
Wearable Robotic Gait Training in Persons with Multiple Sclerosis: A Satisfaction Study

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
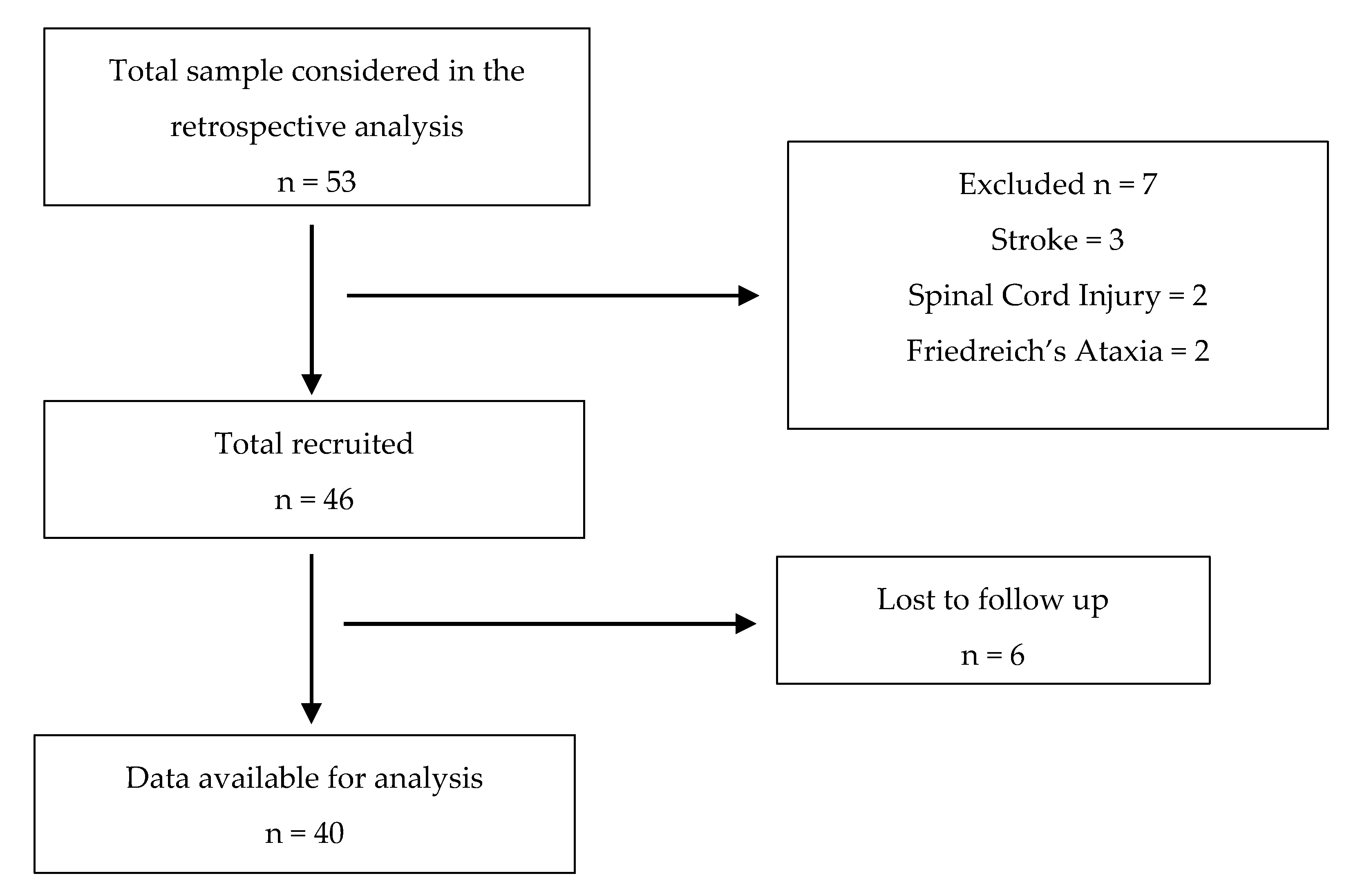
2.2. Participants
2.3. Sample Size
2.4. Outcomes Measures
2.5. Main Description of the Exoskeleton
2.6. Procedure of the Sessions
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Oh, J.; Vidal-Jordana, A.; Montalban, X. Multiple sclerosis: Clinical aspects. Curr. Opin. Neurol. 2018, 3, 752–759. [Google Scholar] [CrossRef]
- Liparoti, M.; Della Corte, M.; Rucco, R.; Sorrentino, P.; Sparaco, M.; Capuano, R.; Minino, R.; Lavorgna, L.; Agosti, V.; Sorrentino, G.; et al. Gait abnormalities in minimally disabled people with Multiple Sclerosis: A 3D-motion analysis study. Mult. Scler. Relat. Disord. 2019, 29, 100–107. [Google Scholar] [CrossRef]
- Rodríguez-Fernández, A.; Lobo-Prat, J.; Font-Llagunes, J.M. Systematic review on wearable lower-limb exoskeletons for gait training in neuromuscular impairments. J. Neuroeng. Rehabil. 2021, 18, 22. [Google Scholar] [CrossRef] [PubMed]
- Morone, G.; Paolucci, S.; Cherubini, A.; De Angelis, D.; Vincenzo, V.; Coiro, P.; Iosa, M. Robot-assisted gait training for stroke patients: Current state of the art and perspectives of robotics. Neuropsychiatr. Dis. Treat. 2017, 13, 1303–1311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Straudi, S.; Benedetti, M.G.; Venturini, E.; Manca, M.; Foti, C.; Basaglia, N. Does robot-assisted gait training ameliorate gait abnormalities in multiple sclerosis? A pilot randomized-control trial. NeuroRehabilitation 2013, 33, 555–563. [Google Scholar] [CrossRef] [PubMed]
- Straudi, S.; Fanciullacci, C.; Martinuzzi, C.; Pavarelli, C.; Rossi, B.; Chisari, C.; Basaglia, N. The effects of robot-assisted gait training in progressive multiple sclerosis: A randomized controlled trial. Mult. Scler. 2016, 22, 372–384. [Google Scholar] [CrossRef]
- Nam, K.Y.; Kim, H.J.; Kwon, B.S.; Park, J.W.; Lee, H.J.; Yoo, A. Robot-assisted gait training (Lokomat) improves walking function and activity in people with spinal cord injury: A systematic review. J. Neuroeng Rehabil. 2017, 14, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alamro, R.A.; Chisholm, A.E.; Williams, A.M.M.; Carpenter, M.G.; Lam, T. Overground walking with a robotic exoskeleton elicits trunk muscle activity in people with high-thoracic motor-complete spinal cord injury. J. Neuroeng. Rehabil. 2018, 15, 109. [Google Scholar] [CrossRef]
- McGibbon, C.A.; Sexton, A.; Jayaraman, A.; Deems-Dluhy, S.; Gryfe, P.; Novak, A. Evauation of the Keeoho exoskeleton for assisting ambulatory activities in people with multiple sclerosis: An open label randomized, cross-over trial. J. Neuroeng. Rehabil. 2018, 15, 117. [Google Scholar] [CrossRef]
- Fernández-Álvarez, L.G.; Núñez-Nagy, S.; Cano-de-la-Cuerda, R. Exoesqueletos portables en personas con lesión medular. Revisión sistemática. RIECS 2020, 5, 86–105. [Google Scholar] [CrossRef]
- Puyuelo, G.; Gil, A.; Cano-de-la-Cuerda, R. Eficacia del sistema robótico de entrenamiento de la marcha tipo lokomat en la rehabilitación de pacientes con lesión medular incompleta. una revisión sistemática. Rehabilitación 2017, 51, 182–190. [Google Scholar] [CrossRef]
- Ortiz, A.; Cano-de-la-Cuerda, R.; Ortiz, L.I.; Gil, A.M. Nuevas tecnologías en la reeducación de la marcha en pacientes con lesión medular incompleta. Una revisión sistemática. Rehabilitación 2015, 49, 90–101. [Google Scholar] [CrossRef]
- Høyer, E.; Opheim, A.; Jørgensen, V. Implementing the exoskeleton Ekso GTTM for gait rehabilitation in a stroke unit-feasibility, functional benefits and patient experiences. Disabil. Rehabil. Assist. Technol. 2020. [Google Scholar] [CrossRef]
- Lajeunesse, V.; Vincent, C.; Roithier, F.; Careau, E.; Michaud, F. Exoskeletons’ desing and usefulness evidence according to a systematic review of lower limb exoskeletons used for a functional mobility by people with spinal cord injury. Disabil. Rehabil. Assist. Technol. 2016, 11, 535–547. [Google Scholar] [CrossRef]
- Androwis, G.J.; Sandroff, B.M.; Niewrzol, P.; Fakhoury, F.; Wylie, G.R.; Yue, G.; DeLuca, J. A pilot randomized controlled trial of robotic exoskeleton-assisted exercise rehabilitation in multiple sclerosis. Mult. Scler. Relat. Disord. 2021, 51. [Google Scholar] [CrossRef]
- Berriozabalgoitia, R.; Bidaurrazaga-Letona, I.; Otxoa, E.; Urquiza, M.; Irazusta, J.; Rodriguez-Larrad, A. Overground Robotic Program Preserves Gait in Individuals with Multiple Sclerosis and Moderate to Severe Impairments: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2021, 102, 932–939. [Google Scholar] [CrossRef] [PubMed]
- Vandebroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Int. J. Surg. 2014, 12, 1500–1524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 2, 89–98. [Google Scholar] [CrossRef]
- Demers, L.; Weiss-Lambrou, R.; Ska, B. Development of the Quebec User Evaluation of Satisfaction with assistive Technology (QUEST). Assist. Technol. 1996, 8, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Larsen, D.L.; Attkisson, C.C.; Hargreaves, W.A.; Nguyen, T.D. Assessment of client/patient satisfaction: Development of a general scale. Eval. Program. Plann. 1979, 2, 197–207. [Google Scholar] [CrossRef]
- Hobart, J.C.; Riazi, A.; Lamping, D.L.; Fitzpatrick, R.; Thompson, A.J. Measuring the impact of MS on walking ability: The 12-Item MS Walking Scale (MSWS-12). Neurology 2003, 60, 31–36. [Google Scholar] [CrossRef]
- Fisk, J.D.; Ritvo, P.G.; Ross, L.; Haase, D.A.; Marrie, T.J.; Schlech, W.F. Measuring the functional impact of fatigue: Initial validation of the fatigue impact scale. Clin. Infect. Dis. 1994, 18, S79–S83. [Google Scholar] [CrossRef] [PubMed]
- Hobart, J.; Lamping, D.; Fitzpatrick, R.; Riazi, A.; Thompson, A. The Multiple Sclerosis Impact Scale (MSIS-29): A new patient-based outcome measure. Brain 2001, 124, 962–973. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Demers, L.; Monette, M.; Lapierre, Y.; Arnold, D.L.; Wolfson, C. Reliability, validity, and applicability of the Quebec User Evaluation of Satisfaction with assistive Technology (QUEST 2.0) for adults with multiple sclerosis. Disabil. Rehabil. 2002, 24, 21–30. [Google Scholar] [CrossRef]
- Vázquez, F.L.; Torres, A.; Otero, P.; Blanco, V.; Attkisson, C.C. Psychometric Properties of the Castilian Spanish Version of the Client Satisfaction Questionnaire (CSQ-8). Curr. Psychol. 2019, 38, 829–835. [Google Scholar] [CrossRef]
- Motl, R.W.; Snook, E.M. Confirmation and extension of the validity of the Multiple Sclerosis Walking Scale-12 (MSWS-12). J. Neurol Sci. 2008, 268, 69–73. [Google Scholar] [CrossRef]
- Khalil, H.; Al-Shorman, A.; Alghwiri, A.A.; Abdo, N.; El-Salem, K.; Shalabi, S.; Aburub, A. Cross cultural adaptation and psychometric evaluation of an Arabic version of the modified fatigue impact scale in people with multiple sclerosis. Mult. Scler. Relat. Disord. 2019. [Google Scholar] [CrossRef] [PubMed]
- Riazi, A.; Hobart, J.C.; Lamping, D.L.; Fitzpatrick, R.; Thompson, A.J. Multiple Sclerosis Impact Scale (MSIS-29): Reliability and validity in hospital based samples. J. Neurol. Neurosurg. Psychiatry 2002, 73, 701–704. [Google Scholar] [CrossRef]
- Pais-Ribeiro, J.L.; Martins da Silva, A.; Vilhena, E.; Moreira, I.; Santos, E.; Mendoça, D. The hospital anxiety and depression scale, in patients with multiple sclerosis. Neuropsychiatr. Dis. Treat. 2018, 14, 3193–3197. [Google Scholar] [CrossRef] [Green Version]
- Hobart, J.; Freeman, J.; Lamping, D.; Fitzpatrick, R.; Thompson, A. The SF-36 in multiple sclerosis: Why basic assumptions must be tested. J. Neurol. Neurosurg. Psychiatry 2001, 71, 363–370. [Google Scholar] [CrossRef] [Green Version]
- Sánchez-Villegas, A.; Martín-Calvo, N.; Gil-Conesa, M.; Martínez-González, M.A. Correlación y regresión lineal simple. In Bioestadística Amigable, 4th ed.; Martínez-González, M.A., Sánchez-Villegas, A., Toledo Atucha, E., Faulin Fajardo, J., Eds.; Elsevier: Barcelona, Spain, 2020; pp. 281–323. [Google Scholar]
- Corbianco, S.; Cavallini, G.; Dini, M.; Franzoni, F.; D’Avino, C.; Gerini, A.; Stampacchia, G. Energy cost and psychological impact of robotic-assisted gait training in people with spinal cord injury: Effect of two different types of devices. Neurol. Sci. 2021. [Google Scholar] [CrossRef]
- Puyuelo-Quintana, G.; Cano-de-la-Cuerda, R.; Plaza-Flores, A.; Garces-Castellote, E.; Sanz-Merodio, D.; Goñi-Arana, A.; Marín-Ojea, J.; García-Armada, E. A new lower limb portable exoskeleton for gait assistance in neurological patients: A proof of concept study. J. Neuroeng. Rehabil. 2020, 17, 60. [Google Scholar] [CrossRef] [PubMed]
- Kozlowski, A.J.; Fabian, M.; Lad, D.; Delgado, A.D. Feasibility and Safety of a Powered Exoskeleton for Assisted Walking for Persons with Multiple Sclerosis: A Single-Group Preliminary Study. Arch. Phys. Med. Rehabil. 2017, 98, 1300–1307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Awad, L.N.; Esquenazi, A.; Francisco, G.E.; Nolan, K.J.; Jayaraman, A. The ReWalk ReStore™ soft robotic exosuit: A multi-site clinical trial of the safety, reliability, and feasibility of exosuit-augmented post-stroke gait rehabilitation. J. Neuroeng. Rehabil. 2020, 17, 80. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Vargas, D.; Ballen-Moreno, F.; Barria, P.; Aguilar, R.; Azorín, J.M.; Munera, M.; Cifuentes, C.A. The Actuation System of the Ankle Exoskeleton T-FLEX: First Use Experimental Validation in People with Stroke. Brain Sci. 2021, 11, 412. [Google Scholar] [CrossRef] [PubMed]
- Platz, T.; Gillner, A.; Borgwaldt, N.; Kroll, S.; Roschka, S. Device-Training for Individuals with Thoracic and Lumbar Spinal Cord Injury Using a Powered Exoskeleton for Technically Assisted Mobility: Achievements and User Satisfaction. Biomed. Res. Int. 2016, 2016, 8459018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bortole, M.; Venkatakrishnan, A.; Zhu, F.; Moreno, J.C.; Francisco, G.E.; Pons, J.L.; Contreras-Vidal, J.L. The H2 robotic exoskeleton for gait rehabilitation after stroke: Early findings from a clinical study. J. Neuroeng. Rehabil. 2015, 12, 54. [Google Scholar] [CrossRef] [Green Version]
- Read, E.; Woolsey, C.; McGibbon, C.A.; O’Connell, C. Physiotherapists’ Experiences Using the Ekso Bionic Exoskeleton with Patients in a Neurological Rehabilitation Hospital: A Qualitative Study. Rehabil. Res. Pract. 2020. [Google Scholar] [CrossRef] [PubMed]
- Holanda, L.J.; Silva, P.M.M.; Amorim, T.C.; Lacerda, M.O.; Simão, C.R.; Morya, E. Robotic assisted gait as a tool for rehabilitation of individuals with spinal cord injury: A systematic review. J. Neuroeng. Rehabil. 2017, 14, 126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, L.E.; Zimmermann, A.K.; Herbert, W.G. Clinical effectiveness and safety of powered exoskeleton-assisted walking in patients with spinal cord injury: Systematic review with meta-analysis. Med. Devices 2016, 9, 455–466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehrholz, J.; Thomas, S.; Kugler, J.; Pohl, M.; Elsner, B. Electromechanical-assisted training for walking after stroke. Cochrane Database Syst. Rev. 2020, 10. [Google Scholar] [CrossRef]
- Kozlowski, A.J.; Bryce, T.N.; Dijkers, M.P. Time and Effort Required by Persons with Spinal Cord Injury to Learn to Use a Powered Exoskeleton for Assisted Walking. Top. Spinal Cord Inj. Rehabil. 2015, 21, 110–121. [Google Scholar] [CrossRef]
- Vaughan-Graham, J.; Brooks, D.; Rose, L.; Nejat, G.; Pons, J.; Patterson, K. Exoskeleton use in post-stroke gait rehabilitation: A qualitative study of the perspectives of persons post-stroke and physiotherapists. J. Neuroeng. Rehabil. 2020, 17, 123. [Google Scholar] [CrossRef]
- Colombo, R.; Pisano, F.; Mazzone, A.; Delconte, C.; Micera, S.; Carrozza, M.C.; Dario, P.; Minuco, G. Design strategies to improve patient motivation during robot-aided rehabilitation. J. Neuroeng. Rehabil. 2007, 4, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| How Much Do You Agree or Disagree with the Following Statements? | |
|---|---|
| 1. The amount of time spent adjusting to the device is short for clinical practice. | 1 2 3 4 5 |
| 2. Device settings can be correctly adjusted to the needs of each patient. | 1 2 3 4 5 |
| 3. The use of the device does not interfere with the supervision and protection of the patient during sessions. | 1 2 3 4 5 |
| 4. The device is compatible with other gait trainings. | 1 2 3 4 5 |
| 5. The device has a positive impact in the patients’ gait. | 1 2 3 4 5 |
| 6. The device is useful in clinical practice. | 1 2 3 4 5 |
| 7. The information provided by the device is easy to understand. | 1 2 3 4 5 |
| 8. The assistance provided by the device to correct the patients is clear (visual and sound feedback). | 1 2 3 4 5 |
| 9. I would recommend this device to other physiotherapists. | 1 2 3 4 5 |
| Measurement | Mean ± SD | Measurement | Mean ± SD |
|---|---|---|---|
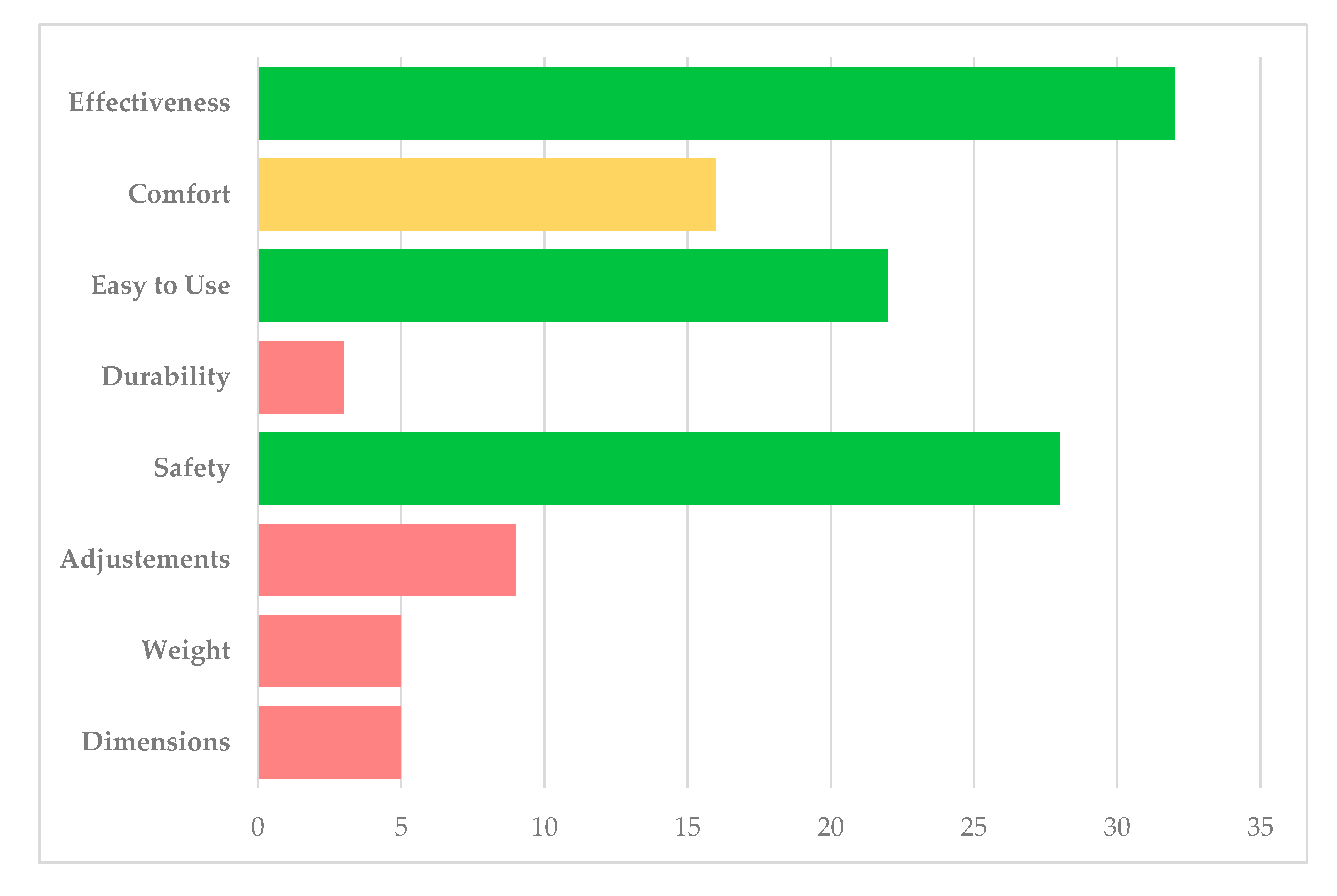
| MSWS | 46.33 ± 9.87 | QUEST 2.0 Dimensions | 4.08 ± 0.93 |
| MSIS Physical | 64.3 ± 18.24 | QUEST 2.0 Weight | 3.80 ± 0.95 |
| MSIS Psychological | 21.5 ± 7.38 | QUEST 2.0 Adjustments | 3.80 ± 1.00 |
| MSIS Total | 85.8 ± 23.28 | QUEST 2.0 Safety | 4.25 ± 0.89 |
| MFIS Physical | 24.78 ± 7.51 | QUEST 2.0 Durability | 3.98 ± 0.96 |
| MFIS Cognitive | 13.28 ± 9.56 | QUEST 2.0 Easy to Use | 3.73 ± 0.92 |
| MFIS Social | 4.33 ± 2.18 | QUEST 2.0 Comfort | 3.65 ± 1.04 |
| MFIS Total | 42.38 ± 16.18 | QUEST 2.0 Effectiveness | 4.03 ± 1.01 |
| SF36 Physical Functioning | 21.5 ± 20.61 | QUEST 2.0 Total (40) | 31.3 ± 5.70 |
| SF36 Physical Role | 42.34 ± 29.23 | CSQ8 | 26.28 ± 4.68 |
| SF36 Bodily Pain | 57.5 ± 27.15 | ||
| SF36 General Health | 35.75 ± 20.46 | ||
| SF36 Social Functioning | 63.44 ± 26.91 | ||
| SF36 Vitality | 37.5 ± 21.93 | ||
| SF36 Emotional Role | 82.5 ± 25.02 | ||
| SF36 Mental Health | 73.63 ± 17.10 | ||
| SF36 Total | 48.91 ± 15.48 | ||
| HADS Anxiety | 5.2 ± 3.32 | ||
| HADS Depression | 5.18 ± 3.23 | ||
| Questions | Mean ± SD | Gender | Age | Years NR | Years MS | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| rho | CI | p | rho | CI | p | rho | CI | p | rho | CI | p | ||
| Question 1 | 3.71 ± 0.88 | 0.394 | −0.173 to 0.765 | 0.163 | 0.151 | −0.413 to 0.631 | 0.607 | 0.372 | −0.198 to 0.754 | 0.190 | 0.227 | −0.345 to 0.676 | 0.434 |
| Question 2 | 4.29 ± 0.59 | 0.144 | −0.418 to 0.627 | 0.623 | 0.685 ** | 0.243 to 0.892 | 0.007 | 0.622 * | 0.136 to 0.867 | 0.018 | 0.655 * | 0.191 to 0.880 | 0.011 |
| Question 3 | 3.93 ± 0.96 | 0.477 | −0.071 to 0.804 | 0.084 | 0.224 | −0.348 to 0.674 | 0.442 | 0.317 | −0.257 to 0.725 | 0.270 | 0.133 | −0.428 to 0.620 | 0.651 |
| Question 4 | 4.71 ± 0.59 | 0.212 | −0.359 to 0.667 | 0.467 | 0.593 * | 0.091 to 0.855 | 0.026 | 0.723 ** | 0.312 to 0.906 | 0.003 | 0.580 * | 0.071 to 0.849 | 0.030 |
| Question 5 | 4.86 ± 0.35 | 0.167 | −0.399 to 0.641 | 0.569 | 0.564 * | 0.048 to 0.842 | 0.036 | 0.510 | −0.028 to 0.819 | 0.062 | 0.358 | −0.213 to 0.747 | 0.208 |
| Question 6 | 4.43 ± 0.62 | 0.396 | −0.170 to 0.766 | 0.161 | 0.175 | −0.392 to 0.646 | 0.549 | −0.021 | −0.546 to 0.515 | 0.943 | 0.298 | −0.276 to 0.716 | 0.300 |
| Question 7 | 4.00 ± 0.53 | 0.382 | −0.186 to 0.759 | 0.178 | −0.235 | −0.681 to 0.338 | 0.419 | 0.084 | −0.468 to0.588 | 0.777 | −0.050 | −0.566 to 0.493 | 0.864 |
| Question 8 | 4.00 ± 0.53 | 0.382 | −0.186 to 0.759 | 0.178 | 0.252 | −0.322 to 0.690 | 0.385 | 0.384 | −0.184 to 0.760 | 0.175 | −0.084 | −0.588 to 0.468 | 0.776 |
| Question 9 | 4.57 ± 0.62 | 0.300 | −0.275 to 0.716 | 0.298 | 0.517 | −0.018 to 0.822 | 0.058 | 0.525 | −0.007 to 0.826 | 0.054 | 0.456 | −0.098 to 0.794 | 0.101 |
| Age | Height | Weight | YearsD | EDSS | Sessions | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| QUEST 2.0 | rho | CI | p | rho | CI | p | rho | CI | p | rho | CI | p | rho | CI | p | rho | CI | p |
| Dimensions | 0.118 | −0.201 to 0.414 | 0.468 | −0.314 * | −0.570 to −0.003 | 0.049 | −0.384 * | −0.621 to −0.082 | 0.015 | 0.151 | −0.168 to 0.442 | 0.352 | 0.024 | −0.290 to 0.333 | 0.882 | 0.107 | −0.212 to 0.405 | 0.511 |
| Weight | 0.016 | −0.297 to 0.326 | 0.920 | −0.036 | −0.344 to 0.279 | 0.827 | 0.064 | −0.253 to 0.368 | 0.694 | 0.013 | −0.300 to 0.323 | 0.937 | 0.216 | −0.102 to 0.494 | 0.181 | 0.201 | −0.118 to 0.482 | 0.213 |
| Adjustments | 0.082 | −0.236 to 0.384 | 0.616 | −0.215 | −0.493 to 0.103 | 0.183 | −0.149 | −0.440 to 0.170 | 0.359 | −0.056 | −0.361 to 0.260 | 0.732 | 0.062 | −0.254 to 0.366 | 0.705 | 0.174 | −0.145 to 0.461 | 0.284 |
| Safety | −0.070 | −0.373 to 0.247 | 0.668 | −0.314 * | −0.570 to −0.003 | 0.048 | −0.281 | −0.545 to 0.033 | 0.078 | −0.076 | −0.379 to 0.241 | 0.639 | 0.050 | −0.266 to 0.356 | 0.761 | 0.257 | −0.059 to 0.526 | 0.110 |
| Durability | 0.111 | −0.208 to 0.408 | 0.497 | −0.334 * | −0.585 to −0.025 | 0.035 | −0.343 * | −0.591 to −0.035 | 0.030 | −0.055 | −0.360 to 0.261 | 0.734 | −0.070 | −0.373 to 0.247 | 0.666 | 0.173 | −0.146 to 0.460 | 0.286 |
| Easy to Use | −0.165 | −0.453 to 0.154 | 0.309 | 0.073 | −0.244 to 0.376 | 0.655 | −0.005 | −0.316 to 0.307 | 0.976 | −0.028 | −0.337 to 0.286 | 0.866 | −0.053 | −0.359 to 0.263 | 0.745 | 0.208 | −0.111 to 0.488 | 0.199 |
| Comfort | −0.149 | −0.440 to 0.170 | 0.357 | 0.087 | −0.231 to 0.388 | 0.592 | −0.148 | −0.439 to 0.171 | 0.362 | 0.031 | −0.283 to 0.339 | 0.848 | 0.139 | −0.180 to 0.432 | 0.393 | 0.198 | −0.121 to 0.480 | 0.220 |
| Effectiveness | −0.061 | −0.366 to 0.255 | 0.709 | −0.239 | −0.512 to 0.078 | 0.137 | −0.255 | −0.525 to 0.061 | 0.113 | −0.092 | −0.392 to 0.226 | 0.573 | −0.071 | −0.374 to 0.246 | 0.664 | 0.357 * | 0.051 to 0.602 | 0.024 |
| Total | −0.030 | −0.338 to 0.284 | 0.856 | −0.233 | −0.508 to 0.085 | 0.147 | −0.267 | −0.534 to 0.049 | 0.095 | −0.033 | −0.341 to 0.281 | 0.841 | 0.027 | −0.287 to 0.336 | 0.869 | 0.265 | −0.051to0.533 | 0.098 |
| CSQ8 | 0.053 | −0.263 to 0.359 | 0.747 | −0.157 | −0.447 to 0.162 | 0.333 | −0.104 | −0.402 to 0.214 | 0.524 | −0.053 | −0.359 to 0.263 | 0.747 | −0.107 | −0.405 to 0.212 | 0.511 | 0.532 ** | 0.264 to 0.724 | <0.001 |
| MSWS | MSIS | MFIS | SF36 | HADS Anxiety | HADS Depression | |||||||||||||
| QUEST 2.0 | rho | CI | p | rho | CI | p | rho | CI | p | rho | CI | p | rho | CI | p | rho | CI | p |
| Dimensions | 0.144 | −0.228 to 0.479 | 0.448 | 0.066 | −0.251 to 0.370 | 0.686 | −0.145 | −0.437 to 0.174 | 0.371 | −0.004 | −0.315 to 0.308 | 0.980 | 0.148 | −0.171 to 0.439 | 0.361 | 0.090 | −0.228 to 0.391 | 0.583 |
| Weight | 0.322 | −0.043 to 0.611 | 0.083 | 0.335 * | 0.026 to 0.585 | 0.035 | 0.270 | −0.045 to 0.536 | 0.092 | −0.161 | −0.450 to 0.158 | 0.322 | 0.169 | −0.150 to 0.456 | 0.297 | 0.065 | −0.252 to 0.369 | 0.692 |
| Adjustments | 0.194 | −0.179 to 0.518 | 0.305 | 0.174 | −0.145 to 0.461 | 0.282 | 0.103 | −0.215 to 0.402 | 0.526 | −0.077 | −0.379 to 0.240 | 0.637 | 0.204 | −0.115 to 0.485 | 0.208 | 0.086 | −0.232 to 0.387 | 0.600 |
| Safety | −0.109 | −0.452 to 0.262 | 0.567 | 0.060 | −0.256 to 0.365 | 0.713 | −0.186 | −0.470 to 0.133 | 0.249 | 0.178 | −0.141 to 0.464 | 0.272 | −0.065 | −0.369 to 0.252 | 0.692 | 0.001 | −0.311 to 0.312 | 0.993 |
| Durability | −0.005 | −0.365 to 0.356 | 0.979 | 0.152 | −0.167 to 0.443 | 0.350 | −0.007 | −0.318 to 0.305 | 0.965 | −0.086 | −0.387 to 0.232 | 0.596 | 0.142 | −0.177 to 0.434 | 0.381 | 0.184 | −0.135 to 0.469 | 0.256 |
| Easy to Use | −0.252 | −0.561 to 0.119 | 0.180 | 0.085 | −0.233 to 0.386 | 0.601 | 0.096 | −0.222 to 0.396 | 0.554 | −0.078 | −0.380 to 0.239 | 0.633 | 0.153 | −0.166 to 0.443 | 0.345 | 0.135 | −0.184 to 0.428 | 0.407 |
| Comfort | −0.194 | −0.518 to 0.179 | 0.305 | 0.379 * | 0.077 to 0.618 | 0.016 | 0.274 | −0.041 to 0.539 | 0.088 | −0.181 | −0.466 to 0.138 | 0.263 | 0.304 | −0.008 to 0.562 | 0.057 | 0.096 | −0.222 to 0.396 | 0.557 |
| Effectiveness | −0.171 | −0.500 to 0.202 | 0.365 | −0.186 | −0.470 to 0.133 | 0.251 | −0.335 * | −0.585 to −0.026 | 0.035 | 0.289 | −0.025 to 0.551 | 0.071 | −0.194 | −0.477 to 0.125 | 0.231 | 0.023 | −0.291 to 0.332 | 0.886 |
| Total | −0.018 | −0.376 to 0.345 | 0.923 | 0.147 | −0.172 to 0.438 | 0.365 | 0.029 | −0.285 to 0.337 | 0.859 | −0.014 | −0.324 to 0.299 | 0.932 | 0.173 | −0.146 to 0.460 | 0.287 | 0.105 | −0.213 to 0.403 | 0.517 |
| CSQ8 | 0.060 | −0.307 to 0.411 | 0.752 | −0.087 | −0.388 to 0.231 | 0.593 | −0.202 | −0.483 to 0.117 | 0.212 | 0.102 | −0.216 to 0.401 | 0.532 | −0.059 | −0.364 to 0.257 | 0.718 | −0.002 | −0.313 to 0.310 | 0.989 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Vázquez, D.; Cano-de-la-Cuerda, R.; Gor-García-Fogeda, M.D.; Molina-Rueda, F. Wearable Robotic Gait Training in Persons with Multiple Sclerosis: A Satisfaction Study. Sensors 2021, 21, 4940. https://doi.org/10.3390/s21144940
Fernández-Vázquez D, Cano-de-la-Cuerda R, Gor-García-Fogeda MD, Molina-Rueda F. Wearable Robotic Gait Training in Persons with Multiple Sclerosis: A Satisfaction Study. Sensors. 2021; 21(14):4940. https://doi.org/10.3390/s21144940
Chicago/Turabian StyleFernández-Vázquez, Diego, Roberto Cano-de-la-Cuerda, María Dolores Gor-García-Fogeda, and Francisco Molina-Rueda. 2021. "Wearable Robotic Gait Training in Persons with Multiple Sclerosis: A Satisfaction Study" Sensors 21, no. 14: 4940. https://doi.org/10.3390/s21144940
APA StyleFernández-Vázquez, D., Cano-de-la-Cuerda, R., Gor-García-Fogeda, M. D., & Molina-Rueda, F. (2021). Wearable Robotic Gait Training in Persons with Multiple Sclerosis: A Satisfaction Study. Sensors, 21(14), 4940. https://doi.org/10.3390/s21144940