
Automatic Segmentation of the Retinal Nerve Fiber Layer by Means of Mathematical Morphology and Deformable Models in 2D Optical Coherence Tomography Imaging

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
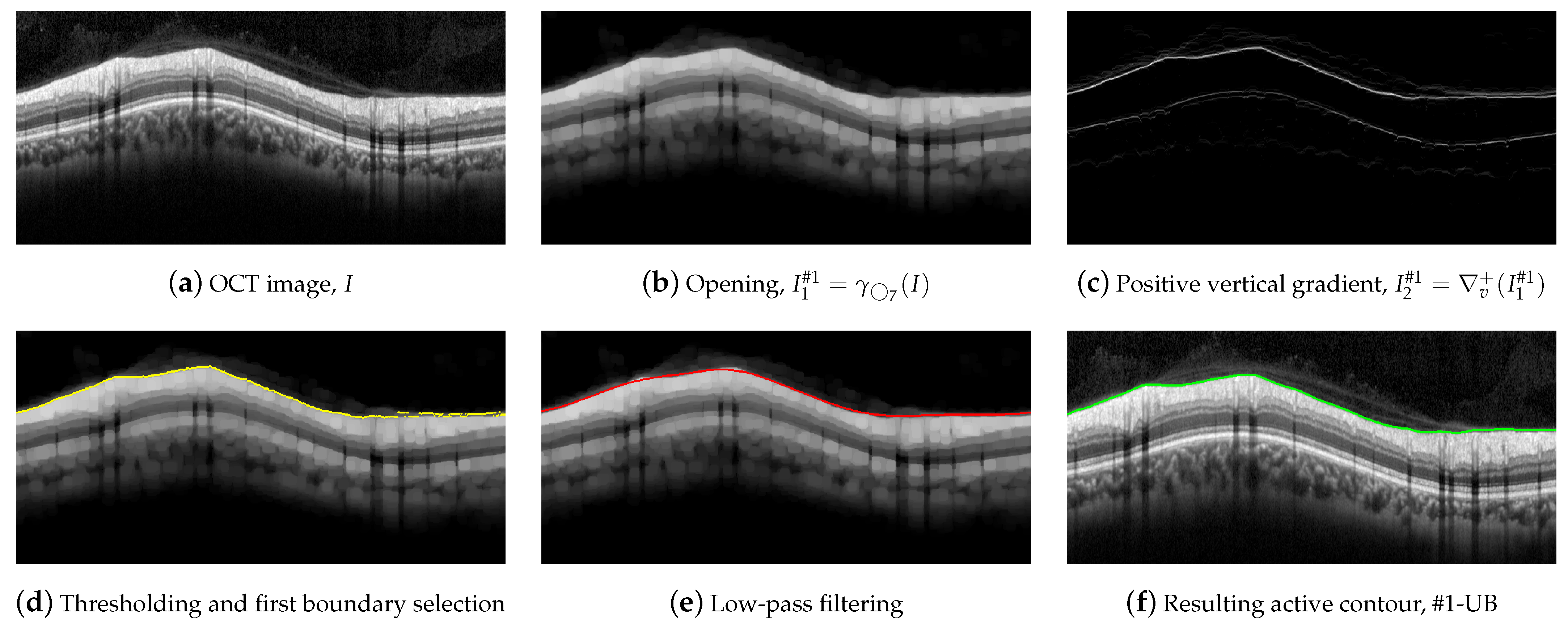
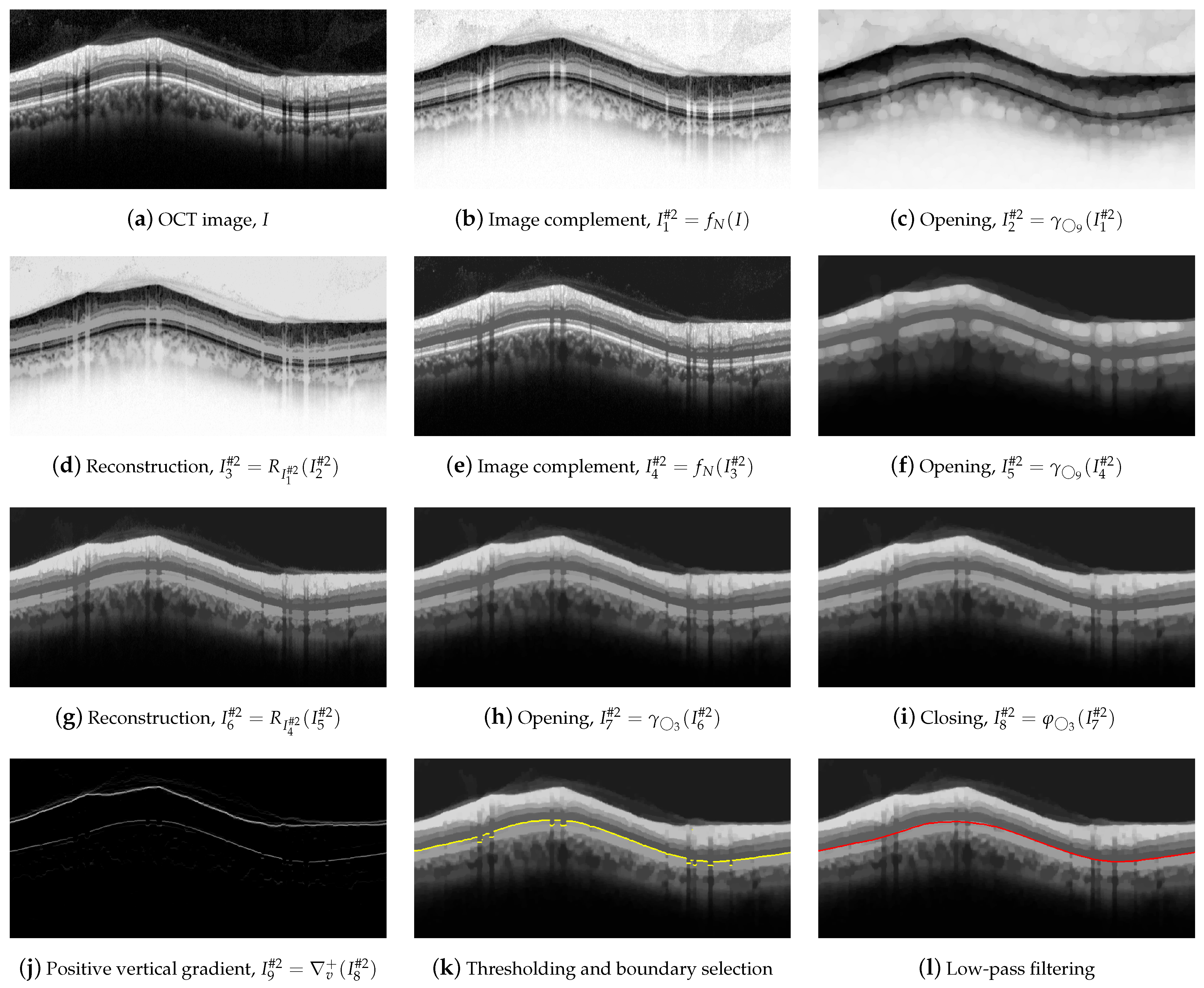
- Preprocessing to reduce the speckle noise and undesired artifacts in peripapillary 2D B-scan OCT images. This filtering is mainly performed by morphological operators.
- Peak detection on positive and negative part of the vertical gradient. This column-wise process (1D scenario) provides a rough detection of the layer’s boundaries.
- Reduction of possible discontinuities in previous coarse detection by processing adjacent columns (2D scenario) with a sliding window low-pass filter.
- Refinement of previous result by the imposition of the physical characteristics of biological tissues. The properties of elasticity and rigidity of the solution are incorporated by using a deformable model (in a 2D scenario).
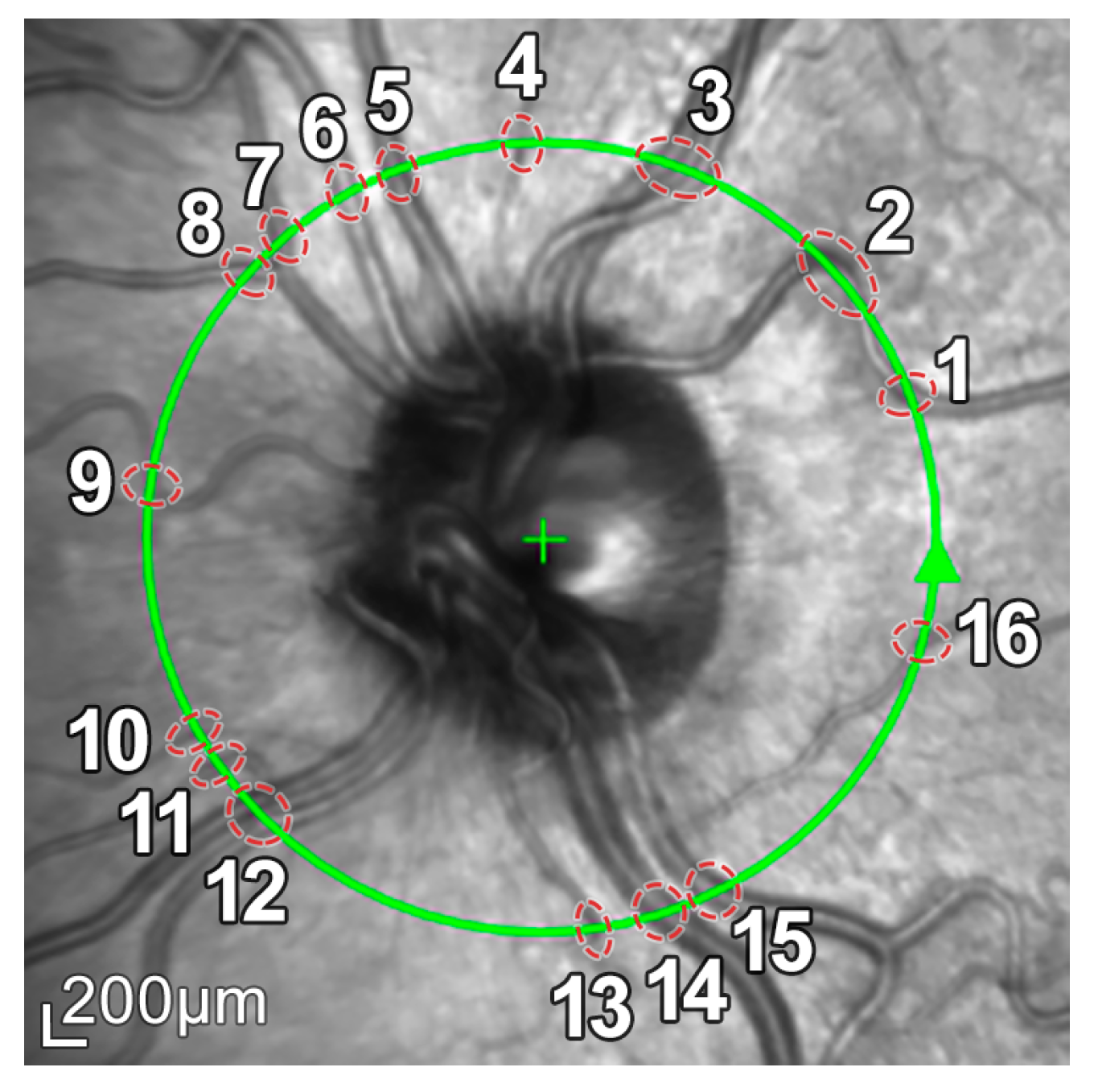
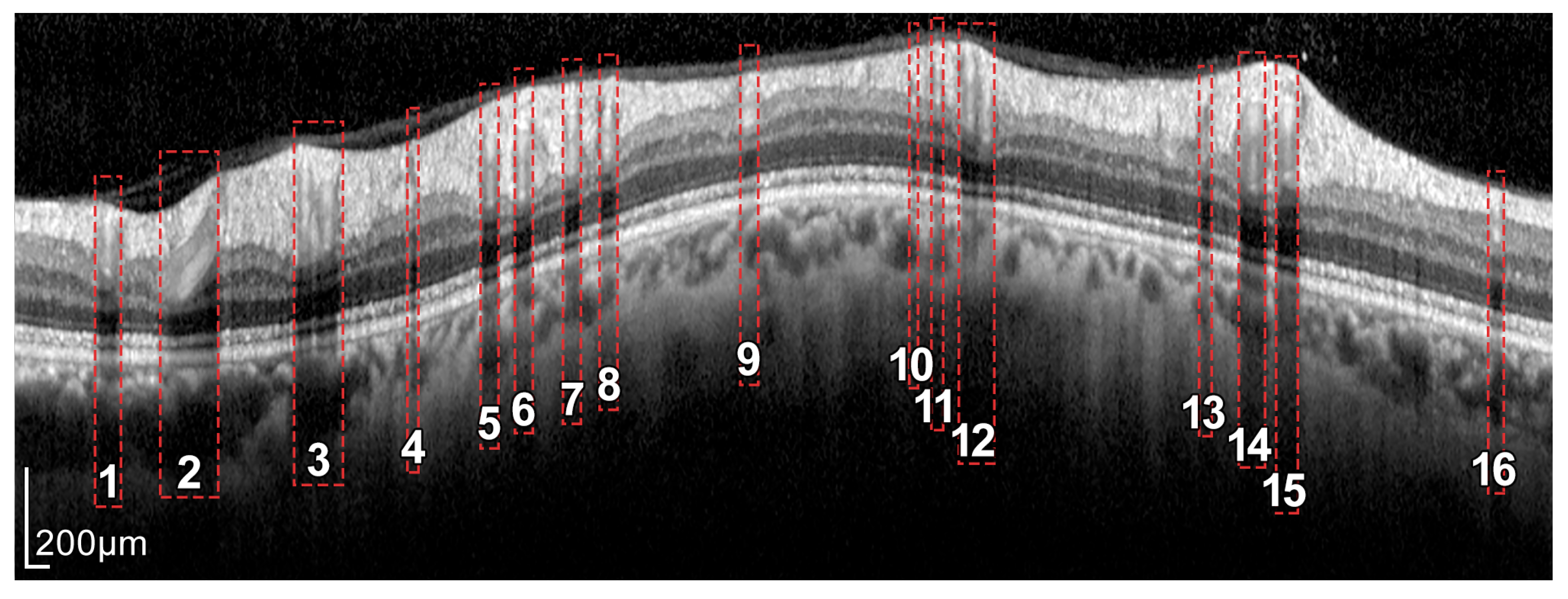
2.1. Materials: OCT Database
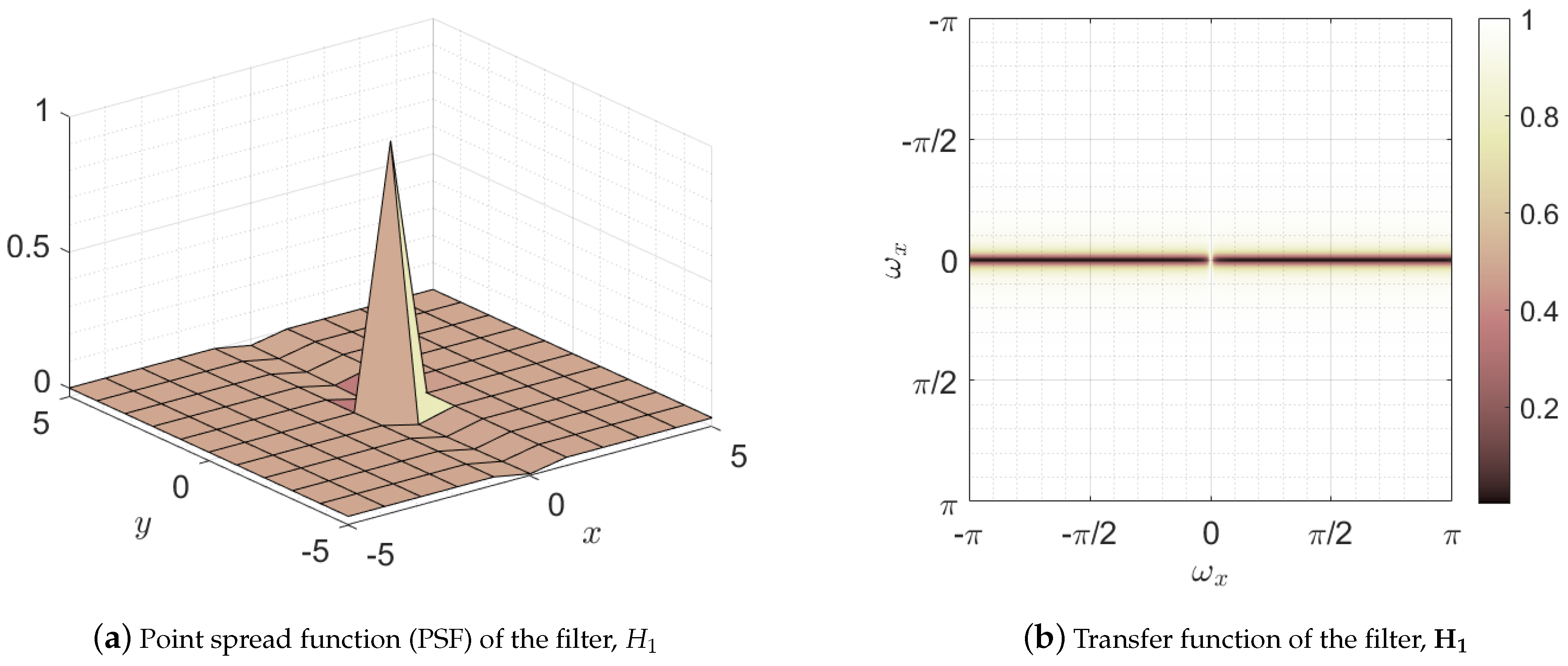
2.2. Preprocessing: Mathematical Morphology
2.3. Boundary Segmentation: Active Contours
2.4. RNFL Layer Segmentation Process
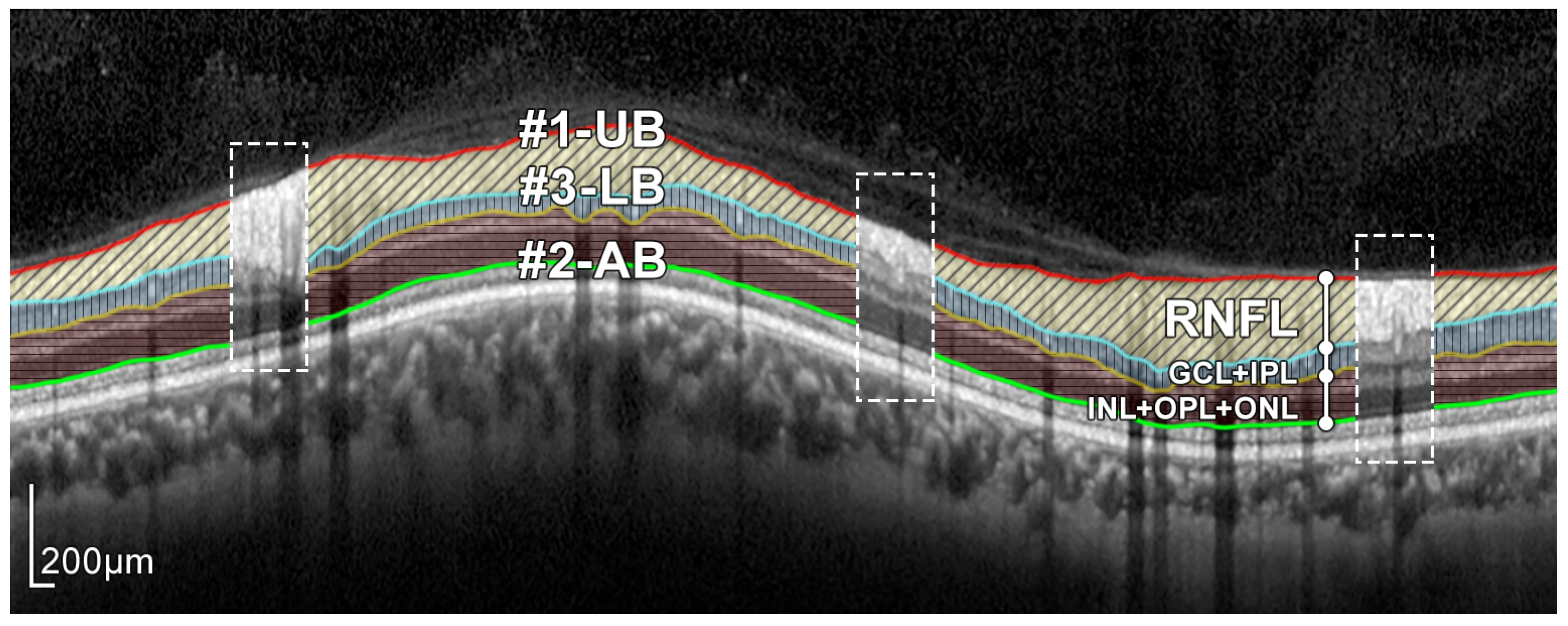
2.5. Segmentation of Boundary #1-UB
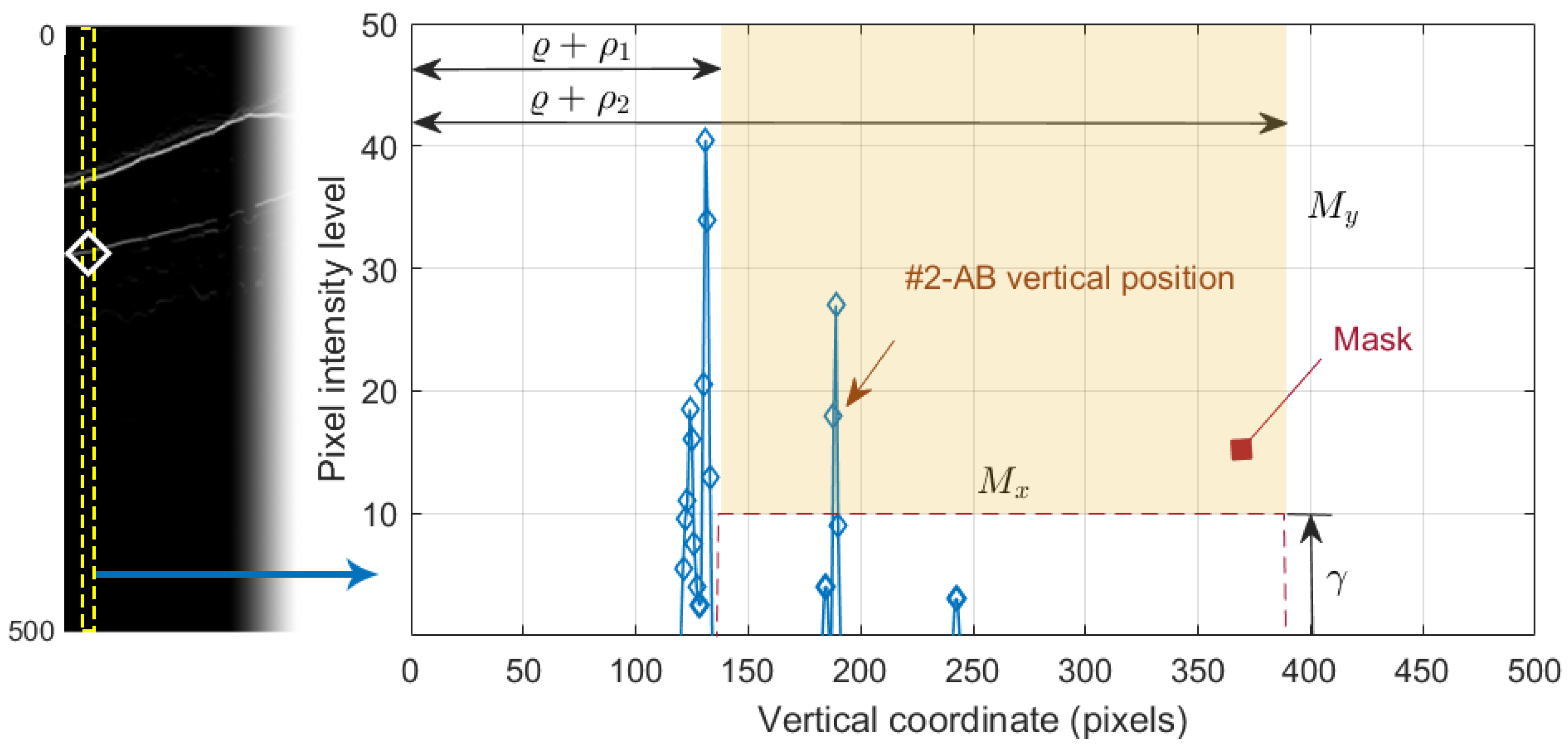
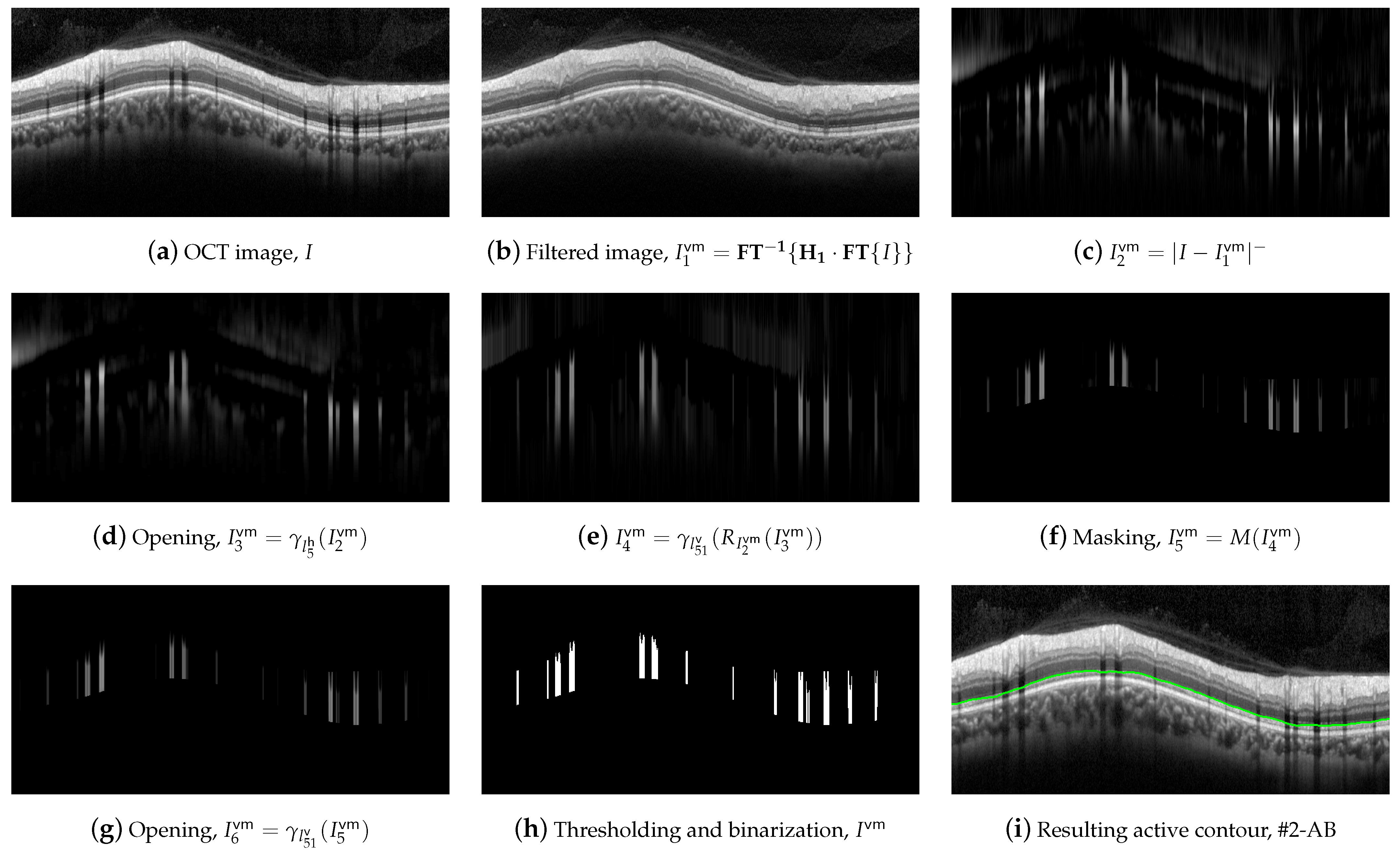
2.6. Segmentation of Boundary #2-AB
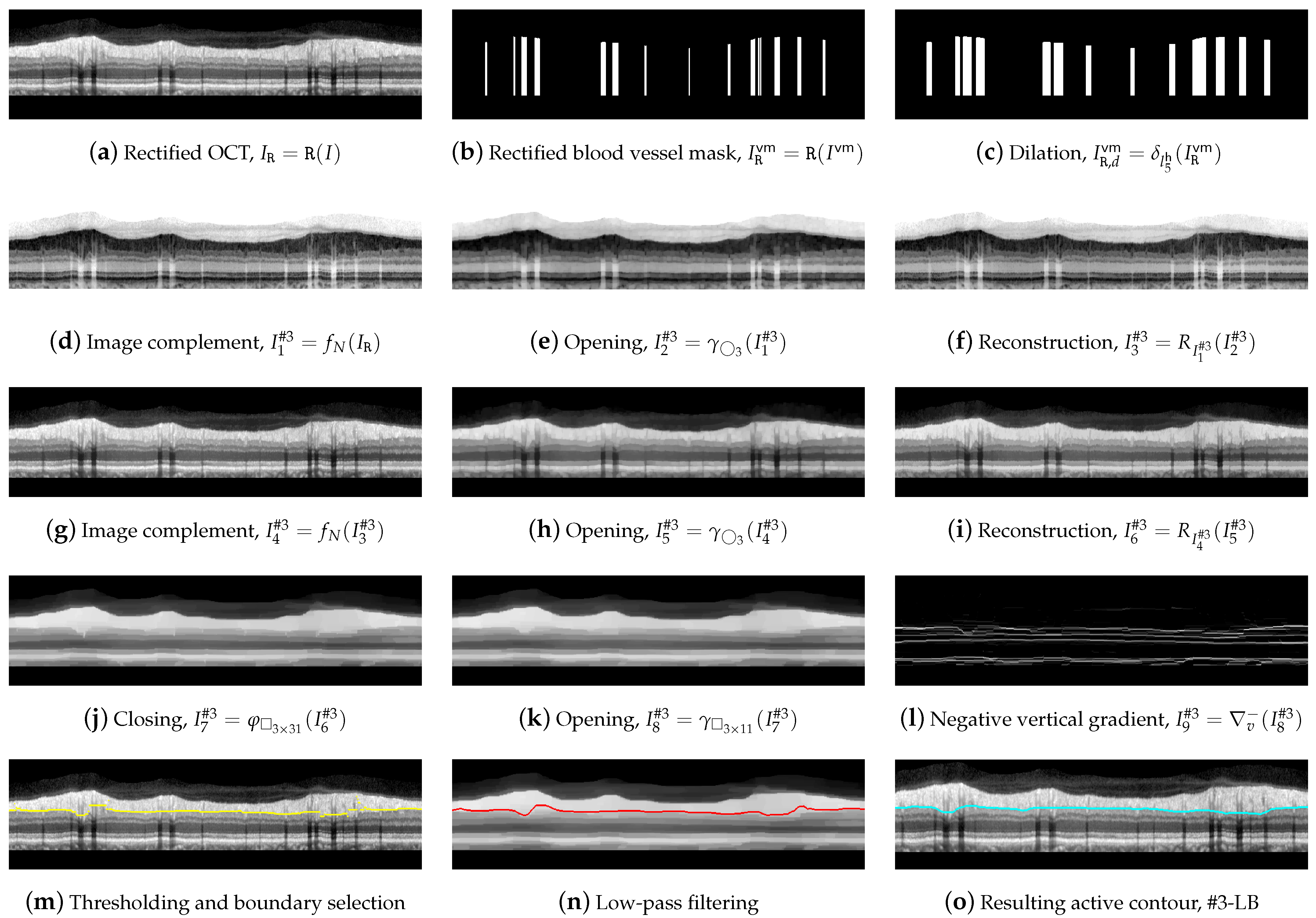
2.7. Segmentation of Boundary #3-LB
2.8. RNFL Thickness Calculation
3. Results
4. Discussion
4.1. Robustness against Parameter Variations and Speckle Noise
4.2. Analysis of the Performance of the Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Correction Statement
References
- Weinreb, R.N.; Khaw, P.T. Primary open-angle glaucoma. Lancet 2004, 363, 1711–1720. [Google Scholar] [CrossRef]
- Tham, Y.C.; Li, X.; Wong, T.Y.; Quigley, H.A.; Aung, T.; Cheng, C.Y. Global Prevalence of Glaucoma and Projections of Glaucoma Burden through 2040: A Systematic Review and Meta-Analysis. Ophthalmology 2014, 121, 2081–2090. [Google Scholar] [CrossRef] [PubMed]
- Casson, R.J.; Chidlow, G.; Wood, J.P.; Crowston, J.G.; Goldberg, I. Definition of glaucoma: Clinical and experimental concepts. Clin. Exp. Ophthalmol. 2012, 40, 341–349. [Google Scholar] [CrossRef] [PubMed]
- Kwon, Y.H.; Fingert, J.H.; Kuehn, M.H.; Alward, W.L. Primary Open-Angle Glaucoma. N. Engl. J. Med. 2009, 360, 1113–1124. [Google Scholar] [CrossRef]
- Swanson, E.A.; Fujimoto, J.G. The ecosystem that powered the translation of OCT from fundamental research to clinical and commercial impact. Biomed. Opt. Express 2017, 8, 1638–1664. [Google Scholar] [CrossRef]
- Huang, D.; Swanson, E.; Lin, C.; Schuman, J.; Stinson, W.; Chang, W.; Hee, M.; Flotte, T.; Gregory, K.; Puliafito, C.; et al. Optical coherence tomography. Science 1991, 254, 1178–1181. [Google Scholar] [CrossRef]
- Kanngiesser, J.; Roth, B. Wavefront Shaping Concepts for Application in Optical Coherence Tomography—A Review. Sensors 2020, 20, 44. [Google Scholar] [CrossRef]
- Badalà, F.; Nouri-Mahdavi, K.; Raoof, D.A.; Leeprechanon, N.; Law, S.K.; Caprioli, J. Optic disk and nerve fiber layer imaging to detect glaucoma. Am. J. Ophthalmol. 2007, 144, 724–732. [Google Scholar] [CrossRef]
- Alasil, T.; Wang, K.; Keane, P.A.; Lee, H.; Baniasadi, N.; de Boer, J.F.; Chen, T.C. Analysis of normal retinal nerve fiber layer thickness by age, sex, and race using spectral domain optical coherence tomography. J. Glaucoma 2013, 22, 532–541. [Google Scholar] [CrossRef]
- Sommer, A.; Miller, N.R.; Pollack, I.; Maumenee, A.E.; George, T. The Nerve Fiber Layer in the Diagnosis of Glaucoma. Arch. Ophthalmol. 1977, 95, 2149–2156. [Google Scholar] [CrossRef]
- Sommer, A.; Katz, J.; Quigley, H.A.; Miller, N.R.; Robin, A.L.; Richter, R.C.; Witt, K.A. Clinically Detectable Nerve Fiber Atrophy Precedes the Onset of Glaucomatous Field Loss. Arch. Ophthalmol. 1991, 109, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Duke SD-OCT. Available online: https://people.duke.edu/~sf59/RPEDC_Ophth_2013_dataset.htm (accessed on 29 September 2021).
- Chiu, S.J.; Allingham, M.J.; Mettu, P.S.; Cousins, S.W.; Izatt, J.A.; Farsiu, S. Kernel regression based segmentation of optical coherence tomography images with diabetic macular edema. Biomed. Opt. Express 2015, 6, 1172–1194. [Google Scholar] [CrossRef] [PubMed]
- MGU-Net. Available online: https://github.com/Jiaxuan-Li/MGU-Net (accessed on 29 September 2021).
- Li, J.; Jin, P.; Zhu, J.; Zou, H.; Xu, X.; Tang, M.; Zhou, M.; Gan, Y.; He, J.; Ling, Y.; et al. Multi-scale GCN-assisted two-stage network for joint segmentation of retinal layers and discs in peripapillary OCT images. Biomed. Opt. Express 2021, 12, 2204–2220. [Google Scholar] [CrossRef] [PubMed]
- The Annotated Retinal OCT Images (AROI) Database. Available online: https://ipg.fer.hr/ipg/resources/oct_image_database (accessed on 29 September 2021).
- Melinščak, M.; Radmilović, M.; Vatavuk, Z.; Lončarić, S. Annotated retinal optical coherence tomography images (AROI) database for joint retinal layer and fluid segmentation. Automatika 2021, 62, 375–385. [Google Scholar] [CrossRef]
- Optical Coherence Tomography Image Database (OCTID). Available online: https://dataverse.scholarsportal.info/dataverse/OCTID (accessed on 29 September 2021).
- Gholami, P.; Roy, P.; Parthasarathy, M.K.; Lakshminarayanan, V. OCTID: Optical Coherence Tomography Image Database. arXiv arXiv:cs.CV/1812.07056, 2019. [CrossRef]
- OCT Data & Color Fundus Images of Left & Right Eyes of 50 Healthy Persons. Available online: https://sites.google.com/site/hosseinrabbanikhorasgani/datasets-1/oct-fundus-right-left (accessed on 29 September 2021).
- Mahmudi, T.; Kafieh, R.; Rabbani, H.; Mehri, A.; Akhlaghi, M.R. Evaluation of asymmetry in right and left eyes of normal individuals using extracted features from optical coherence tomography and fundus images. J. Med. Signals Sens. 2021, 11, 12–23. [Google Scholar] [CrossRef]
- Abràmoff, M.D.; Garvin, M.K.; Sonka, M. Retinal Imaging and Image Analysis. IEEE Rev. Biomed. Eng. 2010, 3, 169–208. [Google Scholar] [CrossRef] [PubMed]
- Quellec, G.; Lee, K.; Dolejsi, M.; Garvin, M.K.; Abramoff, M.D.; Sonka, M. Three-Dimensional Analysis of Retinal Layer Texture: Identification of Fluid-Filled Regions in SD-OCT of the Macula. IEEE Trans. Med. Imaging 2010, 29, 1321–1330. [Google Scholar] [CrossRef] [PubMed]
- Dufour, P.A.; Ceklic, L.; Abdillahi, H.; Schroder, S.; De Dzanet, S.; Wolf-Schnurrbusch, U.; Kowal, J. Graph-Based Multi-Surface Segmentation of OCT Data Using Trained Hard and Soft Constraints. IEEE Trans. Med. Imaging 2013, 32, 531–543. [Google Scholar] [CrossRef]
- Beck, M.; Joshi, D.S.; Berger, L.; Klose, G.; De Zanet, S.; Mosinska, A.; Apostolopoulos, S.; Ebneter, A.; Zinkernagel, M.S.; Wolf, S.; et al. Comparison of Drusen Volume Assessed by Two Different OCT Devices. J. Clin. Med. 2020, 9, 2657. [Google Scholar] [CrossRef]
- Xiang, D.; Tian, H.; Yang, X.; Shi, F.; Zhu, W.; Chen, H.; Chen, X. Automatic Segmentation of Retinal Layer in OCT Images with Choroidal Neovascularization. IEEE Trans. Image Process. 2018, 27, 5880–5891. [Google Scholar] [CrossRef] [PubMed]
- Girish, G.; Thakur, B.; Chowdhury, S.R.; Kothari, A.R.; Rajan, J. Segmentation of intra-retinal cysts from optical coherence tomography images using a fully convolutional neural network model. IEEE J. Biomed. Health Inform. 2019, 23, 296–304. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Lee, K.; Zhang, L.; Sonka, M.; Abramoff, M.D. Stratified Sampling Voxel Classification for Segmentation of Intraretinal and Subretinal Fluid in Longitudinal Clinical OCT Data. IEEE Trans. Med. Imaging 2015, 34, 1616–1623. [Google Scholar] [CrossRef]
- Bogunović, H.; Venhuizen, F.; Klimscha, S.; Apostolopoulos, S.; Bab-Hadiashar, A.; Bagci, U.; Beg, M.F.; Bekalo, L.; Chen, Q.; Ciller, C.; et al. RETOUCH: The retinal OCT fluid detection and segmentation benchmark and challenge. IEEE Trans. Med. Imaging 2019, 38, 1858–1874. [Google Scholar] [CrossRef] [PubMed]
- Schmidt-Erfurth, U.; Klimscha, S.; Waldstein, S.; Bogunović, H. A view of the current and future role of optical coherence tomography in the management of age-related macular degeneration. Eye 2017, 31, 26–44. [Google Scholar] [CrossRef] [PubMed]
- Cabrera Fernández, D. Delineating fluid-filled region boundaries in optical coherence tomography images of the retina. IEEE Trans. Med. Imaging 2005, 24, 929–945. [Google Scholar] [CrossRef]
- Fuller, A.; Zawadzki, R.; Choi, S.; Wiley, D.; Werner, J.; Hamann, B. Segmentation of Three-dimensional Retinal Image Data. IEEE Trans. Vis. Comput. Graph. 2007, 13, 1719–1726. [Google Scholar] [CrossRef]
- Baroni, M.; Fortunato, P.; La Torre, A. Towards quantitative analysis of retinal features in optical coherence tomography. Med. Eng. Phys. 2007, 29, 432–441. [Google Scholar] [CrossRef]
- Boyer, K.; Herzog, A.; Roberts, C. Automatic recovery of the optic nervehead geometry in optical coherence tomography. IEEE Trans. Med. Imaging 2006, 25, 553–570. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Wang, Y.X.; Li, Y. Automatic Choroidal Layer Segmentation Using Markov Random Field and Level Set Method. IEEE J. Biomed. Health Inform. 2017, 21, 1694–1702. [Google Scholar] [CrossRef] [PubMed]
- Yazdanpanah, A.; Hamarneh, G.; Smith, B.R.; Sarunic, M.V. Segmentation of Intra-Retinal Layers From Optical Coherence Tomography Images Using an Active Contour Approach. IEEE Trans. Med. Imaging 2011, 30, 484–496. [Google Scholar] [CrossRef]
- Rossant, F.; Bloch, I.; Ghorbel, I.; Paques, M. Parallel Double Snakes. Application to the segmentation of retinal layers in 2D-OCT for pathological subjects. Pattern Recognit. 2015, 48, 3857–3870. [Google Scholar] [CrossRef]
- Garvin, M.K.; Abramoff, M.D.; Wu, X.; Russell, S.R.; Burns, T.L.; Sonka, M. Automated 3-D Intraretinal Layer Segmentation of Macular Spectral-Domain Optical Coherence Tomography Images. IEEE Trans. Med. Imaging 2009, 28, 1436–1447. [Google Scholar] [CrossRef]
- Kafieh, R.; Rabbani, H.; Abramoff, M.D.; Sonka, M. Intra-retinal layer segmentation of 3D optical coherence tomography using coarse grained diffusion map. Med. Image Anal. 2013, 17, 907–928. [Google Scholar] [CrossRef]
- Novosel, J.; Thepass, G.; Lemij, H.G.; de Boer, J.F.; Vermeer, K.A.; van Vliet, L.J. Loosely coupled level sets for simultaneous 3D retinal layer segmentation in optical coherence tomography. Med. Image Anal. 2015, 26, 146–158. [Google Scholar] [CrossRef]
- Dodo, B.I.; Li, Y.; Eltayef, K.; Liu, X. Automatic annotation of retinal layers in optical coherence tomography images. J. Med. Syst. 2019, 43, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Duan, J.; Tench, C.; Gottlob, I.; Proudlock, F.; Bai, L. Automated segmentation of retinal layers from optical coherence tomography images using geodesic distance. Pattern Recognit. 2017, 72, 158–175. [Google Scholar] [CrossRef]
- Rong, Y.; Xiang, D.; Zhu, W.; Yu, K.; Shi, F.; Fan, Z.; Chen, X. Surrogate-assisted retinal OCT image classification based on convolutional neural networks. IEEE J. Biomed. Health Inform. 2019, 23, 253–263. [Google Scholar] [CrossRef]
- García, G.; del Amor, R.; Colomer, A.; Verdú-Monedero, R.; Morales-Sánchez, J.; Naranjo, V. Circumpapillary OCT-focused hybrid learning for glaucoma grading using tailored prototypical neural networks. Artif. Intell. Med. 2021, 118, 102132. [Google Scholar] [CrossRef]
- Fang, L.; Cunefare, D.; Wang, C.; Guymer, R.H.; Li, S.; Farsiu, S. Automatic segmentation of nine retinal layer boundaries in OCT images of non-exudative AMD patients using deep learning and graph search. Biomed. Opt. Express 2017, 8, 2732–2744. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Li, S.; He, Z.; Guan, H.; Chen, R.; Xu, Y.; Wang, T.; Qi, S.; Mei, J.; Wang, W. DeepRetina: Layer Segmentation of Retina in OCT Images Using Deep Learning. Transl. Vis. Sci. Technol. 2020, 9, 1–17. [Google Scholar] [CrossRef]
- Xiang, D.; Chen, G.; Shi, F.; Zhu, W.; Liu, Q.; Yuan, S.; Chen, X. Automatic Retinal Layer Segmentation of OCT Images With Central Serous Retinopathy. IEEE J. Biomed. Health Inform. 2019, 23, 283–295. [Google Scholar] [CrossRef]
- Morales, S.; Colomer, A.; Mossi, J.M.; Del Amor, R.; Woldbye, D.; Klemp, K.; Larsen, M.; Naranjo, V. Retinal layer segmentation in rodent OCT images: Local intensity profiles & fully convolutional neural networks. Comput. Methods Programs Biomed. 2021, 198, 105788. [Google Scholar] [CrossRef]
- Liu, X.; Cao, J.; Wang, S.; Zhang, Y.; Wang, M. Confidence-Guided Topology-Preserving Layer Segmentation for Optical Coherence Tomography Images With Focus-Column Module. IEEE Trans. Instrum. Meas. 2021, 70, 1–12. [Google Scholar] [CrossRef]
- Soille, P. Morphological Image Analysis: Principles and Applications, 2nd ed.; Springer: Berlin/Heidelberg, Germany, 2003. [Google Scholar]
- Weruaga, L.; Verdú, R.; Morales, J. Frequency Domain Formulation of Active Parametric Deformable Models. IEEE Trans. Pattern Anal. Mach. Intell. 2004, 26, 1568–1578. [Google Scholar] [CrossRef] [PubMed]
- Berenguer-Vidal, R.; Verdú-Monedero, R.; Morales-Sánchez, J. Design of B-spline multidimensional deformable models in the frequency domain. Math. Comput. Model. 2012, 57, 1942–1949. [Google Scholar] [CrossRef]
- Verdú-Monedero, R.; Morales-Sánchez, J.; Weruaga, L. Convergence analysis of active contours. Image Vis. Comput. 2008, 26, 1118–1128. [Google Scholar] [CrossRef]
- Berenguer-Vidal, R.; Verdú-Monedero, R.; Morales-Sánchez, J. Convergence analysis of multidimensional parametric deformable models. Comput. Vis. Image Underst. 2015, 135, 157–177. [Google Scholar] [CrossRef]
- Serra, J. Image Analysis and Mathematical Morphology; Academic Press: London, UK, 1982; Volume I. [Google Scholar]
- Serra, J. Image Analysis and Mathematical Morphology: Theoretical Advances; Academic Press: London, UK, 1988; Volume II. [Google Scholar]
- Xu, C.; Prince, J.L. Gradient Vector Flow Deformable Models; Handbook of Medical Imaging, Isaac Bankman; Academic Press: Cambridge, MA, USA, 2000. [Google Scholar]
- Terzopoulos, D. Deformable models: Classic, topology-adaptive and generalized formulations. In Geometric Level Set Methods in Imaging, Vision and Graphics; Osher, S., Paragios, N., Eds.; Springer: New York, NY, USA, 2003; Chapter 2; pp. 21–40. [Google Scholar]
- Liang, J.; McInerney, T.; Terzopoulos, D. United snakes. Med. Image Anal. 2006, 10, 215–233. [Google Scholar] [CrossRef]
- Bastida-Jumilla, M.; Menchon-Lara, R.; Morales-Sanchez, J.; Verdu-Monedero, R.; Larrey-Ruiz, J.; Sancho-Gomez, J. Frequency-domain active contours solution to evaluate intima-media thickness of the common carotid artery. Biomed. Signal Process. Control 2015, 16, 68–79. [Google Scholar] [CrossRef]
- Kass, M.; Witkin, A.; Terzopoulos, D. Snakes: Active contour models. Int. J. Comput. Vis. 1988, 1, 321–331. [Google Scholar] [CrossRef]
- Terzopoulos, D. The computation of visible surface representations. IEEE Trans. Pattern Anal. Mach. Intell. 1988, 10, 417–438. [Google Scholar] [CrossRef]
- Malladi, R.; Sethian, J.; Vemuri, B. Shape modeling with front propagation: A level set approach. IEEE Trans. Pattern Anal. Mach. Intell. 1995, 17, 158–175. [Google Scholar] [CrossRef]
- Cremers, D.; Schnorr, C.; Weickert, J. Diffusion-snakes: Combining statistical shape knowledge and image information in a variational framework. In Proceedings of the 1st IEEE Workshop on Variational and Level Set Methods in Computer Vision, Vancouver, BC, Canada, 13 July 2001; pp. 137–144. [Google Scholar]
- Wei, P.; Wang, W.; Yang, Y.; Wang, M.Y. Level set band method: A combination of density-based and level set methods for the topology optimization of continuums. Front. Mech. Eng. 2020, 15, 390–405. [Google Scholar] [CrossRef]
- Unser, M.; Aldroubi, A.; Eden, M. B-spline signal processing: Part I - Theory; Part II - Efficient design and applications. IEEE Trans. Signal Process. 1993, 41, 821–848. [Google Scholar] [CrossRef]
- Oppenheim, A.; Schafer, R. Discrete-Time Signal Processing, 2nd ed.; Prentice-Hall: Upper Saddle River, NJ, USA, 1999. [Google Scholar]
- Gonzalez, R.C.; Woods, R.E. Digital Image Processing, 3rd ed.; Prentice-Hall, Inc.: Upper Saddle River, NJ, USA, 2006. [Google Scholar]
- Amor, R.d.; Morales, S.; Colomer, A.n.; Mossi, J.M.; Woldbye, D.; Klemp, K.; Larsen, M.; Naranjo, V. Towards Automatic Glaucoma Assessment: An Encoder-decoder CNN for Retinal Layer Segmentation in Rodent OCT images. In Proceedings of the 27th European Signal Processing Conference (EUSIPCO), A Coruña, Spain, 2–6 September 2019; pp. 1–5. [Google Scholar] [CrossRef]
- Dice, L.R. Measures of the amount of ecologic association between species. Ecology 1945, 26, 297–302. [Google Scholar] [CrossRef]
- Laligant, O.; Truchetet, F.; Fauvet, E. Noise estimation from digital step-model signal. IEEE Trans. Image Process. 2013, 22, 5158–5167. [Google Scholar] [CrossRef]




















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Eye | Healthy | Suspicious | Unhealthy |
|---|---|---|---|
| Left | 88 | 31 | 43 |
| Right | 97 | 32 | 38 |
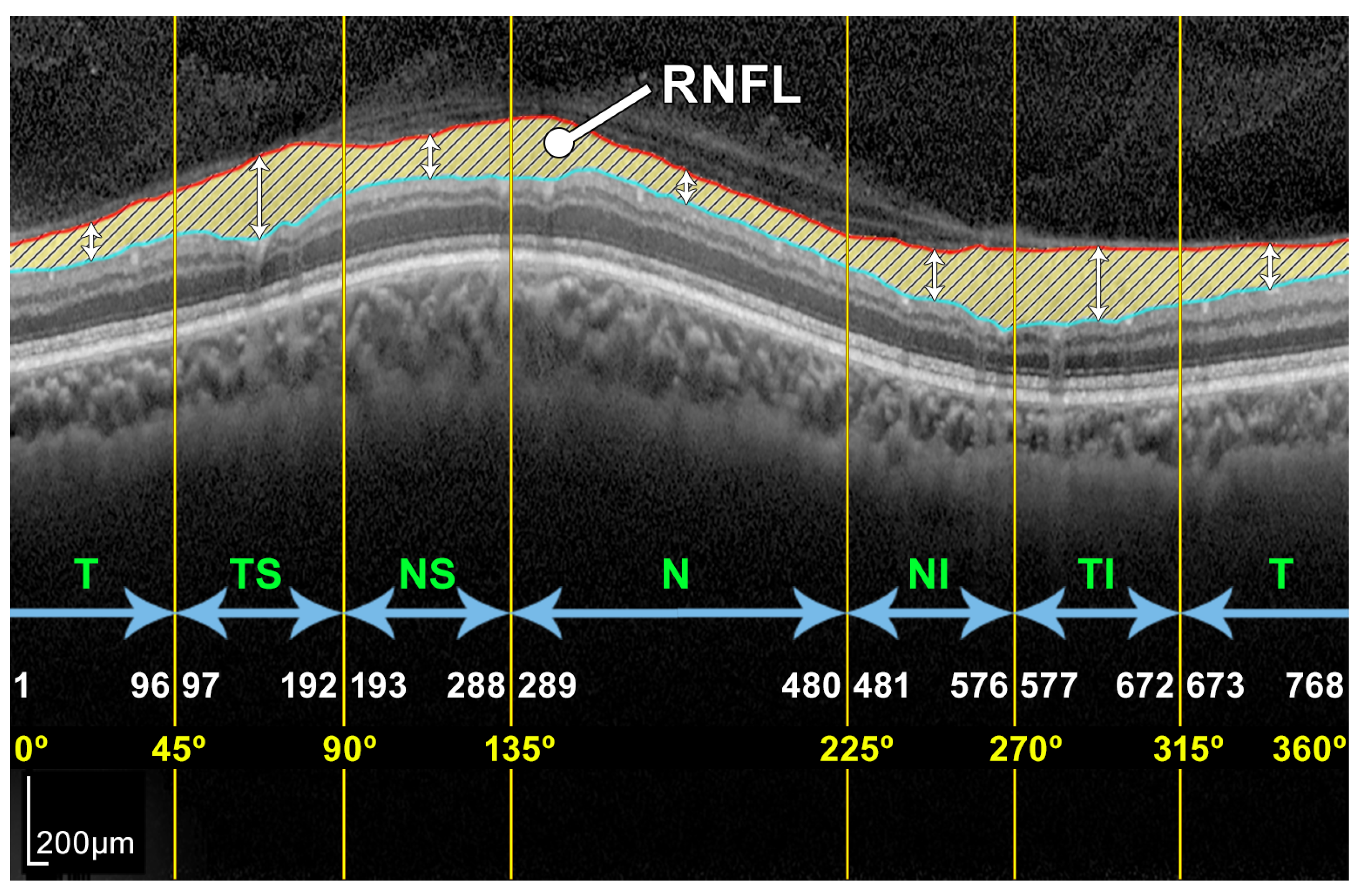
| Sector | Polar (Degrees) | Cartesian (Pixels) | ||
|---|---|---|---|---|
| Min | Max | Min | Max | |
| Temporal (T) | 0° | 45° | 1 | 96 |
| Temporal Superior (TS) | 45° | 90° | 97 | 192 |
| Nasal Superior (NS) | 90° | 135° | 193 | 288 |
| Nasal (N) | 135° | 225° | 289 | 480 |
| Nasal Inferior (NI) | 225° | 270° | 481 | 576 |
| Temporal Inferior (TI) | 270° | 315° | 577 | 672 |
| Temporal (T) | 315° | 360° | 673 | 768 |
| Dice Similarity Coefficient | ||||||
|---|---|---|---|---|---|---|
| Patient 2 | Patient 20 | Patient 69 | ||||
| Sectors | Proposed | H-DLpNet | Proposed | H-DLpNet | Proposed | H-DLpNet |
| Method | Method | Method | ||||
| TS | ||||||
| T | ||||||
| TI | ||||||
| NS | ||||||
| N | ||||||
| NI | ||||||
| G | ||||||
| Sectors | RNFL Thickness Measurement (µm) | |||
|---|---|---|---|---|
| Proposed | H-DLpNet | Spectralis | ||
| Left eye | TS | 122.8 ± 23.6 | 128.5 ± 27.4 | 121.7 ± 30.5 |
| T | 79.0 ± 11.6 | 70.7 ± 13.9 | 67.3 ± 13.3 | |
| TI | 136.2 ± 30.2 | 132.7 ± 31.8 | 127.4 ± 34.8 | |
| NS | 116.0 ± 21.4 | 111.4 ± 28.1 | 105.5 ± 30.2 | |
| N | 86.5 ± 15.7 | 74.7 ± 16.4 | 68.7 ± 19.1 | |
| NI | 114.2 ± 23.6 | 109.1 ± 27.1 | 102.2 ± 28.0 | |
| G | 102.5 ± 13.2 | 96.6 ± 17.0 | 90.9 ± 17.8 | |
| Right eye | TS | 126.5 ± 24.9 | 129.8 ± 25.5 | 125.2 ± 29.5 |
| T | 80.9 ± 14.0 | 72.7 ± 15.6 | 68.6 ± 15.6 | |
| TI | 133.4 ± 26.0 | 131.9 ± 29.9 | 126.0 ± 34.3 | |
| NS | 112.0 ± 23.5 | 106.0 ± 27.6 | 98.6 ± 27.4 | |
| N | 90.9 ± 14.9 | 79.6 ± 16.3 | 72.8 ± 17.9 | |
| NI | 113.4 ± 23.5 | 105.9 ± 25.8 | 102.6 ± 27.3 | |
| G | 103.6 ± 13.6 | 97.3 ± 16.7 | 92.0 ± 17.8 | |
| Sectors | Absolute Thickness Errors (µm) | Relative Thickness Errors | |||
|---|---|---|---|---|---|
| H-DLpNet | Spectralis | H-DLpNet | Spectralis | ||
| Left eye | TS | 13.1 ± 11.8 | 14.5 ± 12.9 | 0.12 ± 0.11 | 0.13 ± 0.12 |
| T | 8.3 ± 6.1 | 11.8 ± 7.8 | 0.11 ± 0.09 | 0.15 ± 0.10 | |
| TI | 10.0 ± 18.1 | 11.9 ± 10.0 | 0.08 ± 0.08 | 0.10 ± 0.11 | |
| NS | 12.3 ± 10.9 | 14.9 ± 12.6 | 0.11 ± 0.10 | 0.14 ± 0.12 | |
| N | 11.7 ± 11.0 | 17.6 ± 13.3 | 0.13 ± 0.12 | 0.20 ± 0.14 | |
| NI | 10.3 ± 9.2 | 13.5 ± 11.4 | 0.10 ± 0.09 | 0.13 ± 0.11 | |
| G | 6.9 ± 6.1 | 10.8 ± 8.0 | 0.07 ± 0.07 | 0.11 ± 0.09 | |
| Right eye | TS | 12.1 ± 10.4 | 12.8 ± 11.2 | 0.10 ± 0.10 | 0.11 ± 0.10 |
| T | 8.3 ± 6.0 | 12.1 ± 7.9 | 0.11 ± 0.08 | 0.15 ± 0.10 | |
| TI | 12.8 ± 11.0 | 15.2 ± 12.4 | 0.11 ± 0.10 | 0.13 ± 0.12 | |
| NS | 10.1 ± 9.5 | 15.2 ± 13.5 | 0.10 ± 0.09 | 0.14 ± 0.12 | |
| N | 11.3 ± 9.3 | 17.3 ± 12.9 | 0.13 ± 0.10 | 0.19 ± 0.14 | |
| NI | 10.9 ± 9.6 | 13.0 ± 10.5 | 0.10 ± 0.09 | 0.12 ± 0.10 | |
| G | 7.4 ± 6.4 | 10.4 ± 7.3 | 0.08 ± 0.07 | 0.11 ± 0.08 | |
| Sectors | Dice Similarity Coefficient | |
|---|---|---|
| H-DLpNet | ||
| Left eye | TS | 0.895 ± 0.082 |
| T | 0.918 ± 0.071 | |
| TI | 0.921 ± 0.057 | |
| NS | 0.898 ± 0.059 | |
| N | 0.893 ± 0.078 | |
| NI | 0.917 ± 0.057 | |
| G | 0.908 ± 0.047 | |
| Right eye | TS | 0.906 ± 0.059 |
| T | 0.919 ± 0.053 | |
| TI | 0.914 ± 0.074 | |
| NS | 0.907 ± 0.054 | |
| N | 0.902 ± 0.063 | |
| NI | 0.917 ± 0.062 | |
| G | 0.911 ± 0.047 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Berenguer-Vidal, R.; Verdú-Monedero, R.; Morales-Sánchez, J.; Sellés-Navarro, I.; del Amor, R.; García, G.; Naranjo, V. Automatic Segmentation of the Retinal Nerve Fiber Layer by Means of Mathematical Morphology and Deformable Models in 2D Optical Coherence Tomography Imaging. Sensors 2021, 21, 8027. https://doi.org/10.3390/s21238027
Berenguer-Vidal R, Verdú-Monedero R, Morales-Sánchez J, Sellés-Navarro I, del Amor R, García G, Naranjo V. Automatic Segmentation of the Retinal Nerve Fiber Layer by Means of Mathematical Morphology and Deformable Models in 2D Optical Coherence Tomography Imaging. Sensors. 2021; 21(23):8027. https://doi.org/10.3390/s21238027
Chicago/Turabian StyleBerenguer-Vidal, Rafael, Rafael Verdú-Monedero, Juan Morales-Sánchez, Inmaculada Sellés-Navarro, Rocío del Amor, Gabriel García, and Valery Naranjo. 2021. "Automatic Segmentation of the Retinal Nerve Fiber Layer by Means of Mathematical Morphology and Deformable Models in 2D Optical Coherence Tomography Imaging" Sensors 21, no. 23: 8027. https://doi.org/10.3390/s21238027
APA StyleBerenguer-Vidal, R., Verdú-Monedero, R., Morales-Sánchez, J., Sellés-Navarro, I., del Amor, R., García, G., & Naranjo, V. (2021). Automatic Segmentation of the Retinal Nerve Fiber Layer by Means of Mathematical Morphology and Deformable Models in 2D Optical Coherence Tomography Imaging. Sensors, 21(23), 8027. https://doi.org/10.3390/s21238027