Can We Accurately Measure Axial Segment Coordination during Turning Using Inertial Measurement Units (IMUs)?



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experiment Procedure
2.3. Data Acquisition
2.4. Data Processing and Data Analysis
2.4.1. Head and Thorax Data Processing
2.4.2. Step Analysis
2.5. Statistical Analysis
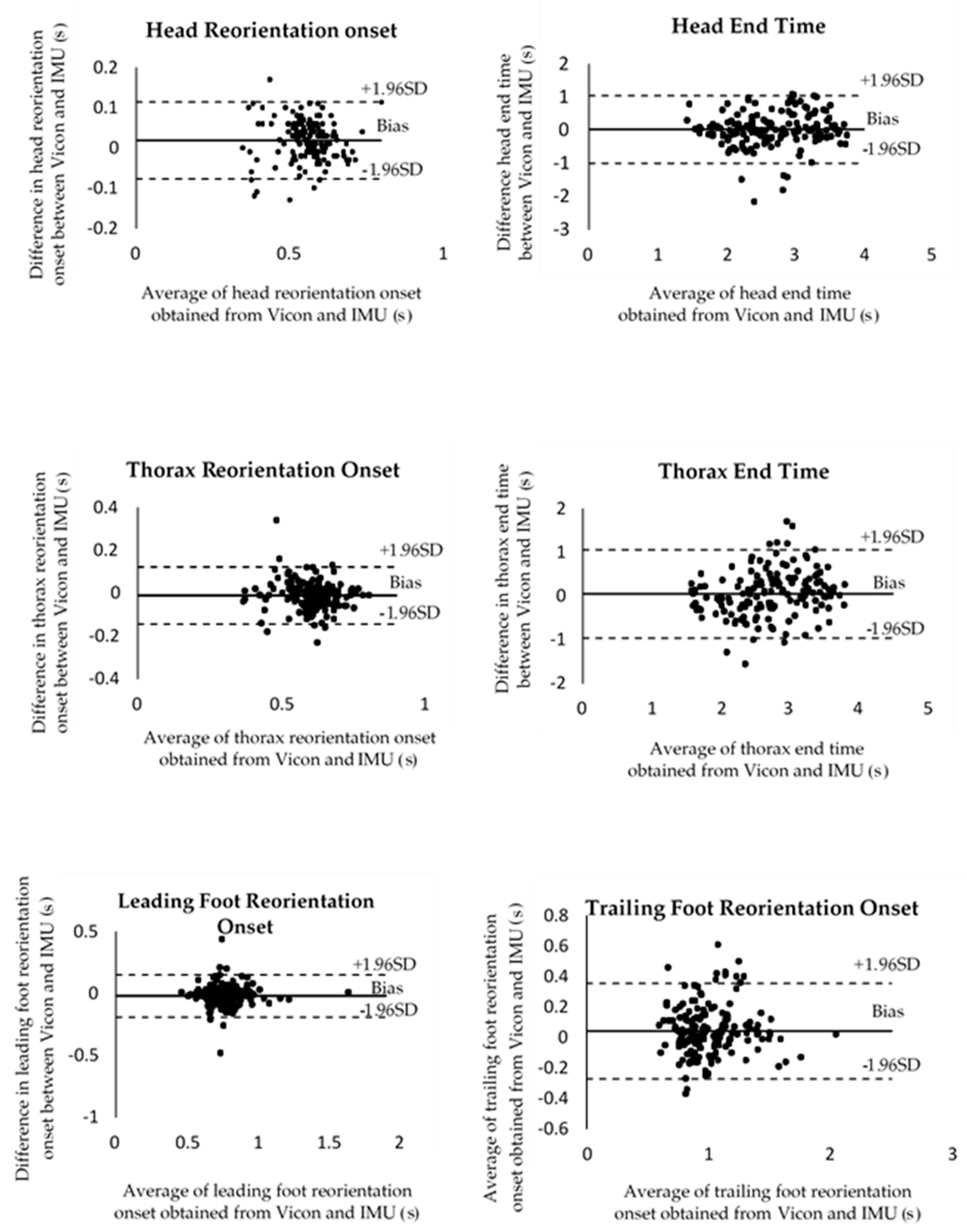
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Andriacchi, T.P.; Alexander, E.J. Studies of human locomotion: Past, present and future. J. Biomech. 2000, 33, 1217–1224. [Google Scholar] [CrossRef]
- Suciu, O.; Onofrei, R.R.; Totorean, A.D.; Suciu, S.C.; Amaricai, E.C. Gait analysis and functional outcomes after twelve-week rehabilitation in patients with surgically treated ankle fractures. Gait Posture 2016, 49, 184–189. [Google Scholar] [CrossRef] [PubMed]
- de Bruin, E.D.; Hubli, M.; Hofer, P.; Wolf, P.; Murer, K.; Zijlstra, W. Validity and reliability of accelerometer-based gait assessment in patients with diabetes on challenging surfaces. J. Aging Res. 2012, 2012, 954378. [Google Scholar] [CrossRef] [Green Version]
- Huxham, F.; Baker, R.; Morris, M.E.; Iansek, R. Head and trunk rotation during walking turns in Parkinson’s disease. Mov. Disord. 2008, 23, 1391–1397. [Google Scholar] [CrossRef]
- Morris, M.E.; Huxham, F.; McGinley, J.; Dodd, K.; Iansek, R. The biomechanics and motor control of gait in Parkinson disease. Clin. Biomech. 2001, 16, 459–470. [Google Scholar] [CrossRef]
- Stozek, J.; Rudzinska, M.; Pustulka-Piwnik, U.; Szczudlik, A. The effect of the rehabilitation program on balance, gait, physical performance and trunk rotation in Parkinson’s disease. Aging Clin. Exp. Res. 2016, 28, 1169–1177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartmann, A.; Luzi, S.; Murer, K.; de Bie, R.A.; de Bruin, E.D. Concurrent validity of a trunk tri-axial accelerometer system for gait analysis in older adults. Gait Posture 2009, 29, 444–448. [Google Scholar] [CrossRef]
- Picerno, P. 25 years of lower limb joint kinematics by using inertial and magnetic sensors: A review of methodological approaches. Gait Posture 2017, 51, 239–246. [Google Scholar] [CrossRef]
- Picerno, P.; Cereatti, A.; Cappozzo, A. Joint kinematics estimate using wearable inertial and magnetic sensing modules. Gait Posture 2008, 28, 588–595. [Google Scholar] [CrossRef]
- Seaman, A.; McPhee, J. Comparison of optical and inertial tracking of full golf swings. Procedia Eng. 2012, 34, 461–466. [Google Scholar] [CrossRef] [Green Version]
- Krüger, A.; Edelmann-Nusser, J. Application of a full body inertial measurement system in alpine skiing: A comparison with an optical video based system. J. Appl. Biomech. 2010, 26, 516–521. [Google Scholar] [CrossRef]
- Barrois, R.P.; Ricard, D.; Oudre, L.; Tlili, L.; Provost, C.; Vienne, A.; Vidal, P.; Buffat, S.; Yelnik, A.P. Observational study of 180 degrees turning strategies using inertial measurement units and fall risk in poststroke hemiparetic patients. Front. Neurol. 2017, 8, 194–204. [Google Scholar] [CrossRef] [Green Version]
- de Morais Faria, C.D.C.; de Carvalho-Pinto, B.P.; Nadeau, S.; Teixeira-Salmela, L.F. 180° turn while walking: Characterization and comparisons between subjects with and without stroke. J. Phys. Ther. Sci. 2016, 28, 2694–2699. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bertoli, M.; Croce, U.D.; Cereatti, A.; Mancini, M. Objective measures to investigate turning impairments and freezing of gait in people with Parkinson’s disease. Gait Posture 2019, 74, 187–193. [Google Scholar] [CrossRef]
- Robins, R.K.; Hollands, M.A. The effects of constraining vision and eye movements on whole-body coordination during standing turns. Exp. Brain Res. 2017, 235, 3593–3603. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Measuring agreement in method comparison studies. Stat. Methods Med. Res. 1999, 8, 135–160. [Google Scholar] [CrossRef] [PubMed]
- Giavarina, D. Understanding Bland Altman analysis. Biochem. Medica 2015, 25, 141–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fleiss, J.L. The Design and Analysis of Clinical Experiments; Wiley: Hoboken, NJ, USA, 1988; p. 304. [Google Scholar]
- Spildooren, J.; Vercruysse, S.; Heremans, E.; Galna, B.; Vandenbossche, J.; Desloovere, K.; Vandenberghe, W.; Nieuwboer, A. Head-pelvis coupling is increased during turning in patients with Parkinson’s disease and freezing of gait. Mov. Disord. 2013, 28, 619–625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brennan, A.; Zhang, J.; Deluzio, K.; Li, Q. Quantification of inertial sensor-based 3D joint angle measurement accuracy using an instrumented gimbal. Gait Posture 2011, 34, 320–323. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Segments | Coefficient of Determination (R2) | Gradient (m) | Intercept (c) | P-Value |
|---|---|---|---|---|
| Displacement (deg) | ||||
| Head | 0.999 | 1.021 | −0.078 | <0.001 |
| Thorax | 0.983 | 0.978 | 3.009 | <0.001 |
| Lt. Foot | 0.997 | 0.924 | 0.509 | <0.001 |
| Rt. Foot | 0.992 | 0.954 | 1.226 | <0.001 |
| Velocity (deg/s) | ||||
| Head | 0.968 | 1.018 | 0.0732 | <0.001 |
| Thorax | 0.777 | 0.685 | 15.589 | <0.001 |
| Lt. Foot | 0.884 | 0.848 | 1.473 | <0.001 |
| Rt. Foot | 0.856 | 0.805 | 3.010 | <0.001 |
| Variables | Vicon (Mean ± SD) | IMU (Mean ± SD) | ICC(2,4) | 95% CI | P-Value |
|---|---|---|---|---|---|
| Head reorientation onset (s) | 0.56 ± 0.07 | 0.55 ± 0.08 | 0.87 | 0.80–0.92 | 0.01 |
| Thorax reorientation onset (s) | 0.59 ± 0.08 | 0.60 ± 0.09 | 0.82 | 0.75–0.87 | 0.046 |
| Leading foot reorientation onset (s) | 0.77 ± 0.14 | 0.79 ± 0.14 | 0.89 | 0.85–0.92 | 0.030 |
| Trailing foot reorientation onset (s) | 1.03 ± 0.25 | 0.99 ± 0.25 | 0.88 | 0.83–0.91 | 0.047 |
| Head end time (s) | 2.68 ± 0.66 | 2.66 ± 0.62 | 0.80 | 0.73–0.86 | 0.579 |
| Thorax end time (s) | 2.71 ± 0.68 | 2.66 ± 0.57 | 0.80 | 0.72–0.85 | 0.240 |
| Peak head Yaw velocity (deg/s) | 193.93 ± 76.54 | 197.13 ± 59.36 | 0.88 | 0.83–0.91 | 0.357 |
| Peak head-thorax separation angle (deg) | 13.17 ± 11.02 | 15.05 ± 11.17 | 0.83 | 0.76–0.81 | 0.040 |
| Total steps (N) | 4.04 ± 1.02 | 4.05 ± 0.98 | 0.97 | 0.96–0.98 | 0.639 |
| Turn duration (s) | 2.55 ± 0.71 | 2.54 ± 0.88 | 0.88 | 0.83–0.91 | 0.151 |
| Step frequency (Hz) | 2.32 ± 0.74 | 2.20 ± 0.83 | 0.80 | 0.73–0.85 | 0.141 |
| Step size (deg) | 68.93 ± 26.44 | 69.00 ± 25.72 | 0.88 | 0.90–0.96 | 0.888 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khobkhun, F.; Hollands, M.A.; Richards, J.; Ajjimaporn, A. Can We Accurately Measure Axial Segment Coordination during Turning Using Inertial Measurement Units (IMUs)? Sensors 2020, 20, 2518. https://doi.org/10.3390/s20092518
Khobkhun F, Hollands MA, Richards J, Ajjimaporn A. Can We Accurately Measure Axial Segment Coordination during Turning Using Inertial Measurement Units (IMUs)? Sensors. 2020; 20(9):2518. https://doi.org/10.3390/s20092518
Chicago/Turabian StyleKhobkhun, Fuengfa, Mark A. Hollands, Jim Richards, and Amornpan Ajjimaporn. 2020. "Can We Accurately Measure Axial Segment Coordination during Turning Using Inertial Measurement Units (IMUs)?" Sensors 20, no. 9: 2518. https://doi.org/10.3390/s20092518
APA StyleKhobkhun, F., Hollands, M. A., Richards, J., & Ajjimaporn, A. (2020). Can We Accurately Measure Axial Segment Coordination during Turning Using Inertial Measurement Units (IMUs)? Sensors, 20(9), 2518. https://doi.org/10.3390/s20092518