A Low-Cost Breath Analyzer Module in Domiciliary Non-Invasive Mechanical Ventilation for Remote COPD Patient Monitoring †

 ,
, 
 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Rationale
2.2. Design Consideration
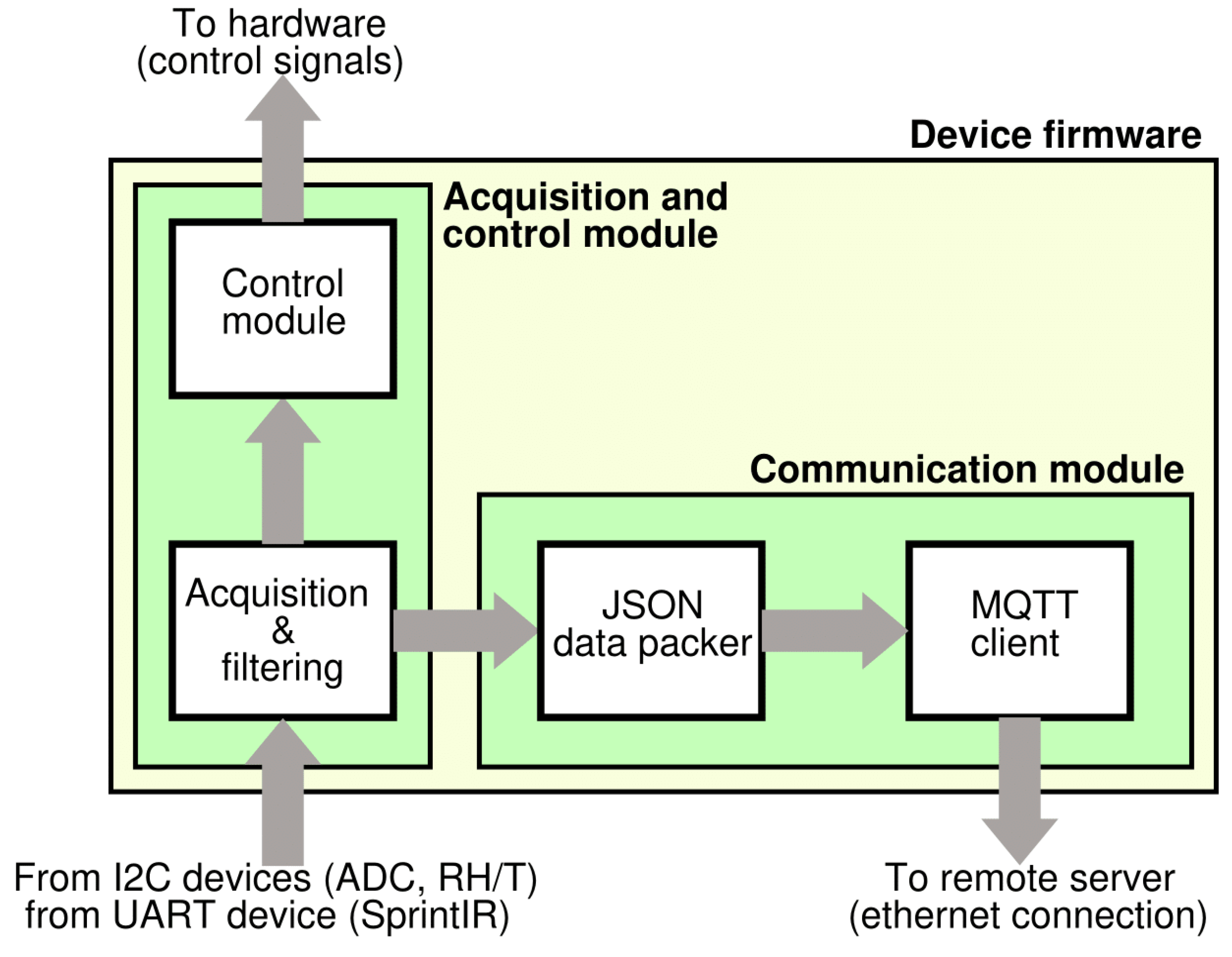
2.3. Hardware and Firmware Design
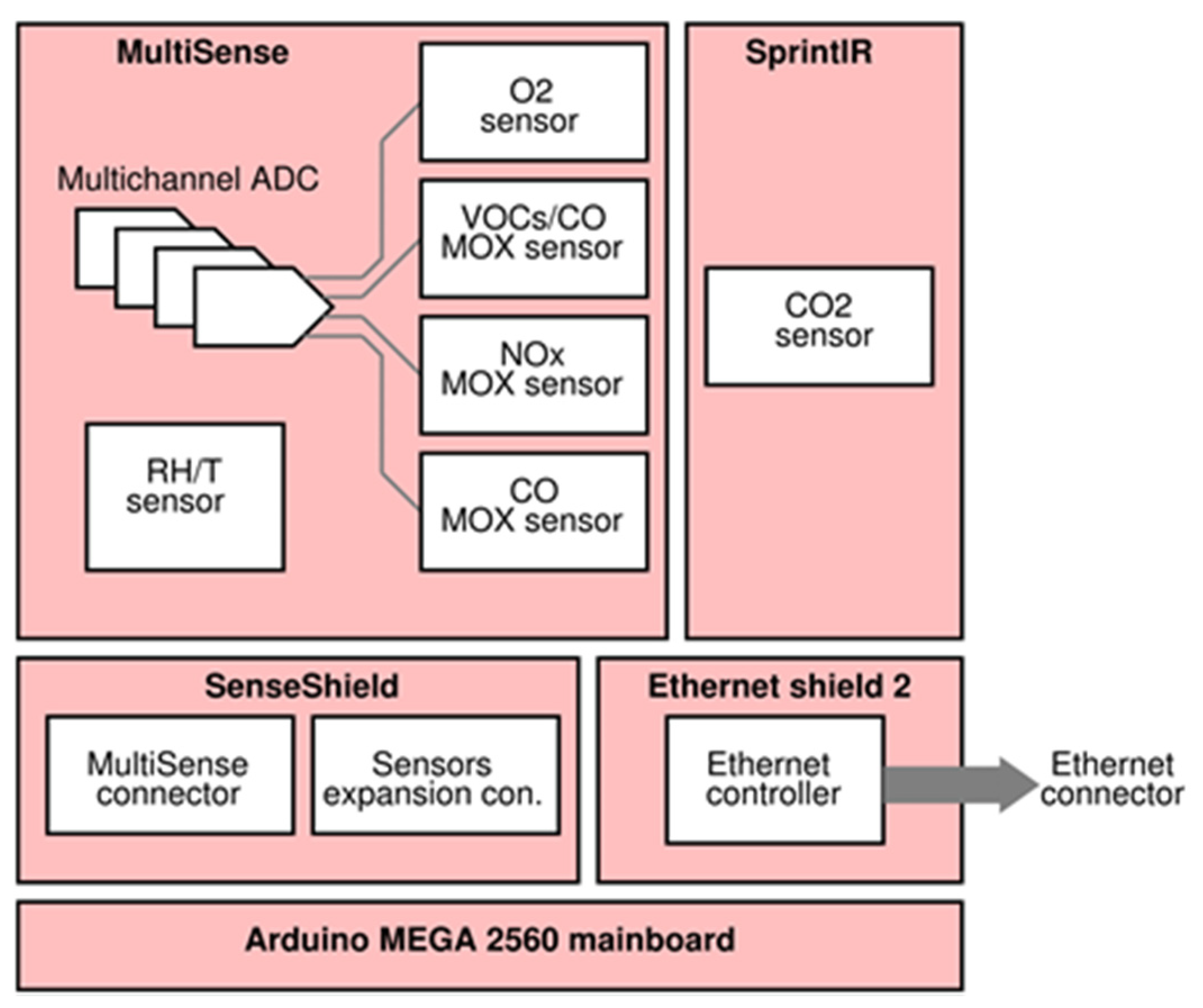
- (1)
- Infrared CO2 sensor: SprintIR™ by Gas Sensing Solutions Ltd., Cumbernauld, United Kingdom;
- (2)
- Electrochemical O2 sensor: KE-25 by Figaro Engineering Inc., Osaka, Japan;
- (3)
- Relative humidity and temperature: SHT75 by Sensirion AG, Staefa ZH, Switzerland;
- (4)
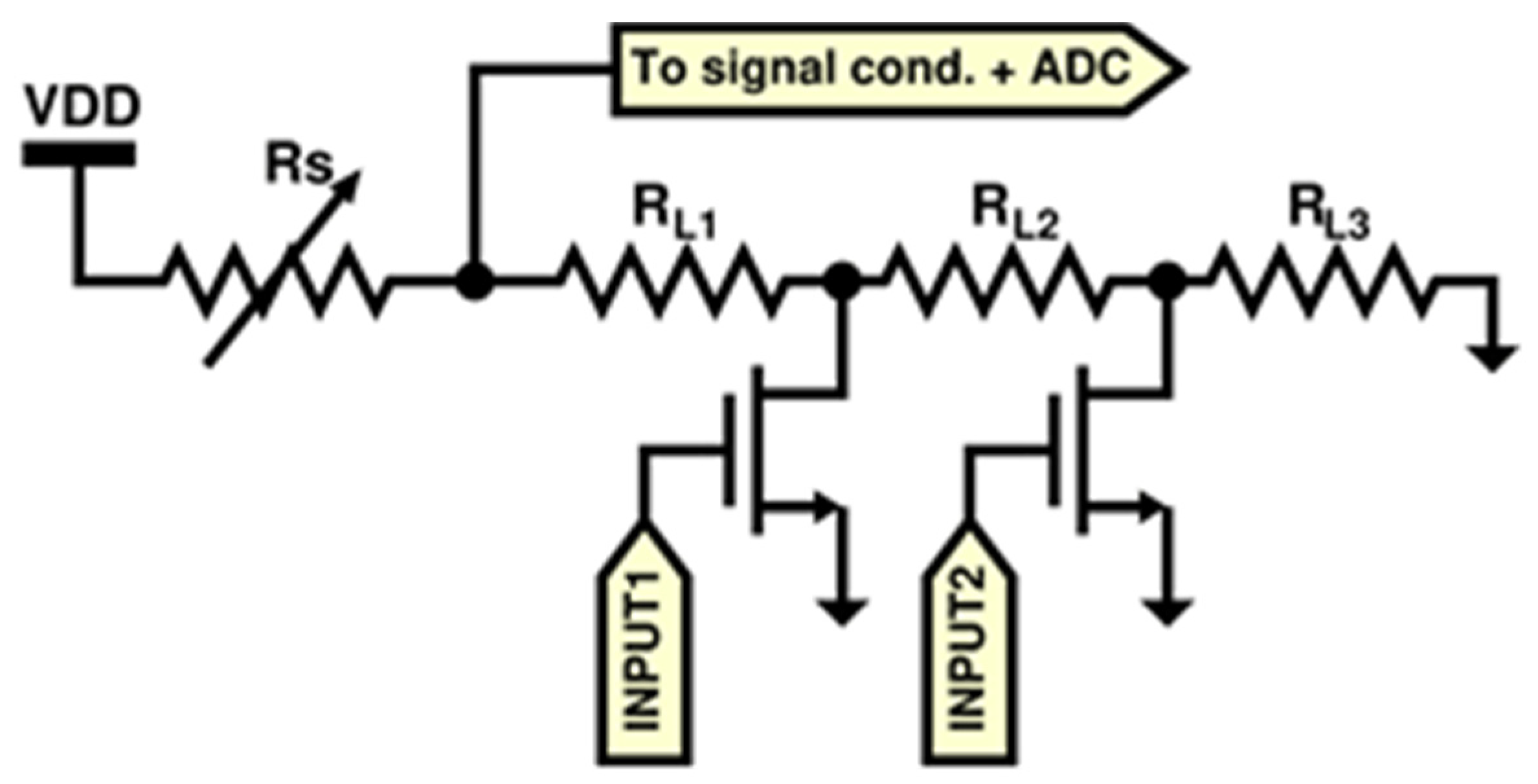
- A dual (NOX-CO) sensor built with MOX technology: MiCS-4514 by SGX SensorTech, Corcelles-Cormondrèche, Switzerland;
- (5)
- A VOC sensor built with MOX technology: AS-MLV-P2 by ams AG, Unterpremstaetten, Austria;
3. Results and Discussion
4. Conclusions
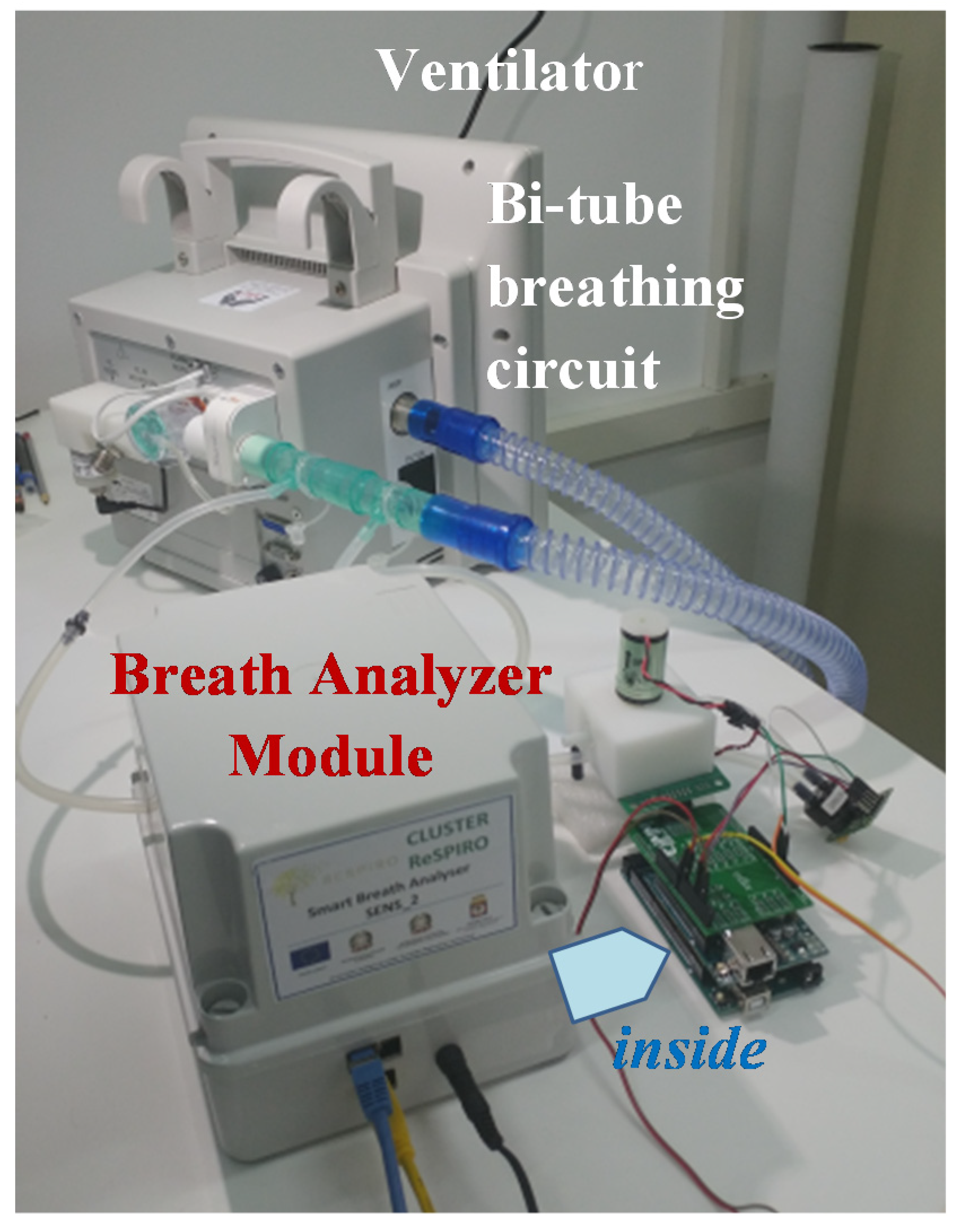
- Universal: it can be used as external module for any ventilator with bi-tube breathing circuit;
- Plug & Play: it requires only basic connections without configuration;
- Low-cost and highly customizable: it is based on low-cost hardware (Arduino);
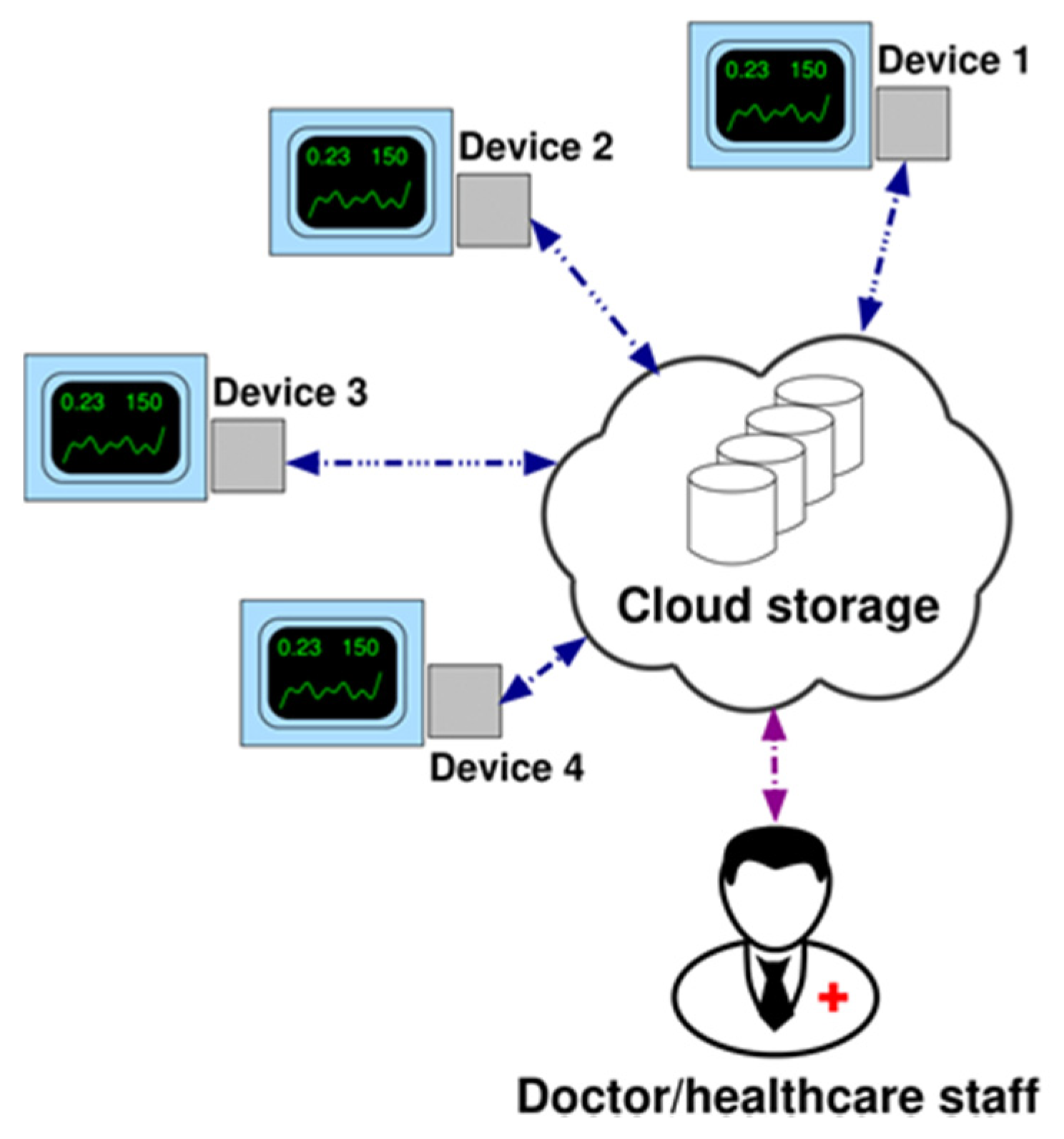
- IoT-oriented: the device can communicate data over TCP/IP communication (wired).
- Flexible to further implementations: the system may be configured for advanced data processing in OMNIACARE hardware/software platform to support local healthcare staff to check the effectiveness of therapy.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| VOC | Volatile Organic Compound |
| COPD | Chronic Obstructive Pulmonary Disease |
| ECOPD | exacerbation of COPD |
| NIV | Noninvasive ventilation |
| NHS | National Health Service |
| TCP/IP | Transmission Control Protocol/Internet Protocol |
| R.H. & T | Relative Humidity & Temperature |
| MFC | Mass Flow Controller |
| GC/MS | Gas Chromatography/Mass Spectroscopy |
| IoT | Internet of Things |
| MQTT | Message Queue Telemetry Transport |
| TLS/SSL | Transport Layer Security/Secure Sockets Layer |
| PCB | Printed Circuit Board |
| SMD | Surface Mounting Devices |
| PTH | Pin Through Hole |
| IDE | Integrated Development Environment |
| PC | Personal Computer |
| ICT | Information and Communication Technology |
| MOSFET | Metal Oxide Semiconductor Field Effect Transistor |
References
- Roussos, C.; Koutsoukou, A. Respiratory failure. Eur. Respir. J. 2003, 22 (Suppl. 47), 3s–14s. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rabe, K.F.; Watz, H. Chronic obstructive pulmonary disease, Seminar. Lancet 2017, 389, 1931–1940. [Google Scholar] [CrossRef]
- Postma, D.S.; Bush, A.; Van den Berge, M. Risk factors and early origins of chronic obstructive pulmonary disease—Review. Lancet 2015, 385, 899–909. [Google Scholar] [CrossRef]
- Pocket Guide to COPD Diagnosis, Management, and Prevention, A Guide for Health Care Professionals, 2020 Report. © 2020 Global Initiative for Chronic Obstructive Lung Disease, Inc.. Available online: www.goldcopd.org (accessed on 23 January 2020).
- Wedzicha, J.A.; Miravitlles, M.; Hurst, J.R.; Calverley, P.M.A.; Albert, R.K.; Anzueto, A.; Criner, G.J.; Papi, A.; Rabe, K.F.; Rigau, D.; et al. Management of COPD exacerbations: A European Respiratory Society/American Thoracic Society guideline. Eur. Respir. J. 2017, 49, 1600791. [Google Scholar] [CrossRef] [Green Version]
- Abbatecola, A.M.; Fumagalli, A.; Bonardi, D.; Guffanti, E.E. Practical management problems of chronic obstructive pulmonary disease in the elderly: Acute exacerbations. Curr. Opin. Pulm. Med. 2011, 17, S49–S54. [Google Scholar] [CrossRef]
- Viniol, C.; Vogelmeier, C.F. Exacerbations of COPD. Eur. Respir. Rev. 2018, 27, 170103. [Google Scholar] [CrossRef] [Green Version]
- Gregoretti, C.; Navalesi, P.; Ghannadian, S.; Carlucci, A.; Pelosi, P. Choosing a ventilator for home mechanical ventilation. Breathe 2013, 9, 395–408. [Google Scholar] [CrossRef]
- Dellaca’, R.L.; Veneroni, C.; Farre, R. Trends in mechanical ventilation: Are we ventilating our patients in the best possible way? Breathe 2017, 13, 84–98. [Google Scholar] [CrossRef]
- Simonds, A.K. Home Mechanical Ventilation: An Overview. Ann. Am. Thorac. Soc. 2016, 13, 2035–2044. [Google Scholar] [CrossRef] [Green Version]
- Durão, V.; Grafino, M.; Pamplona, P. Chronic respiratory failure in patients with chronic obstructive pulmonary disease under home noninvasive ventilation: Real-lifestudy. Pulmonology 2018, 24, 280–288. [Google Scholar] [CrossRef]
- Murphy, P.B.; Hart, N. Home Non-Invasive Ventilation for COPD: How, Who and When? Arch. Bronconeumol. 2018, 54, 149–154. [Google Scholar] [CrossRef]
- Scala, R. Challenges on non-invasive ventilation to treat acute respiratory failure in the elderly. BMC Pulm. Med. 2016, 16, 150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kent, B.D.; Mitchell, P.D.; McNicholas, W.T. Hypoxemia in patients with COPD: Cause, effects, and disease progression. Int. J. Chron. Obstruct. Pulmon. Dis. 2011, 6, 199–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brill, S.E.; Wedzicha, J.A. Oxygen therapy in acute exacerbations of chronic obstructive pulmonary disease. Int. J. Chron. Obstruct. Pulmon. Dis. 2014, 9, 1241–1252. [Google Scholar] [CrossRef] [Green Version]
- Abdo, W.F.; Heunks, L.M. Oxygen-induced hypercapnia in COPD: Myths and facts. Crit. Care 2012, 16, 323. [Google Scholar] [CrossRef] [Green Version]
- Sabato, E.; Sabina, S.; Leo, C.G. Standard Care. In Long-Term Oxygen Therapy; Dal Negro, R.W., Hodder, R., Eds.; Springer-Verlag Italia s.r.l.: Milan, Italy, 2012; pp. 161–170. [Google Scholar] [CrossRef]
- Shigemura, M.; Lecuona, E.; Sznajder, J.I. Effects of hypercapnia on the lung- Symposium Review. J. Physiol. 2017, 595, 2431–2437. [Google Scholar] [CrossRef] [Green Version]
- Sabato, E.; Leo, C.G.; Sabina, S. Continuity of health care in patients with chronic respiratory insufficiency: A macro-model of care integration between hospital and home (Review). Multidiscip. Respir. Med. 2009, 4, 112–120. [Google Scholar]
- Huttmann, S.E.; Windisch, W.; Storre, J.H. Techniques for the Measurement and Monitoring of Carbon Dioxide in the Blood. Ann. Am. Thorac. Soc. 2014, 11, 645–652. [Google Scholar] [CrossRef]
- Thawley, V.; Waddell, L.S. Pulse Oximetry and Capnometry. Top. Companion Anim. Med. 2013, 28, 124–128. [Google Scholar] [CrossRef]
- Duiverman, M.L. Noninvasive ventilation in stable hypercapnic COPD: What is the evidence? ERJ Open Res. 2018, 4, 00012–02018. [Google Scholar] [CrossRef]
- Vincent, T.A.; Gardner, J.W. A low cost MEMS based NDIR system for the monitoring of carbon dioxide in breath analysis at ppm levels. Sens. Actuators B Chem. 2016, 236, 954–964. [Google Scholar] [CrossRef] [Green Version]
- Domingo, C.; Blanch, L.; Murias, G.; Luján, M. State-of-the-Art Sensor Technology in Spain: Invasive and Non-Invasive Techniques for Monitoring Respiratory Variables. Sensors 2010, 10, 4655–4674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guffanti, E.E.; Colombo, D.; Fumagalli, A.; Misuraca, C.; Viganò, A. Telemedicine for Home-Ventilated Patients. In Home Long-Term Oxygen Treatment in Italy—The Additional Value of Telemedicine; Dal Negro, R.W., Goldberg, A.I., Eds.; Springer-Verlag Italia: Milan, Italy, 2005; pp. 133–146. ISBN 978-88-470-0448-1. [Google Scholar]
- Ambrosino, N.; Vitacca, M.; Dreher, M.; Isetta, V.; Montserrat, J.M.; Tonia, T.; Turchetti, G.; Winck, J.C.; Burgos, F.; Kampelmacher, M.; et al. Tele-monitoring of ventilator-dependent patients: A European Respiratory Society Statement. Eur. Respir. J. 2016, 48, 648–663. [Google Scholar] [CrossRef]
- Ambrosino, N.; Vagheggini, G.; Mazzoleni, S.; Vitacca, M. Telemedicine in chronic obstructive pulmonary disease. Breathe 2016, 12, 350–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vitacca, M.; Montini, A.; Comini, L. How will telemedicine change clinical practice in chronic obstructive pulmonary disease? Ther. Adv. Respir. Dis. 2018, 12, 1–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casavant, D.W.; McManus, M.L.; Parsons, S.K.; Zurakowski, D.; Graham, R.J. Trial of telemedicine for patients on home ventilator support: Feasibility, confidence in clinical management and use in medical decision-making. J. Telemed. Telecare 2014, 20, 441–449. [Google Scholar] [CrossRef]
- Mansell, S.K.; Cutts, S.; Hackney, I.; Wood, M.J.; Hawksworth, K.; Creer, D.D.; Kilbride, C.; Mandal, S. Using domiciliary non-invasive ventilator data downloads to inform clinical decision-making to optimise ventilation delivery and patient compliance. BMJ Open Respir. Res. 2018, 5, e000238. [Google Scholar] [CrossRef]
- Govoni, L.; Farrè, R.; Pedotti, A.; Montserrat, J.M.; Dellacà, R.L. An Improved Telemedicine System for Remote Titration and Optimization of Home Mechanical Ventilation. In Proceedings of the IEEE Proc. 2010 5th Cairo International Biomedical Engineering Conference, Cairo, Egypt, 16–18 December 2010; pp. 66–69. [Google Scholar] [CrossRef]
- Battista, L. A new system for continuous and remote monitoring of patients receiving home mechanical ventilation. Rev. Sci. Instrum. 2016, 87, 095105. [Google Scholar] [CrossRef]
- Dixon, L.C.; Ward, D.J.; Smith, J.; Holmes, S.; Mahadeva, R. New and emerging technologies for the diagnosis and monitoring of chronic obstructive pulmonary disease: A horizon scanning review. Chron. Respir. Dis. 2016, 13, 321–336. [Google Scholar] [CrossRef]
- Tomasic, I.; Tomasic, N.; Trobec, R.; Krpan, M.; Kelava, T. Continuous remote monitoring of COPD patients—Justification and explanation of the requirements and a survey of the available technologies. Med. Biol. Eng. Comput. 2018, 56, 547–569. [Google Scholar] [CrossRef] [Green Version]
- Radogna, A.V.; Capone, S.; Di Lauro, G.A.; Fiore, N.; Francioso, L.; Casino, F.; Siciliano, P.; Sabina, S.; Sabato, E. A smart device for supporting mechanical ventilo-therapy. In Proceedings of the IEEE International Conference on IC Design and Technology (ICICDT 2018), Otranto, Italy, 4–6 June 2018; pp. 177–180. [Google Scholar] [CrossRef]
- OMNIAPLACE Solutions. Available online: http://www.omniaplace.it/en-us/Solutions/OmniaCare (accessed on 17 December 2019).
- George, S.C.; Hlastala, M.P. Airway Gas Exchange and Exhaled Biomarkers. Compr. Physiol. 2011, 1, 1837–1859. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, D.; Matsui, M.; Hiroma, T.; Nakamura, T. A lightweight mainstream capnometer with very low dead space volume is useful monitor for neonates with spontanous and mechanical ventilation: Pilot study. Open J. Pediatr. 2012, 2, 127–132. [Google Scholar] [CrossRef] [Green Version]
- Wilson, A.D. Biomarker Metabolite Signatures Pave the Way for Electronic-nose, Applications in Early Clinical Disease Diagnoses. Curr. Metabolomics 2017, 5, 90–101. [Google Scholar] [CrossRef]
- Van de Kant, K.D.G.; Van der Sande, L.J.T.M.; Jöbsis, Q.; Van Schayck, O.C.P.; Dompeling, E. Clinical use of exhaled volatile organic compounds in pulmonary diseases: A systematic review. Respir. Res. 2012, 13, 117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Behera, B.; Joshi, R.; Anil Vishnu, G.K.; Bhalerao, S.; Pandya, H.J. Electronic nose: A non-invasive technology for breath analysis of diabetes and lung cancer patients. J. Breath Res. 2019, 13, 024001. [Google Scholar] [CrossRef] [PubMed]
- Amor, R.E.; Nakhleh, M.K.; Barash, O.; Haick, H. Breath analysis of cancer in the present and the future. Eur. Respir. Rev. 2019, 28, 190002. [Google Scholar] [CrossRef]
- Jia, Z.; Patra, A.; Kutty, V.K.; Venkatesan, T. Critical Review of Volatile Organic Compound Analysis in Breath and In Vitro Cell Culture for Detection of Lung Cancer. Metabolites 2019, 9, 52. [Google Scholar] [CrossRef] [Green Version]
- Christiansen, A.; Rømhild Davidsen, J.; Titlestad, I.; Vestbo, J.; Baumbach, J. A systematic review of breath analysis and detection of volatile organic compounds in COPD. J. Breath Res. 2016, 10, 034002. [Google Scholar] [CrossRef]
- Van Berkel, J.J.B.N.; Dallinga, J.W.; Möller, G.M.; Godschalk, R.W.L.; Moonen, E.J.; Wouters, E.F.M.; Van Schooten, F.J. A profile of volatile organic compounds in breath discriminates COPD patients from controls. Respir. Med. 2010, 104, 557–563. [Google Scholar] [CrossRef] [Green Version]
- Basanta, M.; Ibrahim, B.; Dockry, R.; Douce, D.; Morris, M.; Singh, D.; Woodcock, A.; Fowler, S.J. Exhaled volatile organic compounds for phenotyping chronic obstructive pulmonary disease: A cross-sectional study. Respir. Res. 2012, 13, 72. Available online: http://respiratory-research.com/content/13/1/72 (accessed on 23 January 2020). [CrossRef] [Green Version]
- Bos, L.D.; Sterk, P.J.; Fowler, S.J. Breathomics in the setting of asthma and chronic obstructive pulmonary disease. J. Allergy Clin. Immunol. 2016, 138, 970–976. [Google Scholar] [CrossRef] [Green Version]
- Van Velzen, P.; Brinkman, P.; Knobel, H.H.; Van den Berg, J.W.K.; Jonkers, R.E.; Loijmans, R.J.; Prins, J.M.; Sterk, P.J. Exhaled Breath Profiles Before, During and After Exacerbation of COPD: A Prospective Follow-Up Study. COPD J. Chronic Obstr. Pulm. Dis. 2019, 16, 330–337. [Google Scholar] [CrossRef] [Green Version]
- Van der Schee, M.P.; Paff, T.; Brinkman, P.; Van Aalderen, W.M.C.; Haarman, E.G.; Sterk, P.J. Translating Basic Research Into Clinical Practice-Breathomics in Lung Disease. Chest 2015, 147, 224–231. [Google Scholar] [CrossRef]
- Chow, K.K.; Short, M.; Zeng, H. A comparison of spectroscopic techniques for human breath analysis. Biomed. Spectrosc. Imaging 2012, 1, 339–353. [Google Scholar] [CrossRef] [Green Version]
- Cazzola, M.; Segreti, A.; Capuano, R.; Bergamini, A.; Martinelli, E.; Calzetta, L.; Rogliani, P.; Ciaprini, C.; Ora, J.; Paolesse, R.; et al. Analysis of exhaled breath fingerprints and volatile organic compounds in COPD. COPD Res. Pract. 2015, 1, 7. [Google Scholar] [CrossRef] [Green Version]
- Antonelli Incalzi, R.; Pennazza, G.; Scarlata, S.; Santonico, M.; Petriaggi, M.; Chiurco, D.; Pedone, C.; D’Amico, A. Reproducibility and Respiratory Function Correlates of Exhaled Breath Fingerprint in Chronic Obstructive Pulmonary Disease. PLoS ONE 2012, 7, e45396. [Google Scholar] [CrossRef]
- De Vries, R.; Brinkman, P.; Van der Schee, M.P.; Fens, N.; Dijkers, E.; Bootsma, S.K.; De Jongh, F.H.C.; Sterk, P.J. Integration of electronic nose technology with spirometry: Validation of a new approach for exhaled breath analysis. J. Breath Res. 2015, 9, 046001. [Google Scholar] [CrossRef]
- Finamore, P.; Pedone, C.; Scarlata, S.; Di Paolo, A.; Grasso, S.; Santonico, M.; Pennazza, G.; Antonelli Incalzi, R. Validation of exhaled volatile organic compounds analysis using electronic nose as index of COPD severity. Int. J. Chronic Obstr. Pulm. Dis. 2018, 13, 1441–1448. [Google Scholar] [CrossRef] [Green Version]
- Van Oort, P.M.P.; De Bruin, S.; Weda, H.; Knobel, H.H.; Schultz, M.J.; Bos, L.D.; MARS Consortium. Exhaled Breath Metabolomics for the Diagnosis of Pneumonia in Intubated and Mechanically-Ventilated Intensive Care Unit (ICU)-Patients. Int. J. Mol. Sci. 2017, 18, 449. [Google Scholar] [CrossRef] [Green Version]
- Van Oort, P.M.P.; Nijsen, T.; Weda, H.; Knobel, H.; Dark, P.; Felton, T.; Rattray, N.J.W.; Lawal, O.; Ahmed, W.; Portsmouth, C.; et al. BreathDx—Molecular analysis of exhaled breath as a diagnostic test for ventilator–associated pneumonia: Protocol for a European multicentre observational study. BMC Pulm. Med. 2017, 17, 1. [Google Scholar] [CrossRef] [Green Version]
- Filipiak, W.; Sponring, A.; Baur, M.M.; Filipiak, A.; Ager, C.; Wiesenhofer, H.; Nagl, M.; Troppmair, J.; Amann, A. Molecular analysis of volatile metabolites released specifically by staphylococcus aureus and pseudomonas aeruginosa. BMC Microbiol. 2012, 12, 113. Available online: http://www.biomedcentral.com/1471-2180/12/113 (accessed on 23 January 2020). [CrossRef] [PubMed] [Green Version]
- Gao, J.; Zou, Y.; Wang, Y.; Wang, F.; Lang, L.; Wang, P.; Zhou, Y.; Ying, K. Breath analysis for noninvasively differentiating Acinetobacter baumannii ventilator-associated pneumonia from its respiratory tract colonization of ventilated patients. J. Breath Res. 2016, 10, 027102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shafiek, H.; Fiorentino, F.; Merino, J.L.; López, C.; Oliver, A.; Segura, J.; De Paul, I.; Sibila, O.; Agustí, A.; Cosío, B.G. Using the Electronic Nose to Identify Airway Infection during COPD Exacerbations. PLoS ONE 2015, 10, e0135199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schnabel, R.M.; Boumans, M.L.L.; Smolinska, A.; Stobberingh, E.E.; Kaufmann, R.; Roekaerts, P.M.H.J.; Bergmans, D.C.J.J. Electronic nose analysis of exhaled breath to diagnose ventilator associated pneumonia. Respir. Med. 2015, 109, 1454–1459. [Google Scholar] [CrossRef] [Green Version]
- Humphreys, L.; Orme, R.M.L.E.; Moore, P.; Charaklias, N.; Sahgal, N.; Planas Pont, N.; Magan, N.; Stone, N.; Kendall, C.A. Electronic nose analysis of bronchoalveolar lavage fluid. Eur. J. Clin. Investig. 2011, 41, 52–58. [Google Scholar] [CrossRef]
- Liao, Y.; Wang, Z.; Zhang, F.; Abbod, M.F.; Shih, C.; Shieh, J. Machine Learning Methods Applied to Predict Ventilator-Associated Pneumonia with Pseudomonas aeruginosa Infection via Sensor Array of Electronic Nose in Intensive Care Unit. Sensors 2019, 19, 1866. [Google Scholar] [CrossRef] [Green Version]
- Sibila, O.; Garcia-Bellmunt, L.; Giner, J.; Merino, J.L.; Suarez-Cuartin, G.; Torrego, A.; Solanes, I.; Castillo, D.; Valera, J.L.; Cosio, B.G.; et al. Identification of airway bacterial colonization by an electronic nose in Chronic Obstructive Pulmonary Disease. Respir. Med. 2014, 108, 1608–1614. [Google Scholar] [CrossRef] [Green Version]
- Van Geffen, W.H.; Bruins, M.; Kerstjens, H.A.M. Diagnosing viral and bacterial respiratory infections in acute COPD exacerbations by an electronic nose: A pilot study. J. Breath Res. 2016, 10, 036001. [Google Scholar] [CrossRef]
- Mansour, E.; Vishinkin, R.; Rihet, S.; Saliba, W.; Fish, F.; Sarfati, P.; Haick, H. Measurement of temperature and relative humidity in exhaled breath. Sens. Actuators B Chem. 2020, 304, 127371. [Google Scholar] [CrossRef]
- Popov, T.A.; Kralimarkova, T.Z.; Dimitrov, V.D. Measurement of exhaled breath temperature in science and clinical practice. Breathe 2012, 8, 187–192. [Google Scholar] [CrossRef] [Green Version]
- Niesters, M.; Mahajan, R.; Olofsen, E.; Boom, M.; Garcia del Valle, S.; Aarts, L.; Dahan, A. Validation of a novel respiratory rate monitor based on exhaled humidity. Br. J. Anaesth. 2012, 109, 981–989. [Google Scholar] [CrossRef] [Green Version]
- Caputo, N.D.; Oliver, M.; West, J.R.; Hackett, R.; Sakles, J.C. Use of End Tidal Oxygen Monitoring to Assess Preoxygenation During Rapid Sequence Intubation in the Emergency Department. Ann. Emerg. Med. 2019, 74, 410–415. [Google Scholar] [CrossRef]
- Casey, J.D.; Semler, M.W. Beginning of the End? End-tidal Oxygen as an Outcome in Airway Management Research. EClinicalMedicine 2019, 13, 10–11. [Google Scholar] [CrossRef] [PubMed]
- Arakawa, H.; Kaise, M.; Sumiyama, K.; Saito, S.; Suzuki, T.; Tajiri, H. Does pulse oximetry accurately monitor a patient’s ventilation during sedated endoscopy under oxygen supplementation? Singap. Med. J. 2013, 54, 212–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sensor | Technology | Accuracy | Sensing Range | Power Consumption | Comm. | Sensor Main Features Addressing Sensor Selection for the Breath Analyser Module |
|---|---|---|---|---|---|---|
| SprintIR | NDIR with flow through adapter | ±70 ppm +/− 5% of reading | 0–20% | 35 mW | UART | • Sensing range compatible with hypercapnia levels • Flow adapter cape with 1 inlet and 1 outlet compatible with sidestream connection to system • Application Note AN-128 for operating with Arduino |
| KE-25 | Galvanic cell | ±1% full scale | 0–100% | N/A | Analog (voltage) | • Suitable for medical applications • Linear output voltage signal relative to percent oxygen • No external power supply required for sensor operation • Virtually no influence from CO2 • Threaded top suitable for connection to sensor chamber • Low cost |
| SHT75 (T) | Proprietary CMOSens® | ±0.3 °C | −40 °C–123.8 °C | 90 µW (average) | I2C | • High accuracy • Attractive price-performance ratio • Easy replaceability (pin-type version) • Fully calibrated digital output • Low power consumption • High-end version |
| SHT75 (RH) | Proprietary CMOSens® | ±3.0% | 0–100% | |||
| AS-MLV-P2 | Metal-Oxide | N/A | 30 ppm–500 ppm (taken from CO sensitivity curve, T and RH not mentioned) | 34 mW (heating element at 320 °C) | Analog (Resistance) | • Miniaturized MEMS (micro electromechanical system) devices • High sensitivity to VOCs (AS-MLV-P2 and MICS-4514 (RED)) • High sensitivity to NO2 (MICS-4514 (OX) to catch those exhaled NO molecules, known inflammatory marker, converted in NO2 • Very low power consumption • Surface Mounting Device (SMD) package compatible with Printed Circuit Board Assembly (PCBA) • Compact and simple front-end (conditioning circuit based on buffered voltage divider) • Low cost (10–20 €) • Scarce selectivity compensated by sensor array with cross-sensitivities |
| MiCS-4514 (RED) | Metal-Oxide | N/A | 1 ppm to 1000 ppm (taken from CO sensitivity curve, 25 °C, 50% RH) | 88 mW (heating element) | Analog (Resistance) | |
| MiCS-4514 (OX) | Metal-Oxide | N/A | 0.05 ppm to 10 ppm (taken from NO2 sensitivity curve, 25 °C, 50% RH) | 50 mW (heating element) | Analog (Resistance) |
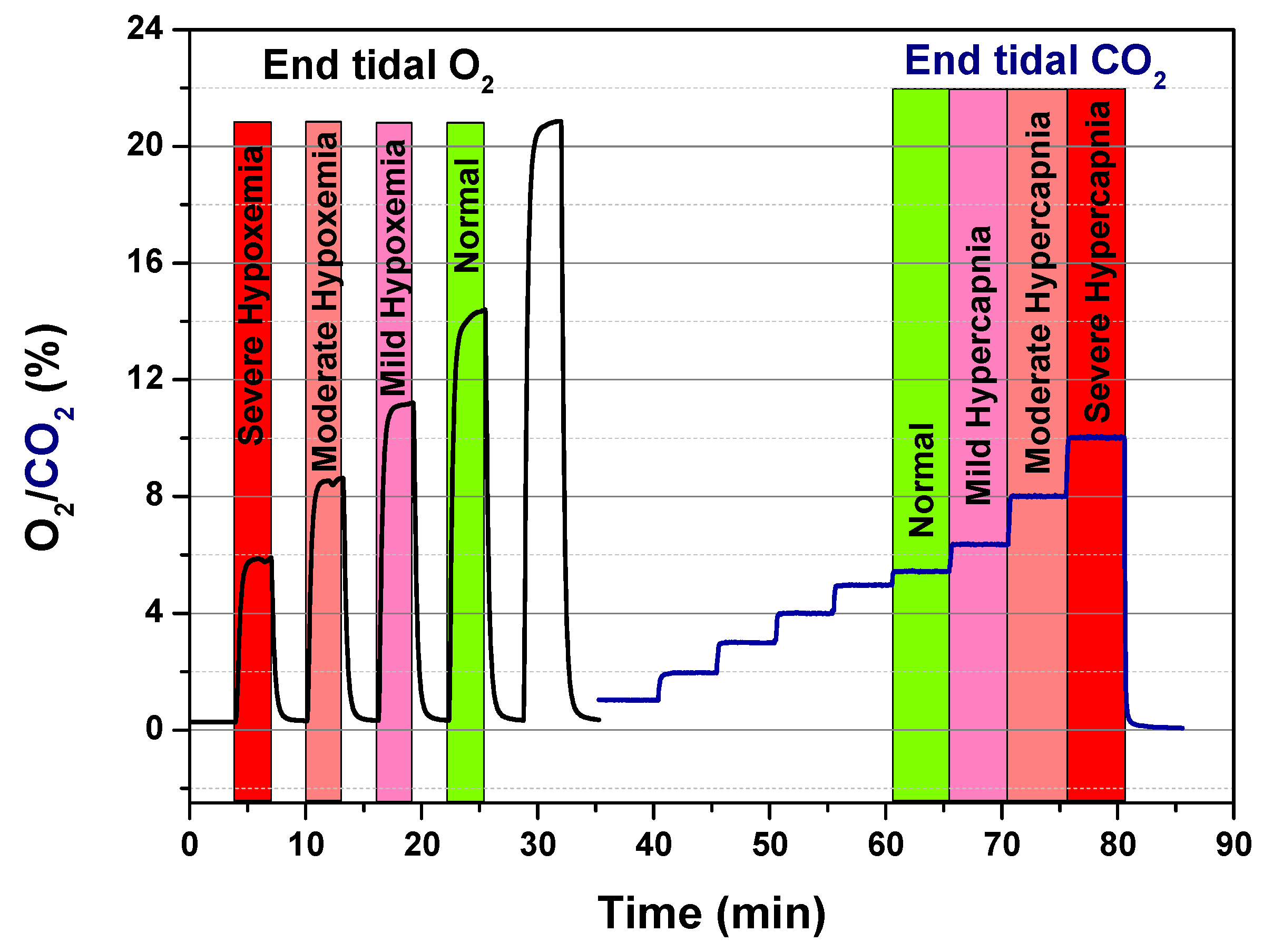
| (mmHg) | O2 (%) | |
| Normoxemia | 100 | 14.0 |
| Mild Hypoxemia | 60–80 | 8.41–11.22 |
| Moderate Hypoxemia | 40–60 | 5.61–8.41 |
| Severe Hypoxemia | <40 | <5.61 |
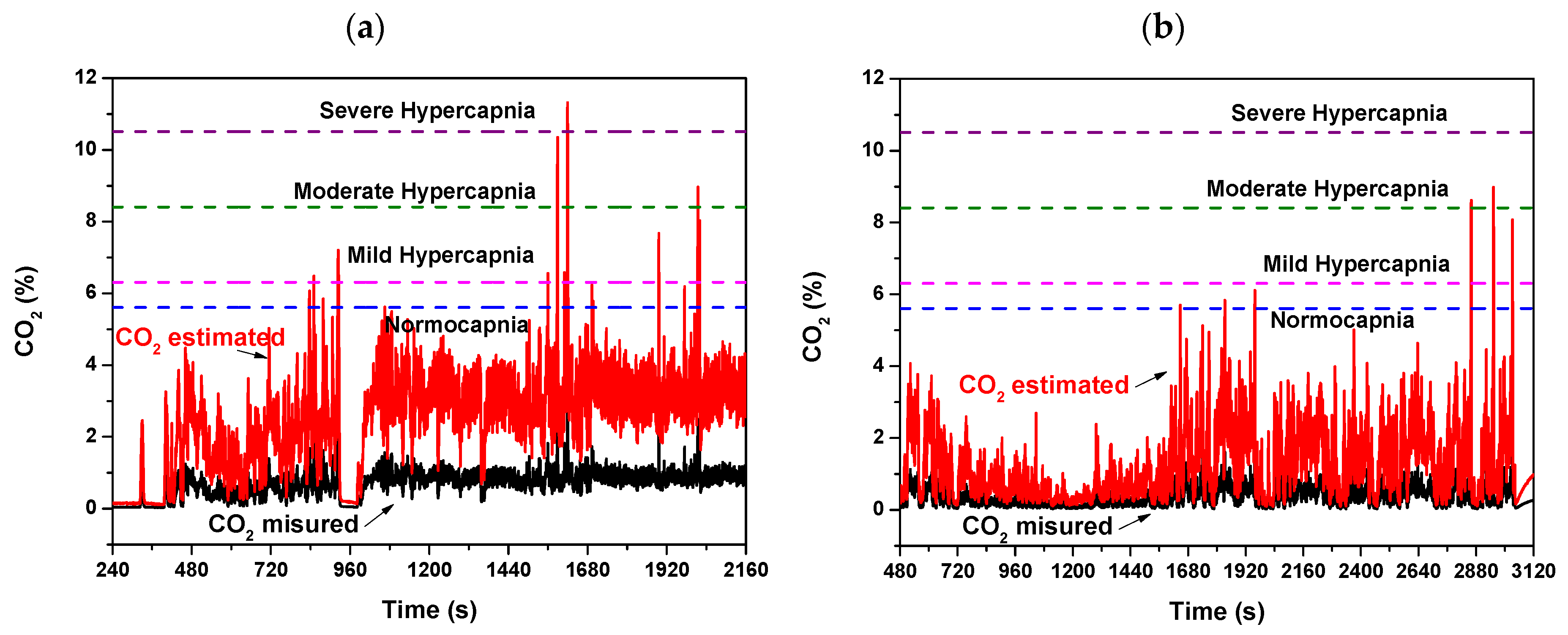
| (mmHg) | CO2 (%) | |
| Normocapnia | 40 | 5.61 |
| Mild Hypercapnia | 45–60 | 6.31–8.41 |
| Moderate HyperCapnia | 60–75 | 8.41–10.51 |
| Severe HyperCapnia | >75 | >10.51 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Radogna, A.V.; Siciliano, P.A.; Sabina, S.; Sabato, E.; Capone, S. A Low-Cost Breath Analyzer Module in Domiciliary Non-Invasive Mechanical Ventilation for Remote COPD Patient Monitoring. Sensors 2020, 20, 653. https://doi.org/10.3390/s20030653
Radogna AV, Siciliano PA, Sabina S, Sabato E, Capone S. A Low-Cost Breath Analyzer Module in Domiciliary Non-Invasive Mechanical Ventilation for Remote COPD Patient Monitoring. Sensors. 2020; 20(3):653. https://doi.org/10.3390/s20030653
Chicago/Turabian StyleRadogna, Antonio Vincenzo, Pietro Aleardo Siciliano, Saverio Sabina, Eugenio Sabato, and Simonetta Capone. 2020. "A Low-Cost Breath Analyzer Module in Domiciliary Non-Invasive Mechanical Ventilation for Remote COPD Patient Monitoring" Sensors 20, no. 3: 653. https://doi.org/10.3390/s20030653
APA StyleRadogna, A. V., Siciliano, P. A., Sabina, S., Sabato, E., & Capone, S. (2020). A Low-Cost Breath Analyzer Module in Domiciliary Non-Invasive Mechanical Ventilation for Remote COPD Patient Monitoring. Sensors, 20(3), 653. https://doi.org/10.3390/s20030653