
A Real-Time, Automatic, and Dynamic Scheduling and Control System for PET Patients Based on Wearable Sensors


Abstract
:1. Introduction
1.1. Reservation Scheduling
1.2. Real-Time Scheduling
1.3. Smart Device Applications
1.4. Current Status and Issues of PET Patient Scheduling
1.5. Overview of Results
1.6. Our Contribution
2. Methods
2.1. System Requirement
2.2. Details of the Proposed System
2.2.1. Initial Phase
2.2.2. Patient Check-In Phase
2.2.3. Patient Indwelling Needle Phase
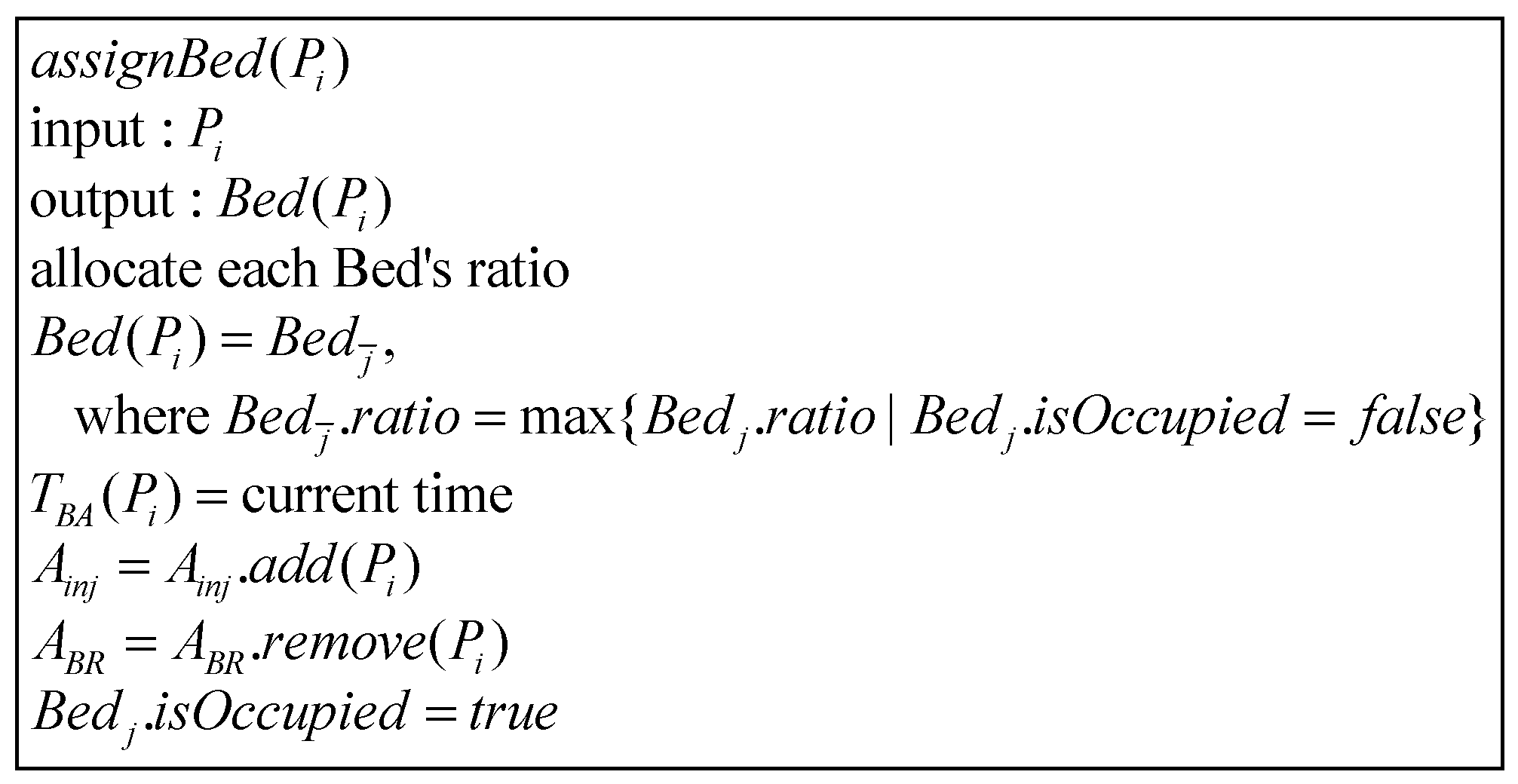
2.2.4. Bed Allocation Phase
2.2.5. Algorithm for Scheduling Examination Room, and Estimating Injection and Examination Time
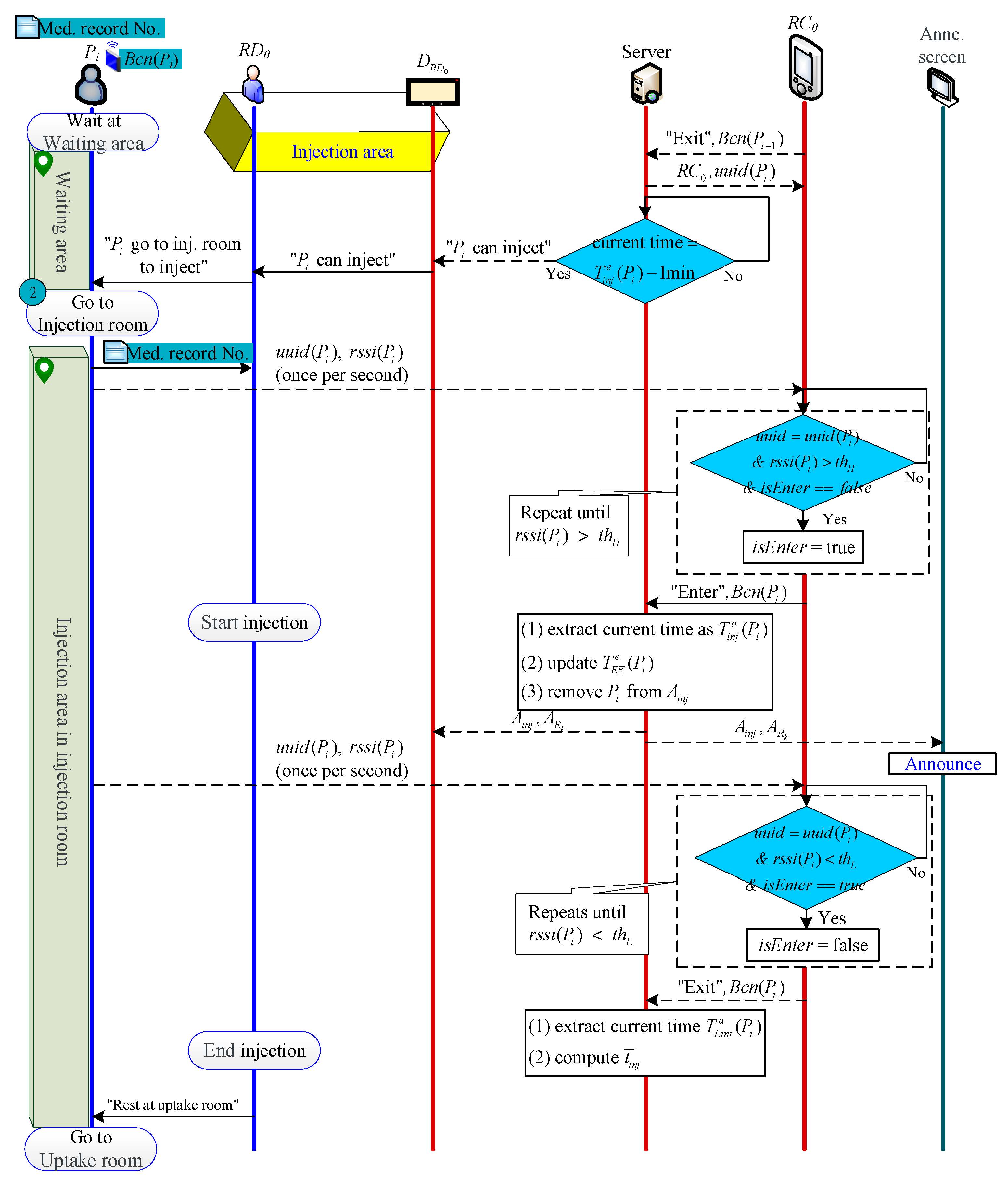
2.2.6. Injection Phase
2.2.7. Scanning Phase
2.2.8. End Examination Phase
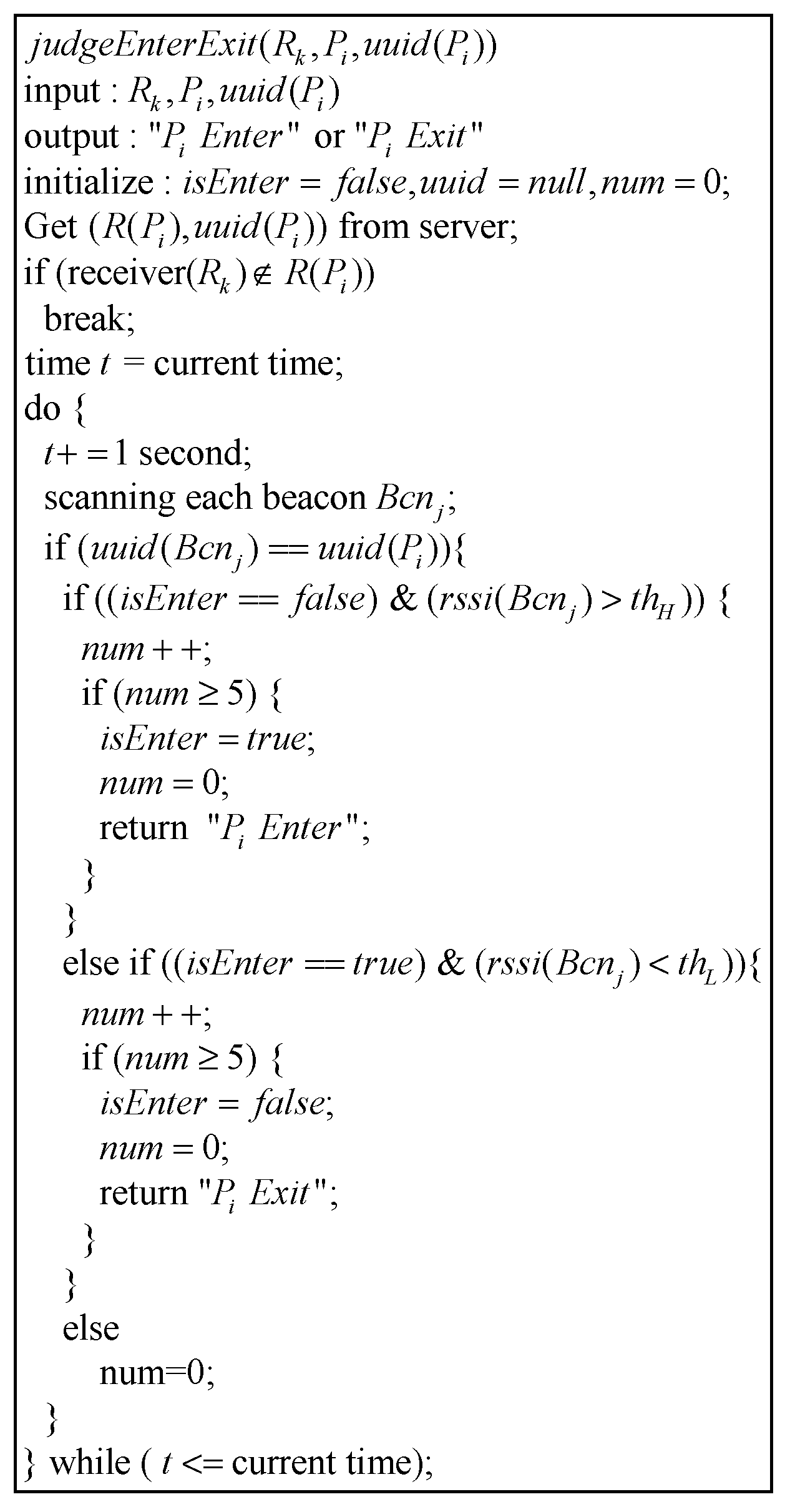
2.2.9. Algorithm to Determine Beacon’s Entering or Leaving from a Certain Area
3. Materials
3.1. Data Collection of Control Group
3.1.1. Patient Check-In
3.1.2. Indwelling Needle and Injection Phase
3.1.3. Patients’ Queue List and Scan Room Waiting List for Each Scan Room
3.1.4. Total Queue List
3.2. Data Collection of Experimental Group
3.2.1. Estimate Time to Indwell Time Initially
3.2.2. Update the Estimated Time to Indwell Needle
3.2.3. Update Available Beds
3.2.4. Schedule Scan Room and Estimate Injection/Scan Time
- A.
- Arrange beds
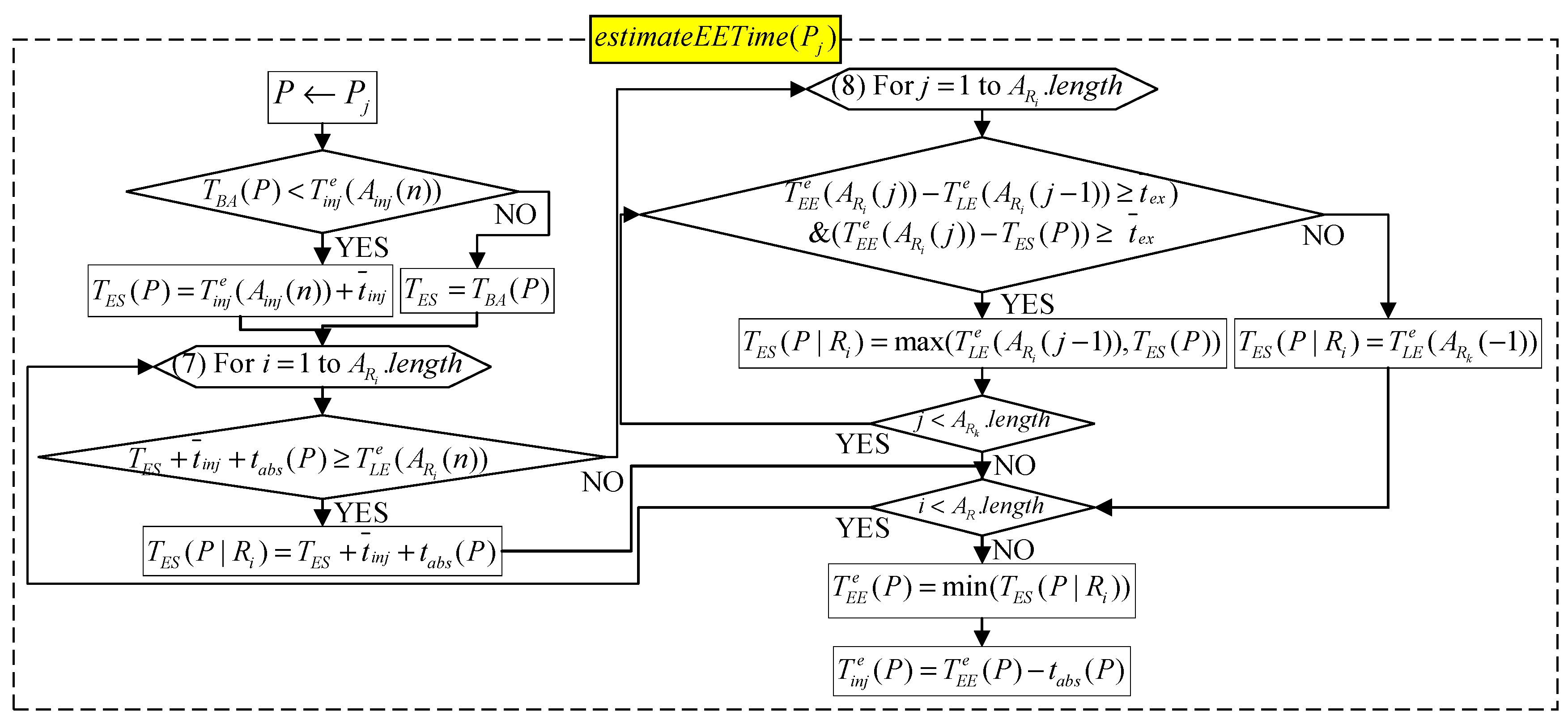
- B. Estimate injection time and scan time
4. Discussion
4.1. Analysis of Indwelling Needle Time
4.2. Analysis of Injection and Scan Times
4.3. Analysis of Allocating Beds
4.4. Overall Improvement
5. Comparison
5.1. Comparison with Proposed and Current Scheduling System
- Scheduling of patient examination order: The system automatically orders the order of patient examinations, eliminating the need for radiographers to manually order.
- Scheduling of each inspection time: The system calculates the best patient examination time for different drug cycle times, and the radiographer does not need to calculate it manually.
- Patient interrupts MS workflow by asking questions about examination time: The system calculates the estimated time of each inspection task and announces it to medical staff and patients, reducing the number of times when medical staff are interrupted by patient inquiries.
- Dispensing reminder: The pharmacist checks the app’s patient injection status to dispense medicine, eliminating the need for MS to call and let the pharmacist dispense medicine.
- Patient estimated time reminder: The system sends a reminder message when the estimated time for each patient task is approaching.
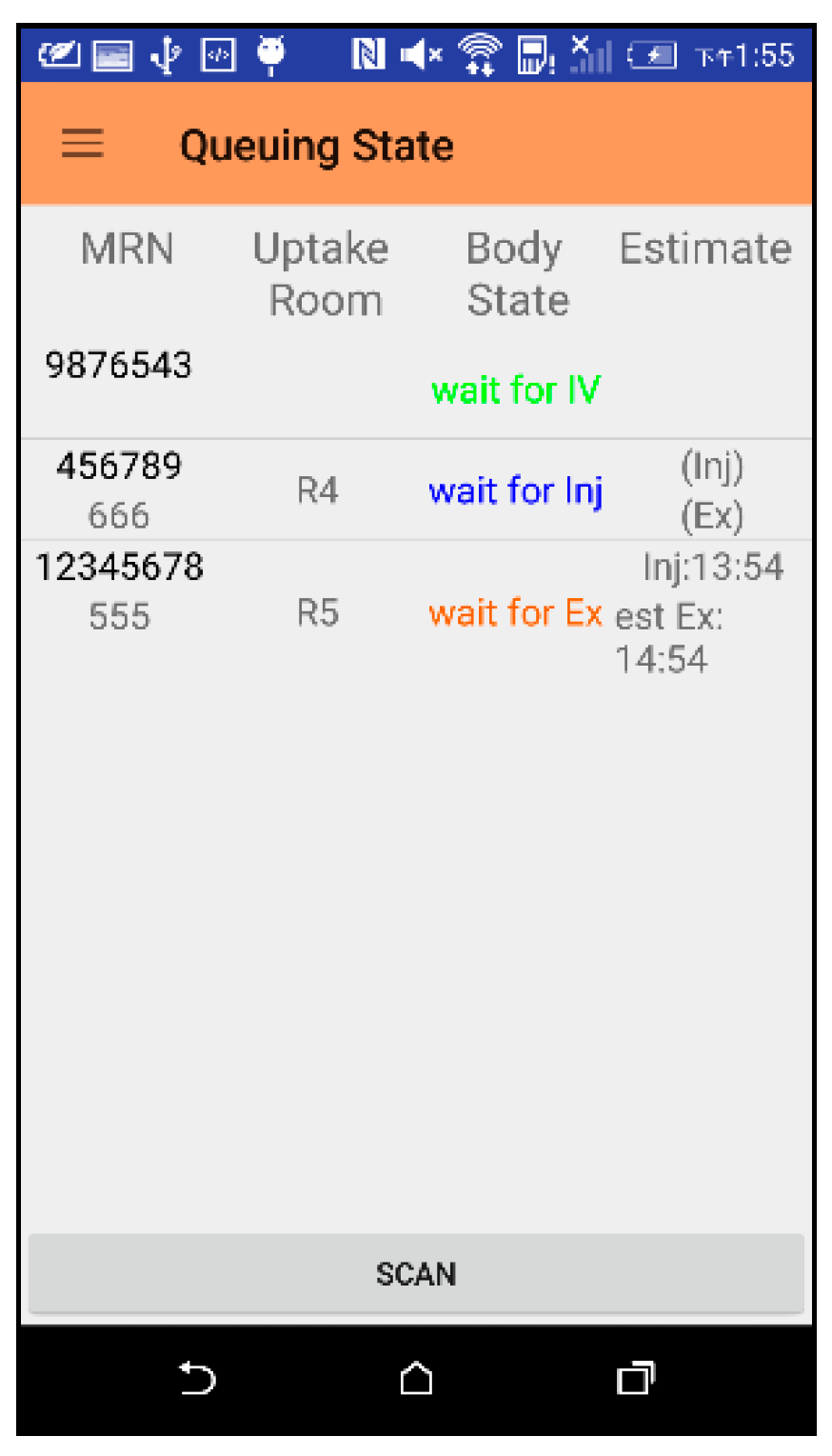
- Patient and family inquiries: Patients and family members can check the examination time by themselves, reducing the number of inquiries.
5.2. Comparison of Proposed and Previous Works
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Burdett, R.L.; Kozan, E. Techniques to effectively buffer schedules in the face of uncertainties. Comput. Ind. Eng. 2015, 87, 16–29. [Google Scholar] [CrossRef] [Green Version]
- Jiang, B.; Tang, J.; Yanb, C. A stochastic programming model for outpatient appointment scheduling considering unpunctuality. Omega 2019, 82, 70–82. [Google Scholar] [CrossRef]
- Qiu, H.; Wang, D.; Wang, Y.; Yin, Y. MRI appointment scheduling with uncertain examination time. J. Comb. Optim. 2019, 37, 62–82. [Google Scholar] [CrossRef]
- Wu, X.; Li, J.; Xu, R.; Yu, T. A simulation study of appointment scheduling for multi-class MRI examination. In Proceedings of the 2016 13th International Conference on Service Systems and Service Management (ICSSSM), Kunming, China, 24–26 June 2016; pp. 1–6. [Google Scholar]
- Xiao, Q.; Luo, L.; Zhao, S.; Ran, X.; Feng, Y. Online appointment scheduling for a nuclear medicine department in a Chinese hospital. Comput. Math. Methods Med. 2018, 2018, 5148215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azadeh, A.; Baghersad, M.; Farahani, M.H.; Zarrin, M. Semi-online patient scheduling in pathology laboratories. Artif. Intell. Med. 2015, 64, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Peng, Y.; Qu, X.; Shi, J. A hybrid simulation and genetic algorithm approach to determine the optimal scheduling templates for open access clinics admitting walk-in patients. Comput. Ind. Eng. 2014, 72, 282–296. [Google Scholar] [CrossRef]
- Montecinos, J.; Ouhimmou, M.; Chauhan, S. Waiting-time estimation in walk-in clinics. Int. Trans. Oper. Res. 2018, 25, 51–74. [Google Scholar] [CrossRef]
- Tantitharanukul, N.; Throngjai, T. Waiting time estimation system for outpatient’s arrival planning. In Proceedings of the 2018 International Conference on Digital Arts, Media and Technology (ICDAMT), Chiangrai, Thailand, 25–28 February 2018; pp. 207–212. [Google Scholar]
- Obulor, R.; Eke, B.O. Outpatient queuing model development for hospital appointment system. Int. J. Sci. Eng. Appl. Sci. 2016, 2, 15–22. [Google Scholar]
- Qu, X.; Peng, Y.; Shi, J.; LaGanga, L. An MDP model for walk-in patient admission management in primary care clinics. Int. J. Prod. Econ. 2015, 168, 303–320. [Google Scholar] [CrossRef]
- Luscombe, R.; Kozan, E. Dynamic resource allocation to improve emergency department efficiency in real time. Eur. J. Oper. Res. 2016, 255, 593–603. [Google Scholar] [CrossRef]
- Burdett, R.L.; Kozan, E. An integrated approach for scheduling health care activities in a hospital. Eur. J. Oper. Res. 2018, 264, 756–773. [Google Scholar] [CrossRef] [Green Version]
- Wiesche, L.; Schacht, M.; Werners, B. Strategies for interday appointment scheduling in primary care. Health Care Manag. Sci. 2017, 20, 403–418. [Google Scholar] [CrossRef] [PubMed]
- Kortbeek, N.; Zonderland, M.E.; Braaksma, A.; Vliegen, I.M.; Boucherie, R.J.; Litvak, N.; Hans, E.W. Designing cyclic appointment schedules for outpatient clinics with scheduled and unscheduled patient arrivals. Perform. Eval. 2014, 80, 5–26. [Google Scholar] [CrossRef] [Green Version]
- Cho, M.; Song, M.; Yoo, S.; Reijers, H.A. An evidence-based decision support framework for clinician medical scheduling. IEEE Access 2019, 7, 5239–15249. [Google Scholar] [CrossRef]
- Yu, J.; Xing, L.; Tan, X.; Ren, T.; Li, Z. Doctor-Patient Combined Matching Problem and its Solving Algorithms. IEEE Access 2019, 7, 177723–177733. [Google Scholar] [CrossRef]
- Jiang, S.; Xiao, R.; Wang, L.; Luo, X.; Huang, C.; Wang, J.-H.; Chin, K.-S.; Nie, X. Combining Deep Neural Networks and classical time series regression models for forecasting patient flows in Hong Kong. IEEE Access 2019, 7, 118965–118974. [Google Scholar] [CrossRef]
- Frisby, J.; Smith, V.; Traub, S.; Patel, V.L. Contextual computing: A Bluetooth based approach for tracking healthcare providers in the emergency room. J. Biomed. Inform. 2017, 65, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Ewing, A.; Rogus, J.; Chintagunta, P.; Logan, K.; Morgan, S.; Hyojung, K. A systems approach to improving patient flow at UVA Cancer Center using Real-Time Locating System. In Proceedings of the 2017 Systems and Information Engineering Design Symposium (SIEDS), Charlottesville, VA, USA, 28 April 2017; pp. 259–264. [Google Scholar]
- Elnahrawy, E.; Martin, R.P. Studying the utility of tracking systems in improving healthcare workflow. In Proceedings of the 2010 8th IEEE International Conference on Pervasive Computing and Communications Workshops (PERCOM Workshops), Mannheim, Germany, 29 March–2 April 2010; pp. 310–315. [Google Scholar]
- Naruse, F.; Kaji, K. Estimation of Person Existence in Room Using BLE Beacon and Its Platform. In Proceedings of the 2018 International Conference on Mobile Computing, Applications, and Services (MobiCASE), Osaka, Japan, 28 February–2 March 2018; pp. 251–257. [Google Scholar]



















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Notation | Definition |
|---|---|
| The i-th patient | |
| The medical staff (nurse) in | |
| The radiographer in the j-th scan room | |
| Server | |
| IV catheter indwelling room | |
| Inner injection room | |
| The k-th examination room | |
| The j-th bed ( = 1, 2, 3, …) | |
| The j-th Beacon | |
| Signal strength of | |
| / | Threshold of RSSI strong/weak signals |
| / | Device of / |
| / | Receivers of / |
| List of patients waiting for IV catheter indwelling | |
| List of patients waiting for injection | |
| List of patients requesting beds | |
| List of available beds | |
| List of patients waiting for | |
| The α-th element of the list | |
| The last α-th element of the list | |
| Body status of (bedridden or non-bedridden) | |
| Drug absorption time of (e.g., 30 min) | |
| Time difference between estimated and actual IV catheter indwelling | |
| Time difference between estimated and actual injection | |
| The average IV catheter indwelling time until the α-th time | |
| The average injection time until the α-th time | |
| The average examination time until the α-th time | |
| The bed of | |
| The Beacon of | |
| The UUID of | |
| The medical record number for | |
| The scan/examination room for | |
| The examination check-out time for | |
| / | The estimated/actual IV catheter indwelling time for |
| / | ’s estimated/actual time to leave the IV room |
| / | The estimated/actual injection time for (e.g., 10:00 a.m.) |
| / | ’s estimated/actual time to leave the injection room |
| The estimated/actual time to enter the examination room for (e.g., 10:00 a.m.) | |
| / | The estimated/actual time to leave the examination room for (e.g., 10:00 a.m.) |
| The bed vacated time of | |
| The bed available time for | |
| The earliest injection time for | |
| The earliest scan/examination time for | |
| The earliest scan/examination time at for | |
| Time for doctor to finish ’s DICOM image interpretation |
| A | B | C | ||
|---|---|---|---|---|
| Bedridden | 6 | 0 | 0 | |
| General and | 1 | 3 | 2 | |
| General | 1 | 2 | 3 | |
| Time Difference | Indwelling Needle | Injection | Scan | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Absolute Value | Relative Value | Ahead Rate | Absolute Value | Relative Value | Ahead Rate | Absolute Value | Relative Value | Ahead Rate | |
| Day 1 | 4.17 | −1.00 | 33% | 4.91 | −4.00 | 91% | 7.00 | 0.25 | 18.2% |
| Day 2 | 3.62 | −1.32 | 58% | 6.50 | −6.50 | 100% | 5.33 | −4.17 | 75% |
| Day 3 | 1.67 | −0.92 | 33% | 12.36 | −12.36 | 100% | 5.91 | −0.43 | 64% |
| Day 4 | 4.73 | −0.58 | 2% | 4.20 | −4.00 | 80% | 9.20 | 1.20 | 30% |
| Day 5 | 1.67 | −1.00 | 54% | 14.91 | −14.91 | 100% | 8.73 | −0.53 | 64% |
| Day 6 | 2.93 | −1.32 | 53% | 8.21 | −8.21 | 100% | 5.71 | 1.00 | 35.7% |
| Day 7 | 2.38 | −0.92 | 50% | 11.27 | 2.87 | 93% | 12.33 | 1.01 | 13% |
| Day 8 | 1.88 | −0.58 | 31% | 5.20 | −4.93 | 53% | 3.93 | 2.33 | 33% |
| Day 9 | 2.71 | −1.00 | 71% | 5.77 | −0.85 | 54% | 7.85 | 0.78 | 0% |
| Day 10 | 2.79 | −1.32 | 63% | 7.31 | −6.69 | 94% | 7.50 | −3.25 | 56% |
| Day 11 | 3.25 | −0.92 | 62% | 4.65 | −4.48 | 78% | 5.74 | 0.96 | 43% |
| Day 12 | 3.53 | −0.58 | 57% | 10.06 | −9.61 | 89% | 8.56 | −6.11 | 72% |
| Average | 2.94 | −0.96 | 47% | 7.95 | −6.14 | 86% | 7.32 | −0.58 | 42% |
| Standard error | 0.93 | 0.26 | 0.18 | 3.32 | 4.61 | 0.16 | 2.14 | 2.45 | 0.23 |
| Indwelling Needle | Injection | Scan | |
|---|---|---|---|
| Maximum | 17 | 23 | 33 |
| Minimum | −12 | −29 | −25 |
| Without b() | With b() | |
|---|---|---|
| Day 1 | 6 min | 2 min |
| Day 2 | 18 min | 16 min |
| Day 3 | 3 min | 1 min |
| Day 4 | 10 min | 6 min |
| Day 5 | 14 min | 7 min |
| Day 6 | 1 min | 1 min |
| Day 7 | 5 min | 1 min |
| Average | 8.14 min | 4.86 min |
| Tasks | Current System | Proposed System | |
|---|---|---|---|
| Medical staff | A. Order scheduling | Manual scheduling (10 s) | App automatic scheduling (0 s) |
| B. Inspection time scheduling | Manual calculation (60 s) | App automatic calculation (1 s) | |
| C. Being interrupted | MS was interrupted due to patients inquiry times (30 s) | MS was not interrupted because patients watched the screen by themselves (0 s) | |
| D. Dispensing reminder | MS calls pharmacist (30 s) | Pharmacist checks the APP device (0 s) | |
| E. Patient estimated time reminder | MS pay attention to patient examination time (anytime) | MS waits for APP notification (0 s) | |
| Patient (family) | F. Time inquiry | Manual inquiry MS (30 s) | View announcements (5 s) |
| [5] | [9] | [12] | Proposed | |
|---|---|---|---|---|
| (1) Real-time automatic scheduling | v | v | ||
| (2) Scheduling for different medicines | v | v | ||
| (3) Dynamic update of prediction time | v | v | v | |
| (4) Immediate provision of predictive inspection time | v | v | ||
| (5) Automatic allocation of general and specific beds | v | v | ||
| (6) Automatic detection of all patients’ tasks periods | v | |||
| (7) Automatic detection and prediction of examination room conditions | v | |||
| (8) Instant rescheduling | v |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiou, S.-Y.; Lin, K.-J.; Dong, Y.-X. A Real-Time, Automatic, and Dynamic Scheduling and Control System for PET Patients Based on Wearable Sensors. Sensors 2021, 21, 1104. https://doi.org/10.3390/s21041104
Chiou S-Y, Lin K-J, Dong Y-X. A Real-Time, Automatic, and Dynamic Scheduling and Control System for PET Patients Based on Wearable Sensors. Sensors. 2021; 21(4):1104. https://doi.org/10.3390/s21041104
Chicago/Turabian StyleChiou, Shin-Yan, Kun-Ju Lin, and Ya-Xin Dong. 2021. "A Real-Time, Automatic, and Dynamic Scheduling and Control System for PET Patients Based on Wearable Sensors" Sensors 21, no. 4: 1104. https://doi.org/10.3390/s21041104
APA StyleChiou, S. -Y., Lin, K. -J., & Dong, Y. -X. (2021). A Real-Time, Automatic, and Dynamic Scheduling and Control System for PET Patients Based on Wearable Sensors. Sensors, 21(4), 1104. https://doi.org/10.3390/s21041104