
Application of a Machine Learning Algorithms in a Wrist-Wearable Sensor for Patient Health Monitoring during Autonomous Hospital Bed Transport




Abstract
:1. Introduction
2. Algorithm Design, Experimental Setup and Data Collection
2.1. Dreyfusian AI Algorithm Design
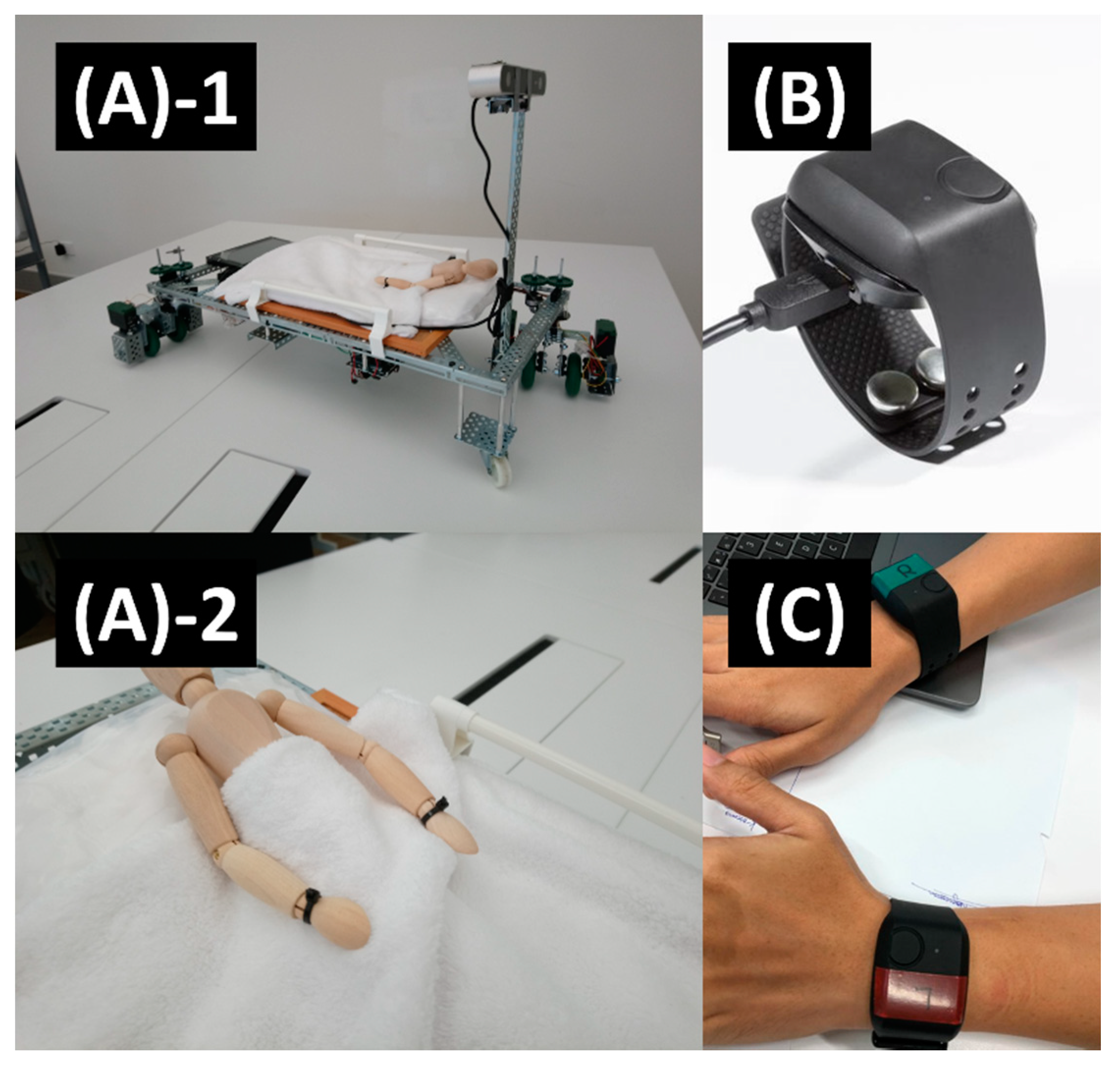
2.2. Experiment Proceedings and Data Collection
3. Results and Discussion
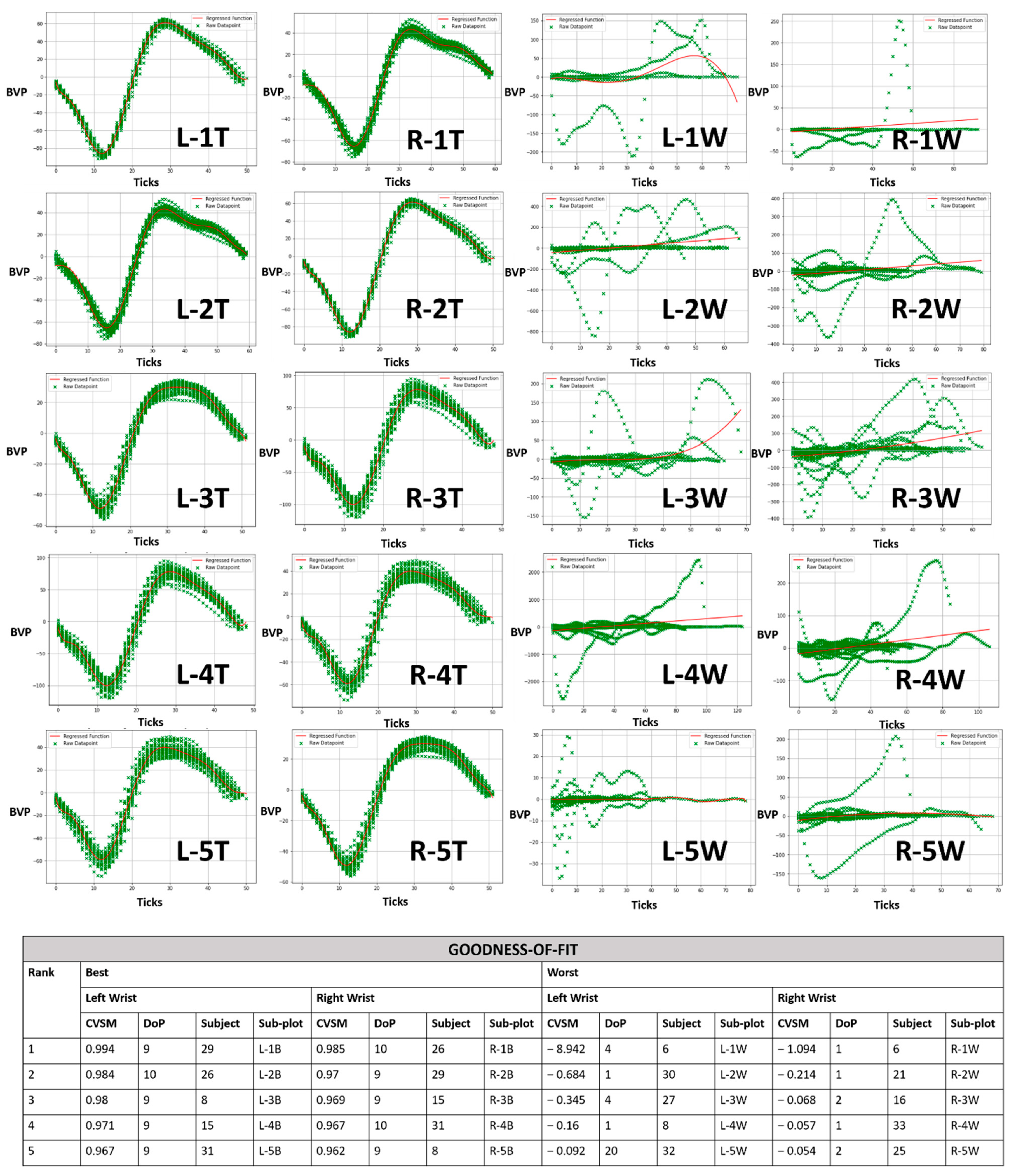
3.1. Goodness of Fit
3.2. Central Tendency
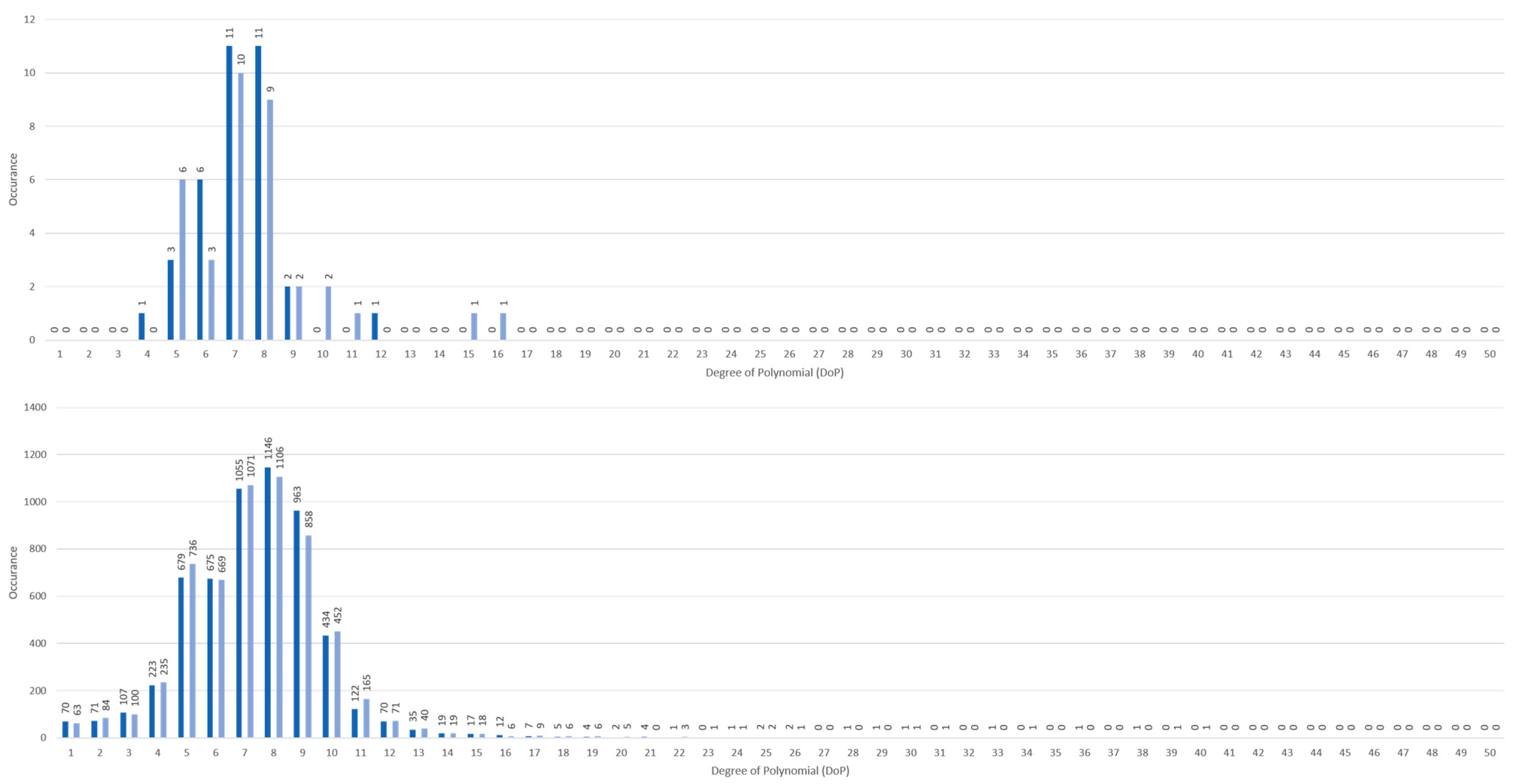
3.3. Efficacy: Degree-of-Polynomial (DoP) Match Rate
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Healthcare Manpower Plan 2020: Caring for the Nation Transforming Tomorrow’s Healthcare. Ministry of Health. 2016. Available online: https://www.moh.gov.sg/content/moh_web/home/pressRoom/highlights/2016/2020-healthcare-manpower-plan.html (accessed on 1 November 2017).
- Soon, S.; Svavarsdottir, H.; Downey, C.; Jayne, D.G. Wearable Devices for Remote Vital Signs Monitoring in the Outpatient Setting: An Overview of the Field. BMJ Innov. 2020, 6, 55. [Google Scholar] [CrossRef] [Green Version]
- McGillion, M.H.; Duceppe, E.; Allan, K.; Marcucci, M.; Yang, S.; Johnson, A.P.; Ross-Howe, S.; Peter, E.; Scott, T.; Ouellette, C.; et al. Postoperative Remote Automated Monitoring: Need for and State of the Science. Can. J. Cardiol. 2018, 34, 850–862. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dreyfus, H.L.; Dreyfus, S.E. Beyond expertise: Some preliminary thoughts on mastery. In A Qualitative Stance: Essays in Honor of Steinar Kvale; ISD LLC: Bristol, CT, USA, 2008; pp. 113–124. [Google Scholar]
- Talal, M.; Zaidan, A.A.; Zaidan, B.B.; Albahri, A.S.; Alamoodi, A.H.; Albahri, O.S.; Alsalem, M.A.; Lim, C.K.; Tan, K.L.; Shir, W.L.; et al. Smart Home-based IoT for Real-time and Secure Remote Health Monitoring of Triage and Priority System using Body Sensors: Multi-driven Systematic Review. J. Med. Syst. 2019, 43, 42. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Matveev, A.S.; Savkin, A.V.; Clout, R.; Nguyen, H.T. A semi-autonomous motorized mobile hospital bed for safe transportation of head injury patients in dynamic hospital environments without bed switching. Robotica 2016, 34, 1880–1897. [Google Scholar] [CrossRef]
- Guo, Z.; Yee, R.B.; Mun, K.R.; Yu, H. Experimental evaluation of a novel robotic hospital bed mover with omni-directional mobility. Appl. Ergon. 2017, 65, 389–397. [Google Scholar] [CrossRef] [PubMed]
- Daniell, N.; Merrett, S.; Paul, G. Effectiveness of powered hospital bed movers for reducing physiological strain and back muscle activation. Appl. Ergon. 2014, 45, 849–856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, J.; Wiggermann, N. Ergonomic evaluation of brake pedal and push handle locations on hospital beds. Appl. Ergon. 2017, 60, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Dreyfus, H.L. What Computers Can't Do: A Critique of Artificial Reason; Harper & Row: New York, NY, USA, 1972; p. 310. [Google Scholar]
- Dreyfus, H.L.; Dreyfus, S.E.; Athanasiou, T. Mind Over machine: The Power of Human Intuition and Expertise in the Era of the Computer; The Free Press: Hong Kong, China, 1986; p. 231. [Google Scholar]
- Dreyfus, H.L. What Computers Still Can't Do: A Critique of Artificial Reason; MIT Press: Cambridge, MA, USA, 1992; p. 354. [Google Scholar]
- Benner, P.E. From Novice to Expert: Excellence and Power in Clinical Nursing Practice; Addison-Wesley Publishing Company, Nursing Division: Menlo Park, CA, USA, 1984; p. 307. [Google Scholar]
- Biswas, D.; Simoes-Capela, N.; van Hoof, C.; van Helleputte, N. Heart Rate Estimation from Wrist-Worn Photoplethysmography: A Review. IEEE Sens. J. 2019, 19, 6560–6570. [Google Scholar] [CrossRef]
- Charlton, P.H.; Birrenkott, D.A.; Bonnici, T.; Pimentel, M.A.; Johnson, A.E.; Alastruey, J.; Tarassenko, L.; Watkinson, P.J.; Beale, R.; Clifton, D.A. Breathing Rate Estimation from the Electrocardiogram and Photoplethysmogram: A Review. IEEE Rev. Biomed. Eng. 2018, 11, 2–20. [Google Scholar] [CrossRef] [Green Version]
- Hwang, D. Monitoring Progress and Adherence with Positive Airway Pressure Therapy for Obstructive Sleep Apnea the Roles of Telemedicine and Mobile Health Applications. Sleep Med. Clin. 2016, 11, 161–171. [Google Scholar] [CrossRef]
- Kozioł, M.; Piech, P.; Maciejewski, M.; Surtel, W. The latest applications of photoplethysmography. Acta Angiol. 2019, 25, 28–34. [Google Scholar] [CrossRef]
- Yang, C.; Veiga, C.; Rodríguez-Andina, J.J.; Fariña, J.; Iñiguez, A.; Yin, S. Using PPG Signals and Wearable Devices for Atrial Fibrillation Screening. IEEE Trans. Ind. Electron. 2019, 66, 8832–8842. [Google Scholar] [CrossRef]
- Hussein, A.F.; Kumar, N.A.; Burbano-Fernandez, M.; Ramirez-Gonzalez, G.; Abdulhay, E.; de Albuquerque, V.H.C. An automated remote cloud-based heart rate variability monitoring system. IEEE Access 2018, 6, 77055–77064. [Google Scholar] [CrossRef]
- Tan, Y.H.; Li, H. Experimental Machine Learning of Finger Photoplethysmography (PPG) for Autonomous Hospital Bed Pushing Framework Using Polynomial Regression. Int. J. Eng. Technol. Manag. Res. 2018, 5, 11. [Google Scholar] [CrossRef]
- Vadrevu, S.; Manikandan, M.S. Real-Time PPG Signal Quality Assessment System for Improving Battery Life and False Alarms. IEEE Trans. Circuits Systs. II Express Briefs 2019, 66, 1910–1914. [Google Scholar] [CrossRef]
- Mahmoudzadeh, A.; Azimi, I.; Rahmani, A.M.; Liljeberg, P. Lightweight photoplethysmography quality assessment for real-time IoT-based health monitoring using unsupervised anomaly detection. In Proceedings of the 12th International Conference on Ambient Systems, Networks and Technologies/4th International Conference on Emerging Data and Industry 4.0/Affiliated Workshops, Warsaw, Poland, 23–26 March 2021. [Google Scholar] [CrossRef]
- Bian, D.; Mehta, P.; Selvaraj, N. Respiratory Rate Estimation using PPG: A Deep Learning Approach. In Proceedings of the 42nd Annual International Conferences of the IEEE Engineering in Medicine and Biology Society, Montreal, QC, Canada, 20–24 July 2020. [Google Scholar] [CrossRef]
- Pradhan, N.; Rajan, S.; Adler, A. Evaluation of the signal quality of wrist-based photoplethysmography. Physiol. Meas. 2019, 40, 065008. [Google Scholar] [CrossRef] [Green Version]
- Chaddad, A.; Katib, Y.; Hassan, L. Future artificial intelligence tools and perspectives in medicine. Curr. Opin. Urol. 2021, 31, 371–377. [Google Scholar] [CrossRef] [PubMed]
- Analyzing a Discrete Heart Rate Signal Using Python. A Tech Blog about Fun Things with Python and Embedded Electronics. Available online: http://www.paulvangent.com/2016/03/15/analyzing-a-discrete-heart-rate-signal-using-python-part-1/ (accessed on 1 November 2017).












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Algorithm Constituent | Historical Data | Immediate Measurement(s) | Binary Decision Making Condition |
|---|---|---|---|
| Dreyfusian Descriptor (Analogy) [13] | “To determine fluid balance, check the patient’s morning weights and daily intake and output for the past three days.” | “Weight gain and an intake that is consistently higher than output…” | “By greater than 500 cc. could indicate water retention, in which case fluid restriction should be started until the cause of the imbalance can be determined.” |
| This work: Autonomous Hospital Bed Transport (AHBT) | Pre-journey dataset (PJ) | In-journey dataset (IJ) | PJ-IJ feature matching to determine if AHBT can continue journey or move to a predesignated stop location. |
| Dataset or Technical Specification(s) | Supervised and segmented PPG waveforms from 5 min just prior to AHBT. PPG data authorized by supervising nurse. | Remotely supervised and segmented sets of PPG waveforms. Sets are latest and non-overlapping of 30 PPG waveforms. | Performed by the most suitable PR ML technique chosen by design matrix evaluation. |
| Factor | Weight | Single-Feature PR [20] | Rule-Based [21] | Multi-Feature [22] | Deep Learning [23] |
|---|---|---|---|---|---|
| Easy to understand | 30% | 25 | 15 | 10 | 10 |
| Explicability | 20% | 15 | 10 | 10 | 5 |
| Not using data sets beyond the individual subject | 20% | 20 | 20 | 20 | 0 |
| No data annotation | 20% | 15 | 20 | 15 | 10 |
| Computation time | 10% | 7 | 9 | 8 | 5 |
| Total Score | 100% | 81 | 75 | 64 | 30 |
| 21 up to <30 | 30 up to <65 | 65 or Older |
|---|---|---|
| 27 | 7 * | 1 # |
| Sensor Included in E4 | Physiological Phenomena | Information Inferred |
|---|---|---|
| Photoplethysmography | Blood volume changes | Cardiac activity |
| Electrodermal activity | Skin’s electrical conductivity | Sweat (Stress) levels |
| Infrared thermopile | Skin’s thermal conductivity | Body heating and cooling |
| Three axis accelerometer | Wrist bodily movements | Wearer’s physical activity |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tan, Y.H.; Liao, Y.; Tan, Z.; Li, K.-H.H. Application of a Machine Learning Algorithms in a Wrist-Wearable Sensor for Patient Health Monitoring during Autonomous Hospital Bed Transport. Sensors 2021, 21, 5711. https://doi.org/10.3390/s21175711
Tan YH, Liao Y, Tan Z, Li K-HH. Application of a Machine Learning Algorithms in a Wrist-Wearable Sensor for Patient Health Monitoring during Autonomous Hospital Bed Transport. Sensors. 2021; 21(17):5711. https://doi.org/10.3390/s21175711
Chicago/Turabian StyleTan, Yan Hao, Yuwen Liao, Zhijie Tan, and King-Ho Holden Li. 2021. "Application of a Machine Learning Algorithms in a Wrist-Wearable Sensor for Patient Health Monitoring during Autonomous Hospital Bed Transport" Sensors 21, no. 17: 5711. https://doi.org/10.3390/s21175711
APA StyleTan, Y. H., Liao, Y., Tan, Z., & Li, K. -H. H. (2021). Application of a Machine Learning Algorithms in a Wrist-Wearable Sensor for Patient Health Monitoring during Autonomous Hospital Bed Transport. Sensors, 21(17), 5711. https://doi.org/10.3390/s21175711