
Modelling and Evaluation of the Absorption of the 866 MHz Electromagnetic Field in Humans Exposed near to Fixed I-RFID Readers Used in Medical RTLS or to Monitor PPE

 , ,
, , 
Abstract
:1. Introduction
1.1. The Internet of Things
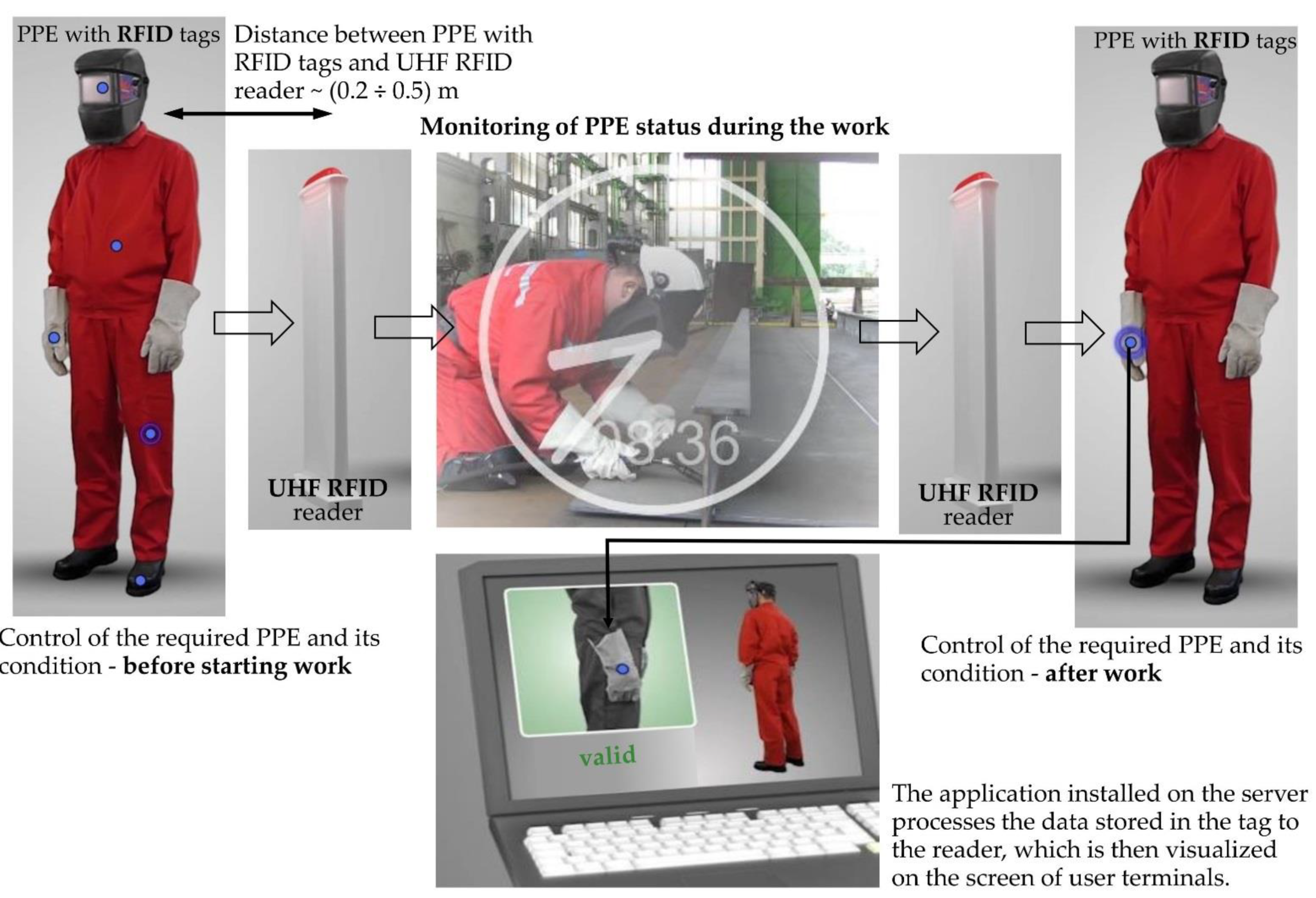
1.2. Examples of Real-Time Location Systems (RTLS) and Personal Protective Equipment (PPE) Monitoring Systems
1.3. The Metrics of Exposure to Radiofrequency EMF
1.4. The Aim
2. Materials and Methods
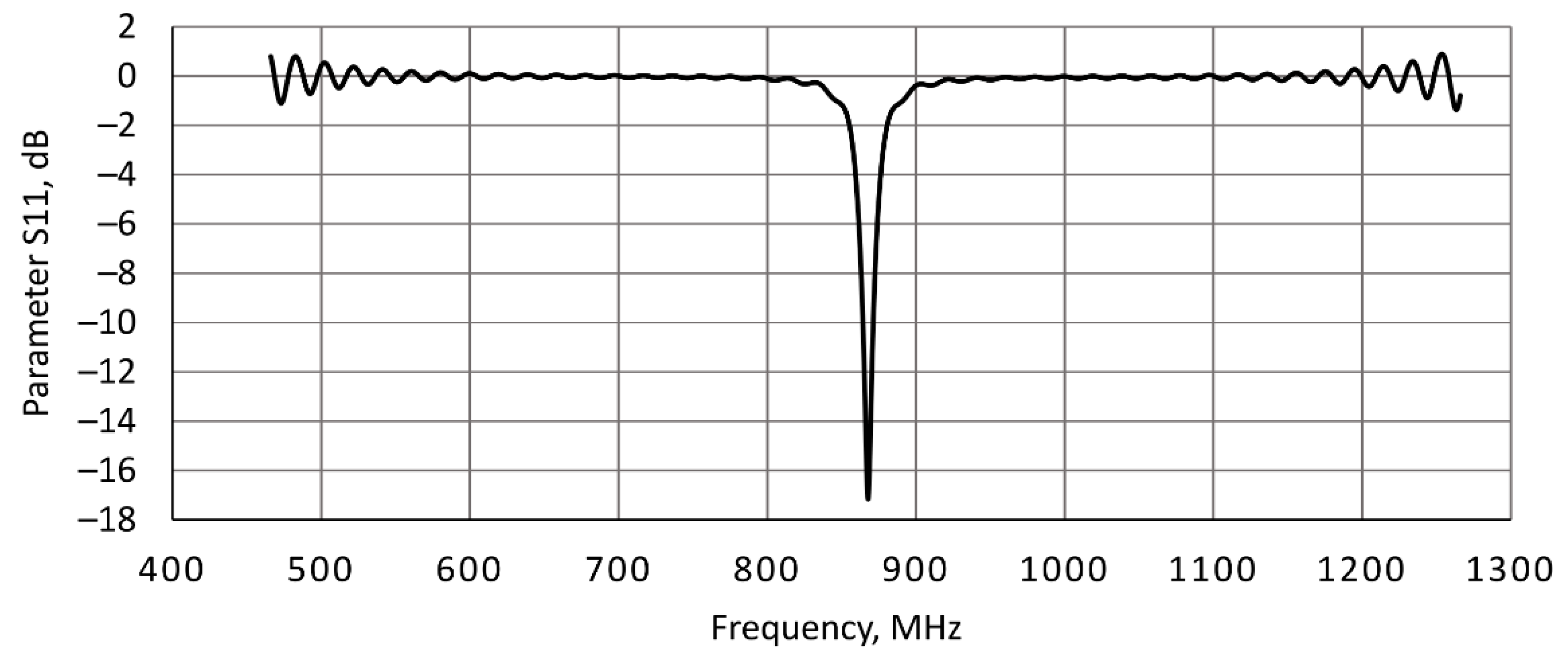
2.1. Numerical Model of the EMF Source
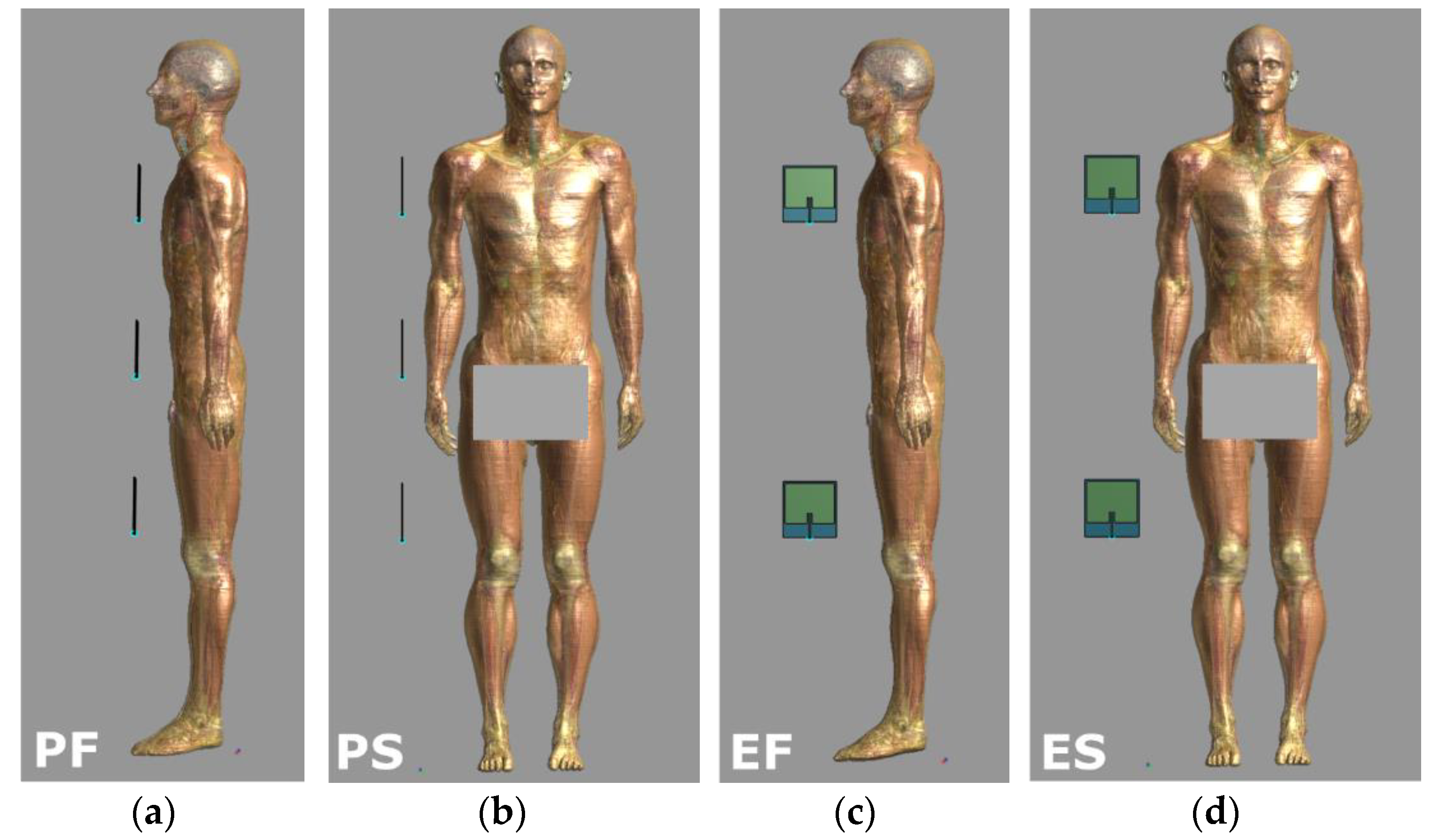
2.2. Exposure Scenarios
- Scenario PF—two or three antennas plane (P) located in front (F) of the human body;
- Scenario PS—two or three antennas plane (P) located to the side (S) of the human body;
- Scenario EF—two or three antennas side-on (E) located in front (F) of the human body;
- Scenario ES—two or three antennas side-on (E) located to the side (S) of the human body.
2.3. Numerical Model of Human Body
2.4. Numerical Simulations
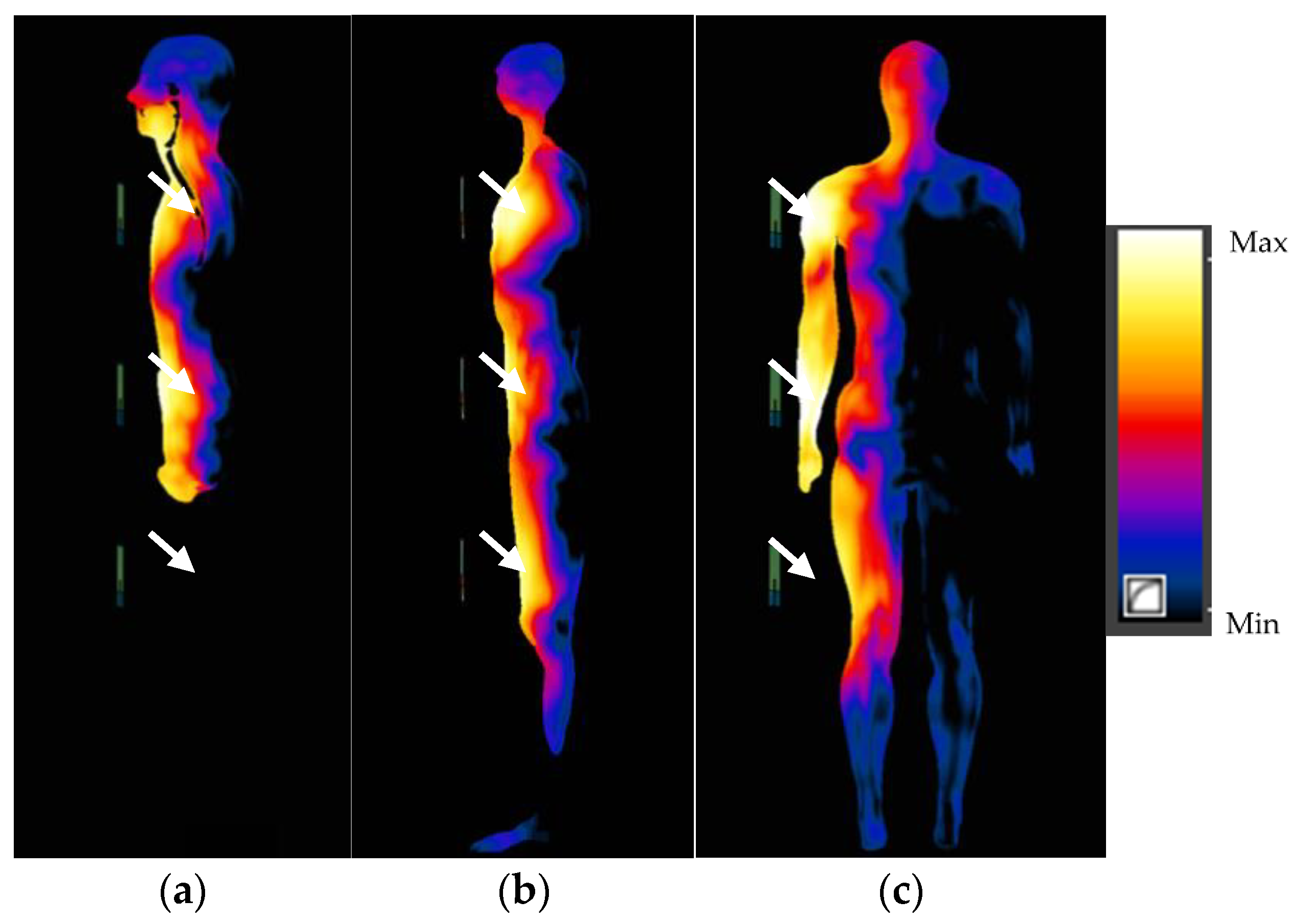
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aceto, G.; Persico, V.; Pescapé, A. The role of information and communication technologies in healthcare: Taxonomies, perspectives, and challenges. J. Netw. Comput. Appl. 2018, 107, 125–154. [Google Scholar] [CrossRef]
- Ashton, K. That ‘Internet of Things’ Thing. Available online: http://www.rfidjournal.com/articles/view?4986 (accessed on 28 April 2021).
- Aceto, G.; Persico, V.; Pescape, A. Industry 4.0 and Health: Internet of Things, Big Data, and Cloud Computing for Healthcare 4.0. J. Ind. Inf. Integr. 2020, 19, 100129. [Google Scholar] [CrossRef]
- Zradziński, P.; Karpowicz, J.; Gryz, K.; Ramos, V. Evaluation of electromagnetic exposure while using ultra-high frequency radiofrequency identification (UHF RFID) guns. Sensors 2020, 20, 202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finkenzeller, K. RFID Handbook. Fundamentals and Applications in Contactless Smart Cards, Radio Frequency Identification and Near-Field Communication, 3rd ed.; John Wiley & Sons, Ltd.: Chichester, UK, 2010; ISBN 978-0-470-69506-7. [Google Scholar]
- Salinas Gómez, F.; Suárez Escobar, N.E.; Vázquez, J. RFID + Wi-Fi system to control the location of biomedical equipment within hospital areas and linked to an intelligent inventory. Health Technol. 2020, 10, 479–483. [Google Scholar] [CrossRef]
- Sing, J.; Brar, N.; Fong, C. The State of RFID Applications in Libraries. Inf. Technol. Libr. 2006, 25, 24–32. [Google Scholar] [CrossRef] [Green Version]
- Butters, A. Radio Frequency Identification: An Introduction for Library Professionals. Australas Public Libr. Inf. Serv. 2006, 19, 164–174. [Google Scholar]
- Reiner, J.; Sullivan, M. RFID in Healthcare: A Panacea for the Regulations and Issues Affecting the Industry? UPS Supply Chain Solutions White Paper; United Parcel Service of America: Alpharetta, GA, USA, 2005; Available online: http://www.stitcs.com/en/RFID/RFID_in_healthcare.pdf (accessed on 28 April 2021).
- Hussain, M.; Amin, Y.; Lee, K.-G. A Compact and Flexible UHF RFID Tag Antenna for Massive IoT Devices in 5G System. Sensors 2020, 20, 5713. [Google Scholar] [CrossRef] [PubMed]
- Wielki, J. Internet Rzeczy i jego wpływ na modele biznesowe współczesnych organizacji gospodarczych [The Internet of Things and its effects on the business models of contemporary business organizations]. Studia Ekonomiczne. Zeszyty Naukowe Uniwersytetu Ekonomicznego w Katowicach 2016, 281, 208–219. [Google Scholar]
- Porter, M.E.; Heppelmann, J.E. How Smart, Connected Products Are Transforming Competition. Harv. Bus. Rev. 2014, 92, 64–88. [Google Scholar]
- Owczarek, G.; Hobaż, A.; Szkudlarek, J. The IoT and PPE. Data security in Smart PPE systems. Health Saf. Int. 2019, 81, 25–33. Available online: https://www.hsimagazine.com/press-release/iot-and-ppe/ (accessed on 28 April 2021).
- Dobbs, R.; Manyika, J.; Woetzel, J. No Ordinary Disruption. The Four Global Forces Breaking All the Trends; Public Affairs: New York, NY, USA, 2015. [Google Scholar]
- Kelm, A.; Laußat, L.; Meins-Becker, A.; Platz, D.; Khazaee, M.J.; Costin, A.M.; Helmus, M.; Teizer, J. Mobile passive Radio Frequency Identification (RFID) portal for automated and rapid control of Personal Protective Equipment (PPE) on construction sites. Automat. Constr. 2013, 36, 38–52. [Google Scholar] [CrossRef]
- Weizman, Y.; Tan, A.M.; Fuss, F.K. Use of wearable technology to enhance response to the Coronavirus (COVID-19) pandemic. Public Health 2020, 185, 221–222. [Google Scholar] [CrossRef] [PubMed]
- Gholamhosseini, L.; Sadoughi, F.; Safaei, A. Hospital Real-Time Location System (A Practical Approach in Healthcare): A Narrative Review Article. Iran. J. Public Health 2019, 48, 593–602. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.-Y.; Chen, J.-J.; Hsiang, T.-R. Design and Implementation of a Real-Time Object Location System Based on Passive RFID Tags. IEEE Sens. J. 2015, 15, 5015–5023. [Google Scholar] [CrossRef]
- Gralewicz, G. System automatycznej identyfikacji i zarządzania środkami ochrony indywidualnej w zakładzie pracy [Systems of automatic identification and management of personal protective equipment in the workplace]. Zarządzanie Przedsiębiorstwem 2014, 1, 31–36. [Google Scholar]
- Álvarez López, Y.; Franssen, J.; Álvarez Narciandi, G.; Pagnozzi, J.; González-Pinto Arrillaga, I.; Las-Heras Andrés, F. RFID Technology for Management and Tracking: E-Health Applications. Sensors 2018, 18, 2663. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). Environmental Health Criteria 137: Electromagnetic Fields (300 Hz–300 GHz); WHO: Geneva, Switzerland, 1993; Available online: http://www.inchem.org/documents/ehc/ehc/ehc137.htm (accessed on 7 June 2021).
- International Agency for Research on Cancer (IARC). IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. Non-Ionizing Radiation, Part. 2: Radiofrequency Electromagnetic Fields; IARC Press: Lyon, France, 2013; Volume 102, Available online: http://monographs.iarc.fr/ENG/Monographs/vol102/mono102.pdf (accessed on 7 June 2021).
- Scientific Committee on Emerging and Newly Identified Health Risks (SCENIHR). Opinion on Potential Health Effects of Exposure to Electromagnetic Fields (EMF); European Commission: Luxembourg, 2015; Available online: http://ec.europa.eu/health/sites/health/files/scientific_committees/emerging/docs/scenihr_o_041.pdf (accessed on 7 June 2021).
- World Health Organization (WHO). Research Agenda for Radiofrequency Fields; WHO: Geneva, Switzerland, 2010; Available online: http://www.who.int/peh-emf/research/agenda/en/index.html (accessed on 7 June 2021).
- European Commission. Horizon Europe-Work Programme 2021–2022. Draft of Annex 4. Health; European Commission: Brussels, Belgium, 2021; Available online: https://sciencebusiness.net/sites/default/files/inline-files/4.%20Health%20Vs6.4%20March.pdf (accessed on 7 June 2021).
- International Commission on Non-Ionizing Radiation Protection (ICNIRP). Guidelines for limiting exposure to time-varying electric, Magnetic, and electromagnetic fields (up to 300 GHz). Health Phys. 1998, 74, 494–522. [Google Scholar]
- International Commission on Non-Ionizing Radiation Protection (ICNIRP). Guidelines for limiting exposure to electromagnetic fields (100 kHz to 300 GHz). Health Phys. 2020, 118, 483–524. [Google Scholar] [CrossRef] [PubMed]
- Institute of Electrical and Electronics Engineers (IEEE) C95.1‐2019. IEEE Standard for Safety Levels with Respect to Human Exposure to Electric, Magnetic, and Electromagnetic Fields, 0 Hz to 300 GHz; IEEE: New York, NY, USA, 2019. [Google Scholar]
- Directive 2013/35/EU of the European Parliament and of the Council of 26 June 2013 on the minimum health and safety requirements regarding the exposure of workers to the risks arising from physical agents (electromagnetic fields) (20th individual Directive within the meaning of Article 16(1) of Directive 89/391/EEC) and repealing Directive 2004/40/EC. Off. J. Eur. Union 2013, L 179/1, 1–21.
- Zradziński, P.; Karpowicz, J.; Gryz, K. Electromagnetic Energy Absorption in a Head Approaching a Radiofrequency Identification (RFID) Reader Operating at 13.56 MHz in Users of Hearing Implants Versus Non-Users. Sensors 2019, 19, 3724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Directive 2014/53/EU of the European Parliament and of the Council of April 16, 2014 on the harmonization of the laws of the Member States relating to the making available on the market of radio equipment and repealing Directive 1999/5/EC Text with EEA relevance. Off. J. Eur. Union 2014, L 153, 62–106.
- European Committee for Electrotechnical Standardization (CENELEC) Final Draft CLC/FprTR 50713. Reasonably Foreseeable Use Conditions when referring to EMF Exposure Assessment; CENELEC: Brussels, Belgium, 2016. [Google Scholar]
- Zradziński, P. Examination of virtual phantoms with respect to their possible use in assessing compliance with the electromagnetic field exposure limits specified by Directive 2013/35/EU. Int. J. Occup. Med. Environ. Health 2015, 28, 781–792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- International Commission on Radiation Protection (ICRP). Adult Reference Computational Phantoms; ICRP Publication: Oxford, UK, 2009. [Google Scholar]
- Hasgall, P.A.; Di Gennaro, F.; Baumgartner, C.; Neufeld, E.; Lloyd, B.; Gosselin, M.C.; Payne, D.; Klingenböck, A.; Kuster, N. IT’IS Database for Thermal and Electromagnetic Parameters of Biological 492 tissues. Version 4.0. 2018. Available online: https://itis.swiss/virtual-population/tissue-properties/downloads/database-v4-0/ (accessed on 28 April 2021).
- International Electrotechnical Commission (IEC)/Institute of Electrical and Electronics Engineers (IEEE) 62704-1:2017. Determining the Peak Spatial-Average Specific Ab-Sorption Rate (SAR) in the Human Body from Wireless Communications Devices, 30 MHz to 6 GHz—Part. 1: General Requirements for Using the Finite-Difference Time-Domain (FDTD) Method for SAR Calculations; IEC: Geneva, Switzerland, 2017. [Google Scholar]
- DG INFSO & EPoSS. Internet of Things in 2020: A Roadmap for the Future. European Commission. Information Society and Media. 2008. Available online: https://docbox.etsi.org/erm/Open/CERP%2020080609-10/Internet-of-Things_in_2020_EC-EPoSS_Workshop_Report_2008_v1-1.pdf (accessed on 28 April 2021).
- Internet of Things–From Research and Innovation to Market Deployment. En: River Publisher Series in Communication. Ovidiu Vermesan, Peter Friess Editors. 2014. Available online: http://www.internet-of-things-research.eu/pdf/IERC_Cluster_Book_2014_Ch.3_SRIA_WEB.pdf (accessed on 28 April 2021).
- The Working Party on the Protection of Individuals with Regard to the Processing of Personal Data. Opinion 8/2014 on the on Recent Developments on the Internet of Things. 14/EN WP 223. Adopted on 16 September 2014. Available online: https://ec.europa.eu/justice/article-29/documentation/opinion-recommendation/files/2014/wp223_en.pdf (accessed on 28 April 2021).
- Zradziński, P.; Karpowicz, J.; Gryz, K.; Morzyński, I.; Młyński, R.; Swidziński, A.; Godziszewski, K.; Ramos, V. Modelling the Influence of Electromagnetic Field on the User of a Wearable IoT Device Used in a WSN for Monitoring and Reducing Hazards in the Work Environment. Sensors 2020, 20, 7131. [Google Scholar] [CrossRef] [PubMed]
- García, M.; Dolores, M.; Ramos, V. Administración segura de medicamentos en los nuevos escenarios electromagnéticos de Internet de las Cosas (IoT). Madrid; Instituto de Salud Carlos III, Unidad de Investigación en Telemedicina y e-Salud. 2018. Available online: http://gesdoc.isciii.es/gesdoccontroller?action=download&id=23/01/2019-940c2c0f70 (accessed on 28 April 2021).
- European Commission. Laws about Internet of Things. Completing a Trusted Digital Single Market for All (COM 2018). Available online: https://ec.europa.eu/digital-single-market/en/laws/76003/74243 (accessed on 28 April 2021).
- ITU–T. Internet of Things Global Standards Initiative. Available online: http://www.itu.int/en/ITU-T/gsi/iot/Pages/default.aspx (accessed on 28 April 2021).
- European Committee for Electrotechnical Standardization (CENELEC) EN 50527-1:2016. Procedure for the Assessment of the Exposure to Electromagnetic Fields of Workers Bearing Active Implantable Medical Devices—Part 1: General; CENELEC: Brussels, Belgium, 2016. [Google Scholar]
- European Committee for Electrotechnical Standardization (CENELEC) EN 60601-1-2:2015. Medical Electrical Equipment—Part. 1–2: General Requirements for Basic Safety and Essential Performance—Collateral Standard: Electromagnetic Disturbances—Requirements and Tests; CENELEC: Brussels, Belgium, 2015. [Google Scholar]
- European Telecommunications Standards Institute (ETSI) EN 302-208 V3.3.1 (2020-08). Radio Frequency Identification Equipment operating in Theband 865 MHz to 868 MHz with Power Levels Up to 2 W and in the Band 915 MHz to 921 MHz with Power Levels Up to 4 W; Harmonised Standard for Access to Radio Spectrum; ETSI: Sophia-Antipolis, France, 2016. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Exposure Scenario | Basic Restrictions/Dosimetric Reference Limits | EMF Frequency | ||
|---|---|---|---|---|
| Whole-Body Average WBSAR, W/kg | Local Head/Torso SAR10g, W/kg | Local Limb SAR10g, W/kg | ||
| Occupational/Person in restricted environments | 0.4 | 10 | 20 | 100 kHz to 6 GHz (ICNIRP 2020, IEEE 2019) 100 kHz to 10 GHz (ICNIRP 1998) 6 to 300 GHz (WBSAR only, ICNIRP 2020) |
| General public/Person in unrestricted environments | 0.08 | 2 | 4 | |
| Exposure Scenario 1 | WBSAR 2, W/kg | SAR10g 3, W/kg | ||||
|---|---|---|---|---|---|---|
| 5 cm | 20 cm | 40 cm | 5 cm | 20 cm | 40 cm | |
| 2 antennas, PF | 0.007 | 0.005 | 0.004 | 0.225 | 0.079 | 0.022 |
| 3 antennas, PF | 0.012 | 0.008 | 0.006 | 0.231 | 0.113 | 0.053 |
| 2 antennas, PS | 0.006 | 0.004 | 0.003 | 0.027 | 0.023 | 0.011 |
| 3 antennas, PS | 0.010 | 0.007 | 0.005 | 0.039 | 0.032 | 0.027 |
| 2 antennas, EF | 0.006 | 0.005 | 0.004 | 0.092 | 0.052 | 0.018 |
| 3 antennas, EF | 0.010 | 0.008 | 0.006 | 0.112 | 0.063 | 0.033 |
| 2 antennas, ES | 0.005 | 0.004 | 0.003 | 0.017 | 0.014 | 0.008 |
| 3 antennas, ES | 0.008 | 0.006 | 0.005 | 0.022 | 0.019 | 0.015 |
| Exposure Scenario 1 at WBSAR = 0.08 W/kg | Input Power to Each Antenna, W | ERP 2 Emitted from Each Antenna, W | ||||
|---|---|---|---|---|---|---|
| 5 cm | 20 cm | 40 cm | 5 cm | 20 cm | 40 cm | |
| 2 antennas, PF | 11 | 15 | 19 | 22 | 26 | 28 |
| 3 antennas, PF | 6.9 | 10 | 13 | 13 | 17 | 19 |
| 2 antennas, PS | 14 | 18 | 22 | 16 | 22 | 31 |
| 3 antennas, PS | 8.4 | 12 | 15 | 11 | 15 | 22 |
| 2 antennas, EF | 12 | 17 | 20 | 19 | 22 | 25 |
| 3 antennas, EF | 8.3 | 11 | 14 | 14 | 15 | 19 |
| 2 antennas, ES | 16 | 21 | 24 | 20 | 26 | 31 |
| 3 antennas, ES | 10 | 14 | 16 | 15 | 20 | 23 |
| Exposure Scenario 1 at SAR10g = 2 W/kg | Input Power to each Antenna, W | ERP 2 Emitted from each Antenna, W | ||||
|---|---|---|---|---|---|---|
| 5 cm | 20 cm | 40 cm | 5 cm | 20 cm | 40 cm | |
| 2 antennas, PF | 8.9 | 25 | 90 | 18 | 44 | 120 |
| 3 antennas, PF | 8.7 | 18 | 38 | 15 | 29 | 55 |
| 2 antennas, PS | 73 | 88 | 190 | 89 | 110 | 270 |
| 3 antennas, PS | 52 | 62 | 75 | 66 | 78 | 110 |
| 2 antennas, EF | 22 | 39 | 110 | 33 | 51 | 140 |
| 3 antennas, EF | 18 | 32 | 60 | 30 | 46 | 83 |
| 2 antennas, ES | 120 | 140 | 250 | 150 | 180 | 320 |
| 3 antennas, ES | 92 | 110 | 130 | 130 | 150 | 190 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zradziński, P.; Karpowicz, J.; Gryz, K.; Owczarek, G.; Ramos, V. Modelling and Evaluation of the Absorption of the 866 MHz Electromagnetic Field in Humans Exposed near to Fixed I-RFID Readers Used in Medical RTLS or to Monitor PPE. Sensors 2021, 21, 4251. https://doi.org/10.3390/s21124251
Zradziński P, Karpowicz J, Gryz K, Owczarek G, Ramos V. Modelling and Evaluation of the Absorption of the 866 MHz Electromagnetic Field in Humans Exposed near to Fixed I-RFID Readers Used in Medical RTLS or to Monitor PPE. Sensors. 2021; 21(12):4251. https://doi.org/10.3390/s21124251
Chicago/Turabian StyleZradziński, Patryk, Jolanta Karpowicz, Krzysztof Gryz, Grzegorz Owczarek, and Victoria Ramos. 2021. "Modelling and Evaluation of the Absorption of the 866 MHz Electromagnetic Field in Humans Exposed near to Fixed I-RFID Readers Used in Medical RTLS or to Monitor PPE" Sensors 21, no. 12: 4251. https://doi.org/10.3390/s21124251
APA StyleZradziński, P., Karpowicz, J., Gryz, K., Owczarek, G., & Ramos, V. (2021). Modelling and Evaluation of the Absorption of the 866 MHz Electromagnetic Field in Humans Exposed near to Fixed I-RFID Readers Used in Medical RTLS or to Monitor PPE. Sensors, 21(12), 4251. https://doi.org/10.3390/s21124251