
Early Detection of Freezing of Gait during Walking Using Inertial Measurement Unit and Plantar Pressure Distribution Data



Abstract
:1. Introduction
2. Materials and Methods
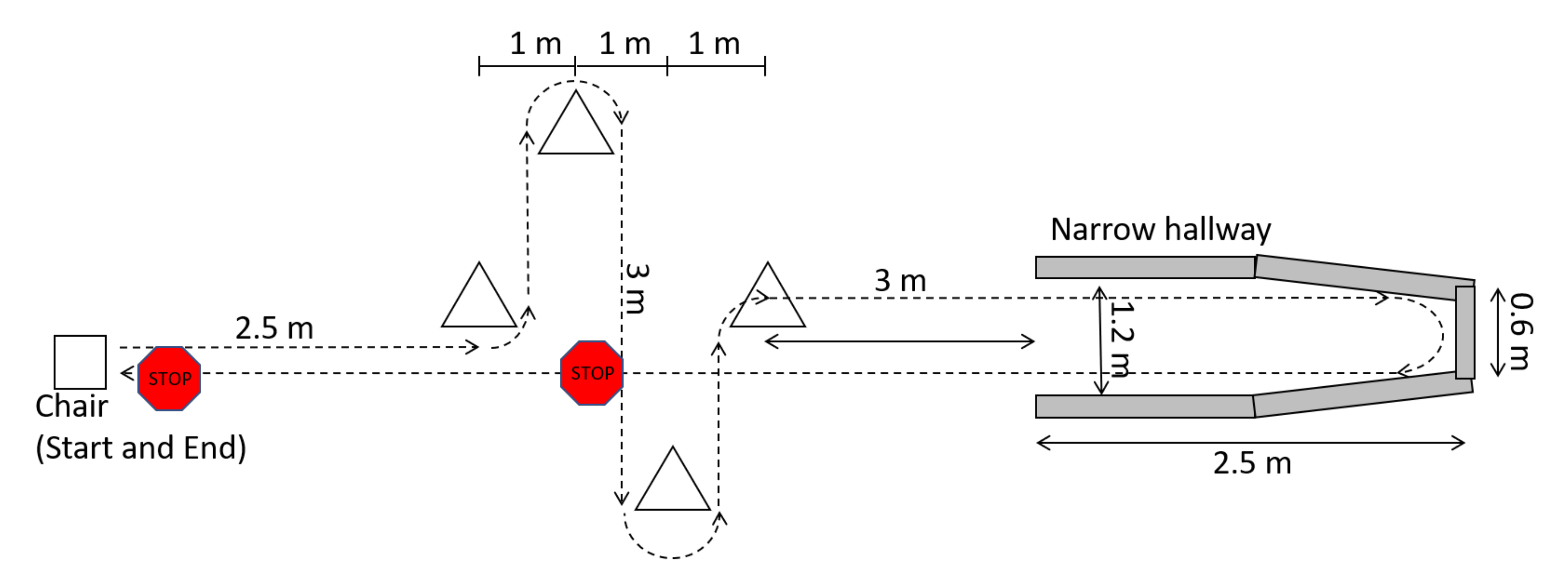
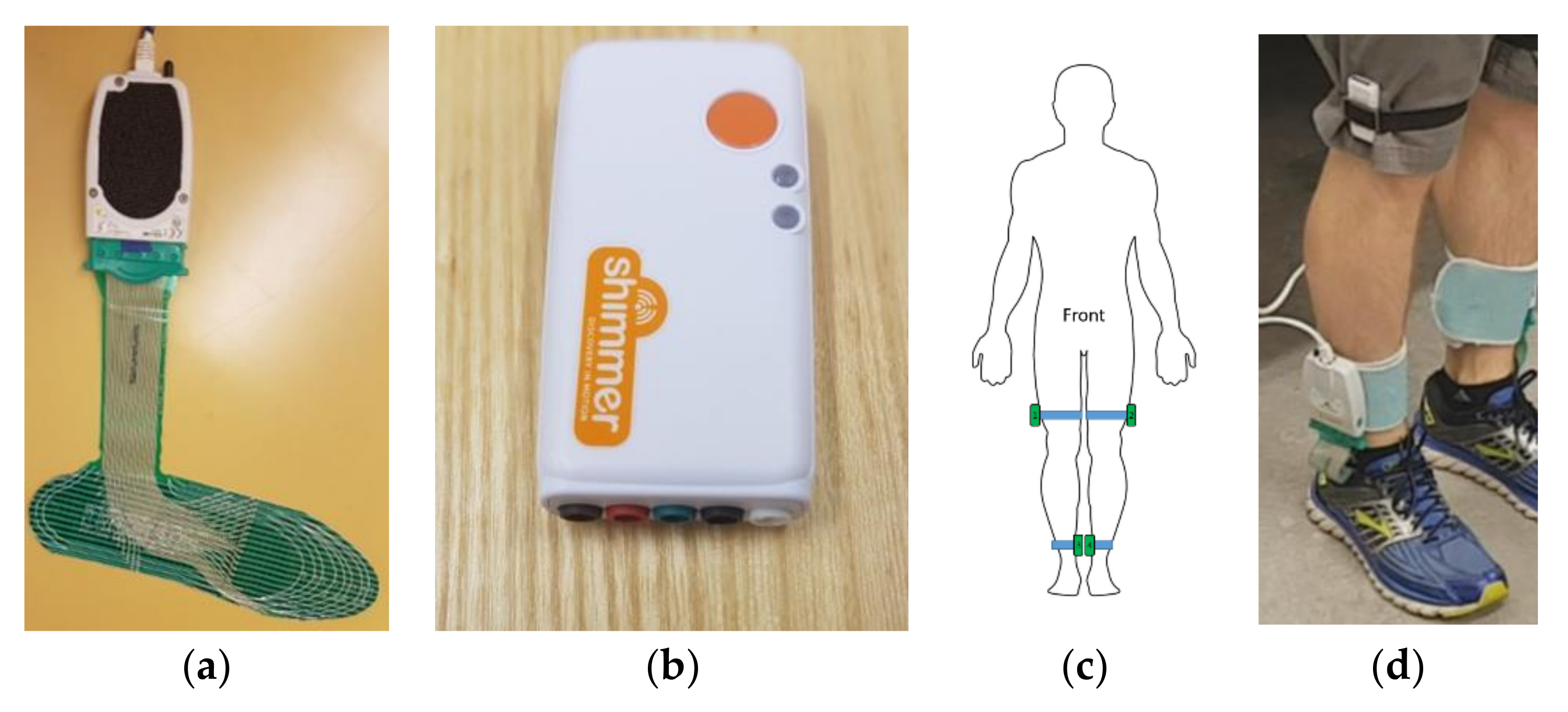
2.1. Data Collection
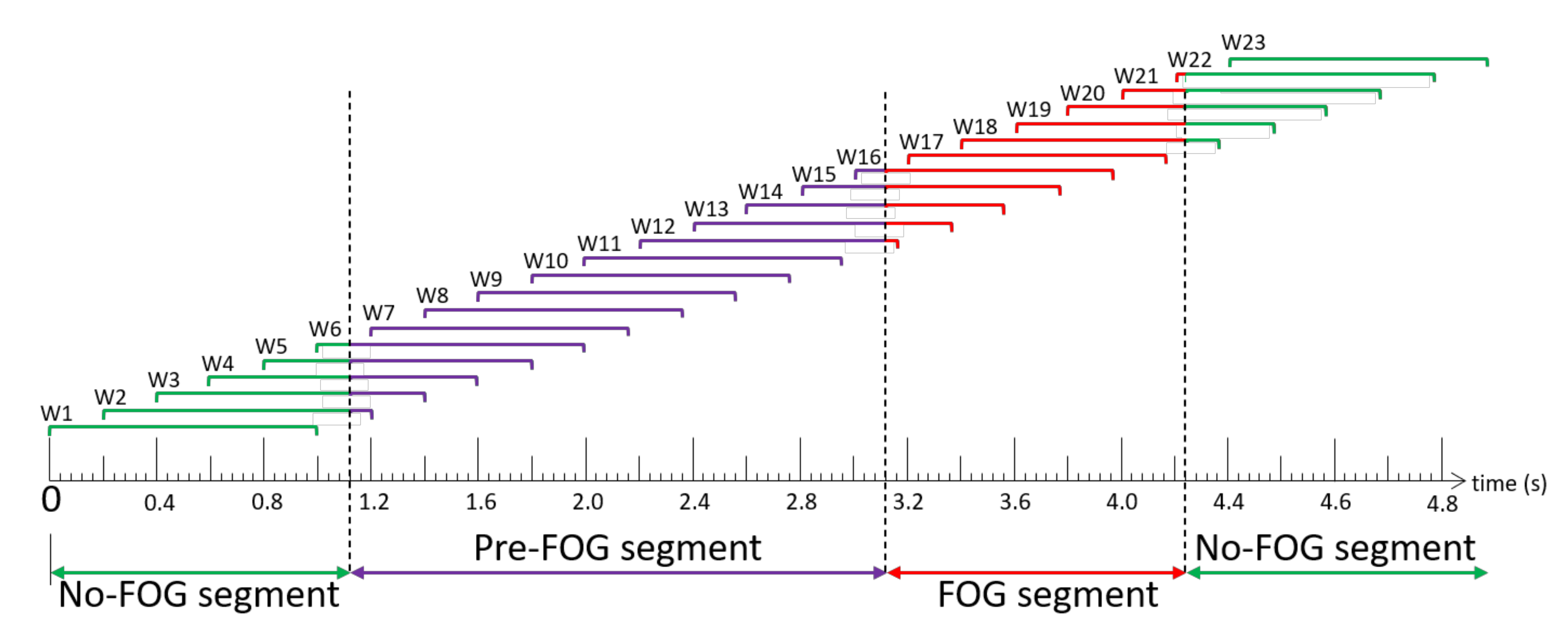
2.2. Labelling and Windowing
2.3. Feature Extraction
2.4. Feature Selection
2.5. Ensemble Model Development
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nutt, J.G.; Bloem, B.R.; Giladi, N.; Hallett, M.; Horak, F.B.; Nieuwboer, A. Freezing of gait: Moving forward on a mysterious clinical phenomenon. Lancet Neurol. 2011, 10, 734–744. [Google Scholar] [CrossRef]
- Okuma, Y.; Silva de Lima, A.L.; Fukae, J.; Bloem, B.R.; Snijders, A.H. A prospective study of falls in relation to freezing of gait and response fluctuations in Parkinson’s disease. Park. Relat. Disord. 2018, 46, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Bloem, B.R.; Hausdorff, J.M.; Visser, J.E.; Giladi, N. Falls and freezing of gait in Parkinson’s disease: A review of two interconnected, episodic phenomena. Mov. Disord. 2004, 19, 871–884. [Google Scholar] [CrossRef]
- Ginis, P.; Nackaerts, E.; Nieuwboer, A.; Heremans, E. Cueing for people with Parkinson’s disease with freezing of gait: A narrative review of the state-of-the-art and novel perspectives. Ann. Phys. Rehabil. Med. 2018, 61, 407–413. [Google Scholar] [CrossRef]
- Nieuwboer, A. Cueing for freezing of gait in patients with Parkinson’s disease: A rehabilitation perspective. Mov. Disord. 2008, 23, S475–S481. [Google Scholar] [CrossRef] [PubMed]
- Pardoel, S.; Kofman, J.; Nantel, J.; Lemaire, E.D. Wearable-sensor-based detection and prediction of freezing of gait in Parkinson’s disease: A review. Sensors 2019, 19, 5141. [Google Scholar] [CrossRef] [Green Version]
- Nieuwboer, A.; Dom, R.; De Weerdt, W.; Desloovere, K.; Janssens, L.; Stijn, V. Electromyographic profiles of gait prior to onset of freezing episodes in patients with Parkinson’s disease. Brain 2004, 127, 1650–1660. [Google Scholar] [CrossRef] [PubMed]
- Ferster, M.L.; Mazilu, S.; Tröster, G. Gait Parameters Change Prior to Freezing in Parkinson’s Disease: A Data-Driven Study with Wearable Inertial Units. In Proceedings of the 10th EAI International Conference on Body Area Networks, Sydney, Australia, 28–30 September 2015; pp. 159–166. [Google Scholar] [CrossRef] [Green Version]
- Mazilu, S.; Blanke, U.; Calatroni, A.; Gazit, E.; Hausdorff, J.M.; Tröster, G. The role of wrist-mounted inertial sensors in detecting gait freeze episodes in Parkinson’s disease. Pervasive Mob. Comput. 2016, 33, 1–16. [Google Scholar] [CrossRef]
- Handojoseno, A.M.A.; Shine, J.M.; Nguyen, T.N.; Tran, Y.; Lewis, S.J.G.; Nguyen, H.T. Analysis and prediction of the freezing of gait using EEG brain dynamics. IEEE Trans. Neural Syst. Rehabil. Eng. 2015, 23, 887–896. [Google Scholar] [CrossRef]
- Torvi, V.G.; Bhattacharya, A.; Chakraborty, S. Deep Domain Adaptation to Predict Freezing of Gait in Patients with Parkinson’s Disease. In Proceedings of the 17th IEEE International Conference on Machine Learning and Applications (ICMLA), Orlando, FL, USA, 17–20 December 2018; pp. 1001–1006. [Google Scholar] [CrossRef]
- Mazilu, S.; Calatroni, A.; Gazit, E.; Roggen, D.; Hausdorff, J.M.; Tröster, G. Feature Learning for Detection and Prediction of Freezing of Gait in Parkinson’s Disease. In Machine Learning and Data Mining in Pattern Recognition; Perner, P., Ed.; Springer: Berlin/Heidelberg, Germany, 2013; Volume 7988, pp. 144–158. ISBN 978-3-642-39712-7. [Google Scholar]
- Arami, A.; Poulakakis-Daktylidis, A.; Tai, Y.F.; Burdet, E. Prediction of gait freezing in Parkinsonian patients: A binary classification augmented with time series prediction. IEEE Trans. Neural Syst. Rehabil. Eng. 2019, 27, 1909–1919. [Google Scholar] [CrossRef] [PubMed]
- Naghavi, N.; Wade, E. Prediction of freezing of gait in Parkinson’s disease using statistical inference and lower-limb acceleration data. IEEE Trans. Neural Syst. Rehabil. Eng. 2019, 27, 947–955. [Google Scholar] [CrossRef] [PubMed]
- Bachlin, M.; Plotnik, M.; Roggen, D.; Maidan, I.; Hausdorff, J.M.; Giladi, N.; Troster, G. Wearable assistant for Parkinson’s disease patients with the freezing of gait symptom. Trans. Inf. Technol. Biomed. 2010, 14, 436–446. [Google Scholar] [CrossRef] [PubMed]
- Nantel, J.; Bronte-Stewart, H. The effect of medication and the role of postural instability in different components of freezing of gait (FOG). Park. Relat. Disord. 2014, 20, 447–451. [Google Scholar] [CrossRef] [PubMed]
- Lees, A.J. The on-off phenomenon. J. Neurol. Neurosurg. Psychiatry 1989, 52, 29–37. [Google Scholar] [CrossRef] [Green Version]
- Suppa, A.; Kita, A.; Leodori, G.; Zampogna, A.; Nicolini, E.; Lorenzi, P.; Rao, R.; Irrera, F. L-DOPA and freezing of gait in Parkinson’s disease: Objective assessment through a wearable wireless system. Front. Neurol. 2017, 8, 406. [Google Scholar] [CrossRef]
- Naghavi, N.; Miller, A.; Wade, E. Towards real-time prediction of freezing of gait in patients with Parkinson’s disease: Addressing the class imbalance problem. Sensors 2019, 19, 3898. [Google Scholar] [CrossRef] [Green Version]
- Silva de Lima, A.L.; Evers, L.J.W.; Hahn, T.; Bataille, L.; Hamilton, J.L.; Little, M.A.; Okuma, Y.; Bloem, B.R.; Faber, M.J. Freezing of gait and fall detection in Parkinson’s disease using wearable sensors: A systematic review. J. Neurol. 2017, 264, 1642–1654. [Google Scholar] [CrossRef] [Green Version]
- Palmerini, L.; Rocchi, L.; Mazilu, S.; Gazit, E.; Hausdorff, J.M.; Chiari, L. Identification of characteristic motor patterns preceding freezing of gait in Parkinson’s disease using wearable sensors. Front. Neurol. 2017, 8, 394. [Google Scholar] [CrossRef] [Green Version]
- Rahimi, F.; Xian, S.Y.; Delrobaei, M.; Jog, M. Characteristics of Gait Freezing: Possibilities for Rehabilitation. In Proceedings of the International IEEE/EMBS Conference on Neural Engineering, San Diego, USA, CA, 6–8 November 2013; pp. 1594–1597. [Google Scholar] [CrossRef]
- Popovic, M.B.; Djuric-Jovicic, M.; Radovanovic, S.; Petrovic, I.; Kostic, V. A simple method to assess freezing of gait in Parkinson’s disease patients. Braz. J. Med. Biol. Res. 2010, 43, 883–889. [Google Scholar] [CrossRef] [Green Version]
- Nantel, J.; de Solages, C.; Bronte-Stewart, H. Repetitive stepping in place identifies and measures freezing episodes in subjects with Parkinson’s disease. Gait Posture 2011, 34, 329–333. [Google Scholar] [CrossRef]
- Plotnik, M.; Giladi, N.; Hausdorff, J.M. Bilateral coordination of walking and freezing of gait in Parkinson’s disease. Eur. J. Neurosci. 2008, 27, 1999–2006. [Google Scholar] [CrossRef]
- Shah, J.; Pillai, L.; Williams, D.K.; Doerhoff, S.M.; Larson-Prior, L.; Garcia-Rill, E.; Virmani, T. Increased foot strike variability in Parkinson’s disease patients with freezing of gait. Park. Relat. Disord. 2018, 53, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Maculewicz, J.; Kofoed, L.B.; Serafin, S. A technological review of the instrumented footwear for rehabilitation with a focus on Parkinson’s disease patients. Front. Neurol. 2016, 7, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neaga, F.; Moga, D.; Petreus, D.; Munteanu, M.; Stroia, N. A Wireless System for Monitoring the Progressive Loading of Lower Limb in Post-Traumatic Rehabilitation. In Proceedings of the International Conference on Advancements of Medicine and Health Care through Technology, Cluj-Napoca, Romania, 29 August–2 September 2011; Springer: Berlin/Heidelberg, Germany, 2011; Volume 36, pp. 54–59. [Google Scholar] [CrossRef]
- Edgar, S.R.; Swyka, T.; Fulk, G.; Sazonov, E.S. Wearable Shoe-Based Device for Rehabilitation of Stroke Patients. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Buenos Aires, Argentina, 31 August–3 September 2010; pp. 3772–3775. [Google Scholar] [CrossRef]
- Howcroft, J.; Kofman, J.; Lemaire, E.D. Prospective fall-risk prediction models for older adults based on wearable sensors. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 25, 1812–1820. [Google Scholar] [CrossRef]
- Howcroft, J.; Lemaire, E.D.; Kofman, J. Wearable-sensor-based classification models of faller status in older adults. PLoS ONE 2016, 11, e153240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeon, H.S.; Han, J.; Yi, W.J.; Jeon, B.; Park, K.S. Classification of Parkinson Gait and Normal Gait using Spatial-Temporal Image of Plantar Pressure. In Proceedings of the 30th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Vancouver, BC, Canada, 20–25 August 2008; pp. 4672–4675. [Google Scholar] [CrossRef]
- Shalin, G.; Pardoel, S.; Nantel, J.; Lemaire, E.D.; Kofman, J. Prediction of Freezing of Gait in Parkinson’s Disease from Foot Plantar-Pressure Arrays using a Convolutional Neural Network. In Proceedings of the 42nd Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Montreal, QC, Canada, 20–24 July 2020; pp. 244–247. [Google Scholar] [CrossRef]
- Pardoel, S.; Shalin, G.; Nantel, J.; Lemaire, E.D.; Kofman, J. Selection of Plantar-Pressure and Ankle-Acceleration Features for Freezing of Gait Detection in Parkinson’s Disease using Minimum-Redundancy Maximum-Relevance. In Proceedings of the 42nd Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Montreal, QC, Canada, 20–24 July 2020; pp. 4034–4037. [Google Scholar] [CrossRef]
- Reches, T.; Dagan, M.; Herman, T.; Gazit, E.; Gouskova, N.A.; Giladi, N.; Manor, B.; Hausdorff, J.M. Using wearable sensors and machine learning to automatically detect freezing of gait during a FOG-provoking test. Sensors 2020, 20, 4474. [Google Scholar] [CrossRef]
- Howcroft, J.; Kofman, J.; Lemaire, E.D. Feature selection for elderly faller classification based on wearable sensors. J. Neuroeng. Rehabil. 2017, 14, 11. [Google Scholar] [CrossRef]
- Bächlin, M.; Roggen, D.; Plotnik, M.; Hausdorff, J.M.; Giladi, N.; Tröster, G. Online Detection of Freezing of Gait in Parkinson’s Disease Patients: A Performance Characterization. In Proceedings of the 4th International ICST Conference on Body Area Networks, Los Angeles, CA, USA, 1–3 April 2009. [Google Scholar] [CrossRef] [Green Version]
- Ahlrichs, C.; Samà, A.; Lawo, M.; Cabestany, J.; Rodríguez-Martín, D.; Pérez-López, C.; Sweeney, D.; Quinlan, L.R.; Laighin, G.Ò.; Counihan, T.; et al. Detecting freezing of gait with a tri-axial accelerometer in Parkinson’s disease patients. Med. Biol. Eng. Comput. 2016, 54, 223–233. [Google Scholar] [CrossRef] [Green Version]
- Moore, S.T.; MacDougall, H.G.; Ondo, W.G. Ambulatory monitoring of freezing of gait in Parkinson’s disease. J. Neurosci. Methods 2008, 167, 340–348. [Google Scholar] [CrossRef] [PubMed]
- El-Attar, A.; Ashour, A.S.; Dey, N.; Abdelkader, H.; Abd El-Naby, M.M.; Sherratt, S.R. Discrete wavelet transform-based freezing of gait detection in Parkinson’s disease. J. Exp. Theor. Artif. Intell. 2018, 1–17. [Google Scholar] [CrossRef]
- Vergara, J.R.; Estévez, P.A. A review of feature selection methods based on mutual information. Neural Comput. Appl. 2014, 24, 175–186. [Google Scholar] [CrossRef]
- Urbanowicz, R.J.; Meeker, M.; Lacava, W.; Olson, R.S.; Jason, H. Relief-based feature selection: Introduction and review. J. Biomed. Inform. 2018, 85, 189–203. [Google Scholar] [CrossRef]
- Tripoliti, E.E.; Tzallas, A.T.; Tsipouras, M.G.; Rigas, G.; Bougia, P.; Leontiou, M.; Konitsiotis, S.; Chondrogiorgi, M.; Tsouli, S.; Fotiadis, D.I. Automatic detection of freezing of gait events in patients with Parkinson’s disease. Comput. Methods Programs Biomed. 2013, 110, 12–26. [Google Scholar] [CrossRef] [PubMed]
- Handojoseno, A.M.A.; Naik, G.R.; Gilat, M.; Shine, J.M.; Nguyen, T.N.; Quynh, T.L.; Lewis, S.J.G.; Nguyen, H.T. Prediction of freezing of gait in patients with Parkinson’s disease using EEG signals. Stud. Health Technol. Inform. 2017, 246, 124–131. [Google Scholar] [CrossRef]
- Borzì, L.; Mazzetta, I.; Zampogna, A.; Suppa, A.; Olmo, G.; Irrera, F. Prediction of freezing of gait in Parkinson’s disease using wearables and machine learning. Sensors 2021, 21, 614. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Feature | Feature Description | Source | Number of Input Parameters | Total Features |
|---|---|---|---|---|
| Time domain features (n = 13) | ||||
| Number, duration, length of COP reversals | Number, length, duration of centre of pressure (COP) path direction reversals per window (n = 3) | [36] | 2 | 6 |
| Number, duration, length of COP deviations | Number, length, duration of mediolateral COP deviations per window. Deviation is the first derivative of COP ML exceeding a threshold of ±0.5 mm/window (n = 3) | [36] | 2 | 6 |
| CV of COP position, velocity, acceleration | Anterior/posterior (AP) and medial/lateral (ML) coefficients of variation (CV) of COP position, velocity, and acceleration (n = 6) | [36] | 2 | 12 |
| Number of weight shifts | Number of times the majority of total GRF (>50%) changed foot (n = 1) | - | 1 | 1 |
| Category total | 25 | |||
| Fast Fourier transform (FFT) features (n = 8) | ||||
| Total power in FFT signal | Power in FFT signal per window as sum of squared amplitude (n = 1) | [37] | 38 | 38 |
| Dominant frequency | Frequency bin with highest amplitude per window (n = 1) | [38] | 38 | 38 |
| Max, min, mean | Maximum, minimum, and mean amplitude of FFT signal (n = 3) | [38] | 38 | 114 |
| Power in locomotion, freeze bands | Power under FFT curve in locomotion band (0.5–3 Hz) and freeze band (3–8 Hz) (n = 2) | [39] | 38 | 76 |
| Freeze index | Ratio of power in freeze band (3–8 Hz) and locomotion band (0.5–3 Hz) (n = 1) | [39] | 38 | 38 |
| Category total | 304 | |||
| Discrete wavelet transform features (n = 14), Haar mother wavelet | ||||
| Variance of coefficients | Variance of the detail and approximation coefficient vectors (n = 2) | [40] | 38 | 76 |
| Max, min, mean | Maximum, minimum, mean of detail and approximation coefficient vectors (n = 6) | [40] | 38 | 228 |
| Max, min, mean energy | Maximum, minimum, mean energy of detail and approximation coefficient vectors (n = 6) | [40] | 38 | 228 |
| Category total | 532 | |||
| Target Class | Nontarget Class | |
|---|---|---|
| Case 1 | Total-FOG: Pre-FOG, Pre-FOG-Transition, FOG | No-FOG |
| Case 2 | Pre-FOG | No-FOG |
| Case 3 | Pre-FOG, Pre-FOG-Transition | No-FOG |
| Case 4 | Pre-FOG-Transition | No-FOG |
| Case 5 | FOG | No-FOG |
| Participant | Years Since Diagnosis | NFOG-Q | UPDRS III | Window Labels | |||
|---|---|---|---|---|---|---|---|
| Pre-FOG | Pre-FOG-Transition | FOG | No-FOG | ||||
| P01 | 16 | 14 | 10 | 217 | 166 | 7 | 3721 |
| P02 | 11 | 21 | 20 | 178 | 171 | 294 | 5188 |
| P03 | 11 | 17 | 13 | 66 | 62 | 17 | 6884 |
| P04 | 10 | 4 | 18 | 0 | 0 | 0 | 2635 |
| P05 | 14 | 20 | 13 | 0 | 0 | 0 | 5331 |
| P06 | 19 | 22 | 29 | 52 | 49 | 162 | 9368 |
| P07 | 5 | 15 | 16 | 725 | 1303 | 766 | 6572 |
| P08 | 12 | 17 | 20 | 75 | 126 | 84 | 4848 |
| P09 | 10 | 18 | 18 | 44 | 30 | 5 | 6848 |
| P10 | 2 | 4 | 15 | 0 | 0 | 0 | 6034 |
| P11 | 5 | 19 | 20 | 0 | 0 | 0 | 9039 |
| Mean (SD) | 10.5 (4.8) | 15.5 (5.9) | 17.5 (4.8) | ||||
| Label total | 1357 | 1907 | 1335 | 66,468 | |||
| Plantar Pressure Features | IMU Features | PP-IMU Features | ||||
|---|---|---|---|---|---|---|
| Relief-F, 5 Features, 5 Splits | mRMR, 25 Features, 5 Splits | Relief-F, 10 Features, 5 Splits | ||||
| Held out Participant | Sens (%) | Spec (%) | Sens (%) | Spec (%) | Sens (%) | Spec (%) |
| P01 | 69.7 | 83.7 | 68.2 | 84.0 | 70.0 | 86.0 |
| P02 | 71.7 | 86.7 | 67.0 | 90.7 | 70.6 | 87.9 |
| P03 | 68.3 | 89.7 | 54.5 | 96.1 | 61.4 | 92.9 |
| P04 | - | 85.4 | - | 91.9 | - | 86.5 |
| P05 | - | 81.3 | - | 88.1 | - | 84.6 |
| P06 | 93.9 | 89.5 | 73.4 | 93.5 | 93.2 | 90.2 |
| P07 | 72.8 | 80.3 | 34.8 | 92.1 | 68.7 | 78.9 |
| P08 | 89.5 | 79.6 | 70.9 | 92.3 | 82.1 | 87.6 |
| P09 | 79.7 | 72.5 | 64.6 | 92.2 | 88.6 | 79.7 |
| P10 | - | 87.7 | - | 90.2 | - | 89.2 |
| P11 | - | 79.4 | - | 88.3 | - | 79.2 |
| Mean (SD) | 78.0 (9.4) | 83.2 (5.7) | 61.9 (12.4) | 91.6 (3.4) | 76.4 (10.8) | 86.2 (4.8) |
| Feature Rank | Feature Description |
|---|---|
| 1 | Dominant frequency of COP velocity in Y (AP) direction for right leg |
| 2 | Dominant frequency of COP velocity in Y (AP) direction for left leg |
| 3 | Dominant frequency of COP velocity in X (ML) direction for right leg |
| 4 | Dominant frequency of thigh acceleration in X (AP) direction for left leg |
| 5 | Number of AP COP path reversals for left leg |
| 6 | Number of AP COP path reversals for right leg |
| 7 | Minimum WT dC of COP position in Y (AP) direction for right leg |
| 8 | Dominant frequency of thigh acceleration in X (AP) direction for right leg |
| 9 | Mean energy of WT aC of COP position in Y (AP) direction for right leg |
| 10 | Mean WT aC of COP position in Y (AP) direction for right leg |
| Pre-FOG (Case 2) | Pre-FOG and Pre-FOG-Transition (Case 3) | Pre-FOG-Transition (Case 4) | FOG (Case 5) | |||||
|---|---|---|---|---|---|---|---|---|
| Held out Test Participant | Sens (%) | Spec (%) | Sens (%) | Spec (%) | Sens (%) | Spec (%) | Sens (%) | Spec (%) |
| P01 | 52.5 | 86.0 | 69.5 | 86.0 | 91.6 | 86.0 | 100.0 | 86.0 |
| P02 | 23.0 | 87.9 | 49.0 | 87.9 | 76.0 | 87.9 | 96.3 | 87.9 |
| P03 | 37.9 | 92.9 | 57.8 | 92.9 | 79.0 | 92.9 | 88.2 | 92.9 |
| P06 | 73.1 | 90.2 | 84.2 | 90.2 | 95.9 | 90.2 | 98.8 | 90.2 |
| P07 | 48.8 | 78.9 | 64.5 | 78.9 | 73.2 | 78.9 | 79.9 | 78.9 |
| P08 | 69.3 | 87.6 | 78.6 | 87.6 | 84.1 | 87.6 | 90.5 | 87.6 |
| P09 | 81.8 | 79.7 | 87.8 | 79.7 | 96.7 | 79.7 | 100.0 | 79.7 |
| Mean (SD) | 55.2 (19.3) | 86.2 (4.8) | 70.2 (13.2) | 86.2 (4.8) | 85.2 (8.9) | 86.2 (4.8) | 93.4 (7.0) | 86.2 (4.8) |
| Pre-FOG (Case 2) | Pre-FOG and Pre-FOG-Transition (Case 3) | Pre-FOG- Transition (Case 4) | FOG (Case 5) | |||||
|---|---|---|---|---|---|---|---|---|
| Held out Test Participant | Sens (%) | Spec (%) | Sens (%) | Spec (%) | Sens (%) | Spec (%) | Sens (%) | Spec (%) |
| P01 | 52.5 | 83.7 | 69.2 | 83.7 | 91.0 | 83.7 | 100.0 | 83.7 |
| P02 | 23.6 | 86.7 | 49.6 | 86.7 | 76.6 | 86.7 | 98.0 | 86.7 |
| P03 | 43.9 | 89.7 | 64.1 | 89.7 | 85.5 | 89.7 | 100.0 | 89.7 |
| P06 | 76.9 | 89.5 | 85.1 | 89.5 | 93.9 | 89.5 | 99.4 | 89.5 |
| P07 | 36.7 | 80.3 | 62.9 | 80.3 | 77.4 | 80.3 | 99.2 | 80.3 |
| P08 | 82.7 | 79.6 | 88.1 | 79.6 | 91.3 | 79.6 | 92.9 | 79.6 |
| P09 | 70.5 | 72.5 | 78.4 | 72.5 | 90.0 | 72.5 | 100.0 | 72.5 |
| Mean (SD) | 55.3 (20.5) | 83.2 (5.7) | 71.0 (12.7) | 83.2 (5.7) | 86.5 (6.4) | 83.2 (5.7) | 98.5 (2.4) | 83.2 (5.7) |
| Pre-FOG (Case 2) | Pre-FOG and Pre-FOG-Transition (Case 3) | Pre-FOG- Transition (Case 4) | FOG (Case 5) | |||||
|---|---|---|---|---|---|---|---|---|
| Held out Test Participant | Sens (%) | Spec (%) | Sens (%) | Spec (%) | Sens (%) | Spec (%) | Sens (%) | Spec (%) |
| P01 | 53.5 | 84.0 | 67.9 | 84.0 | 86.7 | 84.0 | 85.7 | 84.0 |
| P02 | 16.3 | 90.7 | 43.8 | 90.7 | 72.5 | 90.7 | 94.6 | 90.7 |
| P03 | 31.8 | 96.1 | 49.2 | 96.1 | 67.7 | 96.1 | 94.1 | 96.1 |
| P06 | 44.2 | 93.5 | 62.4 | 93.5 | 81.6 | 93.5 | 80.2 | 93.5 |
| P07 | 17.8 | 92.1 | 35.5 | 92.1 | 45.4 | 92.1 | 32.9 | 92.1 |
| P08 | 65.3 | 92.3 | 66.2 | 92.3 | 66.7 | 92.3 | 82.1 | 92.3 |
| P09 | 50.0 | 92.2 | 62.2 | 92.2 | 80.0 | 92.2 | 100.0 | 92.2 |
| Mean (SD) | 39.8 (17.2) | 91.6 (3.4) | 55.3 (11.6) | 91.6 (3.4) | 71.5 (12.7) | 91.6 (3.4) | 81.4 (20.9) | 91.6 (3.4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pardoel, S.; Shalin, G.; Nantel, J.; Lemaire, E.D.; Kofman, J. Early Detection of Freezing of Gait during Walking Using Inertial Measurement Unit and Plantar Pressure Distribution Data. Sensors 2021, 21, 2246. https://doi.org/10.3390/s21062246
Pardoel S, Shalin G, Nantel J, Lemaire ED, Kofman J. Early Detection of Freezing of Gait during Walking Using Inertial Measurement Unit and Plantar Pressure Distribution Data. Sensors. 2021; 21(6):2246. https://doi.org/10.3390/s21062246
Chicago/Turabian StylePardoel, Scott, Gaurav Shalin, Julie Nantel, Edward D. Lemaire, and Jonathan Kofman. 2021. "Early Detection of Freezing of Gait during Walking Using Inertial Measurement Unit and Plantar Pressure Distribution Data" Sensors 21, no. 6: 2246. https://doi.org/10.3390/s21062246
APA StylePardoel, S., Shalin, G., Nantel, J., Lemaire, E. D., & Kofman, J. (2021). Early Detection of Freezing of Gait during Walking Using Inertial Measurement Unit and Plantar Pressure Distribution Data. Sensors, 21(6), 2246. https://doi.org/10.3390/s21062246