
Effect of Short-Term Exposure to Supplemental Vibrotactile Kinesthetic Feedback on Goal-Directed Movements after Stroke: A Proof of Concept Case Series

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Clinical Evaluations
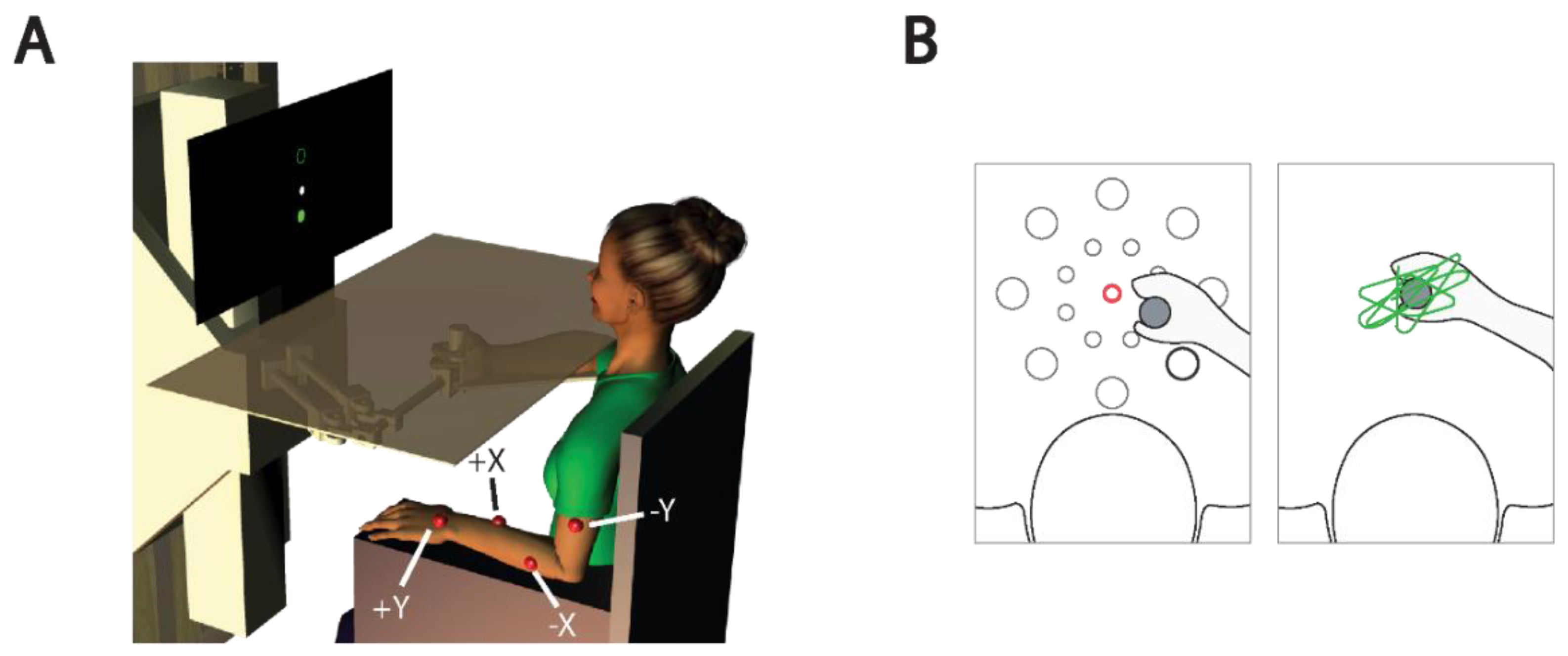
2.3. Experimental Set-Up
2.4. Tasks
2.4.1. Reaching
2.4.2. Stabilizing
2.5. Vibrotactile Interface
2.6. Kinesthetic Feedback Encoding Schemes
2.6.1. State Feedback
2.6.2. Error Feedback
2.7. Experimental Protocol
2.7.1. Familiarization (V+T−)
2.7.2. Practice (VKRT+)
2.7.3. Assessment (V−)
2.8. Subjective Self-Report Evaluation of the Vibratory Stimuli
2.9. Data Analysis
3. Results
3.1. Subjective Evaluations of Supplemental Vibrotactile Feedback
3.1.1. User Satisfaction
3.1.2. Usability
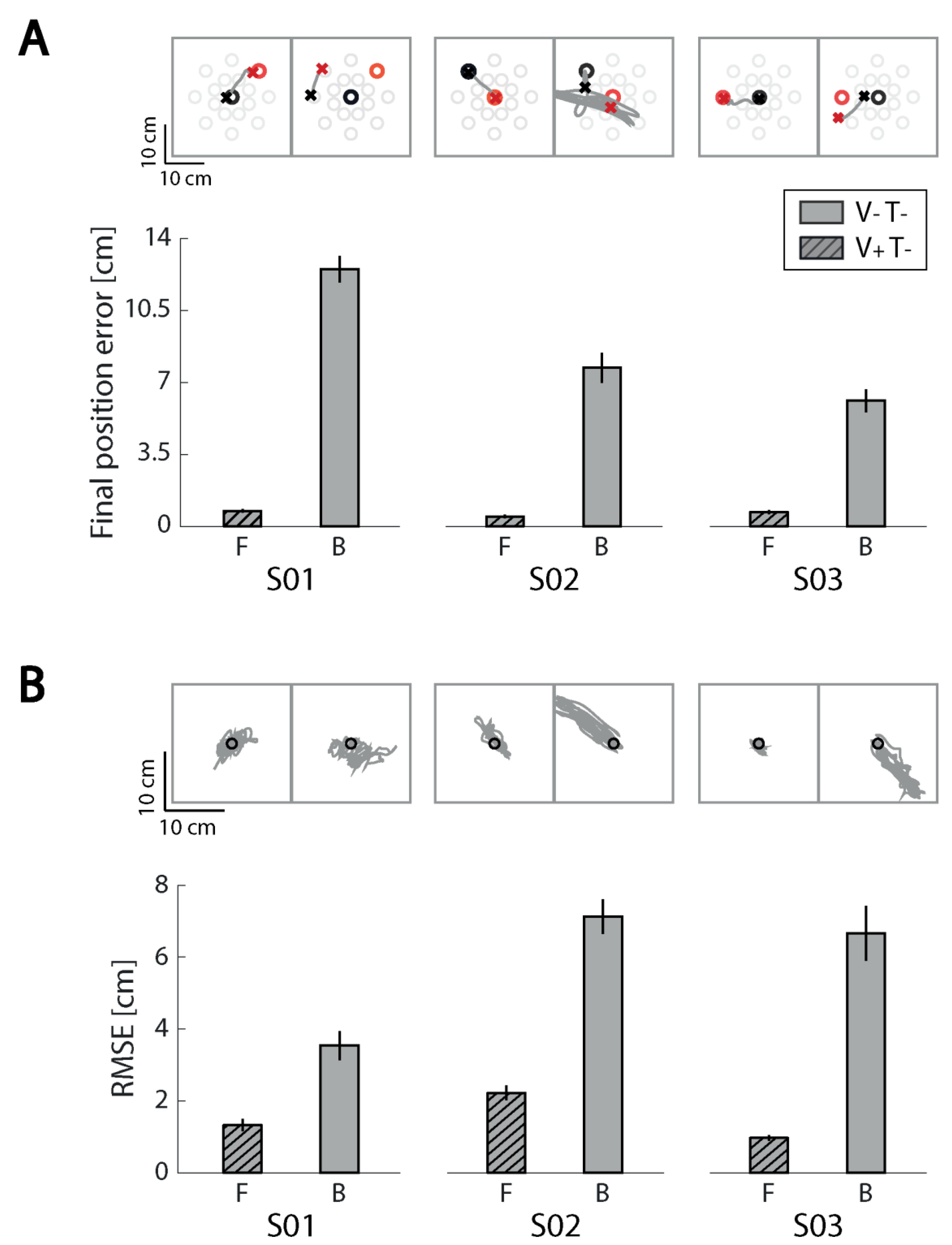
3.2. General Observations on Kinematic Performance with and without Ongoing Visual Feedback
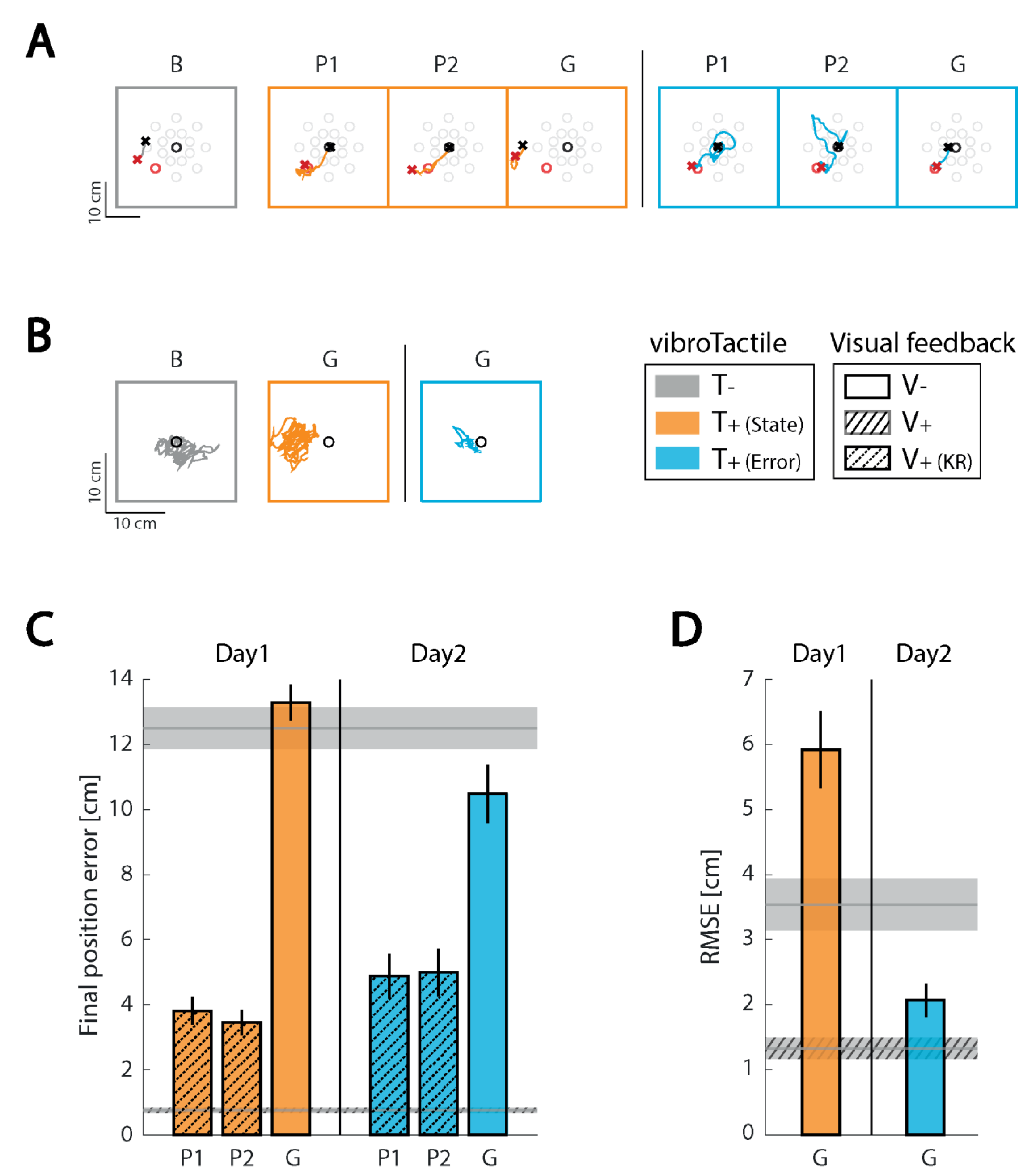
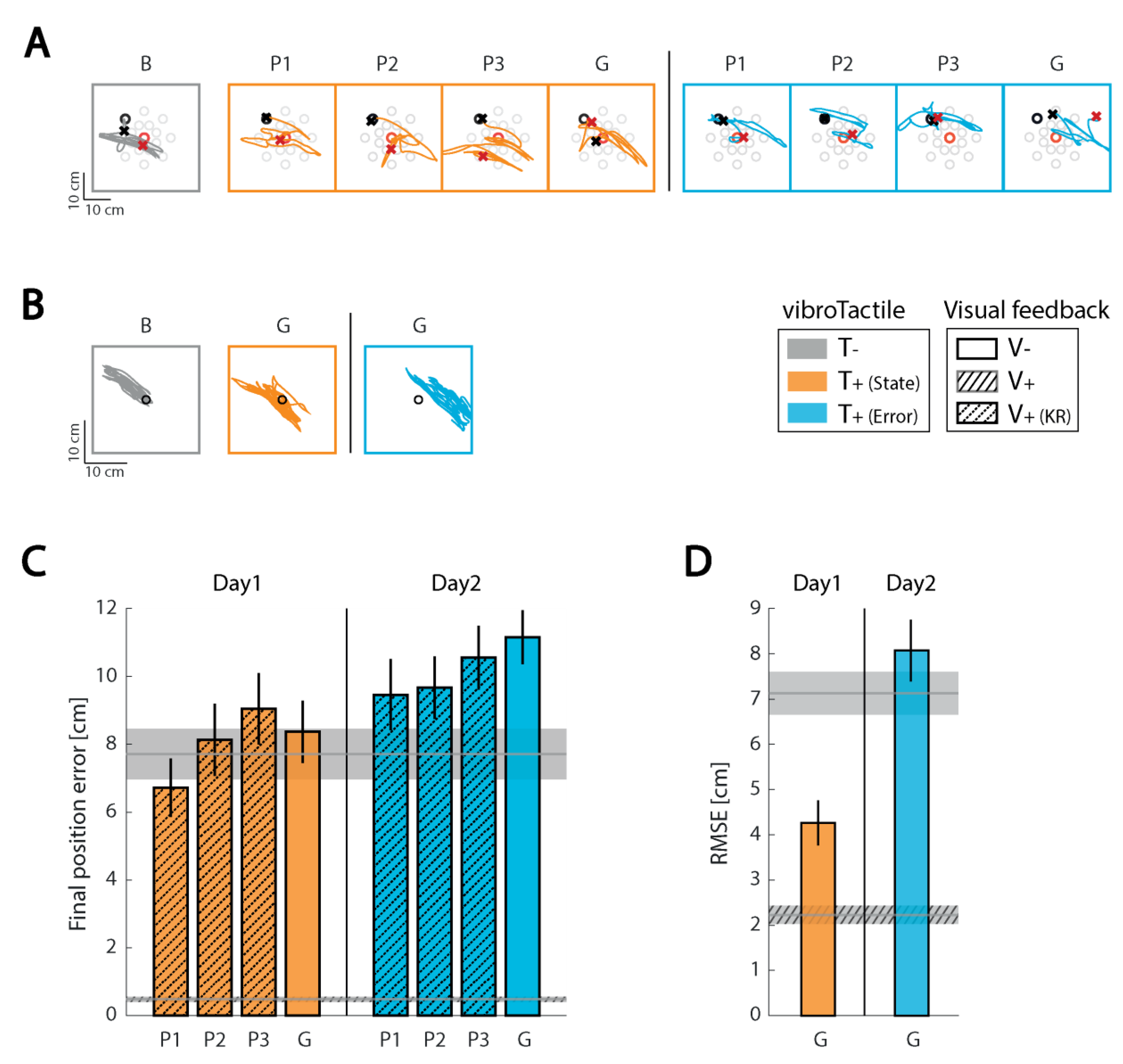
3.3. Effects of Supplemental Kinesthetic Feedback on Performance of Reaching and Stabilizing Tasks
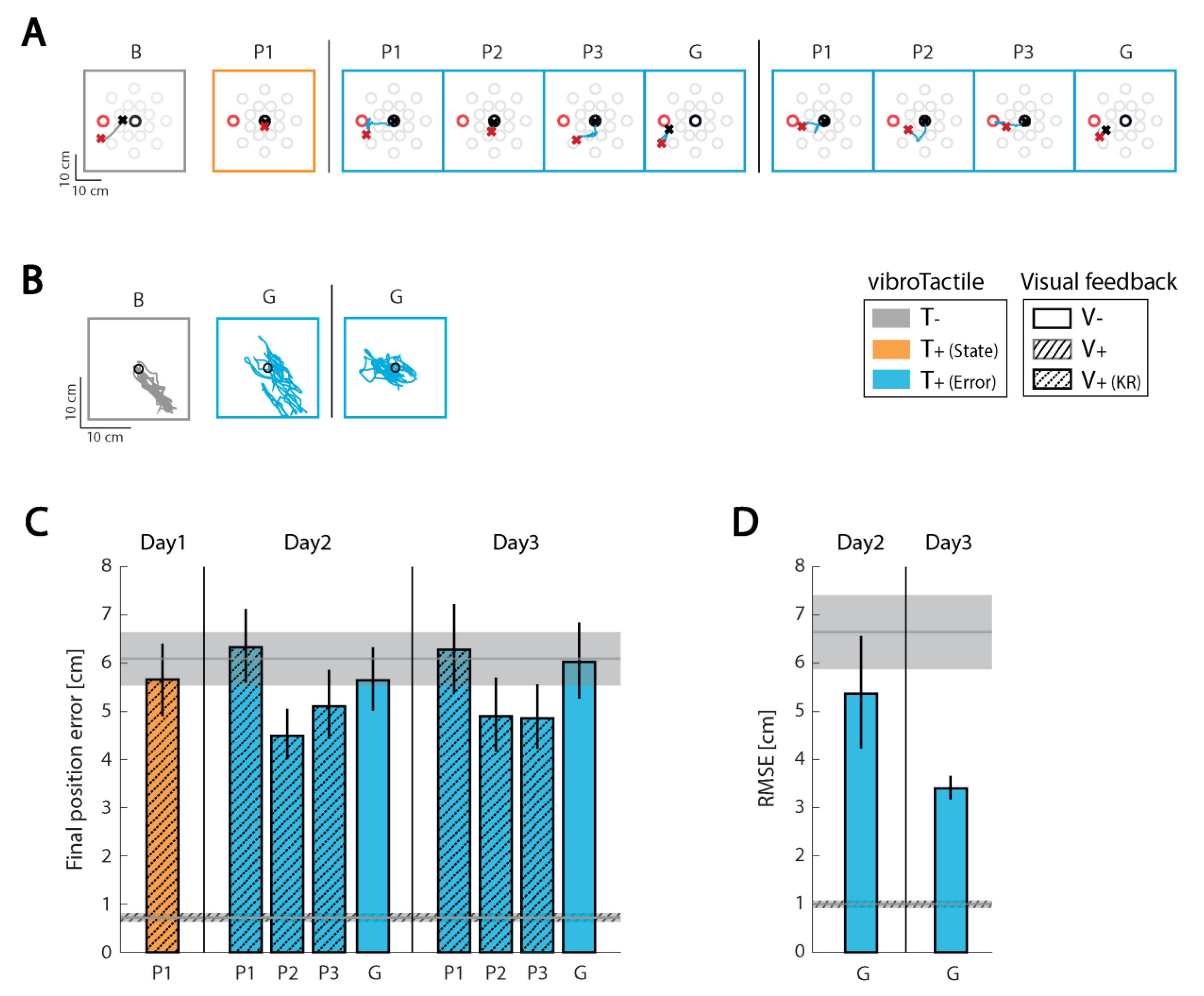
3.3.1. Subject 1 (S01)
3.3.2. Subject 2 (S02)
3.3.3. Subject 3 (S03)
4. Discussion
4.1. Human Performance Enhancement through Vibrotactile Cueing
4.2. Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Feigin, V.L.; Nichols, E.; Alam, T.; Bannick, M.S.; Beghi, E.; Blake, N.; Culpepper, W.J.; Dorsey, E.R.; Elbaz, A.; Ellenbogen, R.G.; et al. Global, regional, and national burden of neurological disorders, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 459–480. [Google Scholar] [CrossRef] [Green Version]
- Langhorne, P.; Coupar, F.; Pollock, A. Motor recovery after stroke: A systematic review. Lancet Neurol. 2009, 8, 741–754. [Google Scholar] [CrossRef]
- Veerbeek, J.M.; Langbroek-Amersfoort, A.C.; Van Wegen, E.E.H.; Meskers, C.G.; Kwakkel, G. Effects of robot-assisted therapy for the upper limb after stroke: A systematic review and meta-analysis. Neurorehabil. Neural Repair 2017, 31, 107–121. [Google Scholar] [CrossRef] [PubMed]
- Kessner, S.S.; Bingel, U.; Thomalla, G. Somatosensory deficits after stroke: A scoping review. Top. Stroke Rehabil. 2015, 23, 136–146. [Google Scholar] [CrossRef] [PubMed]
- Dukelow, S.P.; Herter, T.M.; Moore, K.D.; Demers, M.J.; Glasgow, J.I.; Bagg, S.D.; Norman, K.E.; Scott, S.H. Quantitative assessment of limb postion sense following stroke. Neurorehabil. Neural Repair 2010, 24, 178–187. [Google Scholar] [CrossRef]
- Semrau, J.A.; Herter, T.M.; Scott, S.H.; Dukelow, S.P. Examining Differences in Patterns of Sensory and Motor Recovery After Stroke with Robotics. Stroke 2015, 46, 3459–3469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sainburg, R.L.; Ghez, C.; Kalakanis, D. Intersegmental Dynamics Are Controlled by Sequential Anticipatory, Error Correction, and Postural Mechanisms. J. Neurophysiol. 1999, 81, 1045–1056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scheidt, R.A.; Ghez, C.; Moyer, J.T.; Wolf, J.A.; Finkel, L.H. Separate Adaptive Mechanisms for Controlling Trajectory and Final Position in Reaching. J. Neurophysiol. 2007, 98, 3600–3613. [Google Scholar] [CrossRef] [PubMed]
- Scheidt, R.A.; Stoeckmann, T. Reach adaptation and final position control amid environmental uncertainty following stroke. J. Neurophysiol. 2007, 97, 2824–2836. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abela, E.; Missimer, J.; Wiest, R.; Federspiel, A.; Hess, C.; Sturzenegger, M.; Weder, B. Lesions to Primary Sensory and Posterior Parietal Cortices Impair Recovery from Hand Paresis after Stroke. PLoS ONE 2012, 7, e31275. [Google Scholar] [CrossRef] [Green Version]
- Silva, R.M.; Sousa, E.; Fonseca, P.; Pinheiro, A.R.; Silva, C.; Correira, M.V.; Mouta, S. Analysis and quantification of upper-limb movement in motor rehabilitation after stroke BT. In Converging Clinical and Engineering Research on Neurorehabilitation II; Ibáñez, J., González-Vargas, J., Azorín, J.M., Akay, M., Pons, J., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 209–213. [Google Scholar]
- Coscia, M.; Wessel, M.J.; Chaudary, U.; Millán, J.D.R.; Micera, S.; Guggisberg, A.; Vuadens, P.; Donoghue, J.; Birbaumer, N.; Hummel, F.C. Neurotechnology-aided interventions for upper limb motor rehabilitation in severe chronic stroke. Brain 2019, 142, 2182–2197. [Google Scholar] [CrossRef] [Green Version]
- Gopaul, U.; Carey, L.; Callister, R.; Nilsson, M.; Van Vliet, P. Combined somatosensory and motor training to improve upper limb function following stroke: A systematic scoping review. Phys. Ther. Rev. 2018, 23, 355–375. [Google Scholar] [CrossRef]
- Aman, J.E.; Elangovan, N.; Yeh, I.-L.; Konczak, J. The effectiveness of proprioceptive training for improving motor function: A systematic review. Front. Hum. Neurosci. 2015, 8, 1075. [Google Scholar] [CrossRef] [Green Version]
- Cameron, B.D.; De La Malla, C.; López-Moliner, J. The role of differential delays in integrating transient visual and proprioceptive information. Front. Psychol. 2014, 5, 50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sainburg, R.L.; Poizner, H.; Ghez, C. Loss of proprioception produces deficits in interjoint coordination. J. Neurophysiol. 1993, 70, 2136–2147. [Google Scholar] [CrossRef] [Green Version]
- Ghez, C.; Gordon, J.; Ghilardi, M.F. Impairments of reaching movements in patients without proprioception. II. Effects of visual information on accuracy. J. Neurophysiol. 1995, 73, 361–372. [Google Scholar] [CrossRef]
- Sarlegna, F.R.; Gauthier, G.M.; Bourdin, C.; Vercher, J.-L.; Blouin, J. Internally driven control of reaching movements: A study on a proprioceptively deafferented subject. Brain Res. Bull. 2006, 69, 404–415. [Google Scholar] [CrossRef]
- Bark, K.; Khanna, P.; Irwin, R.; Kapur, P.; Jax, S.A.; Buxbaum, L.J.; Kuchenbecker, K.J. Lessons in using vibrotactile feedback to guide fast arm motions. In Proceedings of the IEEE World Haptics Conference, Istanbul, Turkey, 21–24 June 2011; pp. 355–360. [Google Scholar]
- Cuppone, A.V.; Squeri, V.; Semprini, M.; Masia, L.; Konczak, J. Robot-Assisted Proprioceptive Training with Added Vibro-Tactile Feedback Enhances Somatosensory and Motor Performance. PLoS ONE 2016, 11, e0164511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, V.A.; Risi, N.; Ballardini, G.; Mrotek, L.A.; Casadio, M.; Scheidt, R.A. Effect of Dual Tasking on Vibrotactile Feedback Guided Reaching—A Pilot Study. In Haptics: Science, Technology, and Applications, Proceedings of the 11th International Conference, EuroHaptics, Pisa, Italy, 13–16 June 2018; Springer International Publishing: Cham, Switzerland, 2018; Volume 10893, pp. 3–14. [Google Scholar]
- Risi, N.; Shah, V.; Mrotek, L.A.A.; Casadio, M.; Scheidt, R.A. Supplemental vibrotactile feedback of real-time limb position enhances precision of goal-directed reaching. J. Neurophysiol. 2019, 122, 22–38. [Google Scholar] [CrossRef] [PubMed]
- Guinan, A.L.; Hornbaker, N.C.; Montandon, M.N.; Doxon, A.J.; Provancher, W.R. Back-to-back skin stretch feedback for communicating five degree-of-freedom direction cues. In Proceedings of the IEEE World Haptics Conference, Daejeon, Korea, 14–17 April 2013; pp. 13–18. [Google Scholar]
- Norman, S.L.; Doxon, A.J.; Gleeson, B.T.; Provancher, W.R. Planar Hand Motion Guidance Using Fingertip Skin-Stretch Feedback. IEEE Trans. Haptics 2014, 7, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Battaglia, E.; Clark, J.P.; Bianchi, M.; Catalano, M.G.; Bicchi, A.; O’Malley, M.K. The Rice Haptic Rocker: Skin stretch haptic feedback with the Pisa/IIT SoftHand. In Proceedings of the IEEE World Haptics Conference, Munich, Germany, 5–9 June 2017; pp. 7–12. [Google Scholar]
- Schönauer, C.; Fukushi, K.; Olwal, A.; Kauffman, H.; Raskar, R. Multimodal motion guidance: Techniques for adaptive and dynamic feedback. In Proceedings of the 14th ACM International Conference on Multimodal Interactions, Santa Monica, CA, USA, 22–26 October 2012; pp. 133–140. [Google Scholar]
- Battaglia, E.; Bianchi, M.; Altobelli, A.; Grioli, G.; Catalano, M.G.; Serio, A.; Santello, M.; Bicchi, A. ThimbleSense: A Fingertip-Wearable Tactile Sensor for Grasp Analysis. IEEE Trans. Haptics 2015, 9, 121–133. [Google Scholar] [CrossRef]
- Chen, C.-Y.; Chen, Y.-Y.; Chung, Y.-J.; Yu, N.H. Motion guidance sleeve: Guiding the forearm rotation through external artificial muscles. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, San Jose, CA, USA, 7–12 May 2016; pp. 3272–3276. [Google Scholar]
- Adamovich, S.V.; Merians, A.S.; Boian, R.; Lewis, J.A.; Tremaine, M.; Burdea, G.S.; Reece, M.; Poizner, H. A virtual reality—based exercise system for hand rehabilitation post-stroke. Presence Teleoperators Virtual Environ. 2005, 14, 161–174. [Google Scholar] [CrossRef]
- Rosado, C.; Simone, L. Translational haptic feedback for post-stroke rehabilitation. In Proceedings of the IEEE 33rd Annual Northeast Bioengineering Conference, Stony Brook, NY, USA, 10–11 March 2007; pp. 259–260. [Google Scholar]
- Qiu, Q.; Fluet, G.G.; Saleh, S.; Lafond, I.; Merians, A.S.; Adamovich, S.V. Integrated versus isolated training of the hemiparetic upper extremity in haptically rendered virtual environments. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology, Buenos Aires, Argentina, 31 August–4 September 2010; Volume 2010, pp. 2255–2258. [Google Scholar]
- Conrad, M.O.; Scheidt, R.A.; Schmit, B.D. Effects of Wrist Tendon Vibration on Targeted Upper-Arm Movements in Poststroke Hemiparesis. Neurorehabilit. Neural Repair 2010, 25, 61–70. [Google Scholar] [CrossRef]
- Conrad, M.O.; Gadhoke, B.; Scheidt, R.A.; Schmit, B.D. Effect of Tendon Vibration on Hemiparetic Arm Stability in Unstable Workspaces. PLoS ONE 2015, 10, e0144377. [Google Scholar] [CrossRef] [PubMed]
- Hung, C.-T.; Croft, E.A.; Van Der Loos, H.F.M. A wearable vibrotactile device for upper-limb bilateral motion training in stroke rehabilitation: A case study. In Proceedings of the 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Seattle, WA, USA, 26–30 May 2015; pp. 3480–3483. [Google Scholar]
- Boian, R.; Deutsch, J.; Lee, C.S.; Burdea, G.; Lewis, J. Haptic effects for virtual reality-based post-stroke rehabilitation. In Proceedings of the 11th Symposium on Haptic Interfaces for Virtual Environment and Teleoperator Systems, 2003, HAPTICS 2003, Los Angeles, CA, USA, 22–23 March 2003; pp. 247–253. [Google Scholar]
- Afzal, M.R.; Byun, H.-Y.; Oh, M.-K.; Yoon, J. Effects of kinesthetic haptic feedback on standing stability of young healthy subjects and stroke patients. J. Neuroeng. Rehabil. 2015, 12, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaffe, D.L.; Brown, D.A.; Pierson-Carey, C.D.; Buckley, E.L.; Lew, H.L. Stepping over obstacles to improve walking in individuals with poststroke hemiplegia. J. Rehabil. Res. Dev. 2004, 41, 283–292. [Google Scholar] [CrossRef] [Green Version]
- Afzal, M.R.; Pyo, S.; Oh, M.-K.; Park, Y.S.; Yoon, J. Evaluating the effects of delivering integrated kinesthetic and tactile cues to individuals with unilateral hemiparetic stroke during overground walking. J. Neuroeng. Rehabil. 2018, 15, 33. [Google Scholar] [CrossRef] [PubMed]
- Afzal, M.R.; Lee, H.; Eizad, A.; Lee, C.H.; Oh, M.-K.; Yoon, J. Effects of Vibrotactile Biofeedback Coding Schemes on Gait Symmetry Training of Individuals with Stroke. IEEE Trans. Neural Syst. Rehabil. Eng. 2019, 27, 1617–1625. [Google Scholar] [CrossRef] [PubMed]
- Krueger, A.R.; Giannoni, P.; Shah, V.; Casadio, M.; Scheidt, R.A. Supplemental vibrotactile feedback control of stabilization and reaching actions of the arm using limb state and position error encodings. J. Neuroeng. Rehabil. 2017, 14, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Casadio, M.; Sanguineti, V.; Morasso, P.G.; Arrichiello, V. Braccio di Ferro: A new haptic workstation for neuromotor rehabilitation. Technol. Heal. Care 2006, 14, 123–142. [Google Scholar] [CrossRef]
- Simó, L.S.; Ghez, C.; Botzer, L.; Scheidt, R.A. A quantitative and standardized robotic method for the evaluation of arm proprioception after stroke. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011; pp. 8227–8230. [Google Scholar] [CrossRef] [Green Version]
- Fitts, P.M. The information capacity of the human motor system in controlling the amplitude of movement. J. Exp. Psychol. 1954, 47, 381–391. [Google Scholar] [CrossRef] [Green Version]
- Cipriani, C.; D’Alonzo, M.; Carrozza, M.C. A Miniature Vibrotactile Sensory Substitution Device for Multifingered Hand Prosthetics. IEEE Trans. Biomed. Eng. 2011, 59, 400–408. [Google Scholar] [CrossRef] [PubMed]
- Nolan, M.F. Two-Point Discrimination Assessment in the Upper Limb in Young Adult Men and Women. Phys. Ther. 1982, 62, 965–969. [Google Scholar] [CrossRef] [PubMed]
- Wann, J.P.; Ibrahim, S.F. Does limb proprioception drift? Exp. Brain Res. 1992, 91, 162–166. [Google Scholar] [CrossRef] [PubMed]
- Okamura, A.M. Haptic feedback in robot-assisted minimally invasive surgery. Curr. Opin. Urol. 2009, 19, 102–107. [Google Scholar] [CrossRef]
- Bark, K.; Mcmahan, W.; Remington, A.; Gewirtz, J.; Wedmid, A.; Lee, D.I.; Kuchenbecker, K.J. In vivo validation of a system for haptic feedback of tool vibrations in robotic surgery. Surg. Endosc. 2012, 27, 656–664. [Google Scholar] [CrossRef]
- Holden, M.K.; Todorov, E. Use of virtual environments in motor learning and rehabilitation. In Handbook of Virtual Environments: Design, Implementation, and Applications; CRC Press: Boca Raton, FL, USA, 2002; pp. 999–1026. [Google Scholar]
- Bark, K.; Hyman, E.; Tan, F.; Cha, E.; Jax, S.A.; Buxbaum, L.J.; Kuchenbecker, K.J. Effects of Vibrotactile Feedback on Human Learning of Arm Motions. IEEE Trans. Neural Syst. Rehabil. Eng. 2015, 23, 51–63. [Google Scholar] [CrossRef] [Green Version]
- Tzorakoleftherakis, E.; Bengtson, M.C.; Mussa-Ivaldi, F.A.; Scheidt, R.A.; Murphey, T.D. Tactile proprioceptive input in robotic rehabilitation after stroke. In Proceedings of the IEEE International Conference on Robotics and Automation, Seattle, WA, USA, 26–30 May 2015; pp. 6475–6481. [Google Scholar]
- Collins, J.J.; Chow, C.C.; Imhoff, T.T. Stochastic resonance without tuning. Nature 1995, 376, 236–238. [Google Scholar] [CrossRef] [PubMed]
- Conrad, M.O.; Scheidt, R.A.; Schmit, B.D. Effects of wrist tendon vibration on arm tracking in people poststroke. J. Neurophysiol. 2011, 106, 1480–1488. [Google Scholar] [CrossRef] [Green Version]
- Wolf, F.; Kuber, R. Developing a head-mounted tactile prototype to support situational awareness. Int. J. Human-Computer Stud. 2018, 109, 54–67. [Google Scholar] [CrossRef]
- Lee, B.-C.; Martin, B.J.; Sienko, K.H. Directional postural responses induced by vibrotactile stimulations applied to the torso. Exp. Brain Res. 2012, 222, 471–482. [Google Scholar] [CrossRef]
- Van Der Linden, J.; Johnson, R.; Bird, J.; Rogers, Y.; Schoonderwaldt, E. Buzzing to play: Lessons learned from an in the wild study of real-time vibrotactile feedback. In Proceedings of the Conference on Human Factors in Computing Systems, Vancouver, BC, Canada, 7–12 May 2011; pp. 533–542. [Google Scholar]
- Lieberman, J.; Breazeal, C. TIKL: Development of a Wearable Vibrotactile Feedback Suit for Improved Human Motor Learning. IEEE Trans. Robot. 2007, 23, 919–926. [Google Scholar] [CrossRef]
- Shull, P.B.; Damian, D.D. Haptic wearables as sensory replacement, sensory augmentation and trainer—A review. J. Neuroeng. Rehabil. 2015, 12, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Sienko, K.H.; Seidler, R.D.; Carender, W.J.; Goodworth, A.D.; Whitney, S.L.; Peterka, R.J. Potential Mechanisms of Sensory Augmentation Systems on Human Balance Control. Front. Neurol. 2018, 9. [Google Scholar] [CrossRef] [PubMed]
- Proske, U.; Gandevia, S.C. The proprioceptive senses: Their role in signaling body shape, body position and movement, and muscle force. Physiol. Rev. 2012, 92, 1651–1697. [Google Scholar] [CrossRef] [PubMed]
- Flanders, M.; Tillery, S.I.H.; Soechting, J.F. Early stages in a sensorimotor transformation. Behav. Brain Sci. 1992, 15, 309–320. [Google Scholar] [CrossRef]
- Piovesan, D.; Casadio, M.; Mussa-Ivaldi, F.A.; Morasso, P.G. Multijoint arm stiffness during movements following stroke: Implications for robot therapy. In Proceedings of the IEEE International Conference on Rehabilitation Robotics, Zurich, Switzerland, 29 June–1 July 2011; pp. 1–7. [Google Scholar]
- Mosier, E.M.; Herda, T.J.; Trevino, M.A.; Miller, J.D. The influence of prolonged vibration on motor unit behavior. Muscle Nerve 2017, 55, 500–507. [Google Scholar] [CrossRef]
- Liu, H.; Zhang, Z.; Xie, X.; Zhu, Y.; Liu, Y.; Wang, Y.; Zhu, S.-C. High-Fidelity Grasping in Virtual Reality using a Glove-based System. In Proceedings of the International Conference on Robotics and Automation (ICRA), Montreal, QC, Canada, 20–24 May 2019; pp. 5180–5186. [Google Scholar]
- Gordon, J.; Ghilardi, M.F.; Ghez, C. Impairments of reaching movements in patients without proprioception. I. Spatial errors. J. Neurophysiol. 1995, 73, 347–360. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Sainburg, R.L. Interlimb transfer of visuomotor rotations depends on handedness. Exp. Brain Res. 2006, 175, 223–230. [Google Scholar] [CrossRef]
- Brooke, J. SUS: A “quick and dirty’ usability scale. In Usability Evaluation in Industry; Jordan, P.W., Thomas, B., McLelland, I., Weerdmeester, B.A., Eds.; Taylor and Francis: London, UK, 1996; p. 189. [Google Scholar]
- Demers, L.; Monette, M.; Lapierre, Y.; Arnold, D.L.; Wolfson, C. Reliability, validity, and applicability of the Quebec User Evaluation of Satisfaction with assistive Technology (QUEST 2.0) for adults with multiple sclerosis. Disabil. Rehabil. 2002, 24, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Fitts, P.M.; Posner, M.I. Human Performance; Praeger: Goleta, CA, USA, 1967. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject | Gender | Age (ys) | Type | PS | TSS (ys) | Lesion Location |
|---|---|---|---|---|---|---|
| S01 | F | 68 | I | R | 12.5 | Left basal ganglia, internal capsule, occipital lobe |
| S02 | M | 57 | I | L | 1 | Right basal ganglia, temporal lobe, insula |
| S03 | F | 65 | H | L | 16 | Right occipital lobe |
| Subject | FMA-UE | MAS | CAHAI | NSA | Tuning Fork Test | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| A–D | H | Sh | El | Fa | Wr | Fg | Th | P | S | Contra | Ipsi | ||||
| (0–66) | (0–12) | (0–4) | (0–4) | (0–4) | (0–4) | (0–4) | (0–4) | (0–91) | (0–3) | (0–2) | El | Wr | El | Wr | |
| S01 | 57 | 11 | 1 | 0 | 0 | 0 | 0 | 1 | 80 | 3 | 2 | 6 | 6 | 6 | 6 |
| S02 | 6 | 7 | 1+ | 1+ | 2 | 3 | 3 | 3 | 13 | 0 | 0 | 6 | 5.5 | 7 | 7.5 |
| S03 | 42 | 7 | 1 | 1 | 1 | 2 | 1 | 1 | 24 | 1 | 0 | 5 | 6 | 6 | 6 |
| Subject | Day: Encoding | Familiarization V+T− | Practice VKRT+ | Baseline V−T− | Test V−T+ | ||
|---|---|---|---|---|---|---|---|
| S01 | Day 1: State | R + S | R | R | R + S | R + S | |
| Day 2: Error | R | R | R + S | R + S | |||
| S02 | Day 1: State | R + S | R | R | R | R + S | R + S |
| Day 2: Error | R | R | R | R + S | |||
| S03 | Day 1: State | R + S | R | R + S | |||
| Day 2: Error | R | R | R | R + S | |||
| Day 3: Error | R | R | R | R + S | R + S | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ballardini, G.; Krueger, A.; Giannoni, P.; Marinelli, L.; Casadio, M.; Scheidt, R.A. Effect of Short-Term Exposure to Supplemental Vibrotactile Kinesthetic Feedback on Goal-Directed Movements after Stroke: A Proof of Concept Case Series. Sensors 2021, 21, 1519. https://doi.org/10.3390/s21041519
Ballardini G, Krueger A, Giannoni P, Marinelli L, Casadio M, Scheidt RA. Effect of Short-Term Exposure to Supplemental Vibrotactile Kinesthetic Feedback on Goal-Directed Movements after Stroke: A Proof of Concept Case Series. Sensors. 2021; 21(4):1519. https://doi.org/10.3390/s21041519
Chicago/Turabian StyleBallardini, Giulia, Alexis Krueger, Psiche Giannoni, Lucio Marinelli, Maura Casadio, and Robert A. Scheidt. 2021. "Effect of Short-Term Exposure to Supplemental Vibrotactile Kinesthetic Feedback on Goal-Directed Movements after Stroke: A Proof of Concept Case Series" Sensors 21, no. 4: 1519. https://doi.org/10.3390/s21041519
APA StyleBallardini, G., Krueger, A., Giannoni, P., Marinelli, L., Casadio, M., & Scheidt, R. A. (2021). Effect of Short-Term Exposure to Supplemental Vibrotactile Kinesthetic Feedback on Goal-Directed Movements after Stroke: A Proof of Concept Case Series. Sensors, 21(4), 1519. https://doi.org/10.3390/s21041519