
Dual Mode pHRI-teleHRI Control System with a Hybrid Admittance-Force Controller for Ultrasound Imaging



Abstract
:1. Introduction
2. Methods
2.1. Robot Dynamics
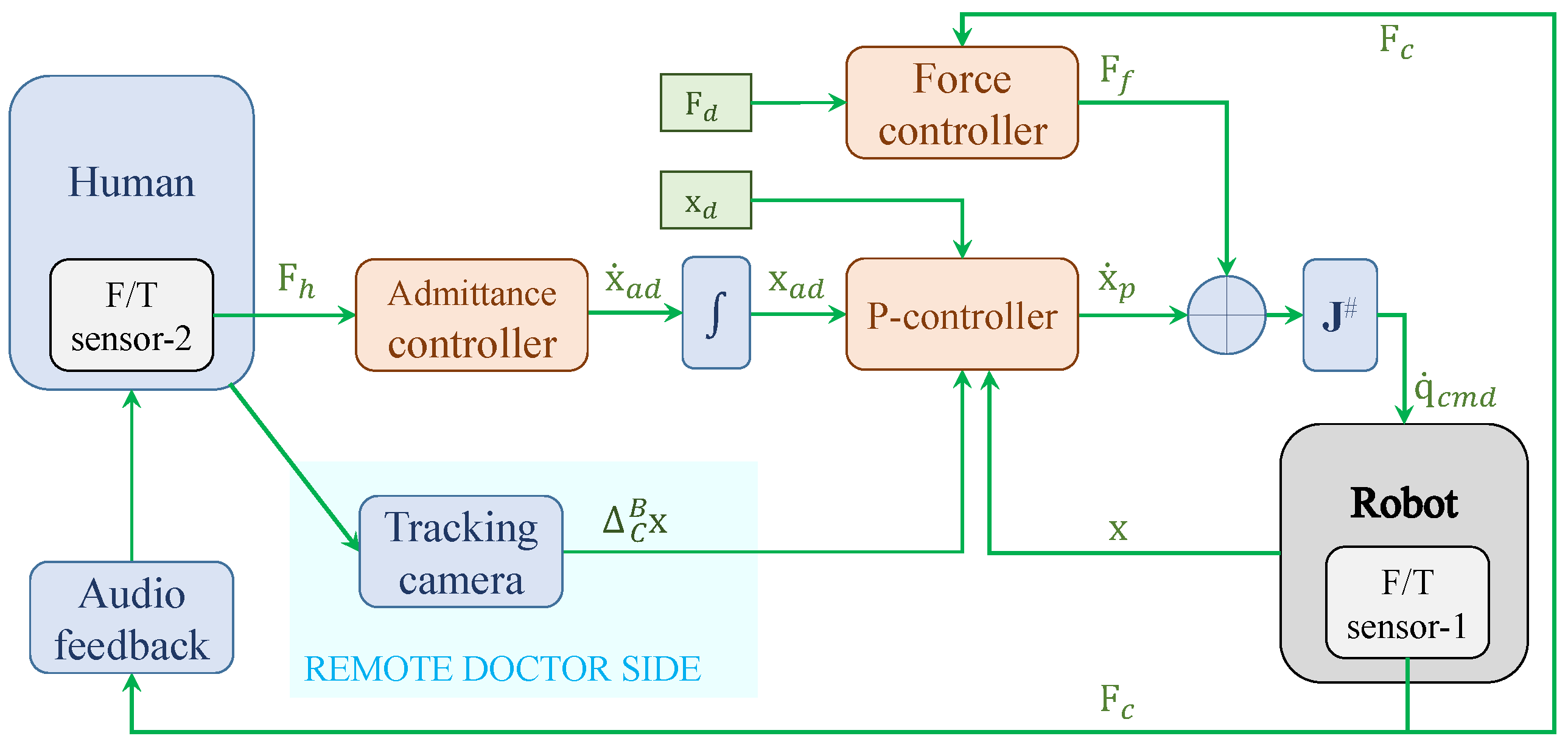
2.2. Admittance Controller for pHRI Mode
2.3. Mapping Algorithm for teleHRI Mode
2.4. Force Controller
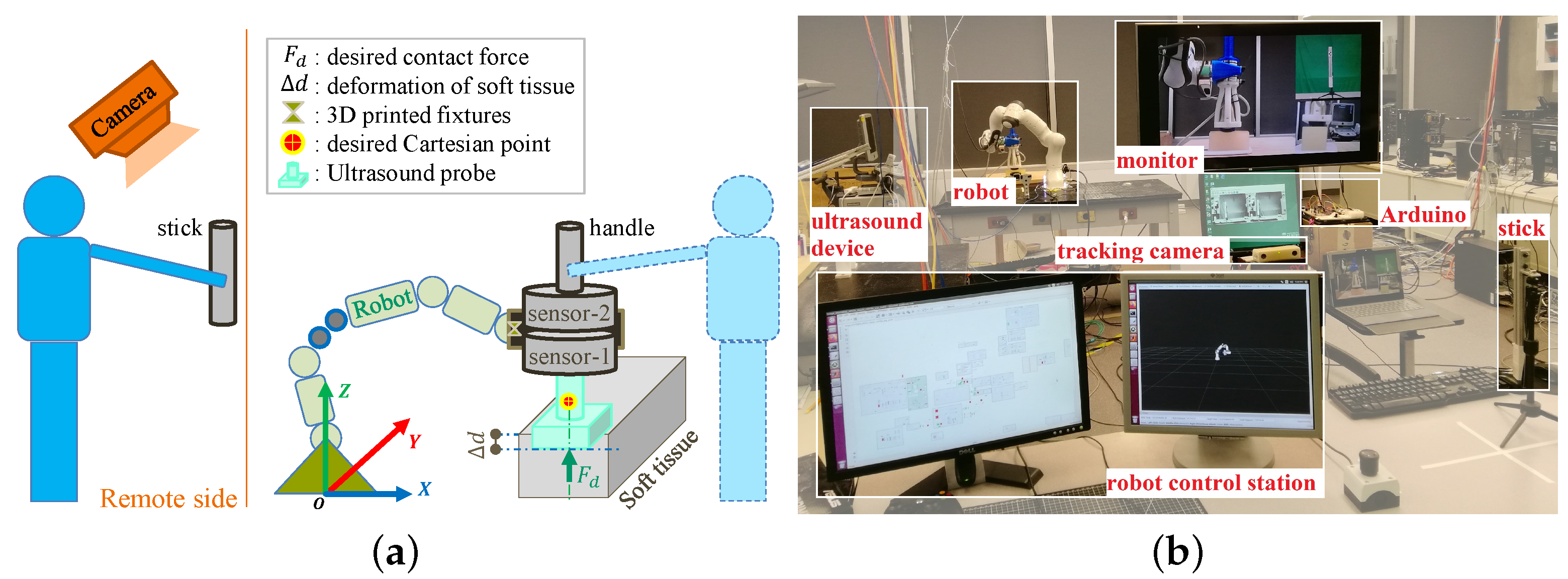
2.5. Apparatus
2.6. Audio Feedback and Haptic Feedback
3. Experiments and Results
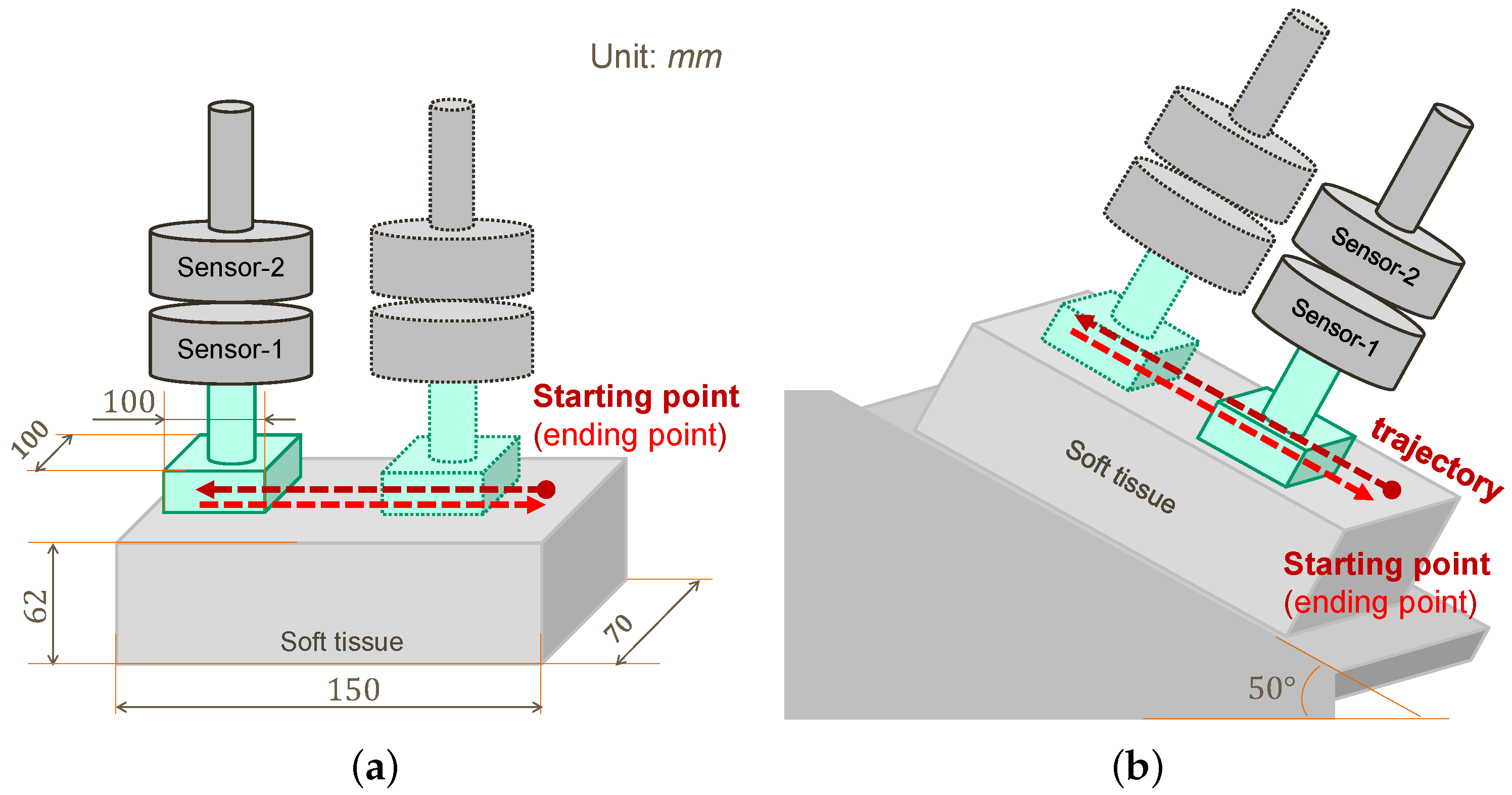
3.1. Procedures and Metrics
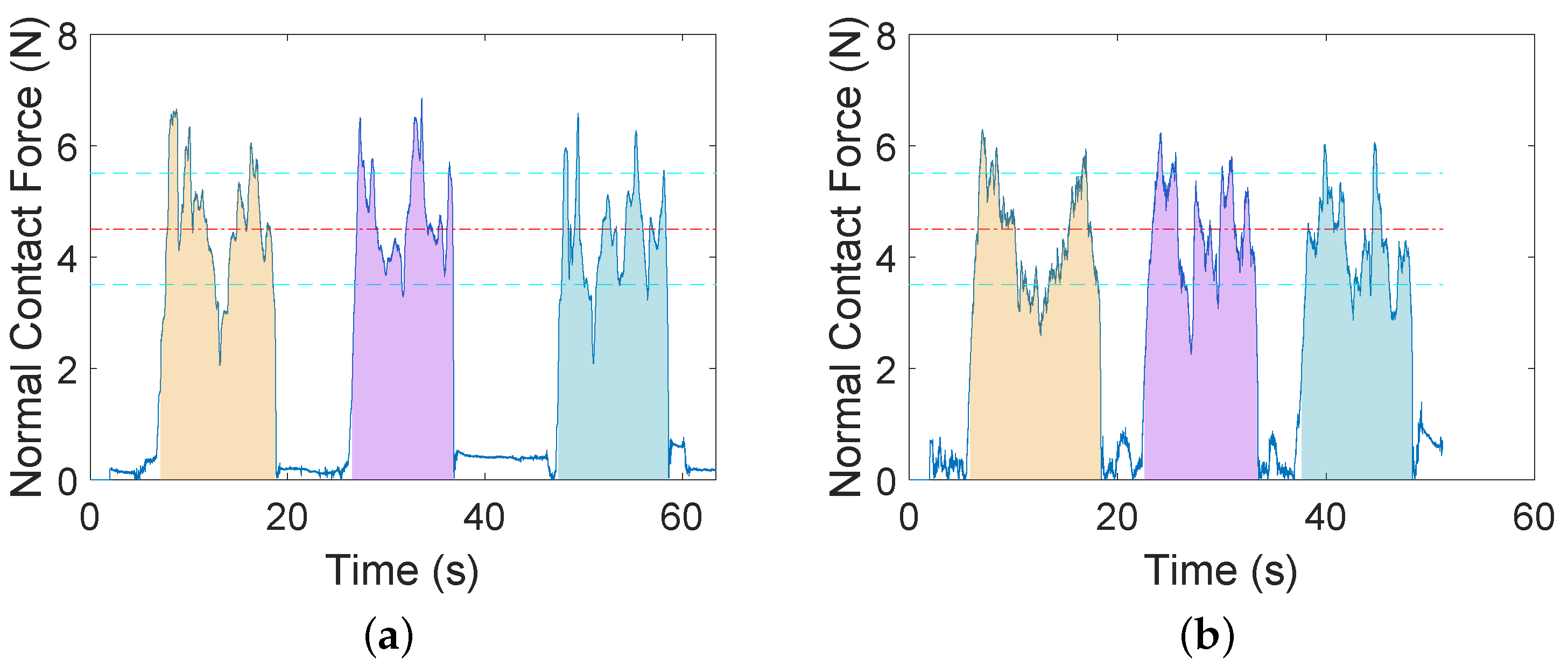
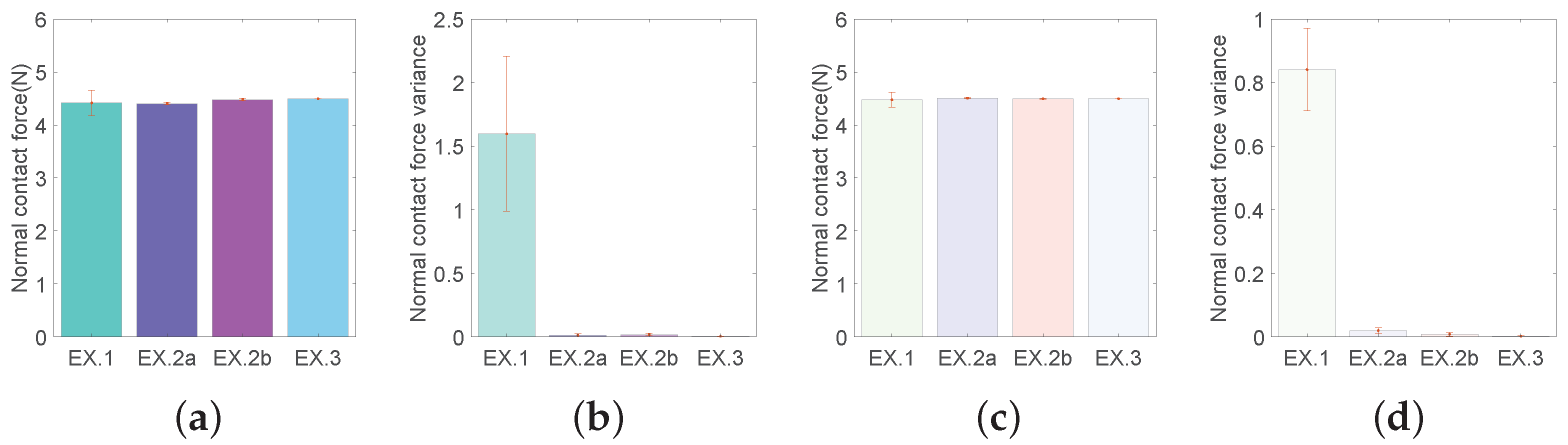
- Normal contact force, mean and variance (squared standard deviation) between the US probe and the soft tissue. The former indicates task performance accuracy while the latter indicates task performance stability.
- User effort, in units of Newton. It is indicated by the force exerted on the robot EE by the human user in pHRI mode, and also serves as input signals for the admittance controller. It is measured by sensor-2, as shown in Figure 1.
- Time percentage. A percentage for retaining the normal contact force within the desired range in one trial.
3.2. Experiment 1: AF vs. AF + HF
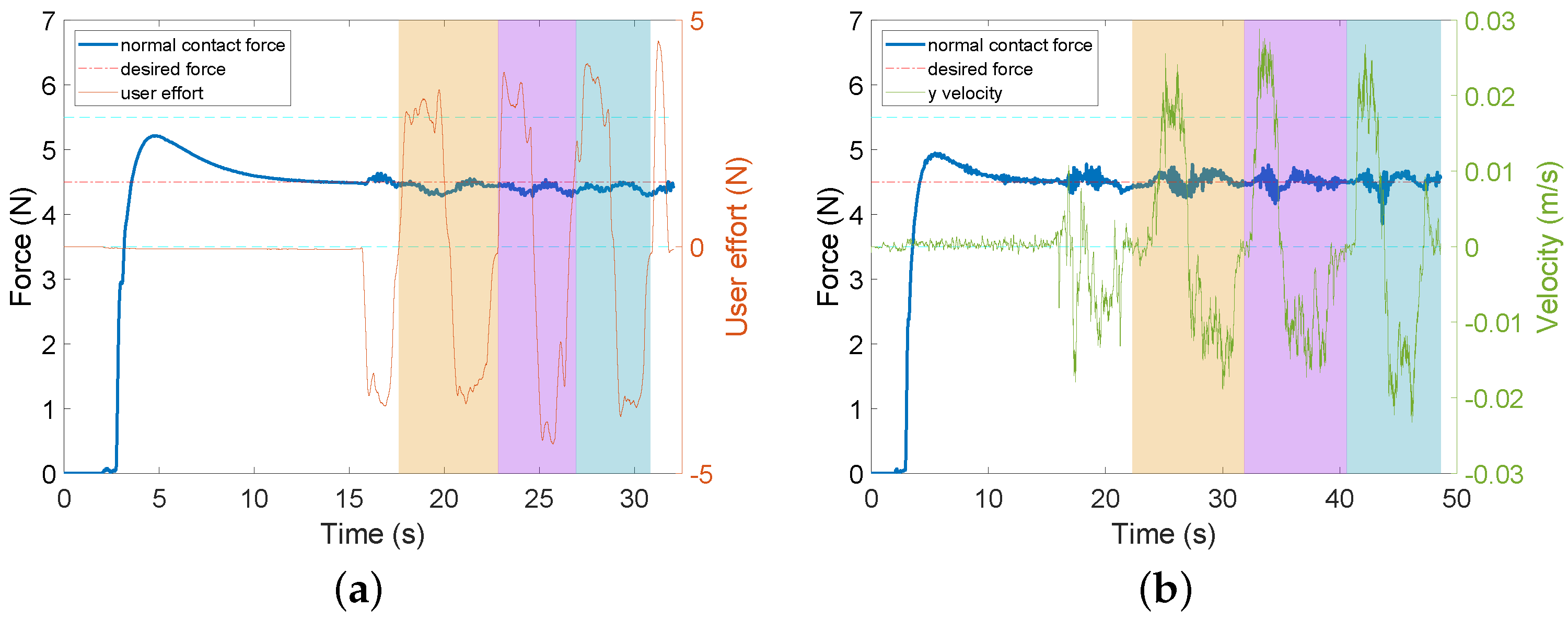
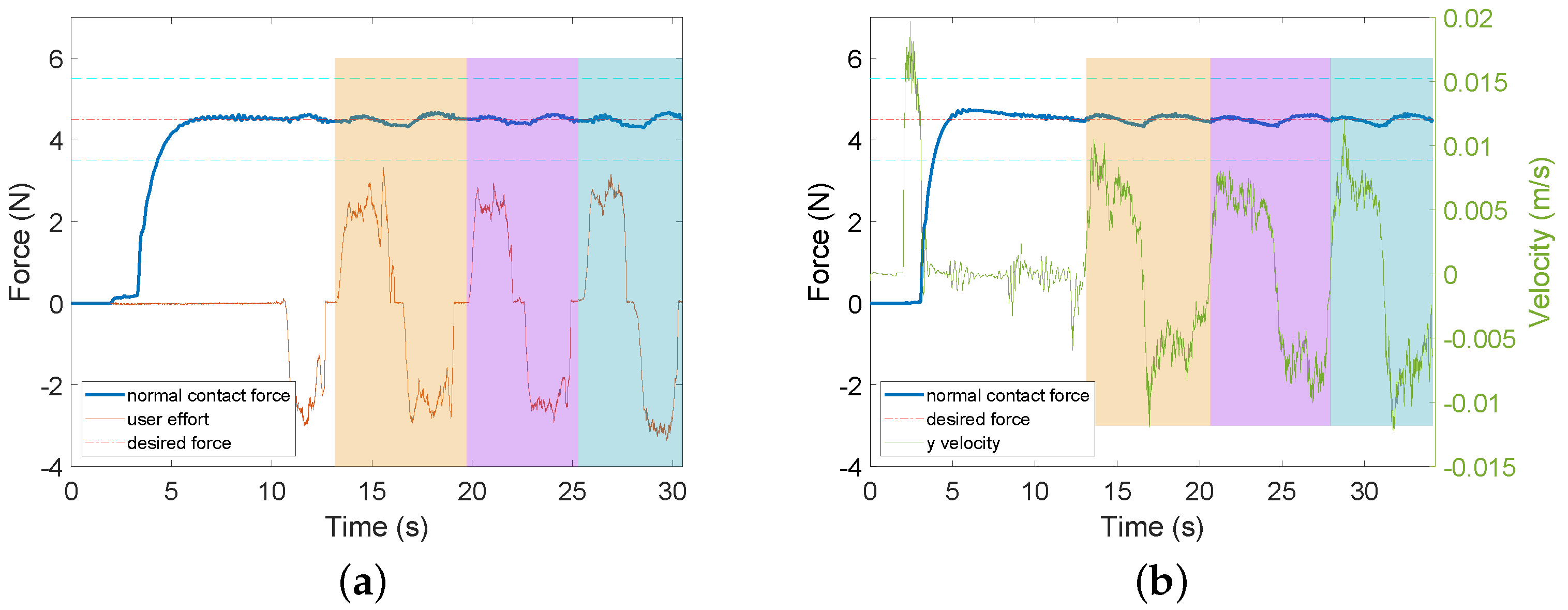
3.3. Experiment 2: AF + FC vs. AF + FC + HF
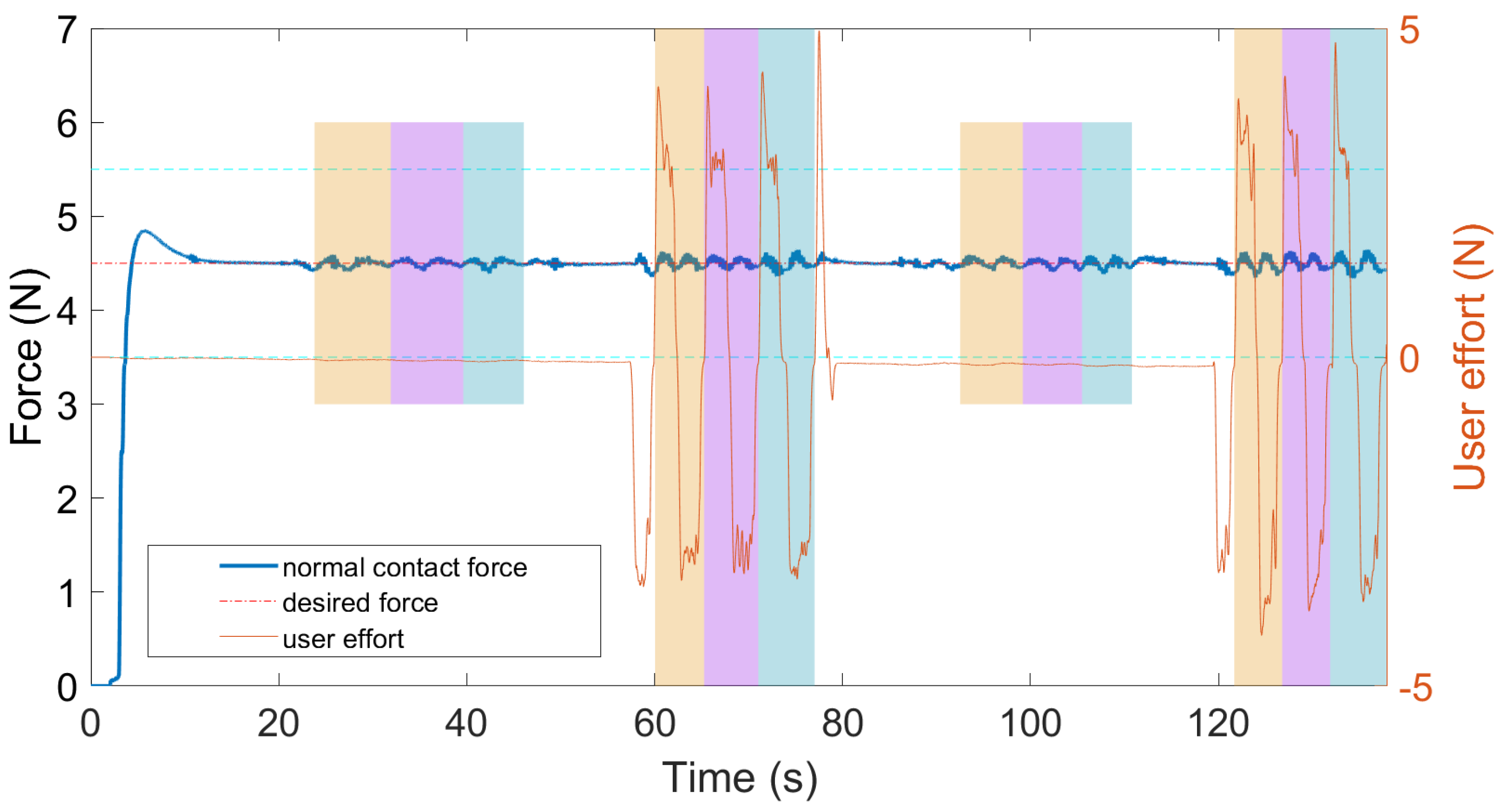
3.4. Experiment 3: Dual-Mode Switching
3.5. Statistical Comparison across Experiments
4. Discussions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean | Variance | ||||
|---|---|---|---|---|---|
| AF + HF (pHRI) | AF (HRI) | AF + HF (pHRI) | AF (HRI) | ||
| (N) | s1 | 4.45 | 4.59 | 2.1316 | 0.9409 |
| s2 | 4.42 | 4.46 | 2.4964 | 0.6561 | |
| s3 | 4.55 | 4.31 | 0.9025 | 0.8100 | |
| s4 | 4.29 | 4.35 | 1.5129 | 0.8464 | |
| s5 | 4.76 | 4.69 | 1.1664 | 1.0404 | |
| s6 | 4.03 | 4.45 | 1.3225 | 0.7744 | |
| (*) | |||||
| Trial 1 | Trial 2 | Trial 3 | Mean ± Std. | ||
|---|---|---|---|---|---|
| pHRI mode (%) | s1 | 55.36 | 51.26 | 47.48 | |
| s2 | 63.52 | 64.64 | 35.83 | ||
| s3 | 62.54 | 72.51 | 75.54 | ||
| s4 | 62.87 | 63.05 | 46.68 | ||
| s5 | 66.73 | 50.50 | 75.56 | ||
| s6 | 53.78 | 59.49 | 50.15 | ||
| (mean ± std.) | |||||
| HRI mode (%) | s1 | 73.91 | 70.40 | 79.09 | |
| s2 | 75.46 | 70.79 | 91.51 | ||
| s3 | 63.92 | 73.29 | 74.15 | ||
| s4 | 64.49 | 72.29 | 80.27 | ||
| s5 | 78.11 | 69.44 | 68.63 | ||
| s6 | 76.31 | 75.85 | 80.72 | ||
| (mean ± std.) | |||||
| Mean | Variance | ||||
|---|---|---|---|---|---|
| AF + FC + HF (pHRI) | AF + FC (HRI) | AF + FC + HF (pHRI) | AF + FC (HRI) | ||
| (N) | s1 | 4.43 | 4.53 | 0.0064 | 0.0121 |
| s2 | 4.41 | 4.51 | 0.0036 | 0.0100 | |
| s3 | 4.41 | 4.50 | 0.0144 | 0.0225 | |
| s4 | 4.42 | 4.49 | 0.0100 | 0.0169 | |
| s5 | 4.36 | 4.51 | 0.0100 | 0.0324 | |
| s6 | 4.39 | 4.52 | 0.0324 | 0.0225 | |
| (*) | |||||
| Mean | Variance | ||||
|---|---|---|---|---|---|
| AF + FC + HF pHRI) | AF + FC (HRI) | AF + FC + HF (pHRI) | AF + FC (HRI) | ||
| (N) | s1 | 4.49 | 4.51 | 0.0289 | 0.0036 |
| s2 | 4.43 | 4.49 | 0.0144 | 0.0025 | |
| s3 | 4.49 | 4.50 | 0.0144 | 0.0121 | |
| s4 | 4.49 | 4.50 | 0.0121 | 0.0064 | |
| s5 | 4.49 | 4.50 | 0.0361 | 0.0081 | |
| s6 | 4.50 | 4.49 | 0.0081 | 0.0196 | |
| Mean | Variance | ||||
|---|---|---|---|---|---|
| pHRI | HRI | pHRI | HRI | ||
| (N) | s1 | 4.50 | 4.50 | 0.0025 | 0.0016 |
| s2 | 4.49 | 4.50 | 0.0049 | 0.0016 | |
| s3 | 4.50 | 4.50 | 0.0036 | 0.0025 | |
| s4 | 4.49 | 4.50 | 0.0064 | 0.0036 | |
| s5 | 4.50 | 4.50 | 0.0049 | 0.0016 | |
| s6 | 4.50 | 4.50 | 0.0049 | 0.0016 | |
| (*) | |||||
| EX.2a | EX.2b | EX.3 | EX.2a | EX.2b | EX.3 | ||
|---|---|---|---|---|---|---|---|
| Mean | Variance | ||||||
| EX.1 | (pHRI) | 0.9031 | 0.5530 | 0.4600 | * | * | * |
| EX.2a | - | * | * | - | 0.4436 | 0.1035 | |
| EX.2b | - | - | 0.1647 | - | - | * | |
| EX.1 | (HRI) | 0.5546 | 0.7033 | 0.6876 | * | * | * |
| EX.2a | - | 0.1099 | 0.1438 | - | * | * | |
| EX.2b | - | - | 0.6109 | - | - | ||
References
- Garzotto, F.; Comoretto, R.I.; Ostermann, M.; Nalesso, F.; Gregori, D.; Bonavina, M.G.; Zanardo, G.; Meneghesso, G. Preventing infectious diseases in Intensive Care Unit by medical devices remote control: Lessons from COVID-19. J. Crit. Care 2021, 61, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Zemmar, A.; Lozano, A.M.; Nelson, B.J. The rise of robots in surgical environments during COVID-19. Nat. Mach. Intell. 2020, 2, 566–572. [Google Scholar] [CrossRef]
- Attanasio, A.; Scaglioni, B.; De Momi, E.; Fiorini, P.; Valdastri, P. Autonomy in surgical robotics. Annu. Rev. Control Robot. Auton. Syst. 2021, 4, 651–679. [Google Scholar] [CrossRef]
- Feizi, N.; Tavakoli, M.; Patel, R.V.; Atashzar, S.F. Robotics and ai for teleoperation, tele-assessment, and tele-training for surgery in the era of covid-19: Existing challenges, and future vision. Front. Robot. AI 2021, 8, 16. [Google Scholar] [CrossRef] [PubMed]
- Welleweerd, M.K.; de Groot, A.G.; de Looijer, S.; Siepel, F.J.; Stramigioli, S. Automated robotic breast ultrasound acquisition using ultrasound feedback. In Proceedings of the 2020 IEEE International Conference on Robotics and Automation (ICRA), Virtual, 31 May–31 August 2020; pp. 9946–9952. [Google Scholar]
- Shah, N.; Bansal, N.; Logani, A. Recent advances in imaging technologies in dentistry. World J. Radiol. 2014, 6, 794. [Google Scholar] [CrossRef] [PubMed]
- Reda, R.; Zanza, A.; Cicconetti, A.; Bhandi, S.; Miccoli, G.; Gambarini, G.; Di Nardo, D. Ultrasound imaging in dentistry: A literature overview. J. Imaging 2021, 7, 238. [Google Scholar] [CrossRef] [PubMed]
- Carriere, J.; Fong, J.; Meyer, T.; Sloboda, R.; Husain, S.; Usmani, N.; Tavakoli, M. An admittance-controlled robotic assistant for semi-autonomous breast ultrasound scanning. In Proceedings of the 2019 International Symposium on Medical Robotics (ISMR), Atlanta, GA, USA, 3–5 April 2019; pp. 1–7. [Google Scholar]
- Fang, T.Y.; Zhang, H.K.; Finocchi, R.; Taylor, R.H.; Boctor, E.M. Force-assisted ultrasound imaging system through dual force sensing and admittance robot control. Int. J. Comput. Assist. Radiol. Surg. 2017, 12, 983–991. [Google Scholar] [CrossRef] [PubMed]
- Akbari, M.; Carriere, J.; Meyer, T.; Sloboda, R.; Husain, S.; Usmani, N.; Tavakoli, M. Robotic Ultrasound Scanning With Real-Time Image-Based Force Adjustment: Quick Response for Enabling Physical Distancing During the COVID-19 Pandemic. Front. Robot. AI 2021, 8, 62. [Google Scholar] [CrossRef] [PubMed]
- Soleymani, A.; Torabi, A.; Tavakoli, M. A Low-cost Intrinsically Safe Mechanism for Physical Distancing Between Clinicians and Patients. In Proceedings of the 2021 IEEE International Conference on Robotics and Automation (ICRA), Xi’an, China, 30 May–5 June 2021; pp. 1–7. [Google Scholar]
- Priester, A.M.; Natarajan, S.; Culjat, M.O. Robotic ultrasound systems in medicine. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2013, 60, 507–523. [Google Scholar] [CrossRef] [PubMed]
- Pierrot, F.; Dombre, E.; Dégoulange, E.; Urbain, L.; Caron, P.; Boudet, S.; Gariépy, J.; Mégnien, J.L. Hippocrate: A safe robot arm for medical applications with force feedback. Med. Image Anal. 1999, 3, 285–300. [Google Scholar] [CrossRef]
- Salcudean, S.E.; Zhu, W.H.; Abolmaesumi, P.; Bachmann, S.; Lawrence, P.D. A robot system for medical ultrasound. In Robotics Research; Springer: London, UK, 2000; pp. 195–202. [Google Scholar]
- Gourdon, A.; Poignet, P.; Poisson, G.; Vieyres, P.; Marche, P. A new robotic mechanism for medical application. In Proceedings of the 1999 IEEE/ASME International Conference on Advanced Intelligent Mechatronics (AIM’99), Atlanta, GA, USA, 19–23 September 1999; pp. 33–38. [Google Scholar]
- Mitsuishi, M.; Warisawa, S.; Tsuda, T.; Higuchi, T.; Koizumi, N.; Hashizume, H.; Fujiwara, K. Remote ultrasound diagnostic system. In Proceedings of the IEEE International Conference on Robotics and Automation (ICRA), Seoul, Korea, 21–26 May 2001; Volume 2, pp. 1567–1574. [Google Scholar]
- Koizumi, N.; Warisawa, S.; Nagoshi, M.; Hashizume, H.; Mitsuishi, M. Construction methodology for a remote ultrasound diagnostic system. IEEE Trans. Robot. 2009, 25, 522–538. [Google Scholar] [CrossRef]
- Duan, B.; Xiong, L.; Guan, X.; Fu, Y.; Zhang, Y. Tele-operated robotic ultrasound system for medical diagnosis. Biomed. Signal Process. Control 2021, 70, 102900. [Google Scholar] [CrossRef]
- Conti, F.; Park, J.; Khatib, O. Interface design and control strategies for a robot assisted ultrasonic examination system. In Proceedings of the Experimental Robotics; Springer: Berlin/Heidelberg, Germany, 2014; pp. 97–113. [Google Scholar]
- Fong, J.; Rouhani, H.; Tavakoli, M. A Therapist-Taught Robotic System for Assistance During Gait Therapy Targeting Foot Drop. IEEE Robot. Autom. Lett. 2019, 4, 407–413. [Google Scholar] [CrossRef]
- Song, P.; Yu, Y.; Zhang, X. A tutorial survey and comparison of impedance control on robotic manipulation. Robotica 2019, 37, 801–836. [Google Scholar] [CrossRef]
- Ott, C.; Mukherjee, R.; Nakamura, Y. Unified impedance and admittance control. In Proceedings of the 2010 IEEE International Conference on Robotics and Automation (ICRA), Anchorage, AK, USA, 3–7 May 2010; pp. 554–561. [Google Scholar]
- Schindlbeck, C.; Haddadin, S. Unified passivity-based cartesian force/impedance control for rigid and flexible joint robots via task-energy tanks. In Proceedings of the 2015 IEEE International Conference on Robotics and Automation (ICRA), Seattle, WA, USA, 26–30 May 2015; pp. 440–447. [Google Scholar]
- Smith-Guerin, N.; Al Bassit, L.; Poisson, G.; Delgorge, C.; Arbeille, P.; Vieyres, P. Clinical validation of a mobile patient-expert tele-echography system using ISDN lines. In Proceedings of the 4th International IEEE EMBS Special Topic Conference on Information Technology Applications in Biomedicine (ITAB), Birmingham, UK, 24–26 April 2003; pp. 23–26. [Google Scholar]
- Gilbertson, M.W.; Anthony, B.W. An ergonomic, instrumented ultrasound probe for 6-axis force/torque measurement. In Proceedings of the 2013 35th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Osaka, Japan, 3–7 July 2013; pp. 140–143. [Google Scholar]
- Salcudean, S.E.; Bell, G.; Bachmann, S.; Zhu, W.H.; Abolmaesumi, P.; Lawrence, P.D. Robot-assisted diagnostic ultrasound–design and feasibility experiments. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention—MICCAI’99; Springer: Berlin/Heidelberg, Germany, 1999; pp. 1062–1071. [Google Scholar]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, T.; Meng, X.; Tavakoli, M. Dual Mode pHRI-teleHRI Control System with a Hybrid Admittance-Force Controller for Ultrasound Imaging. Sensors 2022, 22, 4025. https://doi.org/10.3390/s22114025
Li T, Meng X, Tavakoli M. Dual Mode pHRI-teleHRI Control System with a Hybrid Admittance-Force Controller for Ultrasound Imaging. Sensors. 2022; 22(11):4025. https://doi.org/10.3390/s22114025
Chicago/Turabian StyleLi, Teng, Xiao Meng, and Mahdi Tavakoli. 2022. "Dual Mode pHRI-teleHRI Control System with a Hybrid Admittance-Force Controller for Ultrasound Imaging" Sensors 22, no. 11: 4025. https://doi.org/10.3390/s22114025
APA StyleLi, T., Meng, X., & Tavakoli, M. (2022). Dual Mode pHRI-teleHRI Control System with a Hybrid Admittance-Force Controller for Ultrasound Imaging. Sensors, 22(11), 4025. https://doi.org/10.3390/s22114025