.; Podda, A.S.; Saia, R. Analysis of a Consensus Protocol for Extending Consistent Subchains on the Bitcoin Blockchain. Computation 2020, 8, 67. [Google Scholar] [CrossRef]
- Cachin, C. Architecture of the hyperledger blockchain fabric. In Proceedings of the Workshop on Distributed Cryptocurrencies and Consensus Ledgers, Chicago, IL, USA, 25 July 2016; Volume 310, p. 4. [Google Scholar]
- Androulaki, E.; Barger, A.; Bortnikov, V.; Cachin, C.; Christidis, K.; De Caro, A.; Enyeart, D.; Ferris, C.; Laventman, G.; Manevich, Y.; et al. Hyperledger fabric: A distributed operating system for permissioned blockchains. In Proceedings of the Thirteenth EuroSys Conference, Porto, Portugal, 23–26 April 2018; pp. 1–15. [Google Scholar]
- Thakkar, P.; Nathan, S.; Viswanathan, B. Performance benchmarking and optimizing hyperledger fabric blockchain platform. In Proceedings of the 2018 IEEE 26th International Symposium on Modeling, Analysis, and Simulation of Computer and Telecommunication Systems (MASCOTS), Milwaukee, WI, USA, 25–28 September 2018; pp. 264–276. [Google Scholar]
- Papadopoulos, P.; Pitropakis, N.; Buchanan, W.J.; Lo, O.; Katsikas, S. Privacy-Preserving Passive DNS. Computers 2020, 9, 64. [Google Scholar] [CrossRef]
- Boettiger, C. An introduction to Docker for reproducible research. ACM SIGOPS Oper. Syst. Rev. 2015, 49, 71–79. [Google Scholar] [CrossRef]
- Androulaki, E.; De Caro, A.; Neugschwandtner, M.; Sorniotti, A. Endorsement in Hyperledger Fabric. In Proceedings of the 2019 IEEE International Conference on Blockchain (Blockchain), Atlanta, GA, USA, 14–17 July 2019; pp. 510–519. [Google Scholar]
- Abramson, W.; Hall, A.J.; Papadopoulos, P.; Pitropakis, N.; Buchanan, W.J. A Distributed Trust Framework for Privacy-Preserving Machine Learning. arXiv 2020, arXiv:2006.02456. [Google Scholar]
- Hölbl, M.; Kompara, M.; Kamišalić, A.; Nemec Zlatolas, L. A systematic review of the use of blockchain in healthcare. Symmetry 2018, 10, 470. [Google Scholar] [CrossRef] [Green Version]
- Mayer, A.H.; da Costa, C.A.; da Rosa Righi, R. Electronic health records in a blockchain: A systematic review. Health Inform. J. 2020, 26, 1273–1288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, S.; Chen, K.; Sheth, A. Toward practical privacy-preserving analytics for IoT and cloud-based healthcare systems. IEEE Internet Comput. 2018, 22, 42–51. [Google Scholar] [CrossRef] [Green Version]
- Casino, F.; Dasaklis, T.K.; Patsakis, C. A systematic literature review of blockchain-based applications: Current status, classification and open issues. Telemat. Inform. 2019, 36, 55–81. [Google Scholar] [CrossRef]
- Ming, Y.; Zhang, T. Efficient privacy-preserving access control scheme in electronic health records system. Sensors 2018, 18, 3520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roehrs, A.; da Costa, C.A.; da Rosa Righi, R. OmniPHR: A distributed architecture model to integrate personal health records. J. Biomed. Inform. 2017, 71, 70–81. [Google Scholar] [CrossRef] [PubMed]
- Ichikawa, D.; Kashiyama, M.; Ueno, T. Tamper-resistant mobile health using blockchain technology. JMIR MHealth UHealth 2017, 5, e111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, X.; Zhao, J.; Shetty, S.; Liu, J.; Li, D. Integrating blockchain for data sharing and collaboration in mobile healthcare applications. In Proceedings of the 2017 IEEE 28th Annual International Symposium on Personal, Indoor, and Mobile Radio Communications (PIMRC), Montreal, QC, Canada, 8–13 October 2017; pp. 1–5. [Google Scholar]
- Xia, Q.; Sifah, E.B.; Asamoah, K.O.; Gao, J.; Du, X.; Guizani, M. MeDShare: Trust-less medical data sharing among cloud service providers via blockchain. IEEE Access 2017, 5, 14757–14767. [Google Scholar] [CrossRef]
- Azaria, A.; Ekblaw, A.; Vieira, T.; Lippman, A. Medrec: Using blockchain for medical data access and permission management. In Proceedings of the 2016 2nd International Conference on Open and Big Data (OBD), Vienna, Austria, 22–24 August 2016; pp. 25–30. [Google Scholar]
- Yang, H.; Yang, B. A blockchain-based approach to the secure sharing of healthcare data. In Proceedings of the Norwegian Information Security Conference 2017, Oslo, Norway, 11–15 September 2017. [Google Scholar]
- Al Omar, A.; Rahman, M.S.; Basu, A.; Kiyomoto, S. Medibchain: A blockchain based privacy preserving platform for healthcare data. In Proceedings of the International Conference on Security, Privacy and Anonymity in Computation, Communication and Storage, Guangzhou, China, 12–15 December 2017; pp. 534–543. [Google Scholar]
- Bocek, T.; Rodrigues, B.B.; Strasser, T.; Stiller, B. Blockchains everywhere-a use-case of blockchains in the pharma supply-chain. In Proceedings of the 2017 IFIP/IEEE Symposium on Integrated Network and Service Management (IM), Lisbon, Portugal, 8–12 May 2017; pp. 772–777. [Google Scholar]
- Ali, M.; Shea, R.; Nelson, J.; Freedman, M.J. Blockstack: A New Decentralized Internet. Whitepaper. May 2017. Available online: https://pdos.csail.mit.edu/6.824/papers/blockstack-2017.pdf (accessed on 17 November 2020).
- Dwivedi, A.D.; Srivastava, G.; Dhar, S.; Singh, R. A decentralized privacy-preserving healthcare blockchain for IoT. Sensors 2019, 19, 326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albeyatti, A. White Paper: Medicalchain. MedicalChain Self-Publication, 2018. Available online: https://medicalchain.com/en/whitepaper/ (accessed on 17 November 2020).
- Voigt, P.; Von dem Bussche, A. The eu general data protection regulation (gdpr). In A Practical Guide, 1st ed.; Springer International Publishing: Cham, Switzerland, 2017. [Google Scholar]
- Davari, M.; Bertino, E. Access control model extensions to support data privacy protection based on GDPR. In Proceedings of the 2019 IEEE International Conference on Big Data (Big Data), Los Angeles, CA, USA, 9–12 December 2019; pp. 4017–4024. [Google Scholar]
- Krafft, M.F. A Delphi Study of the Influences on Innovation Adoption and Process Evolution in a Large Open Source Project: The Case of Debian; University of Limerick, Department of Computer Science & Information Systems: Limerick, Ireland, 2010; Available online: http://193.1.102.107/handle/10344/427 (accessed on 17 November 2020).
- English, E.; Kim, A.D.; Nonaka, M. Advancing Blockchain Cybersecurity: Technical and Policy Considerations for the Financial Services Industry. 2018. Available online: https://www.microsoft.com/en-us/cybersecurity/content-hub/advancing-blockchain-cybersecurity (accessed on 17 November 2020).
- Hyperledger Fabric. Client Identity Chaincode Library, 2017. Available online: https://github.com/hyperledger/fabric/blob/release-1.1/core/chaincode/lib/cid/README.md (accessed on 17 November 2020).
- Chokhani, S.; Ford, W.; Sabett, R.; Merrill, C.; Wu, S. RFC 2527: Internet X.509 Public Key Infrastructure Certificate Policy and Certification Practices Framework; Internet Engineering Task Force (IETF), RFC: Fremont, CA, USA, 1999; Available online: https://tools.ietf.org/html/rfc2527 (accessed on 17 November 2020).
- Halfond, W.G.; Viegas, J.; Orso, A. A classification of SQL-injection attacks and countermeasures. In Proceedings of the IEEE International Symposium on Secure Software Engineering, Washington, DC, USA, March 2006; Volume 1, pp. 13–15. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Method | Technology | Access | Verifiability | Privacy-Preserving | GDPR | Performance/Scalability |
|---|---|---|---|---|---|---|
| [24] | AC Scheme | Private | Private | 🗸 | ✗ | 🗸 |
| [32] | Ethereum | Private | Public | ✗ | ✗ | ✗ |
| [31] | Ethereum | Private | Public | ✗ | ✗ | 🗸 |
| [29] | Ethereum | Open | Public/Private | 🗸 | ✗ | ✗ |
| [33] | Bitcoin/Agnostic | Open | Public | 🗸 | 🗸 | ✗ |
| [28] | Agnostic | Open | Private | ✗ | ✗ | 🗸 |
| [25] | Peer-to-peer | Private | Private | ✗ | ✗ | 🗸 |
| [27] | HLF | Private | Private | ✗ | ✗ | 🗸 |
| [26] | HLF | Private | Private | ✗ | 🗸 | ✗ |
| Our work | HLF | Private | Private | 🗸 | 🗸 | 🗸 |
| Number of Records: | 10 | 100 | 1000 | 10,000 | 100,000 | 1,000,000 | |
|---|---|---|---|---|---|---|---|
| PREHEALTH | Read Data Time | 183 ms | 183 ms | 183 ms | 183 ms | 183 ms | 183 ms |
| Write Data Time | 58 ms | 58 ms | 58 ms | 58 ms | 58 ms | 58 ms | |
| PostgresSQL Database | Read Data Time | 1.73 ms | 1.79 ms | 2.38 ms | 8.76 ms | 43.52 ms | 136.19 ms |
| Write Data Time | 4.32 ms | 4.48 ms | 4.47 ms | 4.37 ms | 4.39 ms | 4.45 ms | |
| MedRec—Azaria et al. [29] | Read Data Time | 177 ms | 186 ms | 194 ms | 199 ms | 205 ms | 210 ms |
| Write Data Time | 81.5 ms | 86.9 ms | 79.6 ms | 71.6 ms | 63.2 ms | 79.6 ms | |
| Blockstack—Ali et al. [33] | Read Data Time | 360 ms | 360 ms | 360 ms | 360 ms | 360 ms | 360 ms |
| Write Data Time | 530 ms | 530 ms | 530 ms | 530 ms | 530 ms | 530 ms | |
| PREHEALTH Organizations | PREHEALTH Peers | Number of Records | |||
|---|---|---|---|---|---|
| 1000 | 10,000 | 100,000 | |||
| Healthcenter | Peer 0 | Read Queries | 7.6% | 28.7% | 29% |
| Write Queries | 6.7% | 10.3% | 15.4% | ||
| Peer 1 | Read Queries | 5.1% | 21.8% | 21.7% | |
| Write Queries | 4.9% | 6.7% | 4.2% | ||
| Peer 2 | Read Queries | 4.9% | 23.3% | 22.2% | |
| Write Queries | 5.4% | 6.4% | 4.3% | ||
| Hospital | Peer 0 | Read Queries | 8.3% | 29.4% | 32.3% |
| Write Queries | 9.3% | 11.2% | 13.9% | ||
| Peer 1 | Read Queries | 5.1% | 22.7% | 23.2% | |
| Write Queries | 5.4% | 6.4% | 4.3% | ||
| Peer 2 | Read Queries | 5.4% | 20.7% | 18.7% | |
| Write Queries | 4.9% | 6.6% | 4.2% | ||
| PublicHealth | Peer 0 | Read Queries | 7.6% | 30.5% | 30.3% |
| Write Queries | 11.4% | 12.8% | 8.2% | ||
| Peer 1 | Read Queries | 4.8% | 22% | 20.1% | |
| Write Queries | 5.3% | 6.8% | 4% | ||
| Peer 2 | Read Queries | 5.1% | 23.4% | 22% | |
| Write Queries | 4.7% | 6.6% | 4% | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stamatellis, C.; Papadopoulos, P.; Pitropakis, N.; Katsikas, S.; Buchanan, W.J. A Privacy-Preserving Healthcare Framework Using Hyperledger Fabric. Sensors 2020, 20, 6587. https://doi.org/10.3390/s20226587
Stamatellis C, Papadopoulos P, Pitropakis N, Katsikas S, Buchanan WJ. A Privacy-Preserving Healthcare Framework Using Hyperledger Fabric. Sensors. 2020; 20(22):6587. https://doi.org/10.3390/s20226587
Chicago/Turabian StyleStamatellis, Charalampos, Pavlos Papadopoulos, Nikolaos Pitropakis, Sokratis Katsikas, and William J. Buchanan. 2020. "A Privacy-Preserving Healthcare Framework Using Hyperledger Fabric" Sensors 20, no. 22: 6587. https://doi.org/10.3390/s20226587
APA StyleStamatellis, C., Papadopoulos, P., Pitropakis, N., Katsikas, S., & Buchanan, W. J. (2020). A Privacy-Preserving Healthcare Framework Using Hyperledger Fabric. Sensors, 20(22), 6587. https://doi.org/10.3390/s20226587