Deep Learning-Based Upper Limb Functional Assessment Using a Single Kinect v2 Sensor


Abstract
:1. Introduction
2. Methods
2.1. Upper Limb Kinematic Modeling for Kinect v2
2.2. UWA Kinematic Modeling via 3D Motion Capture System
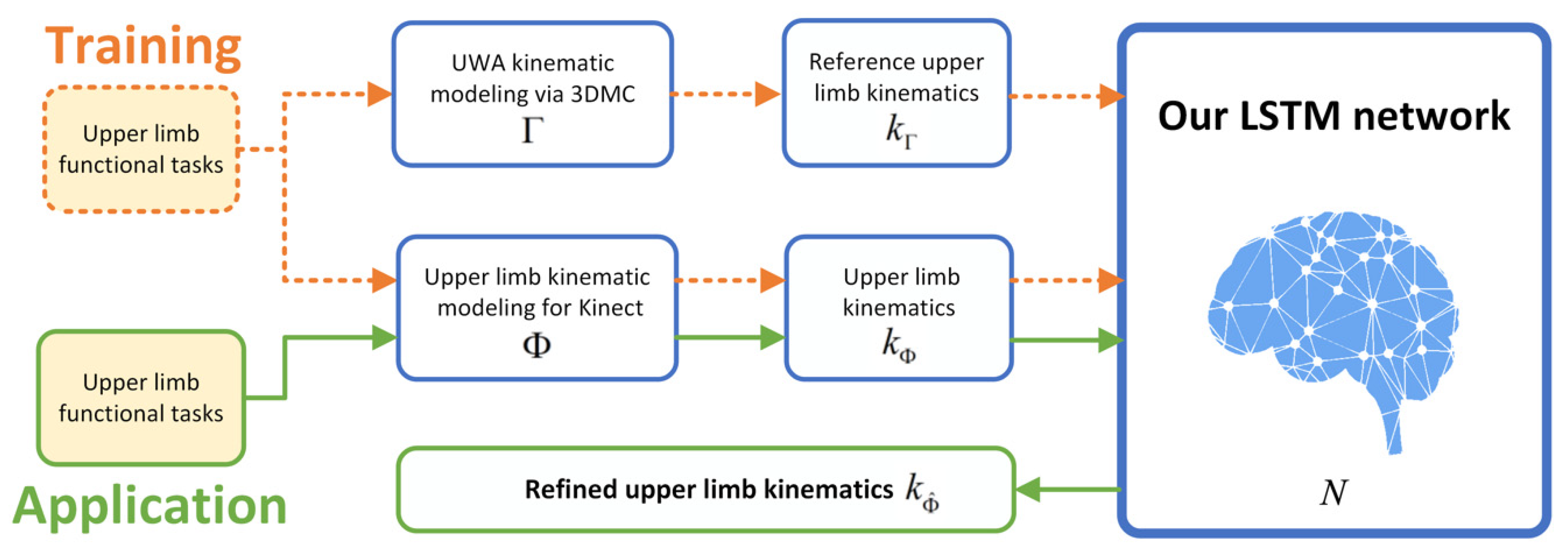
2.3. Long Short-Term Memory Neural Network
3. Evaluation
3.1. Subjects
3.2. Experiment Protocol
3.3. Leave One Subject Out Cross-Validation
3.4. Performance Evaluation and Statistical Analysis of the Deep Learning Refined Kinematic Model
4. Results
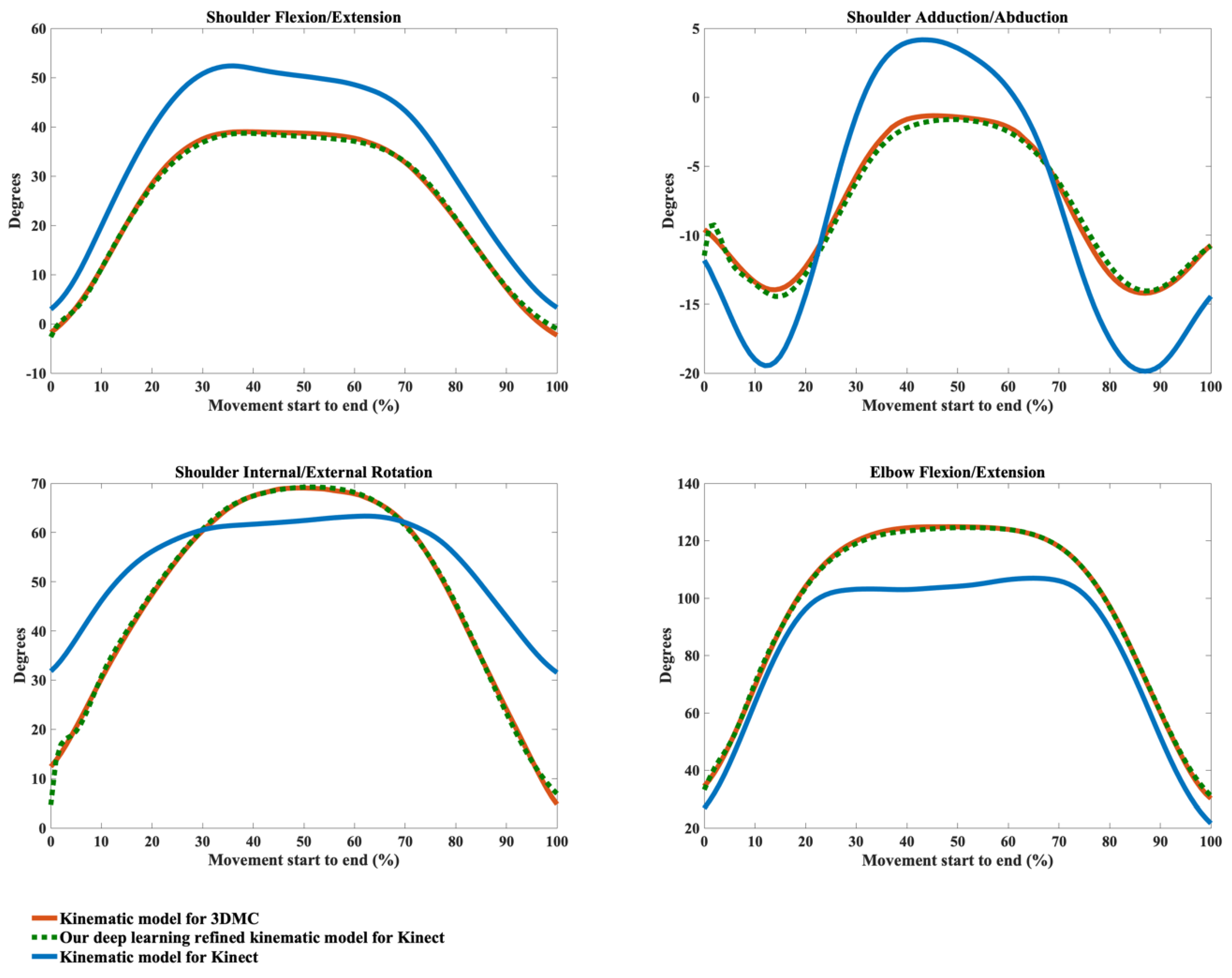
4.1. Joint Kinematic Waveforms Validity
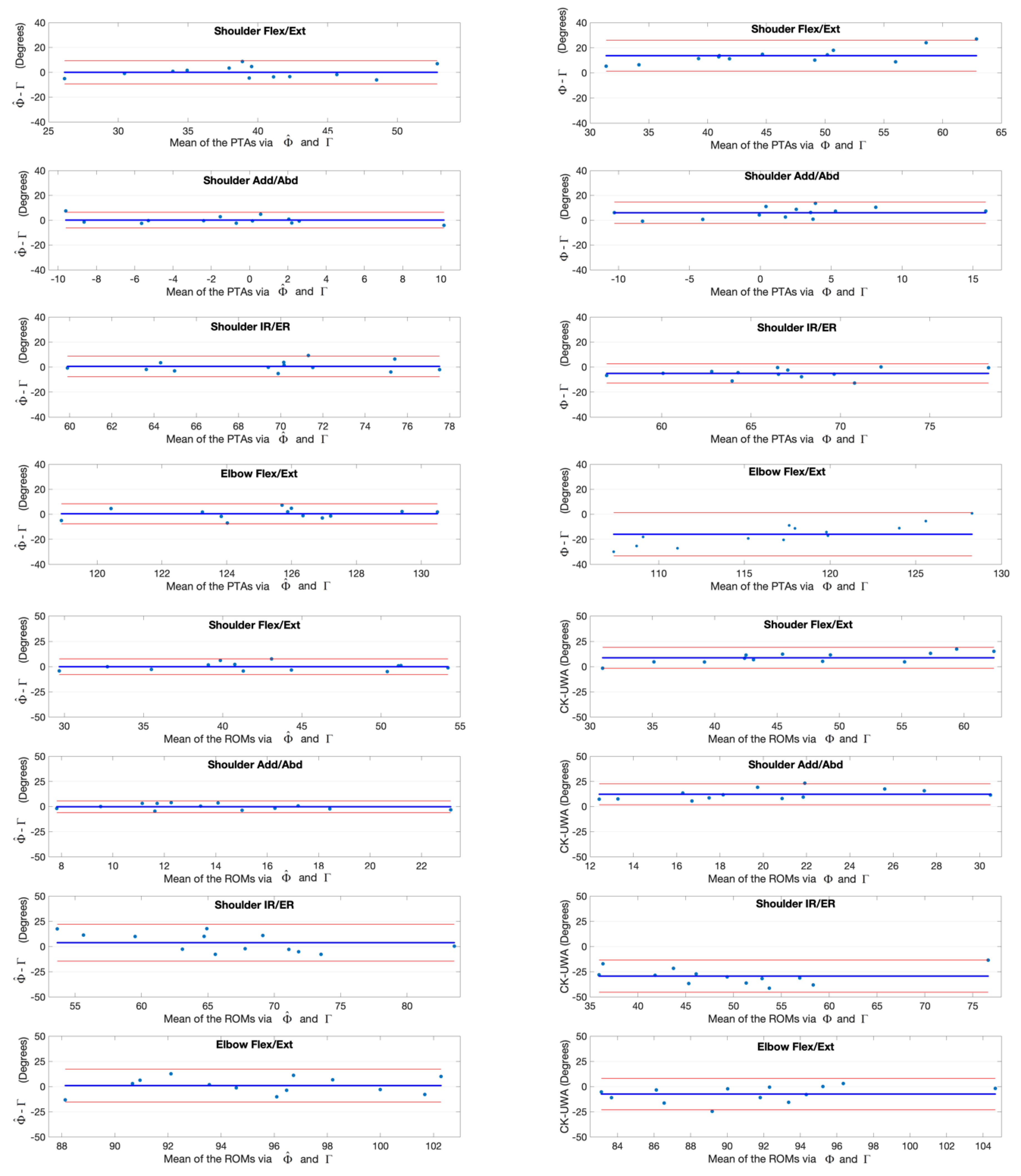
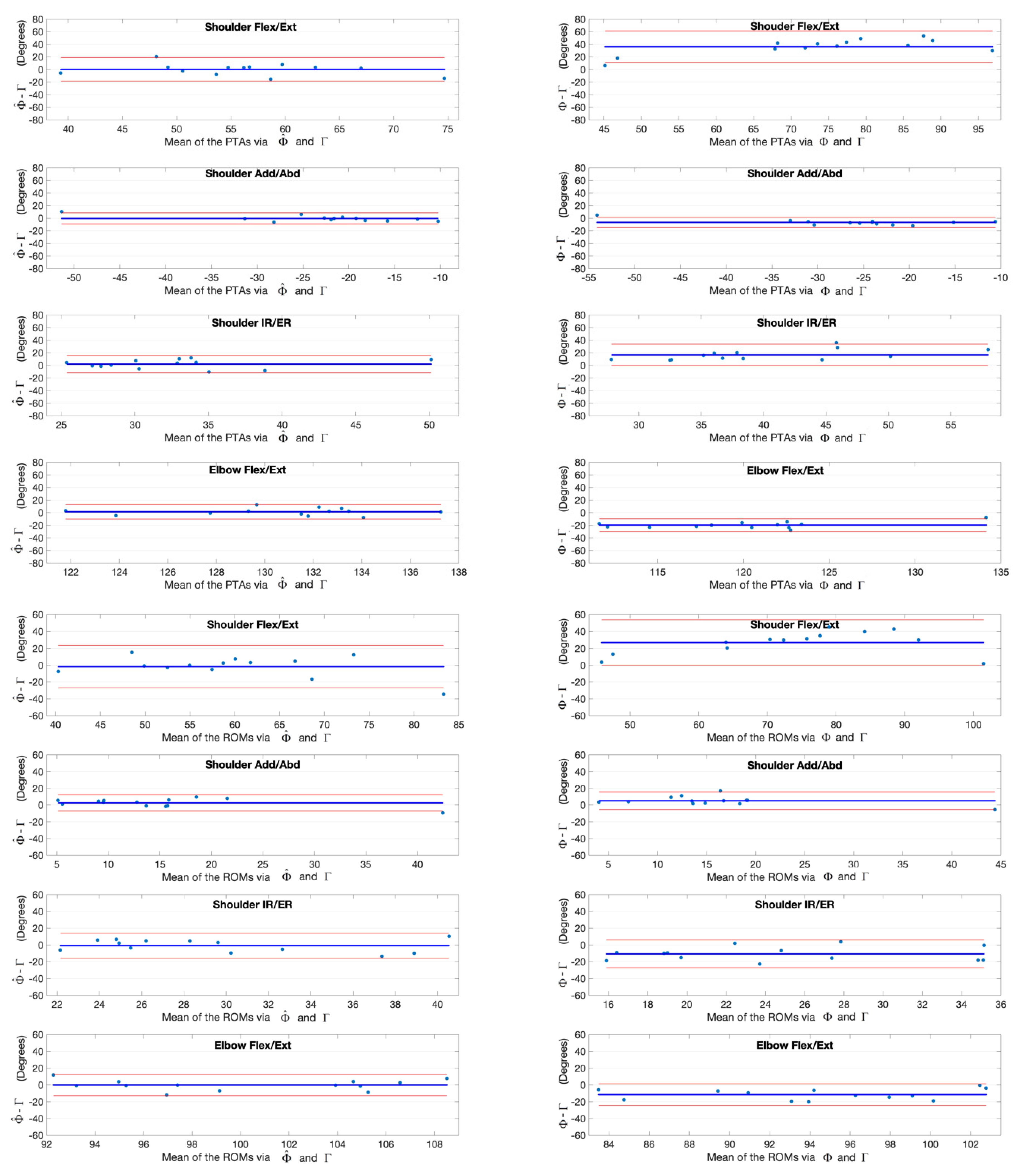
4.2. Joint Kinematic Variables Validity
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Dounskaia, N.; Ketcham, C.J.; Leis, B.C.; Stelmach, G.E. Disruptions in joint control during drawing arm movements in Parkinson’s disease. Exp. Brain Res. 2005, 164, 311–322. [Google Scholar] [CrossRef] [PubMed]
- Dounskaia, N.; Swinnen, S.; Walter, C.; Spaepen, A.; Verschueren, S. Hierarchical control of different elbow-wrist coordination patterns. Exp. Brain Res. 1998, 121, 239–254. [Google Scholar] [CrossRef] [PubMed]
- Reid, S.; Elliott, C.; Alderson, J.; Lloyd, D.; Elliott, B. Repeatability of upper limb kinematics for children with and without cerebral palsy. Gait Posture 2010, 32, 10–17. [Google Scholar] [CrossRef]
- Galna, B.; Barry, G.; Jackson, D.; Mhiripiri, D.; Olivier, P.; Rochester, L. Accuracy of the Microsoft Kinect sensor for measuring movement in people with Parkinson’s disease. Gait Posture 2014, 39, 1062–1068. [Google Scholar] [CrossRef] [Green Version]
- Hoy, M.G.; Zernicke, R.F. The role of intersegmental dynamics during rapid limb oscillations. J. Biomech. 1986, 19, 867–877. [Google Scholar] [CrossRef]
- Putnam, C.A. Sequential motions of body segments in striking and throwing skills: Descriptions and explanations. J. Biomech. 1993, 26, 125–135. [Google Scholar] [CrossRef]
- Zhou, H.; Hu, H. Human motion tracking for rehabilitation—A survey. Biomed. Signal Process. Control 2008, 3, 1–18. [Google Scholar] [CrossRef]
- Jaspers, E.; Feys, H.; Bruyninckx, H.; Cutti, A.; Harlaar, J.; Molenaers, G.; Desloovere, K. The reliability of upper limb kinematics in children with hemiplegic cerebral palsy. Gait Posture 2011, 33, 568–575. [Google Scholar] [CrossRef]
- Mündermann, L.; Corazza, S.; Andriacchi, T.P. The evolution of methods for the capture of human movement leading to markerless motion capture for biomechanical applications. J. Neuroeng. Rehabil. 2006, 3, 6. [Google Scholar] [CrossRef] [Green Version]
- Sarbolandi, H.; Lefloch, D.; Kolb, A. Kinect range sensing: Structured-light versus Time-of-Flight Kinect. Comput. Vis. Image Underst. 2015, 139, 1–20. [Google Scholar] [CrossRef] [Green Version]
- Shotton, J.; Sharp, T.; Kipman, A.; Fitzgibbon, A.; Finocchio, M.; Blake, A.; Cook, M.; Moore, R. Real-time human pose recognition in parts from single depth images. Commun. ACM 2013, 56, 116–124. [Google Scholar] [CrossRef] [Green Version]
- Wang, Q.; Kurillo, G.; Ofli, F.; Bajcsy, R. Evaluation of Pose Tracking Accuracy in the First and Second Generations of Microsoft Kinect. In Proceedings of the 2015 International Conference on Healthcare Informatics, Dallas, TX, USA, 21–23 October 2015; pp. 380–389. [Google Scholar]
- Latorre, J.; Llorens, R.; Colomer, C.; Alcañiz, M. Reliability and comparison of Kinect-based methods for estimating spatiotemporal gait parameters of healthy and post-stroke individuals. J. Biomech. 2018, 72, 268–273. [Google Scholar] [CrossRef] [PubMed]
- Pfister, A.; West, A.M.; Bronner, S.; Noah, J.A. Comparative abilities of Microsoft Kinect and Vicon 3D motion capture for gait analysis. J. Med. Eng. Technol. 2014, 38, 274–280. [Google Scholar] [CrossRef] [PubMed]
- Mentiplay, B.F.; Perraton, L.G.; Bower, K.J.; Pua, Y.H.; McGaw, R.; Heywood, S.; Clark, R.A. Gait assessment using the Microsoft Xbox One Kinect: Concurrent validity and inter-day reliability of spatiotemporal and kinematic variables. J. Biomech. 2015, 48, 2166–2170. [Google Scholar] [CrossRef] [PubMed]
- Clark, R.A.; Pua, Y.H.; Oliveira, C.C.; Bower, K.J.; Thilarajah, S.; McGaw, R.; Hasanki, K.; Mentiplay, B.F. Reliability and concurrent validity of the Microsoft Xbox One Kinect for assessment of standing balance and postural control. Gait Posture 2015, 42, 210–213. [Google Scholar] [CrossRef] [PubMed]
- Clark, R.A.; Pua, Y.H.; Fortin, K.; Ritchie, C.; Webster, K.E.; Denehy, L.; Bryant, A.L. Validity of the Microsoft Kinect for assessment of postural control. Gait Posture 2012, 36, 372–377. [Google Scholar] [CrossRef] [PubMed]
- Paolini, G.; Peruzzi, A.; Mirelman, A.; Cereatti, A.; Gaukrodger, S.; Hausdorff, J.M.; Croce, U.D. Validation of a Method for Real Time Foot Position and Orientation Tracking With Microsoft Kinect Technology for Use in Virtual Reality and Treadmill Based Gait Training Programs. IEEE Trans. Neural. Syst. Rehabil. Eng. 2014, 22, 997–1002. [Google Scholar] [CrossRef]
- Capecci, M.; Ceravolo, M.G.; Ferracuti, F.; Iarlori, S.; Longhi, S.; Romeo, L.; Russi, S.N.; Verdini, F. Accuracy evaluation of the Kinect v2 sensor during dynamic movements in a rehabilitation scenario. In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 5409–5412. [Google Scholar]
- Mateo, F.; Soria-Olivas, E.; Carrasco, J.J.; Bonanad, S.; Querol, F.; Pérez-Alenda, S. HemoKinect: A Microsoft Kinect V2 Based Exergaming Software to Supervise Physical Exercise of Patients with Hemophilia. Sensors 2018, 18, 2439. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Siebourgpolster, J.; Wolf, D.; Czech, C.; Bonati, U.; Fischer, D.; Khwaja, O.; Strahm, M. Feasibility of Using Microsoft Kinect to Assess Upper Limb Movement in Type III Spinal Muscular Atrophy Patients. PLoS ONE 2017, 12, e0170472. [Google Scholar] [CrossRef]
- Mobini, A.; Behzadipour, S.; Saadat, M. Test–retest reliability of Kinect’s measurements for the evaluation of upper body recovery of stroke patients. Biomed. Eng. Online 2015, 14, 75. [Google Scholar] [CrossRef] [Green Version]
- Chang, Y.J.; Chen, S.F.; Huang, J.D. A Kinect-based system for physical rehabilitation: A pilot study for young adults with motor disabilities. Res. Dev. Disabil. 2011, 32, 2566–2570. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.D. Kinerehab: A kinect-based system for physical rehabilitation: A pilot study for young adults with motor disabilities. In Proceedings of the 13th International ACM SIGACCESS Conference on Computers and Accessibility, Dundee Scotland, UK, 24–26 October 2011; pp. 319–320. [Google Scholar]
- Fuertes Muñoz, G.; Mollineda, R.A.; Gallardo Casero, J.; Pla, F. A RGBD-Based Interactive System for Gaming-Driven Rehabilitation of Upper Limbs. Sensors 2019, 19, 3478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vilas-Boas, M.d.C.; Choupina, H.M.P.; Rocha, A.P.; Fernandes, J.M.; Cunha, J.P.S. Full-body motion assessment: Concurrent validation of two body tracking depth sensors versus a gold standard system during gait. J. Biomech. 2019, 87, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; McGorry, R.W.; Chou, L.S.; Lin, J.; Chang, C. Accuracy of the Microsoft Kinect™ for measuring gait parameters during treadmill walking. Gait Posture 2015, 42, 145–151. [Google Scholar] [CrossRef] [Green Version]
- Cai, L.; Ma, Y.; Xiong, S.; Zhang, Y. Validity and Reliability of Upper Limb Functional Assessment Using the Microsoft Kinect V2 Sensor. Appl. Bionics Biomech. 2019, 2019, 7175240. [Google Scholar] [CrossRef] [Green Version]
- Mentiplay, B.F.; Hasanki, K.; Perraton, L.G.; Pua, Y.H.; Charlton, P.C.; Clark, R.A. Three-dimensional assessment of squats and drop jumps using the Microsoft Xbox One Kinect: Reliability and validity. J. Sports Sci. 2018, 36, 2202–2209. [Google Scholar] [CrossRef]
- Mentiplay, B.F.; Clark, R.A.; Mullins, A.; Bryant, A.L.; Bartold, S.; Paterson, K. Reliability and validity of the Microsoft Kinect for evaluating static foot posture. J. Foot Ankle Res. 2013, 6, 14. [Google Scholar] [CrossRef] [Green Version]
- Kobsar, D.; Osis, S.T.; Jacob, C.; Ferber, R. Validity of a novel method to measure vertical oscillation during running using a depth camera. J. Biomech. 2019, 85, 182–186. [Google Scholar] [CrossRef]
- Schmitz, A.; Ye, M.; Shapiro, R.; Yang, R.; Noehren, B. Accuracy and repeatability of joint angles measured using a single camera markerless motion capture system. J. Biomech. 2014, 47, 587–591. [Google Scholar] [CrossRef]
- Xu, X.; Robertson, M.; Chen, K.B.; Lin, J.; McGorry, R.W. Using the Microsoft Kinect™ to assess 3-D shoulder kinematics during computer use. Appl. Ergon. 2017, 65, 418–423. [Google Scholar] [CrossRef]
- Clark, R.A.; Mentiplay, B.F.; Hough, E.; Pua, Y.H. Three-dimensional cameras and skeleton pose tracking for physical function assessment: A review of uses, validity, current developments and Kinect alternatives. Gait Posture 2019, 68, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Sarsfield, J.; Brown, D.; Sherkat, N.; Langensiepen, C.; Lewis, J.; Taheri, M.; McCollin, C.; Barnett, C.; Selwood, L.; Standen, P.; et al. Clinical assessment of depth sensor based pose estimation algorithms for technology supervised rehabilitation applications. Int. J. Med. Inform. 2019, 121, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.B.; Park, Y.; Suh, I.H. Tracking human-like natural motion by combining two deep recurrent neural networks with Kalman filter. Intell. Serv. Robot. 2018, 11, 313–322. [Google Scholar] [CrossRef]
- Timmi, A.; Coates, G.; Fortin, K.; Ackland, D.; Bryant, A.L.; Gordon, I.; Pivonka, P. Accuracy of a novel marker tracking approach based on the low-cost Microsoft Kinect v2 sensor. Med. Eng. Phys. 2018, 59, 63–69. [Google Scholar] [CrossRef]
- Moon, S.; Park, Y.; Ko, D.W.; Suh, I.H. Multiple Kinect Sensor Fusion for Human Skeleton Tracking Using Kalman Filtering. Int. J. Adv. Robot. Syst. 2016, 13, 65. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Unka, J.; Liu, G. Contributions of joint rotations to ball release speed during cricket bowling: A three-dimensional kinematic analysis. J. Sports Sci. 2011, 29, 1293–1300. [Google Scholar] [CrossRef]
- LeCun, Y.; Bengio, Y.; Hinton, G.J. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef]
- Hochreiter, S.; Schmidhuber, J. Long short-term memory. Neural Comput. 1997, 9, 1735–1780. [Google Scholar] [CrossRef]
- Van Andel, C.J.; Wolterbeek, N.; Doorenbosch, C.A.; Veeger, D.H.; Harlaar, J. Complete 3D kinematics of upper extremity functional tasks. Gait Posture 2008, 27, 120–127. [Google Scholar] [CrossRef]
- Winter, D.A. Biomechanics and Motor Control of Human Movement; John Wiley & Sons: Hoboken, NJ, USA, 2009. [Google Scholar]
- Zhang, Y.; Lloyd, D.G.; Campbell, A.C.; Alderson, J.A. Can the effect of soft tissue artifact be eliminated in upper-arm internal-external rotation? J. Appl. Biomech. 2011, 27, 258–265. [Google Scholar] [CrossRef]
- Campbell, A.C.; Alderson, J.A.; Lloyd, D.G.; Elliott, B.C. Effects of different technical coordinate system definitions on the three dimensional representation of the glenohumeral joint centre. Med. Biol. Eng. Comput. 2009, 47, 543–550. [Google Scholar] [CrossRef] [PubMed]
- Campbell, A.; Lloyd, D.; Alderson, J.; Elliott, B. MRI development and validation of two new predictive methods of glenohumeral joint centre location identification and comparison with established techniques. J. Biomech. 2009, 42, 1527–1532. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.; Van der Helm, F.C.; Veeger, H.D.; Makhsous, M.; Van Roy, P.; Anglin, C.; Nagels, J.; Karduna, A.R.; McQuade, K.; Wang, X. ISB recommendation on definitions of joint coordinate systems of various joints for the reporting of human joint motion—Part II: Shoulder, elbow, wrist and hand. J. Biomech. 2005, 38, 981–992. [Google Scholar] [CrossRef] [PubMed]
- Cappozzo, A.; Catani, F.; Della Croce, U.; Leardini, A. Position and orientation in space of bones during movement: Anatomical frame definition and determination. Clin. Biomech. 1995, 10, 171–178. [Google Scholar] [CrossRef]
- Bartlett, R. Introduction to Sports Biomechanics: Analysing Human Movement Patterns; Routledge: Abington, UK, 2014. [Google Scholar]
- Kingma, D.P.; Ba, J. Adam: A method for stochastic optimization. In Proceedings of the International Conference on Learning Representations (ICLR), San Diego, CA, USA, 7–9 May 2015. [Google Scholar]
- Dutta, T. Evaluation of the Kinect™ sensor for 3-D kinematic measurement in the workplace. Appl. Ergon. 2012, 43, 645–649. [Google Scholar] [CrossRef]
- Magermans, D.; Chadwick, E.; Veeger, H.; Van Der Helm, F. Requirements for upper extremity motions during activities of daily living. Clin. Biomech. 2005, 20, 591–599. [Google Scholar] [CrossRef]
- Stanger, C.A.; Anglin, C.; Harwin, W.S.; Romilly, D.P. Devices for assisting manipulation: A summary of user task priorities. IEEE Trans. Rehabil. Eng. 1994, 2, 256–265. [Google Scholar] [CrossRef]
- Anglin, C.; Wyss, U. Review of arm motion analyses. J. Eng. Med. 2000, 214, 541–555. [Google Scholar] [CrossRef]
- Mosqueda, T.; James, M.A.; Petuskey, K.; Bagley, A.; Abdala, E.; Rab, G. Kinematic assessment of the upper extremity in brachial plexus birth palsy. J. Pediatr. Orthop. 2004, 24, 695–699. [Google Scholar] [CrossRef]
- Van Ouwerkerk, W.; Van Der Sluijs, J.; Nollet, F.; Barkhof, F.; Slooff, A. Management of obstetric brachial plexus lesions: State of the art and future developments. Children’s Nerv. Syst. 2000, 16, 638–644. [Google Scholar] [CrossRef]
- Kadaba, M.; Ramakrishnan, H.; Wootten, M.; Gainey, J.; Gorton, G.; Cochran, G. Repeatability of kinematic, kinetic, and electromyographic data in normal adult gait. J. Orthop. Res. 1989, 7, 849–860. [Google Scholar] [CrossRef] [PubMed]
- Garofalo, P.; Cutti, A.G.; Filippi, M.V.; Cavazza, S.; Ferrari, A.; Cappello, A.; Davalli, A. Inter-operator reliability and prediction bands of a novel protocol to measure the coordinated movements of shoulder-girdle and humerus in clinical settings. Med. Biol. Eng. Comput. 2009, 47, 475–486. [Google Scholar] [CrossRef] [PubMed]
- Hassan, E.A.; Jenkyn, T.R.; Dunning, C.E. Direct comparison of kinematic data collected using an electromagnetic tracking system versus a digital optical system. J. Biomech. 2007, 40, 930–935. [Google Scholar] [CrossRef] [PubMed]
- McGinley, J.L.; Baker, R.; Wolfe, R.; Morris, M.E. The reliability of three-dimensional kinematic gait measurements: A systematic review. Gait Posture 2009, 29, 360–369. [Google Scholar]
- Morrey, B.; Askew, L.; Chao, E. A biomechanical study of normal functional elbow motion. J. Bone Jt. Surg. 1981, 63, 872–877. [Google Scholar] [CrossRef]
- Wu, G.; Siegler, S.; Allard, P.; Kirtley, C.; Leardini, A.; Rosenbaum, D.; Whittle, M.; D’Lima, D.D.; Cristofolini, L.; Witte, H. ISB recommendation on definitions of joint coordinate system of various joints for the reporting of human joint motion—Part I: Ankle, hip, and spine. J. Biomech. 2002, 35, 543–548. [Google Scholar] [CrossRef]
- Fong, D.T.P.; Hong, Y.; Chan, L.K.; Yung, P.S.H.; Chan, K.M. A Systematic Review on Ankle Injury and Ankle Sprain in Sports. Sports Med. 2007, 37, 73–94. [Google Scholar] [CrossRef] [Green Version]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Task 1 | Task 2 | Task 3 | Task 4 | ||
|---|---|---|---|---|---|
| Shoulder Flexion /Extension | 0.87 (0.99) | 0.73 (0.13) | 0.77 (0.13) | 0.92 (0.09) | |
| 0.97 (0.20) | 0.95 (0.06) | 0.97 (0.03) | 0.94 (0.08) | ||
| P value | 0.005 | 0.005 a | 0.001 a | 0.249 a | |
| Shoulder Adduction /Abduction | 0.84 (0.10) | 0.55 (0.27) | 0.74 (0.18) | 0.60 (0.22) | |
| 0.88 (0.16) | 0.72 (0.21) | 0.97 (0.02) | 0.79 (0.17) | ||
| P value | 0.133 a | 0.135 | 0.001 | 0.016 | |
| Shoulder Internal /External Rotation | 0.81 (0.10) | 0.64 (0.23) | 0.83 (0.07) | 0.65 (0.17) | |
| 0.98 (0.21) | 0.75 (0.21) | 0.89 (0.11) | 0.75 (0.17) | ||
| P value | 0.001 a | 0.281 | 0.002 a | 0.133 | |
| Elbow Flexion /Extension | 0.93 (0.53) | 0.92 (0.07) | 0.83 (0.07) | 0.83 (0.20) | |
| 0.99 (0.00) | 0.99 (0.01) | 0.99 (0.01) | 0.93 (0.06) | ||
| P value | 0.001 | 0.003 a | 0.001 a | 0.055 a |
| Task 1 | Task 2 | Task 3 | Task 4 | ||
|---|---|---|---|---|---|
| Shoulder Flexion /Extension | 10.54 (4.65) | 27.49 (11.38) | 41.73 (8.19) | 5.44 (2.91) | |
| 4.61 (1.75) | 8.18 (5.35) | 11.50 (7.25) | 4.39 (2.54) | ||
| P value | 0.001 | 0.003 | 0.000 | 0.256 | |
| Shoulder Adduction /Abduction | 5.53 (1.81) | 6.42 (2.41) | 11.91 (4.61) | 6.00 (2.16) | |
| 2.90 (1.42) | 3.88 (2.59) | 5.14 (1.83) | 3.04 (1.72) | ||
| P value | 0.004 | 0.019 | 0.000 | 0.000 | |
| Shoulder Internal /External Rotation | 12.80 (3.22) | 19.39 (6.76) | 31.45 (6.89) | 11.34 (3.44) | |
| 5.60 (2.00) | 7.15 (2.30) | 8.59 (2.91) | 6.16 (3.46) | ||
| P value | 0.000 | 0.000 | 0.000 | 0.001 | |
| Elbow Flexion /Extension | 14.96 (5.90) | 15.83 (4.90) | 25.83 (3.45) | 11.43 (7.10) | |
| 5.56 (1.18) | 7.74 (2.21) | 6.96 (2.92) | 6.53 (2.41) | ||
| P value | 0.000 | 0.000 | 0.000 | 0.028 a |
| Task 1 | Task 2 | Task 3 | Task 4 | ||
|---|---|---|---|---|---|
| Shoulder Flexion/Extension (Degrees) | 53.05 (12.02) | 92.37 (20.33) | 151.50 (9.96) | −40.30 (4.96) | |
| 39.37 (7.22) | 56.14 (11.29) | 107.68 (12.24) | −42.04 (3.77) | ||
| 39.35 (7.95) | 56.37 (8.83) | 105.89 (15.02) | −42.06 (5.56) | ||
| 13.70 (6.39) | 35.99 (15.59) | 45.61 (10.30) | 1.75 (4.27) | ||
| 0.02 (4.79) | −0.24 (9.52) | 1.79 (11.78) | 0.01 (4.21) | ||
| 0.000 | 0.000 a | 0.000 | 0.163 | ||
| 0.987 | 0.930 | 0.594 | 0.990 | ||
| Shoulder Adduction/Abduction (Degrees) | 4.74 (7.98) | −29.41 (9.11) | −55.39 (7.03) | −30.72 (8.56) | |
| −1.19 (4.82) | −23.20 (8.86) | −58.51 (5.68) | −23.39 (5.83) | ||
| −1.28 (6.15) | −22.78 (12.03) | −58.49 (8.30) | −23.72 (6.01) | ||
| 6.02 (4.38) | −6.63 (4.26) | 3.10 (5.60) | −7.00 (3.82) | ||
| 0.10 (3.22) | −0.42 (4.57) | −0.02 (5.21) | 0.33 (3.02) | ||
| 0.000 | 0.002 a | 0.069 | 0.000 | ||
| 0.913 | 0.382 a | 0.988 | 0.700 | ||
| Shoulder Internal/External Rotation (Degrees) | 64.15 (6.30) | 48.43 (11.38) | 52.93 (10.21) | 30.28 (7.98) | |
| 69.76 (5.76) | 33.84 (7.72) | 24.04 (11.88) | 36.46 (4.55) | ||
| 69.22 (5.30) | 31.82 (6.86) | 23.53 (13.20) | 37.89 (6.16) | ||
| −5.08 (3.94) | 16.61 (8.69) | 29.40 (7.55) | −7.61 (9.82) | ||
| 0.53 (4.20) | 2.02 (7.06) | 0.51 (6.97) | −1.43 (7.76) | ||
| 0.001 | 0.000 a | 0.000 | 0.706 | ||
| 0.655 | 0.320 a | 0.795 | 0.517 | ||
| Elbow Flexion/Extension (Degrees) | 109.09 (10.75) | 110.18 (7.49) | 112.17 (3.96) | 65.86 (18.30) | |
| 125.47 (4.18) | 131.26 (5.16) | 146.29 (4.21) | 79.11 (12.15) | ||
| 125.06 (3.42) | 130.05 (5.07) | 144.56 (3.49) | 78.66 (11.85) | ||
| −15.97 (8.83) | −19.87 (5.17) | −32.39 (4.16) | −12.80 (8.54) | ||
| 0.41 (4.07) | 1.21 (5.78) | 1.73 (2.79) | 0.44 (6.70) | ||
| 0.000 | 0.000 a | 0.000 | 0.000 | ||
| 0.723 | 0.466 | 0.045 | 0.816 |
| Task 1 | Task 2 | Task 3 | Task 4 | ||
|---|---|---|---|---|---|
| Shoulder Flexion/Extension (Degrees) | 51.38 (11.66) | 87.53 (19.63) | 146.30 (14.55) | 38.04 (5.78) | |
| 42.63 (7.73) | 60.57 (15.25) | 108.80 (13.44) | 33.87 (4.71) | ||
| 42.50 (7.90) | 58.83 (10.46) | 105.85 (16.30) | 34.15 (5.63) | ||
| 8.88 (4.89) | 28.69 (12.50) | 40.44 (9.88) | 3.89 (2.76) | ||
| 0.13 (3.95) | 1.74 (12.91) | 2.95 (10.88) | −0.28 (3.19) | ||
| 0.000 | 0.000 | 0.000 | 0.000 | ||
| 0.905 | 0.636 | 0.348 | 0.422 a | ||
| Shoulder Adduction/Abduction (Degrees) | 26.26 (6.96) | 18.76 (8.61) | 40.37 (5.62) | 18.02 (7.76) | |
| 13.87 (3.88) | 16.28 (8.48) | 48.76 (5.53) | 12.93 (5.84) | ||
| 14.08 (4.76) | 13.71 (11.13) | 47.36 (7.61) | 12.97 (5.56) | ||
| 12.18 (5.33) | 5.05 (5.32) | −6.98 (7.27) | 5.05 (2.72) | ||
| 0.21 (2.97) | 2.57 (5.00) | 1.40 (4.86) | −0.04 (2.57) | ||
| 0.000 | 0.009 a | 0.000 | 0.000 | ||
| 0.802 | 0.075 a | 0.319 a | 0.861 a | ||
| Shoulder Internal/External Rotation (Degrees) | 35.16 (11.69) | 19.34 (8.35) | 56.44 (19.60) | 15.57 (6.92) | |
| 68.34 (6.47) | 29.17 (6.24) | 47.31 (15.41) | 24.06 (4.26) | ||
| 64.59 (11.25) | 30.07 (7.93) | 45.69 (15.98) | 22.92 (8.05) | ||
| −29.42 (8.16) | −10.73 (8.47) | 10.75 (10.39) | −7.35 (10.31) | ||
| 3.75 (9.33) | −0.90 (7.59) | 1.62 (7.94) | 1.14 (10.10) | ||
| 0.000 | 0.001 | 0.000 | 0.025 | ||
| 0.173 | 0.678 | 0.476 | 0.691 | ||
| Elbow Flexion/Extension (Degrees) | 87.54 (8.21) | 88.70 (7.41) | 87.57 (7.89) | 41.28 (21.06) | |
| 95.03 (5.77) | 100.19 (6.39) | 112.64 (4.22) | 48.93 (12.68) | ||
| 95.03 (5.77) | 100.29 (6.54) | 112.97 (8.97) | 47.82 (15.71) | ||
| −7.49 (7.94) | −11.59 (6.57) | −25.41 (6.84) | −6.54 (7.74) | ||
| 0.92 (8.33) | −0.10 (6.52) | −0.34 (7.55) | 1.11 (7.95) | ||
| 0.005 | 0.001 | 0.000 | 0.010 | ||
| 0.697 | 0.861 | 0.875 | 0.625 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ma, Y.; Liu, D.; Cai, L. Deep Learning-Based Upper Limb Functional Assessment Using a Single Kinect v2 Sensor. Sensors 2020, 20, 1903. https://doi.org/10.3390/s20071903
Ma Y, Liu D, Cai L. Deep Learning-Based Upper Limb Functional Assessment Using a Single Kinect v2 Sensor. Sensors. 2020; 20(7):1903. https://doi.org/10.3390/s20071903
Chicago/Turabian StyleMa, Ye, Dongwei Liu, and Laisi Cai. 2020. "Deep Learning-Based Upper Limb Functional Assessment Using a Single Kinect v2 Sensor" Sensors 20, no. 7: 1903. https://doi.org/10.3390/s20071903
APA StyleMa, Y., Liu, D., & Cai, L. (2020). Deep Learning-Based Upper Limb Functional Assessment Using a Single Kinect v2 Sensor. Sensors, 20(7), 1903. https://doi.org/10.3390/s20071903