
The Effect of Local Cooling at the Elbow on Nerve Conduction Velocity and Motor Unit Behaviour: An Exploration of a Novel Neurological Assessment

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Participants
2.3. Testing Procedure
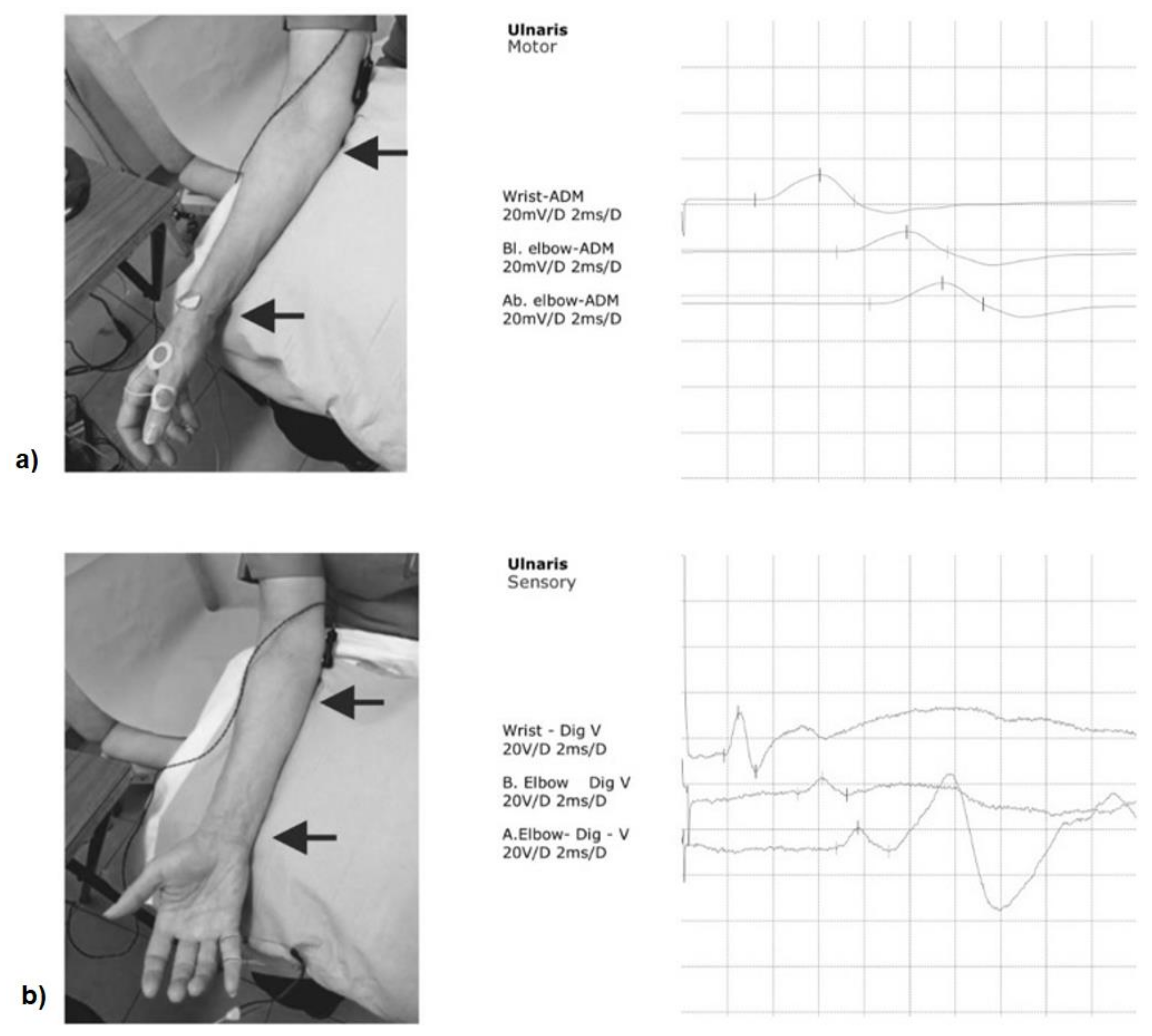
2.4. Nerve Conduction Velocity Tests
2.5. dEMG Data Collection
2.6. dEMG Data Analysis
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gilliatt, R.W.; Willison, R.G. Peripheral nerve conduction in diabetic neuropathy. J. Neurol. Neurosurg. Psychiatry 1962, 25, 11–18. [Google Scholar] [CrossRef] [Green Version]
- Robinson, L.R. Troumatic injury to peripheral nerves. Muscle Nerve 2000, 23, 863–873. [Google Scholar] [CrossRef]
- Smith, K. Conduction properties of central demyelinated and remyelinated axons, and their relation to symptom production in demyelinating disorders. Eye 1994, 8, 224–237. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.-R.; Chang, W.-N.; Chang, H.-W.; Tsai, N.-W.; Lu, C.-H. Effects of age, gender, height, and weight on late responses and nerve conduction study parameters. Acta Neurol. Taiwanica 2009, 18, 242–249. [Google Scholar]
- Kommalage, M.; Gunawardena, S. Influence of age, gender, and sidedness on ulnar nerve conduction. J. Clin. Neurophysiol. 2013, 30, 98–101. [Google Scholar] [CrossRef]
- Henrikson, J.D. Conduction Velocity of Motor Nerves in Normal Subjects and Patients with Neuromuscular Disorders. Master’s Thesis, University of Minnesota, Minneapolis, MN, USA, 1956. [Google Scholar]
- Keirnan, M.C.; Cikurel, K.; Bostock, H. Effects of temperature on the excitability properties of human motor axons. Brain 2001, 124, 816–825. [Google Scholar] [CrossRef] [PubMed]
- Dioszeghy, P.; Stalberg, E. Changes in motor and sensory nerve conduction parameters with temperature in normal and diseased nerve. Electroencephalogr. Clinical Neurophysiol. /Evoked Potentials Sect. 1992, 85, 229–235. [Google Scholar] [CrossRef]
- Algafly, A.A.; George, K.P. The effect of cryotherapy on nerve conduction velocity, pain threshold and pain tolerance. Br. J. Sports Med. 2007, 41, 365–369. [Google Scholar] [CrossRef]
- Freire, B.; Geremia, J.; Baroni, B.M.; Vaz, M.A. Effects of cryotherapy methods on circulatory, metabolic, inflammatory and neural properties: A systematic review. Fisioter Mov. 2016, 29, 389–398. [Google Scholar] [CrossRef]
- Mallette, M.M.; Green, L.A.; Gabriel, D.A.; Cheung, S.S. The effects of local forearm muscle cooling on motor unit properties. Graefe’s Arch. Clin. Exp. Ophthalmol. 2017, 118, 401–410. [Google Scholar] [CrossRef]
- Cheung, S.S.; Montie, D.L.; White, M.D.; Beham, D. Changes in manual dexterity folloing short-term hand and forearm immersion in 10 C water. Aviat. Space Environ. Med. 2003, 74, 990–993. [Google Scholar] [PubMed]
- Alexander, J.; Rhodes, D. Temporal patterns of knee-extensor isokinetic torque strength in male and female athletes following comparison of anterior thigh and knee cooling over a rewarming period. J. Sport Rehabil. 2019, 18, 1–7. [Google Scholar] [CrossRef]
- Dhavaliker, M.; Narkeesh, M.; Gupta, N. Effect of skin temperature on nerve conduction velocity and reliability of temperature correction formula in Indian females. J. Exerc. Sci. Physiother. 2009, 5, 24–29. [Google Scholar]
- Al-Shekhlee, A.; Shapiro, B.E.; Preston, D.C. Iatrogenic complications and risks of nerve conduction studies and needle electromyography. Muscle Nerve 2003, 27, 517–526. [Google Scholar] [CrossRef] [PubMed]
- Gechev, A.; Kane, N.; Koltzenburg, M.; Rao, D.; van der Star, R. Potential risks of iatrogenic complications of nerve conduction studies (NCS) and electromyography (EMG). Clin. Neurophysiol. Pract. 2016, 1, 62–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, T.; Prasad, K.; Lloyd, T. Peripheral neuropathy: Clinical and electrophysiological considerations. Neuroimaging Clin. 2014, 24, 49–65. [Google Scholar] [CrossRef] [Green Version]
- De Luca, C.J.; Adam, A.; Wotiz, R.; Gilmore, L.D.; Nawab, S.H. Decomposition of Surface EMG Signals. J. Neurophysiol. 2006, 96, 1646–1657. [Google Scholar] [CrossRef]
- Balshaw, T.; Pahar, M.; Chesham, R.; Macgregor, L.; Hunter, A.M. Reduced firing rates of high threshold motor units in response to eccentric overload. Physiol. Rep. 2017, 5, e13111. [Google Scholar] [CrossRef]
- Tang, W.; Zhang, X.; Tang, X.; Cao, S.; Gao, X.; Chen, X. Surface electromyographic examination of poststroke neuromuscular changes in proximal and distal muscles using clustering index analysis. Front. Neurol. 2018, 8, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Kawa, M.; Kowza-Dzwonkowska, M. Local cryotherapy in tennis elbow (lateral epicondylitis). Balt. J. Health Phys. Act. 2015, 7, 73–87. [Google Scholar] [CrossRef]
- Dykstra, J.H.; Hill, H.M.; Miller, M.G.; Cheatham, C.C.; Michael, T.J.; Baker, R.J. Comparisons of cubed ice, crushed ice, and wetted ice on intramuscular and surface temperature changes. J. Athl. Train. 2009, 44, 136–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halar, E.M.; A DeLisa, J.; Soine, T.L. Nerve conduction studies in upper extremities: Skin temperature corrections. Arch. Phys. Med. Rehabil. 1983, 64, 412–416. [Google Scholar]
- Preston, D.C.; Shapiro, B.W. Electromyography and Neuromuscular Disorders, 3rd ed.; Elsevier Saunders: London, UK, 2013. [Google Scholar]
- Kline, J.C.; De Luca, C.J. Error reduction in EMG signal decomposition. J. Neurophysiol. 2014, 112, 2718–2728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nawab, S.H.; Chang, S.-S.; De Luca, C.J. High-yield decomposition of surface EMG signals. Clin. Neurophysiol. 2010, 121, 1602–1615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colquhoun, R.J.; Tomko, P.; Magrini, M.A.; Muddle, T.W.D.; Jenkins, N.D.M. The influence of input excitation on the inter- and intra-day reliability of the motor unit firing rate versus recruitment threshold relationship. J. Neurophysiol. 2018, 120, 3131–3139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Luca, C.J.; Contessa, P. Hierarchical control of motor units in voluntary contractions. J. Neurophysiol. 2012, 107, 178–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alexander, J.; Richards, J.; Attah, O.; Cheema, S.; Snook, J.; Wisdell, C. Delayed effects of a 20-minute crushed ice application on knee joint position sense assessed by a functional task during a re-warming period. Gait Posture 2018, 62, 173–178. [Google Scholar] [CrossRef]
- Cornwall, M.W. Effect of temperature on muscle force and rate of muscle force production in men and women. J. Orthop. Sports Phys. Ther. 1994, 20, 74–80. [Google Scholar] [CrossRef] [Green Version]
- Alexander, J.; Selfe, J.; Rhodes, D.; Fowler, E.; May, K.; Richards, J. Mapping knee skin surface sensitivity and temperature following cryotherapy. J. Quant. Res. Rehabil. Med. 2019, 2, 1–5. [Google Scholar]
- Cappelen-Smith, C.; Kuwabara, S.; Lin, C.S.; Mogyoros, I.; Burke, D. Activity-dependent hyperpolarization and conduction block in chronic inflamatory demyelinating polyneuropathy. Ann. Neurol 2000, 48, 826–832. [Google Scholar] [CrossRef]
- Salmons, S.; Sréter, F.A. Significance of impulse activity in the transformation of skeletal muscle type. Nat. Cell Biol. 1976, 263, 30–34. [Google Scholar] [CrossRef] [PubMed]
- Kaji, R.; Sumner, A.J. Ouabain reverses conduction disturbances in single demyelinated nerve fibres. Neurology 1989, 39, 1364–1368. [Google Scholar] [CrossRef] [PubMed]
- Bostock, H.; Grafe, P. Activity-dependent excitability changes in normal and demyelinated rat spinal root axons. J. Physiol. 1985, 365, 239–257. [Google Scholar] [CrossRef]
- Gonzalez-Izal, M.; Cadore, E.; Izquierdo, M. Muscle conduction velocity, surface electromyography variables, and echo intensity during concentric and eccentric fatigue. Muscle Nerve 2013, 49, 389–397. [Google Scholar] [CrossRef]
- Watson, B.V.; Goherty, T.J. Frequency-Dependent conduction block in ulnar neuropathy localized to the elbow. Clin. Neurophysiol. 2010, 121, 2111–2116. [Google Scholar] [CrossRef]
- Burke, D. Frequency-dependent conduction block in carpal tunnel syndrome. Muscle Nerve 2006, 33, 587–588. [Google Scholar] [CrossRef] [PubMed]
- Kuwabara, S.; Nakahama, Y.; Hattori, T.; Toma, S.; Mizobuchi, K.; Ogawara, K. Activity dependent excitability changes in cjronic inflamatory demyelinating polyneuropathy: A microneurographic study. Muscle Nerve 1999, 22, 899–904. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Motor NCV (m/s) Group Mean (SD) | Sensory NCV (m/s) Group Mean (SD) | ||||
|---|---|---|---|---|---|
| Below Elbow to Wrist | Across Elbow | Wrist to 5th Digit | Below Elbow to Wrist | Across Elbow | |
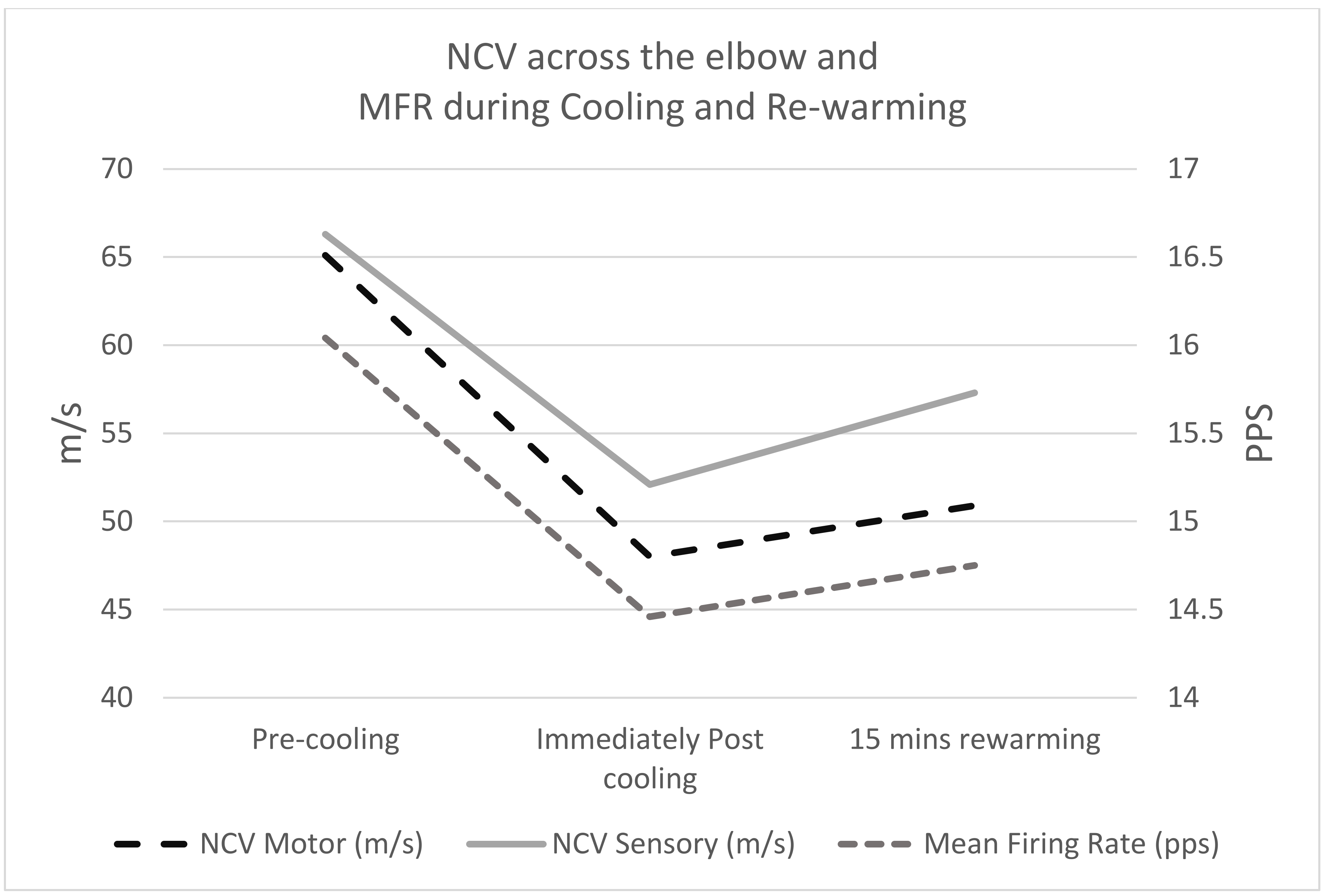
| Pre-cooling | 63.3 (5.1) | 65.1 (6.7) | 58.1 (5.0) | 63.9 (4.7) | 66.3 (6.2) |
| Immediately Post cooling | 62.3 (5.7) | 48.0 (8.1) | 56.4(6.6) | 62.6 (6.0) | 52.1 (7.2) |
| 15 min rewarming | 61.9 (6.5) | 50.9 (8.6) | 55.1 (5.4) | 61.4 (6.1) | 57.3 (8.2) |
| RM ANOVA | p = 0.085 | p < 0.001 | p = 0.020 | p = 0.048 | p < 0.001 |
| Wrist | Below Elbow | Above Elbow | Wrist | Below Elbow | Above Elbow | |
|---|---|---|---|---|---|---|
| CMAP Amplitude (mV) Group mean (SD) | SAP Amplitude (uV) Group mean (SD) | |||||
| Pre-cooling | 10.2 (1.8) | 9.6 (1.8) | 9.0 (2.0) | 26.2 (5.0) | 12.2 (6.3) | 11.7 (5.8) |
| Immediately Post cooling | 9.9 (2.0) | 9.6 (2.1) | 9.0 (2.3) | 26.5 (6.0) | 13.7 (7.9) | 12.4 (6.8) |
| 15 min rewarming | 9.9 (2.8) | 9.4 (2.6) | 9.1 (2.6) | 27.5 (6.5) | 13.6 (7.5) | 12.8 (6.9) |
| RM ANOVA | p = 0.785 | p = 0.835 | p = 0.925 | p = 0.606 | p = 0.739 | p = 0.843 |
| CMAP Duration (ms) Group mean (SD) | SAP Duration (ms) Group mean (SD) | |||||
| Pre-cooling | 4.4 (0.6) | 4.5 (0.6) | 4.7 (0.6) | 2.3 (0.4) | 2.6 (0.6) | 2.4 (0.5) |
| Immediately Post cooling | 4.3 (0.6) | 4.5 (0.7) | 4.5 (0.7) | 2.2(0.4) | 2.7 (0.6) | 2.5 (0.4) |
| 15 min rewarming | 4.5 (0.7) | 4.5(0.7) | 4.6 (0.6) | 2.1 (0.4) | 2.8 (0.6) | 2.4 (0.5) |
| RM ANOVA | p = 0.764 | p = 0.700 | p = 0.179 | p = 0.144 | p = 0.529 | p = 0.600 |
| Mean (SD) | ||||
|---|---|---|---|---|
| Total Mean Firing Rate (pps) | Upper Tertile Firing Rate (pps) | Middle Tertile Firing Rate (pps) | Lower Tertile Firing Rate (pps) | |
| Pre-cooling | 16.04 (2.59) | 20.79 (2.26) | 15.84 (2.01) | 11.35 (1.71) |
| Immediately Post cooling | 14.46 (2.51) | 18.78 (2.49) | 14.42 (1.88) | 10.45 (1.42) |
| 15 min rewarming | 14.75 (2.24) | 20.59 (2.45) | 16.02 (1.62) | 11.23 (1.22) |
| RM ANOVA | p = 0.01 | p = 0.038 | p = 0.038 | p = 0.247 |
| Mean Difference | % Change | Upper and Lower CI of the Difference | p-Value | |
|---|---|---|---|---|
| Motor NCV Across Elbow | ||||
| Pre-cooling vs. post cooling | 17.1 * | 26% | 12.1 to 22.2 | <0.001 |
| Pre-cooling vs. 15 min rewarming | 14.2 * | 22% | 9.4 to 19.0 | <0.001 |
| Post cooling vs. 15 min rewarming | −3.0 | −6% | −6.6 to 0.675 | 0.101 |
| Sensory NCV wrist to 5th digit | ||||
| Pre-cooling vs. post cooling | 1.76 | 3% | −0.08 to 3.60 | 0.059 |
| Pre-cooling vs. 15 min rewarming | 3.02 * | 5% | 0.40 to 5.65 | 0.028 |
| Post cooling vs. 15 min rewarming | 1.27 | 2% | −0.74 to 3.27 | 0.192 |
| Sensory NCV wrist to below elbow | ||||
| Pre-cooling vs. post cooling | 1.32 | 2% | −1.13 to 3.77 | 0.262 |
| Pre-cooling vs. 15 min rewarming | 2.52 * | 4% | 0.29 to 4.74 | 0.030 |
| Post cooling vs. 15 min rewarming | 1.20 | 2% | −0.31 to 2.70 | 0.108 |
| Sensory NCV across elbow | ||||
| Pre-cooling vs. post cooling | 14.2 * | 21% | 10.1 to 18.3 | <0.001 |
| Pre-cooling vs. 15 min rewarming | 9.0 * | 14% | 4.937 to 13.0 | <0.001 |
| Post cooling vs. 15 min rewarming | −5.2 * | −10% | −8.1 to −2.4 | 0.002 |
| Total mean firing rate (pps) | ||||
| Pre-cooling vs. post cooling | 1.58 * | 9% | 0.81 to 2.36 | <0.001 |
| Pre-cooling vs. 15 min rewarming | 1.29 * | 8% | 0.50 to 2.08 | 0.002 |
| Post cooling vs. 15 min rewarming | −0.29 | −2% | −1.06 to 0.48 | 0.454 |
| Upper tertile firing rate (pps) | ||||
| Pre-cooling vs. post cooling | 2.02 * | 10% | 0.27 to 3.76 | 0.029 |
| Pre-cooling vs. 15 min rewarming | 0.20 | 1% | −1.36 to 1.77 | 0.771 |
| Post cooling vs. 15 min rewarming | −1.81 | −10% | −3.86 to 0.23 | 0.076 |
| Middle tertile firing rate (pps) | ||||
| Pre-cooling vs. post cooling | 1.43 * | 9% | 0.05 to 2.81 | 0.044 |
| Pre-cooling vs. 15 min rewarming | −0.17 | 1% | −1.68 to 1.33 | 0.789 |
| Post cooling vs. 15 min rewarming | −1.60 * | −10% | −2.99 to −0.22 | 0.029 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Richards, J.; Gechev, A.; Alexander, J.; Macedo, L.; May, K.A.; Lindley, S.B. The Effect of Local Cooling at the Elbow on Nerve Conduction Velocity and Motor Unit Behaviour: An Exploration of a Novel Neurological Assessment. Sensors 2021, 21, 6703. https://doi.org/10.3390/s21206703
Richards J, Gechev A, Alexander J, Macedo L, May KA, Lindley SB. The Effect of Local Cooling at the Elbow on Nerve Conduction Velocity and Motor Unit Behaviour: An Exploration of a Novel Neurological Assessment. Sensors. 2021; 21(20):6703. https://doi.org/10.3390/s21206703
Chicago/Turabian StyleRichards, Jim, Antonin Gechev, Jill Alexander, Liane Macedo, Karen A. May, and Steven B. Lindley. 2021. "The Effect of Local Cooling at the Elbow on Nerve Conduction Velocity and Motor Unit Behaviour: An Exploration of a Novel Neurological Assessment" Sensors 21, no. 20: 6703. https://doi.org/10.3390/s21206703
APA StyleRichards, J., Gechev, A., Alexander, J., Macedo, L., May, K. A., & Lindley, S. B. (2021). The Effect of Local Cooling at the Elbow on Nerve Conduction Velocity and Motor Unit Behaviour: An Exploration of a Novel Neurological Assessment. Sensors, 21(20), 6703. https://doi.org/10.3390/s21206703